
Abstract
Over the past 30 years investigators have called repeatedly for research on the mechanisms through which social relationships and social support improve physical and psychological well-being, both directly and as stress buffers. I describe seven possible mechanisms: social influence/social comparison, social control, role-based purpose and meaning (mattering), self-esteem, sense of control, belonging and companionship, and perceived support availability. Stress-buffering processes also involve these mechanisms. I argue that there are two broad types of support, emotional sustenance and active coping assistance, and two broad categories of supporters, significant others and experientially similar others, who specialize in supplying different types of support to distressed individuals. Emotionally sustaining behaviors and instrumental aid from significant others and empathy, active coping assistance, and role modeling from similar others should be most efficacious in alleviating the physical and emotional impacts of stressors.
The Problem
Substantial evidence has accumulated over the past few decades showing that social ties and social support are positively and causally related to mental health, physical health, and longevity (Berkman 1995; Cohen and Janicki-Deverts 2009; Cohen and Wills 1985; Ertel, Glymour, and Berkman 2009; House, Umberson, and Landis 1988; Hughes and Gove 1981; Kessler and McLeod 1985; Kessler, Price, and Wortman 1985; Seeman 1996; S. E. Taylor 2007; Stroebe and Stroebe 1996; Thoits 1995; Turner and Turner 1999; Uchino 2004; Umberson and Montez 2010). Evidence also documents that social support buffers the harmful physical and mental health impacts of stress exposure, although these buffering effects are less dramatic and consistent than the direct effects of social ties on health (Cassel 1976; Cobb 1976; Cohen and Wills 1985; House 1981; Kessler et al. 1985; Kessler and McLeod 1985; Thoits 1995; Uchino 2004). Despite robust findings over more than three decades, reviewers have pointed out repeatedly during the same time period that we do not know how social ties or social support actually work to sustain or improve health and well-being. Consider the following statements along with their dates:
“Further research on the proposed mechanism through which social support might operate is clearly indicated” (Cobb 1976:312). “Future work needs to be based on clear theoretical models of mediating processes in support-well-being relationships” (Cohen and Wills 1985: 351). “Attention to intervening mechanisms seems a crucial next step if we wish to truly understand how social support influences psychological well-being” (Thoits 1995:65). “The need to test the proposed theoretical mechanisms is one of the most pressing issues in this [social relationships and physical health] literature” (Uchino 2004:175). “We have documented a strong and reliable association between the diversity of our social networks and our longevity and risk for disease. Even though the basic association was reported 30 years ago (Berkman and Syme 1979), we still do not know why it happens” (Cohen and Janicki-Deverts 2009:377).
It is difficult to explain why research attention has focused so persistently on confirming the beneficial health outcomes of social relationships to the neglect of intervening mechanisms. This is not because explanatory processes are missing in the literature; investigators have suggested a wide range of mechanisms that may be at work. Despite this, only a few reviewers have attempted to organize or prioritize proposed theoretical pathways, and those reviewers have tended to focus either on physical health outcomes (e.g., Berkman et al. 2000; Cohen 2004; Uchino 2004) or mental health outcomes (e.g., Cohen and McKay 1984; Thoits 1986b), but not both. Furthermore, more theoretical attention has been paid to elucidating the effects of social ties/social integration on health and well-being than to understanding how social support acts as a stress buffer. So my goals in this article are threefold: to systematize the theoretical mechanisms proposed in the literature, integrate physical health and mental health models as much as possible into one, and elaborate stress-buffering processes. To aid in these tasks, particularly in the explication of stress-buffering, I will capitalize on a distinction that is not frequently made in the literature, that between primary versus secondary group members in a person’s social network.
Definitions of Terms
For my purposes, social ties refer to connections to and contacts with other people through membership in primary and secondary groups. Primary groups tend to be small in size, informal, intimate, and enduring; examples include family members, relatives, and friends. Primary group members are “significant others” (Sullivan 1953)—persons to whom individuals are emotionally tied and whom they view as important or influential in their lives. Secondary groups tend to be larger, interactions are more formal (guided by rules, regulations, and hierarchical positions), members’ knowledge about one another is less personal, and members may enter and exit such groups at their or others’ discretion, so membership may range from short to extended in duration; work, voluntary, and religious organizations are examples of secondary groups. The primary-secondary distinction is similar to Granovetter’s (1973) differentiation between strong and weak ties, where tie strength depends on the amount of time spent together, the emotional intensity of the relation, the intimacy of mutual disclosure, and the reciprocity in services provided to one another. Ties to a narrow or broad range of primary and secondary groups represent the individual’s degree of social integration. Social ties and social integration are structural aspects of people’s relationships, that is, they indicate how those relationships are patterned or organized. My focus here will be on simple numbers of ties and the primary/secondary nature of those ties in the individual’s social network, but as others have pointed out, a variety of network properties (e.g., frequency of contact, the density, homogeneity, and multiplexity of ties) need further exploration (Berkman et al. 2000; Brissette, Cohen, and Seeman 2000; House et al. 1988).
Social support typically refers to the functions performed for the individual by significant (i.e., primary) others, although I will argue that these functions can be supplied by secondary group members as well. The most frequently mentioned functions are emotional, informational, and instrumental assistance (House and Kahn 1985). Emotional support refers to demonstrations of love and caring, esteem and value, encouragement, and sympathy. Informational assistance is the provision of facts or advice that may help a person solve problems; this category of help can also include appraisal support—feedback about the person’s interpretation of a situation and guidance regarding possible courses of action (Cohen and McKay 1984; Weiss 1974). Instrumental support consists of offering or supplying behavioral or material assistance with practical tasks or problems. Access to these functions of support depends on having one or more structural ties to other people (Lin and Westcott 1991). The size and cohesiveness of a person’s social network and the types of relationships in a network (e.g., primary vs. secondary/strong vs. weak ties) influence the receipt of various kinds of social support (Barrera 1986; Lin, Ye, and Ensel 1999; Wellman and Wortley 1990), a topic to which I will return in the following.
Restrictions in the Scope of This Article
Social “support” is a positive term that connotes beneficent intentions or consequences. The disadvantage of the term is that researcher attention is directed away from the “dark sides” of social relationships. Relationships can be tense, conflicted, or overly demanding (Rook 1990a), namely, sources of stress and strain rather than benefit, and these negative or costly aspects of ties can cancel out the ameliorative effects of social support provisions. Moreover, well-intentioned acts of support sometimes can create offense or distress in recipients rather than comfort (Herbert and Dunkel-Schetter 1992; Wortman and Lehman 1985). Although these are important observations, I persist in using the term support for two reasons: My purpose is to explain the positive, not negative, influences of relations with others—indeed, the inverses of most processes I will describe represent stressors, the “dark side” of social life (Thoits 1985)—and successful support attempts are more common than failed ones (Lehman, Ellard, and Wortman 1986; Martin et al. 1994).
I confine my attention to social psychological processes linking aspects of social relationships to morbidity, mortality, psychological distress, and mental disorder. I recognize that immune, neuroendrocrine, and cardiovascular changes may mediate the connections between social ties/social support and physical health outcomes, and like others, I assume that individuals’ physiological responses can be influenced by the social psychological mechanisms that I will discuss here (e.g., Cohen, Gottlieb, and Underwood 2000; Uchino 2004). Physiological changes represent more immediate health endpoints, more proximate causes of disease or death (Turner 2010; Uchino 2004). Others have capably reviewed physiological mediators of health outcomes (e.g., Cohen 1988; Ertel et al. 2009; Kennedy, Kiecolt-Glaser, and Glaser 1990; Kiecolt-Glaser, Gouin, and Hantsoo 2010; Seeman 1996; Uchino 2004, 2006; Uchino, Cacioppo, and Kiecolt-Glaser 1996), so I will not undertake that task here.
Mechanisms Linking Social Ties To Health
The stress-buffering effects of social support can only be understood by considering the pathways through which social ties affect physical and psychological well-being, so I begin with that issue first. Social relationships are multifaceted, so there are many potential ways that relationships can affect bodily and emotional well-being. I will focus on seven social psychological mechanisms that have been discussed most frequently or prominently in the literature.
Social influence/social comparison
As Berkman and her colleagues (2000) and Stroebe and Stroebe (1996) have observed, social influence/social comparison is one pathway from social ties/integration to health that has often been ignored in the literature. People obtain both normative and behavioral guidance through comparisons with similar others in their reference groups (Festinger 1954; Hyman and Singer 1968; Marsden and Friedkin 1994; Merton and Rossi 1968). Individuals assess the appropriateness of their own attitudes, beliefs, and behaviors against standards that are avowed and/or modeled by reference group members, usually shifting their own to match those of the group. Such influence can occur through simple observing and contrasting of self with others in the social network, without explicit discussion or attempts at persuasion taking place. Norms about health behaviors are acquired through such comparison processes, for example, norms about the appropriateness of using tobacco, alcohol, or drugs; exercising; attending to diet; seeking preventive care or counseling; and complying with medical regimens, among many others. Poor health habits of course are established risks for subsequent morbidity and mortality. Note that reference groups may model risky or preventive health behaviors (Cohen 1988), so social influence through comparison processes may have damaging or protective consequences for health, depending on the reference groups that individuals view as salient and the predominant health beliefs and behaviors within those groups.
Social control
Another form of social influence is more active and direct. All theorists who focus on physical health outcomes identify social control as a key mechanism through which network ties affect health and longevity, primarily through its effects on health behaviors (e.g., Berkman et al. 2000; Cohen 1988; House et al. 1988; Uchino 2004; Umberson 1987; Umberson and Montez 2010). Social control refers to the explicit attempts of social network members to monitor, encourage, persuade, remind, or pressure a person to adopt or adhere to positive health practices. Social control efforts can discourage risky health behaviors but can also backfire if they are perceived as overly intrusive or dominating, creating resentment and resistance to behavior change (Hughes and Gove 1981; Lewis and Rook 1999). Hence, like the social influence/comparison mechanism, social control effects can be beneficial or harmful, depending on the strategies others employ to regulate the person’s behavior.
Social control is almost never mentioned as a mechanism through which social ties could influence mental health outcomes. However, psychological distress and mood, anxiety, and adjustment disorders are frequently presaged or accompanied by too much or too little sleep, too much or too little appetite, or too much smoking or drinking. Family, friends, and coworkers are likely to observe such behavioral changes and comment or attempt to intervene. To the extent that their efforts at regulation are successful, distress, anxiety, or depression may be averted or dampened. Additionally, network members may interpret the individual’s psychological symptoms as serious enough to require professional treatment and press him or her to seek help (Pescosolido, Gardner, and Lubell 1998; Thoits 2011). In short, social control exerted by primary and secondary group members may be just as relevant to mental as to physical health outcomes.
Behavioral guidance, purpose, and meaning (mattering)
There is another more implicit or indirect form of social control that derives from the important fact that all social ties represent role relationships. Roles are positions in the social structure (e.g., husband-wife, parent-child, doctor-patient, friend-friend) to which are attached reciprocal sets of normative rights and obligations (one actor’s rights are the other actor’s obligations, and vice versa). Role obligations are constraining influences on individuals’ desires and behaviors—this is Durkheim’s (1897/1951) point regarding the regulatory functions of norms. Commitments and responsibilities to role partners exert implicit pressures on persons to avoid risky or deviant behaviors and to engage in self-care (Hughes and Gove 1981; Rook and Underwood 2000; Umberson 1987). Much of my own work has been premised on this pathway (Thoits 1983, 1986a, 1992, 2003). I have argued that to the extent that individuals accept their social roles as self-defining (i.e., as identities), they obtain behavioral guidance from role expectations. In other words, individuals know how to behave, and in conventional roles this means conventional (nondeviant) behavior.
Beyond behavioral guidance, I have argued that knowing who we are to others also provides purpose and meaning in life, which in turn guard against anxiety and existential despair. A concept related to this function of role identities is “mattering” (Rosenberg and McCullough 1981). Mattering is defined as believing that one is an object of another person’s attention, one is important to that person, and he or she depends on one for fulfillment of specific needs. Because mattering refers to one’s significance to other people, it seems conceptually close to the notion of obtaining purpose and meaning in life from relationships with role partners. In sum, social ties as role identities should supply behavioral guidance and purpose and meaning in life (or a sense of mattering), which in turn should have positive effects on health habits and psychological well-being, respectively (Berkman et al. 2000; Brissette et al. 2000; Cohen 2004; House et al. 1988; J. Taylor and Turner 2001; Uchino 2004; Umberson and Montez 2010).
Self-esteem
Two other important social psychological mechanisms derive from the role identities represented by social ties: self-esteem and a sense of control or mastery over life. Roles are enacted with varying degrees of success—we may be superb parents, adequate classroom instructors, and enthusiastic but abysmal volleyball players. We evaluate our role performances not only through comparison with socially similar others in relevant reference groups but through imaginatively viewing our performances from the eyes of role partners and other audience members (Cooley 1902; McCall and Simmons 1978; Mead 1934). Self-evaluations in highly valued role domains reliably and positively affect global self-esteem or self-worth—beliefs regarding how good, worthy, or competent we are in general (Rosenberg et al. 1995). Self-esteem, in turn, is associated with lower symptoms of anxiety, depression, and distress and relates positively to life satisfaction and happiness (Baumeister et al. 2003; Taylor and Stanton 2007; Thoits 2003; Turner and Lloyd 1999; Turner and Roszell 1994). In short, self-esteem should mediate between the number and variety of individuals’ social ties/role relationships and their mental health.
Sense of control or mastery
Successful role performances also engender a general sense of control or mastery over life. Role obligations constitute a variety of tasks that must be accomplished on a regular basis. Many, if not most, are practical in nature, such as meeting deadlines, earning money, cleaning house, driving children to activities, and so forth; other requirements may be interactional, such as showing appropriate degrees of respect, controlling one’s feelings, or being sociable and entertaining. Accomplishing such tasks is contingent on the attention, effort, and care that one invests (assuming, of course, that structural circumstances enable rather than hinder such efforts). The more frequently one’s efforts result in adequate to superior task completion, the more strongly one should believe that one has control over what happens in one’s life in general (this should apply to children’s development as well). A global sense of control or mastery may derive from self-efficacy beliefs that emerge in specific domains of endeavor such as academics, athletics, parenting, and so on (Bandura 2001). Perceptions of control or mastery in turn sustain confidence in one’s ability to cope in the face of new challenges or major stressors and thereby should be associated with lower anxiety and depression (Mirowsky and Ross 2003; Taylor and Stanton 2007; Turner and Lloyd 1999; Turner and Roszell 1994) and reduced physiological reactivity to stressors (Taylor et al. 2003; Taylor and Stanton 2007). A sense of control thus should link role performances to health outcomes.
Belonging and companionship
Beyond mechanisms derived from the role relationships on which social ties are based, connections to other people are sources of a sense of belonging (Barrera 2000; Berkman 1995; Cobb 1976; Cutrona and Russell 1990; Thoits 1985; Uchino 2004). Belonging implies acceptance and inclusion by members of one’s primary or secondary groups. Acceptance and inclusion are not automatically granted by group members; they must signal their acceptance of us as a part of the group. With acceptance comes a belief that one “belongs to a network of communication and mutual obligation” (Cobb 1976:300), providing security that one’s needs will be met by the group. A close corollary of acceptance and inclusion is companionship—one has others with whom one can share social activities (Berkman et al. 2000; Cutrona and Russell 1990; Rook 1990b; Rook and Underwood 2000; Stroebe and Stroebe 1996; Uchino 2004). Companionship produces positive affect, which in turn enhances physical and psychological well-being (Rook and Underwood 2000; Uchino 2004). Conversely, lack of companionship, often described as loneliness (a gap between one’s desired and actual ties to others), has been linked to depression, anxiety, poor health habits, and ill health (Cacioppio et al. 2002; Stroebe and Stroebe 1996; Uchino 2004). In short, social ties should influence physical and mental health through belonging and companionship.
Perceived social support
Finally, and importantly, network ties are conduits of emotional, informational, and instrumental support (Lin and Wescott 1991). Interestingly, there is disagreement in the literature regarding whether social support is a mechanism connecting social ties to health outcomes. Some view social support as one of the pathways through which social ties sustain health (Berkman et al. 2000; Uchino 2004), while others see the positive health effects of social ties/integration and of social support as due to “entirely different and independent mechanisms” (Cohen 2004:676; see also Brissette et al. 2000; Cohen 1988; Cohen and Wills 1985; Stroebe and Stroebe 1996). For example, Cohen (2004) explicitly defines social support as “a social network’s provision of psychological and material resources intended to benefit an individual’s ability to cope with stress” (p. 676), while “social connectedness is beneficial irrespective of whether one is under stress” (p. 678).
Cohen and his colleagues may have arrived at this position while wrestling with a pattern of findings in early studies of stress-buffering effects (Cohen and McKay 1984; Cohen and Wills 1985; House et al. 1988): Measures of social ties or integration were reliably and negatively associated with psychological distress, ill health, and mortality, but these structural measures rarely were observed to buffer the impacts of stressors on health outcomes; in contrast, measures of support were rarely associated directly with health or mental health outcomes but repeatedly dampened the harmful consequences of stress exposure. This pattern of findings suggested that the main and the stress-buffering effects of social relationships were produced through different mechanisms.
Since the publication of these reviews in the mid-1980s, subsequent studies have shown that social support, especially perceived emotional support, directly and positively influences physical health and longevity (see reviews in Uchino 2004; Uchino et al. 1996) as well as psychological well-being (e.g., Lin et al. 1999; S. E. Taylor and Stanton 2007; Turner and Lloyd 1999). In essence, studies show that social support is important to well-being both when individuals are and are not facing adversity. Consequently, I share the view that the receipt or the perception of social support should be one of the key pathways from social ties to health endpoints (Berkman et al. 2000; Uchino 2004). However, I think it is likely that social support changes in character when major stressors are present. To explain, it is useful to distinguish between “everyday” and “major stress-related” supportive actions (see also Badr et al. 2001; Lin et al. 1999).
An attentive review of ordinary days (i.e., days devoid of major negative events or exacerbations of ongoing strains) would probably reveal that we routinely obtain demonstrations of love, caring, and understanding from intimates when we recount the day’s minor uplifts and hassles to one another. These demonstrations can sustain a sense that we matter to those we see as significant others and undergird our self-esteem. We also frequently swap useful information or advice with spouses, neighbors, coworkers, church members, and others as we chat about vexing circumstances encountered in our daily activities (e.g., inconvenient bank hours, mistimed traffic lights, overly expensive goods and services). Facts or recommendations from others enable subsequent behavioral changes that make everyday tasks more efficient, economical, or successful and probably sustain our sense of mastery or control over life. Even more importantly, informal discussions with others about impending problems at home, at work, or in other role domains may pinpoint ways to prevent the occurrence of a stressor or de-escalate the appraisal of imminent problems from possible threats to manageable challenges (Cohen and McKay 1984; S. E. Taylor and Aspinwall 1996; Thoits 1985; Uchino 2004). Finally, people in our networks do a myriad of simple, practical favors that speed or ease our usual round of activities at home and at work. Importantly, we are not only the recipients but the givers of everyday support to other people; these are reciprocal exchanges over time. These forms of emotional, informational, and instrumental assistance swapped in everyday interactions are so minor, so commonplace, and so taken for granted as to be virtually invisible as support provisions (Bolger and Amarel 2007; Bolger, Zuckerman, and Kessler 2000). In short, routine or everyday emotional, informational, and instrumental acts are helpful in themselves and also may sustain self-esteem, a sense of mattering to others, and perceived control over minor or impending obstacles and thus indirectly maintain psychological well-being and (through positive affect) physical well-being as well.
The issue of received versus perceived support
My previous examples of everyday support involve actual support provisions, usually termed received support or enacted support. Studies of such transactions have created two puzzles in the support literature. First, received support and perceived support are only weakly related to one another (Lakey et al. 2010; Stroebe and Stroebe 1996; Wethington and Kessler 1986), even though, logically, perceptions of support or support availability should result from actual support provisions and thus should be tightly tied to them. Why such weak associations? As Hobfoll (2009) points out, received support is typically assessed with reference to a particular stressful situation or a delimited time period (e.g., in the past month), while measures of perceived support capture generalizations that have emerged from numerous real instances of help (great and small) supplied by various network members during individuals’ lives. It would be unreasonable to expect concrete acts in specific circumstances to correlate highly with global impressions abstracted from countless such experiences over months or years. Perceptions of support are probably generalized from daily, mostly invisible supportive exchanges occurring over time (Bolger and Amarel 2007; Hobfoll 2009; Uchino 2009).
The second puzzle is that received support has null to weak and, if weak, often contradictory effects on well-being and mortality (sometimes helpful, sometimes detrimental), while the effects of perceived support are stronger and consistently beneficial for mental and physical health (Bolger and Amarel 2007; Uchino 2004, 2009). Why should received and perceived support differ so greatly in their health consequences? One answer may lie again in the measurement issues just described: Generalized perceptions of support should have greater predictive power than specific supportive behaviors that are performed in a delimited situation or time period. A second answer might trace to the ways in which recipients respond to help, especially explicit and unsolicited help. Support recipients have negative reactions to “visible” assistance (Bolger and Amarel 2007; Deelstra et al. 2003), particularly if they have not had a chance to reciprocate (Gleason et al. 2008). Deliberate helpfulness can cause recipients to feel indebted, unjustly overrewarded, too dependent, overcontrolled, or incompetent in the eyes of support providers. In contrast, unsolicited, subtly supplied, effectively invisible aid reduces individuals’ psychological distress substantially (Bolger and Amarel 2007; Bolger et al. 2000).
In sum, everyday invisible received support, but even more so, generalized perceptions of support should mediate the relationships of social ties to various health outcomes. They may also increase a sense of mattering to others, self-esteem, and mastery, as described earlier.
Summing up
Given their common origins in social relationships, the seven mechanisms I have identified are very probably correlated positively with one another, and some, such as self-esteem and mastery, can be quite strongly associated. Nevertheless, these seven theoretical mechanisms are distinguishable constructs, a variety of measures of each are available in the literature (Cohen et al. 2000), and the degree to which they load together or as separate factors can be assessed empirically. Techniques such as confirmatory factor analysis and structural equation modeling can test the utility of each as a mediator and assess the relative strength of each as a determinant of subsequent morbidity, mortality, distress, and disorder. The social psychological literature shows that many of these theoretical mechanisms are positively related to physical and/or mental health outcomes, but we know very little about whether they are in fact the conduits from social ties to those outcomes, as commentator after commentator has observed over the past three decades. It is time to start finding out.
Stress-Buffering: Processes And Mechanisms
In the previous section I argued that “everyday” support intervenes in the social ties to health relationship—especially perceived support derived from helpful exchanges with primary and secondary group members over time. I turn now to the issue of how social support may buffer the harmful impacts of major stressors on bodily and emotional well-being.
Stress-buffering represents a more complex set of processes than the main effect processes described in the preceding section because (of course) one or more major stressors are involved that require the individual to cope or adjust. The stressor may be an acute negative event or an intensified ongoing strain; in either case, the demands created by the exigent situation exceed the usual level of demands in the person’s life and are perceived by the person as taxing his or her abilities to cope (Lazarus and Folkman 1984). This new contingency sets the stress-buffering process in motion. 1 I will argue that when a major adversity occurs, social support ceases to be mostly invisible and reciprocal and becomes visible and deliberate, support attempts “work” through many of the same mechanisms that I described in the previous section, and efficacious support attempts will depend on who in the network is supplying what types of social support: primary group members who are experientially dissimilar to the distressed individual versus secondary group members who are experientially similar.
Visible and deliberate support
I propose that when persons in a social network are alerted to an individual’s calamity, the emotional, instrumental, and informational assistance that is normally exchanged almost invisibly in everyday interaction transforms in character. Network members’ assistance becomes intentional, visible, and focused on changing the individual’s situation and/or feelings. Expectations of reciprocity in everyday support probably are also suspended temporarily; network members recognize that the individual’s attention and effort must focus on dealing with the immediate situation.
Deliberately enacted support in response to the person’s pressing circumstances should validate and reinforce his or her general perception that support is available when needed, especially when that support is offered by others spontaneously. Conversely, if expressions of support are noticeably absent, lukewarm in tone, or reluctantly supplied, the person’s support perceptions will be undermined, especially so if primary group members (spouse, kin, friends) are the ones who are slow to respond—normatively, these are the people one should be able to count on when the going gets tough. If individuals are forced to ask for support from primary group members who are aware of the problematic situation, they may feel resentment and betrayal, and perceptions of available support again will be seriously compromised. Events or strains individuals are believed to have brought on themselves may fall into this latter category. People who are seen as more blameworthy or responsible for their problems receive less help from others; they are considered less “deserving” (see Clark 1987; Stroebe and Stroebe 1996). If the stressor is uncontrollable, the individual should receive more spontaneous, genuine, and generous support from network members than if the problem is one he or she had a hand in creating.
Assuming that the stressful situation is not the individual’s doing and is not so devastating or upsetting that supporters themselves are emotionally overwhelmed and become avoidant to protect themselves from distress (Stroebe and Stroebe 1996), how is it that social support works to buffer the impacts of stress? In previous work (Thoits 1986b), I argued that social support works through the provision of active “coping assistance.” That is, supporters advise or implement problem-focused and emotion-focused coping strategies that they would use themselves if they were facing the same stressor. Coping assistance can include helping the distressed person to see the situation in a different way, suggesting ways to solve the problem, intervening directly in the situation (what might be called “problem-focused supportive strategies”) and encouraging the person to vent feelings, offering a drink or a drug to lessen arousal, and providing distractions from the problem (“emotion-focused supportive strategies”). Coping assistance strategies are stress buffers because—when successful—they quite literally lessen situational demands and/or the person’s emotional reactions to those demands, reducing the physical and psychological consequences of the stressor directly. These tactics may also bolster the distressed person’s sense of personal control, counteracting the stressor’s physical and psychological impacts indirectly through this mechanism.
I now believe that active coping assistance supplies only half of the theoretical story. As I conceived it, coping assistance essentially consists of informational and instrumental support, including manipulating individuals’ emotions in order to change them (Thoits 1986b). Missing from my prior stress-buffering account are what Gottlieb (1978) calls “emotionally-sustaining behaviors”—emotional support. Demonstrations of caring, valuing, and understanding probably do not alter the distressed person’s situational demands or change aspects of his or her physiological or affective reactions directly. Rather, these behaviors likely influence the individual’s physical and emotional state indirectly through several social psychological mechanisms that I described earlier (e.g., mattering, self-esteem, belonging). In short, I suggest that there are two broad categories of supportive behaviors, emotional sustenance and active coping assistance, that influence physical and mental health differently, primarily indirectly through social psychological mechanisms in the case of emotional sustenance and mostly directly in the case of active coping assistance.
I further propose that there are two broad categories of persons who provide these functions, primary group members (significant others) who have not had past personal experience with the stressor that the distressed person is currently facing and secondary group members who do have prior experience (“similar others” or peers). I will argue that these primary and secondary group members provide emotional sustenance and active coping assistance, but the forms of these behaviors, their relative effectiveness, and the mechanisms involved will differ between these two support sources (see Table 1). (Fortunate individuals are those whose significant others include experientially similar others—they will obtain a wider range of effective help from the same supporters.)
The Effectiveness of Support as a Stress Buffer Should Depend on Its Source and Type: A Proposed Classification of Effective Types of Support by Source
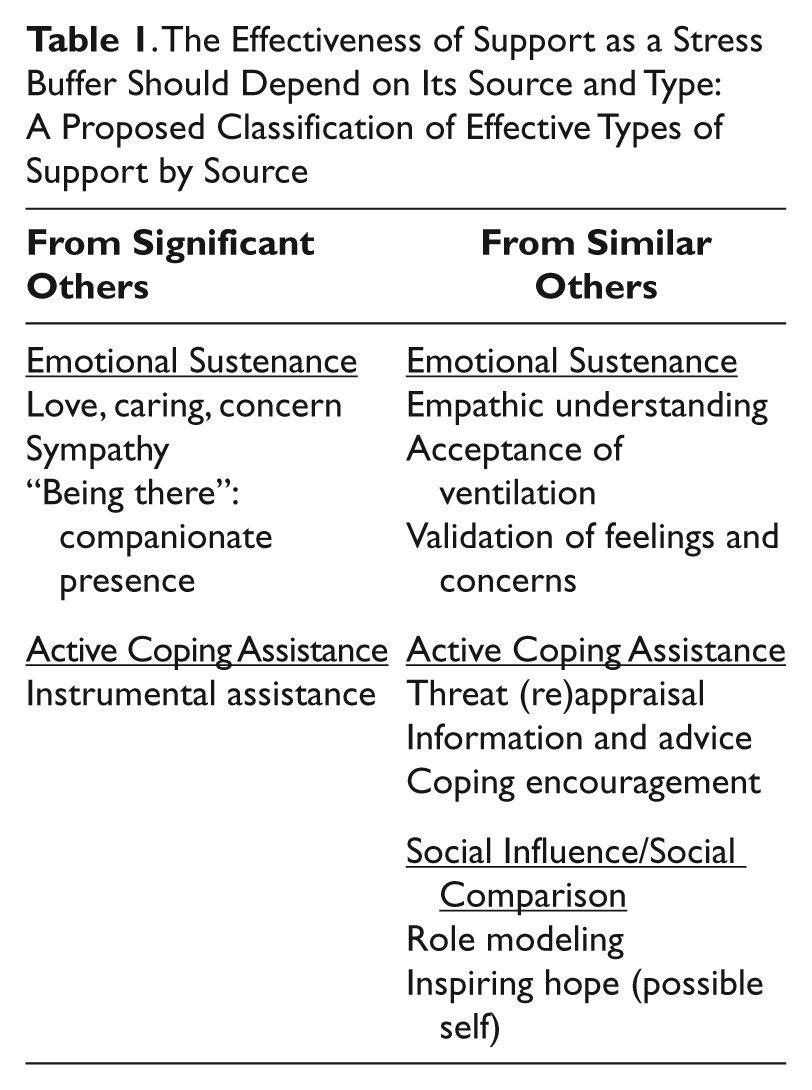
Emotional sustenance: Primary group/significant others
Emotionally sustaining behaviors from primary group members include signaling their understanding of the meaning of the stressor for the individual, sometimes in the form of displays of shock and distress on the individual’s behalf; expressing explicit concern and caring for the individual’s well-being (including more attentive social monitoring of his or her health behaviors); listening to his or her reactions, worries, and tentative plans (sympathy); and accompanying the individual as the upsetting event continues to unfold or spending time with him or her in companionate silence or joint activities (simply “being there”). Significant others’ caring, sympathy, and sheer comforting presence likely reduce psychological distress and harmful physiological arousal through three social psychological mechanisms: confirming the individual’s sense of truly mattering to other people, sustaining his or her sense of self-worth, and bolstering the belief that he or she indeed belongs to and is accepted within a network of caring others (Cobb 1976). Through these mechanisms, emotionally sustaining behaviors should reduce the physical and psychological impacts of adversity. These forms of emotional sustenance should be particularly effective in protecting well-being when they come from primary group members rather than secondary group members; secondary group members generally lack the emotional closeness and commitment to the person that would make such demonstrations probable or as meaningful.
I should note that emotional support may be rebuffed or prevented by distressed persons who wish to shield significant others from upset on their behalf. This is accomplished by withholding information about the problematic situation or the depth and range of one’s emotions and concerns. Such withholding may be typical of men who adhere to traditional masculine gender roles and parents who wish to protect their children. Emotional sustenance should be proffered by significant others and to have stress-alleviating effects only when the distressed person has signaled his or her willingness to talk about the stressor.
Active coping assistance: Primary group/significant others
In addition to emotional sustenance, family, relatives, and friends also offer active coping assistance in a variety of forms: instrumental aid, information and advice, and coping encouragement. I posit that among these various types of help, instrumental support (i.e., financial aid or help with practical tasks) from primary group members will be the most effective in alleviating the harmful effects of stress.
Receiving instrumental support from people in one’s primary circle of ties is normatively more appropriate than from secondary group members; family and friends are traditionally expected to lend a hand (Messeri, Silverstein, and Litwak 1993), so this type of coping assistance should be more frequent from significant others. Material and practical aid may be especially important to the distressed person on two counts: First, it can reduce situational demands directly, lessening physiological arousal and upset. Second, it symbolically conveys that significant others care for and value the distressed person (Cohen and McKay 1984), bolstering his or her sense of mattering and self-esteem. 2 Hence, instrumental coping assistance from primary group members is likely to be an efficacious stress buffer, both directly in its problem-solving effects and indirectly through the message that one matters to others and is esteemed in their eyes.
Significant others also are very likely to offer information, advice, and coping encouragement. Although family and friends intend these acts to be helpful, they can be ineffective for two broad reasons. First, primary group members are typically upset about the individual’s situation themselves, even more so if it creates serious disruptions in their own lives. They are invested in the problem being resolved as quickly as possible to alleviate their own and their loved one’s distress. Invested supporters therefore may minimize the threatening aspects of the problem, insist on maintaining a positive outlook, or pressure the person to recover or problem solve before he or she is ready. These attempts at problem-focused coping assistance can create resentment and resistance in the distressed individual, negating supporters’ intended benefits (Coates and Winston 1983; Dakof and Taylor 1990; Dunkel-Schetter 1984; Martin et al. 1994; Peters-Golden 1982).
Second, and perhaps more important, primary group members often have little or no direct experience with the person’s stressor themselves (S. E. Taylor 2007). 3 Because of experiential dissimilarity, the information or advice they offer will seem too generic, inappropriate, or even misguided to the distressed individual, and their encouraging faith in his or her ability to handle the problem may seem naïve or unrealistic. A sense of alienation or social isolation may follow, again canceling the intended benefits of these forms of coping assistance. In short, because primary group members are often emotionally invested in the person’s recovery and because they frequently are unfamiliar with the specific demands of the stressor, their information, advice, appraisals, and encouragement are likely to be relatively ineffective at softening its health and mental health consequences. More effective coping assistance should come instead from experientially similar others in the secondary network, to whom we now turn.
Emotional sustenance: Secondary group/similar others
Although similar others in secondary groups (e.g., coworkers, supervisors, instructors, church members, voluntary group members) are less personally invested in the individual’s well-being, they engage in other forms of emotionally sustaining behaviors. Direct experiential knowledge is the key to their provisions of effective emotional sustenance as well as active coping assistance. Similar others need not have the same social characteristics (e.g., age, gender, race/ethnicity, socioeconomic status) as the distressed person, but social similarity should boost the utility of the experience-based support they provide.
How does the distressed person come to know that his or her secondary ties include experientially similar others? Social networks spread information about their members’ lives, especially information about tragedies and triumphs. The individual may already know of a similar other, a similar other may hear the bad news and voluntarily come forward, or people in the network may put the two in touch. This is Granovetter’s (1973) point about the “strength of weak ties”: the more extensive the person’s primary and secondary group networks—and the more extensive their networks—the higher the probability the distressed individual will encounter someone with a past similar experience (Gottlieb 1985). Of course, the stressor may be sufficiently rare (e.g., a baby born with a heart defect, a loved one killed by a drunk driver) that peers may not exist in a person’s network of contacts. In that case the distressed person may have to seek support from professionals or from self-help groups of peers in the geographic area or on the Internet.
From previous experience, similar others have an in-depth understanding of the many dimensions and nuances of the stressful situation. Given this, a similar other is able to take the role of the distressed person and imaginatively anticipate his or her emotional reactions and practical concerns. This is the essence of empathy (Clark 1987; Shott 1979). Perceiving empathic understanding can reduce the distressed person’s physiological and affective arousal directly; it is a relief to be understood by someone else, particularly if one’s primary/significant others are unable to grasp the full meaning and implications of the stressful situation that one faces.
Empathic understanding enables distressed individuals to ventilate their feelings and worries with less fear of sanctions. Having “been there” themselves, similar others can tolerate expressions of distress and validate the normalcy of the person’s emotional reactions and worries, rather than deny, criticize, or attempt to change them because they are upsetting or threatening to hear. Ventilation and validation directly reduce arousal and may also indirectly restore the person’s sense of self-worth, shaken by the stressful event itself or by uncertainty about the appropriateness of his or her emotional reactions and concerns (Coates and Winston 1983; Thoits 1986b).
In short, by empathizing, enabling ventilation, and validating feelings and concerns, a similar other is “there” emotionally for the distressed individual, reducing his or her physiological arousal directly and indirectly bolstering his or her possibly weakened self-regard.
Active coping assistance: Secondary group/similar others
In addition to emotional sustenance, similar others offer active coping assistance by supplying information, advice, appraisal feedback, and coping encouragement. Due to past experience, similar others can provide coping assistance that is closely tailored to the exigencies of the problematic situation and known to be effective in solving problems and dampening upset (Suitor and Pillemer 2000; Suitor, Pillemer, and Keeton 1995; Thoits 1986b), lessening situational demands and negative affect directly. Furthermore, guidance and encouragement from knowledgeable others should enhance the distressed individual’s sense of control and reinforce his or her active coping efforts (Berkman 1995). The advice, feedback, guidance, and encouragement supplied by experienced others should be more efficacious in buffering the impacts of adversity than the well-intentioned but less well-informed coping assistance offered by members of the person’s primary network.
Social influence: Secondary group/similar others
Similar others provide support in a third way that does not fit neatly into the categories of emotional sustenance or active coping assistance: They serve as role models who can be observed and emulated (Taylor and Lobel 1989). Similar others are reference individuals against whom the distressed person can compare his or her situational appraisals, emotional reactions, and coping behaviors. He or she studies and imitates the attitudes and behaviors of exemplary others who have gotten through the situation successfully. Similar others’ social influence helps to shape the individual’s coping efforts, reducing situational demands and emotional reactions directly and perhaps indirectly augmenting his or her sense of control over life. Additionally, the sheer existence of peers who have coped effectively with the stressor generates hope; the distressed individual can envision himself or herself in the future, eventually returned to a less beleaguered, everyday life. As a positive emotion, hope counteracts felt tension and upset, and envisioning a desired “possible self” motivates striving toward that goal (Markus and Nurius 1986). In general, similar others’ social influence should guide individuals’ active coping behaviors and motivate continued striving, reducing stressful demands and emotional reactions not only directly but indirectly through a bolstered sense of personal control.
Summing up
In general, significant others’ emotional support (concern and caring, valuing, companionate presence) and instrumental coping assistance should sustain the individual’s sense of mattering, self-esteem, and belonging, which in turn should reduce his or her physiological arousal and emotional distress. Their instrumental support can also lessen the burdens or demands of the problematic situation directly, decreasing the degree of perceived threat and thus the stressor’s physiological and emotional impacts.
Similar others’ emotional sustenance consists of empathic understanding and accepting and validating feelings/concerns, acts that alleviate tension directly as well as shore up wavering self-esteem. Their experientially grounded coping assistance (information, advice, appraisal, and encouragement) directly protects physical and psychological well-being and indirectly fosters a sense of control, which in turn should promote further problem- and emotion-focused coping efforts that diminish the harmful physical and psychological consequences of stress (Taylor and Stanton 2007). Similar others additionally serve as role models to emulate, influencing by example the individual’s coping strategies and sense of personal control.
In short, the relative effectiveness of the support given to the individual and the social psychological mechanisms involved should depend on the type of support supplied and its source: experientially dissimilar versus similar others.
There may be a natural sequence in a distressed person’s encounters with these two sources of support. After the onset of a major stressor, significant others are usually the first to step in with emotional sustenance and instrumental assistance; they are relationally close in the person’s network and normatively obligated to help. As the stressor endures and perhaps generates subsequent difficulties for the individual, primary group members’ abilities or willingness to continue providing support can be depleted. The person may then seek help outside his or her primary network, or experienced secondary group members who have learned about his or her troubles may come forward to offer emotional support and active coping assistance.
Contrasts with “matching” models of stress-buffering
My argument diverges from two other models of stress-buffering that have been proposed in the literature: Cohen and McKay’s (1984) “matching” model and Cutrona and Russell’s (1990) “optimal matching” model. Both sets of theorists assume that the types of social support offered by network members must match the demands of the individual’s stressful situation in order to be efficacious stress buffers. The two models differ in the theoretical aspects of stressors that must be matched.
Cohen and McKay (1984; see also Cohen 1988) argue that stressors can damage the individual’s self-esteem, sense of belonging, ability to appraise the situation, and/or tangible resources. Thus, self-esteem support, belonging support, appraisal support, and tangible support will be needed, respectively. Cohen and McKay (1984) additionally argue that similar others are best able to provide self-esteem and appraisal/informational support; for them, “similar others” are individuals who are comparable to the distressed person in social characteristics, attitudes, personality, or stress experience.
In contrast, Cutrona and Russell (1990) differentiate between controllable and uncontrollable stressors and the life domain in which the stressor occurs. Uncontrollable events require emotional support, particularly comforting, acceptance, and evidence that one is loved. Controllable events require instrumental, informational, and esteem support to aid and encourage the individual’s efforts at problem solving. Stressors that happen in particular life domains require additional specific support provisions. For example, tangible support is needed when assets are lost, reassurance of worth and competence is necessary when failure has occurred, and belonging support is called for when relationships or social roles have been lost or jeopardized. These “optimal matches” between the individual’s needs and support should buffer the physical and psychological impacts of the stressor most strongly.
Both matching models require investigators to identify the types of need evoked by a problematic situation in order to forecast the forms of support that should buffer those situational demands most effectively. In contrast, I have argued more simply that most stressors evoke needs for emotional sustenance and active coping assistance, and supporters typically provide both types of help. Also in contrast, I suggest that the types of emotional sustenance and coping assistance that will most effectively reduce physiological arousal and emotional distress will differ by their source, namely, primary/significant others versus secondary/experientially similar others. Efficacious support from intimates will involve demonstrations of caring and provisions of practical aid—these behaviors are traditionally expected from spouses, relatives, and close friends. Effective support from knowledgeable others (usually persons in the secondary social network) includes empathic understanding, tailored information and advice, and role modeling—actions grounded in supporters’ prior experience. My approach locates the “optimal match” not in a situational need with a supportive act but in a social source with a supportive act, an alternative matching model that may be more predictive as well as less difficult to test.
Concluding Remarks
Obviously, this is a purely theoretical endeavor, inspired by repeated calls over three decades for explication of the mechanisms through which social ties and social support promote and buffer physical health and emotional well-being. I have argued that the social psychological mechanisms that should explain physical health outcomes are substantially the same as those that should account for mental health outcomes and that the same theoretical mechanisms that should mediate the effects of social ties on health and well-being (e.g., sense of mattering, self-esteem, mastery, belonging, social influence) also help to explain how types of support from different network sources produce stress-buffering effects. There is much empirical work to do; research on mediators has only just begun to take off, and detailed studies of stress-buffering dynamics are rare.
Given that three decades of studies have verified the beneficial effects of social ties on health and the stress-alleviating effects of social support, one might be tempted to ask why it matters how social relationships and support produce positive health outcomes. Perhaps all we need to know is that these direct and stress-moderating effects are real and replicable. But to design effective interventions it is crucial to understand intervening mechanisms as well as the relative impact of each of those mechanisms on health outcomes (e.g., Kawachi and Berkman 2001; Seeman 1996; Thoits 1995). By empirically tracing the various pathways from social relationships or supportive acts to physical and emotional well-being, researchers will more closely target potential points of intervention. To date, most interventions have been atheoretical, ad hoc in design, and hit or miss in their effects, producing mixed and disappointing findings (Cohen 2004; Cohen et al. 2000; Hogan, Linden, and Najarian 2002). A clear understanding of how social relationships work to protect well-being is necessary (Gottlieb 2000).
To explicate basic theoretical processes, I have sidestepped a number of issues that must be taken into consideration in future work. First, there is the problem of reverse causality: A person’s preexisting levels of physical and mental health very likely affect his or her possession of social ties and the degree and types of support that he or she perceives or receives from those relationships. Many social psychological mechanisms discussed here (e.g., mattering, self-esteem, mastery, belonging) are probable determinants of individuals’ levels of social integration and support, too (e.g., Thoits 2003). To verify that social ties and supportive behaviors influence physical and mental health through the social psychological conduits that I have hypothesized, longitudinal data or experimental designs will be needed.
Spuriousness is a second issue. Personality factors such as neuroticism, gregariousness, optimism/pessimism, or hostility might explain away the effects of social ties and support on well-being (Cohen 2004; Stroebe and Stroebe 1996; Uchino 2004), as might individuals’ social competence or interactional skills (House et al. 1988). Additionally, community-level social capital or social cohesion (e.g., the density of civic associations, the extent of voluntarism in a community, or even workplace organization) may determine the structure of individuals’ social networks, the degree of support that flows along network ties, and individuals’ physical or mental health (Ertel et al. 2009; Kawachi and Berkman 2001; Lin et al. 1999). Such possible sources of spuriousness will need to be controlled.
Third, there are likely important variations in social integration and in supportive processes by social status and culture (Kawachi and Berkman 2001; S. E. Taylor 2007). The number of ties and the levels and types of support individuals possess depend on their age, gender, race/ethnicity, marital status, and socioeconomic status (e.g., Ertel et al. 2009; Haines, Beggs, and Hurlbert 2008; Kawachi and Berkman 2001; Schnittker 2007; Turner and Marino 1994; Turner and Turner 1999). The processes I have suggested may help to explain status differences in health outcomes, or perhaps these processes may differ significantly by social status, prompting theoretical refinements. Studies also suggest that social integration and supportive dynamics may be contingent on cultural context. Persons socialized in interdependent cultures avoid seeking support in order to maintain harmony, save face, and maintain norms that personal problems should be solved on one’s own; in contrast, individuals raised in Western independent cultures see support networks as resources that can be used to meet personal needs (Badr et al. 2001; S. E. Taylor 2007). The theoretical processes outlined here may be specific to Western cultures in general and to subcultures within the United States that most highly value independence over interdependence in social relationships, an important scope condition that deserves further investigation.
These caveats notwithstanding, repeated calls over three decades for attention to mediating processes suggest that it is time to press forward on this agenda. As a step in this direction, I have suggested a range of social psychological mediators that may be fruitful to explore and argued that different types of support provided by significant and experientially similar others in a person’s network may be efficacious stress buffers through many of the same mechanisms. I look forward to research that revises, refines, and expands these ideas in ways that enable the crafting of effective supportive interventions in the future.
Footnotes
1.
Two other almost trivially obvious but often unremarked contingencies are necessary for the buffering effects of support to unfold: First, persons in the individual’s network must be aware of his or her stressor, else assistance will not be offered. Second, supportive persons who are not themselves the source of the individual’s problem must be available in the network. Unfortunate actors who are in conflict with their sole source of support have few other persons to whom they can turn (and may seek professional help as an alternative). Few (if any) studies assess these contingencies. When studies inadvertently pool together stressful situations in which support givers are and are not available, overall estimates of the power of social support to buffer the impacts of stressors are weakened.
2.
However, instrumental assistance must not be excessive in amount or performed in ways that imply that the provider views the distressed person as incompetent, else such practical help will backfire, creating in the recipient perceptions of indebtedness, dependence, or devaluation (Bolger and Amarel 2007; ![]() ).
).
3.
The exception, as mentioned earlier, would be significant others who are also similar others.