
Abstract
Prior research evaluates the health effects of higher status attainment by analyzing highly similar individuals whose circumstances differ after some experience a “status boost.” Advancing that research, we assess health differences across organizational contexts among two national samples of lawyers who were admitted to the bar in the same year in their respective countries. We find that higher-status lawyers in large firms report more depression than lower-status lawyers, poorer health in the American survey, and no health advantage in Canada. Adjusting for income exacerbates these patterns—were it not for their higher incomes, large-firm lawyers would have a greater health disadvantage. Last, we identify two stressors in the legal profession, overwork and work–life conflict, that are more prevalent in the private sector and increase with firm size. Adjusting for these stressors explains well-being differences across organizational contexts. This study documents the role of countervailing mechanisms in health inequality research.
Does higher status attainment always benefit health? Decades of research have established that individuals positioned higher in a system of stratification report better health relative to those lower in the social hierarchy (Marmot 2004). Yet, a debate lingers on why there is a consistent effect of attained status markers on well-being beyond thresholds of material hardship—what Adler and colleagues (1994) label the “challenge of the gradient.” This challenge obscures two points that have received less attention but are nevertheless relevant for theories of social causation and the social patterning of health: (1) attaining higher status does not enhance well-being uniformly across all contexts, and (2) the health effects of status attainment may hinge on the particular role arrangements and circumstances associated with the attained status (Link, Carpiano, and Weden 2013).
These caveats have sparked calls for the investigation of contexts in which circumstances surrounding status gain offset the health benefits of higher social standing (Lutfey and Freese 2005). The stress of higher status (SHS) perspective formalizes these ideas and articulates their implications for social patterns in stress exposure and health (Schieman and Reid 2009). Our study tests the SHS hypothesis by documenting the ways that status attainment is related to rewards and what Link and his colleagues (2013) call “health-harmful circumstances.” Focusing on a relatively homogenous group of professionals working in the same occupation but different organizational contexts, we ask: Does higher status attainment filter individuals into more-stressful role conditions? And, do stress exposures in these higher-status roles neutralize or even reverse the health-enhancing effects of higher status attainment? In addressing these questions, our study seeks to refine theories about the processes that produce health inequalities.
Background
The Status Boost
One of the main challenges in the literature on the health effects of status attainment involves the precise disentangling of the status gain. Marmot (2004) identified the following concerns related to isolating the effects of status markers on health: One cannot do experiments; this is real life. You cannot simply assign people to different groups. Random assignment to high education or high income, interesting as it might be, is not an option. What we would like to have for example, is a group of people where everyone has a high income, and where education matters little for success. If there were then health differences in status, we could observe whether it matters for health. (P. 21)
In the pursuit of the “real-life” situations that naturally construct the scenarios described by Marmot, researchers have investigated the health effects of winning versus losing in status competitions—for example, an Academy Award or a Nobel Prize (Rablen and Oswald 2008; Redelmeier and Singh 2001). In a compelling formulation of this approach, Link and colleagues (2013) assess the longevity outcomes of Emmy Award winners, baseball players inducted into the Baseball Hall of Fame, and winners of the U.S. presidential election. The authors argue these scenarios are desirable for isolating the effects of higher status attainment insofar as winners and losers are highly alike in their pre-competition attributes. Link and colleagues (2013:197) observe, “Among these otherwise relatively similar individuals, a large gap in relative status is created between winners and nominated losers due to the prestige of winning.” For individuals who won their respective competitions—a “status boost”—some reaped benefits in terms of longevity (Emmy winners), while others experienced no benefits (Hall of Fame inductees). By comparison, presidents encountered a greater mortality risk than their losing competitors.
The question turns to why becoming the president of the United States—a quintessential status boost—has detrimental effects. Drawing from the SHS perspective, Link et al. (2013:209) emphasize that “presidents are exposed to a very stressful job” and that “the important aspect is the circumstances status brings.” When presidential candidates win, they simultaneously lose: their status gain in the role transition to president is coupled with an avalanche of acute and chronic health-harming stressors.
More Generalizable Conditions
Analyses of high-stakes status competitions described above provide provocative findings, but the underlying dynamics might not be broadly applicable. We draw inspiration from Pearlin’s (1989) emphasis on “everyday” stressors to argue for greater analytic precision toward more common role strains. According to Pearlin (1983), The study of how people are affected by their jobs, for example, can also inform us of the consequences of different organizational arrangements, of the function of occupation as a source of social status, or of the values and goals engendered by occupational experience. Roles are thus excellent vantage points from which, if we turn in one direction, we observe the aspects of broader social organization and, if we turn in the other, we observe the behaviour of individuals. (P. 5)
Our study design embraces these ideas while also isolating the effects of the status boost in ways that echo the approach of Link et al. (2013). To do so, we analyze data from two samples of the legal profession: (1) Wave 2 of the After the JD (AJD) study (AJD2), a nationally representative cohort of lawyers who entered the American legal profession in 2000, and (2) the Law and Beyond (LAB) study, a data set comprising a sample drawn from the entire population of individuals admitted to the bar in 2010 in every jurisdiction across Canada. There are three reasons why analyses of these data afford a unique evaluation of Link and colleagues’ (2013) ideas and the SHS hypothesis. First, both data sets include identical or highly similar measures on all study variables. We are therefore able to replicate all analyses to strengthen confidence in our results by distinguishing sample-specific findings from those that are robust across contexts. Second, we address comparability issues by studying individuals who are highly similar in education, degree, occupation, and career stage; we also hold constant factors associated with ability and selection: law school grades, law school rank, and education-related debt. These design features help assuage concerns about sources of unobserved heterogeneity that influence selection processes, status achievements, and health. Third, while study participants share similar statuses prior to graduation, at the time of data collection, they subsequently sorted into positions that differ on core dimensions of the legal profession’s system of stratification: prestige and income. Further, status markers are themselves functions of the organizational contexts in which lawyers are embedded. Thus, unlike studies described above that rely on inference to explain results, we leverage data about the uneven distribution of rewards and stressors across contexts to isolate the effects of status attainment. This is crucial—as Link and colleagues (2013:197) argue, “if a status boost brings salutary conditions, health should be enhanced; if it brings stressful or otherwise harmful circumstances, health should suffer; and if it brings nothing of health relevance at all, no health effects should be observed.” We now examine a key factor that structures the health-relevant conditions most prominent among lawyers: organizational context.
Relative and Material Status in the Legal Profession
Sociologists have long noted that the legal profession is characterized by deep structural divides, with the large law firm sitting at the pinnacle of the prestige ladder (Smigel 1964). Large firms hire associates exclusively from the most elite schools, and their clients are primarily large corporations (Dinovitzer and Garth 2007). Large-firm lawyers are also considered more prestigious because their corporate (higher-status) clients present work that is “purely” legal and that does not require the filtering out of irrelevant material and nonprofessional tasks (Sandefur 2001). Thus, studies of members of the bar demonstrate that large-firm lawyers tend to work in areas of law that are accorded the highest levels of prestige (Heinz et al. 2005).
While the private practice of law is grounded on selling lawyers’ services to clients and time billed—regardless of size—the clients served by smaller-firm lawyers are primarily individuals. As a result, these lawyers tend to engage in professionally “unpure” work, such as trials (Sandefur 2001). The ranks of smaller firms are filled with lawyers with less prestigious educational pedigrees who come from less elite social backgrounds and who rarely cross over to the more prestigious corporate side of the bar (Dinovitzer and Garth 2007).
Private-sector lawyers are often contrasted with those in the public sector who are government employees working within organizational settings characterized by bureaucratic decision making. Dixon and Seron (1995) observe that professional power is lower in the public sector, though lawyers in this sector experience the advantages of more predictable hours. While there is some variance depending on whether one works for federal or state/provincial/local governments, public-sector lawyers are often considered less prestigious and have lower incomes relative to those in small private firms (Heinz et al. 2005).
That large-firm lawyers work in the most prestigious settings is also buttressed by stratification research that focuses on organizational size in the private sector, which strongly shapes income and job-related resources. As Kalleberg and Van Buren (1996:62) assert, “the maxim ‘bigger is better’ is true in the sense that employees of large organizations obtain higher earnings and more fringe benefits and promotion opportunities than do employees in small organizations.”
Collectively, the arguments and evidence presented above underscore the structural divides in the legal profession and their links to status. Here, we wish to emphasize a major point: while we are not able to explicitly measure prestige in our study, we will provide evidence of an income gradient in the legal profession—with large-firm lawyers earning substantially more income, followed by lawyers in smaller firms, and with public-sector lawyers earning the least. While these income gaps between settings are wider in the United States, descriptive research demonstrates the same basic distribution of income in the Canadian context (Dinovitzer 2015). The question then becomes, Do these dimensions of stratification and status in the legal profession shape the distribution of health-relevant conditions—and, ultimately, health outcomes?
The Status–Health Paradox
While the legal profession’s organizational contexts distribute earnings and prestige unequally, what they imply for the patterning of health remains underexplored. Given that lawyers working in large private firms experience the highest prestige and financial remuneration in the profession, it seems reasonable to expect more favorable health returns within this context. But some research documents lower levels of well-being in these settings (Dinovitzer et al. 2004)—potentially indicative of a status–health paradox within the legal profession. By status–health paradox, we refer to a status-based distribution of health outcomes within a given subgroup that does not conform to probabilistic statements about between-group comparisons in the population. The identification of a status–health paradox does not undermine the premises and established evidence that undergirds social stress theory—as Schwartz and Meyer (2010:1112) explain, hypotheses derived from stress paradigm state that “on average, disadvantaged group members will fare worse than advantaged group members in health outcomes. It is important to recognize that some subgroups of the disadvantaged group may fare as well or even better than some subgroups of the advantaged group, and vice versa.” Following that logic, some of this heterogeneity is likely to be nonrandom and thus systematically explicable. Link and colleagues’ (2013) finding that presidential winners are confronted with a greater mortality risk highlights this methodological issue and also typifies a status–health paradox.
If a status–health paradox is discovered, the next step is to identify the mechanisms that produce it. Prominent themes in the lawyer-specific literature that emphasize extreme work hours (overwork) and work–life conflict (WLC) suggest that the SHS hypothesis may help explain any apparent status–health paradox among these professionals. Galanter and Palay (1994) invoke the “tournament of lawyers” metaphor to underscore the ways that firm size reflects a structural source of stress. Larger firms are organized around a promotion-to-partnership system: firms hold a tournament in which the associates of a particular “entering class” compete, with the prize of partnership awarded to some fixed percentage of “top” contestants. This competitive compensation structure incentivizes large-firm lawyers to exhibit maximum effort and exceptional productivity. Because quality and quantity of productivity are difficult for partners to measure, long hours represent a common proxy. Employees might overwork in an effort to win the status competition and secure the economic rewards that presumably follow (Cha and Weeden 2014).
Two concepts central to Blair-Loy’s (2003) research are also germane for our predictions: lawyers are expected to embrace the work devotion schema and embody ideal-worker norms that compel total commitment and unrelenting availability (Wallace 1999). In a qualitative study of lawyers, Epstein and colleagues (1999) observed that logging extreme hours (especially billable hours) has gained a mythical status—characterized as “heroic” by some partners. But there are consequences for such heroism: overwork limits the time, energy, and attention available for other important roles. These stressors are unevenly distributed across practice settings—they are disproportionately experienced by lawyers in the private sector and tend to increase with firm size (Dinovitzer et al. 2004).
The distribution of overwork and WLC in the legal profession corresponds with research guided by the SHS perspective that documents a positive association between these chronic stressors and indicators of status (Schieman and Reid 2009). Chronic stressors, such as overwork and WLC, may suppress the health benefits of higher social standing (Schieman and Reid 2009), but they do not reverse the direction of the socioeconomic status (SES)–health relationship in the population because lower-status individuals still face a greater cumulative and operant burden (Turner, Wheaton, and Lloyd 1995). However, in the high-pressure context of the legal profession, these stressors might overwhelm the resources they are paired with, generating a status–health paradox. As patterns of time-related work demands across practice settings are similar in the United States and Canada (Dinovitzer 2015), adjusting for the uneven distribution of these stress exposures should explain any status–health paradox in both national contexts.
Summary of Hypotheses
Based on the ideas and evidence outlined above, we propose the following:
Data and Methods
Sample
The AJD study (Dinovitzer et al. 2004) is a longitudinal survey of a nationally representative cohort of lawyers admitted to the bar in 2000. The first wave was launched in 2002. A total of 4,538 sample members responded, which is 71% of those located and who met criteria for inclusion. The second wave (AJD2) was launched in 2007, and the sample comprised Wave 1 respondents and nonrespondents. We focused on Wave 2 in the present study because Wave 1 did not include several of our focal measures. The survey yielded 3,705 respondents meeting eligibility criteria. This included 70.4% of first-wave respondents and 26.9% of those who did not respond in Wave 1. The overall response rate for the second wave was 50.6% of eligible members.
The AJD study was based on a two-stage sampling design. The United States was first divided into 18 strata determined by region and size of the new lawyer population. Within each stratum, one primary sampling unit (PSU) was selected. These PSUs comprised (1) the four “major” markets, with more than 2,000 new lawyers each (Chicago, Los Angeles, New York, and Washington, D.C.); (2) five “large” markets, each with between 750 and 2,000 new lawyers (Boston, Atlanta, Houston, Minneapolis, and San Francisco); and (3) nine smaller markets (Connecticut, New Jersey remainder, Florida remainder, Tennessee, Oklahoma, Indiana, St. Louis, Utah, and Oregon).
The second stage sampled lawyers randomly in each of the PSUs proportionately to the national population of U.S. lawyers. The sampled lawyers are representative of lawyers entering the U.S. legal profession who graduated from law school between June 1998 and July 2000 and gained admission to the bar in 2000. For unbiased estimates for underrepresented groups, the survey design included an oversample of 1,465 new lawyers from minority groups (black, Hispanic, and Asian American). Sample weights are applied to all analyses in combination with the “svy” command in Stata 14.1 to adjust for clustering due to the complex study design.
Next, we draw on the 2010 LAB study, which surveyed the population of individuals admitted to the bar in 2010 in every jurisdiction in Canada. Because LAB focused on early-lawyer careers, the design included individuals who graduated from law school after 2007 and were admitted to the bar in 2010. The LAB study was launched in September 2012 with 1,099 complete and eligible responses. After adjusting for eligibility, the final response rate was 46%, while the cooperation rate was 79%. Analyses were weighted to better approximate the distribution of the eligible population of 2010 admittees.
Analyses were restricted to individuals who indicated that they were a practicing lawyer in their primary job and employed at the time of the survey; we excluded individuals who indicated that they were employed by a business that was not a law firm because those cases lack information about firm size in the LAB study. We used multiple imputation by chained equations (MICE) to handle missing values on all predictor variables (White, Royston, and Wood 2011). We included our dependent variables in the imputation models but then employed the multiple-imputation-then-deletion strategy recommended by von Hippel (2007) to exclude cases missing on the dependent variable from all analyses. 1 This procedure yielded 2,576 and 877 cases for self-rated health in the U.S. and Canada, respectively, in our final analytic samples, and 2,488 and 863 cases for depression. We generated m = 50 complete data sets using MICE. To estimate models, each m completed data set was analyzed separately, and then results were combined to minimize uncertainty associated with missing information (Little and Rubin 2002).
Focal Measures
Unless otherwise noted, we use identical measures from the AJD2 and LAB data sets.
Depressive symptoms
Depressive symptoms were measured with a seven-item version of the Center for Epidemiological Studies Depression Scale (Mirowsky and Ross 2003). Respondents were asked, How many days during the past week (0–7) have you: (1) felt you just couldn’t get going; (2) felt sad; (3) had trouble getting to sleep or staying asleep; (4) felt that everything was an effort; (5) felt lonely; (6) felt you couldn’t shake the blues; and (7) had trouble keeping your mind on what you were doing?
We averaged the responses; higher scores indicated more depression (AJD2, α = .85; LAB, α = .89).
Self-rated health
This item asked, Compared to most people your age, how would you rate your health? Would you say your overall health is (1) much better than most people your own age, (2) somewhat better, (3) about the same as most people your own age, (4) somewhat worse, (5) much worse than most people your own age.
We coded responses as follows: “much better” and “somewhat better” were coded 1; “about the same as most people your own age” was coded 2; and “somewhat worse” and “much worse than most people your own age” were coded 3.
Practice setting
Respondents indicated the type of organization they worked for. Those in law firms could select “solo practice” or “private law firm.” They were also asked to indicate how many lawyers work in their firm; these were coded as 2 to 20, 21 to 100, 101 to 250, and 251 plus. The public sector included federal government, state/provincial or local government, legal services, duty counsel, public interest organization, other nonprofit organization, and educational institution. We compared public sector with workers in three categories: (1) solo/small firm (2–20), (2) medium firm (21–100), and (3) large firm (100 plus).
Income
In the AJD2, respondents were asked, “Approximately what was your total compensation (pre-taxes) from your primary employer for the calendar year 2006 in each of the following categories?” One item also measured personal income in the LAB data: “What was your total compensation (pre-taxes) from your primary employer for the calendar year 2011?” In both surveys, prompts were used for earnings from salary, bonuses, profit sharing/equity distribution, and the present value of stock options. Answers were combined to measure respondents’ total income. We coded income into quintiles to make group comparisons and evaluate nonlinearities.
Overwork
One item asked, “In the last week, how many hours did you spend in each of the following activities (if you were on vacation or sick leave last week use last week that you worked).” Prompts asked for hours related to working in the office or firm, working from home on weekdays, working on the weekend, going to networking functions, and participating in recreational activities for networking purposes with other lawyers or clients. Answers were combined to produce total hours. We coded those who worked 60 hours or more per week as 1 and all others as 0.
Work–life conflict
Two items measured WLC. Respondents were asked, “How often does your job interfere with each of the following?” Two statements followed: (1) “your home or family life” and (2) your social or leisure activities.” In the AJD2, responses were recorded on a four-point Likert scale ranging from 1 = “never” to 4 = “frequently.” In the LAB data, responses were recorded on a seven-point Likert scale ranging from 1 = “never” to 7 = “very frequently.” We averaged the items; higher scores reflected more WLC (AJD2, α = .89; LAB, α = .92]. We standardized the indexes for comparability of descriptive statistics and coefficients across contexts.
Control variables
All regression models adjusted for gender, age, race, marital status, and whether the respondent had a child at home. In addition, we also adjusted for variables that may influence practice setting and health. First, law school rank is an important predictor of future practice setting, with those from the most prestigious law schools disproportionately entering large law firms after graduation. If the law school experience at elite institutions entails high competition and pressure, this stress exposure may influence lawyers’ health prior to workforce entry. Second, we adjusted for cumulative law school grade. Higher grades influence the attainment of higher status, as prestigious law firms actively seek out high-performing graduates. On the other hand, the pressure to attain higher grades may represent a stressor that impacts health. We adjusted for law school debt because Dinovitzer (2015) observed that participants working for larger private firms rate debt as a salient concern and a factor in their choice of practice setting—and debt is linked with distress (Drentea and Reynolds 2014).
Plan of Analyses
We first provide descriptive patterns that represent the foundational elements of our hypotheses: the distributions of income, overwork, and WLC across practice settings, as well as the distribution of those two stressors across income groups. Then, in multivariate analyses, we used ordinary least squares regression to evaluate depressive symptoms as the dependent variable. For health, we used ordinal logistic regression. In Model 1, we established the patterns across practice settings. This step tested the higher-status-is-better versus the status–health paradox hypothesis. Public-sector workers represent the reference category primarily because income is our focal measured dimension of SES. This status marker is lowest in the public sector and increases with firm size across private-sector settings. This addresses core issues relating to SES and health: if more income leads to better health, then we should see better health in the private sector, particularly among large-firm lawyers.
In Model 2, we adjusted for income to evaluate the resources-of-higher-status and financial-consolation hypotheses. Models 3 and 4 added overwork and WLC, respectively, to test the SHS hypothesis. These progressive adjustments allowed us to examine changes in coefficient sizes across models (Mirowsky 2013). Comparing logit coefficients across models with different covariates can be problematic, because the scale of these coefficients changes with differences in the latent residual variance across models (see Mood 2010), so we present average marginal effects (AMEs) in all analyses of self-rated health and provide two panels that predict (1) good health and (2) poor health. All multivariate models adjusted for the control variables. To preserve space, descriptive statistics for all study variables are presented in the supplemental material (available in the online version of the article). 2
Results
Key Descriptive Patterns
Before presenting multivariate analyses, we provide a descriptive profile of our focal variables. In the top half of Table 1, the first column demonstrates a clear income gradient across practice settings: individuals in the public sector earn less than those in all private settings. In the private sector, the average level of earnings rises sharply with firm size (see Panels A and B of Figure 1).
Descriptive Patterns among Focal Variables in LAB (2012; N = 913) and AJD2 (2007; N = 2,620).
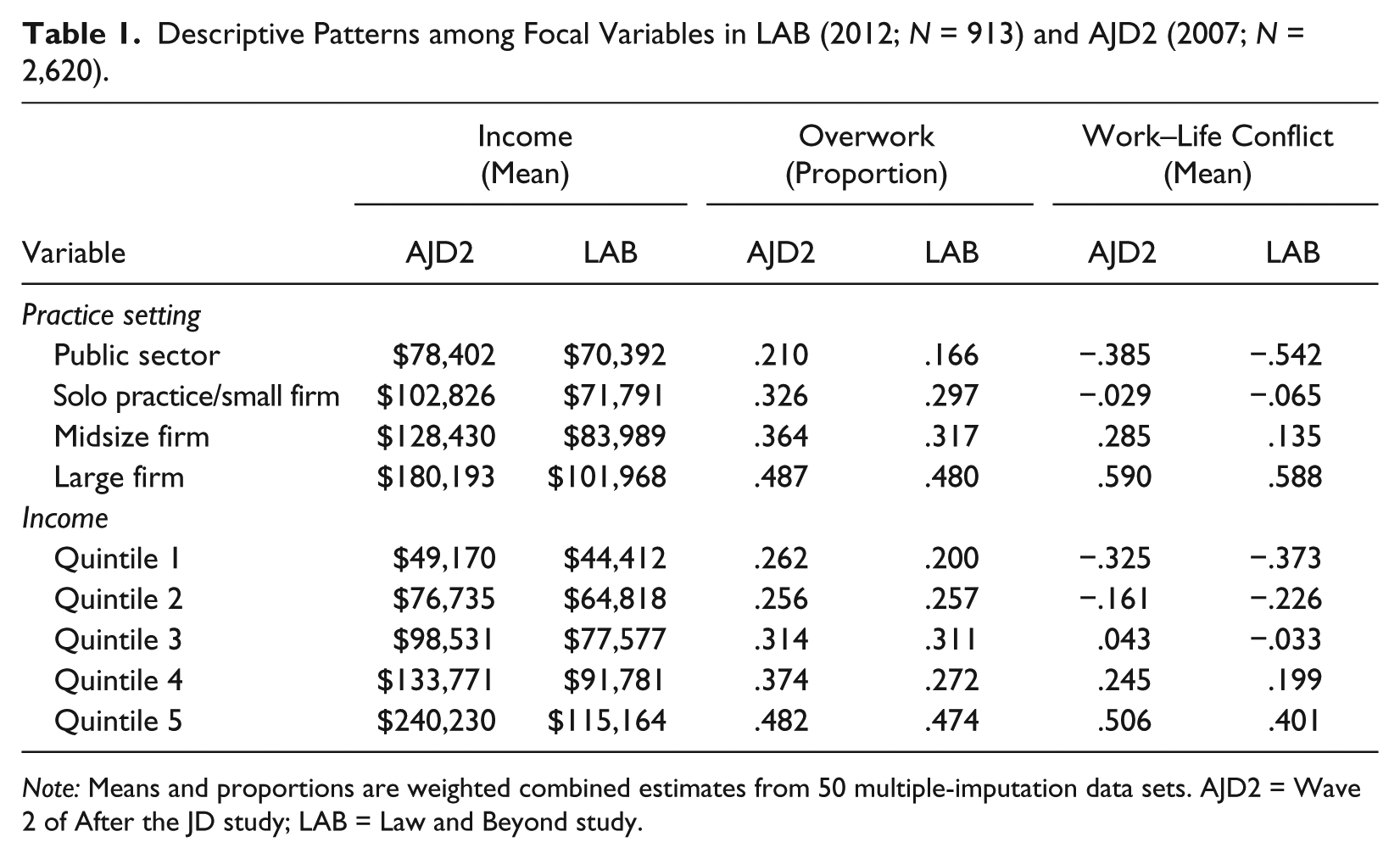
Note: Means and proportions are weighted combined estimates from 50 multiple-imputation data sets. AJD2 = Wave 2 of After the JD study; LAB = Law and Beyond study.
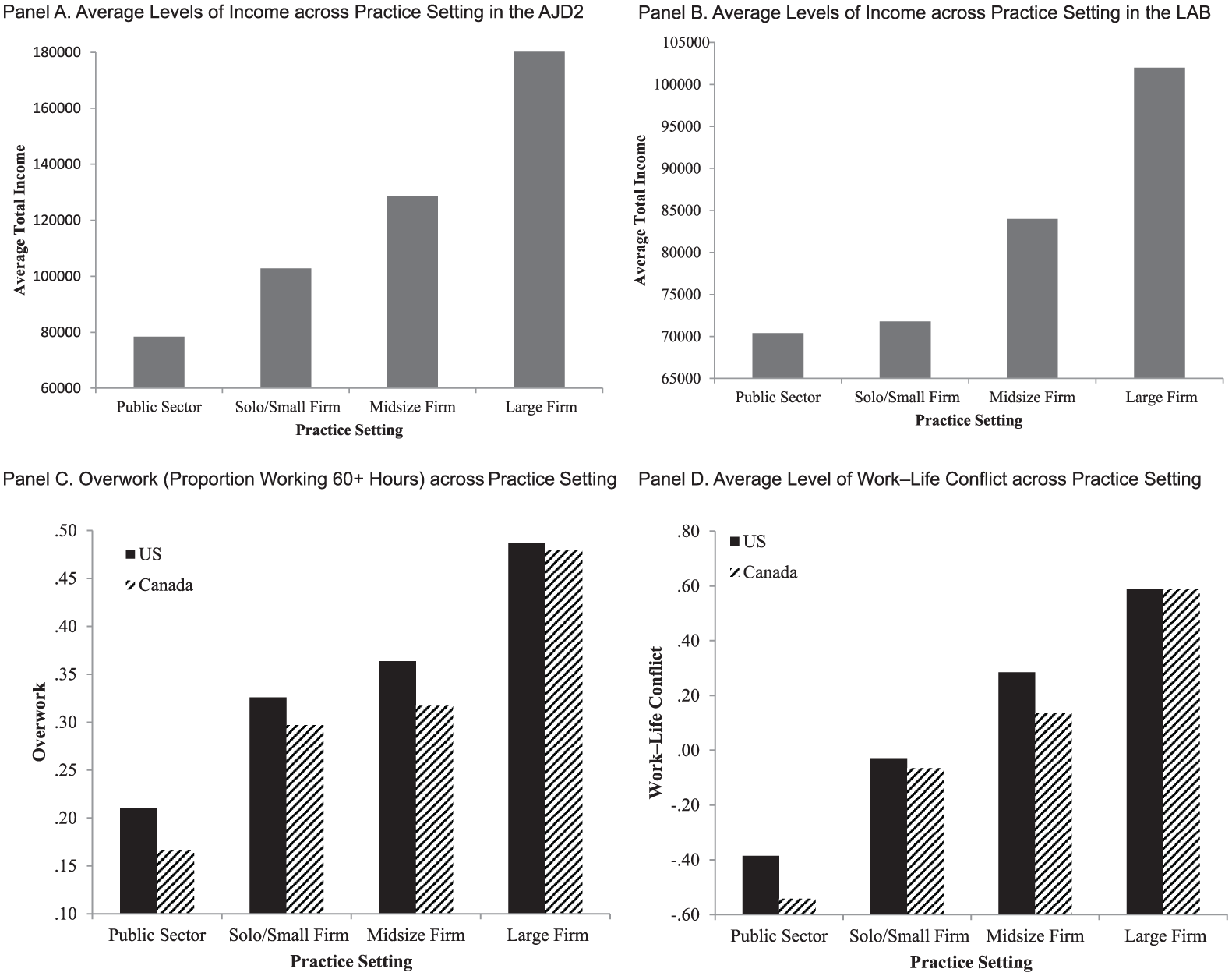
Economic Rewards and Stressors across Practice Setting.
Alongside those greater financial rewards, the patterns of stress exposure across practice settings also reflect a gradient. As columns 2 and 3 in Table 1 indicate, overwork and WLC are lowest in the public sector and rise sharply across private-practice settings (see Panels C and D of Figure 1). Collectively, these patterns present a mixed story about the higher-status-is-better narrative. If “better” is measured by earnings, then individuals working in large private firms are indeed better off. By contrast, if “better” is measured by less overwork and WLC, then individuals working in larger private firms are worse off.
The bottom half of Table 1 reports the distribution of overwork and WLC across income groups—both stressors rise sharply across income quintiles (see Panels A and B of Figure 2). Taken together, these bivariate patterns demonstrate an intimate pairing of higher role stress and higher status (more prestige, better earnings), and these epitomize the countervailing dynamics articulated by the SHS perspective.
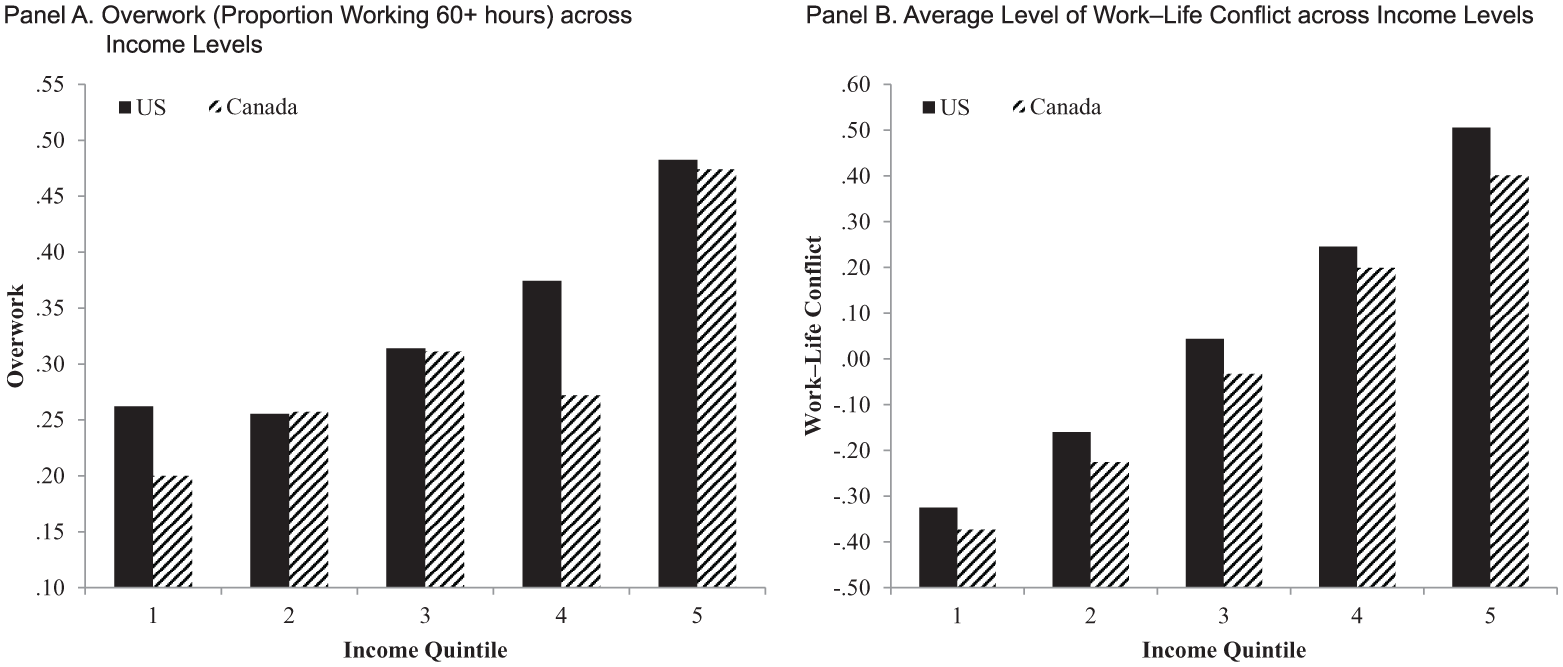
Levels of Stress Exposure across Income Level.
Findings for Depression
Model 1 in Tables 2 and 3 shows that, with the exception of lawyers in midsized firms in the AJD2, individuals in each private-sector setting report significantly higher levels of depressive symptoms compared to those in the public sector. The inclusion of income in Model 2 amplifies these differences, revealing a suppression effect: were it not for the higher incomes in larger firms, the difference in depression between lawyers in large firms and those in the public sector would be even greater. Large-firm lawyers are more likely to have incomes in the highest income quintile—and those individuals, in turn, report the fewest depressive symptoms. The same dynamic reveals a suppression effect for lawyers in midsized firms in the AJD2: after accounting for income in Model 2, the coefficient for these individuals becomes significant.
Depression Regressed on Practice Setting, Income, and Stressors in the AJD2 (2007; N = 2,488).
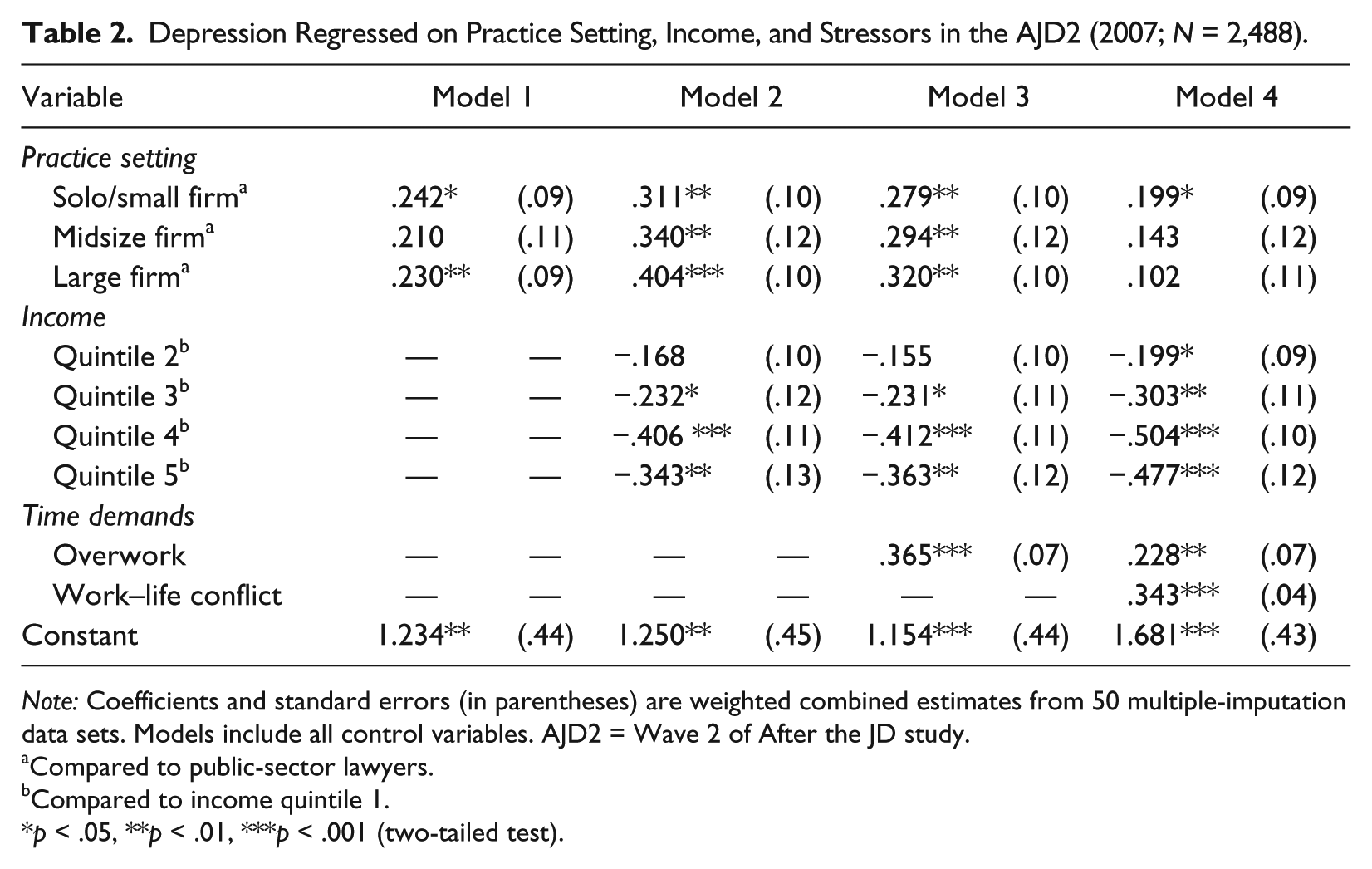
Note: Coefficients and standard errors (in parentheses) are weighted combined estimates from 50 multiple-imputation data sets. Models include all control variables. AJD2 = Wave 2 of After the JD study.
Compared to public-sector lawyers.
Compared to income quintile 1.
p < .05, **p < .01, ***p < .001 (two-tailed test).
Depression Regressed on Practice Setting, Income, and Stressors in the LAB (2012; N = 863).
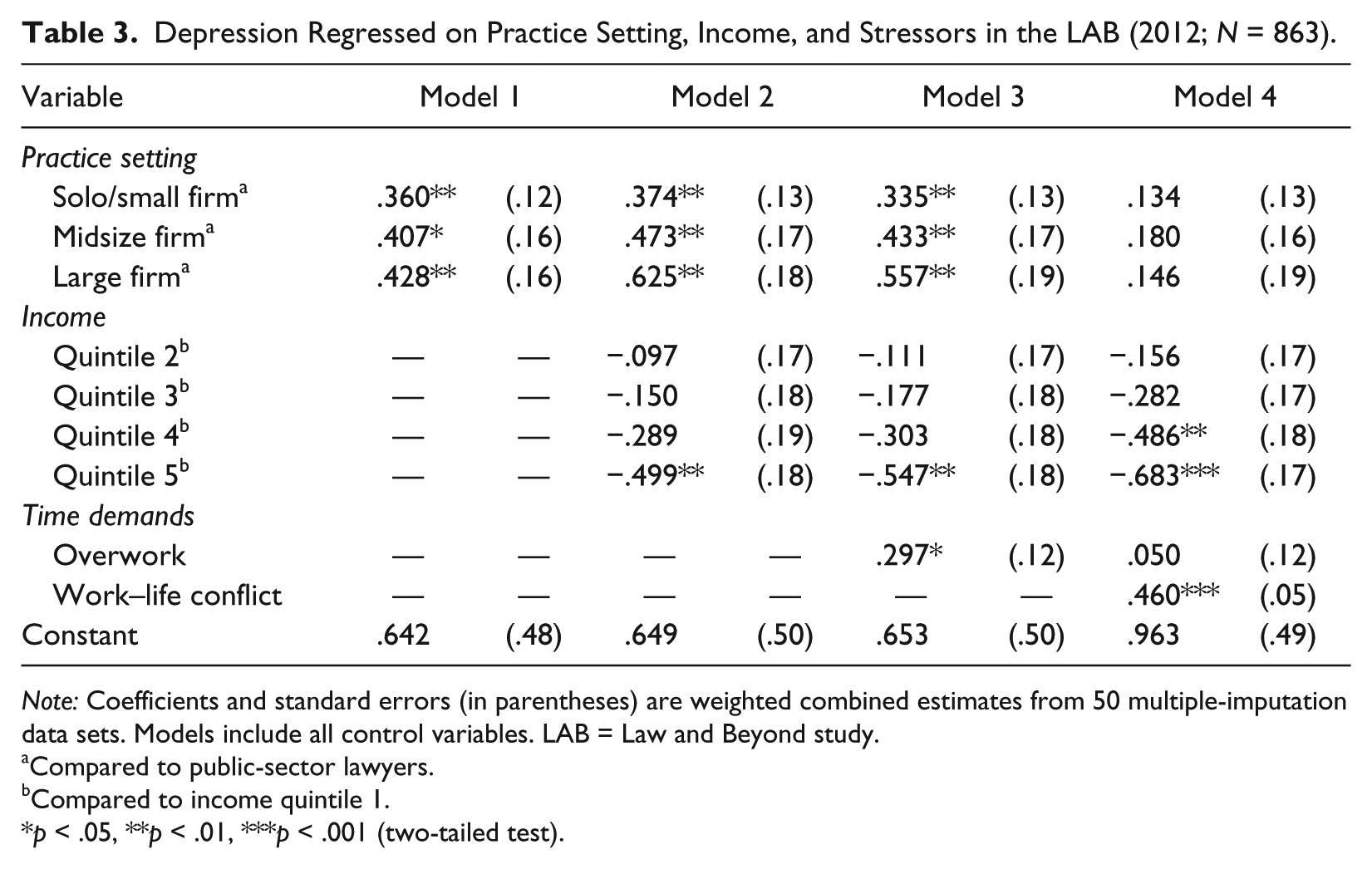
Note: Coefficients and standard errors (in parentheses) are weighted combined estimates from 50 multiple-imputation data sets. Models include all control variables. LAB = Law and Beyond study.
Compared to public-sector lawyers.
Compared to income quintile 1.
p < .05, **p < .01, ***p < .001 (two-tailed test).
The differences in depression between job settings are reduced with the inclusion of overwork (Model 3) in both data sets. In Model 4, differences in depression across settings are reduced to statistical nonsignificance when we adjust for WLC for Canadian lawyers, while solo/small-firm lawyers are the only group that remains significantly different from the public sector in the AJD2. Both of these stressors are associated positively with depressive symptoms. Taken together, adjustments for overwork and WLC reduce differences in depressive symptoms across practice setting to statistical insignificance with the exception of lawyers in small-practice settings in the United States. Thus, if overwork and WLC were distributed evenly across practice settings, there would be almost no differences in depressive symptoms across these contexts. But, as we have demonstrated, overwork and WLC are not evenly distributed; they are more prevalent in the private sector and increase with firm size. Additionally, the significant association between overwork and depression is fully accounted for with the inclusion of WLC in Model 4 in the LAB survey and reduced by roughly 38% in the AJD2 study. This indicates that lawyers who overwork report more depression because they also tend to experience more WLC. Post hoc tests (not shown) revealed no significant differences in depression between private-sector settings across all models in both national contexts.
The findings for income are also compelling. Model 2 shows that those in the top income quintile in Canada, and those in the top three income quintiles in the United States, report significantly fewer depressive symptoms relative to their peers in the lowest income group. The difference between these groups and the lowest earners widens after adjustment for overwork in Model 3. Finally, with the inclusion of WLC in Model 4, the absolute size of the coefficient for the comparison between the fourth income quintile and the bottom income group in Canada increases from –.303 (Model 3) to –.486 (Model 4), and becomes statistically significant (p < .01). Likewise, the size of the coefficient for the comparison between the second income quintile and the bottom income group in the AJD2 increases from –.155 in Model 3 to –.199 and becomes significant (p < .05) in Model 4. These suppression effects indicate that higher overwork and WLC among higher-earning groups conceal what would be greater disparities in depression across the income spectrum.
Findings for Self-rated Health
Panels A (predicting good health) and B (predicting poor health) in Tables 4 and 5 present findings from ordered logistic regression models where the displayed coefficients represent the AMEs. In Panel A, Model 1 shows that the average estimated probability of reporting good health is roughly 7% lower in large firms relative to the public sector in the AJD2 and 11.5% lower in midsized firms relative to the public sector in the LAB study. While these differences are significant (p < .05), all other settings do not differ from the public sector. Additionally, post hoc tests (not shown) revealed that the probability of reporting good health is roughly 6% lower in large firms relative to solo/small firms in the AJD2 (p < .05), while no other differences were observed between private-practice settings in either data set across all models.
Self-rated Health Regressed on Practice Setting, Income, and Stressors in the AJD2 (2007; N = 2,576).
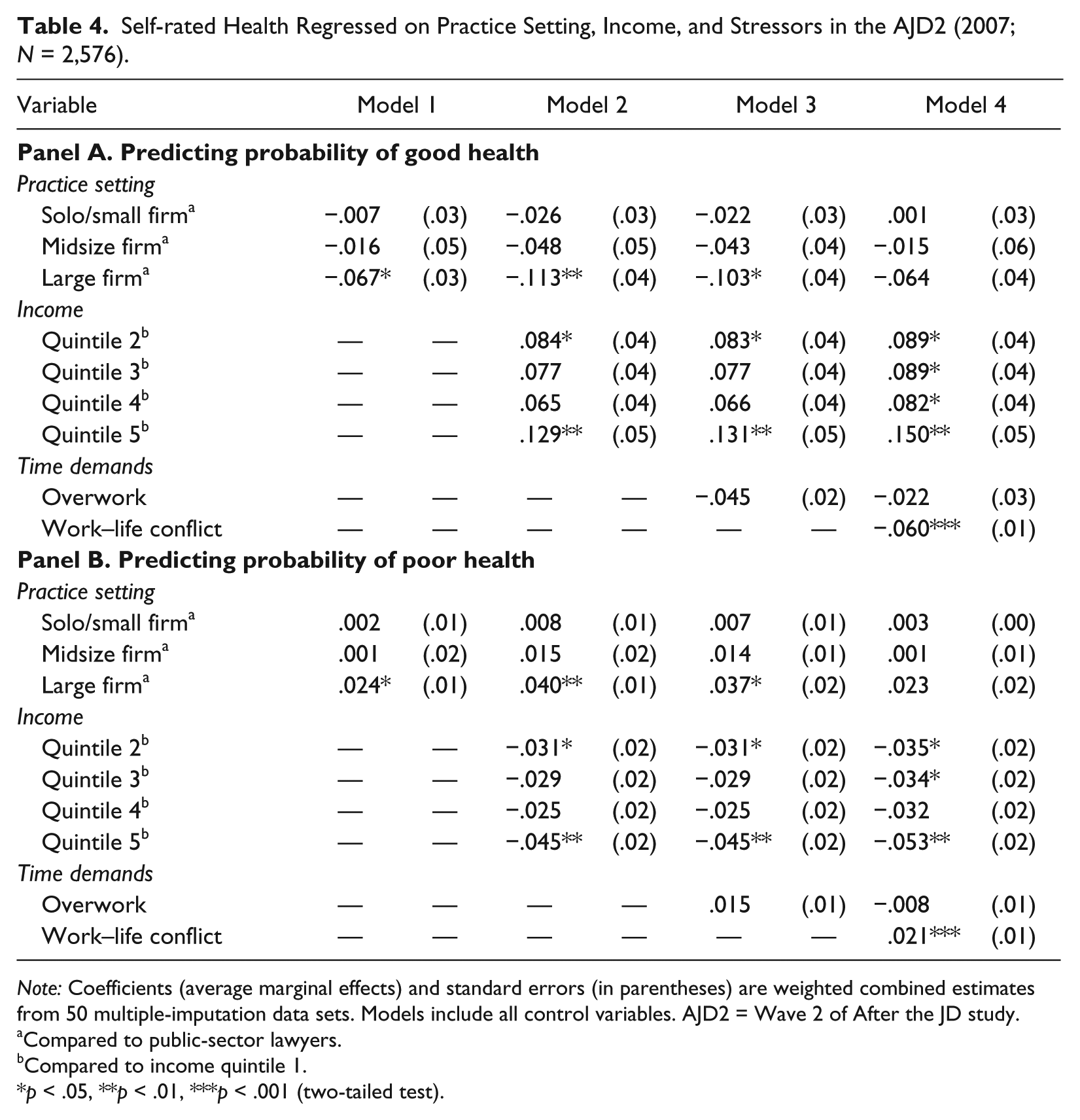
Note: Coefficients (average marginal effects) and standard errors (in parentheses) are weighted combined estimates from 50 multiple-imputation data sets. Models include all control variables. AJD2 = Wave 2 of After the JD study.
Compared to public-sector lawyers.
Compared to income quintile 1.
p < .05, **p < .01, ***p < .001 (two-tailed test).
Self-rated Health Regressed on Practice Setting, Income, and Stressors in the LAB (2012; N = 877).
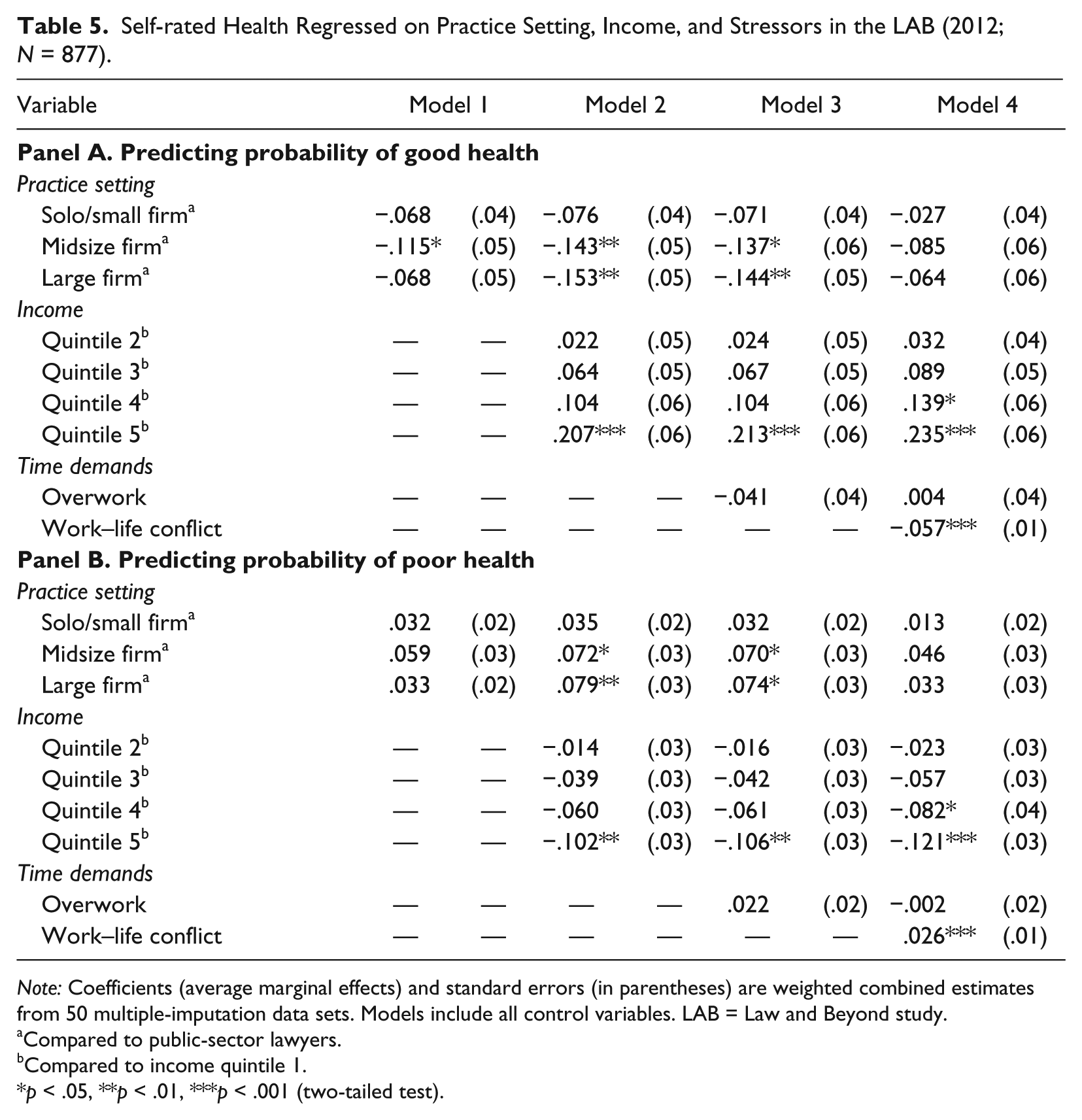
Note: Coefficients (average marginal effects) and standard errors (in parentheses) are weighted combined estimates from 50 multiple-imputation data sets. Models include all control variables. LAB = Law and Beyond study.
Compared to public-sector lawyers.
Compared to income quintile 1.
p < .05, **p < .01, ***p < .001 (two-tailed test).
The magnitude of the AMEs across practice settings are amplified in Model 2. After adjusting for income, the estimated probability of reporting good health for those in American large firms is 11.3% lower compared to public-sector lawyers and 8.7% lower (post hoc test not shown) relative to solo/small-firm lawyers (p < .01). In Model 2 in the LAB data, the predicted probability of reporting good health is roughly 15% lower for individuals in large firms compared to the public sector (p < .01).
Although overwork (Model 3) is not related to good health, Model 4 shows that an increase in WLC significantly decreases the probability of reporting good health in the United States and Canada (p < .001). The inclusion of WLC reduces the differences in the probability of good health across all practice settings to nonsignificance in both data sets. These reductions are due to the fact that WLC decreases the probability of good health and that WLC is more prevalent among lawyers in these settings.
We observe similar patterns for poor health in Panel B. One dissimilarity is that we observe no significant differences among practice settings in Model 1 among Canadian lawyers. However, mirroring the patterns above, the inclusion of income in Model 2 amplifies differences in poor health between settings, while the addition of WLC in Model 4 reduces these differences to nonsignificance in both data sets. Post hoc tests (not shown) revealed that lawyers in large firms have a greater probability of poor health compared to those in the solo/small firms; this difference is magnified with the inclusion of income in Model 2 and is then reduced to nonsignificance after the addition of overwork and WLC in Models 3 and 4. No other differences in good or poor health were observed between private-practice settings.
Turning to income in Panel A of Tables 4 and 5, Model 2 demonstrates that being in the top income quintile increases the probability of reporting good health by about 13% and 21% relative to those in the lowest group in the United States and Canada, respectively. Those in the second quintile in the United States also have a higher probability of good health compared to the lowest earners. The inclusion of WLC in Model 4 reveals a suppression effect: the probabilities of reporting good health for individuals in the third and fourth income quintiles in the AJD2, and in the fourth income quintile in the LAB study, become significantly higher compared to the lowest earners. These suppression patterns are evident because WLC—which is more prevalent among higher earners—decreases the probability of reporting good health (p < .001).
In Panel B of Tables 4 and 5, the income patterns mirror those above. Model 2 demonstrates that being in the top income quintile reduces the probability of reporting poor health by 4.5% and 10.2% relative to those in the public sector in the United States and Canada, respectively. The inclusion of overwork in Model 3 has no effect, but adjustment for WLC in Model 4 reveals a suppression effect—the probabilities of reporting poor health for individuals in the third income quintile in the AJD2, and lawyers in the fourth quintile in the LAB study, become significantly lower compared to the bottom earners. These results suggest that the health benefits of higher income are concealed by higher levels of WLC among the highest-earning lawyers.
Discussion
A relatively straightforward narrative characterizes much prior theorizing and research on social stress: individuals positioned higher in a social hierarchy should experience better health. We demonstrate the ways that this narrative gets complicated when status-based resources are offset by stress exposures across two national contexts. First, we observe a status–health paradox: higher-status lawyers have a mental health disadvantage relative to their peers in the public sector and are no better off in terms of health. Second, the interplay between practice setting and income adds complexity: adjusting for income, health disparities across practice settings become even greater—were it not for higher incomes in larger firms, the health gap between the public sector and larger firms would be even larger. Taken together, these patterns support the status–health paradox and the financial-consolation hypotheses.
While the higher-status-is-better-for-health hypothesis is not supported, we observed that higher earners have fewer depressive symptoms and a lower risk of poor health. As individuals in larger firms tend to have higher earnings, the resources-of-higher-status claim is supported with respect to practice setting and income. Collectively, these cross-cutting patterns produce a suppression effect: lawyers in large firms tend to earn more; earnings are protective for health; holding earnings constant reveals greater health differences.
We also contribute to evaluations of the SHS hypothesis. The hypothesis predicts and our observations confirm three interrelated findings: (1) lawyers in the private sector and in progressively larger firms experience higher levels of overwork and WLC, (2) overwork and WLC are associated positively with depressive symptoms and risk of poor health, and (3) when our models include these stressors (especially WLC), we explain differences in depression and health across organizational contexts.
If health outcomes are unevenly distributed across organizational contexts among otherwise similar individuals, what is it about these settings that generate such patterns? Informed by the sociological study of stress, our focus was drawn to conditions most relevant to role experiences of lawyers. The nature of the work role and concomitant responsibilities reflect the organizational settings in which lawyers are embedded—and this has important implications for stress exposure and health. These discoveries resonate with what Wheaton and Gotlib (1997) call the “power of the ordinary” and the “cumulative effects of structural givens in daily life.” Structural givens in the legal profession—overwork and WLC—vary systematically across practice settings. The power of the ordinary characterizes the potency of chronic stressors in everyday role arrangements. WLC is “ordinary” for lawyers in large private firms—and this is why it is also powerful for the social patterning of depression and health.
While these observations describe individual-level experiences, they also reflect meso- and macrolevel concerns at the intersection of social stratification, medical sociology, and occupational health psychology. As Fenwick and Tausig (1994:268) explain, “stressful jobs are not randomly distributed throughout the economy; rather, they are products of macroeconomic structures and forces such as the economic sector and organizational structure of firms in which the jobs are located.” Our findings reinforce the claim that organizational contexts shape not only material and relative status but also the job conditions to which individuals are exposed—and are thus logically prior to demands, resources, and health (Tausig and Fenwick 2011). These processes make the study of stress a quintessentially sociological endeavor (Pearlin 1989).
Our findings have broader implications for social stress theory and health inequality research. While on the surface our results might seem to challenge established theory and evidence based on the stress process paradigm, we underscore that our findings do not undermine observations about the status–health relationship in the population because, on average, lower-status individuals still disproportionately experience higher rates of physical and mental illness. Lutfey and Freese (2005) articulate this methodological issue and its implications for fundamental cause theory. Describing “countervailing mechanisms” that may put higher-status individuals at greater risk for poor health, Lutfey and Freese (2005:1365) observe that “[f]undamental relationships do not require that all of the pathways between X and Y support the relationship. Countervailing mechanisms may work in the other direction; indeed, the only requirement is that the effects of such mechanisms are cumulatively smaller than the mechanisms producing the fundamental relationship.”
As long as the stressors of higher status do not outweigh the total stress exposure encountered by lower-status individuals, observations concerning the status-based distribution of health outcomes in the population should remain consistent. Yet, social stress researchers should be cognizant of shifts in the nature of work and the structure of the workforce over time and the implications such changes have for patterns of stress exposure and the status–health gradient. In her review of new forms of work, Smith (1997) observed trends toward destabilization and work intensification for professional and managerial workers in recent decades. Destabilization is reflected in rising job insecurity among these groups (Kalleberg 2009), and work intensification is manifest in research demonstrating that higher-SES workers disproportionately encounter chronic stressors, like job pressure, overwork, role blurring, and WLC (Schieman and Koltai 2016). When coupled with an increasing proportion of professionals and managers in the labor force (Esping-Andersen 2002), these temporal trends and current patterns may influence the shape of the SES–health gradient—especially through the middle and upper range of the status spectrum. Future research should thus probe for similar status–health paradoxes in other high-commitment professions.
Our findings also have several practical implications. First, the alleviation of health disparities represents a core and unifying objective in research concerned with the social determinants of health. If this goal is to be applied to the legal profession in North America, then our analyses suggest that policy or organizational interventions should focus on the mitigation of WLC. 3 That is, were it not for the uneven distribution of WLC in the legal profession, there would be no differences in distress or poor health across practice settings. Next, consideration of lawyer well-being would benefit law firms themselves. In its early incarnation, law firms’ promotion to partner tournament system required an “up-or-out” process in which lawyers who were not promoted to partner were let go (Galanter and Palay 1994). Attrition was necessary—if lawyers left the firm because of stress, this created the turnover firms required without any action on their part. Yet the traditional model has changed rapidly in recent years. Law firms continue to promote a small number of associates to partnership, but many are now employed in non-partnership-track positions (Galanter and Henderson 2008). Simultaneously, there is increased demand and competition for these same lawyers from new legal services providers who are offering more flexible workplaces and options to minimize WLC (Williams, Platt, and Lee 2015). Thus, if law firms seek to remain competitive in attracting and retaining associates, they will increasingly need to design work environments that reduce interrole conflict.
One final point of reflection involves comparisons across settings and how these square with our hypotheses. We did not observe statistically significant differences between private-practice settings for depression in either data set. That is, while public-sector lawyers tend to report less depression relative to their higher-status peers, no differences emerged between large, medium, and solo/small firms. Given the gradient in chronic stress exposure across practice settings, we find this result surprising. But we do not believe that this lack of differences undermines our general conclusions—we still observe a status–health paradox in all analyses insofar as higher-status lawyers are either worse off or no better off in terms depression relative to those at the bottom of the status spectrum. Where differences in depression are observed between public-sector lawyers and those in higher-status contexts, these differences can be explained by SHS dynamics. That said, we do observe a distribution of health between practice settings in the United States that better approximates a gradient: large-firm lawyers report a lower probability of good health and a higher probability of poor health relative to those in the public sector and those in solo practices and small firms.
Study Limitations
We acknowledge several potential limitations of our study. First, the cross-sectional nature limits claims about causality. We cannot rule out the possibility that individuals with higher preexisting levels of poor health selected into larger, higher-status firms. Alternatively, individuals with poor health might select less stressful work settings to manage preexisting conditions. Existing evidence, however, has shown that poorer physical and mental health either impair higher status attainment or cause individuals to “drift” downward (not upward) in the social hierarchy (Haas 2006).
Next, while our design and logic echoes that of Link et al. (2013), we recognize that the status boost in our study cannot be assumed to be completely random; it is possible that individuals with certain traits or personality factors—such as ability or neuroticism—select into higher-status firms. Selection bias may therefore complicate a causal interpretation of our findings if these preexisting differences are the underlying cause of both higher status attainment and poor health outcomes. While certainly plausible, the pathways required for such traits to represent true confounders are not necessarily established empirically. For example, neurotic individuals experience more distress (Bienvenu et al. 2004), but a meta-analysis documents that neuroticism is negatively correlated with salary and promotions (Ng et al. 2005). In a similar vein, cognitive ability is positively related to higher status attainment, but ability is generally related to better health outcomes (Singh-Manoux et al. 2005)—although Link et al. (2008) found no significant association between cognitive abilities and health net of SES. Our models also control for two key indicators of ability and practice setting selection: law school grades and law school rank. Nevertheless, we cannot definitively rule out that selection factors in the present study.
We also recognize the potential for alternative mechanisms that may explain our observations. While large organizations provide higher wages, benefits, and prestige, they tend to offer less autonomy (Kalleberg and Van Buren 1996). Control over the labor process, in turn, is inversely related to distress and poor health (Tausig and Fenwick 2011). Social justice work tends to be lower paying (Dinovitzer et al. 2004), and social responsibility and meaningful activity are thought to be core elements of positive human health (Ryff and Singer 1998). Thus, lawyers in less prestigious settings might find their work more rewarding, meaningful, or autonomous—and these factors might contribute to their lower distress and poor health. From a statistical standpoint, however, the existence of an alternative mechanism does not necessarily negate the explanatory role of WLC and overwork. To do so, the putative alternative mechanism would need to (1) be affected by the exposure (practice setting) and (2) confound the association between the intervening variable and the outcome (VanderWeele 2015).
While there are remarkable similarities across national contexts—especially in the distribution of income and stress exposure—subtle differences between Canada and the United States remain unexplained. For example, we observe a health disadvantage for large-firm lawyers relative to the public sector and those in solo/small firms in the United States but not in Canada. We offer two points of speculation. First, these differences could reflect period effects—the U.S. data were collected during the beginning of the Great Recession, and research has documented that this was a tumultuous time for large firms (Wald 2010). The greater health disadvantage for large-firm lawyers in the United States might therefore reflect the added stress of job insecurity. Second, because lawyers in the U.S. sample have been practicing for a longer period, the health differences may be attributable to cohort effects—extreme hours and WLC may lead to greater depression in the short term, but it may take longer for these stressors to initiate diverging health trajectories.
Conclusion
Our inquiry began through our interest in understanding why a material or relative status boost improves the health of some while it harms the health of others. Previous studies focused on winners versus losers in various “status competitions” and produced mixed findings. Link et al. (2013) argued that the effects of a status boost depend on the conditions in the newly acquired role. We advanced prior studies by analyzing data that mimic such rare circumstances. Unlike prior studies, our data contain information about a cohort of individuals whose work lives are generalizable to other high-commitment professional groups as well as information about stressors embedded in their work environments. These design characteristics enabled this study to offer a significant contribution to theories surrounding social causation: we identify a set of patterns that run contrary to our traditional expectations about the relationship between SES and health, and we provide an explanation for this deviation.
Footnotes
Acknowledgements
Previous versions of this manuscript were presented at the 2016 International Conference on Social Stress Research in San Diego, California, and the 2016 American Sociological Association annual meeting in Seattle, Washington. The authors would like to thank Blair Wheaton, Markus Schafer, Geoffrey Wodtke, participants in the Toronto Inequality Workshop, and several anonymous reviewers for their incredibly helpful feedback on earlier versions of this paper.
Notes
Supplemental Material
The descriptive statistics for all study variables are presented in the online version of the article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Social Sciences and Humanities Research Council of Canada (Grant No. 410-2009-2778), the American Bar Foundation, National Science Foundation (Grant Nos. SES0115521 and SES0550605), Access Group, Law School Admission Council, National Association for Law Placement, National Conference of Bar Examiners, and the Open Society Institute. The views and conclusions stated herein are those of the authors and do not necessarily reflect the views of individuals or organizations associated with the After the JD study.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.