
Abstract
Interest has grown in the effects of psilocybin on mental health, but little is known about its naturalistic use alongside alcohol and its relationship to depression and/or anxiety symptoms. Data from the nationally-representative 2024 National Survey Investigating Hallucinogenic Trends of participants who did (n = 1234) or did not (n = 1607) report past-year psilocybin and alcohol co-use were compared on depressive and anxiety symptoms and poor mental health days. Weighted regressions adjusted for age, sex, survey collection period, race, ethnicity, and past-year cannabis and other psychedelic use. Individuals with psilocybin and alcohol co-use had fewer depressive symptoms (B(SE) = −.57(.28), β = −.04, p = .043) than those who used alcohol without psilocybin, suggesting potential benefits of psilocybin in individuals with co-use. After removing cannabis and other psychedelic use covariates, psilocybin use was also related to lower anxiety symptoms. However, given the observational and self-report study design, causal inferences cannot be made. Thus, longitudinal and experimental studies are needed.
Introduction
Psilocybin is a naturally-occurring psychedelic substance that can be derived from over 200 mushroom species (colloquially known as “magic mushrooms”: Rodríguez Arce & Winkelman, 2021). When ingested, it metabolizes into psilocin, a psychoactive compound that acts as an agonist at serotonin receptors, particularly 5-HT2A (Vollenweider & Kometer, 2010). Psilocybin has been used for thousands of years in various indigenous cultures to induce altered states of consciousness (Nichols, 2020). Additionally, a growing literature has shown its therapeutic promise for modern behavioral medicine (Lowe et al., 2021).
Despite its potential therapeutic benefits, psilocybin has been classified as a Schedule I drug in the United States since 1970. Schedule I is the most restrictive category under the Controlled Substances Act (CSA) (Lowe et al., 2021) and pertains to “drugs with no currently accepted medical use and a high potential for abuse” (Drug Enforcement Agency, 2025). However, as recently as 2019, U.S. cities (e.g., Denver, Oakland, Washington, D.C.) and states (e.g., Colorado, Oregon, and New Mexico) began to decriminalize the possession, use, and cultivation of psilocybin (Psychedelic Alpha, 2025), reinvigorating scientific research on psychedelics and their use in therapeutic settings.
Additionally, psilocybin use has become more prevalent in the U.S. For example, lifetime psilocybin use increased by 2.1% in U.S. adults from 2019 to 2023 (Rockhill et al., 2025) and over 7 million U.S. adults reported past-year psilocybin use in 2023-2024 (Hutchison et al., 2025). Compared to other psychedelics and some psychiatric medications, psilocybin has a favorable safety profile, low likelihood of dependence and addiction, and demonstrated efficacy in treating some mental health conditions (Hodge et al., 2023).
Whereas psilocybin is stigmatized, alcohol is one of the most commonly used substances worldwide and poses substantial risk to human health. While the prevalence of alcohol use has been declining in U.S. adults, it is still the most commonly used substance as of 2024 (Patrick et al., 2025). According to the 2024 National Survey on Drug Use and Health (NSDUH), 62.0% and 46.6% of people aged 12 years and over reported that they drank alcohol at least once during the past year and past month, respectively (National Institute on Alcohol Abuse and Alcoholism, 2025). Alcohol is a major contributor to the global burden of disease; is causally linked to more than 200 disease, injury, health condition, and mortality outcomes; and also poses myriad health risks to not only the user but to those around them (Rehm et al., 2017). Notably, alcohol use plays a role in negative mental health outcomes such as depression and anxiety (Rehm et al., 2017). Drinking to cope with negative emotions (Cooper, 1994) has especially been linked to drinking problems, emotional distress, more anxiety and depressive symptoms, and increased alcohol consumption in the long term for young people (Bresin & Mekawi, 2021; D’Aquino & Callinan, 2024; Holahan et al., 2001). Other work suggests that a broader tendency toward negative emotionality in young adults is linked to these coping motives for drinking alcohol (Moss et al., 2025).
Given the detrimental effects of alcohol and growing attention to psilocybin as a treatment for mental health disorders, it is important to investigate the associations that psilocybin and alcohol co-use have with mental health symptoms. A majority (57.1%) of participants in the 2023 Global Psychedelic Survey reported that they used both alcohol and psychedelics (Lake & Lucas, 2025). Of all 11 psychedelics surveyed, psilocybin was used by the most respondents (90.8%; Lake & Lucas, 2024). Literature comparing the co-use of different psychedelics with alcohol is limited, but a meta-analysis of seven preclinical trials showed that psilocybin appears to demonstrate the most potential for reduced depressive and anxiety symptoms and decreased alcohol consumption out of several types of psychedelics (Calleja-Conde et al., 2022).
Much of the work on the potential impact of psychedelics on mental health and alcohol use has been conducted in clinical settings, rather than on naturalistic use in non-clinical populations. For instance, Goodwin et al. (2023) found that patients with treatment-resistant depression had improved depression severity and anxiety three weeks after psilocybin dosing. Furthermore, a review by Min et al. (2024) supports that psilocybin reduces the reactivity of the amygdala to negative stimuli for mood disorders and may work alongside selective serotonin reuptake inhibitors (SSRIs) to reduce depressive symptoms. A meta-analysis also found that across multiple studies, psilocybin combined with behavioral interventions was effective in reducing anxiety and depression symptoms in samples with clinically-elevated mental health symptoms (Goldberg et al., 2020). Finally, a meta-analysis by Metaxa and Clarke (2024) suggested that psilocybin significantly reduced depression symptoms compared to placebo treatments in seven of nine included studies, but that its efficacy may vary by depression type, age, prior psychedelic use, and depression measurement method.
Naturalistic studies, of which there are few, generally indicate that psilocybin is associated with positive mental health and lower substance misuse. For example, one naturalistic study prospectively followed participants from before to after a planned single-dose session of psilocybin use. Participants showed mean reductions in symptoms of anxiety, depression, and alcohol misuse that persisted 2-3 months after the psilocybin dose. Of note, this study also found that some participants (7-11%) reported persistent negative mental health (mood fluctuations and depressive symptoms) after psilocybin use (Nayak et al., 2023). Further, survey-based research on naturalistic use suggests that when individuals use psychedelics, they may decrease their use of other substances, which could contribute to or explain observed symptom changes (Garcia-Romeu et al., 2020).
However, there is mixed evidence regarding the association between naturalistic use of psychedelics (including psilocybin) with mental health and problematic substance use. A study by Black et al. (2025) assessed mental health indicators in the general adult population when psychiatric illnesses and the naturalistic use of psychedelics [including 3,4-Methylenedioxymethamphetamine (MDMA) and “classic” psychedelics such as psilocybin, lysergic acid diethylamide (LSD), and dimethyltryptamine (DMT)] were both present. In adults with psychiatric histories, Black et al. (2025) found that those who had used psychedelics had indicated higher levels of problematic substance use. However, when examining whether psychedelic use amplified these associations, the authors did not find evidence of a stronger combined effect (unlike stimulant or opioid use, which did show significant interaction effects). Importantly, another recent study using NSDUH data found that individuals with mental health struggles or substance use were more likely to use psychedelics (Ahmed et al., 2025). Based on these findings, it is possible that individuals may self-medicate with psychedelics, which raises questions about bidirectionality or a cyclical effect in the relation between psychedelic use and mental health.
It must be emphasized that the current psilocybin literature faces many limitations in terms of generalizability to non-clinical populations and to naturalistic use. For example, clinical trials examining the potential benefits of psilocybin typically have small sample sizes and participants who, by virtue of being in a clinical trial, are not representative of the general population (Halma et al., 2025). One recent systematic review and meta-analysis of studies of psilocybin-assisted therapy for depression confirmed that most trials have had small sample sizes (12-233 participants) (Singleton et al., 2025), highlighting the need for larger, more representative samples. To our knowledge, the Global Psychedelic Survey (Lake & Lucas, 2024) and NSDUH are the only two sources of data on psilocybin and alcohol use using observational design among large non-clinical populations.
A lack of understanding about the potential harms of alcohol and psilocybin co-use restricts the development of public health and harm reduction strategies. Harm-reduction frameworks emphasize that understanding real-world patterns of use is essential to mitigate acute harms and longer-term consequences (Marlatt, 1996). Given the high prevalence of alcohol use, recent increases in psilocybin use, and the limited literature regarding the naturalistic use of psilocybin and its impact on mental health in a broader population, there is critical need to investigate the relationship between psilocybin and alcohol co-use on mental health symptoms. The National Survey Investigating Hallucinogenic Trends (NSIHT) is a novel dataset which can be used to address these gaps in the literature (National Survey Investigating Hallucinogenic Trends (NSIHT), 2024). Thus, the current study of adults who used both alcohol and psychedelics assessed the extent to which mental health indicators differ between individuals who do and do not use psilocybin among a broader sample of individuals with past-year psychedelic use. Thus, the primary purpose of the study was to identify associations between co-use and mental health symptoms, and rather than capture differences between psychedelic users and non-users, we characterized differences related to psilocybin use within alcohol users. Specifically, based on the potential therapeutic benefits of psilocybin in clinical populations, we hypothesized that individuals who use both psilocybin and alcohol would have better self-reported mental health indicators than individuals who use alcohol but do not use psilocybin.
Methods
Cross-sectional survey data were from the nationally-representative 2024 National Survey Investigating Hallucinogenic Trends (NSIHT) that aims to provide population health monitoring focused on U.S. adults who actively use psychedelics across all 50 U.S. states. NSIHT is administered twice yearly by Rocky Mountain Poison & Drug Safety. The current study used data from Quarters 2 and 4 of 2024, the first year of survey administration. The survey used quota sampling to ensure that survey respondents were nationally representative and proportional across six geographic strata, by sex (two strata; male/female), and by age (two strata split at 35 years old). Participants in Colorado and Oregon were oversampled given that these states have the most permissive laws regarding psychedelic use, though oversampling was corrected back down with data weights. Data were weighted using a transport weighting scheme to account for selection biases that might make the sample different from the general population in demographics, health, and/or substance use metrics.
To be eligible for NSIHT, survey participants had to have used at least one psychedelic substance in the past 12 months and be at least 18 years old. Participants were excluded if they showed careless or inattentive response patterns, such as too-brief response time to questions, long sequences of the same answer to drug endorsement questions, and inconsistency in (i.e., a weak correlation between) responses to mental health questions (Ward & Meade, 2023). Careless response exclusions have been demonstrated to be particularly important in these NSIHT data (Black, Rockhill, et al., 2025). The current study further limited the sample to participants who had consumed alcohol at least 12 times in the past 12 months (n = 2841). Within this sample of individuals with any past year psychedelic use, the primary analyses compared those who used alcohol without psilocybin co-use (AP-; n = 1607) to those who co-used alcohol and psilocybin at least once in the past year (AP+; n = 1234).
Measures
Psilocybin Use
Participants were asked: “In the last 12 months have you taken the following psychedelics?/Psilocybin (Magic Mushrooms, Shrooms) or Psilocin? Please say yes even if just once or just a little bit” (coded 0 = “no,” 1 = “yes”). Frequency of psilocybin use was assessed with the following question: “How often have you taken Psilocybin (Magic Mushrooms, Shrooms) or Psilocin in the last 12 months? Pick the best answer.” Answer options were: Once, Several Times, About Monthly, About Weekly, or Daily.
For exploratory analyses, these answers were used to define a 3-category measure of co-use frequency. Each category was as follows: no co-use (if a participant answered that they did not use psilocybin), low-frequency co-use (if a participant responded that they had used psilocybin Once or Several Times), and high-frequency co-use (if a participant responded that they had used psilocybin About Monthly, About Weekly, or About Daily).
Mental Health
Anxiety Symptoms
Using the Generalized Anxiety Disorder 7-item scale (GAD-7) (Spitzer et al., 2006) participants indicated the frequency with which they had experienced each of seven symptoms in the past two weeks [Not at all (0), Several Days (1), More than half the days (2), or Nearly every day (3)]. The sum (range of 0–21) was used as the measure of anxiety symptoms.
Depressive Symptoms
The Patient Health Questionnaire-9 (PHQ-9) (Kroenke et al., 2001) assesses depressive symptoms over the past two weeks. The sum of participants’ responses on nine symptom frequency items [Not at all (0), Several Days (1), More than half the days (2), or Nearly every day (3)] was used to measure participants’ severity of depression (range of 0–27).
Poor Mental Health Days
Participants responded to the following question, taken from the 2019 Behavioral Risk Factor Surveillance System (BRFSS) using a scale of 0–30 days: “Now thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?” (Centers for Disease Control (CDC), 2020).
Covariates
Covariates were age in years (whole number), sex assigned at birth (0 = male, 1 = female), racial identity (0 = no, 1 = yes for each identity: American Indian/Alaska Native, Asian, Black or African American, Native Hawaiian or Other Pacific Islander, white, and Other), ethnicity (0 = not Hispanic or Latino, 1 = Hispanic or Latino), quarter of survey collection (Quarter 2 or Quarter 4 of 2024), past-year use of cannabis (0 = none, 1 = at least once), and use of a psychedelic other than psilocybin (0 = none, 1 = at least once). These other psychedelics included: ayahuasca, dimethyltryptamine (DMT), ketamine/esketamine, ibogaine, lysergic acid diethylamide (LSD), 3,4-methylenedioxymethamphetamine (MDMA), 3,4-methylenedioxyamphetamine (MDA), peyote, San Pedro, synthetic mescaline, phencyclidine (PCP), Salvia divinorum, 4-bromo-2,5-dimethoxyphenethylamine (2C-B), 5-methoxy-N, N-dimethyltryptamine (5-MeO-DMT). Further information on the prevalence of use of these psychedelics in the current sample is available in the 2024 NSIHT report (Rocky Mountain Poison & Drug Safety, 2025).
Data Analysis
Study, methods, and hypotheses were pre-registered in the Open Science Framework (OSF) in October 2025. For the primary analyses, three linear regressions with data response weights were run to determine whether there were differences between the alcohol with psilocybin co-use (AP+) and alcohol without psilocybin co-use (AP-) groups on anxiety symptoms, depressive symptoms, and poor mental health days, after adjusting for covariates to isolate the effects of co-use patterns. Linear regression was selected to accommodate continuous variables, and the data were weighted to mitigate selection bias and strengthen generalizability to the national population in terms of demographics, health, and/or substance use metrics. This weighting scheme is consistent with prior work (Black et al., 2019) and recommendations from the NSIHT study developers.
Follow-up analyses then removed cannabis and other psychedelic use covariates from each model to examine whether any group differences on mental health symptoms shown in the primary models were partially explained by other substance use. This analysis also permits examination of true naturalistic differences between the groups, allowing that co-occurring use of cannabis and other psychedelics may be components of a broader behavioral phenotype associated with psilocybin co-use.
Exploratory analyses further parsed these groups, to determine whether the frequency of past-year psilocybin use was related to participants’ mental health. Three weighted linear regressions were used to compare the three-category co-use groups (AP−, alcohol with low frequency psilocybin co-use, and alcohol with high frequency psilocybin use). As with the primary analyses, follow-up analyses were run without cannabis and other psychedelic use covariates in each model.
Results
Descriptive Statistics
Descriptive Statistics
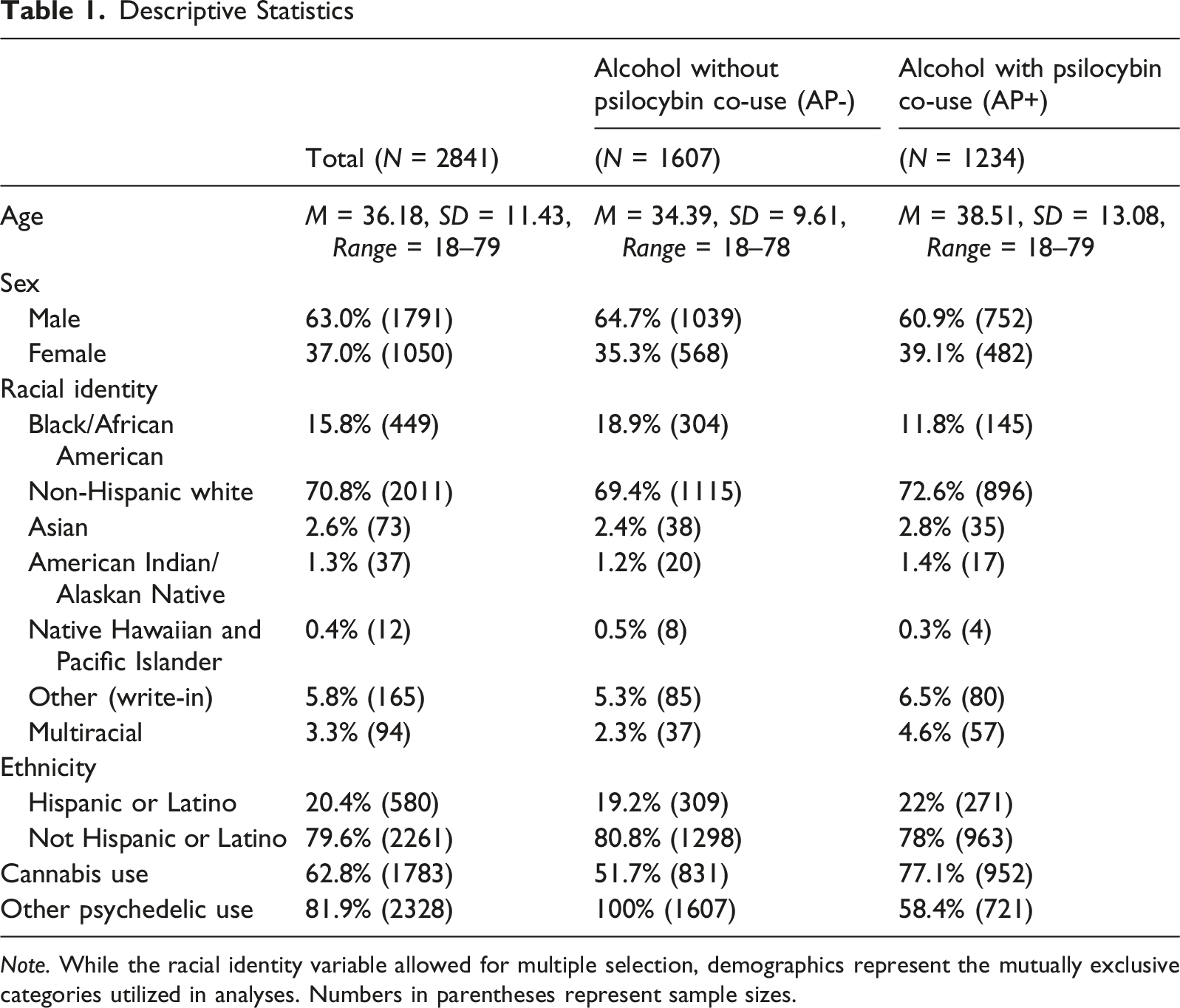
Note. While the racial identity variable allowed for multiple selection, demographics represent the mutually exclusive categories utilized in analyses. Numbers in parentheses represent sample sizes.
Associations Between Alcohol and Psilocybin Co-Use and Mental Health Symptoms
Weighted Linear Regressions Comparing the Alcohol Without Psilocybin Co-use (AP-) Group and the Alcohol-Psilocybin Co-use Group (AP+) on Mental Health Symptoms
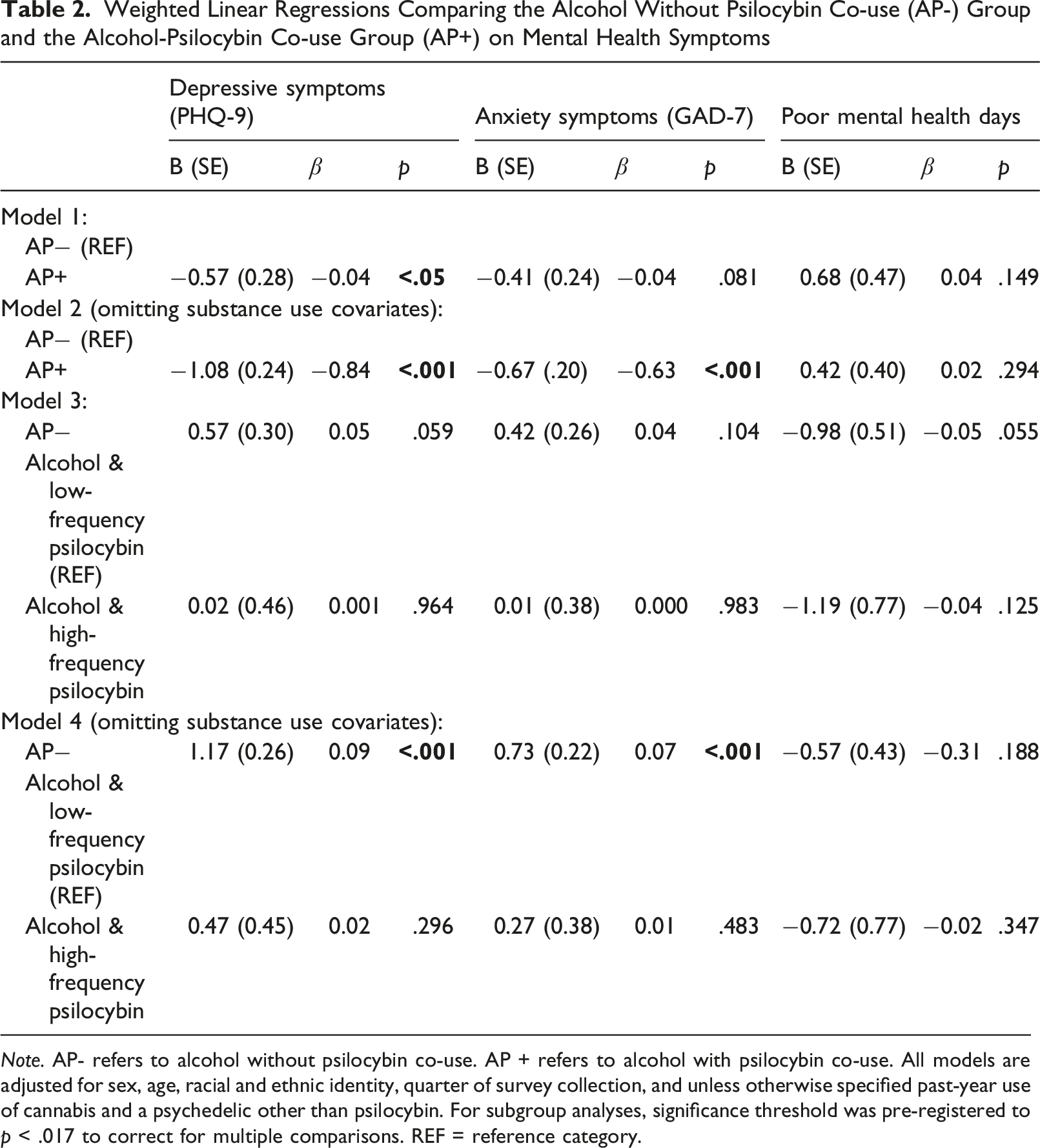
Note. AP- refers to alcohol without psilocybin co-use. AP + refers to alcohol with psilocybin co-use. All models are adjusted for sex, age, racial and ethnic identity, quarter of survey collection, and unless otherwise specified past-year use of cannabis and a psychedelic other than psilocybin. For subgroup analyses, significance threshold was pre-registered to p < .017 to correct for multiple comparisons. REF = reference category.
In follow-up analyses that did not adjust for cannabis and other psychedelic use, the AP + group had significantly lower depression (B(SE) = −1.08(.24), β = −0.08, p < .001) and anxiety (B(SE) = −0.67(0.20), β = −0.06, p < .001) scores than the AP− group (reported in Table 2). There were no significant group differences on poor mental health days [Table 2 about here].
Exploratory Subgroup Analyses
Exploratory analyses that included substance use covariates did not support significant differences among the co-use frequency groups on the mental health symptoms (Table 2).
Next, these analyses were re-run without adjusting for cannabis and other psychedelic use. Group differences on depressive and anxiety symptoms were primarily explained by low rather than high frequency psilocybin co-use. Specifically, AP- participants experienced greater depressive symptoms (B(SE) = 1.17(0.26), β = 0.09, p < .001) and anxiety symptoms (B(SE) = 0.73(0.22), β = 0.07, p < .001) than those who used alcohol with low frequency psilocybin, whereas the low and high frequency psilocybin groups did not differ. There were no significant group differences on poor mental health days.
Discussion
There has been growing interest over the past two decades in the clinical potential of psilocybin to treat mental health disorders. At the same time, psilocybin use has escalated among the general population (Rockhill et al., 2025), indicating the need to investigate naturalistic use along with commonly used substances, such as alcohol. In the current study, we used data from a nationally-representative sample of adults who use hallucinogens in the past year to examine how alcohol and psilocybin co-use versus alcohol without psilocybin co-use relates to depression, anxiety, and poor mental health days.
Individuals who regularly used alcohol and had used psilocybin at least once in the past year reported lower depression than those who used alcohol without psilocybin, but there were no group differences on anxiety or poor mental health days. In secondary analyses that did not adjust for cannabis and other psychedelic use, individuals with psilocybin co-use had significantly lower depression and anxiety scores. Given that cannabis and other psychedelic use effects were in the opposite direction (associated with poorer mental health symptoms), the inclusion of these covariates may suppress the effects of psilocybin and alcohol co-use associations with lower depression and anxiety symptoms.
These findings are consistent with growing clinical trial research suggesting that psilocybin may lead to improvements in anxiety and depression (Goldberg et al., 2020; Singleton et al., 2025), and extends prior evidence that similar associations may be observed in alcohol-using individuals (Daroui et al., 2025). In addition, whereas the primary analyses isolated the effects of psilocybin and alcohol co-use on mental health, the follow-up analyses with substance use covariates removed may better generalize to the real-world context of co-use (without controlling for other polysubstance use) and its relationship with mental health.
Exploratory subgroup analyses that parsed out frequency of psilocybin use suggested that the main mental health results were primarily explained by low rather than high frequency psilocybin co-use. This preliminary finding coincides with previous evidence that indicates occasional, intentional psychedelic use may be associated with more favorable psychological outcomes than high-frequency use (Lake & Lucas, 2024; St. Arnaud & Sharpe, 2023). It is critical to evaluate frequency of substance use in research studies within real-world settings, as this suggests that the mental health benefits of psilocybin that are observed in clinical contexts may not be uniformly applicable across all patterns of psilocybin use.
Given this complexity, it is important to note that frequency of use is only one dimension of naturalistic psilocybin use, and it does not capture the highly variable contexts, motivations, and doses associated with real-world consumption. A recent latent profile analysis of nonclinical psilocybin users has identified distinct use patterns defined by the intersection of frequency and quantity (Gray et al., 2025). For instance, individuals may use psilocybin at high frequencies (e.g., multiple times a week) but in very small, sub-perceptual amounts; these “microdosers” are often motivated by self-improvement, productivity, or emotional regulation. Conversely, others may use psilocybin infrequently (e.g., a few times a year) but ingest larger “macrodoses” for spiritual, recreational, or therapeutic purposes, sometimes seeking a psychological reset to alleviate mental health symptoms. A third group (“chippers”) may use light-to-moderate doses infrequently to influence mood at certain social events. The NSIHT survey did not assess doses or use context; however, we speculate that the low-frequency group driving our results likely encompasses a heterogeneous mix of occasional recreational users and those taking infrequent therapeutic macrodoses. Consequently, readers should interpret these frequency findings with caution, as frequency alone does not fully encapsulate the complex dose and setting effects of naturalistic psilocybin use. Future studies should prioritize examining these associations.
Psilocybin may be associated with lower depressive symptoms among alcohol-using individuals for several reasons. Psilocybin has been shown to promote cognitive flexibility and emotional openness (Min et al., 2024; Reiff et al., 2020), and also appears to acutely alter emotional processing, including reduced recognition to negative emotional cues. Neuroscientific research highlights that psilocybin may stimulate the 5-HT2A/1A receptor and reduce feelings of social exclusion (Preller et al., 2016) and also lower amygdala reactivity after negative stimuli (Kraehenmann et al., 2015), which may be particularly relevant given the link between social stress, negative affect, and alcohol use patterns (Colder & Chassin, 1993; de Wit et al., 2003; Keyes et al., 2011). Furthermore, some research has suggested that mystical experiences are associated with symptom improvement, but these relationships remain correlational and may reflect broader psychological processes rather than a single causal mechanism (Kangaslampi, 2023). Together, these mechanisms may contribute to better mental health among individuals who co-use psilocybin and alcohol, particularly when the use of psilocybin is infrequent, as suggested in the present exploratory analyses.
Study Limitations
There are various limitations to be considered when interpreting the findings of this study. First, the data are cross-sectional, preventing causal inferences regarding psilocybin use and mental health symptoms. These questionnaires relied on self-report, which made them susceptible to both social desirability and recall bias. Although participation was anonymous, it is possible that participants may have felt hesitant to disclose their true psilocybin, cannabis, or alcohol use due to the illicit or stigmatized nature of this behavior in many states. The nature of the questions may have also facilitated recall bias: it may not be a reasonable assumption that participants would have been accurately able to remember details of their substance use over the past 12 months. Further, although the NSIHT study strategically uses broad recruitment strategies to obtain a nationally representative sample of adults with past-year hallucinogen use, and NSIHT data are weighted for race/ethnicity, but this sample was predominantly white and male. Future studies could also enhance recruitment of more diverse populations to better understand the relationship between psilocybin use and mental health among racial, ethnic, and gender minority individuals. In addition, because NSIHT only samples adults who have used hallucinogens, it was not possible to make comparisons to individuals who had only used alcohol without any other psychedelic use. Moreover, as this dataset did not include any substance-naïve individuals, we were unable to compare mental health indicators to a non-user group. Lastly, exact alcohol and other substance use consumption (e.g., frequency, volume, potency) was not specifically quantified in the survey. This lack of specificity limits the ability to determine how different patterns and quantities of co-use relate to mental health symptoms.
Future Directions
Subsequent studies on age-related and motivational differences in psilocybin use could help identify who may experience benefits versus harms. As Hutchison et al. (2025) note, psilocybin use is rising for many adult age groups, yet motivations and outcomes may differ between younger and older individuals. Understanding these distinctions could inform age-specific harm reduction and education strategies.
Furthermore, it is important to examine recreational versus therapeutic use of psilocybin to clarify its associations with mental health, as well as patterns of co-use. More studies are needed to evaluate the risks of psilocybin use and potential adverse psychological effects in naturalistic settings. Building on recent recommendations (Hutchison et al., 2025), future work should also prioritize studying psilocybin as it is used outside clinical environments, where potency and dose (e.g., micro- vs. macro-dose) vary widely. Research should explore how factors such as mushroom variety, set (a person’s headspace or mindset) and setting (their environment), as well as simultaneous co-use with other substances can impact both an individual’s immediate experience with psilocybin use and their long-term outcomes. Using observational or ecological momentary assessment designs may be valuable for capturing these phenomena in real-time. This research can aid in understanding how psilocybin use may differ among patients in controlled clinical settings compared to individuals in naturalistic settings.
Footnotes
Acknowledgements
The authors thank Joshua Black and the team at Rocky Mountain Poison & Drug Safety (RMPDS) for sharing the NSIHT dataset. The opinions, findings, and conclusions reported herein are those of the authors, and are in no way meant to represent corporate opinions, views, or policies of the RMPDS. RMPDS does not warrant nor assume any liability or responsibility for the accuracy, completeness, or usefulness of any information presented in this paper.
Ethical Considerations
As the current study involved analysis of existing survey data, no IRB approval was needed.
Consent to Participate
The original survey was evaluated by a research ethics committee in accordance with the Declaration of Helsinki and provided written informed consent forms to participants.
Author Contributions
CRediT: Author contributions included: Conceptualization (Cservenka, Obrochta); Data curation (Hummel); Formal analysis (Hummel); Methodology (Cservenka, Hummel, Kerr, Obrochta); Project administration (Cservenka); Supervision (Cservenka, Kerr); Visualization (Hummel); Writing - original draft and revisions (Hummel, Obrochta); Writing - review & editing (Cservenka, Hummel, Kerr, Obrochta).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NSIHT is designed and operated by Rocky Mountain Poison & Drug Safety (RMPDS) through Grant No. 75S20124P00003 funded by the U.S. Substance Abuse and Mental Health Services Administration (SAMHSA). The views expressed here are those of the authors and not of SAMHSA or the US Department of Health and Human Services. Data used with permission from Rocky Mountain Poison and Drug Safety.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Study, methods, and hypotheses were pre-registered in the Open Science Framework (OSF) on October 17, 2025 (Obrochta et al., 2025). Data are available from the Rocky Mountain Poison & Drug Safety (RMPDS) team. Teams wishing to use these data, or to replicate or extend our analyses, may request data from the stewards of those data sources.