
Abstract
The health consequences of marital dissolution are well known, but little work has examined the impact of health on the risk of marital dissolution. We use a sample of 2,701 marriages from the Health and Retirement Study to examine the role of serious physical illness onset in subsequent marital dissolution via either divorce or widowhood. We use a series of discrete time event history models with competing risks to estimate the impact of husband’s and wife’s physical illness onset on risk of divorce and widowhood. We find that only measures of wife’s illness onset are associated with elevated risk of divorce, while measures of either spouse’s illness onset is associated with elevated risk of widowhood. Further, in the case of heart problems, we find that this gender difference is statistically significant. These findings suggest health as a determinant of marital dissolution in later life via both biological and gendered social pathways.
A large body of literature has identified marital status as a strong predictor of health and well-being. Not only are the married healthier than the unmarried (e.g., Lillard and Waite 1995; Umberson 1992), but studies also find that both divorce and widowhood are precursors to declines in physical and mental health (e.g., Hughes and Waite 2009; Williams and Umberson 2004). Less attention, however, has been paid to how health may be a determinant of marital status. Work in this area has tended to focus on the positive selection of the healthier into marriage (e.g., Byrne et al. 1989; Smith and Smith 2010), but poor health may be an equally important force for selection out of marriage. Biological processes associated with poor health and illness increase mortality risk (Murphy, Xu, and Kochanek 2013) and thus elevate the risk of marital dissolution via widowhood. However, physical illness may also increase divorce risk via social processes by operating as a stressor on the marital relationship, leading to lower marital quality (Amato 2010; Daniel et al., 2009; Yorgason, Booth, and Johnson 2008). Illness may initiate changes to spouses’ roles—in particular, increasing caregiving responsibilities for the healthy spouse—which can tax marital relationship dynamics (Wolff and Kasper 2006). Illness may also decrease household income due to the inability of one or both spouses to work (Teachman 2010), which may also increase marital strain.
Only a few studies have examined the role of poor health in subsequent divorce, and these studies are mixed in their findings, with some finding poor health positively associated with elevated divorce risk (Joung et al. 1998; Teachman 2010; Wilson and Waddoups 2002) and others finding no association (Charles and Stephens 2004). These studies also tend to examine relatively young samples, although the implications of poor health for divorce may be particularly important as individuals age. Chronic morbidity incidence increases with age (Crimmins and Beltrán-Sánchez 2011), while decreasing mortality associated with several chronic diseases (Crimmins 2004) means that individuals are living longer with chronic illnesses and marriages are at decreased risk of dissolution due to widowhood than in the past. One consequence of this increased likelihood of longer term survival with chronic illness may be increased divorce risk.
The relationship between spousal health and divorce may also vary by gender. Small clinical studies have found a larger risk of divorce when wives become ill than when husbands do (e.g., Glantz et al. 2009) or in particular, when wives as opposed to husbands are diagnosed with cancer (Carlsen et al. 2007). This variation by gender is consistent with the increasing advantage enjoyed by men in (re)marriage markets over the life course due to an ever-expanding pool of potential partners and with findings that husbands may find caring for an ill spouse more stressful than do wives (England 2005). While the few clinical studies finding gender differences in the impact of illness on divorce risk are intriguing, these results have not been replicated in large social surveys or across an array of illnesses.
We use a sample of marriages from the initial cohort of the nationally representative Health and Retirement Study (HRS; 1992–2010) to examine the relationship between serious physical illness onset (i.e., cancer, heart problems, lung disease, and/or stroke) among marriages in which at least one spouse is middle-aged at baseline and subsequent marital dissolution due to either divorce or widowhood. We also look at whether the relationship between illness and marriage dissolution varies by specific illness or in the case of divorce, by gender. Estimating competing risk models for divorce and widowhood (compared with remaining married) for this sample contributes to research addressing trends in the relative contributions of divorce and widowhood to marriage dissolution at older ages (Stevenson and Wolfers 2007). Examining several types of physical illnesses/conditions enables a consideration of how the risk of divorce may be impacted by the associated characteristics of each illness/condition, such as level of disability, chronicity, and social meaning. Finally, analyzing the risk of divorce by whether it is the husband or wife who experiences illness onset furthers understanding of gendered experiences at the intersections of health and marriage in later life.
Background
Health as a Determinant of Marital Status
The relationship between marital status and health is well known. Numerous studies have documented the health benefits to getting married (Lillard and Waite 1995; Umberson 1992). Studies also find negative health consequences of marital dissolution due to either divorce (Hughes and Waite 2009; Williams and Umberson 2004) or widowhood (Hughes and Waite 2009). The vast majority of this literature, however, has focused on the impact of marital status and transitions on health rather than on the impact of health on subsequent marital status.
Much of the literature focusing on health as a determinant of marital status has focused on positive selection of the healthy into marriage (e.g., Byrne et al. 1989; Fikkan and Rothblum 2012; Gortmaker et al. 1993; Smith and Smith 2010). Some other studies also suggest that health not only functions as a determinant of entry into marriage but also of marital dissolution. Beyond the obvious pathway between a partner’s health decline and subsequent widowhood, a few studies have examined physical health as a risk factor for marital dissolution via divorce. A meta-analysis of social and economic consequences of stroke among working-age adults also found some evidence of an elevated divorce risk following stroke as well as increased marital conflict and decreased sexual activity (Daniel et al. 2009), which may be precursors for divorce. Other studies have found that the relationship between illness and divorce may vary by specific illness. To illustrate, a Norwegian study did not find strong evidence for elevated divorced following cancer diagnosis, except for cervical and testicular cancers, which tend to strike younger individuals than many other cancers (Syse and Kravdal 2007). However, some studies find no evidence that poor health is a risk factor for divorce. For example, in their examination of marriages among mostly working-aged individuals, Charles and Stephens (2004) did not find disability related to subsequent divorce.
While the extant literature does not demonstrate a clear association between illness onset and risk of divorce, there are several reasons why we may expect that illness onset is linked to subsequent divorce. First, a sick individual may require assistance with daily personal care tasks, and for those who are married, the ill individual’s spouse is most often the primary caregiver (Wolff and Kasper 2006). Caregiving has been identified as a source of psychological strain that may lead to increased morbidity and mortality among caregivers themselves (Schulz and Beach 1999). Second, caregiving may alter the relationship dynamics between husband and wife in ways that are distressing, particularly if initial marital quality was low (Choi and Marks 2006). In addition, one spouse’s illness may affect household income by interfering with either the ill or caregiving spouse’s ability to engage in gainful employment. While both job loss and earnings shocks have been linked to elevated divorce risk (Charles and Stephens 2004; Weiss and Willis 1997), Singleton (2012) demonstrated that the impact of work-preventing disability onset on divorce was greatest among younger and better educated men, which suggests that lost potential earnings may not be as meaningful for older couples.
A limitation of most of the studies that examine health and divorce is a focus on relatively young populations. Recent evidence suggests, however, that divorce at older ages is on the rise. The number of divorces occurring among adults aged 50 and older has doubled in the past two decades, and in 2010, one in four divorces occurred among those over 50 (Brown and Lin 2012). Late middle age and early older ages are the stages in the life course when many individuals experience the onset of serious health conditions, and given more permissive attitudes toward divorce and the more frequent experience of divorce earlier in life (Uhlenberg and Myers 1981), illness onset may be an increasingly important risk factor for divorce among more recent cohorts of older Americans.
One prior study of marriages in which at least one spouse was in late middle or early old age found that marriages in which only one spouse was ill were at elevated risk of divorce compared with marriages in which both spouses were healthy, but only among marriages in which both spouses reported high levels of marital satisfaction (Wilson and Waddoups 2002). This study represents an important first step in the examination of the potential consequences of illness for divorce in middle and older ages. However, this study suffers from several limitations, most notably that health is assessed with self-rated health measures rather than with illness diagnosis. While self-rated health measures are highly correlated with objective measures of health (Molarius and Janson 2002), such measures are also subject to drawbacks, such as gender differences in health-rating styles (Grol-Prokopczyk, Freese, and Hauser 2011) and the role of inputs not specifically related to physical health such as depression (Molarius and Janson 2002) or even marital quality itself, raising concerns of endogeneity.
Variation in the Relationship between Illness and Marital Dissolution
Most studies analyzing the effects of health on marital dissolution either have used relatively general measures of health or have examined a single condition; however, different illnesses/conditions may have different implications for marital dissolution. First, variation in the association of specific illnesses with death (Murphy et al. 2013) will impact the relative risks of widowhood versus divorce. Illnesses associated with high mortality risk, such as heart disease, are associated with lower risk of divorce simply because increased mortality risk makes it less likely that both spouses will remain alive, a basic condition for whether the marriage is at risk of divorce or not.
In addition, illnesses also vary in the extent and duration of associated disabilities, which have implications for caregiving burden, work limitations, and curtailment of other life domains. Stroke, for instance, is the leading cause of major long-term disability (Roger et al. 2012) and might create more chronic stressors for a marriage than an illness like cancer, which is often associated with more modest, shorter term disability linked to treatment side effects. Cognitive decline-related disability, which is associated with illnesses such as stroke or heart disease, may be more stressful for caregivers than physical disability alone (Pinquart and Sörensen 2003). In addition, the duration and probability of recovery from a disability may induce variation in the relationship between the associated illness and divorce. Divorce risk might be higher for conditions such as chronic obstructive pulmonary disease (COPD) in which recovery is unlikely and caregiving may extend for many years.
Illnesses also vary in their social meanings, which may have implications for their impact on divorce. Levels of research funding, positive media attention, and societal support vary across conditions and illnesses (Best 2012; Kedrowski and Sarow 2007), with cancer, heart disease, and stroke being the subjects of large public health and advertising campaigns, while illnesses such as COPD—which has a direct association with the stigmatized behavior of smoking (Mannino and Buist 2007)—receive little attention. Such campaigns increase public awareness and popular support for these conditions—which may lessen the emotional burden for couples living with them. But perhaps as important, they also influence the availability of concrete resources such as support groups, which can play an important role in buffering the stress of illness. These differences across health conditions may influence how couples perceive their struggle against an illness and their hopefulness for the future—perceptions that may impact their adjustment to caregiving and care-receiving roles.
Gender, Illness, and Marital Dissolution
Gender may also moderate the relationship between poor health and marital dissolution. A few clinical studies have found higher divorce risks when wives, as opposed to husbands, experience cancer (Glantz et al. 2009; Kirchhoff et al. 2012) or for cancers that affect only women, such as cervical cancer (Carlsen et al. 2007). These findings, however, have been gleaned from relatively young (Kirchhoff et al. 2012) or small samples (Glantz et al. 2009) and are limited to the study of cancer.
Several social processes suggest that middle-aged and older couples may be at greater risk of divorce when wives become ill than when husbands do. First, because sex ratios become increasingly skewed toward women at older ages given women’s greater longevity (Austad 2006), and because men tend to marry women younger than they are (Presser 1975), older men are advantaged in the remarriage market by a larger pool of potential partners than is available to older women. Marriage markets are skewed as well by the stronger normative value of youthful beauty for women in that “women are devalued [as potential partners] as they age more than men are” (England and McClintock 2010:814). Indeed, not only are men much more likely to remarry than women (Shafer and James 2013), the older men are at remarriage, the greater the age gap is with their wives (England and McClintock 2010).
In addition, gender norms regarding the role changes that frequently accompany illness may yield gender differences in the relationship between illness and subsequent divorce. Women are socialized and habituated to caregiving for others across the life course (England 2005), and studies suggest that this extends to caring for ill husbands (Wolff and Kasper 2006). However, caregiving is not fully reciprocated by husbands for sick wives; wives receiving care were more likely to report experiencing gaps in needed caregiving from their spouses than husbands (Allen 1994). Given the gendered nature of caregiving and care receiving and caregiving’s frequent stressful nature, it is plausible that situations in which ill wives are dependent on husbands for care are more stressful than when wives are caring for ill husbands. On the other hand, illness may be more detrimental in cases where ill husbands must withdraw from employment, given the traditional emphasis on breadwinning for men (Becker 1981). However, as evidenced by Singleton’s (2012) study on disability, earnings, and divorce, the importance of breadwinning may be less important at older ages when labor force detachment and declines in earnings for men are more age-normative compared with earlier periods of the life course.
Data and Methods
Data
We used data from Waves 1 through 10 of the RAND Health and Retirement Study data file, a user-friendly, harmonized data set generated from the original HRS files. The HRS is an ongoing, nationally representative, prospective panel study of Americans over the age of 50 years. Detailed health and socioedemographic information has been collected from respondents and their spouses (regardless of the spouse’s age) every two years since 1992. We focused on the original HRS sample in which at least one spouse within the marriage is aged 51 to 61 at baseline, as prior work has identified this approximate age range where the risk of divorce is highest in the later life course (Brown and Lin 2012).
Analytic Sample
We constructed our analytic sample of marriages based on 9,348 HRS individuals who are married to one another at baseline (Wave 1), yielding 4,674 marriages. As we are interested in the role of serious physical illness onset as a risk factor for marital dissolution, we excluded marriages in which either spouse reports having ever had any of the four chronic conditions of interest at baseline, reducing the sample size to 3,104 marriages. If we were to include those who had ever had any of the serious illnesses of interest, we might be selecting for particularly robust marriages, biasing downward our estimates of the relationship between illness and divorce. Further, we do not know the date of diagnosis for illness at baseline relative to date of marriage, making it impossible to ascertain the duration of time in which couples lived with illness prior to the study. We also excluded marriages that dissolve either due to divorce/separation or widowhood in the second wave (1994) as it cannot be ensured that our key independent variable, illness onset, in Wave 2 preceded a change in marital status (see Statistical Analysis, in the following), reducing the sample size to 2,786 marriages. Additionally, we excluded those missing information on any covariates (missing data results in a loss of approximately 2.2% of marriages) or with a weight of zero, yielding a final analytic sample of 2,701 marriages, which correspond to 16,940 wave-to-wave marriage periods for the pooled illness model. Analyses were weighted using Wave 1 household weights and clustered at the individual marriage-wave level. Our selection criteria facilitated the identification of the effect of illness onset on marital dissolution but decreased the representativeness of our sample and thus the generalizability of our findings to all marriages in the sampling frame age range. Though our data are not nationally representative of all marriages in this age range, our sample does consist of a random sample of marriages in this select healthy population and thus has a considerable advantage over many other studies examining marital status that have relied on convenience samples.
Measures
Dependent Variable: Marital Dissolution Due to Divorce or Widowhood
The main outcome of interest is whether a Wave 1 marriage ends in divorce or widowhood in a subsequent wave. A marriage was defined to dissolve due to widowhood if either spouse died between consecutive waves and the marriage was intact in the penultimate wave. A marriage was defined to dissolve in divorce if either spouse reported being divorced since the prior wave or in the rare case that either spouse divorced and remarried between consecutive waves and thus never reported being divorced if either spouse’s total marriage count increased.
Key Independent Variable: Physical Illness Onset of Husband or Wife
The primary independent variable is respondent or spousal illness onset. We focus on the onset of four major life-threatening illnesses, cancer, heart problems, lung disease, and stroke, which together comprise a substantial portion of chronic disease burden in the United States (Murphy et al. 2013) and pose a risk for marital dissolution via the death of an individual spouse as well as potentially via divorce. Chronic illness onset measures were based on measures of whether respondent reported a new diagnosis of a particular disease by a doctor since the last interview wave—enabling us to identify the timing of initial illness onset. We examined whether husband or wife experienced the new onset of any of these four conditions (results in Table 3) as well as the onset of each specific condition modeled simultaneously (results in Table 4). Illness onset was entered as a time-varying measure and was lagged by one period to ensure that illness onset precedes marital dissolution. The illness onset variable was coded as 1 for each subsequent wave in order to acknowledge that the full impacts of illness onset may not be fully experienced until a substantial period of time has elapsed following illness onset. Consistent with prior studies, cancer diagnosis excludes skin cancers. Heart problems include “heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems,” and lung disease includes but is not limited to “chronic lung disease such as chronic bronchitis or emphysema.”
Other Baseline Covariates
We also include measures of several factors that prior research has found to be associated with divorce and/or widowhood (via individual mortality). Given the challenges of interpreting time-varying covariates as potential mechanisms for illness onset (see Goodliffe 2003) and for additional substantive reasons (e.g., income typically declines for both sick and well individuals in this age range), none of the covariates listed in the following are time-varying. These include: age (in years), college education (1 = yes, 0 = no), race-ethnicity (1 = nonwhite and/or Hispanic, 0 = white, non-Hispanic), marital duration (1 = less than 10 years, 0 = more than 10 years), and initial marital satisfaction. Marital satisfaction was ascertained with the following question: “Are you very satisfied, somewhat satisfied, about evenly satisfied and dissatisfied, somewhat dissatisfied, or very dissatisfied with your marriage?” The original assumed-interval measure is retained with “very satisfied” as the reference category for the marital satisfaction measure. Marriages were coded as remarriages if the Wave 1 marriage was a remarriage for either spouse. We also include a measure of husband and wife age differences at baseline; the age difference categories include: wife older by 11 or more years, wife older by 5 to 10 years, wife older by 3 or 4 years, husband and wife within 2 years’ age of one another (reference category), husband older by 3 or 4 years, husband older by 5 to 10 years, and husband older by 11 or more years.
We also include measures of socioeconomic status: total household income at baseline, total household non-housing assets at baseline, and home ownership at baseline. We include both measures of income and assets as prior research suggests that assets may be an especially important predictor of health at older ages (Robert and House 1996). We include measures of both total household (non-housing) wealth and home ownership because the former reflects relatively liquid assets at baseline while the latter reflects less liquid assets that represent a substantial component of wealth holdings for many Americans. Missing values for income and assets were imputed by RAND. Household income is based on the sum of husband’s and wife’s income from earnings, pensions and annuities, Supplemental Security Income and Social Security Disability, Social Security, unemployment and worker’s compensation, and other government transfers and then coded into quintiles (bottom quintile is reference). Non-housing assets are coded into five categories: negative wealth (i.e., debt), $0 to $50,000 (reference category), $50,000 to $100,000, $100,000 to $250,000, and $250,000 or more. We also include dichotomous indicators for health insurance for both husband and wife.
Due to collinearity, we were unable to simultaneously model both spouses’ education, race-ethnicity, or marital satisfaction. Models presented use husband’s education and race-ethnicity and wife’s marital satisfaction, as there is less missing data for wife’s reports of marital satisfaction, and there is also more variation in martial satisfaction among wives compared with husbands (not shown). Additional analysis (not shown) indicated that results do not differ if wife’s race-ethnicity or education is used instead of husband’s or if husband’s marital satisfaction is used.
Statistical Analysis
To assess risk of marital dissolution, we estimated a series of discrete time event history models with competing events using multinomial logistic regression. Divorce/separation (referred to as “divorce” hereafter) or widowhood were modeled as competing events, as marriages with at least one spouse in the HRS age range are at risk for both divorce and widowhood. The continuously married category is the reference category. We employ a closed cohort design in which Wave 1 marriages are followed until the marriage dissolves or is censored. We focus on the cohort of Wave 1 marriages since this is the only time period in which marital satisfaction—a key covariate of interest—is collected. We generated a marriage-period data set in which each marriage contributes a marriage-period until marital dissolution occurs or until the marriage is censored. A marriage is defined as censored if the Wave 1 marriage remains intact through 2010 or if either spouse misses a wave. For marriages in which spouses differed in the number of waves they participated in the survey, the minimum observation length of the two spouses was taken and the marriage was subsequently coded as censored. Marriages are not followed after a wave is missed, as critical information (e.g., new illness onset) is missing and is difficult to impute. Additional analysis of survey attrition revealed that many marriages attrit (939 marriages out of 2,701 total, or 34.8%; results in Table 2). Though attrition is considerable, the analytic decision to include marriages in the risk set until attrition maximizes available information compared with, say, deletion of couples that ever attrit. Furthermore, prior research has noted that attrition rates for a two-person household in HRS is nearly identical to a one-person household (Banks, Muriel, and Smith 2011), which suggests that the attrition in our sample was not significantly altered by using either spouse’s attrition status. Period (length of observation) was included as both a linear and quadratic term as results from log-likelihood ratio tests suggested including both linear and quadratic terms had better model fit compared with only including the linear term (not shown). These linear and quadratic period terms can alternatively be interpreted as reflecting the aging of husbands and wives, controlling for their baseline age. We present results both as log odds and as marginal effects with other covariates held at their means, which can be interpreted as probabilities (Long and Freese 2006).
Results
Descriptive statistics are displayed in Table 1. Marriages are much more likely to end by widowhood than divorce. Twenty-four percent of marriages dissolve due to widowhood, compared with 6% due to divorce. In addition, there is considerable attrition over the 18 years of the study—35% of marriages attrit before the end of the study period—more than are lost via widowhood and divorce combined. The distribution of initial illness onset for husbands and wives as well as timing of divorce and widowhood by wave can be found in Table 2. Not surprisingly, there is a substantial amount of new chronic illness onset (cancer, heart problems, lung disease, and/or stroke) among husbands and wives (Table 2) within marriages. Consistent with prior research, we observe an increase in physical illness incidence across waves (as husbands and wives age), and husbands experience higher illness incidence than wives. Looking at the distribution of divorce and widowhood by wave, we see that widowhood is a more common pathway out of marriage than divorce in all waves.
Analytic Sample Weighted Baseline Descriptive Statistics, Health and Retirement Study (1992–2010) (n = 2,701 Marriages).
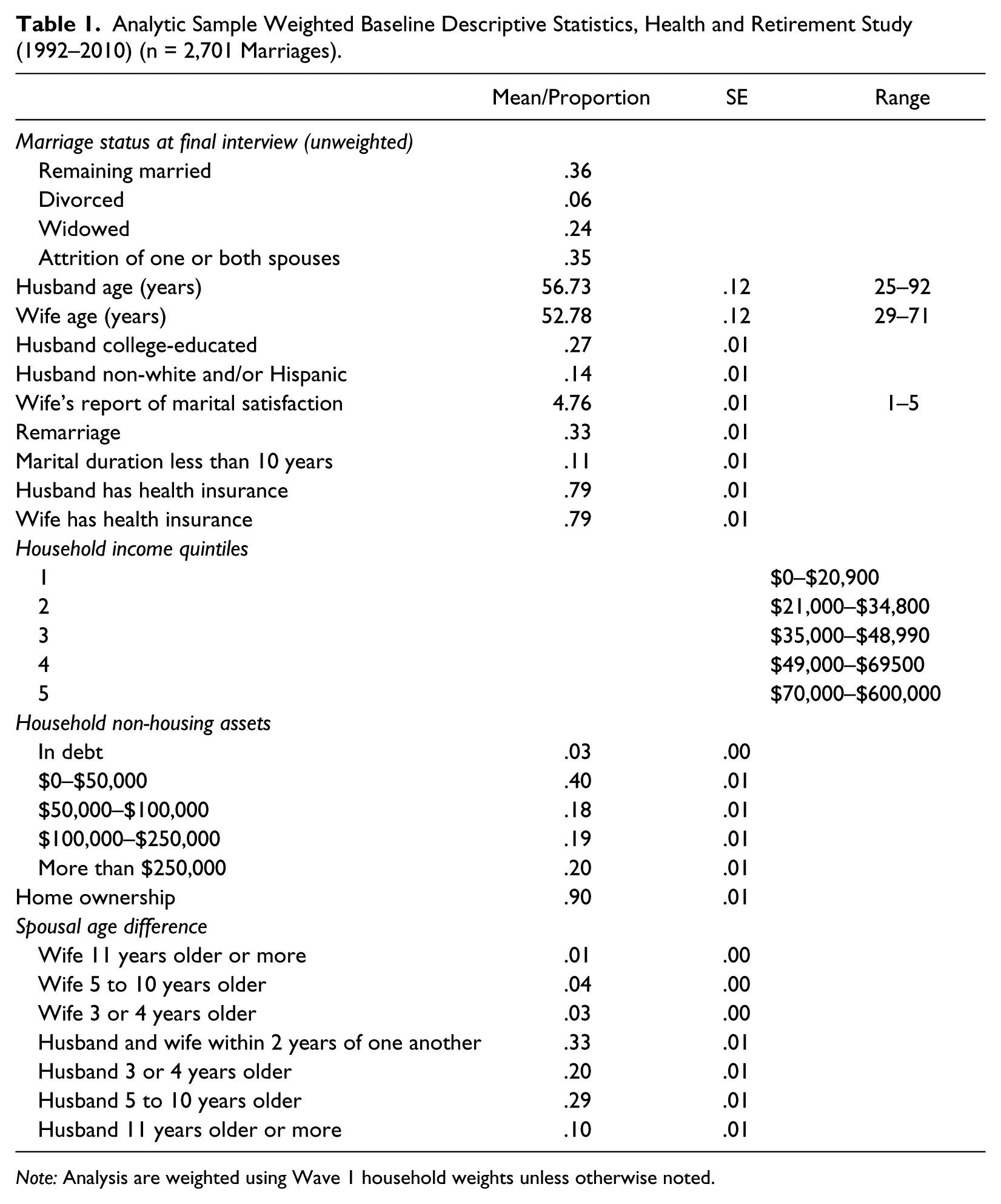
Note: Analysis are weighted using Wave 1 household weights unless otherwise noted.
Divorce, Widowhood, Attrition, and Illness Onset by Wave, Health and Retirement Study (1992–2010).
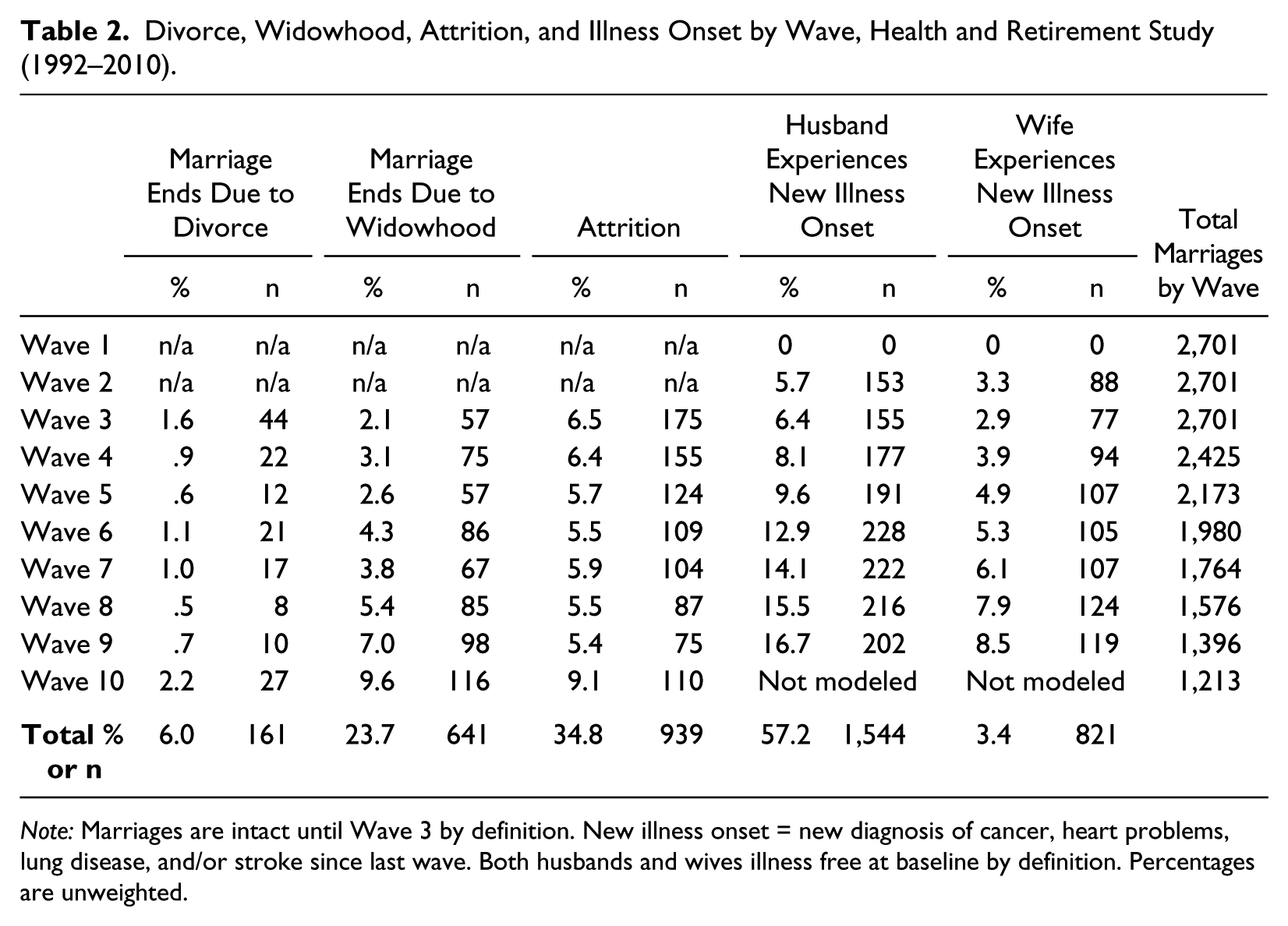
Note: Marriages are intact until Wave 3 by definition. New illness onset = new diagnosis of cancer, heart problems, lung disease, and/or stroke since last wave. Both husbands and wives illness free at baseline by definition. Percentages are unweighted.
Table 3 displays multinomial logistic regression models predicting marital dissolution due to divorce or widowhood as a function of onset of any of the four illnesses (cancer, heart problems, lung disease, and/or stroke). Husband’s illness onset is not associated with subsequent divorce compared with remaining married. In contrast, wife’s illness onset is positively associated with 1% higher probability of subsequent divorce compared with remaining married. However, we fail to reject a test of the null hypothesis that the coefficients for husband’s illness onset and wife’s illness onset are equal (p = .1532). This post hoc test represents a formal test of a gender difference in the relationship of illness onset and divorce. Our failure to reject this hypothesis suggests that there is truly no gender difference in the relationship between illness onset and divorce. However, given that divorce is relatively rare in this population, an alternative explanation is that the study is under-powered for such a test. In addition, we find that poor baseline marital satisfaction is positively associated with subsequent divorce, as is husband being much (11 years or more) older than wife. Husband’s health insurance appears to be protective against divorce. The statistically significant negative period quadratic term indicates nonlinearity in the risk of divorce over the study period. More specifically, consistent with prior work, the risk of divorce decreases with long periods of marital duration.
Multinomial Logistic Regression Results: Marriage Ending via Divorce or Widowhood Compared to Remaining Married by Pooled Illness Onset (Cancer, Heart Problems, Lung Disease, and/or Stroke) and Other Covariates, Health and Retirement Study (1992–2010) (n = 2,701 Marriages; 16,940 Marriage Periods).
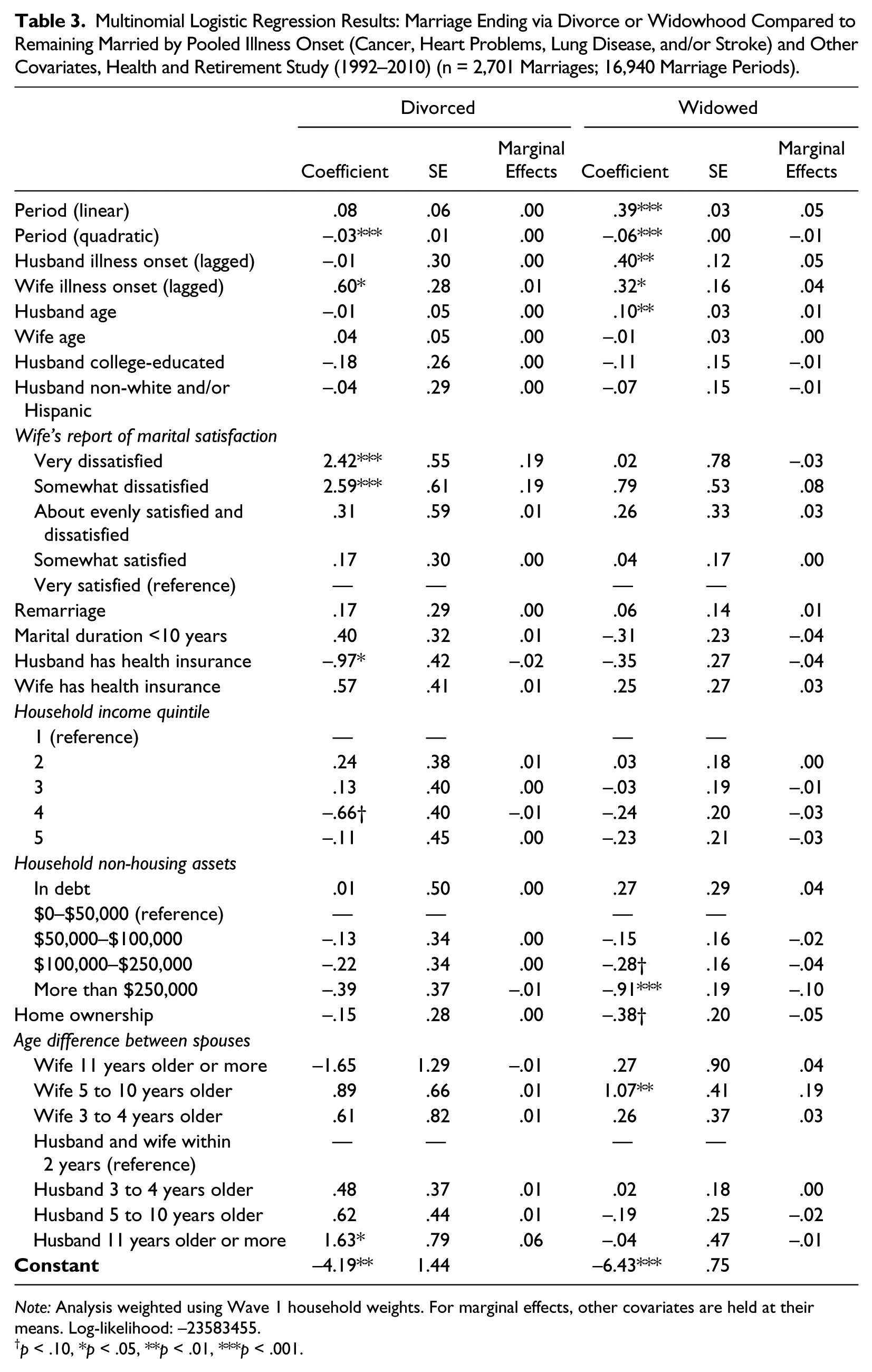
Note: Analysis weighted using Wave 1 household weights. For marginal effects, other covariates are held at their means. Log-likelihood: –23583455.
p < .10, *p < .05, **p < .01, ***p < .001.
Turning to the risk of subsequent widowhood versus remaining married, we see that husband’s illness onset is associated with 5% higher probability of widowhood, and wife’s illness onset is associated with 4% higher probability of widowhood compared with staying married. As for divorce, we fail to reject a test of the null hypothesis that the coefficients for husband’s illness onset and wife’s illness onset are equal. Husband age is positively associated with widowhood, which may reflect dimensions of health not captured by the chronic disease onset measure. High levels of non-housing assets are protective against widowhood at the p < .05 level, as is home ownership at the p < .10 level. Marriages in which wives are 5 to 10 years older than husbands are also more likely to dissolve via widowhood. Finally, the (positive) linear and (negative) quadratic period terms are also statistically significant, indicating that marital dissolution via widowhood increases with time but at a slower rate as time elapses.
Next we turn to illness-specific (with separate indicators for cancer, heart problems, lung disease, and stroke) associations with marital dissolution in Table 4. Neither husband’s nor wife’s cancer or lung disease onset is associated with subsequent divorce. Wife’s heart problems onset (but not husband’s) is positively associated with a 2% higher probability of subsequent divorce compared with staying married. Further, we reject a null hypothesis of the equality of the heart problem onset coefficients for husband and wife at the p < .05 level, providing support that the relationship between heart problem onset and divorce is gendered. Wife’s stroke onset is positively associated with a 3% higher probability of divorce compared with staying married; however, this association is not statistically significantly different from the coefficient for husband’s stroke (p = .3818), which is itself not statistically significant. Associations between other covariates and divorce and consistent with the results presented in Table 3.
Multinomial Logistic Regression Results: Marriage Ending via Divorce or Widowhood Compared to Remaining Married by Specific Illness Onset and Other Covariates, Health and Retirement Study (1992–2010) (n = 2,701 Marriages; 16,940 Marriage Periods).
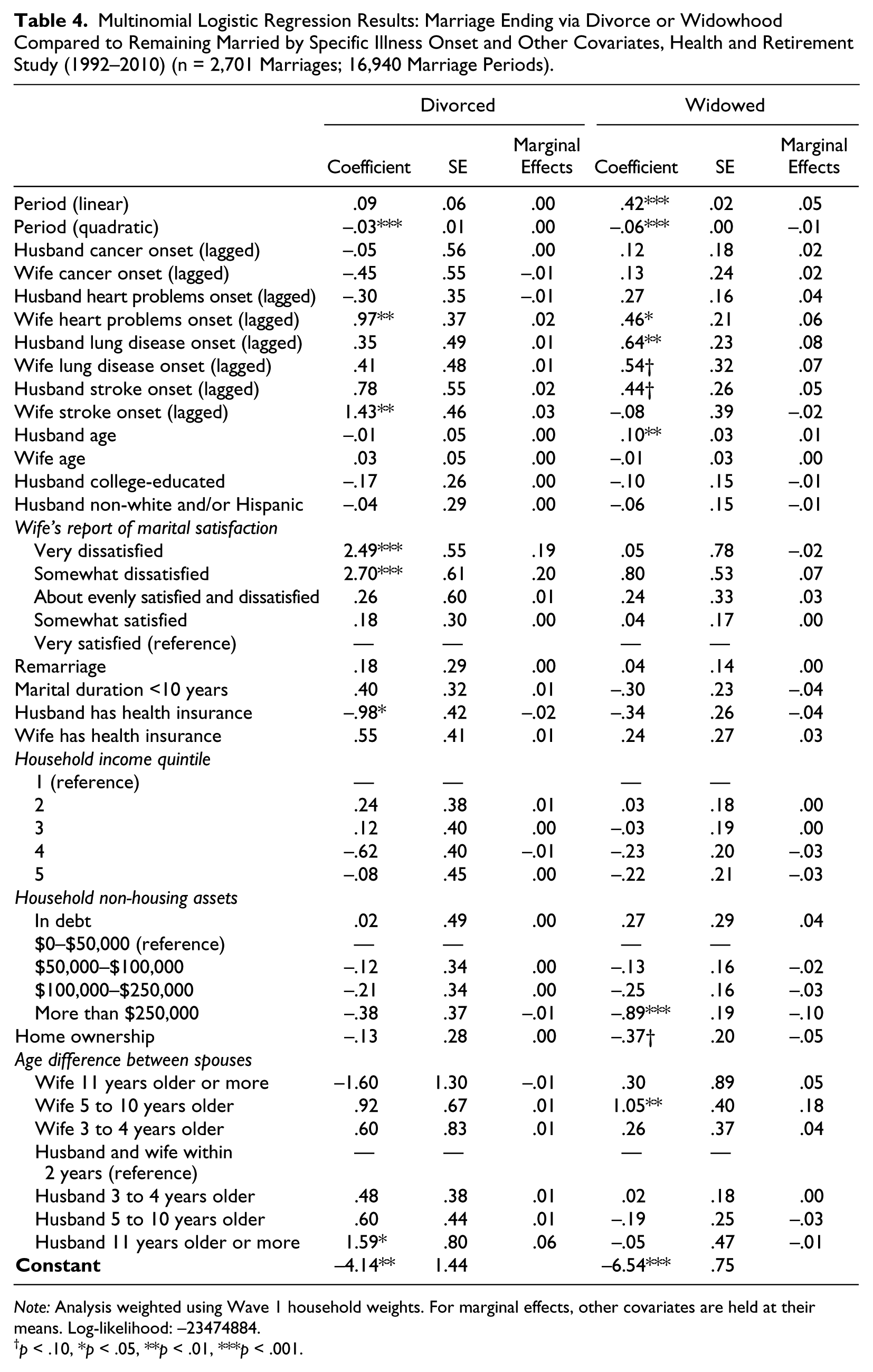
Note: Analysis weighted using Wave 1 household weights. For marginal effects, other covariates are held at their means. Log-likelihood: –23474884.
p < .10, *p < .05, **p < .01, ***p < .001.
Looking at marital dissolution due to widowhood, we see that neither husband’s or wife’s cancer diagnosis, nor husband’s heart problems onset, nor wife’s stroke onset are associated with elevated risk of widowhood. Wife’s heart problems onset is associated with a 6% higher probability of marital dissolution via widowhood compared with remaining married. Husband’s lung disease onset is associated with 8% higher probability of widowhood, and wife’s lung disease onset is associated with 7% higher probability of widowhood compared with remaining married, though the relationship for wives is only marginally significant. Husband’s stroke onset has a marginally significant statistical association with 5% higher probability of widowhood. We fail to reject the null hypothesis of equality of coefficients by gender for each specific illness. Associations between other covariates and widowhood are quite similar to results presented in Table 3.
Supplementary Analysis
We also conducted several supplementary analyses. First, we conducted a first-differences pooled ordinary least squares model (estimating the linear probability of divorce vs. remaining married) to assess the robustness of our results to unobserved time-invariant variables that might be correlated with our observed covariates and thus bias our results. Our first differences estimate of the probability of divorce following wife’s illness onset was not statistically significant. Thus, we conclude that our findings are not robust to unobserved time-invariant variables. This suggests that unobserved characteristics—such as marital commitment—may impact the relationship between illness and subsequent divorce risk. We looked at Catholic religious identity of husband and/or wife as well as whether either (or both spouses) have children. Neither Catholic identity nor the number of children predicted divorce at the p < .05 level when added to the panel of covariates examined in the main analyses, and the main substantive findings remained unchanged. In addition, we included controls for husband’s and wife’s baseline self-rated health, as there may be meaningful physical health variation not captured by the absence of ever-diagnosis of the focal physical illnesses at baseline. Again, our substantive findings remain unchanged, though the self-rated health of both partners independently predicts widowhood. We also included baseline smoking status as a covariate that did not change substantive findings, though both husband’s and wife’s current smoking also predict marital dissolution due to widowhood. Additionally, we tested for interactions between illness onset and a variety of other covariates, including marital satisfaction, race-ethnicity, and education added to the model with main effects. Interactions were not statistically significant. Finally, we re-ran our main analyses without weights; results were substantively quite similar.
Discussion
The present study examined whether measures of illness onset constituted a risk factor for marital dissolution at middle and older ages. In our analysis examining the onset of any of four serious illnesses (cancer, heart problems, lung disease, and/or stroke), we find that only wife’s illness onset is associated with elevated risk of divorce, while either husband or wife’s illness onset is associated with elevated risk of widowhood. However, we fail to reject the null hypothesis of equality of coefficients by gender in these pooled models, which suggests that there is no difference in divorce risk depending on which spouse experiences onset of any of these conditions. When we turn to specific illnesses, we find some evidence that the relationship between illness onset and divorce varies by specific illness. Wife’s (lagged) heart problems onset and stroke onset are both statistically significant positive predictors of divorce, while none of the measures of husband’s illness onset are associated with divorce. In addition, we reject the null hypothesis of equality of coefficients for husband’s heart problems onset and wife’s heart problems onset (p < .05). These hypothesis tests are critical in the formal evaluation of gender differences and provide evidence that the association between heart problems and divorce depends on the gender of the spouse who becomes ill. Taking pooled and disease-specific results together, these findings suggest that the relationship between disease and divorce risk varies by gender in the case of one specific health condition—heart problems.
Prior work has shown that the physiological symptoms of aspects of cardiovascular disease such as heart attacks vary by gender (Riedinger et al. 2001). Our work suggests that the impacts of cardiovascular disease on marriage, at least in the case of divorce, also vary by gender. Our finding that cancer onset was not associated with divorce is in contrast to prior clinical studies that found elevated divorce risks for reproductive cancers (Carlsen et al. 2007; Syse and Kravdal 2007). Besides concerns about selection issues and differently aged samples, our lack of findings for cancer may reflect further variation within the experience of cancer, though a more fine-grained analysis by type of cancer also comes at an additional cost to statistical power.
An important caveat to our results is that in four out of five cases, we fail to reject the null hypothesis of equality of coefficients by gender. We fail to reject the null hypothesis in the case of pooled illness, cancer, lung disease, and stroke onset. The only case in which we reject the null hypothesis of equality of coefficients across gender is for heart problems. In addition, that we do not find husband’s illness to be a predictor of divorce in either pooled or illness-specific models does not mean that husband’s health does not constitute a risk factor for divorce in other circumstances. Future work should examine other dimensions of health (e.g., disability, mental illness) in a variety of diverse samples to further understanding of how life course stage and the lived experience of illness are related to the relationship among health, divorce, and gender.
Our focus on illness and divorce in middle and older ages contributes to understanding the risk factors for divorce in later life, which constitute a growing share of all divorces (Brown and Lin 2012). Still, it is important to acknowledge that the majority of divorces occur earlier in life, when illness is less common (and less normative), which may make it more stressful to marriages. Recent research examining marriages among younger people found that husbands’ –but not wives’ –work-limiting health conditions were associated with elevated risk of divorce (e.g. Teachman 2010). These findings may reflect greater emphasis on husbands’ employment earlier in the life course. Taken together, the present study and prior work on divorce across the life course point to the importance of contextualizing divorce risk factors in conjunction with other factors, such as race and class. Further, given greater economic symmetry between spouses in more younger cohorts, birth cohort as well as age may alter the extent to which spouse’s gender modifies illness onset as a risk factor for divorce.
Finally, though divorce is increasing at older ages and our study provides some evidence that health is a risk factor for divorce in the case of heart problems, it is important to remember that widowhood is a more frequent pathway out of marriage than divorce and that health is more strongly associated with widowhood than divorce. In the case of pooled illness onset, wife’s illness onset is associated with a 1% increase in the risk of divorce, and there is no association between husband’s illness onset and divorce. In contrast, husband’s and wife’s illness onset are associated with a five and four percentage point increase in the risk of widowhood, respectively.
Prior work has suggested that the better health of the married is not just due to the healthier selecting into marriage but beneficial social processes (i.e., social causation) occurring within marriages, such as spouses encouraging one another in healthy lifestyle practices (Umberson 1992). Our work indicates that health selection processes should not be discounted and should be considered more carefully on both conceptual and methodological grounds in future research. Specifically, researchers should consider how health operates as a stressor on marriages, and should exercise caution in interpreting cross-sectional studies as evidence of the benefits of marriage. Further, these selection processes are gendered in nature. Women are vulnerable to marital dissolution in the face of illness through both widowhood and divorce. Women’s greater longevity compared with men’s (Austad 2006) and the typical partnering of women with men who are older than them (England and McClintock 2010) mean that married women are likely to survive their husbands. Consequently, women are more likely to experience widowhood than men. Our work indicates that in the case of heart problems, women’s health has consequences for marital dissolution as women’s own illness (but not their husband’s illness) elevates their risk of divorce. In turn, both widowhood and divorce have large consequences for health (Hughes and Waite 2009; Williams and Umberson 2004).
Prior research highlights variations in illness experience by gender, which may influence risk of divorce for wives and husbands. For example, women often report more symptoms, pain, and depressive symptoms following the onset of chronic illness (Stanton, Revenson, and Tennen 2007). Differences in illness experiences among men and women may reflect variation in biological and social processes in relation to the specific illness.
We now discuss some additional caveats to our work. First, in sensitivity analysis, we found that the relationship between wife’s illness and subsequent divorce was not statistically significant when we accounted for unobserved time-invariant characteristics using a first differences model. While this raises cautions as to the causal effect of illness on divorce, it highlights a critical issue regarding the complex dynamics between health, marital stability, and other unobserved factors, such as commitment to the idea of marriage. More broadly, this finding highlights the importance of considering selection and unobserved heterogeneity in assessing the relationship between marriage and health. In addition, time-varying characteristics likely impact the interpretation of our findings. For example, while we restricted the sample to marriages in which both spouses were free of the illnesses of interest at baseline, it is possible that marital quality dynamics over time influenced the development and management of illnesses prior in important ways we could not fully account for in the observational window and with available measures. We attempted to address this limitation in supplementary analysis by controlling for husband’s and wife’s self-rated health, but unobserved heterogeneity cannot be eliminated, nor can we account for marital quality dynamics either before or after Wave 1. An additional limitation pertains to the reliance of respondent reports of physician diagnosis to establish chronic illness onset. Namely, the issue is that diagnosis is not synonymous with actual onset and is conditional on medical care access, health literacy, and recall. As such, our measures may underestimate illness onset, biasing our estimates of the relationship between illness and divorce downward. However, we believe that while this is a limitation of our health measures, it does not pose a serious threat to our results. First, the conditions examined—cancer, heart problems including heart attack, lung disease including “chronic lung disease such as chronic bronchitis or emphysema,” and stroke—are quite serious conditions that frequently require individuals to seek medical care and are likely quite memorable personal experiences. Second, surveys are conducted every two years, reducing respondent recall burden. Finally, we account for (baseline) health insurance, which is a good proxy for health care access. In fact, health insurance access among husbands is independently associated with a lower risk of divorce. Taken together with recent work (Sohn 2015) on the protective role of obtaining health insurance via a spouse (especially a husband) against divorce, this finding highlights how an additional aspect of health care—health insurance—impacts gendered risk factors for divorce.
Another limitation of this research is the reliance of self-reported marital status. Prior research has noted that marital status is misreported; however, it is most often misreported by divorced individuals with deceased former spouses (Weaver 2000). This suggests that the divorce among our sample may be underestimated while widowhood may be overestimated. In addition, our data do not permit us to observe which spouse initiates divorce. Prior work, mostly examining younger Americans, finds that about two-thirds of divorces are initiated by women (Brinig and Allen 2000). The gendered nature of marriage markets at older ages that privilege men suggests that men would be more likely to initiate divorce following wife’s illness because men have more options for new partnerships than women. On the other hand, sick wives who are not receiving adequate care from their husbands might rather divorce than remain married to a poor caregiver. In addition, we cannot differentiate between cohort, period, and age effects. The recent finding that divorce in middle and older ages has been increasing likely reflects a combination of factors, including the aging of cohorts with more favorable attitudes toward divorce, the experience of divorce earlier in the life course as a fairly normative event, and improvements in medical care that benefit all older adults. Further, we do not examine age variation within the “middle and older ages” group. For many conditions, illness onset becomes increasingly normative as individuals age. The normative timing of illness onset in the later life course may make illness less stressful for individuals as well as decrease the availability of (at least similarly aged) relatively healthy potential mates.
Finally, substantial (35%) attrition occurred over the course of the study; however, previous research has noted that prior health and illness status does not significantly impact attrition rates in the HRS (Banks et al. 2011). Moreover, Michaud et al. (2006) find that respondents who temporarily attrit (i.e., return to the survey at a later date) in the HRS are noticeably different from non-attritors and respondents who completely attrit, which suggests excluding temporary attritors may make our sample less biased. Additionally, Michaud and van Soest (2008) observed an attrition rate of approximately 10% per wave (or 5% annually) among married couples in the original HRS cohort. Given our risk group criteria (i.e., healthy couples), our attrition rate corresponds with previous estimates. While prior health status does not appear to influence attrition rates, socioeconomic status has been shown to influence response rates and retention in the HRS (Banks et al. 2011). Therefore, any selection effect from attrition would most likely bias downward both estimates of the relationship between illness onset and both divorce and widowhood to the extent that lower SES couples are more vulnerable to divorce and death in the face of health problems. Given that the amount of attrition (35%) is greater than the combined number of events for the competing outcomes of divorce (6%) and widowhood (24%), it is not possible to dismiss entirely the possibility that study findings have been biased by attrition.
This work suggests several avenues for future research. First, future work should examine the roles of caregiving, income loss, and labor force detachment as mechanisms linking illness with subsequent divorce. Additional studies should also examine other dimensions of health and well-being as risk factors for divorce. Recent work, for example, found that sexual activity and psychological well-being were important mediators of the relationship between physical health decline and declines in marital quality (Galinsky and Waite 2014). Future work should also differentiate between illness diagnosis and disability, as the consequences of illness onset may operate both through the social stigma of diagnosis as well as through the disabling process associated with many illnesses.
Our findings suggest that older women’s health experiences impact their risk of divorce. Other research has shown that following chronic illness onset, women often report more physical and psychological distress, which may directly or indirectly influence divorce risk. Nevertheless, married women diagnosed with a serious health condition may find themselves at increased risk of divorce and may have to manage disease sequelae while experiencing the stressors associated with divorce. These women may be particularly vulnerable to further health declines considering the negative health consequences associated with marital dissolution. While it may not be as great of a concern for older women (especially over the age of 65 years eligible for Medicare), previous research has noted that following divorce, women often experience health insurance loss (Lavelle and Smock 2012). Post-divorce women who do not qualify for public coverage or must switch coverage—to either public or private health insurance—may lose access to health care when it is needed most. Given the increasing concern of the aging population and health care costs, policymakers should be aware of relationship between disease and risk of divorce.
Footnotes
Acknowledgements
Thank you to Samuel Isaacson, Dustin Brown, Sarah Burgard, James House, I-Fen Lin, and Susan Brown for helpful advice and productive conversations. We are also grateful to N.E. Barr for editorial assistance.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a National Institute on Aging training grant to the Population Studies Center at the University of Michigan (T32 AG000221).