
Abstract
Prior research based on studies of heterosexual populations suggests that men’s health benefits more from marriage than women’s, in part because women do more than men to influence the health habits of their spouse. We extend this work by using dyadic survey data from 838 spouses in 419 gay, lesbian, and heterosexual marriages to consider differences in social control tactics across same-sex and different-sex couples—that is, how spouses monitor and regulate each other’s health habits. Results suggest that although gender differences in social control are common, gendered patterns sometimes differ depending on whether one is in a same-sex or different-sex marriage. Results also point to the importance of health habits as strong drivers of relationship dynamics across gay and lesbian as well as heterosexual marriages.
The married are in better health and live longer than the unmarried (particularly in comparison to the previously married), and this pattern is stronger for men than women (Rendall et al. 2011; Waite 1995). One explanation for this marital advantage is that spouses influence each other’s health behaviors (e.g., exercise, healthy eating, moderate drinking) by imposing demands, threats, requests, or rewards to that end, a process referred to as the social control of health behavior (Umberson 1992). Over the past two decades, numerous studies have addressed how men and women in heterosexual marriage attempt to influence their spouse’s health behaviors, and these studies show that women are more likely than men to impose control over their spouse’s health behaviors (e.g., Lewis et al. 2004; Rook et al. 2011; Umberson 1992). This gender difference is fundamental to previous work on marriage and health behavior and explanations for why men benefit more from marriage than women (Rendall et al. 2011; Waite 1995). However, past research is limited because it is based on assumptions of gender difference within heterosexual marriage.
We work from a gender-as-relational perspective to consider whether and how gendered patterns of social control depend not only on one’s own gender but also on whether one is in a same-sex or different-sex marriage. Gender-as-relational approaches emphasize that the ways men and women enact gender depend on whether they are interacting with a man or a woman (Goldberg 2013; Springer, Hankivsky, and Bates 2012; West and Zimmerman 2009). Thus, a comparison of same-sex and different-sex couples is needed to consider whether/how the ways men and women enact social control over a spouse’s health habits unfold differently when one is interacting with a partner of the same versus different sex. For example, women may work harder than men to influence their spouse’s health habits but only in the context of a different-sex marital relationship wherein male partners elicit more social control from women. These relational processes are important because health behaviors contribute to disparities in health, illness, and mortality by gender, sexual orientation, and marital status (Institute of Medicine 2011). Moreover, comparing marital dynamics of same-sex and different-sex spouses can broaden our understanding of gendered health and relationship dynamics and challenge taken-for-granted assumptions about gender, marriage, and health based on different-sex couples.
In this study, we analyze dyadic survey data collected from a purposive sample of both spouses in 124 gay, 171 lesbian, and 124 heterosexual married couples (N = 838 individuals) to examine gender and union status (i.e., same-sex/different-sex marriages) variation in social control dynamics. We consider how much spouses want to change each other’s health behaviors (eating, exercise, and drinking), the types of social control tactics used by spouses to influence each other’s health habits, and how spouses react to each other’s social control efforts. We also consider whether social control efforts are related to a spouse’s health behaviors or are dependent on one’s own health habits relative to those of their spouse. For example, respondents’ own drinking habits likely influence how they feel about their spouse’s drinking habits and thus the need to control or influence their partner’s habits. We also take advantage of data that are uniquely suited to addressing social control of health habits from a gender-as-relational perspective. Past studies on marital dynamics tend to utilize data from only one spouse, failing to consider the perspective of both spouses on a dyadic level, even in heterosexual populations. Yet dyadic data are essential to understanding how spouses influence each other both within and across gay, lesbian, and heterosexual couples (Carr and Springer 2010; Lewis and Butterfield 2005; Umberson et al. 2015). For example, dyadic data allow us to leverage both spouses’ reports of social control and health behavior and consider these reports from the perspective of men married to men, men married to women, women married to men, and women married to women.
Background
Although individuals of higher socioeconomic statuses select into marriage, evidence suggests that marriage benefits health and longevity through biological, social, behavioral, and psychological pathways (Rendall et al. 2011). Social control is one behavioral pathway through which spouses may influence each other’s health (Rendall et al. 2011; Waite 1995). Efforts to influence health behaviors include direct control such as telling, reminding, or threatening a spouse in an effort to influence the spouse’s behavior and indirect attempts at control such as altering the social environment in ways that promote healthier behavior in a spouse (Umberson 1992). For example, direct social control might include telling a spouse to stop drinking. Indirect social control might include watering down alcohol available in the home. The available evidence suggests that more direct control efforts (e.g., directly telling a spouse to change their behavior) as well as more affirming control efforts (e.g., praising a spouse’s behaviors) are more likely than other types of tactics (e.g., indirect tactics or criticizing a spouse’s behaviors) to promote health-enhancing behaviors in heterosexual unions (Lewis and Butterfield 2005, 2007; Tucker 2002; Tucker and Anders 2001).
While most research on social control has been cross-sectional, the available longitudinal evidence suggests long-term benefits for health behavior. For example, research based on a nationally representative sample found that direct social control is associated with reduced smoking over a three-year period for both men and women and increased physical activity for women (Umberson 1992). Longitudinal evidence from a nonrepresentative sample also supports the association of social control with subsequent smoking reductions for men but not women (Westmaas, Wild, and Ferrence 2002). Long-term benefits of social control for health may occur because spouses enact social control in response to their spouse’s ongoing health-risk behaviors in ways that lead to improvement in those behaviors over long periods of time (Lewis and Butterfield 2005). For example, on a daily basis, one may be more likely to try to control the drinking habits of a spouse who is a heavy drinker, yet these control attempts may lead to a reduction in the amount the spouse drinks over a longer period of time. From this perspective, “social control may be both a consequence and a cause of health-related behavior” (Lewis and Butterfield 2005:419). In this study, we focus on ongoing social control efforts in relation to a spouse’s current health behaviors.
Gender, Marriage, and Social Control
Prior studies on social control in heterosexual marriage consistently find that women are more likely to serve as agents of social control and men are more likely to be the targets of social control (Berg and Upchurch 2007; Rook et al. 2011; Umberson 1992). The available evidence also suggests that women are more likely than men in heterosexual marriages to use a range of different strategies to influence their spouse’s health habits, including direct and indirect tactics as well as supportive and coercive tactics (Lewis et al. 2004; Tucker and Anders 2001; Tucker and Mueller 2000). But studies that focus solely on heterosexual respondents may obfuscate understanding of gendered relationship and health behavior dynamics. A gender-as-relational perspective suggests that gender is “dynamic and situational” (Springer et al. 2012:1661) and the enactment of gender varies across social contexts and depends on with whom one is interacting (Goldberg 2013; West and Zimmerman 2009). From this perspective, the ways men and women influence a spouse’s health habits (and the response of their spouse) likely unfold differently depending on whether they are married to a man or a woman.
Gendered relationship dynamics in heterosexual marriages are typically explained in terms of different skills and expectations for men and women in the context of marriage, along with gender inequality in marital roles (Ferree 2010; Ridgeway 2011). Structural systems of gender impose different constraints, opportunities, and obligations on men and women that promote women’s sense of responsibility and attention to the health and well-being of others (especially children and spouses) while encouraging men’s greater independence and inattention to the needs of others as well as their own health (Courtenay 2000; Umberson et al. 2017). A gender relations perspective further emphasizes that social conditions persist through social practices that reflect enactment of “hegemonic masculinity” and “emphasized femininity”—idealized views of how men and women should behave, including the ways they care for their partners and the types of health behaviors they engage in (Peralta 2007). For example, women tend to be more focused on care work activities, and men tend to engage in more health-risk behaviors (Courtenay 2000). Structural systems of gender then help to explain why, within heterosexual marriages, women are more likely than men to monitor and regulate their spouse’s health behaviors in an effort to promote their spouse’s health (Markey, Gomel, and Markey 2008; Rook et al. 2011; Umberson 1992).
Gender differences in the ways that heterosexual spouses monitor and influence each other’s health behaviors raise questions about how this type of spousal influence might look for men and women in same-sex marriages. A gender-as-relational perspective (Springer et al. 2012) suggests that men and women in same-sex as well as different-sex unions would be influenced by social conditions that promote gendered patterns of attention/inattention to a spouse’s health/health habits. If this is the case, then women in same-sex unions would be more likely than men in same-sex unions to monitor and regulate their spouse’s health habits because women would be more likely than men to see health work as central to their marital role (Umberson et al. 2016). Gendered patterns of social control may also unfold differently within same-sex unions partly because same-sex partners are more likely to share their spouse’s views about health and health behavior and less likely to be in a marriage that emphasizes inequality between spouses (Holway, Smith, and Perry-Jenkins 2012); these patterns may further differ for men and women within same-sex unions because women are more attuned to and responsive to their spouse’s health (Umberson et al. 2016, 2017). On the other hand, if men are more likely to elicit social control efforts from their spouses, then men in same-sex unions may enact more social control than women in same-sex unions. Moreover, because heterosexuality is a key component of hegemonic masculinity, men in same-sex marriages may be less constrained by structural systems of gender that shape how men monitor and regulate their spouse’s health behaviors.
Health behavior discordance
Gender and sexuality patterns of social control must be considered in relation to gendered health behaviors. Whereas patterns of health behavior in heterosexual marriages often differ for men and women (e.g., men are more likely than women to drink heavily), health behaviors in same-sex marriages may be characterized by more similarity between spouses. A recent study using dyadic data shows that same-sex spouses are more similar to each other than different-sex spouses in their smoking, drinking, and exercise habits, with greater concordance for lesbian than gay spouses (Holway, Umberson, and Donnelly 2018). Consequently, gender and sexuality patterns of health behavior may intersect to uniquely shape social control efforts in marital relationships.
Same-sex spouses’ more similar perspectives on health behaviors could lead to different ways of responding to each other’s health habits in comparison to heterosexual couples. Recent qualitative research finds that men and women in long-term same-sex (cohabiting) unions often engage in teamwork in an effort to mutually reinforce both partners’ positive health habits; in contrast, in heterosexual couples, one partner typically takes the lead in a one-sided campaign to influence the other partner’s behavior, and it is almost always the woman who takes the lead (Reczek and Umberson 2012). Markey and colleagues (2016) analyzed dyadic data collected from a convenience sample of gay, lesbian, and heterosexual couples to study eating habits and found that respondents were more likely to regulate each other when the partner weighed more and weight discordance between partners was greater. The study by Markey and colleagues (2016), the only study we are aware of that begins to address social control in same-sex compared to heterosexual couples, relied on a sample of young adults (mean age 30) in relatively short-duration relationships (minimum 6 months, average 4.91 years); moreover, respondents varied in commitment (e.g., dating) and did not include legally married same-sex couples. However, legal marriage, particularly of longer duration, is the type of relationship shown to be most beneficial to health (LeBlanc, Frost, and Bowen 2018; Rendall et al. 2011; Waite 1995; Wight, LeBlanc, and Badgett 2013). Moreover, studies suggest that marriage becomes more important to health with advancing age (Williams and Umberson 2004). In the present study, we focus on legally married gay, lesbian, and heterosexual couples who have been together an average of 15 years (average age = 48.6 years) to consider each spouse’s social control efforts (and reactions to social control efforts) with respect to several different health behaviors.
Spousal reactions to social control
Dyadic data allow consideration of each spouse’s perspective on health behaviors relative to the other spouse. Notably, reactions to social control efforts, especially social control efforts that are perceived as critical or demanding, are not always positive. Evidence suggests that spouses may ignore these efforts (Tucker and Anders 2001), do the opposite of what the spouse wants (Franks et al. 2006; Tucker 2002; Tucker and Anders 2001), or find the spouse’s social control efforts upsetting (Helgeson et al. 2004; Rook et al. 2011; Tucker and Mueller 2000). Some evidence suggests that these reactions may vary for men and women in heterosexual couples. For example, Tucker (2002) finds that women are marginally more likely than men to engage in health behavior that is the opposite of what their spouse intended, yet they found no gender difference in ignoring a spouse’s social control efforts. Moreover, August and Sorkin (2010) report that compared to men, women may respond more strongly to their spouse’s social control efforts in both positive (e.g., feelings of appreciation) and negative (e.g., feelings of hostility) ways. A gender-as-relational perspective further suggests that compared to different-sex couples, men and women in same-sex unions would be more likely to share approaches to managing health behaviors (as well as being more strongly matched on health behaviors), and this shared perspective may result in less negative reactions to a spouse’s social control efforts.
The Present Study
We extend prior work on social control by analyzing dyadic data to consider whether men and women feel more (or less) compelled to influence their partner’s behaviors, use different types of social control tactics (direct, indirect), or respond to social control attempts in different ways (e.g., appreciative, irritated)—and how these processes may differ for same-sex and different-sex marriages. We consider whether/how patterns of social control depend on the partner’s health behaviors and discordance between spouses on health behaviors. A gender-as-relational perspective along with prior research lead to the following specific hypotheses:
Hypothesis 1: Women will be more likely than men to want to change their spouse’s health habits (exercise, eating, alcohol consumption).
Hypothesis 2: Compared to men, women will use more indirect and direct social control tactics in an attempt to influence their spouse’s health habits.
Hypothesis 3: Women will be more likely than men to react to their spouse’s social control efforts (in both positive and negative ways; e.g., feeling irritated or appreciative), and women will be less likely to ignore their spouse’s social control efforts.
Hypothesis 4: The gender effects in Hypotheses 1 to 3 will be more apparent for men and women in different-sex marriages than for men compared to women in same-sex marriages.
Hypothesis 5: Partner health behaviors and spousal discordance on specific health behaviors will explain the gender and sexuality effects found in Hypotheses 1 to 4.
Data and Methods
Data
An important feature of the data for this study is the dyadic design. A growing number of studies point to the importance of dyadic data for studying close relationships (e.g., Galinsky and Waite 2014; Iveniuk et al. 2014; Waite et al. 2017), and dyadic data from couples are now available in some national data sets (e.g., Health and Retirement Study and National Social Life, Health and Aging Project). These data sets, however, do not include substantial numbers of same-sex couples or measures of social control. For the current study, we analyzed dyadic survey data collected from spouses who were legally married and aged 35 to 65 at the time of data collection. The Health and Relationships Project (HARP) data are from a questionnaire designed by the lead author and completed online by both spouses in same-sex and different-sex marriages in 2014 to 2015. The questionnaire took about 45 minutes to complete, and spouses completed surveys independently. The analytic sample included 838 individuals (419 couples) in 124 male same-sex marriages, 171 female same-sex marriages, and 124 different-sex marriages. The study was described to participants as focused on understanding how marriage affects health.
Massachusetts was selected as the study site because it was the first state in the United States to legalize same-sex marriage in 2004 and thus had a large population of married same-sex couples in long-term unions, the focus of the study. Same-sex couples who married from 2004 to 2012 and were between the ages of 35 and 65 were identified through the Massachusetts Registry of Vital Records and invited to participate through letters mailed to their address (about 70% of same-sex couples). Approximately 40% of different-sex couples were recruited by using publicly available demographic household data in Massachusetts (household location by city was selected to match city location of same-sex spouses selected through the Vital Records office). Participating couples could refer both same-sex and different-sex married couples who met the study requirements (30% of same-sex couples and 60% of different-sex couples were identified through such referrals). Some participants moved from Massachusetts or referred married family members and friends living outside of Massachusetts (about 50% of couples).
The sample was recruited in a systematic and purposive way to create comparable groups of gay, lesbian, and heterosexual married couples. Participants were matched on age, relationship duration, and state of residence. Due to past legal restrictions on marriage for same-sex couples, we measured total relationship duration based on the total number of years partners lived together (years cohabiting and married combined). Average relationship duration was 16 years for gay couples, 14 years for lesbian couples, and 16 years for heterosexual couples. We do not have information on whether respondents were in first or subsequent marriages, a limitation of our data. Descriptive data in Table 1 show that on average, spouses in same-sex marriages were slightly older, included fewer racial-ethnic minority respondents, and were more highly educated compared to spouses in different-sex marriages. Although the study sample is more highly educated and includes fewer racial-ethnic minorities than national estimates, the difference between same-sex and different-sex couples in the study sample parallels the difference found in national estimates (i.e., same-sex couples are less likely to include racial-ethnic minorities and more highly educated than different-sex couples; Gates 2015). We emphasize, however, that this purposive sample is not representative of the larger U.S. population and should not be generalized as such. Given the structure of the dyadic data, in the Results section, we refer to the respondent as the actor and the respondent’s spouse as the partner to distinguish each spouse’s report within dyads.
Descriptive Information on Demographic Characteristics and Study Variables from the Health and Relationships Project (HARP) (n = 838 individuals; 419 marriages).
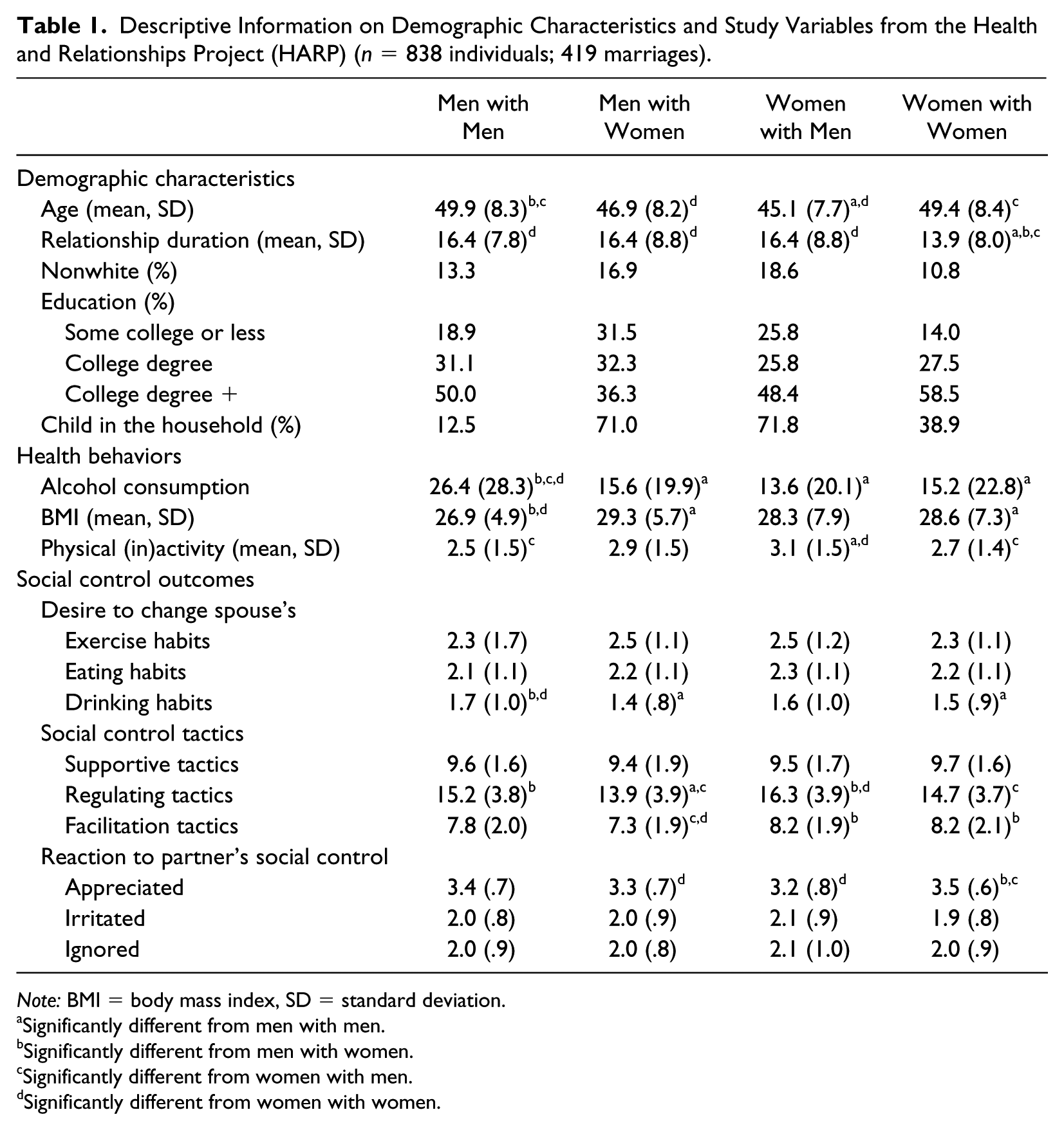
Note: BMI = body mass index, SD = standard deviation.
Significantly different from men with men.
Significantly different from men with women.
Significantly different from women with men.
Significantly different from women with women.
Measures
Social control
We considered three aspects of social control as dependent variables: desire to change a partner’s health habits, social control tactics used to influence a partner, and reactions to a partner’s social control efforts. Response options for each social control question described in the following included: 1 = not at all, 2 = a little, 3 = some, and 4 = quite a bit. Responses to questions were summed and standardized to create the measures described in the following.
For desire to change health habits, actors were asked how much they would like their spouse to change their: (a) exercise habits, (b) eating habits, and (c) drinking habits. Three types of social control tactics were assessed (adapted from Butterfield and Lewis 2002). We assessed direct social control with six questions assessing how often actors used the following regulation tactics to influence their partner’s health habits: (a) ask or remind your spouse to change their habits, (b) express worry or concern, (c) express frustration or irritation, (d) state how important it is to you, (e) drop hints, and (f) try to reason with your spouse, be logical. Indirect social control was based on three questions assessing how often actors used the following facilitation tactics to influence their partner’s health habits: (a) model the behavior, (b) offer to make changes with your spouse, and (c) change the environment. We also constructed a measure of supportive tactics based on three questions that were a blend of direct and indirect social control. Actors were asked how often they used the following tactics to try to influence their spouse’s health habits: (a) provided encouragement and support, (b) praised or complimented your spouse, and (c) used humor, made jokes. Items used to measure social control tactics were adapted from measures reported in previous work on social control (e.g., Butterfield and Lewis 2002). We also considered actors’ reports on three types of reactions to their partner’s social control efforts to influence their health habits. Actors were asked how often they felt the following when their partner tried to influence their health habits: (a) appreciative, (b) irritated, and (c) inclined to ignore their spouse. Items used to measure response to social control were adapted from Tucker and Anders (2001).
Health behavior
We considered three measures to assess health behaviors. Physical activity was constructed based on answers to questions regarding how often the respondent engaged in both moderate (e.g., taking a walk or using a vacuum cleaner) and vigorous activity (e.g., running or lifting heavy objects) on the following scale: 1 = several times a week or more, 2 = about once a week, 3 = several times a month, 4 = about once a month, 5 = less than once a month, and 6 = never. Answers to these two questions were summed and divided into quintiles to create five groups of nearly equal sample size. The group in the top quintile represents the 20% of the sample that is the most physically inactive. The final measure of physical inactivity included five categories ranging from 1 = most active to 5 = most inactive. Body mass index (BMI) was constructed based on self-reported height and weight and is a continuous measure ranging from 15 to 50. We top-coded BMI at 99% to account for a small number of extreme outliers. Alcohol consumption was based on the average number of days respondents drink per month multiplied by the typical number of drinks respondents reported consuming on days that they drink. We top-coded this variable at 90 drinks per month to reduce skew due to outliers. On average, respondents drank 18.35 alcoholic beverages per month. We also addressed the importance of spousal discordance on health habits. We measured actor-partner discordance on each health behavior by subtracting the partner’s value from the actor’s value. Thus, positive values indicate when the actor reported higher values on physical inactivity, higher BMI, and higher alcohol consumption than their partner, whereas negative values indicate when the actor had lower values compared to their partner.
Covariates
In all models, we adjusted and controlled for covariates that may be independently associated with social control, including relationship duration (in years, as described previously), educational attainment (less than college degree as reference category, college degree, more than college degree), and race (1 = nonwhite). Significant associations between covariates and outcomes are described in the text but not presented in the tables; full information on all associations are available on request.
Analytic Strategy
We used mixed-effects multilevel modeling to examine gender differences in social control while accounting for the nested structure of the data and to account for interdependence between married spouses. The term mixed refers to the inclusion of both fixed (i.e., standard regression coefficients) and random (i.e., variability in model intercepts and slopes) effects in the estimated models. Both members of dyads are included in the analyses as actors and partners because we have self-report data from both spouses. We specified respondents as nested within couples; however, models were estimated with only a random intercept but not a random slope because dyads contain only two respondents. We specified that this random intercept has an error structure consisting of equal variances and one pairwise covariance per couple to account for interdependence between couples. Multilevel modeling also allows for the estimation of effects when dyadic samples include both distinguishable (i.e., different-sex) and indistinguishable (i.e., same-sex) dyads. We employed the factorial method, an extension of the Actor-Partner Interdependence Model (West, Popp, and Kenny 2008). This method is preferred over models with a four-group comparison variable because the factorial method provides separate main effects for actor (or respondent) gender (women compared to men), and partner gender (married to a woman compared to married to a man) and an interaction effect of actor and partner gender (same-sex dyad compared to different-sex dyad). We then used these regression estimates to calculate predicted scores for four groups: men married to men, men married to women, women married to men, and women married to women. The equations for models examined in the current study were as follows (where individual i is nested within dyad j):
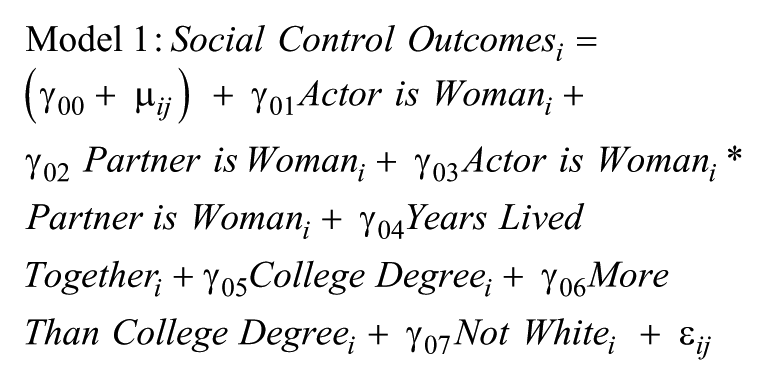


We first tested whether actor gender (i.e., actor is woman) was a significant predictor of each social control outcome and then tested whether partner gender (i.e., partner is woman) was a significant predictor after controlling for actor gender (Model 1). The interaction of actor gender and partner gender in this model (same-sex couple in tables) tested whether the actor gender and partner gender effects depend on whether one is married to a same- or different-sex spouse. We included the partner/spouse’s health behavior in Model 2 and actor-partner health behavior discordance in Model 3 to examine whether the gender effects found in Model 1 differed after taking health behaviors into account.
Results
Desire to Change Spouse Health Behavior
We begin by examining how the desire to change a spouse’s health behaviors varies for men and women in same-sex and different-sex unions. Figure 1 illustrates these differences (based on results from Table 2, Model 1 in each panel) for each health behavior. Men and women in different-sex unions were more likely than men and women in same-sex unions to want to change their partner’s exercise habits, as indicated by the negative and significant interaction term for same-sex couples (Panel A). There were no significant main or interaction effects of actor gender or partner gender on actor’s desire to change partner eating habits (Panel B). Actors were more likely to want to change a partner’s drinking habits when their partner was a man (regardless of gender of actor or whether one was in a same-sex or different-sex union) (Panel C). Having more than a college degree was associated with greater desire to change a spouse’s drinking habits; there were no other significant associations between controls and desire to change a spouse’s health behaviors.
Actor’s Desire to Change Partner Health Habits in Relation to Actor and Partner Health Behaviors (Health and Relationships Project [HARP], n = 838 individuals; 419 marriages).
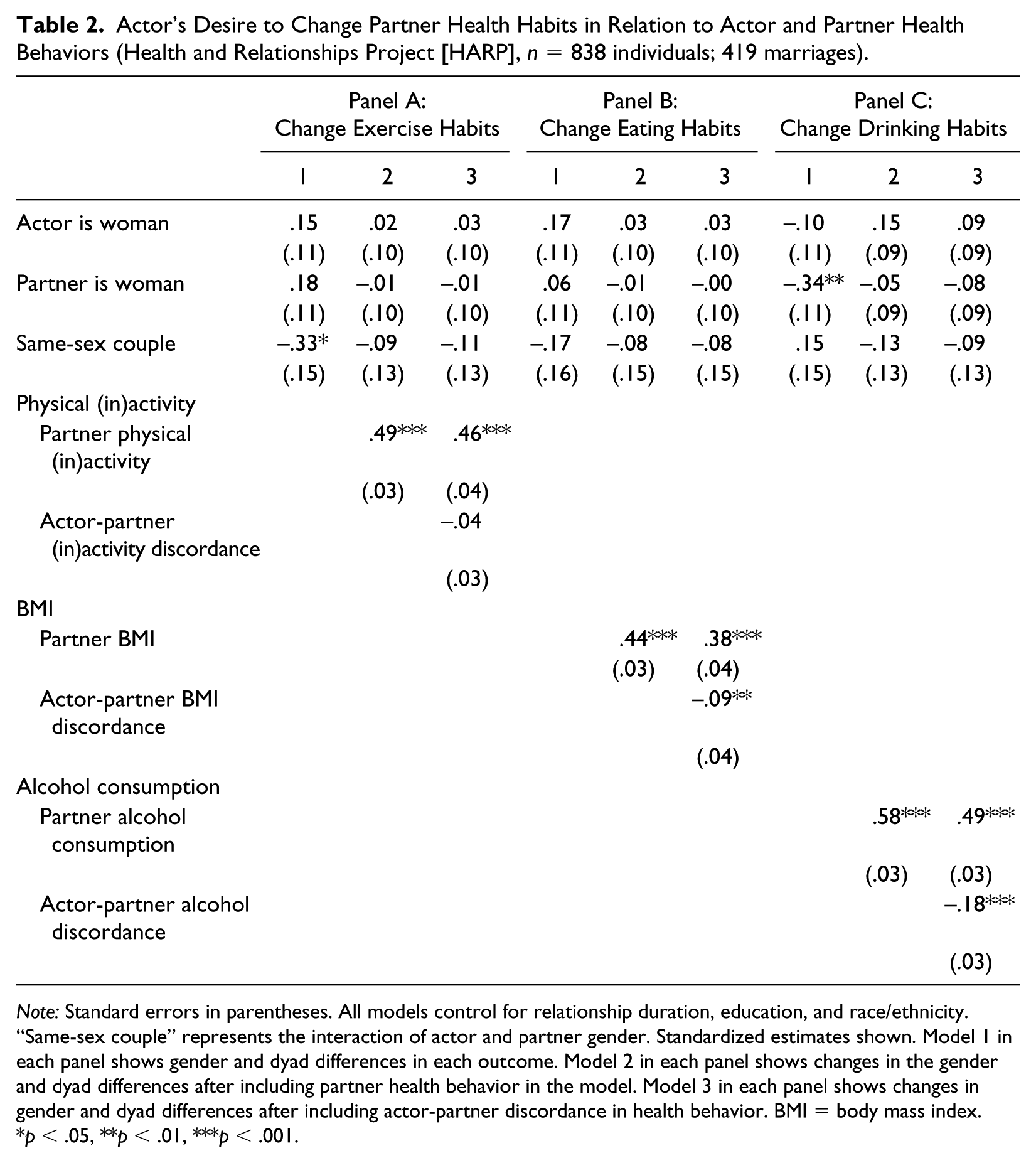
Note: Standard errors in parentheses. All models control for relationship duration, education, and race/ethnicity. “Same-sex couple” represents the interaction of actor and partner gender. Standardized estimates shown. Model 1 in each panel shows gender and dyad differences in each outcome. Model 2 in each panel shows changes in the gender and dyad differences after including partner health behavior in the model. Model 3 in each panel shows changes in gender and dyad differences after including actor-partner discordance in health behavior. BMI = body mass index.
p < .05, **p < .01, ***p < .001.
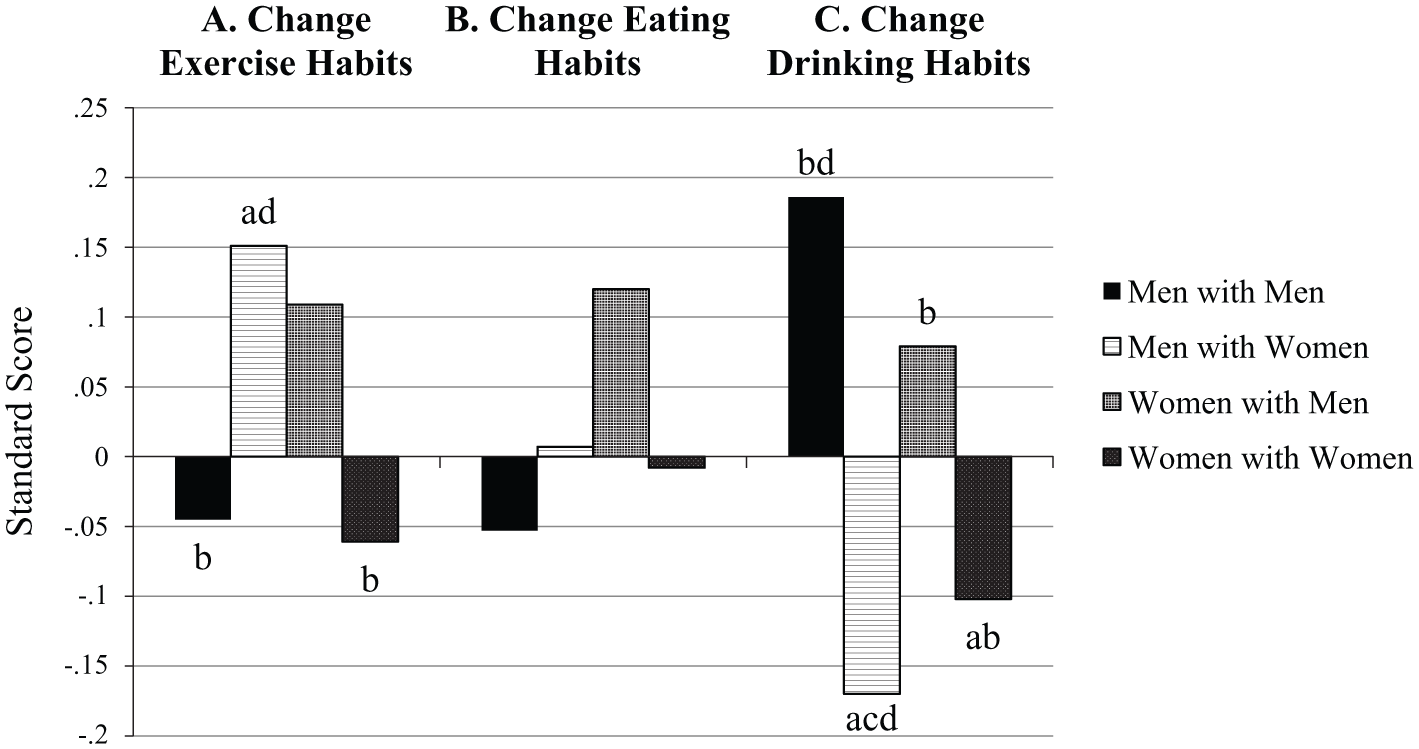
Predicted Standard Scores for Desire to Change Partner Health Habits (based on results from Table 2, Model 1).
Table 2 also addresses how partner health behavior (Model 2) and partner health behavior relative to actor health behavior (actor-partner discordance) (Model 3) influence the desire to change a partner’s health habits. Panel A, Model 2 shows that actors had a greater desire to change their partner’s exercise habits if their partner was more physically inactive. This association fully attenuated the dyad effect, suggesting that spouses in different-sex marriages were more likely to want to change their partner’s exercise habits because their partners were more likely to be physically inactive compared to individuals in same-sex marriages. There was no significant association between actor-partner discordance on physical inactivity or the desire to change a spouse’s exercise habits after controlling for partner physical inactivity (Panel A, Model 3). Partner BMI (Panel B, Model 2) and actor-partner discordance in BMI (Panel B, Model 3) were both significant, indicating that actors had a greater desire to change their partner’s eating habits when their partner weighed more and their partner’s BMI was higher than their own BMI. Models 2 and 3 in Panel C show that actors were more likely to want to change a partner’s drinking habits when their partner drank more and the actor drank less than their partner. The partner gender effect in Model 1 was no longer significant in Model 2, suggesting that the greater alcohol consumption of men compared to women explained the greater desire to change drinking habits for respondents (both men and women) when they were married to a man.
Social Control Tactics
Figure 2 (based on results from Table 3, Model 1 in each panel) summarizes results from the assessment of group variation in three types of social control tactics used to influence partner health behaviors. Figure 2 (Panel A) shows no significant differences in the use of supportive tactics across groups. We found a significant actor gender effect and partner gender effect predicting the use of regulation tactics. These effects were additive, as illustrated in Figure 2, Panel B, such that women married to men used regulation tactics the most and men married to women used regulation tactics the least. Figure 2, Panel C shows a significant partner gender effect, suggesting that men married to women were least likely to use facilitation tactics. Longer relationship duration was associated with greater use of supportive tactics; there were no other significant associations between control variables and tactics.
Actor’s Social Control Tactics in Relation to Actor and Partner Health Behavior (Health and Relationships Project [HARP], n = 838 individuals; 419 marriages).
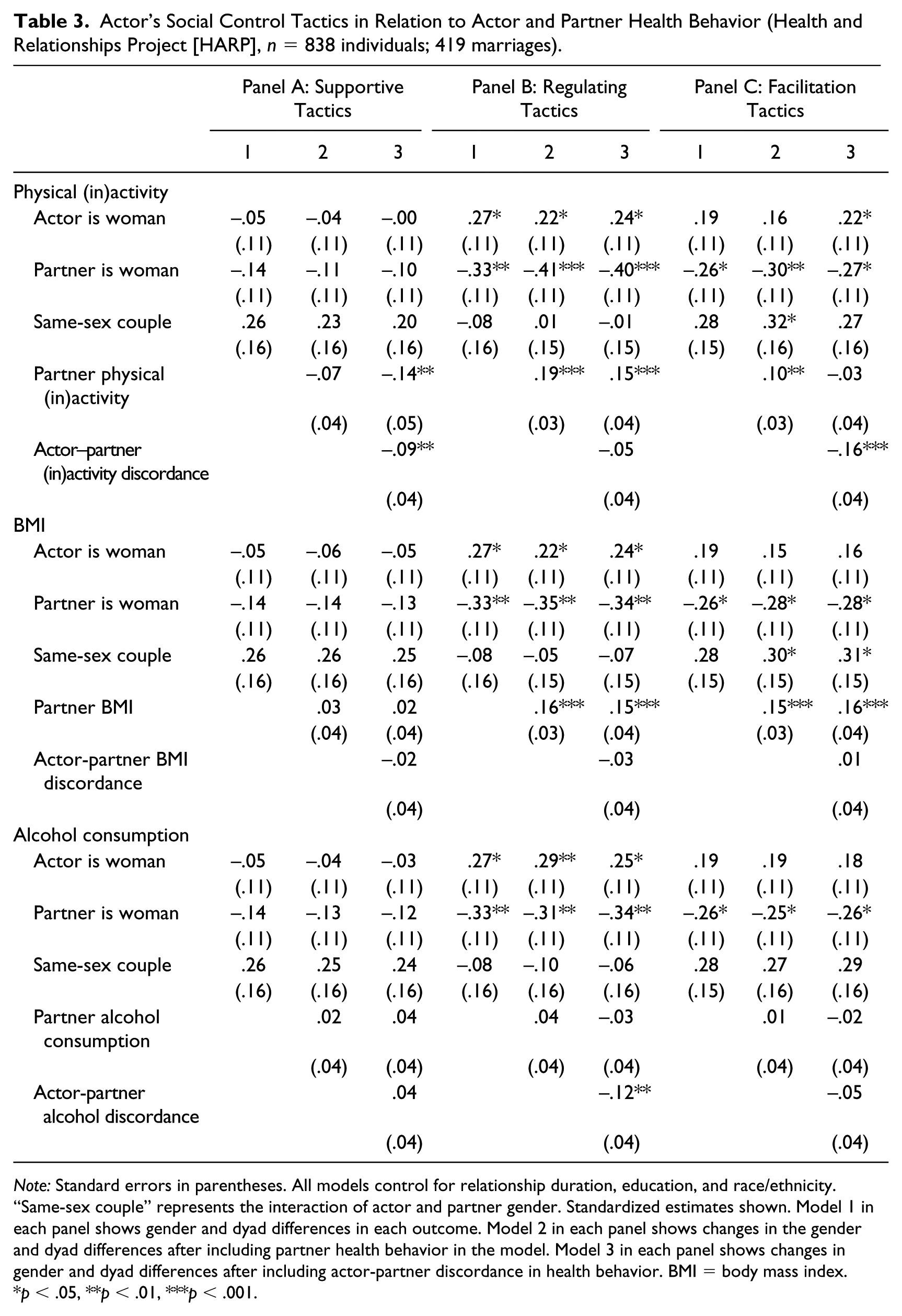
Note: Standard errors in parentheses. All models control for relationship duration, education, and race/ethnicity. “Same-sex couple” represents the interaction of actor and partner gender. Standardized estimates shown. Model 1 in each panel shows gender and dyad differences in each outcome. Model 2 in each panel shows changes in the gender and dyad differences after including partner health behavior in the model. Model 3 in each panel shows changes in gender and dyad differences after including actor-partner discordance in health behavior. BMI = body mass index.
p < .05, **p < .01, ***p < .001.
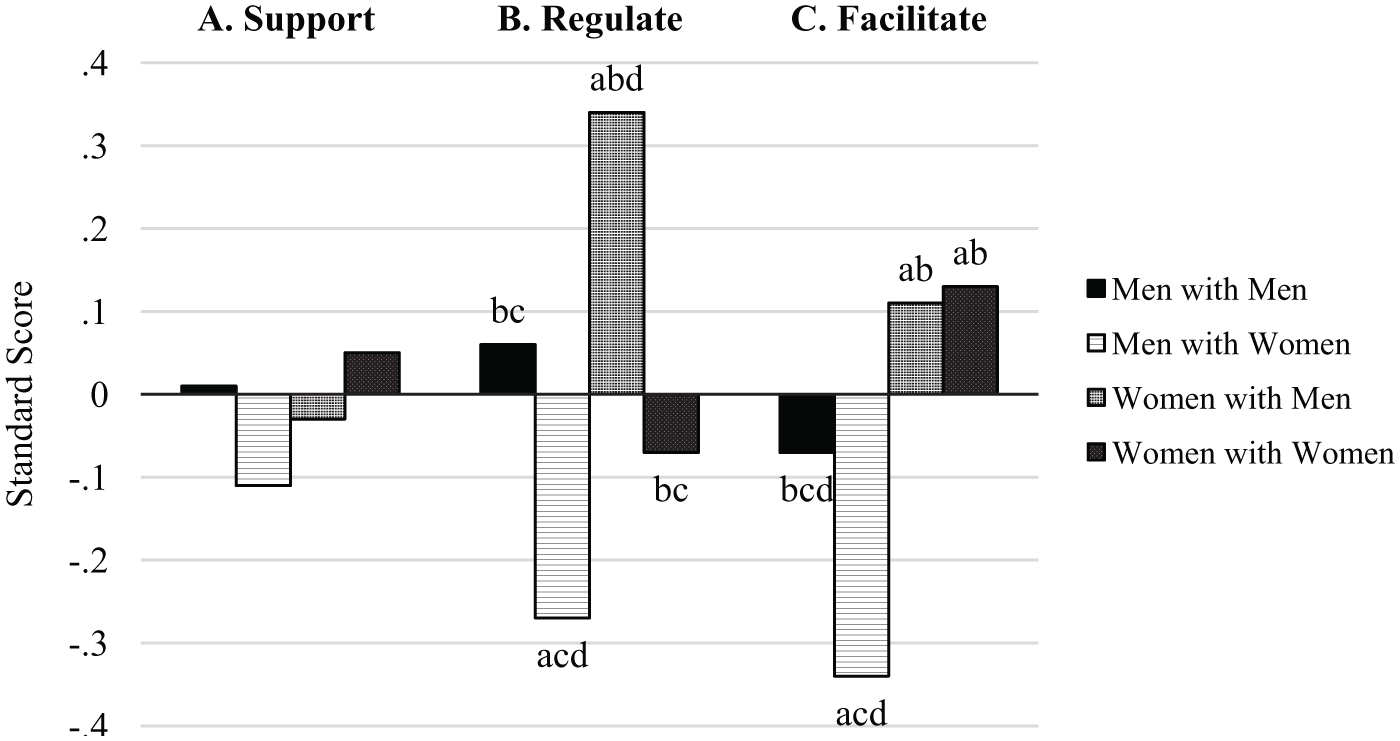
Predicted Standard Scores for Social Control Tactics (based on results from Table 3, Model 1).
Table 3 also addresses whether partner health behavior and actor-partner discordance on three health behaviors explain group differences in each type of social control tactic. Results in Table 3 reveal very little variation in the use of supportive tactics based on partner health behavior (Panel A, Model 2) or actor-partner discordance in health behavior (Panel A, Model 3), with the exception that actors provided less supportive social control for partners who were more inactive, particularly when actors were less physically inactive than their partners (Panel A, Model 3).
Model 2 in Panel B (Table 3) shows that actors reported more attempts to directly regulate a partner’s behavior when their partner was more physically inactive or more overweight. Only actor-partner discordance in alcohol use predicted regulation tactics such that actors regulate partners more when partners drink more than actors. Partner health behavior and actor-partner discordance in health behavior did not change the significant gender differences in regulation tactics found in Model 1.
Actors also reported more facilitation tactics when their partner was more physically inactive or heavier (Table 3, Panel C, Model 2). However, the association between facilitation tactics and partner physical inactivity was explained by actor-partner discordance in physical activity, such that actors who were less physically inactive than their partners reported more facilitation tactics (Panel C, Model 3). Gender differences in facilitation tactics were generally unchanged with the addition of partner health behavior and actor-partner health behavior discordance. However, actor gender became significant with the addition of both partner and actor-partner discordance in physical inactivity (Model 3), suggesting that women are more likely to use facilitation tactics on their partner because they are less inactive than their partner.
Reactions to Social Control from One’s Spouse
Figure 3 (based on Table 4, Model 1 in each panel) summarizes results assessing group variation in respondents’ reactions to social control efforts from their spouse. We found a significant actor gender effect and a dyad gender effect predicting the degree to which actors appreciated their partner’s social control efforts. These effects operated in different directions, as illustrated in Figure 3, Panel A, such that women married to men were the least likely to appreciate social control from a spouse and women married to women were most likely to appreciate social control from a spouse. Results shown in Figure 3, Panel B reveal no gender differences across groups in terms of feeling irritated by social control efforts from a spouse. Panel C in Figure 3 shows that women married to men are more likely than women married to women to ignore social control efforts from a spouse. Those with a college degree or higher reported greater appreciation of their spouses’ social control efforts compared to those without a college degree. No other controls were significant.
Actor’s Reaction to Partner’s Social Control Tactics in Relation to Actor and Partner Health Behavior (Health and Relationships Project [HARP], n = 838 individuals; 419 marriages).
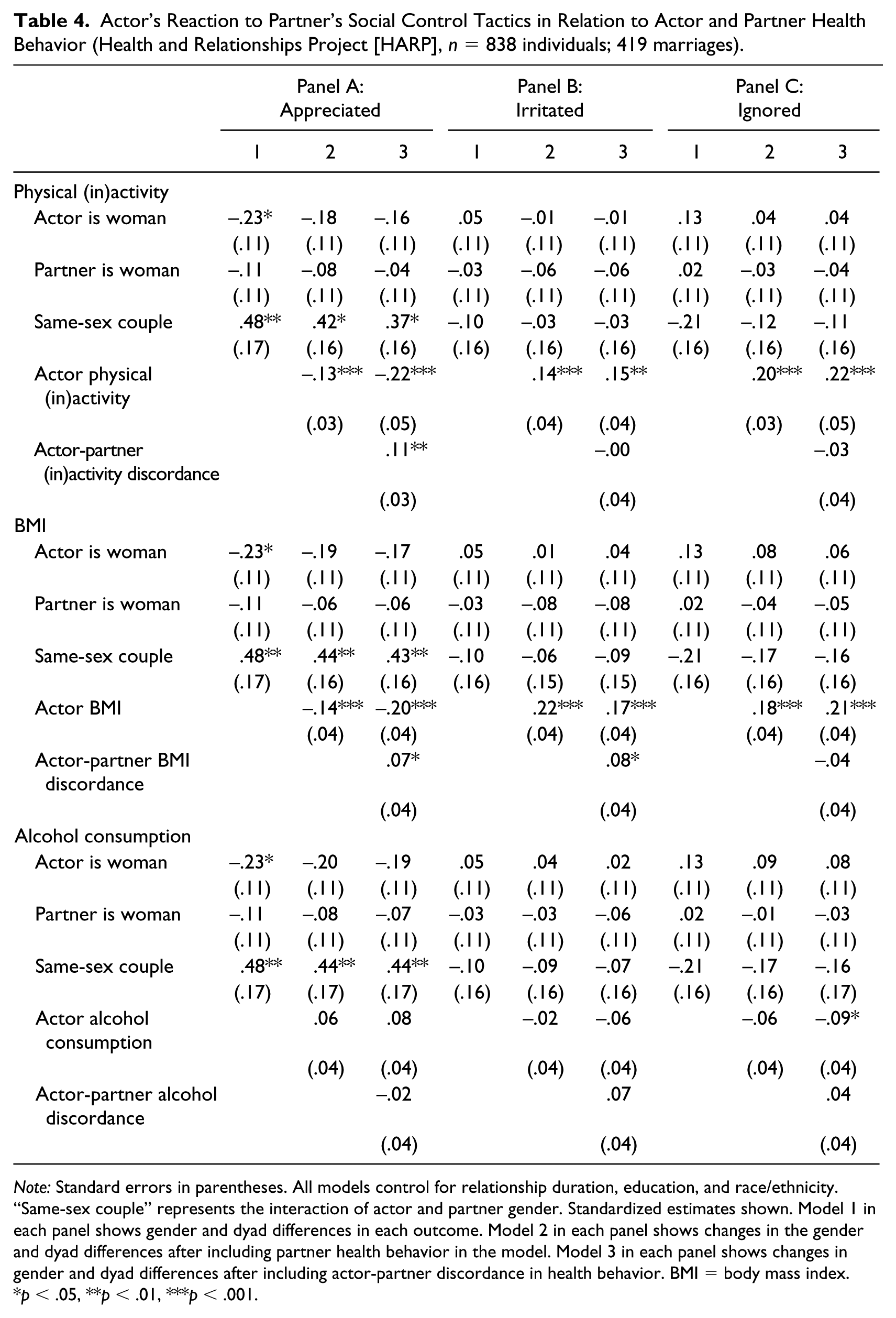
Note: Standard errors in parentheses. All models control for relationship duration, education, and race/ethnicity. “Same-sex couple” represents the interaction of actor and partner gender. Standardized estimates shown. Model 1 in each panel shows gender and dyad differences in each outcome. Model 2 in each panel shows changes in the gender and dyad differences after including partner health behavior in the model. Model 3 in each panel shows changes in gender and dyad differences after including actor-partner discordance in health behavior. BMI = body mass index.
p < .05, **p < .01, ***p < .001.
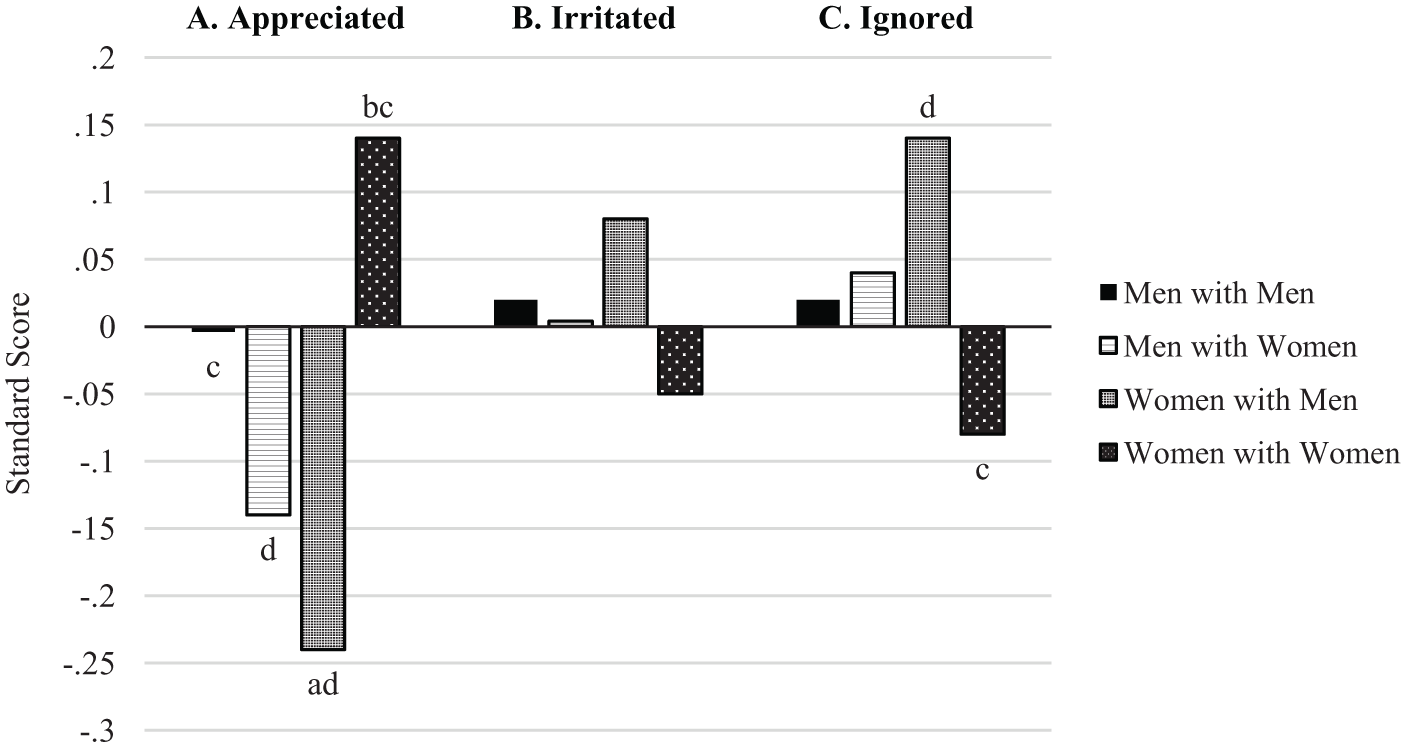
Predicted Standard Scores for Reactions to Social Control (based on results from Table 4, Model 1).
In Table 4, we considered whether/how actor health habits and actor-partner health behavior discordance (on physical activity, body mass index, and alcohol consumption) were associated with how the actor feels about social control from their partner. Actors who had lower physical inactivity and lower BMI than average reported greater appreciation of their spouses’ social control efforts (Table 4, Panel A, Model 2). Moreover, after controlling for partner health behavior, actors reported greater appreciation when they reported greater physical inactivity and BMI than their partners (Panel A, Model 3). The inclusion of actor health behavior and discordance reduced the actor gender effect, which likely reflects gender differences in physical activity, BMI, and alcohol consumption. Compared to physical activity and BMI, alcohol consumption was much less strongly tied to reactions to social control efforts.
Results in Panels B and C, Model 2 (Table 4) show that respondents who were more physically inactive and those who were heavier reported feeling more irritated by their spouse’s social control efforts and more likely to ignore their spouse’s social control efforts. Those with lower alcohol consumption than average were also more likely to ignore their spouse. Only greater actor-partner discordance on BMI, with actors heavier than their partner, was associated with feeling more irritated by spouses’ attempts to influence their behavior (Panel B, Model 3).
Summary of Support for Hypotheses
Overall, we find little support for Hypothesis 1—that women are more likely than men to want to change their spouse’s health habits. However, both men and women are more likely to want to change their spouse’s drinking habits if their spouse is a man. We find general support for Hypothesis 2 in that women are more likely than men to use indirect and direct social control (i.e., facilitation and regulation) to influence their spouse’s health habits. Hypothesis 3, suggesting stronger reactions (positive and negative) to social control by women compared to men is not supported. Hypothesis 4, suggesting that gender effects in Hypotheses 1 to 3 are more apparent for different-sex marriages is generally supported. For example, respondents in different-sex marriages (regardless of gender) are more likely than respondents in same-sex marriages to want to change their spouse’s exercise habits, and women married to men report more regulation of their spouses than women married to women. In addition, women married to men are less likely to appreciate their spouse’s social control, whereas women married to women are more likely to appreciate their spouse’s social control. Hypothesis 5, suggesting that partner health behavior and spousal discordance on health behavior will explain gender and union status effects in Hypotheses 1 to 4, is generally not supported, with the exception that across marital dyads, spouse’s less healthy habits explain why respondents want to change their spouse’s behaviors.
Discussion
Decades of research on heterosexual marriage and health have emphasized gender difference within marriage, with women devoting more effort toward protecting their spouse’s health than men (Rendall et al. 2011; Waite 1995). This literature points to women’s influence over men’s health behaviors as contributing to the marital advantage in health for men. Yet most prior research on marriage and health behavior has failed to consider the experiences of gay and lesbian couples. We work from a gender-as-relational perspective to suggest that gendered patterns of spousal influence over health behaviors may unfold differently for same-sex and different-sex couples. We take advantage of a unique data set that includes reports from both spouses in midlife same-sex and different-sex marriages. We consider how much spouses want to change each other’s behaviors, the tactics they use to influence each other, and how spouses feel about each other’s attempts to influence their behaviors. We also consider how the health behaviors of both spouses shape these patterns. An overarching theme from our results is that even though health behavior and health behavior discordance between partners are strong predictors of social control dynamics, these variables do not fully explain the gendered patterns of social control tactics used by spouses to influence each other’s health habits. This theme suggests that the gendered patterns in our results are quite robust even in the face of powerful contextual effects of health habits.
A second important theme concerns the gendered patterns—if we focus solely on the results for different-sex couples in our sample, patterns of social control are consistent with prior research in that women are more likely than men to be the agents of control in trying to influence their spouse’s health habits, whereas men are more likely than women to be the targets of such efforts (e.g., Berg and Upchurch 2007; Rook et al. 2011; Umberson 1992). However, our inclusion of men and women in same-sex couples disrupts the traditional interpretation of gendered marital dynamics in relation to health behavior. Our findings support the gender-as-relational perspective in that social control dynamics depend not only on gender of the agent and target of social control but also whether one is in a same-sex or different-sex marriage. For example, women are more likely than men to attempt to regulate a spouse’s health habits, but this pattern is stronger for women married to men than women married to women. Men are less likely than women to attempt to regulate their spouse’s health habits, but this pattern is stronger for men married to women than men married to men. More indirect efforts at influencing a spouse’s health habits (i.e., facilitation) are gendered in a different way in that women are more likely than men to report the use of these tactics—but this is the case in same-sex as well as different-sex marriages. Notably, indirect social control tactics are a kind of stealth tactic in that the target spouse may not even be aware of the social control. While previous research has suggested that women are more likely than men in different-sex unions to use these indirect, or stealth, control tactics (e.g., Tucker and Mueller 2000; Umberson 1992), this is the first study to show that women are more likely than men in same-sex marriages to use indirect/stealth tactics to influence their spouse’s health habits.
We also find gendered patterns concerning how spouses feel about each other’s efforts to influence their health habits—in terms of feeling appreciative, irritated, or inclined to ignore their spouse. Prior research suggests that heterosexual women may be less appreciative of a spouse’s social control efforts because these efforts from husbands are perceived as inappropriate or unkind (Markey et al. 2008). In line with this work, we also find that women married to men feel less appreciative of their spouse’s social control efforts compared to other groups. However, our inclusion of same-sex couples shows that this is not true for all women. In fact, women married to women feel most appreciative of their spouse’s efforts in comparison to other respondents, whereas women married to men feel least appreciative of these efforts. Women married to women may be more appreciative of their spouse’s social control efforts because their spouse is more likely to use social control tactics that are supportive rather than critical or coercive (Reczek and Umberson 2012)—a topic that should be further explored in future research.
In sum, our results suggest that although gender differences in social control/health behavior dynamics are often apparent for men and women in different-sex marriages, these gendered patterns sometimes unfold in different ways depending on whether one is married to a man or woman—a pattern supporting the proposition that gender is relational (Springer et al. 2012; West and Zimmerman 2009). Though social conditions associated with gender often put responsibility for the health needs of others on women, partner inequality in attending to a spouse’s health needs is greater within different-sex couples than within same-sex couples. These findings add to prior research suggesting greater partner equality in various types of work within different-sex compared to same-sex unions (Reczek and Umberson 2016).
Gender, Health Behavior, and Health Behavior Concordance between Spouses
Our findings also point to the importance of health habits as strong drivers of relationship dynamics for spouses in both same-sex and different-sex marriages. Although efforts to influence a spouse’s health behaviors may lead to improved health behaviors over long periods of time, at any given point in time, spouses may be most motivated to influence the health habits they are most concerned about (Lewis and Butterfield 2005). The present results provide strong and consistent evidence that respondents desire more change in their spouse’s health habits and devote more effort toward changing their spouse’s health behaviors (through both direct and indirect tactics) when they are married to a spouse who weighs more, is more physically inactive, or drinks more—especially when respondents report healthier habits than their spouse. These patterns point to the salience of health behaviors for marital relationships generally. However, discordance in spouses’ health habits is more likely for different-sex than same-sex couples (Holway et al. 2018). Because of greater health behavior discordance in different-sex couples, individuals (especially women) in different-sex marriages may be prompted more often to influence their spouse’s health behaviors. Future research should delve more deeply into the ways in which health behaviors both influence and are influenced by marital dynamics for same-sex as well as different-sex couples.
Future research should also consider the implications of social control and health habits for marital quality and psychological well-being. Social control may result in improved health and health habits over months and years, yet on a more short-term or daily basis, these dynamics may increase marital strain, diminish marital quality, and increase psychological distress of both partners (Franks et al. 2006; Helgeson et al. 2004; Rook et al. 2011). Moreover, given recent research suggesting that stress affects marital dynamics in different ways for same-sex and different-sex couples (Donnelly, Umberson, and Kroeger 2018; Umberson et al. 2016), the effects of health behavior dynamics and the perceived stress of being the provider or the recipient of social control efforts may differ for same-sex and different-sex unions. For example, recent research suggests that physical illness may be more stressful for women than men in both same- and different-sex unions, although the stress is greater for women in different-sex marriages compared to women in same-sex marriages (Umberson et al. 2017). In sum, future research should consider the short-term and long-term effects of social control efforts on marital quality, psychological well-being, and health behaviors as well as health—for men and women in same- and different-sex marriages.
Limitations
The present study advances understanding of gendered marital and health behavior dynamics by analyzing dyadic data from same-sex and different-sex spouses. However, limitations should be noted. First, respondents in our study are aged 35 to 65 and represent members of a birth cohort who grew up in a period when marriage was not a legal option and discrimination against sexual minorities was more common and severe (Hammack et al. 2018). Members of these birth cohorts who formed long-term unions and eventually married may represent a highly select population. There is selection of more educated and affluent heterosexuals into marriage (Rendall et al. 2011), but this process of selection may be stronger for sexual minority populations. On the other hand, same-sex couples of this cohort may have been more limited in investing in their partner’s health because lifelong legal commitments were not available. Third, the use of cross-sectional data limits our ability to assess causal order. Fourth, as with any study based on self-reports, response bias may occur, and it is possible that positive response bias may be more common in reports from gay and lesbian spouses for whom legal marriage is relatively new and more politically fraught. Finally, purposive sampling was used as a recruitment strategy, and this limits the generalizability of the results.
Conclusion
This study goes beyond the traditional focus on heterosexual marriage by including men and women in same-sex marriages to shed new light on the gendered marital dynamics associated with health behaviors that may in turn influence long-term health and mortality risk. Decades of research have highlighted how women do more than men to influence their spouse’s health habits, to the health benefit of men. In turn, policymakers and practitioners have devoted considerable effort to harnessing heterosexual marital relationships in an effort to promote population health, and U.S. policies have emphasized the impact of marital ties on health behaviors (U.S. Department of Health and Human Services 2010, N.d). The present results suggest that public policy should consider how same-sex marriage may promote population health, particularly for sexual minority populations (LeBlanc et al. 2018; Wight et al. 2013). Same-sex spouses, like heterosexual spouses, actively work to influence and improve each other’s health habits, and they, like their heterosexual counterparts, do even more of this work when their spouse’s health habits are worse than their own habits. The growing number of same-sex married couples in the United States (Gates and Brown 2015) along with sexual minority health disparities (Institute of Medicine 2011) and gender inequality within heterosexual marriage (Ferree 2010; Ridgeway 2011) demand inclusion of same-sex couples in future research on marriage and health. This approach can shift the focus from gender difference within marriage to a focus on marital dynamics across gendered relational contexts and has the potential to expand our understanding of gender and health dynamics within heterosexual marriages as well as same-sex marriages.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, by grant R21AG044585 from the National Institute on Aging (PI, Debra Umberson); grant P2CHD042849 awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development; and grant T32 HD007081, Training Program in Population Studies, awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Amanda M. Pollitt also acknowledges support from the National Institute on Alcohol Abuse and Alcoholism (grant F32AA025814). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.