
Abstract
Social change produces alterations in society that necessitate changes in sociological theories. Two significant changes affecting health lifestyle theory are the behaviors associated with the COVID-19 pandemic and the digitalization of society. The health-protective practices emerging from the ongoing pandemic and the recent parade of other newly emerging infectious diseases need to be included in the theory’s framework. Moreover, the extensive digitalization of today’s society leads to the addition of connectivities (electronic networks) as a structural variable. Connectivities serve as a computational authority influencing health lifestyle practices through health apps and other digital resources in contrast to collectivities (human social networks) as a normative authority. The recent literature supporting these features in an updated and expanded model of health lifestyle theory is discussed.
The purpose of this article is to update and expand health lifestyle theory with a focus on changes engendered by the COVID-19 pandemic and the digitalization of society. The theory was originally formulated to provide a conceptual framework modeling the varying directions and stylizations of collective health behaviors (Cockerham 2005, 2021). Given the dominance of methodological individualism in theorizing during the latter part of the twentieth century (Smelser 1997), a major goal of the theory was to call attention to the reality of the influence of social structures on health lifestyles. Assigning the dominant priority in lifestyle choices to individuals as agents of their behavior neglected the boundaries and configurations placed on their choices by the social structures in their lives. As Graham Scambler (2018:95) aptly put it: “There is never a non-structured social world.” Consequently, lifestyles are not the random behaviors of disconnected individuals; instead, they have an aggregate form characteristic of the groups and social classes in which they hold membership.
Health lifestyles are defined as collective patterns of health-related behavior based on choices from options available to people according to their life chances (Cockerham 2005; Cockerham, Rütten, and Abel 1997). As noted long ago by Max Weber ([1922] 1978), a person’s life chances (or chances in life) are socially determined, and social structures are an arrangement of those chances. Therefore, the aforementioned definition of health lifestyles takes both structure (life chances) and agency (life choices) into account because it is the interaction between structure and agency as a dialectical process that is decisive in configuring a person’s health lifestyle.
Other views similarly depict health lifestyles as bundles, constellations, or clusters of health behaviors that occur in patterns and are reinforced by group-level identities and norms (adams et al. 2022; Mollborn, Lawrence, and Hummer 2020; Mollborn, Lawrence, and Saint Onge 2021; Mollborn and Modile 2022). The behaviors in question typically involve food choices, levels and types of alcohol consumption, smoking, exercise, and the like that affect one’s health and life span. Health lifestyles not only reflect “notions of what constitutes good or poor health” and “knowledge about health promotion” (Krueger, Bhaloo, and Vaillancourt 2009: 1382), but they are also powerful determinants of a person’s health and longevity. According to Jason Wasserman and Brian Hinote (2011:44), “Lifestyle is now the most significant predictor of health and mortality.”
This is seen in a sizable body of research attesting to the substantial role of health lifestyles in health and mortality outcomes (Behrens et al. 2013; Cockerham et al. 2017; Khaw et al. 2008; Loef and Walach 2012; Mollborn et al. 2020; Saint Onge and Krueger 2017; Schnermann et al. 2021; van Dam et al. 2008; Zhang 2021). Estimates of added years of life expectancy associated with a healthy lifestyle at age 50 in the United States range from 7 to 14 additional years beyond that of people with unhealthy lifestyles (Li et al. 2018; Metha and Myrskylä 2017). Health lifestyle theory provides a model of the social variables influencing the behavioral choices (good and bad) people make that impact their health.
Background
The rationale for updating health lifestyle theory can be traced to the observation made decades ago by Lewis Coser (1977) in his critically acclaimed book Masters of Sociological Thought. Coser maintained that sociological theorists and their theories are best understood in relation to the intellectual and social contexts prevalent in their time. Such contexts reveal that social change is a prime catalyst for the emergence of various sociological theories at specific points in history. Changes in society showcase the need, shape the conceptualizations, and endorse the explanatory power or obsolescence of theories.
Theories in medical sociology likewise result from or are influenced by social change but additionally take health matters into account, including temporal variations in a society’s burden of disease. Health lifestyle theory fits this format as it originated in the late twentieth and early twenty-first centuries to explain collective forms of health behavior in response to changes that continue today in (1) disease patterns, (2) modernity, and (3) social identities (Cockerham 2005).
Disease Patterns
The first and foremost change signaling the importance of lifestyles for health was the long-term epidemiological transition from infectious to chronic diseases as the leading cause of mortality globally. The timeline of this transition through its different stages is from prehistory to around 1960 (Omran 1971). In each period, lifestyles increased in significance as a health determinant (Cockerham 2021). Such lifestyles were linked over time to cardiovascular dysfunctions, pulmonary disease, some cancers, Type 2 diabetes, kidney disease, obesity, and various other chronic afflictions (e.g., Behrens et al. 2013; Christensen and Carpiano 2014; Cockerham et al. 2017; Cockerham, Bauldry, and Sims 2022; Lawrence, Mollborn, and Hummer 2017; Loef and Walach 2012; Murimi et al. 2015). Moreover, in a proposed new transitional stage for the present era—the “Hybristic” or mixed stage—risky behaviors (unhealthy lifestyles) are viewed as a major cause of death from both chronic and infectious diseases (Rogers and Hackenberg 1987).
The link to infectious diseases is especially noteworthy. The resurgence of infectious diseases in the late twentieth and early twenty-first centuries flips Omran’s (1971) epidemiologic transition theory back to its beginning in a return to many of the features of its initial “Age of Pestilence.” Infectious diseases have returned with a ferocity as urbanization, globalization, climate change, and human penetration into formerly remote areas uncovered new viruses and put them at large in society (Barrett 2021). While coping with infectious diseases has been an ongoing problem for developing countries historically, COVID-19, in particular, illustrates the power of pestilence to disrupt social life today on a global scale. The study of social behavior in relation to infectious diseases will undoubtedly command much greater attention going forward. Exposure to infection and coping with epidemics and pandemics involve health lifestyle practices that need to be researched more fully. These practices are relevant not only because of their centrality in responding to changing disease patterns but also because of how they are differentially interpreted and integrated into public policies.
Modernity
As the industrial and postindustrial ages faded into history, the current late modern era emerged in which many traditional centers of power and authority were weaker (Bauman 1992, 2000; Beck 1992; Giddens 1991). For medicine, this meant somewhat lessened professional power compared to the mid-twentieth century (Ritzer and Walczak 1988). Decision-making authority and direct control of the marketplace by the medical profession was reduced by government cost controls and insurance programs, private health insurance company mandates, managed care systems, large corporate health care conglomerates, and a modification in the traditional patient–physician relationship featuring the direct participation of patients in decisions about their health care (Pescosolido and Boyer 2021). The latter development was boosted by the public diffusion of medical information and advice on the Internet and the widespread distribution of digital devices to access this knowledge (Henwood and Marent 2019; Lupton 2013, 2018).
Nevertheless, the medical profession remains the ultimate authority on “health” and gatekeepers to medical care. They maintain their powerful role in wellness advocacy (preventive checkups, evidence-based best practice standards, value-based care, etc.) and promoting healthy lifestyle behaviors. Adopting a healthy lifestyle in partnership with health care providers or independently gives people more control over maintaining or enhancing their health and living longer. As a result, health in today’s modernity is normatively viewed as an achievement (“a goal to work toward”) rather than a taken-for-granted physical condition passively accepted as is by the individual (Cockerham 2005, 2021). The pursuit of health by way of a healthy lifestyle has become not only a societal norm in economically advanced countries (VanHeuvelen and VanHeuvelen 2021) but also a duty (Lupton 2013).
Two major features of modern life affecting health lifestyles are COVID-19 and digitalization. COVID-19 exemplifies the pervasive rise of newly emerging infectious diseases in contemporary society (Barrett 2021), while the ascendancy of digitalization as a global mode of communication and information-sharing now extends electronically into the pursuit of healthiness (Henwood and Marent 2019; Lupton 2018). Responses to COVID-19 do not require a reformulation of health lifestyle theory, but the pandemic illustrates that lifestyle choices will change depending on the circumstances. Digitalization, for its part, provides an extensive range of information, data-driven measures, and assessments of health practices and lifestyles that are now available literally at the fingertips of users. Wearable and other technologies utilized in the pursuit of health qualify as a lifestyle practice.
Social Identities
Lifestyle consumer habits surfaced in the late twentieth century as a leading indicator of individual and group social identities (Bauman 1992; Chaney 1994; Giddens 1991). Pierre Bourdieu (1984), for example, in his seminal study Distinction, noted the relevance of a person’s “ distance from necessity,” in which the further away a person was from having to concentrate on acquiring his or her basic needs for survival, the more freedom, time, and resources that person had to develop and refine his or her personal tastes in line with a more privileged class status. Lower social strata, having to focus more on obtaining life’s necessities, did not have the range of options and resources to pursue such refinements. Instead, they had tastes more applicable to their particular situation in life. Thus, one’s tastes or choices, exhibited in a lifestyle, serve as evidence of class position and social identity. As Anthony Giddens (1991:81) once explained, lifestyles fulfill utilitarian needs and give a material form to particular narratives of social identity. Narratives about social identities (who one is) are articulated via lifestyles.
For example, identity theory, with its roots in symbolic interaction, helps us understand a person’s social identity is composed of self-views (self-categorizations) that evolve through occupying various roles in society and memberships in particular groups and social classes (Burke and Stets 2009; Stryker 1987). Narratives communicating social identities include styles of living and are verified through recognition as such on the part of others. “If identity is like a continuous story [biographies] being told through different ways of living,” says David Chaney (1994:125), “then lifestyles can be thought of as genres—narrative modes—that collect themes and resources to ground particular stories.”
Health lifestyles likewise express a person’s narrative about who they are (Frie and Janssen 2009; Jaye et al. 2018; Mollborn and Lawrence 2018; Mollborn, Lawence, and Saint Onge 2021; Mollborn and Modile 2022; Stead et al. 2011). For instance, Bourdieu (1984) depicted how social tastes in food, drink, and sports preferences were indicative of differences in class standing. Moreover, in an era in which health is an achievement, a positive social identity and cultural capital accrue to those who strive (work) to be healthy. This is seen in a qualitative study by Stefanie Mollborn and Adenife Modile (2022) that found the family socialization of socioeconomically privileged young adults imparted standards of discipline and a sense of high moral worth concerning a healthy diet and exercise that were missing in the cultural capital of lower strata counterparts. “Our findings,” state Mollborn and Modile (2022:7), “underscore the roles of not just health behaviors, but identities, narratives, norms, and understandings of health as core aspects of health lifestyles.”
Consequently, there are normative complexities about health lifestyle behaviors that bestow not only different levels of healthiness but status and moral values signifying social boundaries between people. According to Kirstin Frie and Christian Janssen (2009:221), “Unmistakable socially distinct associations of being healthy, healthy behaviour and leading a healthy lifestyle make it possible for social groups to perceive one another according to these characteristics as well as to distinguish themselves from other social groups.”
This circumstance accords health lifestyles symbolic power (Korp 2008) and pushes the behaviors into the realm of health politics and health inequality as people on the lower end of the social gradient have fewer opportunities for healthy lifestyles (Frie and Janssen 2009; Mollborn, Lawrence, and Saint Onge 2021; Phelan and Link 2013). The symbolic power of a healthy lifestyle is based on its value as a “social good” that legitimatizes particular modes of thinking and acting about health and delegitimizes others that harm health and are at odds with the norms of the affluent (Korp 2008). Therefore, as Giddens (1991:5) concluded decades ago, the lifestyle concept has taken on a particular significance in understanding contemporary social life. It has likewise taken on special importance with respect to a person’s identity and social status in relation to their health.
Health lifestyle theory, as noted, was intended to advance understanding of how lifestyles impact the health of different social groups and serve as a theoretical framework for empirical research on the topic. It has become “a mature theory in medical sociology used to explain the combination of health behaviors and their associations with health outcomes” (VanHeuvelen and VanHeuvelen 2021: 205). However, the COVID-19 pandemic and the spread of digitalization in society provide a new social context for the theory to address. The remainder of this article will discuss what these developments mean for an expanded theoretical model.
The COVID-19 Pandemic and the Rise of Infectious Diseases
In the late 1960s, infectious diseases were thought to be possibly disappearing as significant health hazards (Barrett 2021; Barrett and Armelagos 2013; Oldstone 2010). However, by the 1980s, a parade of newly emerging infectious diseases was underway. First was HIV/AIDS (1983), followed by H5N1 avian influenza (1996), the West Nile virus (1999), SARS (2002 to 2003), MERS (2012), H7N9 avian influenza (2013), Ebola (2014), Zika (2016), COVID-19 (2019), and monkeypox (2022). Different viruses appear year after year, infecting many people, making them sick, and sometimes killing them. They usually come from far-flung places and are not generally recognized as significant health risks or emerging new infectious diseases until they spread into major metropolitan areas (Barrett 2021). Yet they carry with them the message that infectious diseases are repetitive and significant threats to global health.
COVID-19 and its rapid spread resulted in the deaths of over 6 million people to date and significant disruptions to social and economic life on a global scale (Barrett 2021; Cockerham and Cockerham 2021; Ryan 2021). The World Health Organization (2022) calculated that the full death toll directly or indirectly associated with COVID-19 during 2020 to 2021 was nearly 15 million. It is an event of historic proportions. This pandemic and other recent outbreaks forecast a much greater focus in medical sociology on infectious diseases. The same can be said of health lifestyle theory.
This is because health lifestyles have significant roles in the onset, spread, prevalence, and methods of coping with infectious diseases. For example, in the COVID-19 pandemic, a health lifestyle practice played a causal part. Although its exact route to humans may never be confirmed, the best genome evidence thus far suggests the SARS-CoV-2 virus jumped from bats to an animal (pangolins) to humans (Han 2020; Lam et al. 2020; Pekar et al. 2022). The likely site for transmission to humans was an outdoor food market in Wuhan, China (Worobey et al. 2022). What brought an infected animal and potential human hosts together was a health lifestyle practice featuring the consumption of recently killed wild animals whose natural energy adherents believe will transfer directly to the person eating it (Zhong, Crang, and Zeng 2020).
Once the pandemic was underway, health lifestyle practices contributed to levels of sickness and mortality in three ways. First, negative health lifestyle behaviors featuring a disregard for or situational inability to engage in protective practices were significant in spreading the infection. Second, positive health lifestyle practices aimed at coping with the pandemic and preventing infection, such as frequent handwashing and sanitizing, staying at home, social distancing, wearing protective masks, and getting vaccinated, were mandated by public health authorities as normative behaviors. Social distancing and home isolation led to more walking and bicycling outdoors but also to more snacking and consuming alcohol indoors (Vincent 2023). However, acceptance or rejection of COVID practices was prompted by structural variables, such as socioeconomic status (SES), age, gender, and the influence of social networks and political ideologies (Cockerham and Cockerham 2021; Hill et al. 2022; Mollborn, Mercer, and Edwards-Capen 2021; Ryan 2021).
Vaccination, for example, had the greatest likelihood of ending the pandemic but became a highly divisive lifestyle practice because of fear of harm by vaccines and a political issue as an infringement on individual rights (Cockerham and Cockerham 2021; Hill et al. 2022). Women were found to have greater COVID-19 vaccine hesitancy than men, especially those with low SES, while lacking a college education was a significant variable among the vaccine-hesitant for both sexes (Morales, Beltran, and Morales 2022). Women were more concerned about safety (side effects) and men by conspiracy theories. Men were significantly more likely to minimize the threat.
The third contribution of health lifestyles to the pandemic are those practices that had earlier caused or contributed to the onset of comorbid conditions, such as heart disease, hypertension, diabetes, pulmonary ailments, and obesity. COVID-19 deaths were highest among individuals with these conditions, especially those with already compromised immune systems and breathing problems. In the United States, comorbid conditions and mortality from COVID-19 were most common among older people, males, African Americans, Hispanics, and lower social strata (Abrams and Szefler 2020; Price-Hayward et al. 2020; Yancy 2020).
The COVID-19 pandemic and the likelihood of future large-scale viral infections with social connotations point to the flexibility of health lifestyle theory in explaining different health problems in different time periods and locales. The COVID-19 pandemic is an example of the theory’s capability to address the spread of and response to the SARS-CoV-2 virus among particular population groups. Consequently, COVID-19-related health practices and those associated with infectious diseases generally should be included in the theory’s repertoire of health lifestyle actions. Other practices in the future may replace these routines but currently remain relevant behaviors.
Digitalization
Digitalization is the second change that needs to be brought into health lifestyle theory. Although the digitalizing of society was well underway before the COVID-19 pandemic, the outbreak accelerated the use of digital technologies for work, entertainment, and interpersonal communication because of the requirement for social distancing to keep people apart (Airoldi 2022). This circumstance includes greater use of wearable technologies, such as Fitbit health and fitness trackers and smartwatches, and electronic links to sites (i.e., websites, webinars, apps, subscription exercise and yoga services, streaming video sites, virtual classes, social media sources, blogs, and podcasts) for participating in and managing various types of health lifestyle practices. Some digital devices provide information and measures (biodata) of an individual’s physiological functioning, sleep patterns, exercise routines, diet, menstrual cycles, and other health-related assessments (Hardey 2019; Henwood and Marent 2019; Lupton 2013, 2018; Petersen 2019; Williams, Coveney, and Meadows 2015).
This development includes the use of health and fitness apps (software applications) to assist health lifestyle management, apps for electronic links to health care providers and health information, and patient-centered apps for managing a disease or self-diagnosis (Peng et al. 2016:1). Apps also allow individuals to interact directly with health care personnel by electronic means, search databases, generate their own health records, and determine their health status. People are no longer limited to computers and can alternatively utilize their smartphones, smartwatches, and tablets as a form of mobile health, or mHealth. Health lifestyle practices and outcomes can be monitored through the tracking and quantification of bodily signs and behaviors (Pols, Willems, and Aanestad 2019). All of which are indicative of living in a still emerging late modern society where adopting a healthy lifestyle accords people more control over their health situation and digital devices provide the information and databases to monitor and assess that control.
Digitalization needs to be included in health lifestyle theory because it is an electronic means to learn about, measure, evaluate, and record lifestyle practices. Data can be linked to other people and their practices and to databases in an electronic network. This is accomplished by introducing a nonhuman element—algorithms (step-by-step computational instructions) that operationalize the organization, visualization, and preservation of data—to the network. According to Manuel Castells (2010:500), the network form of organization is not new; what is new is that digitalization enabled electronic networks to expand throughout entire social structures. For example, approximately 95 percent of the population in North America is connected to the Internet (Internet World Stats 2022).
Moreover, online health networks can function in ways that offline social networks cannot by instantly transcending geographical boundaries, maintaining varying levels of anonymity, connecting quickly with people of similar experiences, and linking online interactions with offline health (Zhang and Centola 2019:101–102). This digital hyperconnectivity has been described in sociology as “a defining act of our time” (Brubaker 2020:749).
The question thus arises as to whether digitalization should be inserted as a collectivity that is already a structural element in health lifestyle theory or as a different type of structural variable. Ori Schwarz (2021:51) argues that electronic social network sites introduce the notion of the “connective” as a new and different type of entity analytically distinct from the individual, the interpersonal, and collectivities. Health lifestyle theory regards collectivities as collections of human actors (i.e., families, friends, peers, and colleagues) linked together through particular social relationships, such as kinship, religion, work, and political ideologies (Cockerham 2005). They constitute intersubjective “thought communities” (Zerubavel 1997) in that their shared norms, values, ideals, and social perspectives reflect a particular collective worldview. Collectivities, according to Weber ([1922] 1978), have meaning in the minds of individuals, partly as something existing and partly as something with normative authority. In this role, they can “have a powerful, often a decisive, causal influence on the course of action of real individuals” (Weber [1922] 1978:14).
By contrast, connectivities merge human and nonhuman components in a different type of association. The network it represents is neither a durable nor temporary human collectivity; instead, it is an electronic connectivity continuously recalculated and remodeled by algorithms based on streams of data generated by users and machine learning systems and recorded (Airoldi 2022; Schwarz 2021:69). Although connectivities are a tool to be used to understand, monitor, and enhance one’s health, they have the structural qualities of producing and influencing user dispositions and practices as a computational authority (Airoldi 2022:145), that is, as a reference metric for decisions about initiating, continuing, or modifying a health lifestyle. Computational authority differs from normative authority in that its influence centers on one’s own biodata rather than group, class, or societal norms. The two forms of authority operate in tandem when one is integrated with the other.
As such, it represents another form of health lifestyle participation and measurement. Given its widespread utilitarian prominence, connectivities need to be added to health lifestyle theory as a distinct structural category and the role of its data-based feedback assessments of lifestyle practices for the user researched accordingly. There is a paucity of research on the effects and effectiveness of digitalization on health lifestyles thus far. One expected social pattern, however, is that the use of digital devices for health purposes is primarily lodged among higher SES groups and younger adults.
Updated/Expanded Model
The updated theoretical model is shown in Figure 1. The arrows between boxes indicate hypothesized causal relationships. The model states, as shown in Box 1 of Figure 1, that there are four categories of structural variables: (1) class circumstances; (2) age, gender, and race-ethnicity; (3) collectivities and connectivities; and (4) living conditions. The structural variables (Box 1) provide the social environment within which socialization and experience occur (Box 2) that influence and shape dispositions toward particular preferences in life choices (Box 3) while also comprising a person’s life chances (Box 4).
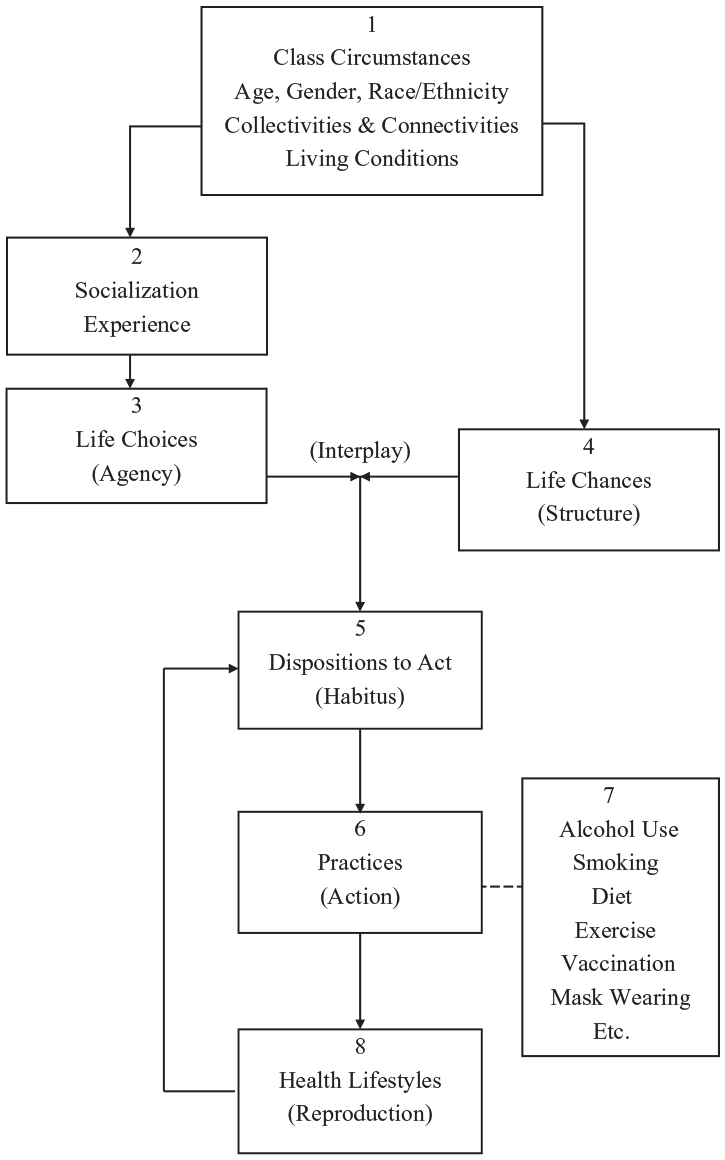
Health Lifestyles Paradigm.
Class Circumstances
Class is the only sociodemographic variable indicative of a person’s material well-being (Chibber 2022). As such, it has profound implications for a person’s level of health and choice of health lifestyle practices. Class circumstances or SES establish the catalog of options available for the individual to choose from and the rank order of preferences for the individual. Consequently, class circumstances are the key structural variable in determining health lifestyle patterns (Carpiano, Link, and Phelan 2008; Christensen and Carpiano 2014; Cockerham 2005, 2021; Lawrence et al. 2020; Mollborn and Modile 2022; Rees Jones et al. 2011; van den Broek 2021).
Research in Western societies has traditionally shown that the health lifestyles of the upper and upper-middle classes are the healthiest overall of any social strata and that such lifestyles progressively become less healthy the lower a person’s social status. More affluent classes as a whole have the highest participation in leisure-time sports and exercise, more nutritious diets, often moderate drinking, little or no smoking, more preventive checkups by physicians and dentists, and greater opportunities for rest, relaxation, and coping successfully with stress (Andrews, Hill, and Cockerham 2017; Antunes 2011; Burdette et al. 2017; Carpiano et al. 2008; Lawrence 2017; Margolis 2013; Narcisse et al. 2009). The upper and upper-middle classes are also the first to adopt new health strategies and practices to keep themselves healthy (Missinne, Daenekindt, and Bracke 2015; Missinne, Neels, and Bracke 2014; Phelan and Link 2013). This includes the greater likelihood of using digital devices to manage their health lifestyles (Hardey 2019; Peng et al. 2016).
This pattern is not always universal, however, as seen in countries that have experienced rapid economic development, such as China. Several Chinese studies show the most affluent groups are more likely to have diets high in fat and sugar content, be more sedentary and obese, and smoke and drink more than those in lower social strata (Chen, Yang, and Liu 2010; Miao and Wu 2016; Schafer and Kwon 2012). The affluent adopt these unhealthy behaviors because they see these choices as privileges to be enjoyed with their purchasing power and higher status (Chen et al. 2010:144). Other research utilizing health lifestyle theory finds both the most healthy and most risky health lifestyles in high-SES groups (Wang 2019). Low-SES groups showed lifestyles that were a mixture of healthy and harmful practices.
Among elderly Chinese, however, those who are the most socioeconomically advantaged are most likely to have the healthiest lifestyles (Zhang 2021). This outcome suggests that the higher SES–healthiest lifestyle link exists in China but is most fully evident later in life. Consequently, the effects of social class on health lifestyles and the lifestyles themselves can be geographically or locally distinct. This is not inconsistent with health lifestyle theory that “expects group norms and understandings of ‘healthy’ behavior to vary from one place to another” (Mollborn, Lawrence, and Saint Onge 2021:392). Local social structures influence local outcomes.
While there is considerable evidence that health lifestyles are generally healthier overall at the top of society in the West than at the bottom, this outcome does not mean they are exclusively healthy. While some individuals may have lifestyles featuring either uniformly (concordant) healthy or unhealthy behaviors, others have a health lifestyle consisting of combinations of healthy and unhealthy (discordant) practices. Some U.S. studies emphasize the discordant nature of health lifestyle practices that suggests they are the norm (Saint Onge and Krueger 2017), especially during adolescence and young adulthood, when these age groups experiment with risky health behaviors (adams et al. 2022; Daw, Margolis, and Wright 2017; Lawrence et al. 2020; Mollborn and Lawrence 2018; Mollborn, Lawrence, and Saint Onge 2021).
In addition to finding discordant practices in adolescence and young adulthood, these studies did not uncover significant social class differences. Nevertheless, inconsistent or reversed findings for the effects of higher SES (personal or parental) on the health lifestyles of adolescents and young adults (adams et al. 2022; Burdette et al. 2017; Lawrence et al. 2020) are not unrealistic, considering these are transitional stages of life that affect youth of all class circumstances. As Elizabeth Lawrence and her colleagues (2020:14) determined: “Associations with SES thus appear to be developmentally specific, and socioeconomically based identities may become more salient in adulthood than in earlier life.”
This seems to be the case given that studies in the United States, Western Europe, and China find that higher SES adults are more fully represented in the healthiest lifestyles, especially in middle and older ages, compared to lower strata individuals (Cockerham, Wolfe, and Bauldry 2020; de Vries et al. 2008; Kroesen 2019; van den Broek 2021; Zhang 2021). Lawrence et al. (2020:14) suggest that despite experimentation when younger, high SES groups “come to reject risky health lifestyles as they complete advanced education, establish long-term relationships, and enter into occupational careers.” In sum, it can be said that individual health lifestyles often include a mixture of health-promoting and health-harming behaviors that are nonetheless aligned along social gradients throughout most of the life course, with the healthiest practices usually associated with higher SES and the least healthy with lower SES.
Age
Turning to age, a current research trend is to combine health lifestyle and life course theories to account for changes and continuities in health lifestyle practices at different stages in the life cycle (Burdette et al. 2017; Cockerham et al. 2020; Keyes et al. 2015; Lawrence et al. 2017, 2020; Mize 2017; Mollborn and Lawrence 2018; Mollborn et al. 2014, Mollborn, Lawrence, and Saint Onge 2021). In a pioneering study, Mollborn and her colleagues (2014) found that even preschool children have health lifestyles, which serve as precursors to health lifestyles in middle childhood. Although young children have little agency in choosing their health lifestyle as parents generally make the decisions, they do express judgments over what health-related practices they like or dislike. Social background was found particularly significant as children in disadvantaged households were likely to have lifestyles with greater health risks (i.e., less personal safety, food insecurity, less sleep, and more exposure to secondhand smoking and violence). Consistent with health lifestyle theory, primary socialization in the home was a crucial factor in a child’s health behavior. The decisive variable was not just age but class, as this and other studies (Mollborn, Lawrence, and Krueger 2021; Mollborn and Modile 2022) find that parental SES is reflected in the health lifestyles of their young children.
Other life course studies find that childhood and adolescent health lifestyles go on to influence those in young adulthood (Burdette et al. 2017; Daw et al. 2017; Lawrence et al. 2017; Lee et al. 2018; Mize 2017; Mollborn and Lawrence 2018). However, as noted, adolescent health lifestyles are often inconsistent as family influence competes with that of schools and peers, which, in the case of peers, is likely discordant (adams et al. 2022; Mollborn and Lawrence 2018; Stead et al. 2011). Parental class standing declines in strength as a determining factor in health lifestyles during adolescence (Burdette et al. 2017; Mollborn and Lawrence 2018).
In middle and old age, the aging process influences people to recognize the need to take better care of their health (Jaye et al. 2018). While it might be surmised that there is a general tendency toward healthy lifestyle practices in older ages, this is not necessarily the case. Stability with the past tends to be more common than change in health lifestyles at this time of life (Burgard et al. 2018; Cockerham et al. 2020; Lawrence et al. 2020; Rees Jones et al. 2011), unless the person has been diagnosed with a chronic disease that needs to be managed with healthier lifestyle choices (Cockerham et al. 2020).
Rather than seeing a steady upward arc of continued improvement in health lifestyles as one ages, there is evidence that earlier practices become “locked in” at older ages along class lines (Rees Jones et al. 2011). That is, social class distinctions seem to retain their significance at older ages, with healthier lifestyles remaining typical of people higher on the social scale compared to those toward the bottom (Cockerham et al. 2020; McGovern and Nazroo 2015; Rees Jones et al. 2011; Shaw et al. 2014). As people age, they carry their health lifestyle along with them as part of an age-specific cohort into the next stage of their life course, modifying or keeping the lifestyle as is while adjusting to an older and physically different body.
Gender
Gender is another significant structural variable stratifying health lifestyles in that women generally have healthier lifestyles than men, except for exercise (Annandale 2021; Cockerham 2021; Mollborn et al. 2020). This is the case even though there is research showing more variation within genders than between them (Mollborn et al. 2020). Gender’s imprint on health lifestyle practices begins during childhood as females are socialized to take care of their bodies, visit physicians more frequently than males, and deal with being sick more often. Childbearing, childrearing, and caregiving roles are also significant. Women usually adopt and maintain positive health lifestyles during pregnancy and postnatal care and socialize their children to be healthy. All of which suggest a like-minded habitus among many women featuring durable dispositions toward good health habits (Cockerham 2018).
This is not to say that all women engage in healthy lifestyle practices, as a recent decline in life expectancy among less educated White women in various low-income rural counties in the United States has been associated with smoking, opioid drug use, and obesity (Cockerham 2014; Montez and Zajacova 2013). Nevertheless, by young adulthood, most women have mostly healthy lifestyles (Mollborn et al. 2020). Men are more likely to smoke and consume alcohol than women, eat less healthy foods, be violent, drive fast, take more health risks, have more accidents, suffer more injuries, and die younger (Dolan 2011). Men with an exaggerated (hegemonic) sense of masculinity are less likely to seek preventive care and more likely to engage in risky health behaviors (Cockerham 2018; Dolan 2011; Smith and Dumas 2019; Springer and Mouzon 2011). This outcome seems to apply particularly to working-class men and others further down the social scale who maintain a heightened sense of masculinity concurrent with a marginal social status (Smith and Dumas 2019). Whereas gender is a strong predictor of health lifestyle practices in its own right, it can also be affected by class distinctions, as people higher on the social scale, regardless of gender, usually have healthier lifestyles (Audet et al. 2017; Christensen and Carpiano 2014; Cockerham 2021; Mollborn et al. 2020; Saint Onge and Krueger 2017; Smith and Dumas 2019).
Race and Ethnicity
Race and ethnicity are seriously underresearched with respect to health lifestyles. Studies focusing on the health lifestyles of Asians and Hispanics are absent from the literature. Research on Black Americans is limited, but existing comparisons show that non-Hispanic Blacks are not as likely as non-Hispanic Whites to drink heavily but are more likely to have a less healthy diet and less leisure-time exercise (Keyes et al. 2015; Saint Onge and Krueger 2011, 2017; Zapolski et al. 2014). While proportionately more Black men smoke than either White men or White women, Black women smoke less than Black men and Whites generally (Ho and Elo 2013; Pampel 2008). Smoking for men and poor diets and lack of exercise for both men and women stand out as particularly unhealthy lifestyle practices among Black Americans (Cockerham et al. 2020; Hattery and Smith 2011).
Research on Black–White differences in health lifestyles and cardiovascular disease found both racial groups engaged in a combination of healthy and unhealthy lifestyles, with those primarily lodged in the latter category showing an elevated risk of coronary heart disease and higher mortality (Cockerham et al. 2017). A significant difference was that in each of four lifestyle configurations, Blacks showed a higher probability of excessive energy intake from dietary choices than Whites—indicative of the potential for obesity. Other research shows in an all-Black sample that higher SES Black adults in late middle age have healthier lifestyles than those in the same age group with a lower SES, consistent with health lifestyle theory (Cockerham et al. 2022).
Living Conditions
The structural attributes of collectivities (normative authorities) and connectivities (computational authorities) have been previously discussed, while the fourth structural category of importance in the health lifestyle model is living conditions. The living conditions variable pertains to the natural and built environments of neighborhoods and places people live and work. It refers to the effects on health lifestyles that result from differences in climate; housing; basic utilities like heating, sewers, and safe water; neighborhood amenities such as restaurants, grocery stores, parks, and recreational facilities; and personal safety. The environment within which a person spends their life makes it probable or improbable for achieving and maintaining a healthy lifestyle in the living conditions at hand.
Health lifestyles are obviously most effective in producing health in positive living situations and least effective in disadvantaged neighborhoods where poor health behaviors and unhealthy settings are common (Fitzpatrick and LaGory 2011; Frohlich and Abel 2014; van den Broek 2021). An innovative extension of the living conditions variable in health lifestyle theory to the level of countries shows the importance of national contexts for acquiring a healthy lifestyle (VanHeuvelen and VanHeuvelen 2021).
Completing the Model
As previously stated, life choices and life chances interact dialectically, and the outcome commissions the formation of dispositions to act in certain ways (a habitus) shown in Box 5 (Figure 1), leading to practices (action) shown in Box 6 involving alcohol use, smoking, diet, exercise, vaccinations, use of health apps, and other health-related actions represented as examples in a dotted line to Box 7. Multiple health practices combine to constitute an overall health lifestyle (Box 8) whose enactment leads to its reproduction (or modification) through feedback to the habitus.
Although the emphasis on structure may suggest that the model is one of downward conflation or structural determinism, this is not the case, given that agency is represented in the model. As Anne Hammarstörm et al. (2015:14) point out, health lifestyle theory is an “agency within structure model.” A basic premise of the theory is that people choose their lifestyle, but the range of choices is constrained or enabled by what is structurally possible and influenced by the style common to their class circumstances and other structural variables.
The dispositions toward action, as noted, constitute a habitus, which is a cognitive map or set of perceptions routinely guiding and evaluating a person’s choices and options. It is a process of thinking in which social norms and cultural conventions are internalized in the mind, along with the individual’s own inclinations, preferences, and interpretations that predispose them toward certain behaviors and not others. Although the term “habitus” may be uncommon, it is an old concept that originated with Aristotle and was refined by a host of scholars over time, including Thorstein Veblen, Edmund Husserl, Weber, Marcel Maus, Norbert Elias, and especially Bourdieu (Cockerham 2018; Wacquant 2016). For example, Weber ([1922] 1978:536) saw the habitus as a disposition to see the world in a particular way and behave accordingly.
According to Bourdieu (1998), one of the principal functions of habitus is that of providing a unity of style linking the practices of a single agent to a class of agents that brings together people who are very similar to each other but different from people elsewhere. Bourdieu finds that the habitus retranslates the relational characteristics of a social position into a lifestyle reflecting a set of chosen practices that differentiates itself from the choices of persons in other social classes. As Amy Burdette et al. (2017:522) observe, “Health lifestyle theory suggests that social statuses work to shape qualitatively different patterns of behaviors in individuals that may not be summarized in terms of simple counts of healthy or unhealthy behaviors.” This is because the health behaviors of individuals cluster in varying ways and form diverse combinations of health practices within different lifestyle configurations. The result is good health and longevity for some people and the opposite for others.
Conclusion
Social change produces alterations in society that necessitates adaptations or expansions in sociological theories. This update of health lifestyle theory does not change its basic premises but adds new factors. Two major changes affecting health lifestyle theory today are the COVID-19 pandemic and the digitalization of society. Other social changes possibly affecting patterns of health lifestyles already present in society are climate change, globalization, the fluidity of sexuality, and polarization in norms, values, and politics. However, COVID-19 represents a special case in that it solidifies the rise of newly emerging infectious diseases as a threatening fixture in modern society. Consequently, as seen in Figure 1, the normative health lifestyle practices (e.g., vaccination, mask-wearing, social distancing, etc.) emerging from the ongoing pandemic need to be included in the model where applicable as additional practices (action). Vaccination, in particular, has taken on enhanced social importance and could easily join alcohol use, smoking, diet, and exercise as fundamental health lifestyle practices (see, e.g., Saint Onge and Krueger 2017).
Also, the extensive digitalization of today’s society and its effects on health lifestyles mark it as a new and influential practice. This change leads to joining connectivities with collectivities (both constitute networks) to health lifestyle theory as a structural variable. Connectivities serve as a computational authority influencing health lifestyle practices through health apps and other digital resources (electronic networks) in contrast to collectivities (human social networks) as a normative authority. The recent literature supporting these features in an expanded model of health lifestyle theory is discussed.
The traditional impact of class circumstances on health lifestyles is also reviewed in light of findings showing the effects of SES on health lifestyles to be inconsistent or reversed for some higher SES persons in adolescence and young adulthood. However, this is a transitional period across the life course and a time of experimentation for youth in all social strata. Continuity with one’s social origins typically resumes in adulthood and appears locked in by older ages. Social class remains a key determinant of health lifestyles. Whereas class position shapes lifestyles, it can also be said that a person’s lifestyle likewise identifies their class membership because the two variables are so closely intertwined.