
Abstract
A dominant discourse in the social sciences theorizes that religious diversity puts individuals’ health at risk via interreligious hostility. However, this discourse overlooks the different subtypes of religious diversity and the moderation of political institutions. To better understand the issue of diversity and health, in this study, we distinguish between two subtypes of religious diversity—polarization and fractionalization—and argue that their impacts on health are heterogeneous. Using a sample of 67,399 individuals from 51 societies drawn from the 2010–2014 wave of the World Values Survey, our multilevel analyses show that religious polarization is negatively associated with individual health, whereas the health effects of religious fractionalization are positive. Moreover, the associations between religious polarization/fractionalization and individual health are found to depend on the democratic level of the state. In more democratic countries, the negative effects of polarization on health are mitigated, and the positive effects of fractionalization are stronger.
Sociological classics have long pointed out the importance of religious context in shaping individual health or health-related behavior (e.g., Durkheim [1897] 2008). Recent works on religious context and health have so far focused on two aspects of religious context: contextual religiosity (often operationalized as community-, county-, country-level means of individual religiosity variables, e.g., religious service attendance frequency, frequency of prayer, etc.) and religious population share (e.g., measured as the percentage of respondents or congregations affiliating with a particular religious tradition/denomination within a specific area; Blanchard et al. 2008; Dwyer, Clarke, and Miller 1990; Holt et al. 2006; Hsieh 2017; Nicholson, Rose, and Bobak 2009; Nie and Yang 2019; Stroope and Baker 2018). Both previously listed approaches consider the contextual role of religious phenomena at the aggregate level as an effective force sui generis. In a globalizing and multicultural world, the increasing level of religious diversity has become an important socio-ecological phenomenon that has sparked intense debate over its political consequences (e.g., Huntington 1998; Putnam and Campbell 2012; Wuthnow 2005). However, the intriguing role of such diversity on the well-being of individuals is rarely examined in empirical studies.
There are contrasting hypotheses about religious diversity and individual well-being. A large body of past works theorized religious diversity as a source of interreligious hostility (e.g., Blau 1974; Huntington 1998; Wuthnow 2005), which may bring forth religion-related tensions and conflicts that are adverse to individual well-being. However, a small group of studies suggested that religious diversity is a valuable collective resource that may facilitate interreligious learning and strengthen religious communities (e.g., Madsen 2007; Trejo 2009; Yang and Ebaugh 2011), thus generating more health benefits for individuals. The two contrasting arguments raise a question: Does religious diversity benefit or impair individual health? Alternatively, is it possible that both arguments offer some insight and are valid in different contexts?
In this article, we argue that the existing arguments fall short of understanding the health impacts of religious diversity due to two limitations. First, the field has overlooked different types of religious diversity (polarization and fractionalization) and has subsumed them all under the umbrella of “diversity.” Interreligious antagonism may be more severe in a country where a religious majority confronts a large minority group than in a society where multiple small-size religious groups coexist. Second, the relationship between religious diversity and health may be contingent on the democratic level of the state. Recent studies demonstrated that democratic institutions are critical social determinants of the overall health of a population (Barnish et al. 2018; Muntaner et al. 2011). Extending this line of research, we further argue that democratic institutions can moderate the link between religious diversity and health by reducing interreligious conflicts and protecting freedom of association. In other words, this study attempts to (1) examine the relationships between different types of religious diversity and individual health and (2) explore the moderating potential of the democratic level of the state on such relationships.
To achieve these goals, we apply multilevel regression modeling techniques to the sixth wave of the World Values Survey (2010–2014), a large international survey data set that contains important information on religious composition. In the following sections, by drawing on prior theories and research, we elaborate on potential mechanisms and set out a series of empirical expectations. Finally, we discuss our findings in light of theories of religious diversity, the role of politics in population health, and the religion-health link.
Background
Religious Context and Health
Since the founding era of sociology, there has been a long tradition of research focusing on religion and health. The literature has emphasized the influences of religious context on population health, mortality rates, or health-related behaviors (e.g., Blanchard et al. 2008; Durkheim [1897] 2008; Dwyer et al. 1990; Holt et al. 2006; Hsieh 2017; Nicholson et al. 2009; Nie and Yang 2019; Stroope and Baker 2018). This group of studies often measured the concept of religious context as context religiosity and religious population share.
What has been understudied in the aforementioned literature is the health-related effects of religious diversity. Religious diversity is different from contextual religiosity and religious population share. Contextual religiosity indicates how religious a population living in a particular area generally is but falls short of revealing if one religion dominates in that population or if there are several religions with approximate sizes. Religious population share refers to the size of one particular denomination or religious tradition within a specific locality, whereas religious diversity accounts for the number and the respective proportions of coexisting religions.
The health effects of religious diversity deserve careful attention because of the growing heterogeneity of religious composition in many parts of the world over recent decades. The recent massive immigration in both the United States and Europe led to the expansion of non-Christian religions (Pew Research Center 2017; Wuthnow 2005), and there has been a significant increase in the number of adherents of nontraditional religions in regions such as East Asia and Latin America (Pew Research Center 2014; Yang 2006). Additionally, this is an important issue because theorists have argued that religious diversity may weaken the plausibility of religion or lead religion to be more fundamentalist, with implications for religion’s relation to individuals (e.g., Berger 2014). So far, few scientific studies have been devoted to investigating how religious diversity shapes individual well-being and health outcomes. Notable exceptions include Ellison, Burr, and McCall’s (1997) work that shows city-level suicide rates and religious homogeneity are related in the United States. However, this study did not account for individuals’ overall health and told little about the dynamics outside the United States. Recently, some studies on individual health included a religious diversity index as a control variable, but these studies did not discuss the diversity-health link in a comprehensive way (Stavrova, Fetchenhauer, and Schlösser 2013; Stroope and Baker 2018). Generally, how religious diversity influences individual health is understudied empirically and theoretically.
Diversity to Conflict or Diversity to Solidarity?
A dominant discourse in the social sciences theorizes religious diversity as a source of discrimination, intolerance, and conflict, which is disruptive for social cohesion and individual well-being. This discourse highlighting the detrimental effects of religious diversity can be traced back to Blau’s (1974) theory of social structure. This theory proposes that on one hand, differentiation along the lines of social categories such as religion fortifies segregation and produces hostility between groups. On the other hand, sharing the same group affiliation contributes to the formation of informal friendship and secondary groups and shapes a cohesive public culture in the media, politics, and civil society. Recent studies further expressed the concern that religious diversity makes it difficult for people to share a sense of common identity and values and thus brings in the danger of social disintegration and conflict (e.g., Huntington 1998; Putnam and Campbell 2012; Wuthnow 2005). Wuthnow (2005:89) argued that religious diversity is a challenge in the United States because it “raises the specter of a frayed society, drawn in different directions by competing lifestyles, ethnic identities, national loyalties, customs, and beliefs.” In addition, scholars of religion pointed out that in diverse societies, actual or perceived competition between religious groups over power or economic resources may result in undesirable outcomes, including between-group mistrust and violence (Brubaker 2015; Gorski and Türkmen-Dervişoğlu 2013; Juergensmeyer 2018; Olson and Li 2015).
If the aforementioned arguments associating religious diversity and interreligious tension are correct, individuals will have poorer health in more religiously diverse settings. First, religion-related stigmatization may be severe in religiously diverse contexts. People who are stigmatized by other groups are likely to experience more stress and have fewer opportunities to obtain health and economic resources (Link and Phelan 2001). The adverse experiences in daily life—discrimination and prejudice—may be chronic stressors that can cause long-term dysfunction in physical and mental adjustment (Aneshensel 1992; Hu, Yang, and Luo 2017; Mezuk et al. 2013; Taylor, Buunk, and Aspinwall 1990; Yang, Hu, and Schieman 2019). Second, religion-based social segregation may reach high levels in diverse contexts. Some social capital studies argued that population heterogeneity is associated with lower levels of bridging social ties and civic engagement (Lancee and Dronkers 2011; Putnam 2007). According to the argument of these social capital studies, it is possible that people in religiously diverse contexts tend to withdraw from civic life and lose social capital, which is negative for individual well-being. Third, the occurrence of religious conflict events with personal or property damage may be a shocking-event stressor. This type of stressor inhibits the brain’s regulation of hormones and leads to an increased risk of physical illness (Kiecolt-Glaser 1999; Selye 1978). Overall, due to stigmatization, low levels of outgroup connections, and religious violence, people are likely to be less healthy in more religiously diverse societies.
This diversity-to-conflict argument contradicts the well-received discourse that praises the merits of multiculturalism. It is argued that multicultural interaction facilitates the exchange of ideas, provides opportunities for innovation, and inspires competition for the common good that benefits the whole society (Herring 2009; Page 2008; Putnam 2007). However, in terms of religious diversity, only a few previous studies suggested that it can benefit individual health. As shown by case studies from East Asia (Bays 2011; Madsen 2007), Latin America (Trejo 2009), and the United States (Yang and Ebaugh 2011), interreligious interaction often provides opportunities for religious groups in these settings to learn from each other and to strengthen themselves. In addition to cross-religion learning, another possible mechanism linking diversity and solidarity is that religious diversity may motivate clergies to better accommodate religious followers. The clergy’s accommodations, such as improving religious services, providing social services, and launching missionary works, may strengthen their communities (Stark and Finke 2000).
Following this line of reasoning that diversity leads to solidarity, religious diversity should benefit individual health. First, cohesive religious groups may be more effective in generating social capital. The social capital accumulated within a religious group may further encourage people to participate in other civic organizations (Putnam 2001). People belonging to these groups can obtain social and emotional support and build ties with their peers. Social capital has been demonstrated to be important for improving health (Elgar et al. 2011; Wu et al. 2018). 1 Second, religious groups with stronger solidarity may be more potent in regulating health-related behavior. Tight-knit networks and frequent interaction within such groups can prompt people to internalize religious norms and can function as social control over deviant behavior. Third, religious diversity likely benefits individual health by promoting volunteering. In the United States, past research found that people are more likely to volunteer in counties with higher levels of religious diversity (Borgonovi 2008). In this research, it was argued that because people in more diverse counties are more committed to their religious group, they are willing to and readily available to be recruited to volunteer. The positive effect of volunteering on individual overall health has been demonstrated (Piliavin and Siegl 2007). Therefore, generally speaking, religious communities in diverse contexts are more cohesive and offer more health benefits.
Although the existing scholarship, as reviewed previously, features contrasting propositions on the relationship between religious diversity and health, we suggest that the arguments may not be as contradictory as they seem. It is possible that each argument is valid only in some contexts where the meaning and content of diversity differ. To explore the contingent nature of the diversity-health relationship, in the following section, we first differentiate between two types of religious diversity that have different meanings for interreligious relations and individual health. We then discuss how the health impacts of religious diversity are conditioned on democratic institutions. Generally speaking, we propose that whether religious diversity benefits or impairs individual health depends on specific religious configuration and the democratic level of the state.
Religious Polarization and Religious Fractionalization
Religious polarization and fractionalization represent two types of religious diversity. Although they are conceptually distinguished from one another and also measured differently, popular discourses often confuse polarization with fractionalization. Polarization indicates how much a population is divided by a few similarly strong subgroups, with its extreme case being a population composed of two groups of equivalent size. In comparison, fractionalization refers to the degree to which a population is composed of a number of different small-size groups.
Interreligious conflicts may be more likely to break out in polarized societies than in fractionalized or homogeneous societies. First, in more polarized countries, mutual prejudice and hatred between religious groups may be more severe. Intergroup relation studies found that people belonging to a majority group may perceive being threatened when they face a large-size outgroup and thus become hostile toward outsiders. Intergroup relations may deteriorate due to the majority group’s hostility toward outgroups (Blumer 1958; Bobo and Hutchings 1996; Quillian 1996; Stephan and Stephan 2000). A polarized society means a population is divided as a majority group versus one or two large minority groups. As a result, religious groups in this circumstance may become hostile toward each other. Second, it may be easier to encourage or mobilize people into interreligious conflicts in more polarized countries. Because each religious group composes a substantial portion of the whole population, a single group may provide a sufficient recruitment pool for violent collective actions (Esteban and Ray 1999; Montalvo and Reynal-Querol 2005; Reynal-Querol 2002). Therefore, a demographic composition characterized by religious polarization is conducive to intergroup antagonism. In such a context, the adverse impacts theorized as the diversity-to-conflict mechanism may prevail over the beneficial effects that religious diversity may have on individual health. We hypothesize as follows:
Hypothesis 1: Religious polarization is negatively associated with individual health.
Intergroup dynamics may be different in countries characterized by religious fractionalization. In societies where multiple small-size religious groups coexist, each group hardly perceives other groups as severe threats because none of them have an overwhelming strength. The interreligious dynamics in early America provide a supportive case for this argument. Heclo (2007) concluded that the religious composition in the American colonies was so diverse that no sects could keep up with persecuting others. Therefore, religious diversity facilitated a growing trend toward mutual toleration and amicability in the United States. Moreover, social movement scholars argued that mobilizing diverse groups with different identities and beliefs is more difficult and costly than mobilizing an internally homogenous group (Montalvo and Reynal-Querol 2005; Polletta and Jasper 2001). According to this perspective, the size of any particular religious group in a factionalized society is limited and the cost of coordination across multiple distinct groups is high. Thus, organizing large-scale, communal conflicts between religions is more difficult in more fractionalized societies. In fact, before this modern scholarship, the pacifying effect of religious fractionalization had been pointed out by classic social thinkers. Voltaire ([1733] 1980:41), for example, about 300 years ago, wrote: “If there were only one religion in England there would be danger of despotism, if there were two they would cut each other’s throats, but there are thirty, and they live in peace and happiness.” The increasing level of religious fractionalization would probably not undermine interreligious relations, whereas religious groups in this context could generate more health benefits for individuals as suggested by the diversity-to-solidarity mechanism. We propose the second hypothesis:
Hypothesis 2: Religious fractionalization is positively associated with individual health.
The Moderating Effects of Democracy
A growing body of studies has focused on the political determinants of population health (Barnish et al. 2018; Mackenbach, Hu, and Looman 2013; Muntaner et al. 2011). Some of these studies found that people living in democracies are healthier than those under the rule of nondemocratic regimes. Moving beyond the existing studies, we argue that the democratic level of the state may moderate the relationships between polarization/fractionalization and health. This is because the extent to which the diversity-to-conflict and the diversity-to-solidarity mechanisms affect population health depends on the political context.
As articulated by the diversity-to-conflict mechanism, religious polarization may impair people’s health because it may cause between-religion conflicts. This conflict-triggering effect of polarization may be mitigated by democratic institutions. Political scientists noted that countries that are more democratic experience fewer internal conflicts (Gleditsch and Ruggeri 2010; Goldstone et al. 2010; Hegre et al. 2001). An important reason for this pattern is that democratic institutions (e.g., elections and legislatures) provide opportunities for people to voice grievances, pursue interests, and resolve disputes. These institutions function as a substitute for using conflict to achieve these purposes. When interreligious hostility and struggles arise, democratic institutions make it possible to address them peacefully and promptly. By contrast, when democratic institutions are weak or nonexistent, resorting to violence becomes more attractive. Consequently, minor discrimination, prejudice, and mistrust between religious groups may escalate into large-scale and severe conflicts, resulting in more damage to social and individual well-being.
The positive effects of religious fractionalization on health may also be conditioned on democracy. A political prerequisite for the diversity-to-solidarity mechanism is that freedom of association and speech are protected. Democracies encourage people to form civic associations to address their own issues (e.g., O’Donnell and Schmitter 2013; Tocqueville [1835] 2010), whereas nondemocratic regimes are suspicious of civic engagement, using various tactics such as repression of violence and prohibition of donations to prevent citizens’ engagement in civic life (Puddington 2016). Many people will be deterred from civic life if the access to civic associations, including religious groups, is restricted and if the participation in these associations incurs punishment. Under such a circumstance, even if religious fractionalization provides opportunities for people of different religions to come into contact with and learn from one another, it will be difficult for religious individuals under political restriction to join collective religious activities, accumulate social capital, and learn religious norms, let alone build a cohesive community. In other words, when the freedom of association and speech is guaranteed by democratic institutions, the diversity-to-solidarity mechanism may work. Overall, democratic institutions amplify the beneficial aspects of religious diversity and mitigate the negative aspects.
Hypothesis 3: The negative effects of religious polarization on individual health are weaker in more democratic countries.
Hypothesis 4: The positive effects of religious fractionalization on individual health are stronger in more democratic countries.
Data and Methods
The main data source for our research was the sixth wave (2010–2014) of the World Values Surveys (WVS), which includes about 86,000 respondents from 60 societies (Inglehart et al. 2014). The WVS are nationally representative surveys based on a form of stratified random sampling to obtain representative national samples. 2 In addition, we drew country-level variables from Polity IV data, World Bank data, and Religion and State data. Descriptive statistics are presented in Table 1. Respondent frequency per country and nation-level variables are shown in Table A in the online version of the article.
Summary Statistics for All Study Variables from the 2010–2014 World Values Survey.
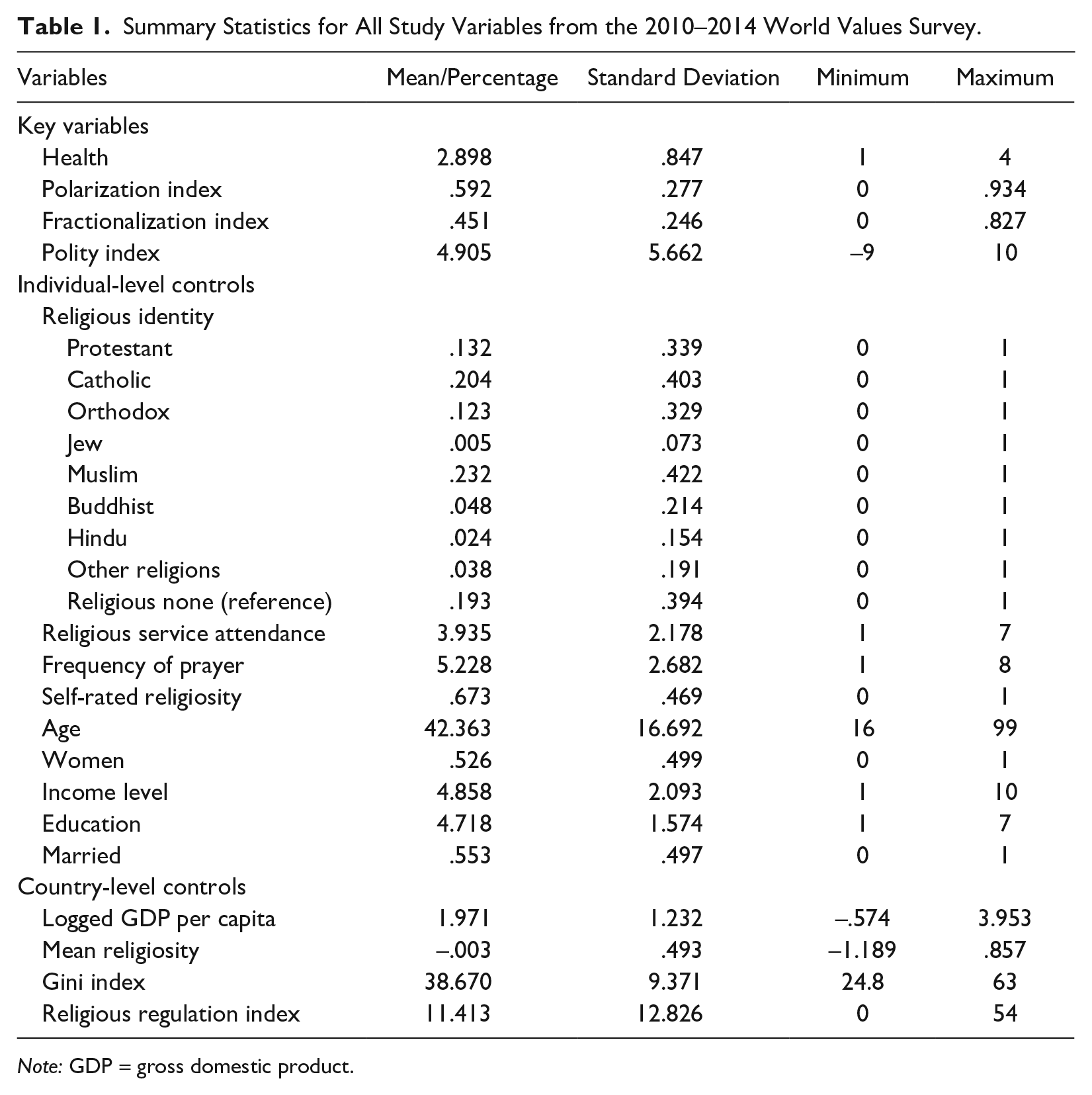
Note: GDP = gross domestic product.
Outcome Variable
Self-rated health has been demonstrated to be a valid and reliable assessment of individuals’ overall health status and has been widely used in previous research focusing on individuals’ health (e.g., Boardman 2004; Ferraro and Farmer 1999; Frankenberg and Jones 2004; Idler and Benyamini 1997; Jylhä 2009). In a review of self-reported measures of health, self-reports were found to exceed the predictability of physician assessment (Ferraro and Farmer 1999). The self-rated health question in the sixth wave of WVS was asked as, “How would you describe your state of health these days?” Reversed coded responses were (1) poor, (2) fair, (3) good, and (4) very good. We estimated multilevel linear and logistic regression models, respectively, for this health variable. This is because many studies examining self-rated health coded this question as a continuous variable (e.g., Hayward and Elliott 2014; Huijts and Kraaykamp 2011; Stavrova 2015), whereas others treated it as a binary variable (e.g., Idler and Benyamini 1997; Stroope and Baker 2018). We followed both approaches to code the health variable. The linear and logistic models produced substantively identical results. We report the linear model results as the main findings and then summarize the logistic results in Table B in the online version of the article. Second, we also estimated ordered logistic models that yielded identical results to the linear and the logistic models. However, we found that the proportional odds assumption was violated. Also, Zajacova and Dowd’s study (2011) showed that the test-retest reliability of ordinal measures of self-rated health is not ideal for U.S. adults. We thus decided to focus on the linear and logistic findings. The ordered logistic model findings can be provided on request.
Key Predictors
We followed widely used approaches in existing studies to measure religious fractionalization and polarization. Religious fractionalization is often measured with a variant of the Herfindahl index (e.g., Delhey and Newton 2005; Grim and Finke 2007). The formula for the fractionalization index is as follows:

where n refers to each group, and x is the proportion of each group per country. The index denotes the probability of two randomly selected individuals belonging to different groups. It ranges from 0 to 1, with higher values indicating higher levels of religious fractionalization. Although this index is extremely popular across disciplines, as a form of quadratic function, it has nonunique values when more than two groups exist. In practice, although this index does accurately reflect the level of fractionalization expressed as the chance of a random encounter, it cannot uniquely depict the relative sizes of all groups, a problem to be ameliorated by the polarization index in the following. For example, different configurations of three groups whose total sizes add up to 100% may result in close fractionalization scores: the configuration of 65%A + 18%B + 17%C and the configuration of 49%A + 49%B + 2%C yield similar fractionalization scores, around .48. However, the first scenario represents a low-fractionalization society with a dominant Group A (65%), whereas in the latter, Group A and Group B are evenly matched in size.
For the purpose of differentiating the landscape of religious diversity beyond fractionalization, we adopted the polarization index, initially proposed by Montalvo and Reynal-Querol (2005). The index of polarization is with the following form:

This index represents how far the distribution of the religious groups is from the (.5, 0, 0, . . . 0, .5) distribution, a bipolar demographic composition that is the highest level of polarization. The multiplier of 4 scales the summated scores to the highest point of 1. The polarization index ranges between 0 (lowest) and 1 (highest). With the polarization index and the fractionalization index simultaneously modeled, we could be more confident about both the substantive meaning and arithmetic comprehensiveness of contextual religious diversity.
We classified the respondents in the WVS into nine categories of religious identity: Protestant, Catholic, Orthodox, Muslim, Buddhist, Jew, Hindu, other, and religious none. 3 Using these nine categories, we calculated the size of each religious group per country based on the proportion of respondents and then produced the fractionalization and polarization indices. A comparison of religious composition across countries may illustrate the difference between the polarization and fractionalization indices. For example, the Kazakhstan sample consists of 51.1% Muslims, 26.6% Orthodox Christians, 20.2% with no religious affiliation, and 2% other small groups. There is a religious majority coexisting with a substantial-size minority. Based on the formulas presented previously, its composition is at a high level of polarization (.85) and at a medium level of fractionalization (.63). The case of Singapore is different. In this country, 26.8% of the respondents reported affiliating with Buddhism, 16.5% with Islam, 10.8% with Protestantism, 7.2% with Hinduism, 6.7% with Catholicism, .3% with Judaism, 12.6% with other religions, and 19.1% with no religious affiliation. For Singapore, the polarization index is medium (.55), but the fractionalization index is high (.83). In contrast to Kazakhstan and Singapore, all respondents from Tunisia were Muslims. The two indices are both 0 in this case.
To further clarify the association between the polarization and fractionalization indices, we made a scatter and linear-prediction plot for the indices with each country of our sample as a unit (see Figure 1). We conducted two separate linear regression predictions with the .5 polarization score as the cutoff point. As shown in Figure 1, the indices are positively correlated when they are at low levels (the left part of Figure 1). Because the population in each of the countries shown in the left part of Figure 1 is dominated by one religion, the fractionalization and polarization indices are both low. Nevertheless, the correlation becomes negative when the indices reach high levels (the right part of the graph). The countries with the highest polarization scores have intermediate levels of religious fractionalization.
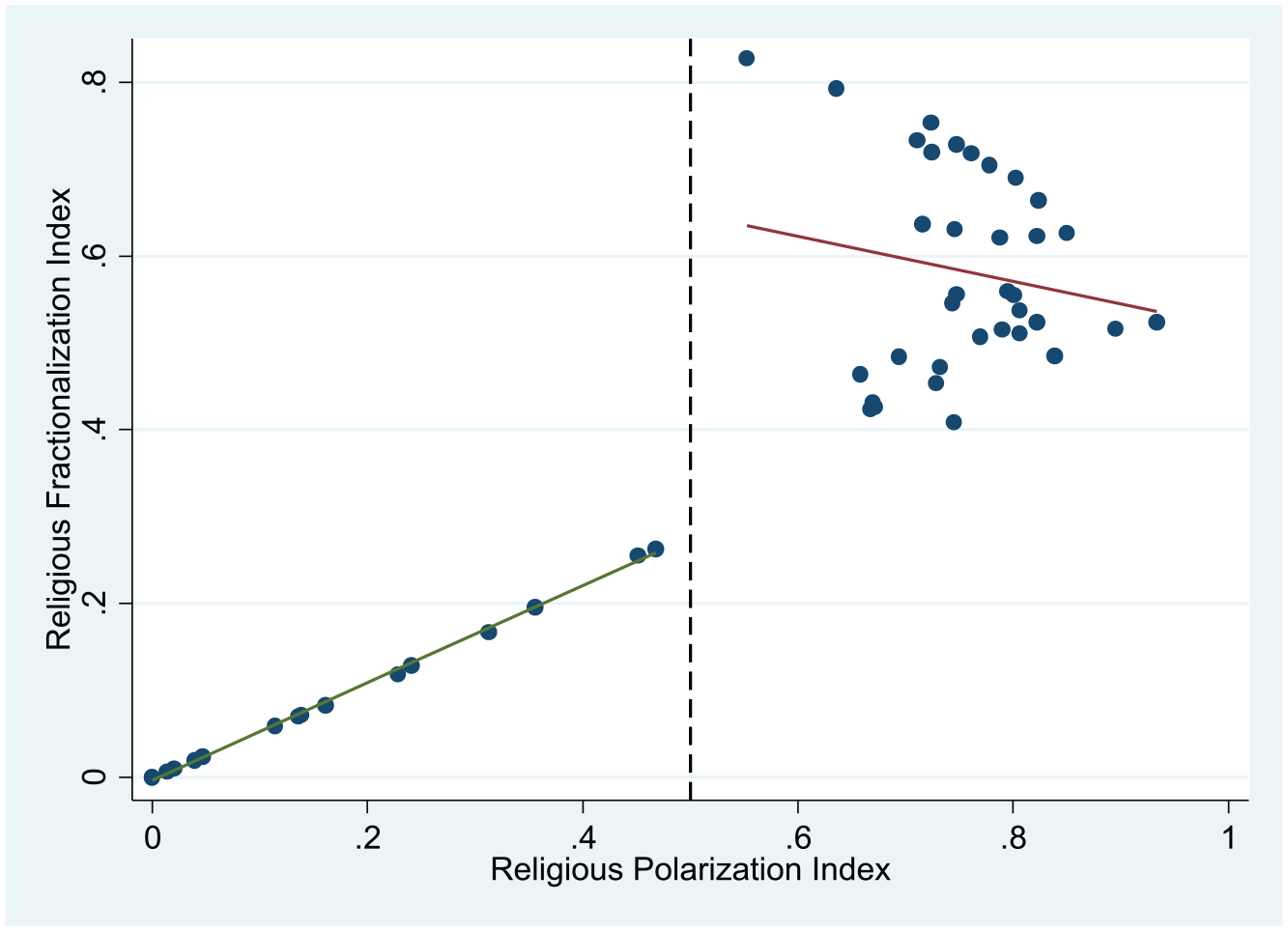
The Scatter and Linear Prediction Plot of the Religious Fractionalization and Polarization Indices.
We used the polity index from the Polity IV project to measure democracy in each country. Polity project data have been used widely in previous research (e.g., Muntaner et al. 2011; Schofer and Fourcade-Gourinchas 2001). This project provides annual measures for the authority characteristics of all states in the world for purposes of comparative and quantitative analysis. It accounts for the competitiveness of executive recruitment, the openness of executive recruitment, the constraints on the chief executive, and the competitiveness of political participation. The polity index ranges from −10 (strongly autocratic) to 10 (strongly democratic).
Control Variables
We controlled for common sociodemographic variables that were found to be associated with health (Deaton 2015; Elo 2009): age (coded in years), sex (women = 1, men = 0), marital status (married = 1, else = 0), educational degree (range, 1 = no formal education, 7 = university degree or above), and self-rated income level (range, 1 = lowest group, 10 = highest group).
To control for different dimensions of individual religiosity that are relevant to health (Fetzer 2003; Pew Research Center 2019; Stavrova 2015), we included religious service attendance (“Apart from weddings and funerals, about how often do you attend religious services these days?” Responses were reverse-coded from 1 = never to 7 = more than once a week), frequency of prayer (“Apart from weddings and funerals, about how often do you pray?” Reverse-coded responses ranged from 1 = never to 8 = several times a day), and self-rated religiosity (I am a religious person = 1, I am a nonreligious person/an atheist = 0) in the models. In addition, we also controlled for the nine categories of religious identity in the models.
In terms of country-level control variables, we added the natural log of 2010 gross domestic product per capita (in U.S. dollars) and the Gini index, which were both drawn from the World Bank data, because the associations between the economic factors and health indicators have been well documented in the literature (e.g., Cole 2018; Kelley and Evans 2017). Past works noted that country-level religiosity influences population health (Stavrova 2015; Stroope and Baker 2018). Therefore, we also controlled for this factor by calculating the country-level mean of standardized and combined religious service attendance, frequency of prayer, and self-rated religiosity. Previous research also found that religious regulation influenced the link between religion and health (Hayward and Elliott 2014; Hsieh 2017). To control for religious regulation, we used the religious regulation index from the Religion and State project (Fox 2008), a composite measure of government restrictions on formal religious organizations, public religious speech, access to places of worship, and other religious practices and institutions. The index ranges from 0 to 54, with higher scores indicating higher regulation levels.
Statistical Analysis and Missing Values
We used multilevel modeling to incorporate both individual- and country-level variables. In this study, individual respondents were nested within different countries. Using ordinary regression would violate the assumption that cases are independent of each other and therefore miscalculate the error. Multilevel modeling was thus appropriate for this study because it allowed for simultaneous consideration of errors clustered at multiple sampling frames.
A major source of missing data was that several study variables were missing for all respondents in nine countries. 4 Thus, the inclusion of these variables in the models would remove 11,417 individual cases from these countries, around 13.2% of the total sample. Additionally, there were 7,456 more missing cases in the remaining data, 8.6% of the total sample. We used two strategies to handle the missing data. The first was the listwise deletion of all the missing values, a common strategy adopted by most researchers who use the WVS data (e.g., Huijts and Kraaykamp 2011; Ruiter and de Graaf 2006). This resulted in an analytic sample of 67,399 cases, 51 country-level units. We report the model results based on this sample as our main findings (Table 2). The second strategy was a combination of listwise deletion and multiple imputation. We deleted the missing data from the nine countries. This part of missing data was presumably missing not at random. In other words, the missingness of the data did not depend on the observed cases. We then imputed the missing values in the remaining sample using the chained equation method. Following this widely practiced procedure, we excluded those observations with missing data on the dependent variable in estimating the models. The model results based on the imputed sample, which contained 74,574 cases, are presented in Table D in the online version of the article. As we discuss later, the results based on the listwise-deletion sample are consistent with the results obtained from the imputed data set.
Multilevel Linear Regression Models on Self-Rated Health from the 2010–2014 World Values Survey (Individual N = 67,399; Country N = 51).
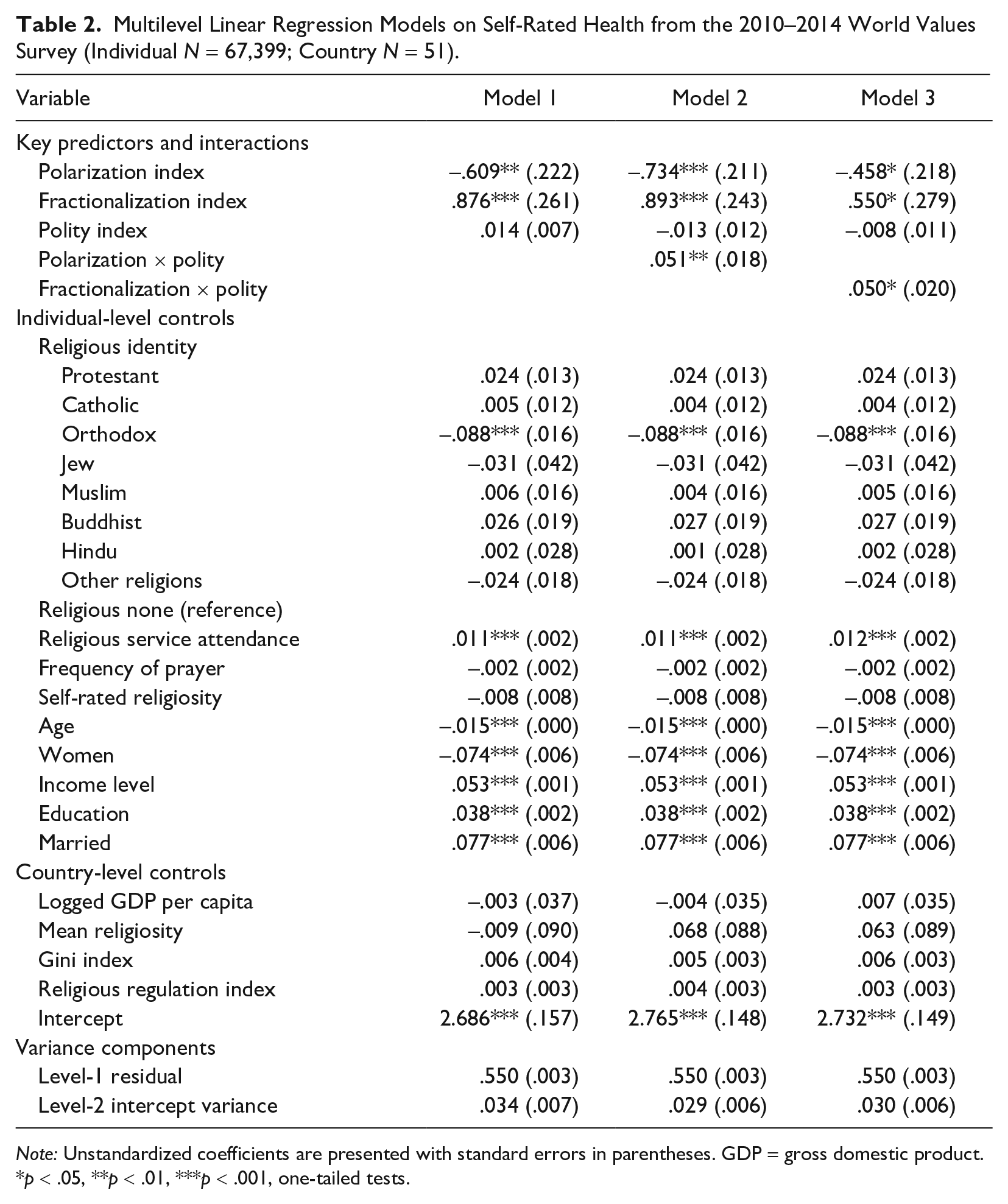
Note: Unstandardized coefficients are presented with standard errors in parentheses. GDP = gross domestic product.
p < .05, **p < .01, ***p < .001, one-tailed tests.
Results
Main Findings
We first ran an unconditional model without any covariates (not shown). The intraclass correlation is about .107. 5 This means that around 10.7% of the total variance in individual health can be attributed to between-country differences. Because there is substantial variation in individual health status across countries, it is appropriate to use the multilevel regression models to account for the between-country variance along with the within-country variance.
We included religious polarization and religious fractionalization in Model 1 in Table 2, adjusting for control variables. The polarization index is negatively associated with the health variable (β = −.609, SE = .222). This suggests that people living in societies with higher polarization levels tend to have poorer health. This finding lends support to Hypothesis 1, which expects a negative association between religious polarization and individual health. In terms of the fractionalization index, it is positively associated with self-rated health (β = .876, SE = .261). This finding suggests that people in more fractionalized societies report better health than those in less fractionalized societies, which is in line with Hypothesis 2. Religious diversity variables’ effect sizes look substantial when compared with other significant factors in the model, such as education (β = .038, SE = .002). For example, the health gap between one person who lives in a highly fractionalized society (1 SD above the mean) and another one who lives in a society with low fractionalization (1 SD below the mean) is .42 on a 4-point scale, other things being equal. For the education variable, the self-rated health of an individual with a university degree or above is .23 higher than that of those with no formal education, other things being equal.
We now move on to the interaction models. Model 2 estimated the interaction of the religious polarization index and the polity index and showed a significant interaction. Figure 2 plots this interplay with all control variables set at their respective means. As the polarization index increases, the predicted health level drops considerably for societies with a low polity score (1 SD below the mean), while it decreases slightly for societies with a high polity value (1 SD above the mean). This suggests that the adverse effects of religious polarization on individual health are less pronounced in countries with higher democratic levels. The dots in Figure 2 represent three countries with a unique combination of the polity index and the polarization index: Brazil (high polarization and high polity), Kazakhstan (high polarization and low polity), and Thailand (low polarization and middle polity). The predicted health of people living in Brazil is lower than that of Thailand yet higher than that of Kazakhstan. This result is in line with Hypothesis 3.
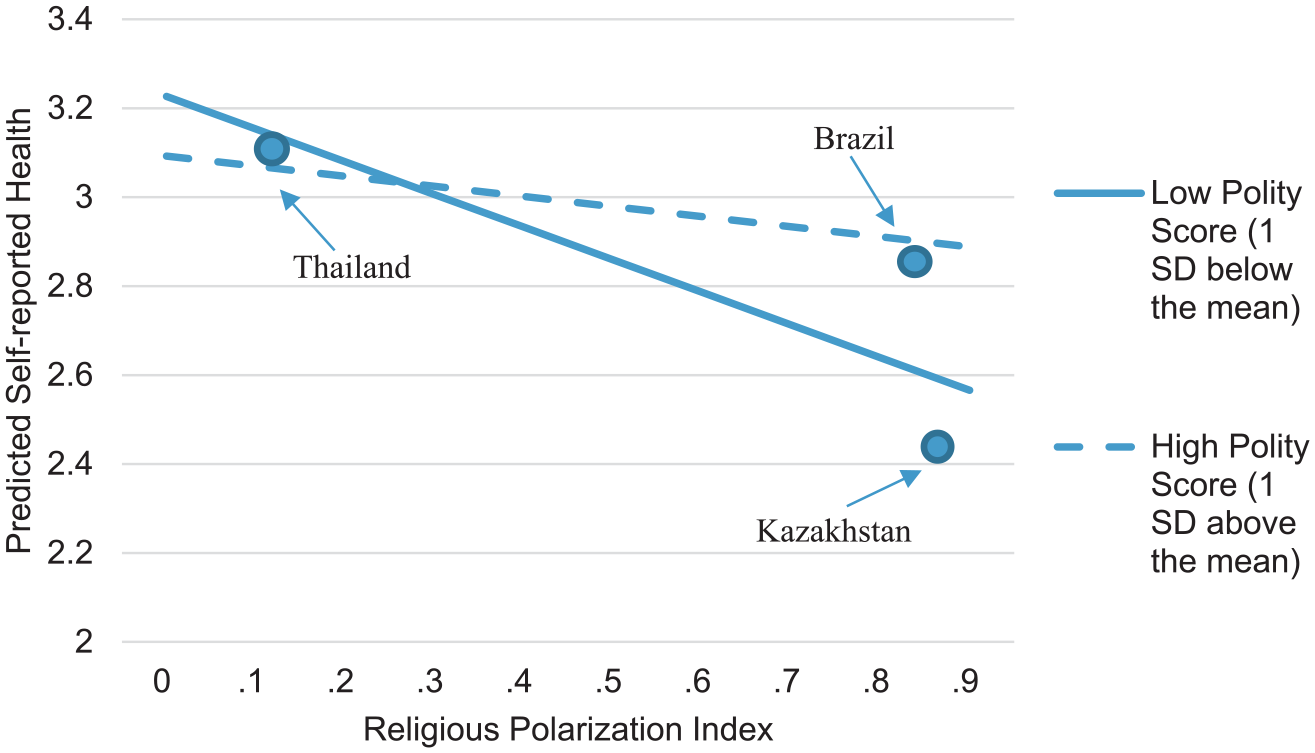
Predicted Interaction Effects of the Religious Polarization Index and the Polity Index.
Model 3 shows that the fractionalization index significantly interacts with the polity index. Figure 3 displays the predicted self-rated health level based on this interaction, with all control variables being set at their respective means. According to Figure 3, the predicted health level grows as the fractionalization index increases. For the societies with a higher polity score, the change in the predicted health level is more substantial. In addition, the three dots represent the United States (high fractionalization and high polity), Singapore (high fractionalization and low polity), and Romania (low fractionalization and high polity). Individuals in the United States have a higher predicted health level than those from Singapore and Romania. Overall, this finding offers evidence for Hypothesis 4, that the positive effects of religious fractionalization are stronger in more democratic countries.
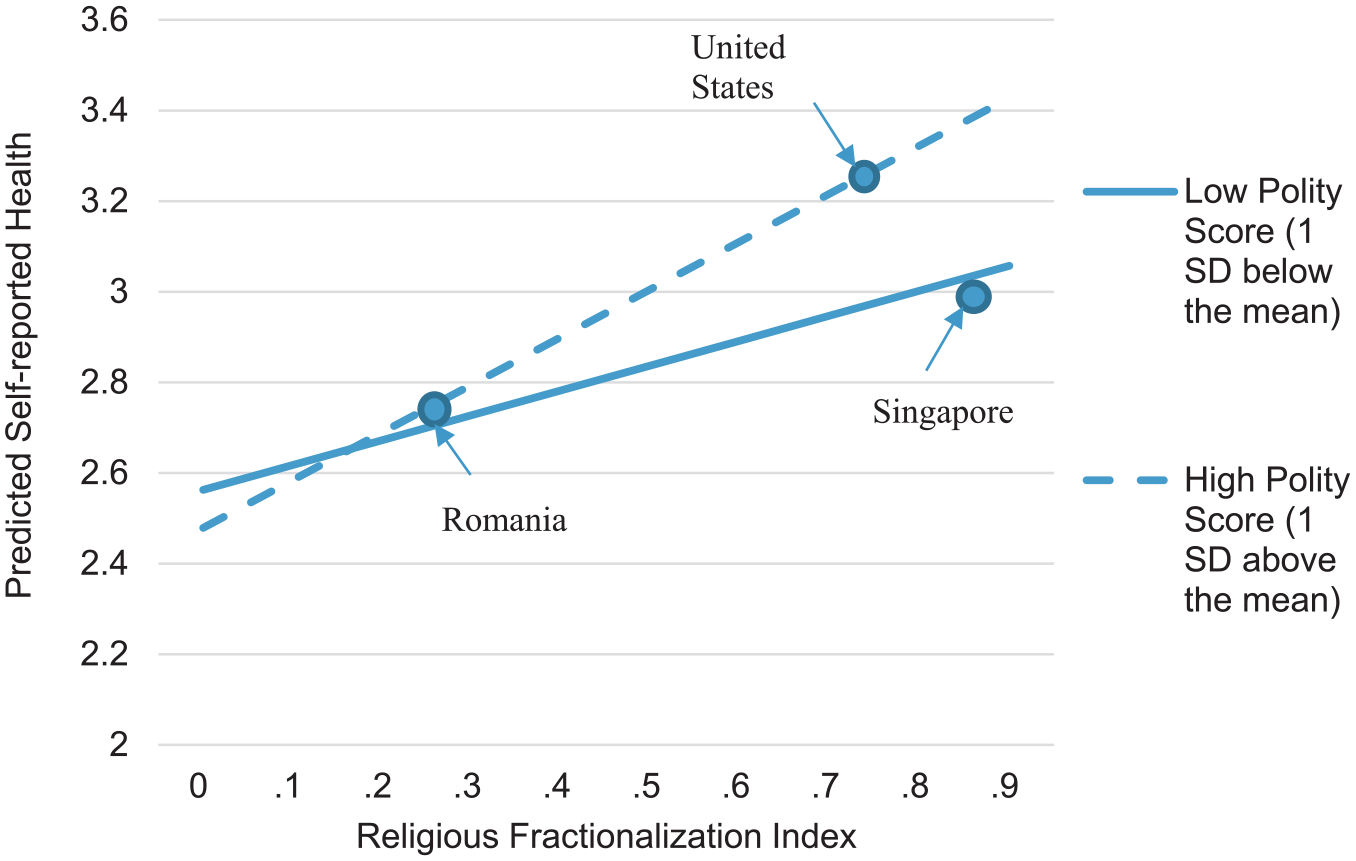
Predicted Interaction Effects of the Religious Fractionalization Index and the Polity Index.
Sensitivity and Additional Analysis
As we explained in the variable coding section, we conducted a sensitivity analysis by using a binary form of the self-reported health variable (very good/good = 1, poor/fair = 0). The multilevel logistic regression models (see Table B in the online version of the article) report similar results to the main findings in Table 2. This proves that the core findings of this study are robust across different approaches to address the outcome variable.
One may argue that ethnic diversity is closely related to religious diversity and thus is a potential confounder, although they are distinctive dimensions in demographic heterogeneity. The WVS data provide information on respondents’ ethnic background. The ethnicity question of the WVS is adjusted for each country. For U.S. respondents, for example, there were four categories: (1) non-Hispanic white, (2) black, (3) Hispanic, and (4) other. In Singapore’s sample, the ethnic categories were (1) Caucasian white; (2) South Asian Indian, Pakistan, and so on; (3) Chinese; (4) Malay; (5) Eurasian; and (6) other. We applied the diversity formulas and created the ethnic polarization and fractionalization scores for each society of the analytic sample. Our key findings still persisted in the models controlling for the ethnic diversity indices (see Table C in the online version of the article).
As we mentioned in the methodology section, we replicated the models based on the multiple-imputation sample. The core findings are consistent between the listwise-deletion models and the multiple-imputation models (see Table D in the online version of the article). This provides further evidence for the robustness of the findings.
Discussion
We investigated whether the diversity of a nation’s religious landscape shapes individuals’ general health and how the health effects of religious diversity vary across political contexts measured by the level of democracy. By combining individual survey data and national data with more than 67,000 respondents from 51 countries, we found that religious polarization has an adverse effect on individual health, whereas religious fractionalization is positively associated with individual health. The effect sizes of both the fractionalization and polarization indices are substantial compared with the other common socioeconomic factors of health. Moreover, we found that democracy moderates the relationships between religious polarization/fractionalization and individuals’ health. We demonstrated that the negative impacts of religious polarization are higher in countries with lower democratic levels, whereas the health benefits of religious fractionalization are higher in more democratic countries.
The present study has rich implications for the literature. First, this study advances the knowledge of how the religious context is related to individuals’ overall health. Previous studies in this area mainly focused on contextual religiosity and religious population share. What was overlooked in these studies is the growing heterogeneity of religious composition in many countries. To fill the gap in past works, we explored the nuances in the interrelationship between religious diversity and general health.
Moreover, this study is related to a heated discussion on religious diversity, social cohesion, and individual well-being. On one hand, religious diversity is often described as being erosive to shared societal norms and values or is suggested as a source of struggles (e.g., Huntington 1998; Putnam 2007; Stephan and Stephan 2000; Wuthnow 2005), thus having detrimental effects on health. On the other hand, religious diversity arguably inspires interreligious exchanges and motivates religious groups to be more cohesive (Page 2008; Trejo 2009; Yang and Ebaugh 2001), bringing forth more health benefits to individuals as a result. We consider the diversity-to-conflict argument and the diversity-to-solidarity argument as both limited and partially valid. The debate has failed to differentiate between polarization and fractionalization, two separate types of religious diversity with different meanings for individual health. In addition, the debate has not recognized that the relationship between religious diversity and health is contingent on democracy. As suggested by this study’s findings, the diversity-to-conflict argument is supported in high-polarization societies with weak democratic institutions, whereas the diversity-to-solidarity argument finds evidence in high-fractionalization societies with consolidated democratic institutions.
This study also extends a growing literature on the “dark side” of religion. Existing studies have already pointed out that religion is multifaceted and that some dimensions of religion are associated with poorer health. For example, a group of studies showed that religious people, on some occasions, experience psychological problems such as spiritual struggles, depression, and religious doubt (Ellison et al. 2013; Exline, Yali, and Sanderson 2000; Jasperse, Ward, and Jose 2012; Krause and Wulff 2004). Also, individuals who belong to a marginalized religion are exposed to cultural conflicts and thus are more likely to have depression (Hu et al. 2017). Differing from the individual- and micro-level perspective of these studies, the present study further shows how the polarized configuration of the religious composition may be adversely related to individual health.
Finally, our study adds to the health-and-politics literature and provides a new perspective for understanding how democratic institutions shape health outcomes. Human health is determined by factors at multiple ecological levels. A holistic and integrated understanding of health requires us to see the social processes that rendered micro-level physiological phenomena to emerge. The social support, networks, institutional resources, cultural membership, and material advantages, among other social factors, fundamentally determine the chances that we contract, get labeled and diagnosed, receive treatment for, and recover from illnesses. National contextual factors such as religious diversity and democracy reflect such underlying fundamental social processes. In the recent decade, the consequences of political factors—such as democracy, the welfare state, and women’s representation—on population health have become an emerging research area within health literature. In particular, scholars have found that democracy is health promoting. Moving beyond existing studies, in the present study, we find that democracy moderates the associations between religious diversity variables and individual health. Furthermore, we theorize that democratic institutions provide peaceful channels to address grievance and disputes, which help mitigate interreligious tension, and protect the freedom of association and speech, which allows religious groups to generate social capital.
There are some limitations to our study, which we welcome future research to address. First, we proposed several potential mechanisms underlying the associations between national religious diversity and individual health, but the data did not enable us to directly examine these mechanisms. Future multilevel research should assess these mechanisms when cross-national data sets provide needed information. Second, another limitation in our research involves the measurement equivalence of self-rated health. Although self-rated health proves to be a valid and effective measure, there are concerns that subjective measures for well-being may not share the same respondent understanding across cultures. To explore this issue, several studies found that most well-being measures are invariant across cultures, but they also noted that caution is necessary when conducting cross-cultural comparative research (Bieda et al. 2017; Tov and Diener 2007; Veenhoven 2012). These studies have provided supportive evidence for the cross-national equivalence of the self-rated health measure. Nevertheless, we acknowledge that there may be unrecognized measurement problems in our data and encourage additional qualitative research to explore this issue. Third, as noted by Lim and MacGregor’s (2012) and Stroope and Baker’s (2018) studies, there may be a problem in the link between macro-level religious context and micro-level interaction between different groups. In a country where the nation-level religious fractionalization is high, it is possible that each religious group is spatially segregated from others. In this case, religious fractionalization at nation-level may not increase micro-level daily interaction across group boundaries. Future research can further contribute to the understanding of health and religious diversity by using subnational-level data.
Although some unsolved issues remain, our research contributes to the knowledge of religious context and health. This study shows that the religious composition of a society is related to the general health of individuals and that democratic institutions are important in shaping the religion-health link. These findings move beyond prior studies by showing that a full understanding of the religion-health relationship needs to consider the nature of the local religious composition. More broadly, early theorists such as Weber (1948) and Durkheim ([1897] 2008) pointed out that religious beliefs, activities, and institutions were deeply shaped by social contexts. Following these theories, recent scientific studies of religion have paid closer attention to how the social outcomes of religion—such as trust, voluntary work, and civic engagement—are contingent on the national context (e.g., Lu, Jung, and Bauldry 2019; Olson and Li 2015). Extending this line of research, our study further shows that the religion-health link depends on the political context.
Supplemental Material
Supplemental_Material – Supplemental material for The Two Faces of Diversity: The Relationships between Religious Polarization, Religious Fractionalization, and Self-rated Health
Supplemental material, Supplemental_Material for The Two Faces of Diversity: The Relationships between Religious Polarization, Religious Fractionalization, and Self-rated Health by Yun Lu and Xiaozhao Y. Yang in Journal of Health and Social Behavior
Footnotes
Supplemental Material
Tables A through D are available in the online version of the article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Junior Scholar Project of the Ministry of Education of the People’s Republic of China “Political Islam and Perception of China in Belt and Road Countries” (18YJC840024).
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.