
Abstract
Faith healing in sub-Saharan Africa has primarily been studied qualitatively among Pentecostal-Charismatic groups, and considered as its own phenomenon with little attention to its relationship to other modes of healing. Using data from Malawi, a religiously diverse African country with high HIV prevalence, we find that faith healing is pervasive across multiple religious traditions. For individuals, attending a faith healing congregation is associated with lower levels of generalized worry about AIDS, and this association is driven by those who switched churches before AIDS became widespread in rural areas. Use of condoms and traditional medicine are, on the other hand, positively associated with worry about AIDS. We argue that faith healing can be understood as a third therapeutic system that coexists with the well-documented biomedical and traditional systems. The success of faith healing approaches lies in their unique ability to combine individual-pragmatic and communal-ritualized aspects of healing to inform interpretations of the AIDS epidemic and its consequences.
The generalized AIDS epidemic in sub-Saharan Africa intersects with every area of social life and is a widespread concern. While the expansion of access to biomedical prevention and treatment strategies such as HIV testing and condoms has been central to the global prevention agenda (Heimer 2007; Schoepf 2001), alternative therapeutic systems such as faith healing and traditional medicine continue to inform how individuals interpret the epidemic, avoid infection, and live with its consequences (Probst 1999; Peltzer 1999). Analyses of the rapid growth of Pentecostal-Charismatic Christianity across southern Africa emphasize the marketing of faith healing as an invaluable product in this context (Dilger 2007; Becker and Geissler 2007; Gifford 2004). Faith healers are different from traditional healers in their reliance on the world religions of Christianity and Islam to provide both legitimacy for their own practice and the symbolic tools to give meaning to health and illness (Schoffeleers 1991).
Unfortunately, what we know about faith healing practices is limited to ethnographic evidence from Pentecostal-Charismatic churches. It remains unclear whether or not faith healing is practiced among other religious groups in sumethodsb-Saharan Africa or whether it has benefits that are measurable and distinct from other types of healing strategies. To understand the prevalence of faith healing as a collective practice, we must investigate where it is found, how it is practiced, and how it enhances or impedes well-being vis-à-vis other therapeutic models.
This study uses survey data from three religiously and ethnically distinct regions of rural Malawi to explore faith healing in the context of a generalized AIDS epidemic. We investigate the following: (1) the prevalence of faith healing across religious groups; (2) the relationship between faith healing and congregation-level engagement with biomedical and traditional strategies; and (3) the experiences of individuals living within the epidemic, measured by individual level of worry about AIDS. Our goal is to determine the extent to which faith healing functions as a third therapeutic system relative to the biomedical and traditional models, with distinct consequences for how individuals experience the generalized AIDS epidemic. Following several decades of increasing ethnographic attention to local and alternative modes of healing in the region, to our knowledge ours is the first quantitative analysis of faith healing in sub-Saharan Africa.
Theoretical Background
Throughout Africa’s colonial history, bodily healing has been a major locus of the struggle for power, expressed in the ability to name a cause of illness and to advance effective treatment (Probst 1999; Vaughan 1991; Feierman 1985). Yet scholarly accounts vary in the extent to which they view biomedicine as having transformed “African subjectivities” and in their assessments of the extent to which individuals in sub-Saharan Africa both understand themselves as biomedical subjects and use biomedical logics to understand their world (Vaughan 1991). Most scholars agree that health seeking in sub-Saharan Africa today is the result of a complex process of agency and exchange on the part of both the colonizers and the colonized and that traditional and biomedical therapeutic systems coexist in contemporary sub-Saharan Africa. Yet, while some see the introduction of biomedicine as a fundamental rupture with traditional understandings of health (Westerlund 2006; Probst 1999; Baylies 1986), others are skeptical of the extent to which this has been the case, citing the persistence of alternative therapies alongside the innovations of biomedicine (Vaughan 1991; Feierman 1985).
This debate has generated two schools of thought on contemporary health systems in sub-Saharan Africa. The first sees health-seeking behavior as motivated by pragmatic decision making on the basis of individual experiences, and the second views it as fundamentally motivated by deep-seated cultural forms expressed through collective rituals (Comaroff 1980). These two perspectives lead us to expect the interaction of multiple therapeutic systems to produce very different results. The pragmatic model focuses on cooperation between systems, asserting that individuals in sub-Saharan Africa have readily adopted imported biomedical technologies and utilize these alongside traditional interpretations and treatments (Liddell, Barrett, and Bydawell 2005; Morris 1986; Feierman 1985). Recognizing that these two systems rely on different assumptions about health and the spiritual world, the pragmatic perspective emphasizes the ability of individuals to simultaneously navigate both systems to treat their ailments. In understanding and treating AIDS, for example, individuals “switch easily between biomedical and religious interpretations of HIV” (Dilger 2007:70). Traditional healing is characterized as “a parallel health care system” (Kale 1995:1182) that should be recognized for its effectiveness within its own system of meaning. According to this view, faith healing practices further contribute to community health and benefit the individual health consumer who can access multiple practitioners and therapies at the same time (Peltzer 1999).
In contrast, the ritualized behavior model focuses on the contestation between systems, emphasizing the fundamental incongruities in the assumptions underlying Western medicine and African traditional medicine (Westerlund 2006; Some 1998; Okwu 1979). Given its privileged status in colonial regimes, the introduction of Western medicine dominated and altered schemas of health and healing in African societies (Probst 1999; Baylies 1986), and healing became a central arena of public contestation over meaning. This process profoundly affected African notions of healing, in that “healing, like illness, changed from being a formerly very public, communal affair to an increasingly individual, private concern” (Probst 1999:126). Thus, the importation of Western medicine transformed the structure of healing from collective ritual to individual-focused treatment.
The generalized AIDS epidemic in sub-Saharan Africa has thrown these larger theoretical and historical issues into stark relief. The biomedical prevention slogan “Abstain, be faithful, use condoms” focuses on individual behavior change and is well known even in the most remote areas of the Continent (Trinitapoli 2009; Pfeiffer 2004; Watkins 2004). International AIDS organizations have invested heavily in social marketing techniques aimed to “sell” Western biomedical strategies and products—including HIV testing and counseling (HTC), condoms, and antiretroviral treatment—to African governments and communities, assuming that universalizing knowledge of and access to these technologies is the key to arresting the epidemic (Heimer 2007; Pfeiffer 2004; Baylies 2000). Yet some authors have argued that the biomedical therapeutic system, with its focus on individualistic risk assessment and behavior change, has done little to address the social component of the epidemic (Heimer 2007; Watkins 2004; Pfeiffer 2004; Schoepf 2001). While HIV infection may rest in the individual’s body alone, the experience of living in the context of such an epidemic is essentially communal. If traditional and faith healing approaches address the social aspects of disease more fully, they are likely to gain appeal in the context of AIDS.
Studies in Malawi demonstrate that traditional healing practices remain widespread today and typically involve a one-on-one consultation with a traditional healer known as a sing’anga (Rands 1989; Morris 1986). One study found that many of those treated in clinics for sexually transmitted infections had already been treated by traditional doctors (Zechariah et al. 2002). Another study found similar patterns among tuberculosis patients and reported cases in which traditional healers claimed to have cured individuals of the disease (Brouwer et al. 1998). Today, there are generally two types of such healers, although the line between them is not always clearly marked (Morris 1986). Herbalists (asing’anga azisamba) are primarily concerned with using herbal remedies to treat individual ailments, while spiritual diviners (asing’anga amizimu) focus more intensely on disease etiology and accessing the spiritual world. In Malawi, both types of asing’anga often prescribe the wearing of amulets or charms both to ward off infections and to heal (Rands 1989).
Postcolonial African governments have had ambivalent relationships with traditional healers. In some places they have been outlawed (e.g., Mozambique and South Africa) or heavily restricted in their freedom to practice (Kale 1995). Where no official restrictions exist, traditional medicine often carries a social stigma of backwardness from the perspective of governments and nongovernmental organizations. The AIDS epidemic in Malawi has been marked by sporadic discoveries of new herbal treatments (e.g., mchape) producing significant public controversy and tension with government health officials (Probst 1999). This has had far-reaching implications for traditional medicine as a therapeutic system relative to other options. Although we have found no systematic evidence demonstrating that traditional healing practices have declined during the postcolonial period, several authors have argued that the political tensions between governments and traditional healers are squelching engagement in these practices and providing fertile ground for the growth of faith healing as an alternative (Peltzer 1999; Probst 1999; Feierman 1985).
Within Africanist anthropology, faith healing has already been discussed as a third distinct system of healing (Schoffeleers 1991) that combines elements from both traditional and biomedical systems (Peltzer 1999). For example, African-independent churches in southern Africa feature three distinct forms of faith healing: public healing during church services, healing by immersion in water (also public), and private healing through consultation with a prophet (Peltzer 1999; Cox 1994). Evidence of this hybrid nature is found in faith healing’s unique combination of (1) a focus on the experiences of individuals and their responsibility to seek their own healing, (2) strong ritualized and communal practice, and (3) the incorporation of biomedical diagnoses into understanding illness (Dilger 2007; Singleton 2001; Poloma and Hoelter 1998).
Studies of Pentecostal churches in sub-Saharan Africa suggest that the public ritual of praying for miraculous healing during church services and special events, coinciding with acts of repentance, has become the most prevalent form of faith healing (Dilger 2007; Adogame 2007; Poloma and Hoelter 1998). These rituals link moral purification to physical healing and provide disease narratives that invoke tropes of moral decay and disintegration (Adogame 2007; Becker and Geissler 2007; Dilger 2007; Liddell et al. 2005). Faith healing thus serves to restore the individual’s moral status in the community while solidifying the notion that the ultimate causes of AIDS are moral and communal and that the only lasting cures are spiritual ones.
The dialectic between individual experience and ritual action in battling affliction (Comaroff 1980) is perhaps nowhere more apparent than in the case of faith healing. Yet faith healing is also unique in that access to it is somewhat dependent on religious group membership. Switching between churches is quite common in Malawi (Englund 2007), and while financial barriers prevent many people in sub-Saharan Africa from accessing clinics and traditional healers, faith healing can be accessed without additional expenditures when an individual joins a faith healing congregation. Faith healing as a health-seeking strategy thus encompasses both the actions of faith healing leadership and the actions of the individuals who seek membership in faith healing congregations in order to get healing.
Faith healing is often assumed to be unique to Pentecostals and African-independent churches, but there are several reasons to suspect that faith healing may appear more widely in Malawi. First, the historical record offers dozens of examples of religious groups making healing a central part of their message in the context of an epidemic (Stark 1996). Second, over the past 30 years the religious landscape of Africa, like in Latin America and Asia, has experienced both a rise in Pentecostal churches and a “Pentecostalization” of churches that predate the Pentecostal movement (Martin 2002). In other words, churches that were not originally associated with faith healing, accounts of miracles, or the “born again” label have been heavily influenced by the success of Pentecostalism and have begun to engage in “Pentecostal” practices, as is seen in the case of the Catholic Charismatic Renewal movement (Jenkins 2006; Robert 2000). Third, our own fieldwork in Malawi over a period of six years has indicated both the fluidity of denominational labels there and the prominence of faith healing in public discourse (Manglos, 2010; Trinitapoli 2006, 2009).
The ways in which each of the three healing systems described above interact with, interpret, and attempt to treat the generalized AIDS epidemic illuminate their relationships to one another and the distinct characteristics of each. While most studies of the relationship between these three systems of healing have been ethnographic and local (Peltzer 1999; Schoffeleers 1991; Comaroff 1980), our present analyses provide the first quantitative assessment of the extent of faith healing relative to other systems, as well as an evaluation of its unique impacts. Noting the communal and experiential nature of faith healing and of living within a generalized AIDS epidemic, we use a measure of worry about AIDS as a way to tap into these impacts.
Research Questions
The goal of this study is to assess the extent to which faith healing in Christian and Muslim religious congregations functions as a third therapeutic system with a distinct relationship to the experience of living within the generalized AIDS epidemic in Malawi. To that end, we ask the following three research questions:
How prevalent are faith healing practices across religious traditions in Malawi?
Do leaders of faith healing congregations have distinct attitudes toward the other two systems of healing (biomedical and traditional)?
How is involvement with each of the three health systems associated with worry about AIDS for individuals?
Data And Method
Data
This article uses two linked data sets to examine faith healing at both the congregational and individual levels and to predict AIDS worry by measures of prior health-seeking practices. The Malawi Diffusion and Ideational Change Project (MDICP) is a panel study on family planning and AIDS in Malawi. It began in 1998, with roughly 3,000 respondents from three rural districts: Balaka in the south, Rumphi in the north, and Mchinji in the central region. This analysis uses wave 3 of the MDICP (MDICP-3), which was fielded in the summer of 2004 when HIV prevalence was about 14 percent among adults ages 15 to 49 and the technology to test individuals for HIV had not yet become available to most of the population (Angotti et al. 2009; Measure DHS 2004). The Malawi Religion Project (MRP) is an offshoot of the MDICP, designed to examine the role of religious institutions in the context of a generalized AIDS epidemic. In order to obtain a random sample of religious leaders for the MRP, respondents from MDICP-3 were asked to identify their places of worship and their religious leaders. In the summer of 2005, the MRP research team completed interviews with 187 religious leaders named by MDICP-3 respondents, which represented a response rate of 93.5 percent (adams and Trinitapoli 2009; Social Networks Project 2005). By using a hypernetwork sampling approach (Chaves et al. 1999; McPherson 1982), the MRP produced a random sample of religious congregations in rural Malawi, and it is, therefore, suitable for making generalizations about the religious landscape of this area.
Congregation-Level Measures
Denomination
In MRP interviews, congregational representatives reported on key congregational characteristics, including current and historical religious traditions. These reports were coded into a set of six categories based on salient historical and contemporary distinctions (Steensland et al. 2000): Catholic, Muslim, Pentecostal, African-independent churches, mission Protestant (including Presbyterian, Anglican, Baptist), and new mission Protestant (including Seventh-Day Adventist, Church of Christ, Jehovah’s Witness). The categories used here are not identical to those used by Steensland and colleagues (2000) but instead reflect a translation of their coding strategy to the Malawian context. The strategy takes into account the historical period in which the various religious traditions were first established in the region as well as several defining theological characteristics (adams and Trinitapoli 2009).
Dimensions of faith healing
In order to capture the multidimensionality of faith healing, we examine multiple measures, as reported by the religious leaders, of each congregation in the MRP survey. We explore four distinct aspects of healing at the institutional (i.e., congregational) level: (1) healing discourse, (2) healing practices, (3) healing-related growth, and (4) healing identities.
We assess discourse on healing using the question, “How often do you talk about healing in a sermon or religious service?” Congregations with leaders who report preaching about healing at least monthly are coded 1 for this measure. In order to tap into healing practices, we use data from a question asking, “In the past month, have you or another leader of this congregation participated in any healings?” This measure is a naturally dichotomous variable and is employed as such to measure actual healing practices (coded 1 if yes, 0 if no). To tap into healing-related organizational growth, we use data from a question asking, “Do you think anyone has joined your congregation because they noticed supernatural healings or other miracles taking place in your church?” Those who answered “yes, many” are classified as having healing-related growth (coded 1), while those responding “yes, a few” or “no” are classified as not having had healing-related growth (coded 0). Finally, to tap into healing-related congregational identity, we use data from a question asking, “Do miraculous healings characterize your congregation?” Those with affirmative answers are coded 1 (0 otherwise). However, for particular analyses, we also examine congregations characterized (1) by any of these four dimensions of healing, (2) by none of these, and (3) by the number of healing characteristics of the congregation, through a simple additive index (ranging from 0 to 4).
Engagement with biomedical prevention strategies
Leaders were asked about the frequency with which they discuss a number of topics during their weekly religious services. Topics include the following: morality generally, sexual morality in particular, HIV, illness, death and the afterlife, and politics. We use the leaders’ reports to distinguish those who talk explicitly about AIDS on a regular basis (“every week” or “almost every week” coded 1) from those who do not (coded 0). Religious leaders may give advice that reinforces or that contradicts the prevention messages articulated by the government, international nongovernmental organizations, and local health organizations. In reporting on the type of private advice they have given to members during the past year, we distinguish those who have privately advised members to use condoms or encouraged members to go for HTC (coded 1) from those who have not (coded 0) to assess leader engagement with biomedical strategies for HIV prevention.
Congregational relationship to traditional health practices
As mentioned above, three of the most common practices of traditional medicine persisting today are visiting diviners (known as asing’anga amizimu) visiting herbalists (asing’anga azisamba), and wearing amulets to protect from negative spiritual forces. To assess the acceptability of engagement with traditional health practices at the congregation level, we measure religious leaders’ attitudes about these three common practices. In particular, they were asked (1) whether it is acceptable to consult a sing’anga amizimu (diviner), (2) whether it is acceptable to consult a sing’anga azisamba (herbalist), and (3) whether it is acceptable to wear an amulet (or put one on one’s child) for protection. Additionally, we include a measure of whether the leader has ever privately advised a member to consult an herbalist. All four variables are coded dichotomously (affirmative responses coded 1, otherwise 0).
Individual-Level Measures
Generalized AIDS worry
To assess the associations between membership in a faith healing congregation and the experience of living within the generalized epidemic, we use a dummy variable to differentiate individuals who report worrying a lot about AIDS from those who worry a little or do not worry at all. We conceptualize reduced levels of AIDS-related worry as a positive indicator of health for several reasons. First, the existing literature on faith healing already suggests that the partial alleviation of such worry through communal rituals of repentance and regeneration may be one of the most empirically visible effects of faith healing practice (Dilger 2007; Becker and Geissler 2007). Second, a sizable body of research demonstrates that generalized worry about AIDS reflects actual risk of infection. Evidence from Uganda and Malawi demonstrates that risk perceptions closely mirror actual sero-prevalence patterns for age and sex, but it also shows that worry about AIDS is far more prevalent than infections, as individuals tend to overestimate their own risk of infection (Anglewicz and Kohler 2009; Smith and Watkins 2004; Kengeya-Kayondo et al. 1999). One’s level of AIDS worry is thus reflective of both one’s actual level of risk and the generalized amplification of worry in his or her setting. Further evidence of this is that, while Malawi’s overall HIV prevalence is just under 12 percent (United Nations Programme on HIV/AIDS 2008), the percentage of those in our sample who report being “very worried” about AIDS is 41 percent. Given this, it is highly unlikely that low levels of worry about AIDS indicate ignorance or carelessness with regard to AIDS. Yet we note that the over-assessment of risk can be problematic, too, as believing oneself already to have HIV may discourage individuals from getting tested or from making the effort to protect themselves.
Engagement with biomedical strategies
We measure engagement with biomedical strategies using two of the most common prescriptions for prevention coming from the public health community: condom use and testing. Because neither strategy was widespread in 2004, we use dichotomous measures of “ever use” of condoms and “ever tested” for HIV to mark the utilization of biomedical strategies to deal with the epidemic (affirmative answers coded 1, otherwise 0).
Engagement with traditional strategies
Our measures of individual engagement with traditional healing mirror those at the congregation level but tap actual behaviors. We asked whether the respondent had (1) visited a sing’anga amizimu (doctor of spirits or diviner), (2) visited a sing’anga azisamba (herbalist), or (3) worn an amulet or put one on his or her child during the past year. All three are coded dichotomously (affirmative responses coded 1, otherwise 0).
Membership in a faith healing congregation
By attaching the characteristics of their congregations to each individual, we determine whether an individual regularly attends a congregation in which any of the four dimensions of healing are present. As a first step, we examine the differences between those who attend faith healing congregations and those who do not. To assess the extent to which individuals in Malawi access faith healing by switching congregations, we then separate individuals by the nature and timing of their membership in a faith healing congregation. Using in-depth religious histories from the MDICP-3, we constructed a categorical measure distinguishing among four groups: (1) those not in a faith healing congregation, (2) those who have been lifelong members of a faith healing congregation, (3) those who switched into a faith healing congregation before 1999 (when first AIDS became visible in rural areas), and (4) those who switched into one since 1999.
Individual-level controls
Prior research from Malawi has illustrated the complex linkages among gender, socioeconomic status (SES), age, and risk, suggesting that young females (15–24) are at particularly high risk for infection by their partners, while infections peak at older ages for men (LeClerc, Matthews, and Garenne 2009; Glynn, Caraël, and Auvert 2001). Prevalence also tends to be highest among wealthy and educated individuals, though these relationships vary by country and by gender (Hargreaves and Glynn 2002; Mishra et al. 2007). We use a dummy variable to distinguish men from women (male = 1, female = 0), and we control for the respondent’s age using a squared term, since the relationship between age and AIDS-related outcomes tends to be curvilinear (Timæus and Jasseh 2004). We use two measures to tap variation in SES in this sample: a dummy variable to indicate that the respondent has attended secondary school and a four-item additive index of the number of durable household goods (mattress, bicycle, radio, pit-latrine) owned, which has been widely used in studies on Malawi (e.g., Anglewicz et al. 2009).
Analytic Plan
We begin our analysis with a focus at the congregational level. We present a univariate summary of our congregation-level variables, an analysis of multiple measures of faith healing by denomination, and bivariate analyses of the relationship between congregational faith healing and religious leaders’ attitudes toward each of the other two therapeutic systems. This allows us to assess the prevalence and nature of faith healing within congregations and to determine whether those characterized by faith healing feature distinct attitudes toward the other two systems.
We then move to examining faith healing at the individual level, with a descriptive overview of the individual-level characteristics, followed by multivariate analyses that combine the individual-level data from the MDICP-3 with the congregation-level data to answer whether membership in or switching into a faith healing congregation is associated with high levels of worry about AIDS. Ancillary analyses exploring the importance of congregation-level predictors for individual-level AIDS worry revealed no significant congregation-level associations and are not presented here (available upon request). Since individuals are nested within congregations in the linked data, however, we still use multilevel logistic regression models. To deal with missing data, we imputed 10 data sets using the “ice” command in Stata. Estimates from multiple imputation have been shown to be more accurate than those using single imputation techniques (Acock 2005). All 10 data sets were then combined, and estimates were generated in Stata 10 using the “mim” procedures for working with multiply imputed data sets (Royston, Carlin, and White 2009).
Results
Prevalence and Distribution of Faith Healing Indicators
Table 1 reveals that an overwhelming majority of religious leaders are engaged with two of the three dimensions of the biomedical system we examine here. Religious leaders talk frequently about AIDS (72 percent) and encourage members to access HTC (67 percent), while only about one-quarter has advised members to use condoms as a method of prevention. While the acceptance of herbalists exceeds 40 percent, the other two traditional practices (amulets and diviners) receive very low levels of support from religious leaders. As expected, only a small minority in each tradition approves of these practices, and approval is highest (though not high) among Muslim and African-independent church leaders (analyses not shown). This supports Morris’s (1986) suggestion that herbal medicine is widespread and that most people have knowledge of it and use it, often without relying on divination or religious rituals. In general, we find that religious leaders in Malawi make this distinction between herbalists and diviners, generally accepting the former and rejecting the latter.
Summary Statistics for Congregational Engagement with Three Therapeutic Systems
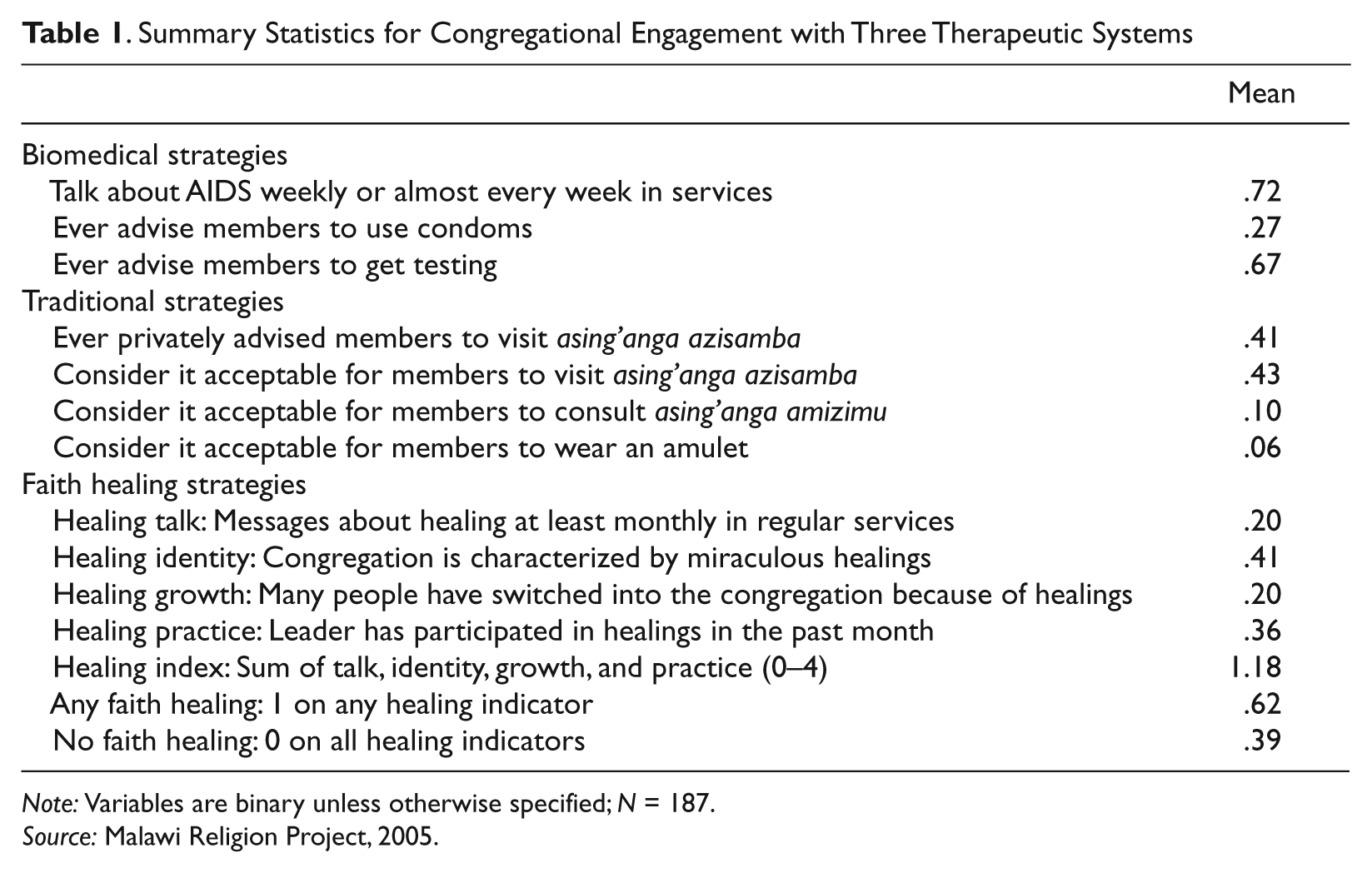
Note: Variables are binary unless otherwise specified; N = 187.
Source: Malawi Religion Project, 2005.
The literature on religion in sub-Saharan Africa has treated faith healing as a practice that is unique to Pentecostal and Charismatic groups or in some cases older Apostolic and Zionist movements (Meyer 2004; Peltzer 1999). In our data, however, a very different story emerges. Summary statistics for each of our faith healing indicators—capturing domains of discourse, practice, identity, and healing-related growth—reveal that 62 percent of all congregational leaders report that at least one indicator of faith healing characterizes their congregations. Just under half report that their congregations are characterized by miraculous healings. Indicators that require respondents to reference actual events (i.e., preaching and actual healings) within a recent time period yield similarly high levels of prevalence.
When we assess the prevalence of each dimension of healing by religious tradition (presented in Table 2), we reach a similar conclusion: Faith healing is widespread across different types of congregations. A higher proportion of Pentecostal leaders report the presence of faith healing characteristics in their congregations; yet in all categories except New Mission Protestant a majority of congregations is engaged in faith healing by at least one of our measures. Since very little has been written about New Mission Protestant groups and their adaptations in sub-Saharan Africa, we refrain from offering any in-depth interpretations of their low levels of faith healing, noting only that they (1) tend to place heavy emphasis on regulating lifestyle (e.g., diet, sexual behavior, Sabbath observation), (2) have had something of an enclave nature, and (3) are profoundly distinct from the older Mission Protestant tradition (i.e., Presbyterians and Anglicans) with which they are frequently and erroneously associated.
Prevalence of Faith Healing Characteristics in Congregations, by Denomination
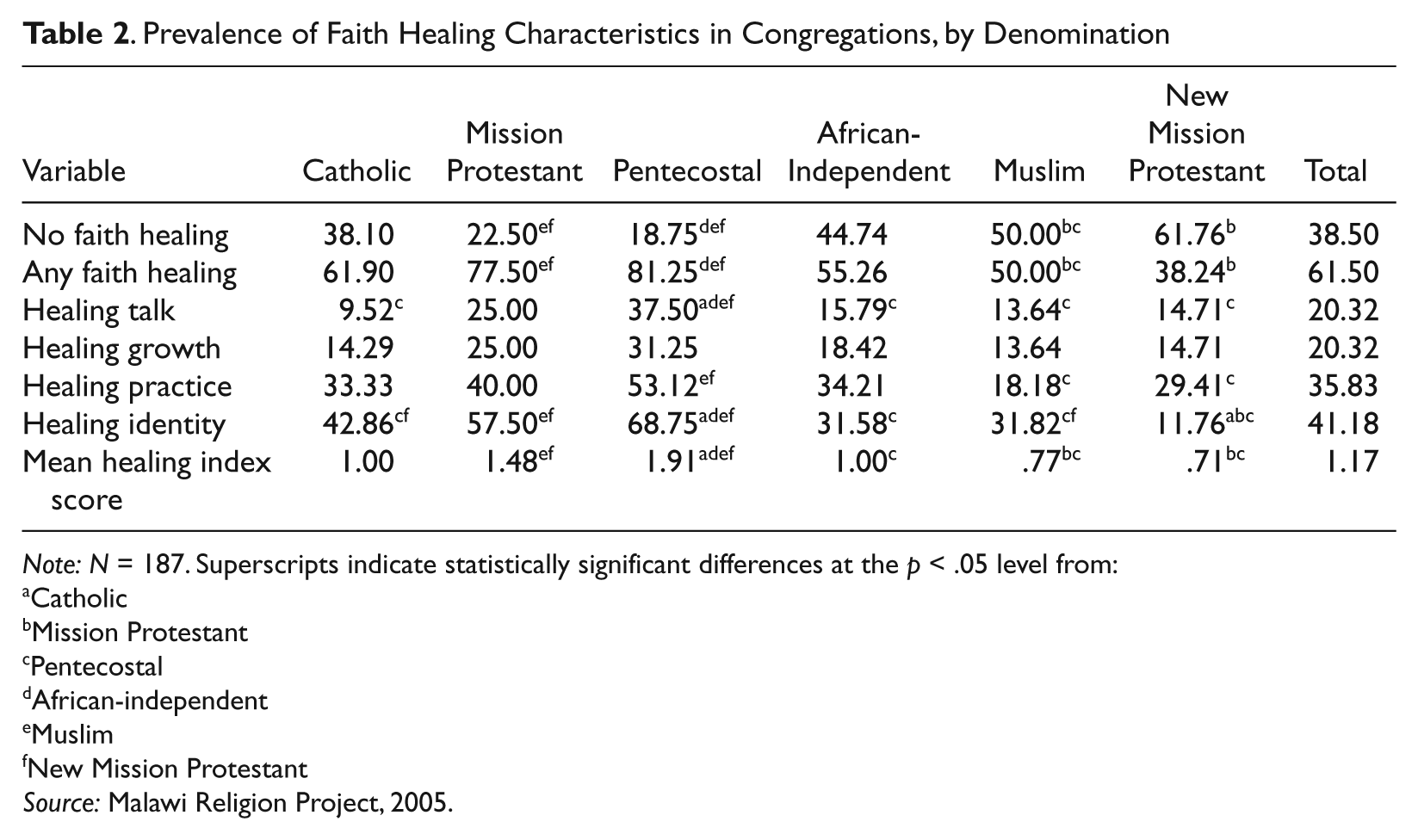
Note: N = 187. Superscripts indicate statistically significant differences at the p < .05 level from:
Catholic
Mission Protestant
Pentecostal
African-independent
Muslim
New Mission Protestant
Source: Malawi Religion Project, 2005.
Attitudes toward Biomedical and Traditional Systems
Table 3 shifts the focus from denominational differences to the question of how faith healing congregations engage with the other two systems. Cross-tabulations show the association between being a healing congregation and (1) engaging with biomedical prevention strategies and (2) accepting traditional healing strategies. Leaders of faith healing congregations are significantly more likely to report preaching frequently about AIDS than leaders of those not characterized by faith healing. They are also more likely to encourage members to seek HTC, though the difference is not statistically significant (p < .11). Faith healing and non–faith healing leaders do not differ in their approach to condom use, a finding that is consistent with recent literature highlighting the moral and cultural issues surrounding the uptake of condoms as a preventive strategy (Tavory and Swidler 2009; Pfeiffer 2004).
Congregational Engagement with Other Two Therapeutic Systems: Number of Responses and Percentages (in parentheses)
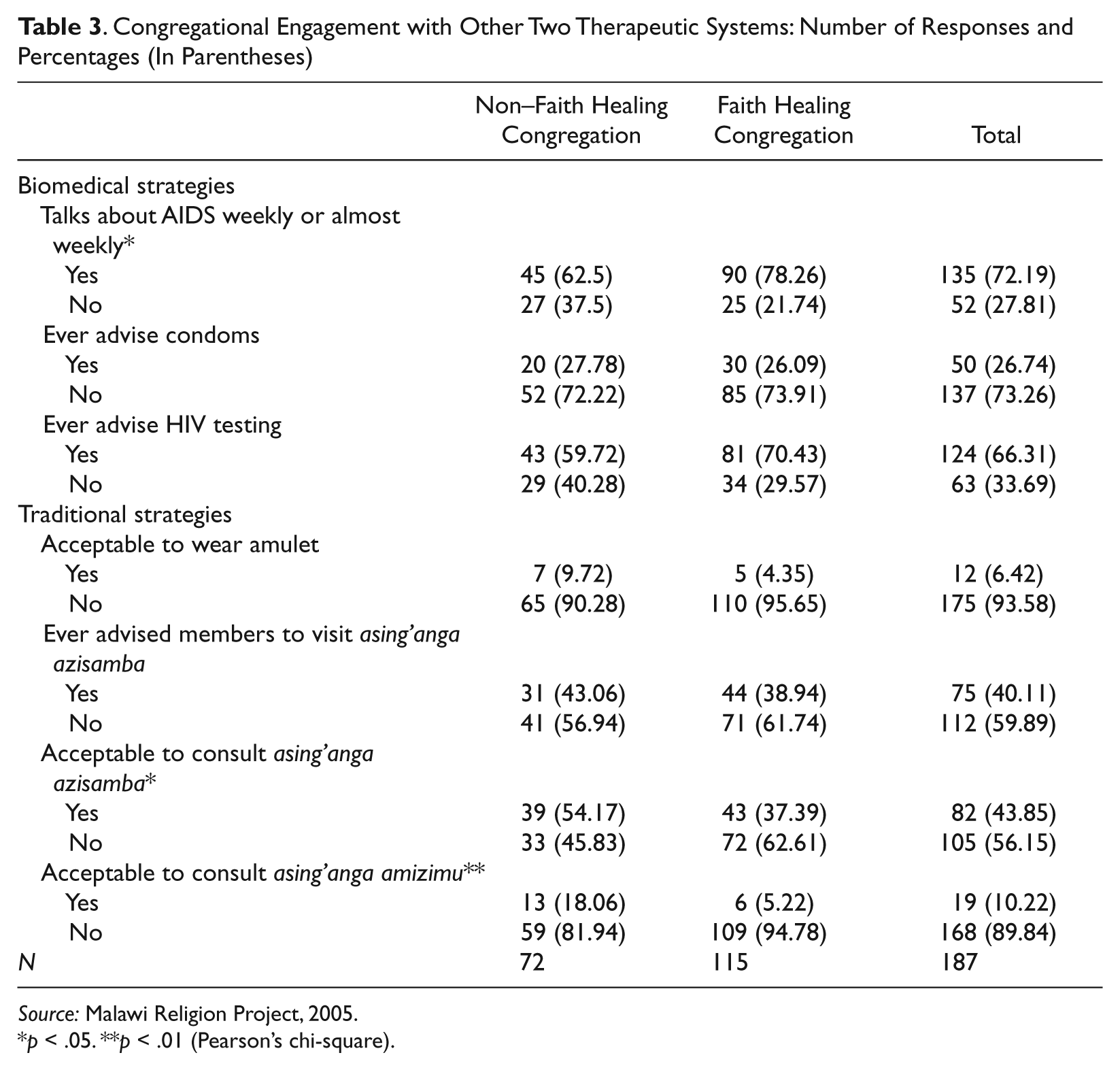
Source: Malawi Religion Project, 2005.
p < .05. **p < .01 (Pearson’s chi-square).
The relationship between faith healing and acceptance of traditional strategies is fairly ambiguous. Leaders of faith healing congregations are less likely than their counterparts to consider visits to herbalists and diviners acceptable. The acceptability of amulets and encouragement to seek help from an herbalist, however, do not vary by whether or not a congregation is a healing one.
Individual Membership in Faith Healing Congregations as a Health-Seeking Strategy
Turning to questions about how individuals engage with the three systems, Table 4 provides a descriptive overview of the MDICP sample. The results underscore our assertion that widespread worry about AIDS characterizes generalized epidemics. While biomarker data from the MDICP revealed that adult HIV prevalence in 2004 was about 8 percent in this sample (Anglewicz and Kohler 2009), 41 percent of respondents reported being very worried about AIDS, and the mean value for the three-level measure of AIDS worry is 2.06. In 2004, 18 percent of the sample had been tested for HIV at some point, and 20 percent reported having used a condom in the previous year. About equal numbers had worn an amulet and visited asing’anga amizimu (17 percent), though the two practices were not highly correlated (r = .18). Visits to asing’anga azisamba were more prevalent, with nearly one-third of the sample having consulted an herbalist in the past year.
As we would expect from the high prevalence of faith healing reported at the congregational level, a majority (64 percent) of the sample attend a congregation characterized by discourse, practice, growth, or identity related to faith healing. This table also shows the percentage of the overall sample that have been in faith healing congregations since birth (35 percent), who have switched into one before 1999 (21 percent), and who have switched into one since 1999 (8 percent).
Descriptive Overview of the Malawi Diffusion and Ideational Change Project Sample (Individuals)
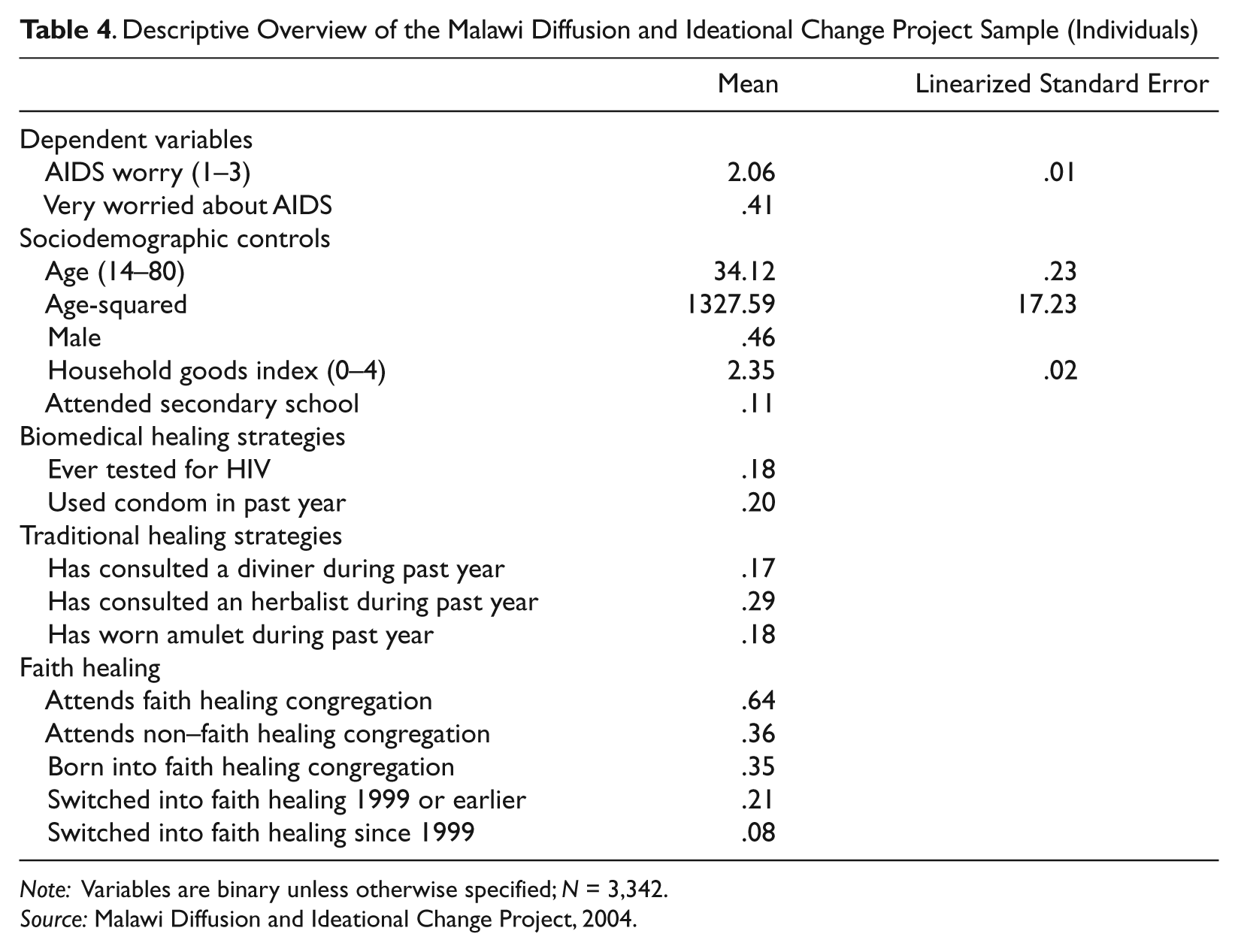
Note: Variables are binary unless otherwise specified; N = 3,342.
Source: Malawi Diffusion and Ideational Change Project, 2004.
Table 5 presents a series of logistic regression models predicting high levels of worry about AIDS. The models are ordered to examine associations for the biomedical system, the traditional system, and the faith healing system separately before assessing the three simultaneously. Women are consistently more worried than men, but education and age have no association with level of self-reported worry, which strongly supports one of our primary assumptions—that AIDS in Malawi is a truly generalized epidemic. In examining the relationship between biomedical strategies and AIDS-related worry, model 1 also demonstrates that having been tested for HIV is negatively associated with worry, while having used a condom in the past year is associated with high levels of worry. Model 2 examines how engagement with the traditional health system is associated with worry about AIDS, showing that two of the three types of traditional practices we examine are associated with increased worry. Since this relationship could operate in either direction, we make no claims here about causality. Model 3 reveals a significant negative association between belonging to a faith healing congregation and worry about AIDS. In model 4, we separate those from the faith healing group into three categories on the basis of when they entered into the congregation, revealing that the overall effect is driven by those who switched prior to 1999. Because this relationship is not present for those who were born into faith healing congregations or those who switched more recently after the widespread onset of the epidemic, it is unlikely that current switches are motivated by higher levels of worry about AIDS. Instead, it seems likely that those who have been attending a faith healing congregation for a long period of time have been more resistant to worry about the epidemic. When we simultaneously measure the relationships that biomedical, traditional, and faith healing strategies have to AIDS-related worry (model 5), all of the observed associations remain consistent.
Coefficients and Standard Errors from Random Effects Logistic Regression Models Predicting High Level of Worry about AIDS
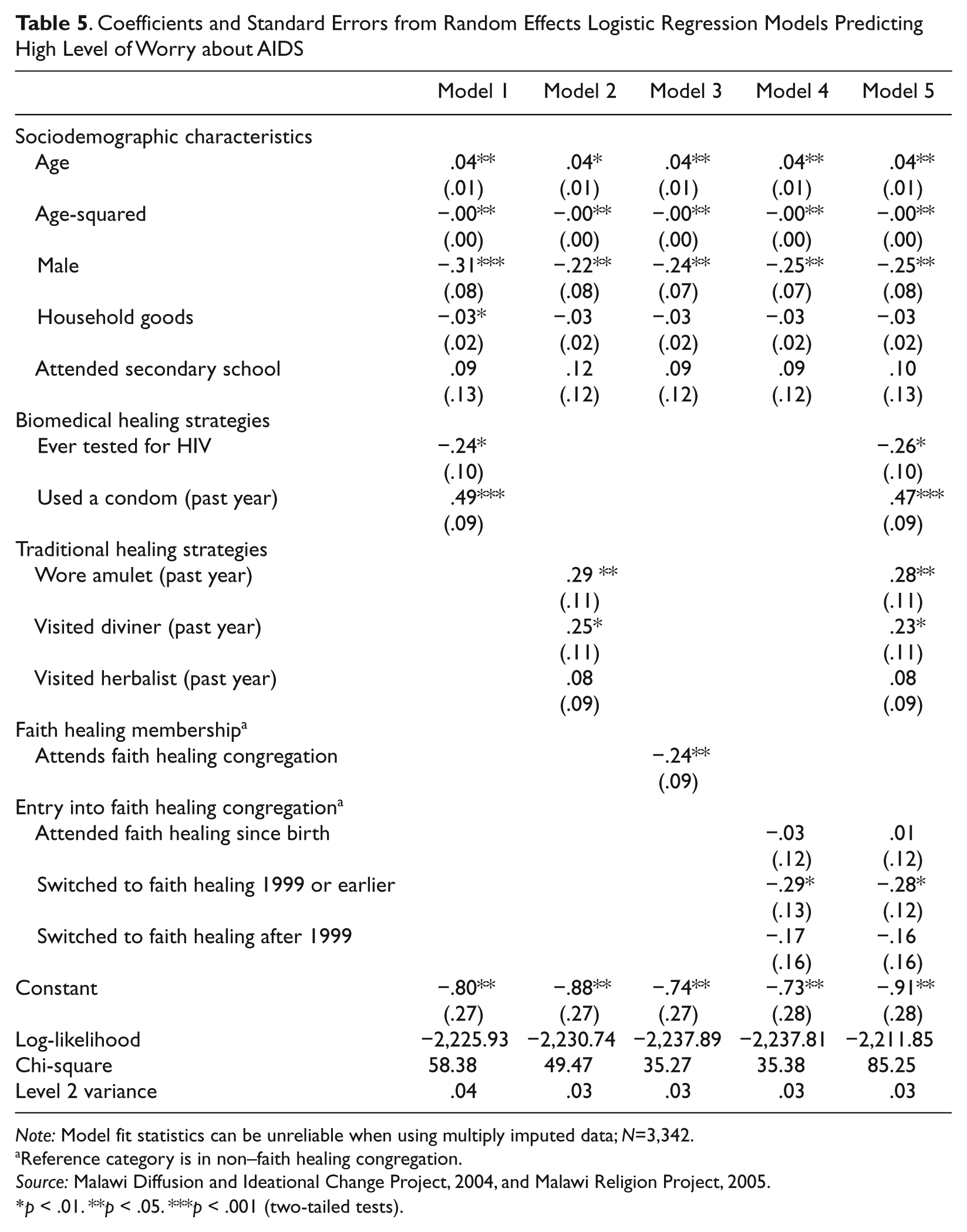
Note: Model fit statistics can be unreliable when using multiply imputed data; N=3,342.
Reference category is in non–faith healing congregation.
Source: Malawi Diffusion and Ideational Change Project, 2004, and Malawi Religion Project, 2005.
p < .01. **p < .05. ***p < .001 (two-tailed tests).
Discussion
Our analyses reveal that faith healing is practiced widely in all types of religious congregations in Malawi. Faith healing congregations are slightly less accepting of traditional healing than their non–faith healing counterparts, but they are equally—if not more—engaged with biomedical prevention strategies. For individuals, we find that those who participate in faith healing congregations are less likely to be very worried about AIDS. However, this association is driven by those who joined a faith healing congregation before the epidemic was visible; it does not hold for those who switched recently or those who were born into a faith healing congregation.
Based on these results, we argue that faith healing congregations are meaningfully engaged with their biomedical counterparts. Faith healing represents a third distinct therapeutic system, and individuals engage in this third system alongside biomedical and traditional therapies. This engagement has a unique ability to restore Malawians’ confidence and trust in their future health by connecting them to a ritual community of healing. Faith healing is thus a prevalent, multidimensional, and cross-denominational set of practices that reflects a broader concern with health seeking in a resource-constrained environment.
By contrast, religious leaders generally draw clear symbolic boundaries to reduce their members’ involvement in traditional strategies. Few religious leaders condone visits to diviners, regardless of their relationship to faith healing. This distinction does not depend on whether asing’anga deal with health (both types do). Rather, acceptability of traditional practices for religious leaders appears to depend on whether healers invoke supernatural powers in their methods.
As expected, Pentecostal congregations are most likely to be practicing faith healing and to score very high on our index of faith healing indicators. Yet the Mission Protestant churches closely follow Pentecostals as the most actively engaged in faith healing, and they are followed by African-independent congregations, Catholic parishes, mosques, and then New Mission Protestants. The significant number of mosques engaging in faith healing is surprising and may indicate a substantial cross-fertilization among religious groups as well as the potential of all religious traditions to adapt to the needs and concerns of the local context. While faith healing may have its roots in Pentecostalism or African-independent churches, it is not exclusive to these traditions.
In a resource-deprived setting like rural Malawi, faith healing can be accessed by joining a new congregation, and our results show that this act of engagement at a particular time is central to the process of alleviating worry about AIDS. Since we do not observe lower levels of worry among all members of faith healing congregations, we conclude that the agency exercised in joining a faith healing congregation is critical for understanding how faith healing interacts with the experience of epidemic illness. Since 70 percent of recent switchers joined congregations that practice some form of faith healing, we feel confident in our assertion that faith healing is not likely to recede as a practice anytime soon. We predict that faith healing will become more prevalent as these congregations grow and as other, non–faith healing congregations adopt faith healing practices. The fact that only those who switched before 1999 reported less worry about AIDS suggests that the measurable effects of this health-seeking strategy are not immediate but arise over the long term. This time-ordered evidence also makes it unlikely that the relationship is working in the opposite direction, where those who switched already had lower levels of worry over AIDS. Our analyses did not reveal any compelling associations between congregational characteristics (AIDS discussions and faith healing) and individuals’ levels of worry. This, too, suggests that individuals are not necessarily shaped by their religious context just by proximity. Congregational influences may require either a more direct engagement with individuals (e.g., Trinitapoli 2009) or the personalization of a problem by the individual to become salient for people’s lives.
By contrast, the fact that both condom use and engagement with traditional medicine are associated with higher levels of worry about AIDS suggests that these prevention strategies are more directly motivated by higher levels of worry and a feeling of increased individual risk. Condom use remains low in Malawi, and previous studies have shown use to be strongly motivated by perceived risk (Tavory and Swidler 2009; Chimbiri 2007). As for traditional practices, they are engaged in privately rather than publicly and thus focus on the individual’s own sense of personal risk rather than communal, holistic, and relational healing. Having been tested for HIV, on the other hand, is associated with decreased worry because it adds another dimension: knowledge of one’s actual status. Since worry about AIDS is more prevalent than HIV infection itself and since HIV-negative diagnoses are more common than positive ones, testing tends to alleviate overall worry (Anglewicz and Kohler 2009).
As health-seeking strategies go, there is, of course, a big difference between getting tested (for example) and joining a new religious congregation. While testing is primarily about accessing knowledge about one’s health and well-being, religious switching may be motivated by a number of factors, with marriage and moving being the most common impetuses for reaffiliation (Trinitapoli 2007). Most switches—even those into faith healing congregations—are not consciously motivated by personal concern over AIDS. Yet the fact that having accessed a faith healing community is associated with lower levels of AIDS worry suggests that limiting our understanding of health-seeking strategies to individualistic and conscious behaviors is too simplistic. Regardless of their motivation for joining, those who join faith healing congregations may be more invested in its activities. Over time, regular discussions of healing as a spiritual problem with spiritual solutions and participation in the miraculous healing rituals that occur within faith healing congregations may have heightened salience for joiners (Singleton 2001).
As the epidemic has expanded, individuals who have been steeped in a context where faith healing is a real and accessible possibility are less vulnerable to worries about infection. Throughout sub-Saharan Africa, the AIDS epidemic is widely understood as a sickness of communities and not just a malady affecting numerous individuals (Dilger 2007; Becker and Geissler 2007). Here, the potential dangers of an HIV-positive diagnosis include both physical illness and loss of standing within the community, and both are framed as having spiritual solutions. The ritual nature of faith healing practices is essentially a communal treatment in which collective repentance is invoked to symbolically restore relationships within the community and provide comfort.
Our study represents an important first step in addressing faith healing as a widespread practice and as a relevant public health issue within the context of the generalized AIDS epidemic, but it suffers from several important limitations. As mentioned above, ritual communal healing is a process that brings into play both pragmatic concerns about health and theoretical questions about collective religious schemas. This interaction is deep and complex, and the type of survey data used here can only scratch the surface of understanding how behaviors such as health seeking are constructed subconsciously and through interaction. While our endeavor underscores the tremendous value of high-quality survey data that include contextual information on organizations such as congregations, we are limited by our reliance on cross-sectional data from congregations; thus, we are only able to indicate the possible temporal mechanisms underlying this relationship. Since faith healing takes a diversity of forms, more research is necessary for determining which dimensions of faith healing are most salient for making key distinctions across contexts. This will be particularly important for research in places like sub-Saharan Africa where faith healing is widespread and growing. Finally, our findings raise critical questions about how participation in faith healing rituals shapes individual attitudes toward and levels of engagement with the biomedical and traditional health systems.
Conclusion
Our central theoretical argument has been that faith healing should be considered as a third therapeutic system, which should not be conflated with either biomedical or traditional modes of healing. What makes faith healing unique from the other two is its continued emphasis on treating the community as well as the individual and on bringing order back into social relationships and the spiritual world. What we see in Malawi is the persistence of multiple types of healing, just as a pragmatic model of healing would predict. Yet faith healing also works gradually and subconsciously to reduce generalized worry about AIDS, indicating that ritually constructed cultural elements are also at work. The debate about pragmatism and ritualism stands to benefit from this evidence as scholars aim to elucidate the relationships between cultural forms and individual agency. As Comaroff (1980: 655) states, “Whether in terms of healing or of any other cultural domain, change must be examined as a dialectic between cultural order and subjective experience, a dialectic mediated by specific historical circumstance.” Health seeking is neither purely pragmatic nor purely culturally determined; it is the result of a complex interplay of individual experiences, social interactions, structural constraints, and cultural flows. In our study, we observe the strongest associations between faith healing and worry among those for whom collective rituals and individual agency converge in the form of making the switch into a faith healing congregation. Future studies of faith healing promise both to enhance our understanding of how local communities are responding to their most pressing health concerns and to illuminate the process by which people are motivated to seek health and combat illness in a diversity of ways.
Footnotes
Acknowledgements
We gratefully acknowledge the assistance of the local Malawi Diffusion and Ideational Change Project and Malawi Religion Project teams, as well as Mark Regnerus and Susan Watkins for their critical feedback on earlier drafts. Dr. Eliza Pavalko and five anonymous JHSB reviewers provided thoughtful and constructive feedback throughout the review process. Molly Martin and Wayne Osgood provided practical advice on our modeling strategy.
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: Data collection for the Malawi Diffusion and Ideational Change Project was supported by Rockefeller Foundation (National Institute for Child and Human Development) grants R01-HD41713 and R01-HD373-276; NIA grant AG1236-S3; and the Center for AIDS Research and the Center on the Demography of Aging, both at the University of Pennsylvania. Data from the Malawi Religion Project were supported by National Institute for Child and Human Development grant R01-HD050142-01. Additional institutional support was provided by the University of Texas at Austin Population Research Center.