
Abstract
Existing research on the life course origins of adult health has extensively examined the influence of childhood socioeconomic conditions, family structure, and exposure to trauma. Left unexplored are the potential long-term health effects of sociocultural exposures, such as religiosity at earlier phases of the life course. Integrating life course models of health with literature on the health-protective effects of adult religiosity, we consider how adolescent and midlife religiosity combine to structure the physical health profiles of adults past age 50. Using more than 35 years of representative data from the National Longitudinal Survey of Youth 79 (NLSY79), we found that the stability of frequent religious practice over time was associated with better health composite scores and lower disease burden. Causal mediation analyses revealed that part of this association is driven by a lower risk of smoking for consistent, frequent attenders. Adulthood religiosity also mediated the relationship between frequent early-life religious attendance and health.
One of the most widely replicated findings over the past several decades in the sociology of health is that frequent religious attendance is linked to a vast array of favorable outcomes, including self-reported physical health, low chronic disease burden, and delayed mortality (Hummer et al. 2010; VanderWeele 2017). The association between attendance and health has been documented in regional and nationally representative samples from the United States and beyond (Hummer et al. 2010; Nicholson, Rose, and Bobak 2009), in studies representative of general communities (Oman et al. 2002), and among ethnic-specific samples (Hill et al. 2005). It has likewise been found among diverse age groups, including adolescents and young adults (Kirk and Lewis 2013), the middle-aged (Hummer et al. 2010), and the oldest-old (Lawler-Row and Elliott 2009). Yet despite comprehensive attention to each of these separate age categories, studies of religion and health have largely ignored the process of aging and how religious attendance from different stages of life matter over the long term.
Although a comprehensive life course understanding of religion and health is not yet established, literature on the “long arm of childhood”—particularly the long-term effects of early socioeconomic disadvantage, family structure, and trauma—has been a topic of great interest (Ferraro, Schafer, and Wilkinson 2016). Indeed, events or conditions affecting social, cognitive, and emotional development during early years of life are now known to have profound implications on later-life health. To some extent, this may operate directly through physiological developmental mechanisms (Berens, Jensen, and Nelson 2017). However, there is also compelling evidence that childhood exposures sort individuals into distinctive life course pathways that carry their own risks and resources and ultimately affect adult health (Pudrovska and Anikputa 2014; Willson and Shuey 2016). The bottom line of research on the long arm of childhood is that “people are never completely separated from the imprint of their origins” (Pearlin 2010:212). Although this is well understood in the context of conditions such as socioeconomic advantage or disadvantage, surprisingly few studies have investigated the role of early sociocultural exposures such as religious participation.
The goal of this study is to apply life course models of health, particularly pathway and mobility perspectives, to the case of religious attendance as an early-life exposure. Religious attendance shows a strong connection to good health in cross-sectional or short-term longitudinal designs, but does an early dose have long-term consequences? We also consider whether distinct patterns of religious mobility from adolescence to early middle-age are linked to health, paying special attention to health behaviors as a life course pathway to explain the potential benefits of consistently high and/or increasing religiosity. Using more than 35 years of data from the National Longitudinal Survey of Youth (NLSY79), this is the first study to prospectively document how adolescent and midlife religiosity combine to structure the physical health profiles of adults past age 50.
Background
Life Course Models of Health
The life course perspective provides an analytic framework to undertake this more expansive analysis of religion and health. This perspective emphasizes the importance of early life for later health outcomes while drawing attention to the modifiability of life experiences through transitions (Pudrovska and Anikputa 2014; Willson and Shuey 2016). Most research exploring the connections between early life and later life outcomes focuses on socioeconomic exposures and mobility while ignoring patterns of religious continuity and change (Willson, Shuey, and Elder 2007).
Life course models of health tend to emphasize either the role of direct, enduring effects from childhood or the ways in which childhood conditions affect health through—or in combination with—intervening adulthood circumstances (Pudrovska and Anikputa 2014; Willson and Shuey 2016). We focus on the pathway and mobility processes in the life course because religion is acknowledged to have indirect effects on health (Koenig, King, and Carson 2012).
Continuity and Change in Religiosity from Adolescence to Young Adulthood
Viewing religiosity through the respective lenses of the life course pathway and social mobility models involves assessing how individuals gain, lose, or hold steady in their religious behaviors over time. Children raised in religious households tend to remain religiously involved into adulthood (Upenieks, Schafer, and Mogosanu 2019). In early childhood and adolescence, parents influence the religious orientations of their children by attending religious services with them and stressing religious values in the home (Min, Silverstein, and Gruenewald 2018). Recent evidence suggests that almost two thirds of children who grow up attending church at least weekly go on to be regular attenders as adults (Bengtson 2013).
Despite these strong rates of intergenerational religious transmission, religious pathways are far from deterministic (Hardie, Pearce, and Denton 2016). Typically, decreases in religiosity occur as individuals progress from adolescence into adulthood (Uecker, Regnerus, and Vaaler 2007). This overall pattern of decline is more strongly pronounced for religious service attendance than for other dimensions of religiosity, such as religious salience (Uecker et al. 2007). Reasons for declines in religiosity are no doubt complex. One explanation is that many young people fail to fully embrace the faith of their forebears. Once they have left the parental home, these adults may lose interest in attending church (Pearce and Haynie 2004). Another explanation relates to health behaviors. Young adults engaging in behaviors that are stigmatized by their religious group (e.g., sexual activity or alcohol or tobacco use) may be socially disqualified or rejected (Adamczyk 2009).
Meanwhile, increases in religious attendance over the life course are often documented among those who transition into marriage and parenting roles (Schleifer and Chaves 2017; Uecker, Mayrl, and Stroope 2016). Married couples may return to religious communities to seek religious teachings that could strengthen their marriage by giving it a spiritual purpose (Mahoney 2010). New parents, for their part, may want their child to receive religious training and often increase their own religiosity in the process. Furthermore, individuals that intensify their religiosity over time often do so to gain meaning in life and to have a resource for coping with loss or stress (Silverstein and Bengtson 2018).
The extensive body of literature on religious attendance and health has thus far not assessed when religious exposure matters for mid- and later-life health: Does early religiosity still matter even for those who fall away from formal participation? Likewise, we have limited knowledge about how continued exposure to religious participation is connected to health.
Religious Pathways to Midlife Health
Multiple mechanisms have been suggested to explain the well-established connection between adult religious attendance and better health (Koenig et al. 2012). These include the availability of social support from members of religious congregations (Krause 2006), better health behaviors (Hummer et al. 2010), and greater meaning in life (Park 2005). Given the multifarious benefits linked to adult religious attendance, we argue that adult attendance mediates the effects of early religious exposure on health. Pathway models “emphasize that the effects of earlier exposures are mediated by later exposures” (Pudrovska and Anikputa 2014:452). Therefore, benefits of early-life religious exposure may become manifest later in the life course by increasing the likelihood of continued religious practice. In other words, we argue that early religiosity is the more fundamental cause of good health, whereas adult religiosity operates as a downstream, intervening variable. To our knowledge, this mediation framework, although a mainstay in research on socioeconomic conditions, has yet to be tested with respect to religiosity.
Hypothesis 1: Childhood religiosity affects midlife health through adult religiosity.
Religious Mobility and Health Over the Life Course
The social mobility model recognizes the importance of conditions early in the life course for promoting access to resources and avoidance of risks but also acknowledges that the effects of early conditions on health can be altered, reversed, or exacerbated by future circumstances (Pudrovska and Anikputa 2014; Willson and Shuey 2016). The religious mobility model thus argues that it is the unique patterning of adolescent and midlife religiosity that matters for health. We see this as a complementary—not contradictory—model to the life course pathway model because effects of religious transitions and/or stability could themselves be mediated by subsequent intervening mechanisms.
Existing literature suggests that high, stable religious attendance is optimal for midlife health. First, people’s health behavioral habits are often solidified in their late adolescence and early adult years. Children learn norms about health behavior during the early stages of life (Kim-Spoon et al. 2014) but typically come to fully own these habits once they leave the parental home (Guo and Metcalfe 2019). Accordingly, religious attendance appears to have a cumulative effect throughout adolescence and young adulthood such that stable, frequent attendance during this period reduces the risk of negative health behaviors, including smoking and heavy drinking (Chen and VanderWeele 2018; Desmond, Morgan, and Kikuchi 2010; Guo and Metcalfe 2019). Consistent participation in formal religious activities connects individuals to a community of believers who may encourage less risky coping mechanisms to deal with stress and who may impose sanctions on those who violate health norms (Koenig et al. 2012). Comparisons of the influence of religiosity on substance use across the transition to adulthood suggest that the protective effect of religiosity is stronger in early adulthood than adolescence (Freeman 2019). By early adulthood, religious individuals appear to have fully understood and internalized religious requirements to treat the body as a “sacred” instrument to be used in service to God. These attitudes have been linked to healthier behavior (see Mahoney et al. 2003).
The developmental importance of young adulthood also implies that increasing levels of religious attendance are linked to health behaviors and long-term health. Past research found that increased religious attendance was also associated with nonuse (Desmond, Ulmer, and Bader 2013) as well as desisted and nonpersistent use of substances such as alcohol (Guo and Metcalfe 2019; Ulmer et al. 2012). In this scenario, health behaviors may play a key role in how individuals negotiate their religious identities. A deliberate increase in religious attendance may signify an acceptance of religious directives, such as to “treat one’s body as a temple,” and promote abstinence from, or lower usage of, risky substances.
The corollary to the anticipated benefits of stable or increasing religious attendance is that individuals decreasing their religious attendance will experience relatively worse health behaviors, precipitating worse later-life health. Health behaviors likely inform individuals’ decision to leave organized religion. For instance, adolescents who decrease their religious involvement over time, relative to stable attenders, are more likely to initiate alcohol and other forms of substance use (Guo and Metcalfe 2019; Ulmer et al. 2012). One implication of these findings is that early-life religious exposure is not sufficient to directly shape health behaviors throughout the life course. We might therefore expect the health of those who decline in religious attendance to be on par with those who are stably nonattenders.
Although informative, this past research on changes in religious participation and health behaviors over time has been plagued by a few limitations. First, most studies have been conducted on nonrepresentative samples, such as predominantly white and highly educated women in the Nurses’ Health Study (Chen and VanderWeele 2018; Li, Stampfer, et al. 2016). Second, existing work has only captured religious attendance and health behaviors at a very limited window of time, usually during the period from adolescence to young adulthood (Desmond, Morgan, and Kikuchi 2010; Guo and Metcalfe 2019), thus limiting the knowledge of how changes in religious attendance affect health behaviors during midlife and beyond.
Hypothesis 2: Consistently high and/or increasing religiosity from adolescence to early middle age is associated with better adult health behaviors (smoking and drinking) than is consistently low and/or decreasing religiosity.
Hypothesis 3: Effects of consistently high and/or increasing religiosity are mediated through health behaviors (smoking and drinking) ensuing throughout adulthood.
These hypotheses are novel because, to our knowledge, no prior study has used nationally representative data to track individuals’ religious lives from adolescence to midlife and measured health once respondents were age 50 or older. This is an important oversight because health behaviors may coevolve with religious behavior over time. Thus, there is a crucial need for research spanning a greater portion of the life course. Figure 1 displays a visual representation of our conceptual model and hypotheses.
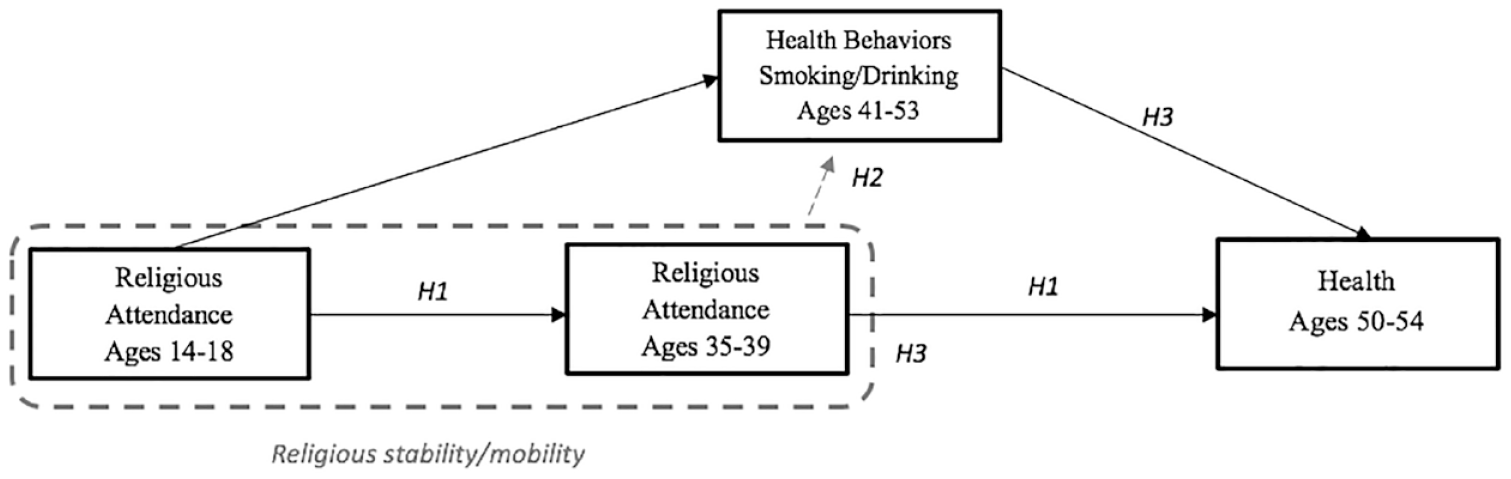
Conceptual Model of Religion and Health over the Life Course
Data and Methods
Sample
Data came from the National Longitudinal Survey of Youth. The NLSY79 originally comprised a sample of 12,686 men and women born between 1957 and 1964 who were living in the United States when the survey began. Interviews were conducted either face-to-face or by telephone. When first interviewed in 1979, respondents were between 14 and 22 years old. In this study, we restricted the sample to those respondents who were between the ages of 14 and 18 in 1979. 1 This age range captured only those who were adolescents and presumably remained in the parental home rather than those past the age of legal adulthood who had likely transitioned to college or into the labor force. We assume that young people’s religious attendance is relatively less voluntary at this stage of life, and so imposing this sample restriction provided the most accurate depiction of religiosity in the household of origin. Survey respondents were interviewed every year between 1979 and 1994 and every other year since 1994. The 2014–2015 wave marked the 26th round of data collection, with respondents ages 50 to 58.
Dependent Variables
This study used two measures of health as outcome variables. First, we employed a subscale of the SF-12 Health Composite Score (Ware, Kosinski, and Keller 1998). This was measured in the 2014–2015 wave of the NLSY79 when respondents were between 50 and 58 years of age. We used the Physical Component Summary subscale of the SF-12. Respondents were asked questions about their physical functioning (e.g., the ability to perform moderate activities), limitations due to physical problems, physical pain (e.g., interfering with work), and general health perception (poor, fair, good, very good, or excellent). Appendix A in the online version of the article contains a list of items that comprise this measure. Scores were normed with a mean of 50, ranged from 0 to 75, and had a standard deviation of 10 (Ware et al. 1998). Higher scores on this scale indicated better health.
As a second measure of health, we included a count of self-reported chronic health conditions. This information was also collected in 2014–2015. At this survey wave, respondents were asked whether a medical professional had ever diagnosed them with the following six health conditions: high blood pressure, diabetes, cancer, lung problems, heart problems, and stroke. We created a count variable ranging from zero (no chronic conditions) to six (all chronic conditions).
Focal Independent Variable: Religious Attendance
Religious attendance was measured at two time points in the NLSY79: in 1979 (baseline), when the study respondents in our sample were between 14 and 18 years old, and again in 2000, when study respondents were between 35 and 39 years old. Respondents were asked, “In this past year, about how often have you attended religious services?” To ensure reasonably large categories, we modeled religious service attendance as a three-category variable: low/no religious attendance (not at all and several times a year or less), moderate religious attendance (once per month and two to three times per month), and high attendance (once per week and more than once per week).
To measure religious mobility, we created a nine-category variable that captured all possible transitions from one attendance category in 1979 to another attendance category in 2000. This span of 21 years was long enough to encompass the full transition to adulthood and caught participants at the onset of middle age.
Mediating Variables: Health Behaviors
We included two measures of health behaviors in our analysis. Recall that health behaviors were posited as potential mechanisms to explain the effects of religious practice stability/transitions on later-life health. The first was a cumulative measure of smoking. At four time points in the NLSY79 study (2008, 2010, 2012, and 2014), respondents were asked about the frequency with which they smoked over the last year (0 = none, 1 = fewer than 10 cigarettes per day, 2 = more than 10 but fewer than 20 cigarettes per day, 3 = more than 20 but fewer than 30 cigarettes per day, 4 = more than 30 but fewer than 40 cigarettes per day, 5 = more than 40 but fewer than 50 cigarettes per day, and 6 = more than 60 cigarettes per day). Across these four measurement years, we took the average score for respondents on this variable to create a cumulative measure of smoking (M = 2.70, SD = 2.54, α = .93). 2
In a similar fashion, we also created a cumulative measure of heavy drinking. This was measured at five time points during the NLSY79 study (2006, 2008, 2010, 2012, and 2014). Respondents were asked, “How often have you had 6 or more drinks on one occasion during the last 30 days?” (0 = never in the last 30 days, 1 = less often than once a week, 2 = 1 or 2 times per week, 3 = 3 or 4 times per week, 4 = 5 or 6 times per week, 5 = every day). 3 As with smoking, we created a cumulative measure of drinking by taking an average of the scores for each respondent across the five time points (M = .46, SD = .77, α = .86).
All available measures of smoking and drinking in the NLSY79 come after 1979 and 2000. Because smoking and drinking are proposed mechanisms for why consistently high religious attendance may promote better health later in the life course, it was crucial that they be measured after both measurements of religion (2000) but before the measurement of health (2014–2015).
Additional Covariates
Several additional covariates are included in the analyses, grouped into three categories.
Demographic covariates
Gender was coded as 1 = female, 0 = male. Race was coded as white (reference), black, and Hispanic. Age was captured in 2014–2015, when respondents were between 50 and 54 years of age.
Childhood covariates
Childhood socioeconomic status (SES) was measured at the 1979 survey by education level (reference = less than high school) and work status of the household head (1 = working for pay, 0 = not working). Additional analyses also considered childhood family income in 1979. Results were robust to the inclusion of this variable, but we ultimately removed it from final models because of high amounts of missing data and because it was highly correlated with parental education and work status. Parental abuse and affection were both retrospectively measured in 2014–2015, when respondents were asked how often a parent or adult in your home “ever hit, beat, kick, or physically harm you in any way” (0 = never, 1 = once, 2 = more than once). Parental affection was coded from 0 = no parental affection to 3 = a great deal. We also include a retrospective measure of childhood health, measured in 2014 (1 = poor, 5 = excellent). A variable for parental family structure contrasted those in two-parent homes with those with at least one stepparent, a single parent, or another type of family arrangement. We also adjusted for the number of siblings a respondent had, whether the respondent was born in the United States (1 = yes, 0 = no), and child residence type (town or city [reference], in country, not on farm, and on farm or ranch). We also considered whether the respondent lived in the American South (1 = yes, 0 = no) because religious norms tend to be stronger in this region of the country.
Analyses also featured a measure of respondents’ religious affiliation early in the life course (1979). We contrasted those reporting no religious affiliation with nondenominational Protestant, Baptist, Methodist, Presbyterian, Roman Catholic, Jewish, and conservative Protestant religious affiliations.
Adulthood achieved covariates
Finally, selected analyses also adjusted for several achieved adulthood characteristics. These included the respondent’s education, measured in 2000, at the same time point as the second measure of religious attendance (0 = less than high school, 1 = high school, 2 = some college, 3 = college degree, 4 = more than a college degree). At the 2014–2015 interview, respondents were asked for a complete marital history up to that point. We created a variable that contrasted those who had been stably married throughout their lives (reference group) with those who had been married twice, those who had been married more than two times, and those who have never married in their lives. For descriptive statistics for all study variables, see Appendix B in the online version of the article.
In the interest of a parsimonious presentation of results, we do not show the results pertaining to these controls in our main tables. However, these can be found in Appendix C in the online version of the article (for models pertaining to SF-12 health composite scores) and Appendix D in the online version of the article (for models relevant to health conditions).
Analytic Plan
Ordinary least squares regression analysis with robust standard errors was conducted to assess the impact of religiosity on health composite scores. Because chronic health conditions formed a count variable (with 64% of the sample reporting no chronic conditions), a series of different count models was used. Likelihood ratio tests showed that negative binomial regression models fit the data best compared with both Poisson regression and a zero-inflated regression model. Multiple imputation with chained equations was used (m = 20) to deal with missing data in all regression analyses. To produce consistent samples across the two dependent variables, we did not impute values for those missing on either of the dependent variables (SF-12 health composite score and chronic health conditions; see Von Hippel 2007). This yielded a final analytic sample of 3,609 cases. Results were also consistent using the listwise deletion method for addressing missing data.
Mediation analyses were conducted using parametric mediation (using the paramed command in Stata 14; Emsley and Liu 2013). Parametric mediation extends the traditional Baron and Kenny (1986) mediation procedure and uses counterfactual definitions of direct and indirect effects. Estimates from two parametric regression models were used to construct the controlled direct effect, the natural direct effect, and the natural indirect effect, the latter of which is the focus of typical mediation analyses. The natural indirect effect is calculated with respect to each mediator, conditional on the measured covariates (see Valeri and VanderWeele 2013). The natural indirect effect assumes that exposure is set to some level a and then compares what would have happened if the mediator were set to an alternative value a*. Moreover, 95% confidence intervals were calculated using the default delta method after verification that results using bootstrapped intervals were essentially identical. According to Valeri and VanderWeele (2013), the estimates will take a causal interpretation only in the absence of any residual confounding.
We also applied inverse-probability-of-attrition weights to all analyses to adjust for sample attrition. Following a previous study using identical waves of the NLSY79 (Kerr et al. 2018), we included the following predictors to construct the weights: age, gender, ethnicity, whether the respondent was a U.S. citizen, the region of the country the respondent was raised in, parent’s education, parental work status, childhood family structure, and childhood parental abuse. We also note here that all parametric mediation analyses were performed on unweighted NLSY79 data. Currently, survey weights are not supported within the paramed command in Stata. As a result of this difference, the coefficients representing the total effects differ slightly from our main analyses compared with our mediation analyses.
Results
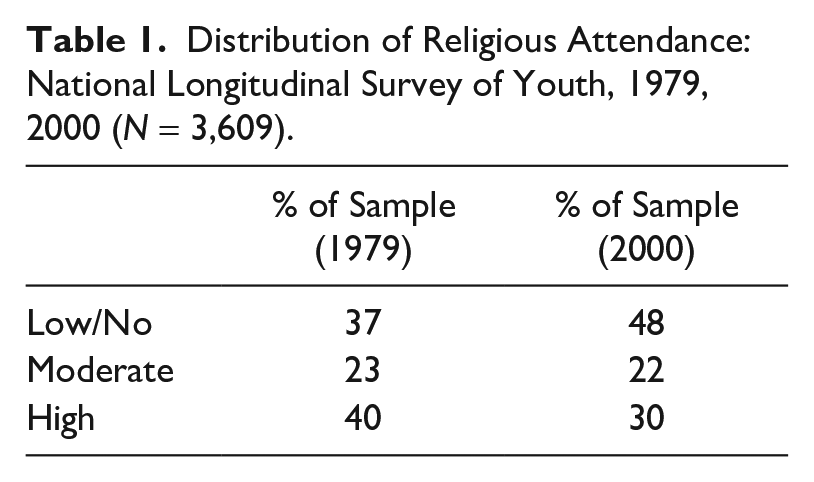
Table 1 shows the distribution of religious attendance in 1979 and again in 2000. Just over one in five respondents fell in the moderate attendance category both as adolescents and as adults in their mid-30s. Change was considerable, however, at high and low frequencies of attendance. In 1979, high attendance was most commonly reported (40%), followed by low/no attendance (37%). By 2000, this pattern reverses, and nearly half the sample reported low/no attendance, whereas only 30% reported high attendance.
Distribution of Religious Attendance: National Longitudinal Survey of Youth, 1979, 2000 (N = 3,609).
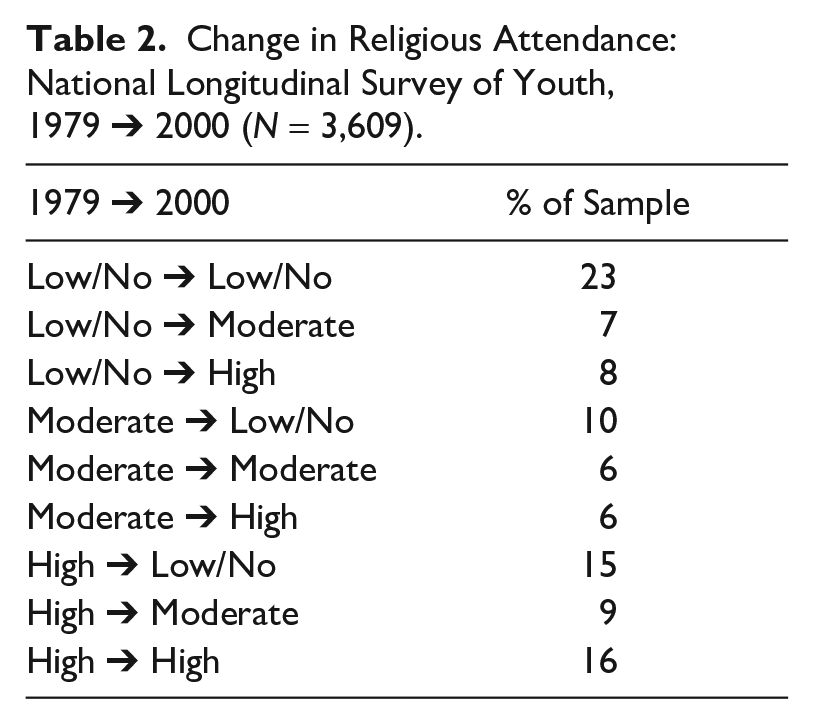
Although informative, the overall attendance distributions at two points in time mask person-level transitions in which individual respondents maintain, increase, or downshift their religious practice. Table 2 displays the frequency of each transition category between adolescence and early middle age. The two most common categories reflect religious stability, with 23% of the sample remaining nonattenders and 16% remaining frequent attenders. Stable moderate attendance, however, was a far less common experience (6% of the sample). Nearly one in six respondents dropped all the way from high to low/no attendance, although increases in religious attendance were also observed. Indeed, 15% of the sample moved from low/no attendance to the medium or to high categories, whereas an additional 6% of the sample underwent a transition from medium to high attendance.
Change in Religious Attendance: National Longitudinal Survey of Youth, 1979 ➔ 2000 (N = 3,609).
Results from ordinary least squares (OLS) regression analysis are displayed in Table 3 as unstandardized regression coefficients for health composite scores. Results from negative binomial models for predicting chronic health conditions are displayed in Table 4 as incident risk ratios (IRR). Because the same modeling strategy was applied to each outcome variable, we discuss results for each model pertaining to both health composite score and chronic health conditions.
Ordinary Least Squares Regressions Results Predicting SF-12 Health Composite Scores, National Longitudinal Survey of Youth (N = 3,609).
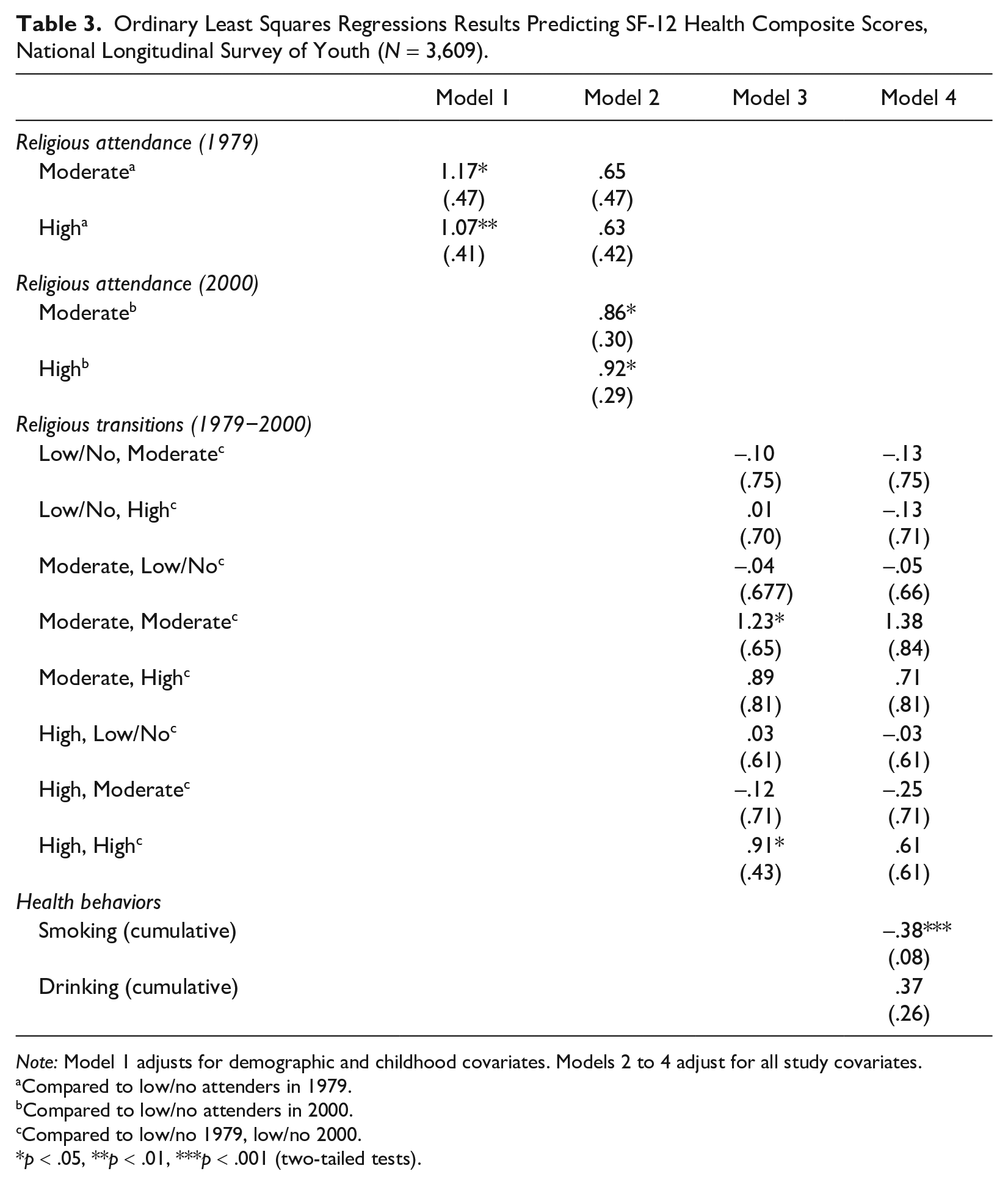
Note: Model 1 adjusts for demographic and childhood covariates. Models 2 to 4 adjust for all study covariates.
Compared to low/no attenders in 1979.
Compared to low/no attenders in 2000.
Compared to low/no 1979, low/no 2000.
p < .05, **p < .01, ***p < .001 (two-tailed tests).
Negative Binomial Regressions Results Predicting Count of Chronic Health Conditions, National Longitudinal Survey of Youth (N = 3,609; Incident Risk Ratios Shown, with 95% Confidence Intervals).
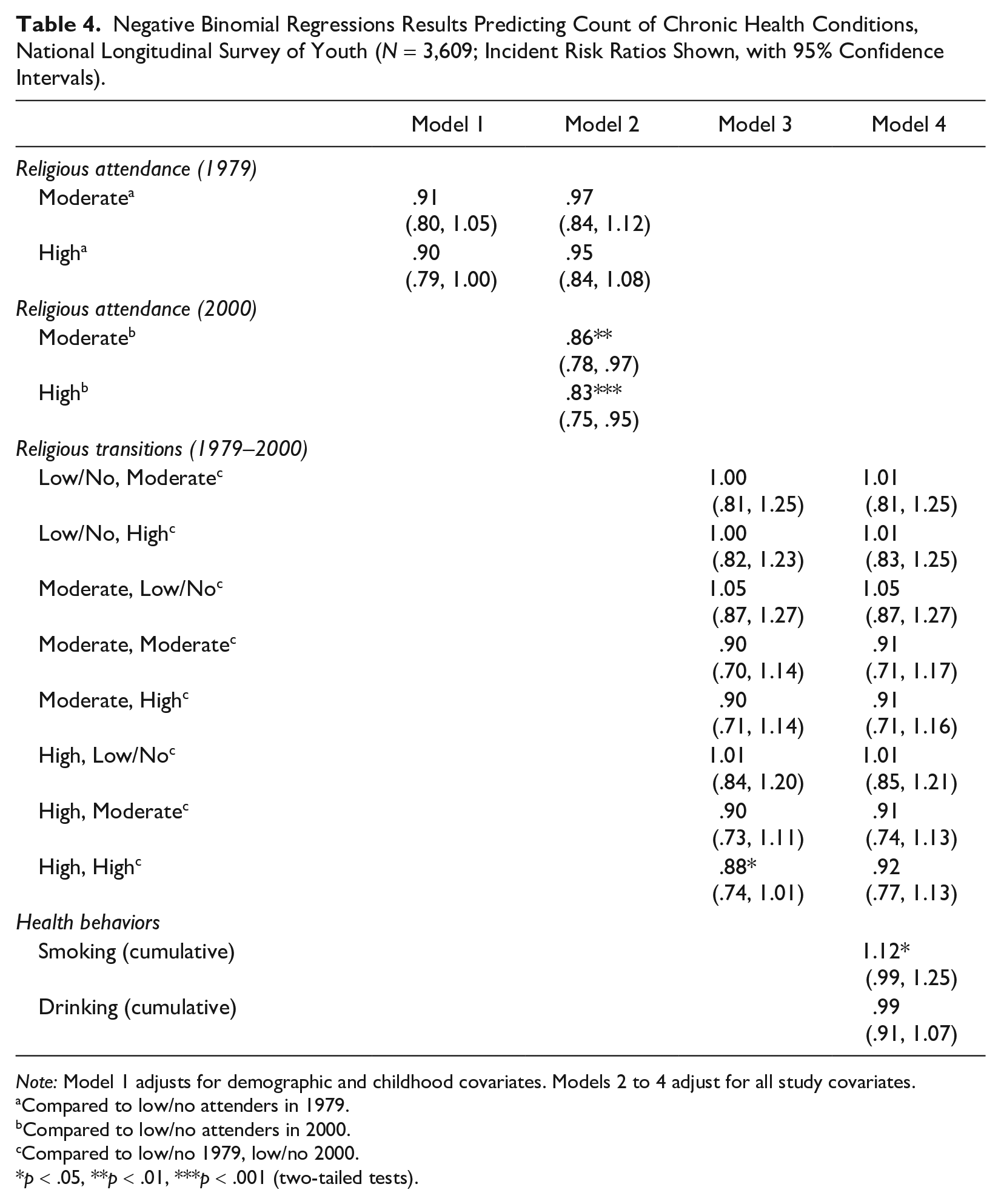
Note: Model 1 adjusts for demographic and childhood covariates. Models 2 to 4 adjust for all study covariates.
Compared to low/no attenders in 1979.
Compared to low/no attenders in 2000.
Compared to low/no 1979, low/no 2000.
p < .05, **p < .01, ***p < .001 (two-tailed tests).
Model 1 of Tables 3 and 4 assesses the direct effect of early religious attendance in 1979 on midlife health. Model 1 does not include controls for adulthood characteristics (education and marital status) or religious attendance later on in the life course. As such, it adjusts only for time-invariant covariates and conditions in childhood. Results from Model 1 provide provisional support for Hypothesis 1 (that there is a link between early religiosity and adult health that could be accounted for by later religiosity) but only for the health composite score (Table 3). For SF-12 health composite scores, those who were high and moderate attenders in 1979 reported better health composite scores in 2014 compared with low attenders in 1979 (b = 1.17 and b = 1.07, p < .01 and p < .05, respectively). This provides evidence to support Hypothesis 1. On the other hand, relative to those with low religious service attendance in 1979, neither moderate attenders nor high attenders reported a lower risk of chronic health conditions (Table 4). This does not support Hypothesis 1.
Model 2 adds in adulthood religious attendance (measured in 2000) while controlling for education and marital status (adulthood achieved covariates) and all of our demographic and childhood covariates. This model provides a more complete test of our first hypothesis, to examine whether early religiosity influences later-life health through adulthood religiosity. Results suggest that relative to the low attenders, both moderate and frequent attenders at early midlife (2000) had higher health composite scores (b = .86, b = .92, p < .05, respectively). Moreover, results from Model 2 suggest that the addition of religious attendance in 2000 reduced the association between early-life attendance and health to nonsignificance. As will be considered in further formal mediation analyses, this provides support for Hypothesis 1 and suggests that the influence of childhood religious attendance on health is mediated by attendance later in the life course.
As indicated previously, the mediation hypothesis was already ruled out for chronic health conditions. Still, for attendance in 2000, those attending moderately and frequently both reported lower risk of chronic health conditions compared with midlife nonattenders (IRR = .86, p < .01, and IRR = .83, p < .001, respectively).
As a formal test of Hypothesis 1 for composite health scores, we conducted a parametric mediation analysis that assessed whether adult religiosity mediates the relationship between early-life religious attendance and health composite scores in later life. The results for this mediation analysis are displayed in Table 5. Here, the exposure terms being compared were a* = 0 (low/no religious attendance in 1979) and a* = 1 (high religious attendance in 1979). The natural indirect effect of midlife religious attendance (2000) was .20 (p < .01). This suggests that health composite scores would increase by .20 if childhood religious attendance was high but religious attendance in adulthood was high instead of low. Religious attendance in adulthood explained 25% (indirect effect .20 / total effect .80) of the influence of early-life religious attendance.
Parametric Mediation Analyses for Midlife Religious Attendance (2000), National Longitudinal Survey of Youth SF-12 Health Composite Scores (N = 3,609).
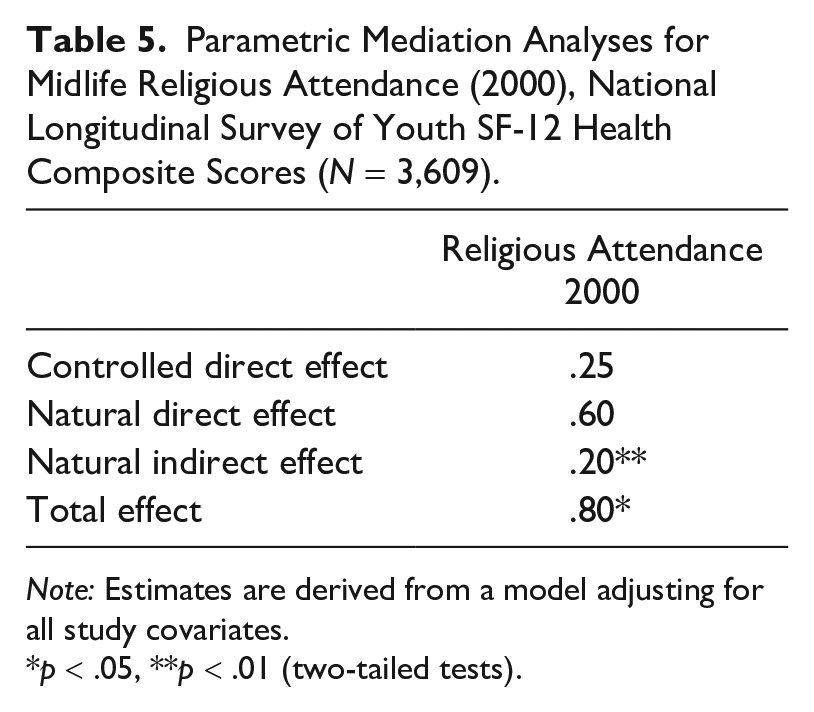
Note: Estimates are derived from a model adjusting for all study covariates.
p < .05, **p < .01 (two-tailed tests).
Before discussing Models 3 and 4 of Table 4, we describe results of a test of Hypothesis 2 (shown in Figure 2), which predicted that consistently high and/or increasing religiosity would be associated with better adult health behaviors (smoking and drinking) than consistently low and/or decreasing religiosity. These expectations help integrate the pathway and mobility life course models; establishing that particular patterns of religious stability/change are associated with distinctive health behavior profiles would substantiate our plans to test such behavioral pathways as mediators of life course religiosity.
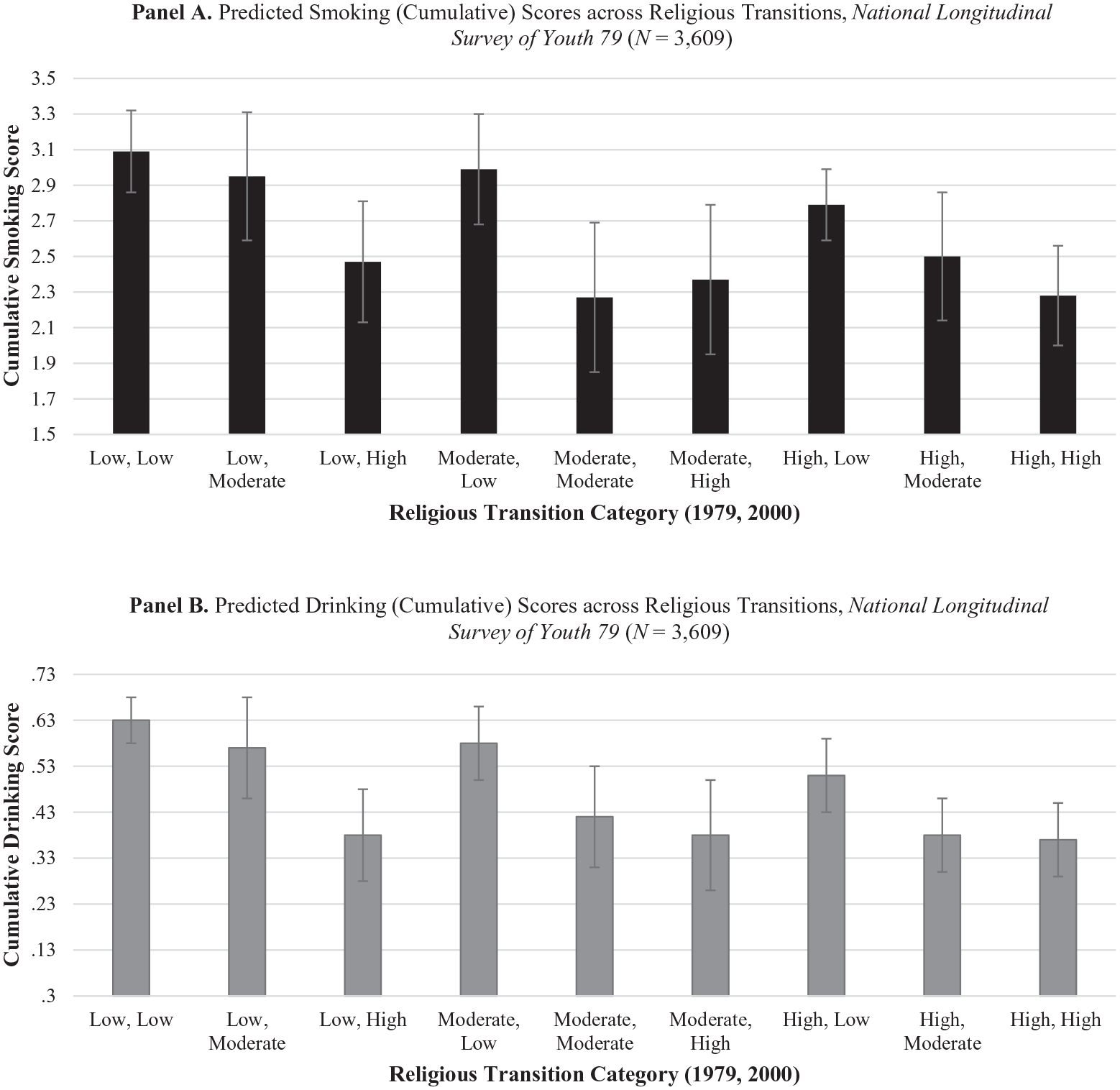
Predicted Health Behavior Scores across Religious Transition Categories
Results provide support for Hypothesis 2. Using OLS regression with robust standard errors, we regressed cumulative smoking and drinking scores on religious stability, controlling for all childhood and adulthood covariates. Figure 2 plots predicted cumulative drinking and smoking scores across each of the nine religious transition categories shown in Table 2, with 95% confidence intervals displayed.
Consistent with Hypothesis 2, we find that those with stably high religious attendance had lower cumulative smoking scores (b = –.81, p < .001) and drinking scores (b = –.26, p < .001) relative to the consistent nonattenders. We also found evidence that increasing religiosity from early life to midlife was associated with better health behaviors. Those increasing from low/no to high religious attendance between early life and midlife had lower smoking (b = –.62, p < .01) and drinking scores (b = –.25, p < .001) than stably low attenders. Likewise, those who progressed from moderate levels of attendance in early life to high levels by midlife also had lower smoking (b = –.72, p < .001) and drinking scores (b = –.25, p < .001). As shown in Figure 2, those who experience a decline in religiosity from moderate to low/no and from high to low/no levels of attendance have significantly higher cumulative smoking scores relative to the stably high attenders. Moreover, those declining from moderate to low/no, high to low/no, and high to moderate attendance had higher drinking scores than stably high attenders. In fact, those declining from high to low attendance between early life and midlife have cumulative drinking scores that are statistically indistinguishable from the stable nonattenders, as depicted in the 95% confidence interval overlap between these two transition categories.
We now examine whether these health behaviors help explain the link between life course religiosity and late-life health. This returns our attention to Tables 3 and 4. The results from Model 3 of Table 3 show that relative to consistently low religious attenders, a consistently moderate or high level of religious attendance is associated with better health composite scores (b = 1.23, p < .05, b = .91, p < .05, respectively). 5 For chronic health conditions, it was only those that reported consistently high religious attendance across the two time points that had a lower risk of chronic health conditions (IRR = .88, p < .05). Contrary to Hypothesis 3, however, there is no evidence to suggest that increasing religious attendance over time was associated with health relative to the consistent nonattenders.
Supplemental analyses (not shown) found that relative to those that experienced any decrease in religious attendance, those with stably moderate and high levels of religious attendance had better health composite score (b = .85 and b = 1.09, p < .05, respectively) and stably high attenders had a lower risk of chronic health conditions (IRR = .89, p < .05).
Hypothesis 3 proposed that the effects of consistently high religiosity would be mediated through health behaviors, an explanation quite plausible in light of the patterns shown in Figure 2. Model 4 in Tables 3 and 4 thus introduces the cumulative health behavior measures of drinking and smoking. Including these variables reduces the effect of moderate-moderate and high-high religious attendance on health composite scores. The inclusion of health behaviors likewise reduces the coefficient for high-high religious attendance for chronic health conditions. Unsurprisingly, higher levels of cumulative smoking are associated with lower health composite scores on the SF-12 (b = –.38, p < .001), although cumulative measures of drinking fail to associate significantly with the outcome. 6 For chronic health conditions, the cumulative measure of smoking—but not drinking—is also associated with a higher likelihood of reporting a chronic health conditions (IRR = 1.12, p < .05).
Parametric mediation analyses offer a formal test of Hypothesis 3. We only examine stably high levels of attendance here because those increasing their religious attendance were not found to differ from consistent nonattenders. The two exposure levels being compared are a* = 0 and a* = 1, where 0 = low/no attendance consistently from 1979 to 2000 and 1 = high religious exposure across the life course (consistent weekly attendance or more from 1979 to 2000). Results presented in Table 6 suggest that high attendance has a significant natural indirect effect through smoking but not through drinking. Findings imply that health composite scores would increase by .09 (p < .01) if religious attendance was high, but smoking levels were changed from the level associated with low/no religious attendance to the level associated with high religious attendance. To put this in context, the average smoking score (on a 6-point scale) for those that had consistently low/no attendance at religious services is 3.39 and is much less, 1.91, for those who consistently regularly attended. Smoking explains 15% of the relationship between stability of religious attendance and health composite scores (.09 indirect effect / –.62 total effect). There was no significant natural indirect effect for drinking, a point we reflect on in the discussion section.
Parametric Mediation Analyses for Health Behaviors, National Longitudinal Survey of Youth (Religious Stability, 1979–2000; N = 3,609).
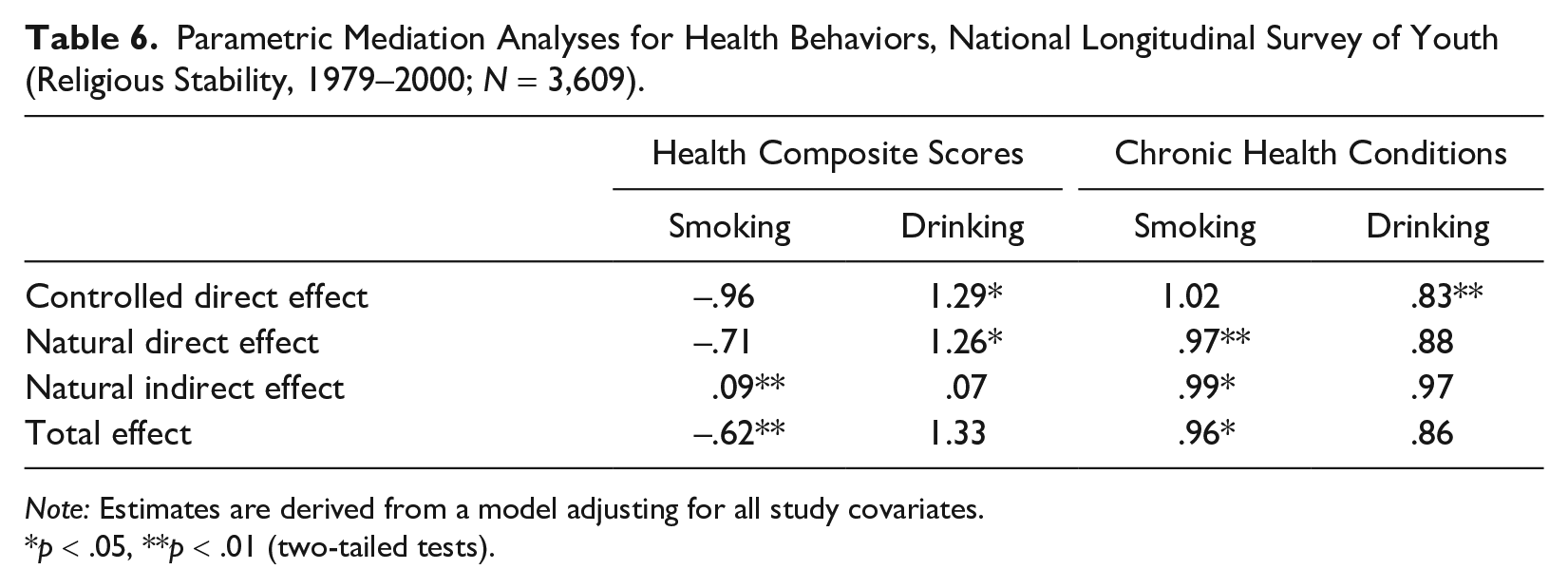
Note: Estimates are derived from a model adjusting for all study covariates.
p < .05, **p < .01 (two-tailed tests).
We observe a similar pattern of results for chronic health conditions. The IRR for natural indirect effects through smoking was .99. This suggests that religious attendance would decrease the count of chronic health conditions by a factor of .99 if religious attendance was high and with smoking subjected to counterfactual manipulation. For interpretability, we convert the IRR to log odds so the direct and indirect will sum to the total effect. Cumulative measures of smoking thus explain 25% (log odds: –.0101 / –.0408) of the relationship between stability of high religious attendance and risk of chronic health conditions. As with health composite scores, there was no significant mediation by the cumulative measure of drinking.
Supplementary Analyses
Ancillary analyses considered whether there were any denominational differences in adulthood smoking and drinking behavior. For the cumulative smoking and drinking scores by religious denomination, see Appendix E in the online version of the article. A two-way analysis of variance revealed that cumulative smoking scores (F = 8.27, p < .0001) and drinking scores (F = 2.71, p < .01) varied significantly across childhood religious denominations.
On the whole, Catholic and Jewish respondents appear to have much lower average smoking and drinking scores compared with almost all Protestant groups (also see Garcia et al. 2013; Whooley et al. 2002). We did not find that any of our main results were moderated by religious denomination. Mediation pathways documented in our main analysis were supported across every religious denomination, with the exception of individuals that reported no religious denomination in childhood.
Discussion
Although much is known about religion and health and about health inequalities over the life course, to date, there has been little attempt to integrate these two bodies of work. Considerable evidence suggests that religious attendance is health-protective (Hummer et al. 2010; Koenig et al. 2012), but most studies have used cross-sectional data or longitudinal data limited to short periods of time, such as early or late adulthood (Desmond, Morgan, and Kikuchi 2010). The current study sought insights from life course pathway and mobility models to gain a more expansive view of how religious participation shapes adult health.
Our results support both the pathway model and mobility model. For mobility processes, consistently moderate and frequent religious practice from early life to later life was associated with better overall health than was consistent nonattendance, and consistently high attendance predicted a reduced risk of chronic health conditions. These findings suggest benefits of stable religious attendance over time. This is consistent with prior research on the transition from adolescence to young adulthood and on attendance transitions among older women (Chen and VanderWeele 2018; Li, Okereke, et al. 2016). However, the current study overcomes some of the limitations of this past work by using nationally representative data following individuals over 35 years.
Stable religious attendance was associated with the best health outcomes of all the religious transitions groups studied. Consistent attendance over the life course may promote the buildup of religious capital, a “familiarity with a religion’s doctrines, rituals, traditions, and members that enhances the satisfaction one receives from participation in that religion” (Iannaccone 1990:2009). Feeling highly satisfied with one’s religious participation helps people feel that they “fit in” with their congregation (Hayward and Elliott 2011); this, in turn, may boost well-being by strengthening members’ adherence to their religious groups’ health-promoting social norms.
Our results also revealed that those who declined in religious attendance over time had similar health profiles to those who never attended in adolescence and in their mid-30s. That is, they fared worse in health composite scores and chronic conditions than the stable attenders. This finding is consistent with a prior cross-sectional, retrospective study of the general population that found religious disaffiliates to experience poorer health compared with those consistently affiliated (Fenelon and Danielsen 2016).
We also found no evidence that increasing religious attendance was associated with better health relative to the consistent nonattenders. Building spiritual capital may be a gradual process over the life course, so health may not be responsive to relatively recent upswings in religious behavior. Unfortunately, we could not ascertain whether attendance change occurred just prior to the second measurement point in the NLSY79 (when respondents were in their mid-30s) or at some point closer to adolescence. It is also important to recognize that gaining or losing religiosity may be endogenous to other life course processes, such as turning points or crises, that may also have health effects (Harris et al. 2012).
Besides mobility findings, empirical support was also garnered for the pathway model. For one, the health-protective role of early-life religious attendance was fully explained by adulthood religiosity. There was therefore no evidence that starting life in a religious home had any influence on adult health net of later attendance. That said, early-life religious attendance made midlife attendance far more likely, a finding supported by previous research (Bengtson 2013). These mediation patterns parallel the indirect effects commonly reported in research on socioeconomic status (Pudrovska and Anikputa 2014; Willson and Shuey 2016). For the case of religion, pathway processes could demonstrate that exercising personal choice in religious involvement as an adult reflects stronger commitment to faith than childhood exposure; the agency involved in remaining religious often solidifies commitments to healthy eating, exercise, and avoiding harmful substances (Guo and Metcalfe 2019).
Health behaviors were a second pathway hypothesized to explain the link between early-life religious exposure and/or the continuity of religious practice and later life health. Causal mediation analyses found adult smoking to explain the effect of early-life religious attendance and the effect of continued religious practice. Whereas earlier work considered the role of religiosity in preventing negative health behaviors in the transition to adulthood (Desmond, Kikuchi, and Budd 2010; Guo and Metcalfe 2019), our study considers midlife health behaviors and beyond. Continued involvement in a religious community from adolescence to midlife reduces the likelihood of smoking and thus bears close connection with one’s overall health at ages 50 through 58.
Unlike smoking, we observed no mediating role for drinking behavior in this study. Although heavy alcohol consumption has negative health implications, regular smoking carries more robust associations with health outcomes (Hart et al. 2010). And although some evidence suggests that moderate levels of drinking may even be beneficial for health—especially the cardiovascular system (Stockwell et al. 2016)—there was no evidence in our analyses that the functional form of the relationship between drinking and health was nonlinear.
Although not the primary focus of our hypotheses, our analysis uncovered several interesting patterns about the life course consequences of religious attendance on health behaviors. As with overall health, lower levels of smoking and drinking were observed only for people who maintained steady religious practice between early life and midlife. Prior studies suggest that the negative association between religiosity and negative health behaviors grows stronger as individuals progress from adolescence to young adulthood (Freeman 2019). The results from the current study extend this observation into middle age and reiterate that early-life religious exposure is not sufficient to reduce the risk of later negative health behaviors. In fact, the health behavior profiles of those who were highly observant in adolescence but decline in attendance over time are statistically indistinguishable from the stable nonattenders. Although reasons for religious decline were not asked of the NLSY79 respondents, it is possible that some individuals decrease their religiosity because they wish to engage in risky health behaviors that do not align with the tenets of their faith (Hill et al. 2019). This selection process may help explain why those people who maintain frequent religious practice over time possess a health advantage.
As for the health outcomes considered in this study, religion was found to benefit health composite scores more than the count of chronic health conditions, both in total and indirect effects. One potential reason for this discrepancy by health outcome is that self-reports of chronic disease are more prone to measurement error (e.g., an individual has not seen a medical professional to be diagnosed with the disease). Errors in self-report would likely have the effect of biasing the regression coefficients toward the null (Obisesan et al. 2006). There is likely no such bias for health composite scores, which ask respondents to think about their current health status but do not require that a threshold for diagnosis be met. Nevertheless, future research looking at how religiosity influences well-being should continue to consider multiple indicators of health.
Limitations and Future Directions
This study is subject to a number of limitations. First, we could not address whether the benefits of stable attendance over the life course were derived from continuous practice in one faith community or whether switching religious affiliation and faith communities offered similar health benefits. Although a thorough list of religious traditions was measured in 1979 in the NLSY79, only a very condensed list of religious traditions was available at 2000. Thus, we were unable to document changes in religious affiliation. It may be that under usual circumstances, it is beneficial to remain within the same faith tradition to maintain consistency of belief and facilitate sustained interactions with co-congregants. But there may be factors that push individuals to change their affiliation, even within cognate denominations, to gain a more positive religious experience (see Hoge, Johnson, and Luidens 1994). The complexities of religious switching and their implications for health should be pursued in future work.
Second, there are other potential pathways connecting frequent religious attendance to adulthood health that we were unable to test with the NLSY79. One important mechanism that should be tested in future research is access to social support over time. Involvement in a congregation holds out the promise of developing long-term, supportive relationships that may potentially span the better part of the life course (Ellison and Levin 1998). Taken together, the social and tangible resources housed within religious congregations should be health promoting over the life course and could be a mechanism accounting for the effects of sustained attendance.
Third, it is important to recognize that our indicator of early-life religious exposure was not measured until respondents were adolescents. Parental religiosity could matter even earlier in the life course. For instance, maternal religious attendance may influence a child’s health in utero by reducing the likelihood of the mother smoking (Burdette et al. 2012). Future research should continue to consider how religiosity across generations shapes health over the long term.
Despite these limitations, our study suggests that religion is an important sociocultural exposure that can be integrated into existing life course models of health. Consequences of childhood socioeconomic exposures and experiences of trauma have become well understood (Ferraro et al. 2016; Willson, Elder, and Shuey 2007; Wilson and Shuey 2016), justifiably commanding continued attention from scholars of health and the life course. We hope this trend endures but believe that salient sociocultural issues—including religiosity—also deserve a place at the table. Understanding pathways and patterns of religious engagement throughout human lives will ultimately help us achieve a better understanding of how childhood contexts shape adult health.
Supplemental Material
Supplemental_Material – Supplemental material for Religious Attendance and Physical Health in Later Life: A Life Course Approach
Supplemental material, Supplemental_Material for Religious Attendance and Physical Health in Later Life: A Life Course Approach by Laura Upenieks and Markus H. Schafer in Journal of Health and Social Behavior
Footnotes
Acknowledgements
The authors are grateful to Christopher G. Ellison, Andrew Miles, Scott Schieman, Jeremy Uecker, the editor, and three anonymous reviewers for comments on a previous version of this article. An earlier version of this article was presented at the 2018 Association for the Sociology of Religion Conference (Philadelphia, United States) and the 2020 American Sociology Association Annual Meeting (San Francisco, United States).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ontario Ministry of Research and Innovation Early Researcher Award and the Canadian Social Sciences and Humanities Research Council Joseph Arnand Bombardier Graduate Scholarship.
Supplemental Material
Appendices A through E are available in the online version of the article.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.