
Abstract
Doctors (and sociologists) have a long history of struggling to understand why patients seek medical help yet resist treatment recommendations. Explanations for resistance have pointed to macrostructural changes, such as the rise of the engaged patient or decline of physician authority. Rather than assuming that concepts such as resistance, authority, or engagement are exogenous phenomena transmitted via conversational conduits, we examine how they are dynamically co-constituted interactionally. Using conversation analysis to analyze a videotaped interaction of an oncology patient resisting the treatment recommendation even though she might die without treatment, we show how sustained resistance manifests in and through her doctor’s actions. This paradox, in which the doctor can both recommend life-prolonging care and condition resistance to it, has broad relevance beyond cancer treatment; it also can help us to understand other doctor–patient decisional conflicts, for instance, medication nonadherence, delaying emergent care, and vaccine refusal.
Keywords
Why do people see doctors for help but resist their advice? Major literatures on seeking medical help, patient adherence, and physician authority have tackled this question from varied perspectives over the past 70 years. In an end-of-life context, it is well established that patients with advanced cancer have poor prognostic awareness (Loučka et al. 2021). It is also well known that making prognoses is notoriously difficult (Christakis 2001), and there are social and structural reasons that physicians avoid end-of-life discussions (Spencer et al. 2017). More recently, a growing body of work has examined how doctors and patients interactionally facilitate and impede the uptake of treatment recommendations in real time—showing how notions of compliance, resistance, and authority are not just static or essentialist concepts but also dynamically co-constituted by actors.
Building on social psychological and cognitive veins of research, these studies of patient–provider interactions raise important questions about whether and how providers themselves may contribute to (or impede) patient uptake of recommendations through interaction. For example, existing studies point to the importance of first establishing patients’ understandings of their conditions to cultivate receptivity. Singh et al. (2017) examined how treatment discussions are facilitated when physicians first summarize the meaning of prior results. Relatedly, Maynard, Cortez, and Campbell (2016) show how the use of “appreciation sequences”—initiated after scan results summarizing the utility of treatment in prolonging their lives—helps terminally ill patients accept the current situation before discussion of next steps. These interactional strategies are remarkably similar to patterns observed in delicate news delivery, where it is common to elicit the perspective of one’s interlocuter and integrate it into the delivery of news that might otherwise be face-threatening or create a rupture of the social fabric (Maynard 1996). In a departure from earlier decades in which “noncompliance” was conceived as a patient characteristic (Spencer 2018), these studies of interaction shift the analytic focus to how doctors and patients jointly create outcomes.
Under this umbrella of interaction studies, research on patient resistance, often referred to as simply “resistance” (cf. Sidnell and Stivers 2012; Stivers 2007), has been growing for over 20 years in sociology, communication, and health services research. This work is focused on how patients resist treatment recommendations both actively and passively across contexts such as primary care (Koenig 2011; Mangione-Smith et al. 2003), neurology (Toerien 2021), vaccine discussions (Opel et al. 2015), oncology (Roberts 1999; Tate 2022), pediatrics (Stivers 2005a), and psychiatry (McCabe 2021; Thompson and McCabe 2017). Further work has been done cross-culturally to demonstrate that this practice emerges across the globe (Bergen et al. 2017; Lindström and Weatherall 2015). In this context, resistance is defined as an interactional practice demonstrating any nonacceptance of a recommendation at the time acceptance is normatively due. Patients routinely orient to treatment recommendations as proposals that they can either accept, reject, or modify after they are delivered (Costello and Roberts 2001; Heritage and Sefi 1992; Stivers and Timmermans 2020). Resistance, by definition, occurs in the local conversational context, sequentially following the treatment recommendation. Distinct from conceptualizations of political forms of resistance explored in literatures on social movements (Hynes 2013), this is a technical definition about in situ behavior and is a subset of broader questions of how patient adherence may unfold over time, even days or months down the road.
Resistance is also evidenced by how other interactants respond to it. If recommendations are not accepted immediately after they are delivered, doctors themselves treat patients as resistant by doing their own interactional work to pursue acceptance, such as adjusting the recommendation, justifying, and bargaining—even in the context of more subtle forms of resistance such as short periods of silence (Stivers 2005a; Stivers and McCabe 2021; Tate 2022). In other words, if doctors perceive an utterance as resistance, it is visible in their response.
This interactional resistance happens frequently. A recent special issue of Social Science and Medicine indicates that 10% to 40% of medical encounters involve some treatment disagreement depending on the country and clinical context, often manifesting through resistance (see Stivers and McCabe 2021). Patient resistance has been found to delay progress toward the next clinical activity—closure of the visit—because it launches a treatment negotiation between doctor and patient (Stivers 2007; Stivers and Timmermans 2021). In his study of primary care, Koenig (2011) argues that through resisting, patients help shape treatment plans. In pediatrics, Stivers and Timmermans (2021) describe how parents rarely demand antibiotics outright but deploy more subtle strategies to resist physician assertions that antibiotics are inappropriate for their children. This research shows how interactions are not simply conduits for information—medical recommendations asserted and resisted—but ways patients can assert their agency while also shaping treatment plans and contributing to clinical outcomes. Importantly, these approaches largely conceptualize resistance as originating from patients, an issue we return to in the following.
We build on and extend these literatures through conversation analysis (CA) of a single case showing a high-stakes oncology interaction. CA is a method concerned with the organization of social actions across contexts and how relations between individuals are built and maintained (Schegloff 1987). CA approaches are informed by Goffman’s (1955) interaction order, which encompasses one’s “face” (claims to an immediate identity) and their larger personal identity (e.g., a lawyer, a mother). In his American Sociological Association presidential address, Goffman (1983) argued that interaction is itself an institution worthy of study as the central mediator undergirding the operation of larger institutions through agreed-on structures and behavioral logics. CA is also shaped by Garfinkel’s (1963) assertions that social actions are comprised of shared understandings and methods of producing talk and responding to others, rendering the larger interactional project culturally meaningful. CA investigates both the position of an action (when something is said) and its composition (how it is said), supporting a turn-by-turn analysis of how individuals achieve order in interactional projects, like seeking help from an oncologist. To do this, CA focuses on how an action is delivered through talk, understood, and responded to by others in a process of shared sensemaking (Garfinkel 1967; Heritage 1984b; Schutz 1972).
There are two main CA strategies for studying interaction. In the first, researchers build collections of fragments of interaction focused on a single phenomenon or pattern across multiple cases. In these studies, a collection of conversational fragments is analyzed to show how a type of action operates (e.g., news deliveries, resistance) and its consequences. For example, scholars have examined processes of medicalization through inappropriate antibiotic prescribing (Stivers 2007), the avoidance of end-of-life discussions (Tate 2022), and management of clinical certainty in genomics (Stivers and Timmermans 2016). Other scholars have investigated the ways face-threatening news is broken to patients (Maynard 1996) and how this advances physicians’ professional authority (Maynard 1991).
A second CA strategy, our focus in this article, is to examine how this extant body of knowledge can be brought to bear on a single interaction. Beyond just serving as a testing ground for the application of earlier studies, the single case strategy creates opportunities for extending existing work, consistent with qualitative strategies of examining deviant cases to test results and build theory (Seale and Silverman 1997; Stivers and Timmermans 2021; Tate 2020; Timmermans and Tavory 2022). In his 1987 paper, Schegloff describes how studying a collection of fragments may explain 499 out of 500 cases, but the single case approach has the potential to shed light on the outlier—that 500th case. Single case analyses have been applied in different settings, examining how physicians interpret patient compliance (Lutfey 2004), discuss hospice (Lutfey and Maynard 1998), facilitate patient acceptance (Gill 2019) and, in a now classic paper, how a 911 call goes awry (Whalen, Zimmerman, and Whalen 1988).
Indeed, the case we analyze is unusual in several ways. An interaction that might, at first glance, be written off as chaotic or driven unilaterally by a resistant patient instead is revealed to be orderly and revealing of how deeply consequential interactional dynamics can be. The patient in this case is a 37-year-old otherwise healthy mother, diagnosed with aggressive cancer and an unfavorable prognosis, who walks away from the interaction without accepting treatment despite pressure from the oncologist. In what follows, we extend existing studies of patient resistance by showing how (1) the oncologist’s initial actions, not the patient’s, set the stage for the patient’s resistant displays; (2) the format of the doctor’s treatment recommendation and the embodiment of presuppositions about the patient’s preexisting knowledge condition resistance; (3) the patient mobilizes a portfolio of interactional strategies to impede uptake of the recommendation, including but not limited to overt resistance; (4) the doctor plays an important role in sustaining the resistance rather than resolving it; and (5) the outcome of the conversation—nonacceptance—results from the ways both interactants co-constitute resistance, using tools identified in previous studies but bringing them together in ways that expand beyond the parameters of existing work.
Background
Patient Engagement
A burgeoning literature has emerged considering how patients have changed over time in response to changes in physician authority. Paradigms of shared decision-making and patient-centered care provide a broad umbrella for conceptualizing these shifts away from a model where physicians unilaterally dictate treatments and patients comply to one where patients are more knowledgeable and active. Access to the Internet, proliferation of pharmaceuticals, and changes in health surveillance have all contributed to these broader orientations to patient roles (Conrad 2005)—in Anspach’s (2011:xx) words, creating a democratization of diagnosis in which the membrane separating expert medical and lay understandings has become more permeable.
More recently, in his influential Reeder address, Timmermans (2020) suggests that “engaged” is a more accurate descriptor of today’s patient. Evidence shows that patients have become more likely to assert preferences, offer candidate diagnoses, and present symptoms in service of preferred outcomes. Resistance is yet one more way of displaying engagement. But the mechanics of patient engagement extend far beyond the stereotype of the opinionated “cyberchondriac” who comes to the doctor with Internet research in hand, requesting specific treatments and leaning on doctors for preferred outcomes. There remains more to understand about how patients and providers dynamically cocreate engaged patient conversations in ways that shape outcomes.
We respond to and help elaborate the research agenda on patient engagement embedded in Timmermans’s (2020) work. Specifically, we are concerned with the ways that patient engagement is not unidirectional, with patients showing engagement and physicians responding. If we take seriously the conversation analytic premise that talk is not just a conduit for information but action in and of itself—that how and when things are said matter as much as what is said—then we must also take seriously the implication that physicians dynamically co-constitute patient engagement. In this case, we leverage a single case to illustrate exactly how a doctor can not only invite but also condition a display of patient resistance, eventually resulting in nonacceptance of treatment. This is an uncommon occurrence but theoretically critical insofar as it shows precisely how patient engagement is not unilateral. It is by virtue of its atypical nature that a single case analysis is the most robust analytic strategy for this interaction.
Interactional Studies of Resistance and Treatment Recommendations
Timmermans (2020) notes that the patient-centered care paradigm incentivizes patient involvement by encouraging physicians to make space for patient concerns. This, Stivers and Timmermans (2021) argue, also carries the function of inviting patient resistance. Studies on resistance are informed by the conversational framework of progressivity, in which interactants move through an interactional sequence toward accomplishment of some project—such as treating a medical problem—without interruption from an intervening action (Schegloff 1979, 2007). Interactants, both in ordinary conversation and institutional exchanges—such as legal questioning, news interviews, and doctor–patient interaction—routinely display preferences for progressivity (Raymond 2016; Stivers and Robinson 2006).
Patients can shape the direction of the medical encounter through their ability to accept, reject, or resist the recommendation (Stivers 2005a; Stivers and Timmermans 2021). When patients resist, they can do so actively or passively (Stivers 2005b). Active resistance involves overtly challenging, questioning, or rejecting the recommendation, whereas passive resistance involves tacit forms of nonacceptance, such as silence or minimal acknowledgments like “Mhm” or “Yeah.” Although not overtly resistant, Heritage and Sefi (1992:395) establish these responses constitute resistance because they “do not acknowledge or accept [the treatment] as advice.”
Patients demonstrate that they have the right to accept or resist through interactional strategies used to respond to recommendations. Stivers and Timmermans (2020) describe how parents resist pediatric epilepsy treatments through displaying their preferences, expressions of fear, and experience. In the context of pressing doctors for antibiotic prescriptions for their children, Stivers and Timmermans (2021) similarly show how parent strategies set the stage for resisting the recommendation that antibiotics are inappropriate. A recent special issue in Social Science & Medicine highlights what happens when patients display resistance and engagement but not necessarily in the rational ways that physicians might prefer in the historical wake of compliance paradigms (see Stivers and McCabe 2021).
In theory, doctors could accept patients’ resistant positions—which would support progressivity—and move to close the visit (Stivers 2007; Stivers and Timmermans 2020). Yet studies have shown that doctors do not readily accede to resistance. Instead, they attempt to pursue acceptance before moving to the visit’s closure (Lindström and Weatherall 2015; Stivers 2005a, 2005b). Doctors do this by putting in interactional work to negotiate acceptance, such as offering concessions, changing the recommendation (Stivers 2005b), or using persuasive tactics (Gill 2019; Tate 2019, 2020).
CA studies identify several strategies that doctors use to promote patient alignment. For example, by providing an inventory of treatments used, doctors can create an interactional “on ramp” for discussion of more treatment (Maynard et al. 2016; Singh et al. 2017). Gill (2019) finds that addressing patients’ possible misconceptions about their cancer diagnosis supports advocacy for treatment in otherwise delicate territory. Similarly, doctors can encourage treatment acceptance by mobilizing clinical reasoning, thus giving patients windows into their diagnostic process prior to recommending treatment (Peräkylä 1998). More generally, using similar language as patients in describing the problem or soliciting patient perspectives and incorporating it into talk (Maynard 1989) are effective for aligning with patients (Lutfey and Maynard 1998). In advanced cancer care, “exhausted current treatment” statements are used in ways that avoid discussion of poor prognosis so that even when there are no further treatment options, patient alignment is interactionally cultivated (Cortez, Maynard, and Campbell 2019). Lindström and Weatherall (2015) find that in cases of strong patient resistance, physicians raised patients’ ultimate right to refuse treatment recommendations.
Notably, the oncologist in our analysis does not engage in the interactional strategies that have been shown to mitigate resistance from the patient in advance, a quality that makes it atypical compared to broader research and warrants single case analysis. Instead, as we elaborate, she delves into discussion of an aggressive treatment without contextualization. As a result, the patient’s lack of treatment uptake is itself a form of resistance. As the discussion unfolds, this dynamic is heightened as the patient continues to resist the proposed treatment plan and the doctor tries to persuade her to accept. Together, they dynamically facilitate patient engagement through intersubjectively conditioning and sustaining resistance.
The Power of a Single Case Analysis
In their classic article, Whalen et al. (1988) use a single case strategy to demonstrate how a 911 call in 1984 in Dallas, Texas, took a fateful turn “when words fail[ed].” In this incident, an ambulance was delayed while a dispatcher argued with the caller, who was trying to procure help for his stepmother. By the time the ambulance arrived, the woman had died. The confusion on the call captured local and national media attention, raising questions of how a 911 call—a routine step in the provision of health care—could have gone so wrong.
The single case approach affords a unique close analysis of the turn-by-turn unfolding of this negotiation, providing specific examples of the contours of misalignment. Whalen et al. (1988) deftly illustrate how the in situ sequential organization of interaction is key to understanding the conflict unfolding on this call. Features of the call perceived as refusal, resistance, and emotional distress can also be understood as outcomes from a turn-by-turn organization of talk. As a result, a conflict that appears to be about a dispatcher refusing to help can instead be seen as a tension between the dispatcher’s bureaucratic work tasks and ways that the caller unwittingly misinterprets that workflow, resulting in interactional problems. The conversation was not simply a neutral conduit for service provision, but talk-as-action also constituted the service itself.
We take a similar single case approach to examine interaction between a cancer patient and her oncologist. The patient in this case is faced with a metastatic cervical cancer diagnosis, and she does not accept the treatment recommendation from her oncologist, who mobilizes evidence that the treatment plan—derived from clinical guidelines—could extend her life. This case has several unique features that help expose otherwise obscured characteristics in terms of how interactions are facilitated, resisted, and blocked. First, the consultation ends without treatment acceptance despite extensive physician pressure. By comparison, in their study of pediatric epilepsy clinics, Stivers and Timmermans (2020) found that physicians were able to convert resistance to acceptance in 95% of cases in their collection. Second, the oncologist spends most of the visit talking about treatment with no prior discussion of test results. By contrast, Singh et al. (2017) show that 77% of interactions adhere to a general structure in which treatment talk comes after discussion of symptoms and test/scan results. Third, although prognoses are notoriously avoided, here prognosis is covered explicitly, providing opportunity to analyze its structure. Fourth, it is unusual to have a video-recorded example of life-and-death decision-making. As such, this case is an exemplar revealing how competing agendas emerge sequentially in a high-stakes decision-making exchange and the multiple sources that lead to nonacceptance at the visit’s closure. A single case analysis strategy allows us to observe how a wide variety of well-studied phenomena operate synergistically in one interaction in ways that tell us something about how patient resistance happens and is sustained across a single encounter alongside a physician’s push for treatment.
Data And Methods
This single case was part of a larger cross-sectional corpus of 90 video-recorded interactions between a convenience sample of oncologists and their patients at two urban academic teaching hospitals in the western United States. The first author was ethnographically steeped in these data, recording the videos over a three-year period (2014–2017), and has published a series of articles focused on interactional patterns identified in the data set (Tate 2019, 2020, 2022). We chose this case because it was atypical in these data for a patient to repeatedly resist a proposed treatment, especially in the context of metastatic cancer, particularly such a young patient with a pessimistic prognosis. We operationalized this patient’s resistance based on (1) technical definitions as described in the introduction: an interactional practice demonstrating any nonacceptance of a recommendation at the time acceptance is normatively due and (2) evidence that the physician herself responds to the patient’s talk as resistant. As analysts, we were agnostic as to the moral valence of the interaction that unfolds in this case. For these reasons, we began our analysis by asking how treatment resistance could emerge and go unresolved. Research protocols were Institutional Review Board approved, and all participants provided written informed consent prior to recording. After consent, the camera—situated on a tripod in the corner of the exam room—was turned on, and the first author exited the room before the provider entered.
The first author transcribed the encounter according to conversation analytic conventions (see Appendix A), designed to capture not only what was said but also notate how interactants deliver words (e.g., emphasis, silence, sighing, interrupting, questioning intonations), which sheds important light on the actions being produced and their receipt (see Hepburn and Bolden 2012; Stivers and Timmermans 2020, 2021). We next analyzed this case using CA methods (Heritage 1984b; Sidnell and Stivers 2012). We began our analysis at the start of the treatment recommendation phase of the visit (Byrne and Long 1976; Robinson 2003; Waitzkin 1991), as the doctor transitions from reviewing the patient’s surgical incision to launching into a recommendation for chemotherapy and radiation. We then examined every following turn at talk and analyzed the information delivered, particularly how it was delivered and subsequently registered and responded to by the opposing interactant. The interaction was analyzed until the visit’s closing sequence. Further details of the treatment recommendation timeline shown in the excerpts we present in the analysis are found in Figure 1.
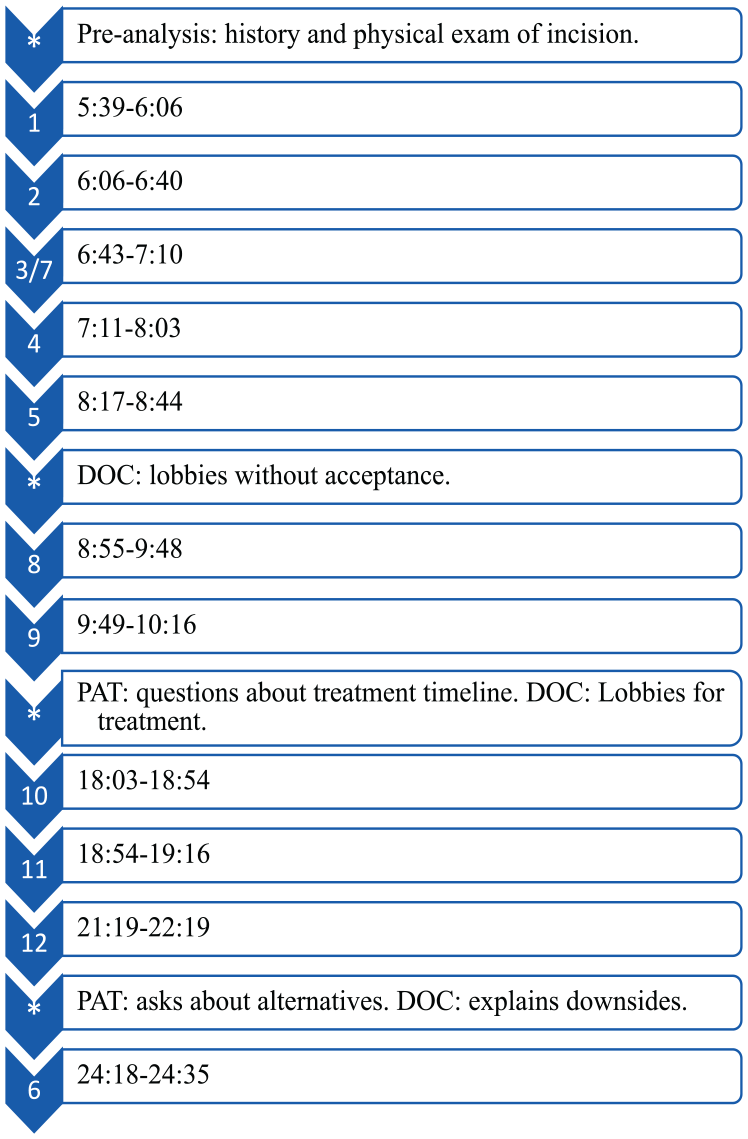
Treatment Recommendation Timeline of Excerpts.
In this case, a 37-year-old female recently had surgery to remove her cervix, uterus, and a nearby lymph node after the cervix was found to have cancerous cells on it. The video recording captured the postsurgical appointment between the patient and her gynecologic oncologist, who performed the surgery. The patient, clothed, was seated on the exam table. She faced the doctor, who sat on a swivel stool. A nurse stood behind the doctor, and the patient’s mother, who only spoke Spanish, sat to the side of the patient. At the start of the visit, the doctor examined the patient’s incision and discussed side effects from the incision. After offering to prescribe lidocaine gel for some incision-area discomfort, the doctor launched into a recommendation for chemotherapy and radiation followed by more chemotherapy as a next step in the patient’s care.
Results
We first describe the doctor’s grounds for recommending treatment to the patient paraphrased and out of sequential order. We characterize these as “informings”—some “tellable” matter that one individual is knowledgeable about and shares with another, unknowing, individual (Heritage 1984a). Like Whalen et al. (1988), we consider these the “particulars” of information provided to the patient about the warrant for further treatment: We found clear cell cancer in the cervix and lymph node, which means it had spread. This cancer is rare and very aggressive. After surgery, you still may have small cancer cells remaining in your body. The best treatment for this is starting chemotherapy and radiation followed by more chemotherapy soon. The prognosis for your type of cancer is thirty-five percent survival after five years with treatment. If you don’t treat this cancer soon, it will be deadly. Because you are young and healthy, we expect you to do well on treatment. We will watch you closely to control side effects.
To medical providers, the patient’s lack of treatment acceptance may seem irrational. Taken together, the doctor’s informings reveal that the cancer is rare and aggressive and that the patient will certainly die if she does not pursue treatment. Yet treatment nonacceptance is the outcome. Why?
We argue, like Whalen et al. (1988), that taking such informings out of their sequential order—produced, registered, and responded to—deludes the interactional project at hand. This analysis shows that the sequential environment through which these informings emerge and the ways that the treatment is resisted and negotiated make clear the patient’s barriers to understanding the cancer as deadly and reveal tensions in the doctor–patient interaction that emerge in response to the patient’s resistance.
Diagnostic Informings and the Emergence of Resistance
First, we make the claim that the sequential environment in which the doctor provides diagnostic news shapes how the patient understands and responds to the recommendation. The doctor’s provision of news to the patient—which include the particulars of her diagnosis—happens after the recommendation, either in response to the patient’s questions or as a counter to the patient’s resistance, and across several minutes. We argue that because the diagnostic news is not delivered to the patient sequentially prior to the recommendation as grounds for the recommendation, the patient lacks access to a warrant for treatment when she receives the recommendation, at which point acceptance or rejection is due. This results in the patient meeting the treatment recommendation with resistance through questioning the recommendation after its delivery, delaying acceptance.
This also results in the patient being unable to realize the news in a sequentially relevant way. Central to a news delivery sequence, as Maynard (1997) describes, is realization, where the recipient demonstrates knowledge of the news “in a way that indicates cognitive apprehension” (Maynard 1996:109). Realization is critical to relations between interactants because it facilitates a shared understanding of the social world and makes “daily life available” to others (Maynard 1996:128). Here, the patient realizes diagnostic news in a slot instead designed for acceptance of the treatment recommendation, thus demonstrating what the doctor orients to as resistance.
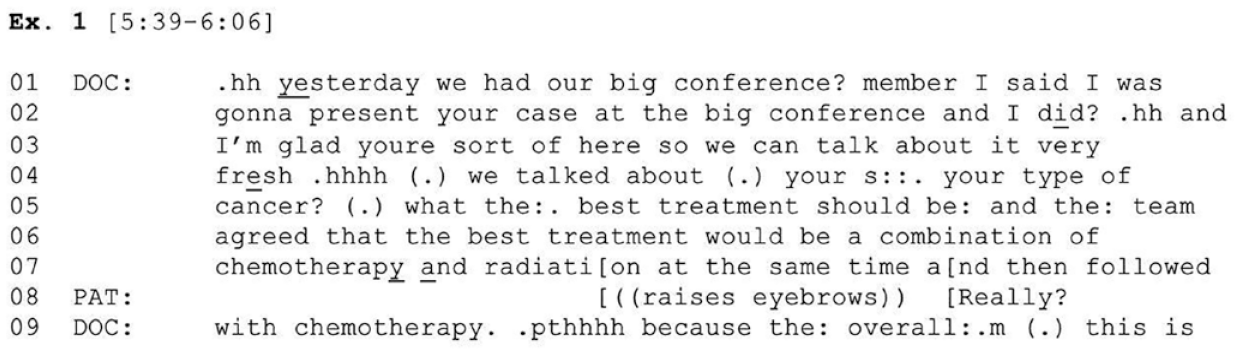
The doctor prefaces her recommendation as the result of a discussion with colleagues at a “big conference” (line 01). While invoking colleagues’ consensus, the doctor recommends chemotherapy and radiation followed by more chemotherapy, framing it as the “best” treatment. The patient responds midrecommendation with the newsmark “Really?” Extract 1 (Figure 2) (line 08; see Jefferson 1981), treating this information as news through registering surprise when acceptance is normatively due—initial mild resistance (Stivers 2007). Prior to its delivery, the recommendation is justified on grounds that the patient’s case was presented to experts who reached consensus about the “best” path forward. Her doctor is referencing the tumor board—a multidisciplinary group of oncologists who meet to review complex cases and craft treatment plans. At the time the recommendation is delivered, its diagnostic grounds have only been presumed. Although acceptance is normatively due here (Koenig 2011; Stivers 2005b), the patient is still dealing with the news that she has further treatment ahead, which comes as a surprise due to her presupposition that treatment was complete.
Extract 1.
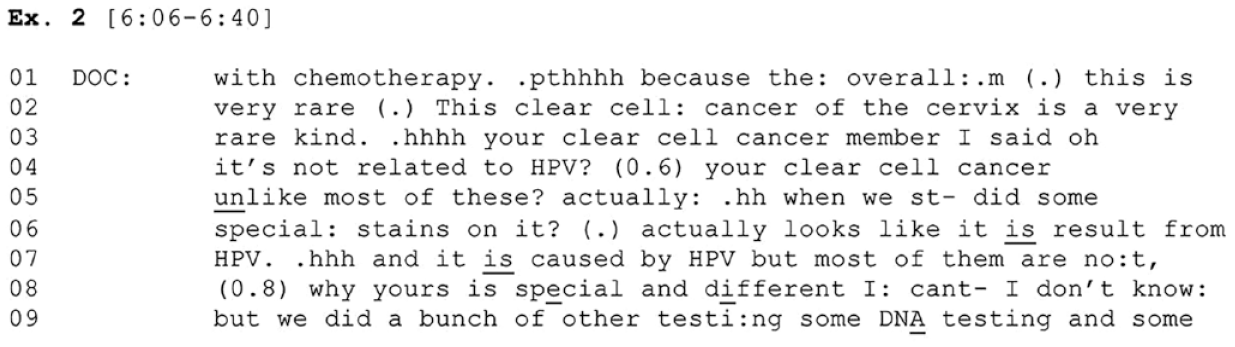
In subsequent extracts in this section, we see more of the doctor’s diagnostic news leak out to the patient across several minutes after the recommendation, leaving no sequentially appropriate slot for news realization. In Extract 2 (Figure 3), following the recommendation, the doctor provides the patient with initial diagnostic news about the nature of the cancer, explaining that she has a very rare cancer linked to HPV, although it was originally thought to be unrelated.
The cancer is set apart from “most” cervical cancers unrelated to HPV. This informing is proffered in second position (i.e., responding to an initiated action), as an account (Heritage 1988), and responds to the patient’s initial resistance from Extract 1 (Figure 2). Because the diagnostic informing is delivered as an answer to the patient’s newsmark “Really?,” there is no slot for the patient to next respond to or register this diagnostic information as news. The doctor continues to explain the nature of testing to the patient.
Extract 2.
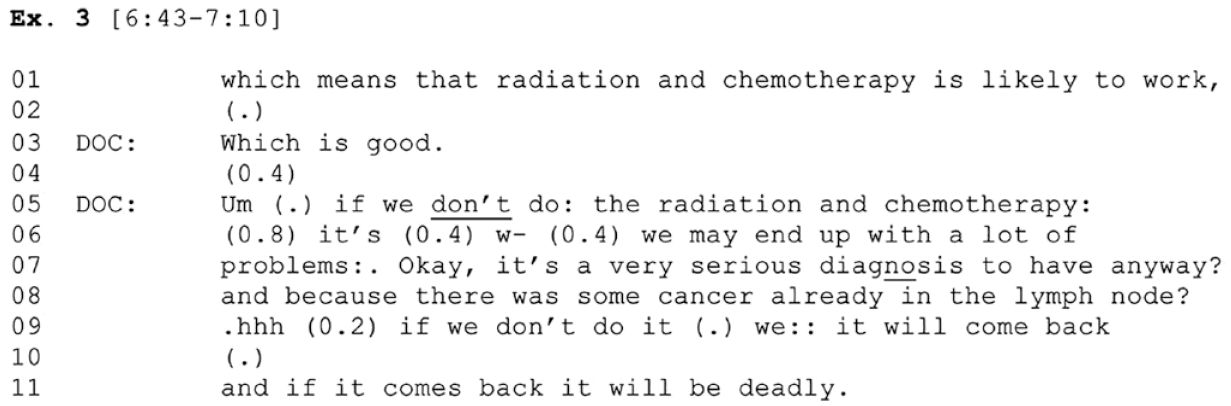
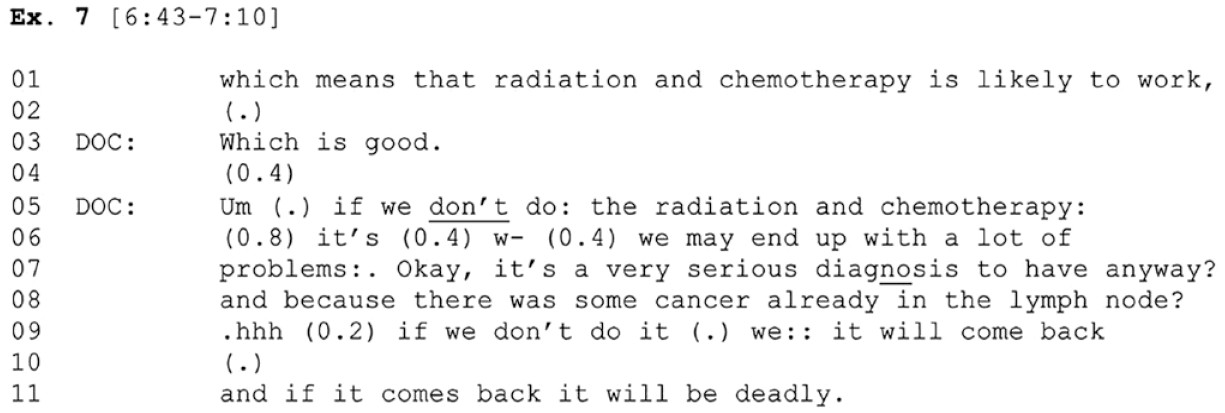
In Extract 3 (Figure 4), the doctor explains an upshot, that the proposed treatment is “likely to work” (line 01). After no uptake from the patient, the doctor indexes the likelihood of treatment efficacy as good news. Following still no uptake, the doctor responds with a hypothetical outcome should the patient not accept as a counter to the patient’s resistance: “if we
Extract 3.
After the doctor continues underscoring the serious nature of the cancer, in Extract 4 (Figure 5), she links these potential problems to the importance of treatment, reiterating the treatment recommendation, “So our best goal? is to get rid of it now.” In overlap, the patient asks in a yes-no interrogative format, “so right now right? Now I: um:. I don’t have cancer or I
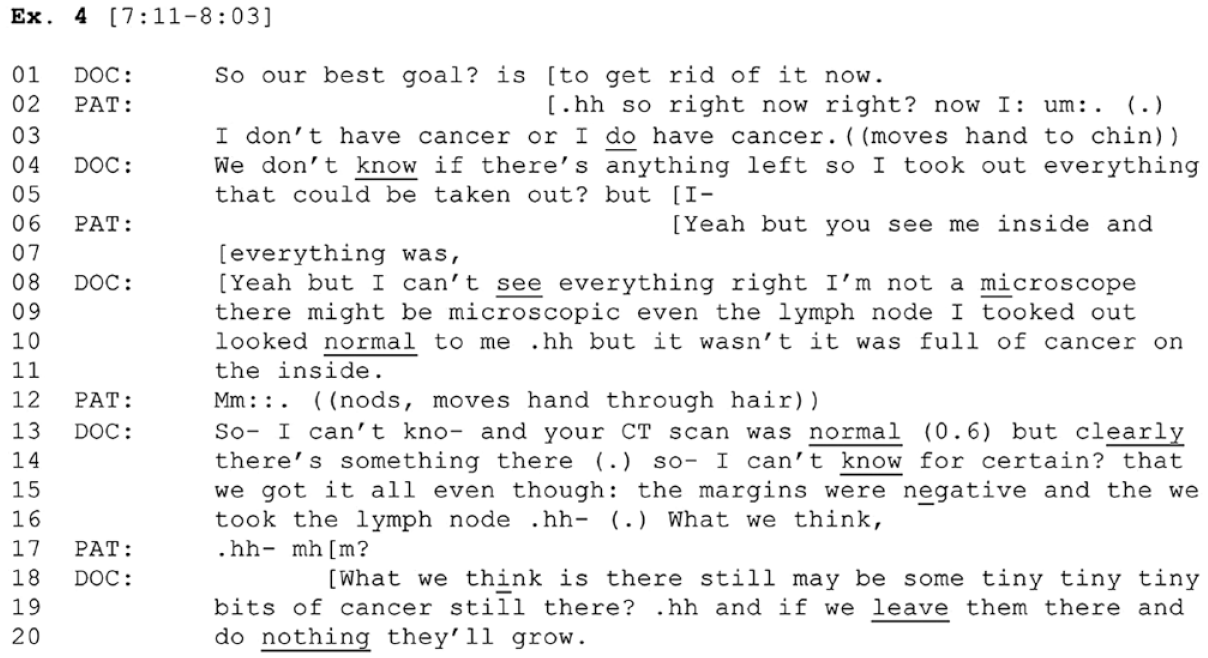
Extract 4.
This is met with the patient’s rejection of that response, “but you see me inside” Extract 4 (Figure 5) (line 06). At this point, an answer to the question—whether the patient has cancer remaining—is still relevant. The doctor responds with further uncertainty, that she is not a microscope so was unable to see everything during surgery, and provides an account for her recommendation, that “there still may be some tiny tiny tiny bits of cancer still there? and if we
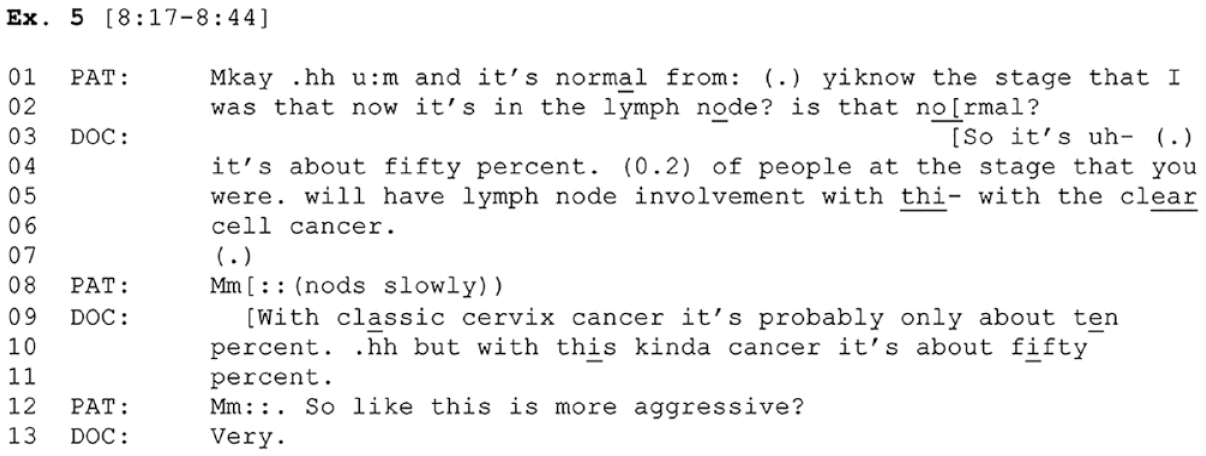
Next, the patient continues to receive news about the serious nature of her diagnosis from the doctor in a piecemeal way (Extract 5; Figure 6). Following more treatment endorsements by the doctor and patient questions about side effects, another piece of diagnostic news is delivered, this time drawing contrast between this type of cancer and “classic” cervical cancer. The news again arrives in second position, occasioned by a question from the patient about whether the cancer’s spread to a lymph node is “normal” for her stage (Extract 5 (Figure 6) (line 01). Embedded in this question is a concern with the cancer’s behavior. In response, the doctor offers more diagnostic news, this time explaining that 50% of cases with this diagnosis spread to the lymph node, whereas “classic” cervical cancer spreads only 10% of the time. This informs the patient of the relative likelihood of spread. The patient responds to this news through clarification, “so like this is more aggressive?” Extract 5 (Figure 6) (line 12), to which the doctor offers a strong affirmative, “Very” Extract 5 (Figure 6) (line 13). Here, the patient reveals that in addition to not sharing her doctor’s presupposition that she still needs treatment, she also lacks information that this cancer is aggressive.
Extract 5.
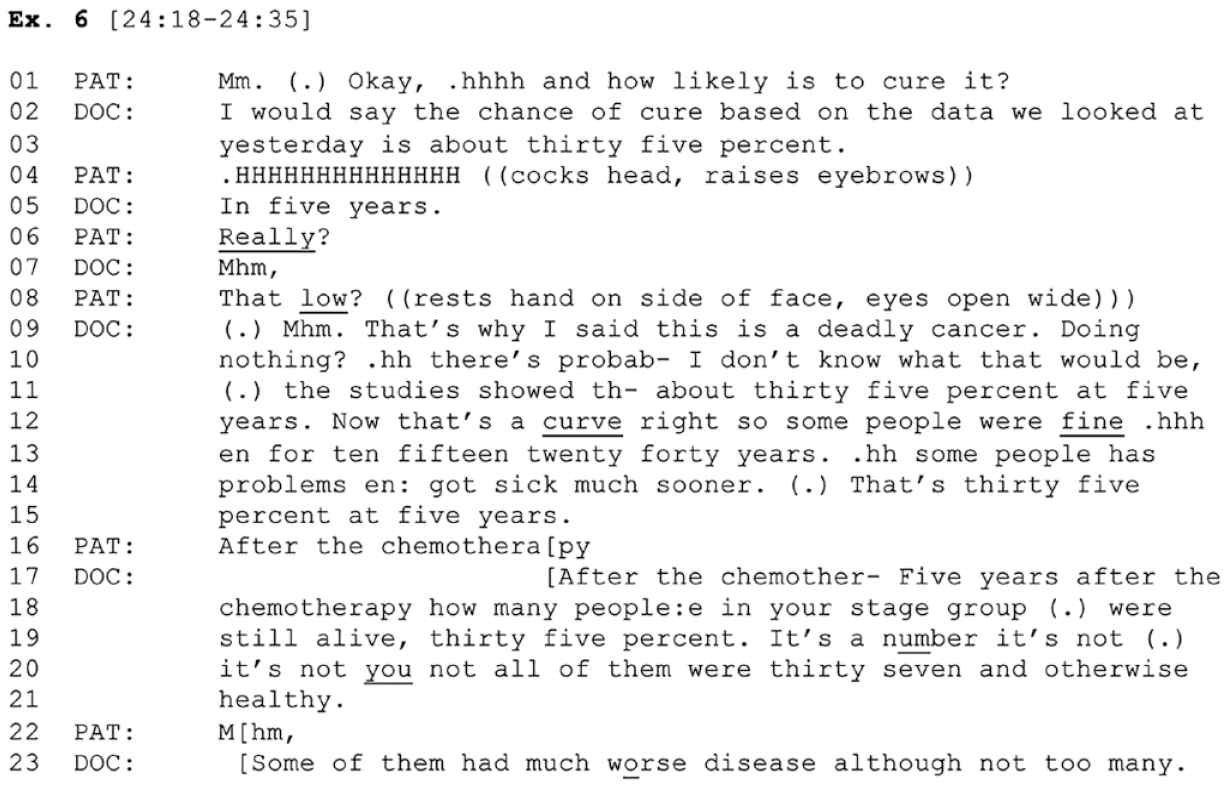
After further lobbying without acceptance happens across several more minutes, the patient asks about the likelihood of cure (Extract 6; Figure 7). In response, the doctor puts forth that the patient has a 35% chance of cure. The patient responds with surprise using a pronounced in-breath Extract 6 (Figure 7) (line 04). The doctor next expands that this prognosis is a five-year estimate, which the patient registers with a newsmark, “Really?” Extract 6 (Figure 7) (line 06), and then explicates her reaction, “That
Extract 6.
In this section, we have argued that because the patient does not have access to the same diagnostic presuppositions as the doctor at the time of the recommendation due to a lack of diagnostic information provided prior to the recommendation, the recommendation is met with resistance rooted in the patient’s lack of understanding the recommendations’ grounds. The patient’s actions are hearable as resistance because she receives diagnostic news postrecommendation in sequential positions normatively designed for acceptance of treatment. Throughout this sequence, the doctor has delivered five different pieces of diagnostic news to the patient—notably after the recommendation—as either counters to resistance or in response to the patient’s questions about treatment. Because news is being leveraged to push for a position as part of a counter or as an answer to a question, there is no sequentially relevant slot for the patient to realize it as news or respond to it as such. This leaves news delivery sequences unresolved or occasions the patient to respond with further questions, demonstrating resistance.
When Advocating for Treatment Turns Adversarial
In the prior section, we showed that the particulars relevant to the patient’s diagnosis and thus relevant to a treatment decision emerge after the treatment recommendation and across several minutes rather than being provided by the doctor before the recommendation as justification. This sets up the patient to respond with resistance, as she deals with the receipt of new information in sequential slots designed for acceptance. This section will analyze a subsequent consequence of the doctor delivering diagnostic news out of sequence. Here, we focus on the way the doctor responds to resistance, ultimately showing that these diagnostic informings postrecommendation produce an environment where advocating for treatment turns adversarial. In what follows, we show the doctor employing a variety of strong persuasive techniques to steer the patient toward acceptance. This leads to an adversarial environment because the patient is being pushed to treat in the context of learning information about her diagnosis.
Recall that after the doctor delivers her treatment recommendation, the patient registers surprise and minimal resistance. The doctor responds with an account, that she examined the patient’s cancer postsurgery and learned that the cancer is HPV-related and thus “very rare.” In Extract 7 (Figure 8; shown earlier as Extract 3, Figure 4), the doctor next continues with an upshot, that the treatment is “likely to work” (Figure 8) (line 01). Following no response from the patient, the doctor explicitly indexes her informing as good news, again receiving no uptake. The doctor shifts to offer a hypothetical scenario should the patient not accept the recommendation, orienting to a possible refusal: If she does not pursue treatment, the patient will have “a lot of problems.” As discussed earlier, the doctor explains to the patient she has a “serious diagnosis.” She then continues her efforts to counter the patient’s resistance, setting forth an alternate outcome should the patient not accept: The cancer will recur, and “it will be deadly.” This practice, “invoking death” (Tate 2020), is a form of strong leverage to push for acceptance in resistant environments. In their article, Stivers and Timmermans (2020) explicitly define this practice as a “threat.” Importantly, the doctor moves to this practice even before the patient has demonstrated active resistance to the recommendation. Here, as in subsequent cases in this section, the doctor pushes back on the patient’s resistance in the same turn that she is providing new diagnostic informings, linking news delivery with adversarial interactional practices advocating for acceptance.
Extract 7.
The patient next asks about other treatment options (Extract 8; Figure 9). After the doctor responds that there are no other recommended treatments, the patient reveals the grounds for her question: “Because I am really scared of chemo” Extract 8 (Figure 9) (line 05), further specifying her concern about kidney and liver failure. Here, she demonstrates what Stivers and Timmermans (2020) label “fear based” resistance. The doctor counters this resistance in overlap through coaxing (Stivers and Timmermans 2020) by reassuring the patient that they are “very careful” and can give “hydration” and “special medicines” to minimize chemo’s effects. She concedes the possibility of complications with treatment, although counters that concern through emphasizing frequent monitoring and her team’s experience: “We know how to give the medicine” Extract 8 (Figure 9) (lines 16 and 17). She next upgrades her persuasion to a threat-oriented response, again orienting to potential refusal, “if we do nothing? kidneys and liver failing will not be your problem” Extract 8 (Figure 9) (lines 17 and 18), implicitly linking back to her earlier comment that should the patient not treat, she will die. At the same time, she minimizes the patient’s concerns about treatment affecting her organs. After a pause in which the patient does not offer uptake Extract 8 (Figure 9) (line 18), the doctor reveals, “what
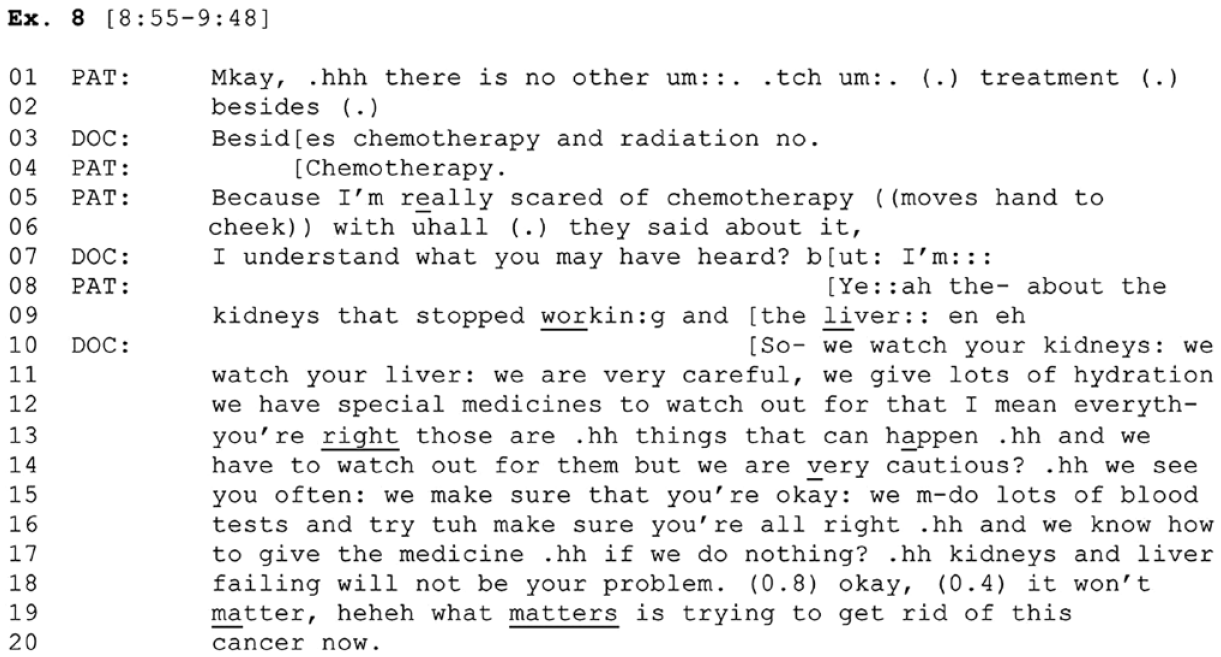
Extract 8.
The patient continues with questions (Extract 9; Figure 10), building off the doctor’s earlier statements implicating the cancer’s severity through its ability to spread to vital organs Extract 9 (Figure 10) (line 01).
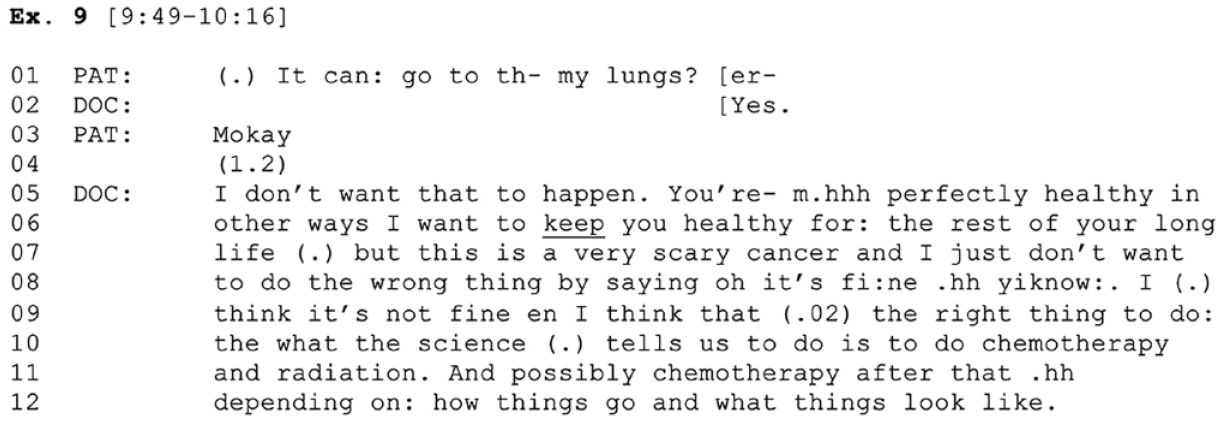
Extract 9.
After the doctor’s yes response, which the patient registers Extract 9 (Figure 10) (lines 02 and 03), the doctor continues to push for treatment by rooting her recommendation in a desire to keep the patient healthy “for the rest of [her] long life” Extract 9 (Figure 10) (lines 06 and 07), implying that not only would the treatment work short term, but it would also prolong life long term. Here, the possibility of spread is again used to counter the patient’s position by reinvoking the doctor’s own role in keeping the patient healthy. Next, the doctor puts forth that it would be “wrong” of her to accept the patient’s position, “by saying oh it’s fi:ne” Extract 9 (Figure 10) (line 09). Then, she positions treating as the “right thing to do:” Extract 9 (Figure 10) (line 09) and, like in Extract 1, situates herself as an institutional actor guided by scientific evidence Extract 9 (Figure 10) (line 10). In this turn, the doctor responds to resistance with a moral valence in favor of treatment, implying some objective moral reality in which accepting treatment is “right” and refusing is “wrong.”
The patient next asks the doctor whether she herself would pursue chemotherapy in this situation (Extract 10; Figure 11). The doctor provides a yes response, accounting there is “n
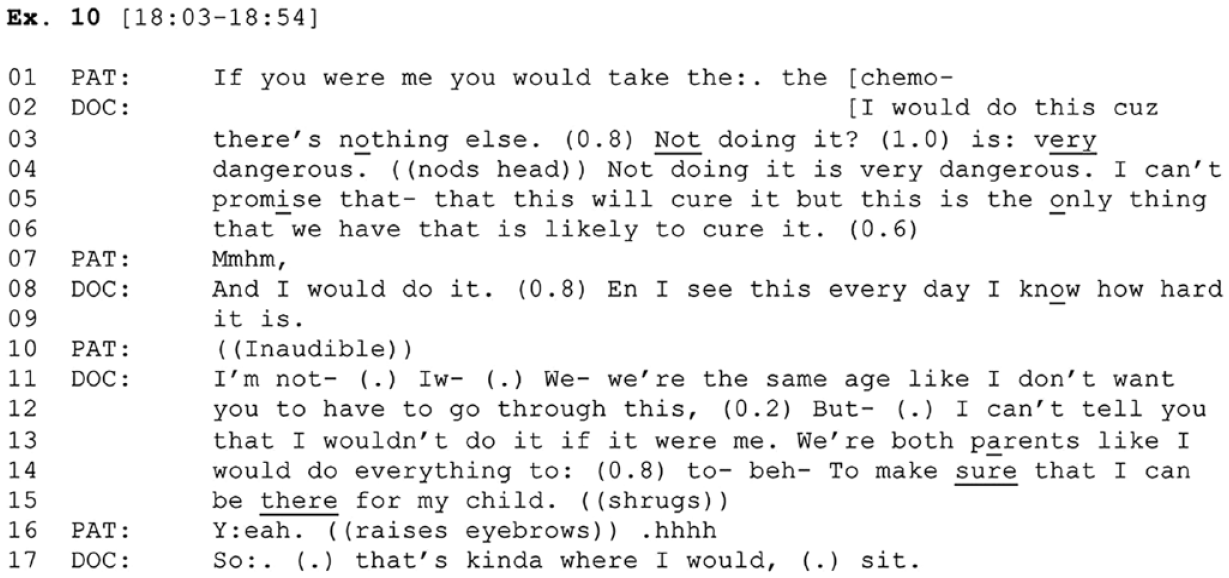
Extract 10.
The patient continues questioning (Extract 11; Figure 12), this time revealing more specific concerns about the treatment’s potential to kill her. This is an upgrade from the earlier concern about treatment impacting organs (Extract 8; Figure 9). The doctor concedes yet minimizes this outcome by drawing on her own experience, “I’ve never seen it” Extract 11 (Figure 12) (line 02). After the patient responds with a sigh Extract 11 (Figure 12) (line 03), the doctor adds on “I don’t think so” Extract 11(Figure 12) (line 04), pulling back on her prior stance of never having seen this outcome. Her turn launch includes laughter Extract 11 (Figure 12) (line 04), further modulating her original stance (Shaw, Hepburn, and Potter 2013). The doctor continues, linking her professional identity to protecting the patient from adverse side effects, “I mean I- w- that’s my job is to prot
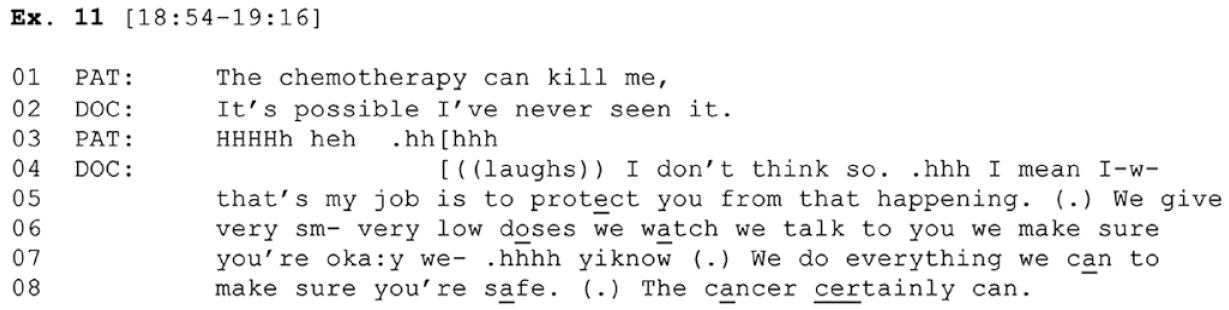
Extract 11.
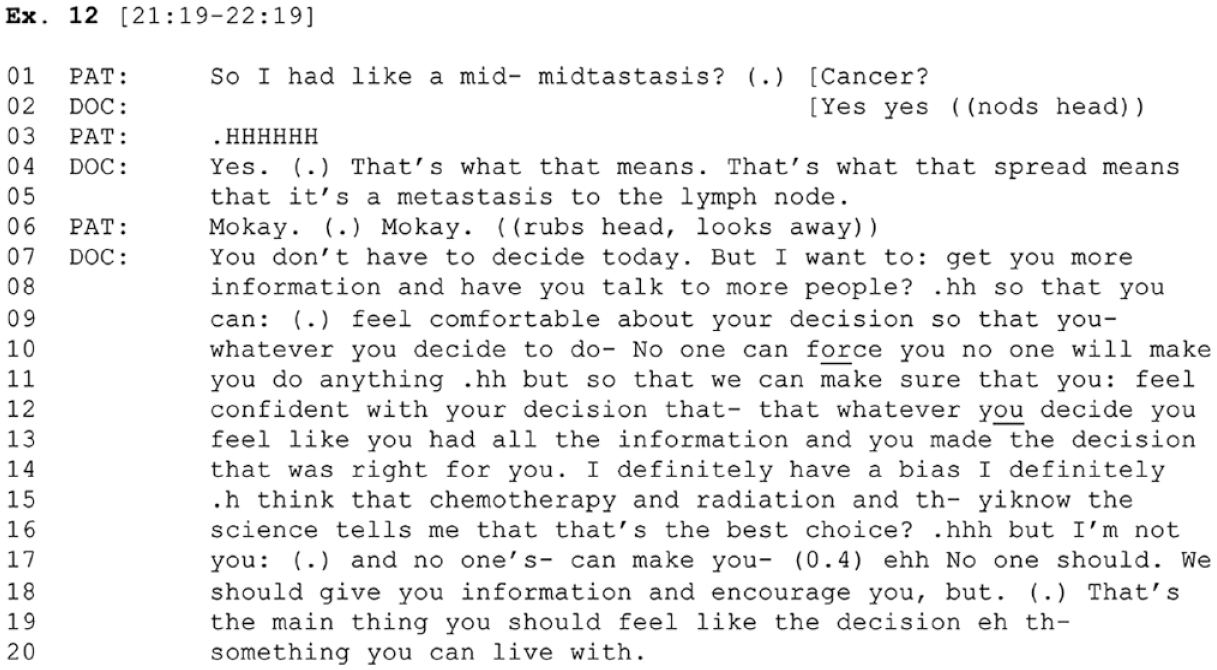
The patient subsequently asks the doctor about alternative treatments, which the doctor explains have their own set of bad side effects and can worsen disease. Next, in Extract 12 (Figure 13), the patient transitions to questions about the severity of her cancer, this time asking whether it is metastatic (line 01). Recall the doctor earlier produced diagnostic informings explaining that the cancer had spread (Extracts 3–5; Figures 4–6). The patient’s question here suggests she has not yet linked this to a metastatic diagnosis and that such a label is meaningful. The doctor confirms the patient has metastatic disease. The patient registers this with an emphatic in-breath (line 03), treating this information as newsworthy (Heritage 1984a). The doctor elaborates, making the explicit link between metastatic disease and its spread to a lymph node. In response to the patient’s acknowledgement (line 06), the doctor steers the discussion toward the visit’s closure, explaining that a decision does not need to be made at this visit (line 07). This position stands in contrast to earlier exchanges (Extracts 4 and 8; Figure 5 and 9) in which the doctor emphasized that the cancer needed to be treated “now.” The doctor continues with an account that repositions her role as one that delivers information and connects the patient with other experts so that she can feel comfortable with her decision (line 10). The doctor moves on to affirm the patient’s own deontic primacy over the recommendation (Stevanovic and Peräkylä 2012), in this case, her control over whether she accepts and implements treatment. She reframes her past actions as motivated by ensuring the patient is informed and confident in her decision rather than motivated by coercion. This position stands in striking contrast with actions produced in prior extracts.
Extract 12.
In the first section, we reviewed how the absence of diagnostic informings before the recommendation occasioned a resistant patient, exemplified through delaying acceptance through pauses and questioning. In this section, we reviewed a second consequence of the absence of informings, one where the doctor meets patient resistance with adversarial, rather than affiliative, treatment advocacy tactics. This is accomplished largely through addressing the consequences of refusing rather than the reasons to accept by invoking death at multiple points. This is also achieved through linking acceptance to morality, either as an objective “right” choice or as a responsible parenting decision.
Further compounding the nature of these practices is that they are produced as the patient learns about her diagnosis and the warrant for treatment. Of note, the doctor does not incorporate strategies that conversation analysts have found facilitate acceptance, such as mobilizing clinical reasoning prior to delivering the recommendation (Heritage and Stivers 1999; Peräkylä 1998) or using a perspective display sequence to prompt the patient to first indicate their own understanding and then drawing on this talk to more gently break delicate news (Maynard 1989, 1996). Instead, the patient’s resistance, conditioned by the doctor’s sequentially out-of-order news delivery, is met with adversarial counters.
Discussion
Studies of changes in doctor–patient relationships can and do take many forms, but ultimately, any understanding of evolution in this arena is incomplete without empirical examination of in situ interaction. We use conversation analysis of a single case to examine how treatment resistance is dynamically constituted in a high-stakes oncology consultation. In this case, an otherwise healthy 37-year-old patient receives a life-threatening cancer diagnosis with a poor prognosis, and the doctor recommends treatment that the patient does not accept. At first glance, this interaction may be assumed as driven by a patient who is not inclined to cooperate with her physician or as simply a chaotic and disorderly conversation. To the contrary, our detailed analysis of this unusual case shows how interactional order is sustained even when there is unexpected conflict and misunderstanding.
In this case, sustained conflict originates with the doctor—the person best positioned to help the patient. The doctor, seeking treatment acceptance, paradoxically sets the patient up to resist as she fails to establish diagnostic grounds prior to proposing treatment. The doctor subsequently meets patient resistance with predominantly coercive efforts. Thus, it is the doctor, not the patient, who conditions the displays of resistance, which, in turn, block acceptance. Ultimately, no treatment decision is made during this visit. Due to its atypical nature, the single case we analyze here offers novel but powerful leverage on questions of how resistance can be conditioned and sustained collaboratively by both patients and physicians, much in the vein of deviant case analysis in qualitative methods generally.
The patient’s resistance and the doctor’s assertions of authority are both sequential accomplishments, contingent on each other’s utterances. The patient is heard as resistant as she tries to make sense of an aggressive treatment recommendation when she did not possess basic information about her diagnosis. In a standard news delivery sequence, there would be an interactional slot for showing receipt of diagnostic news (Maynard 1996). Here, however, diagnostic information is embedded in the recommendation, thus omitting a position for the patient to realize news. She is thus put in the difficult position of trying to understand her diagnosis in a conversational spot designed for treatment acceptance. As the patient struggles to understand her situation, her responses are heard by the doctor as resistant, who mobilizes adversarial strategies to leverage her position, such as persuasion and threats. Far from being an extrinsic characteristic of the patient, her resistance is made possible by the interactional strategies mounted by the doctor. This analysis shows how real-time interactions matter for understanding heralded concepts such as patient engagement, resistance, and medical authority.
Extant studies have shown that physician authority is robust despite patients’ diverse interactional strategies for resisting recommendations. Although others (Heritage and McArthur 2019; Stivers and Tate 2023) have found in an era of increased patient autonomy and empowerment that diagnoses are less important than symptom relief in lower stakes environments, here the patient holds the doctor accountable for diagnosis because a burdensome treatment is proffered without her experience of symptoms. As a result, she raises concerns about work, symptoms, organ failure, and treatment burdens that may be viewed as moot to the doctor, who argues that the patient will die without treatment. In terms of medical help gone awry, the patient seeks help for a problem defined differently by the doctor.
Previous research has shown how doctors can be involved in shaping resistance. Stivers (2005a) has found that doctors in pediatric primary care condition resistance through the way they recommend treatment. Recommendations for a particular treatment (e.g., “I’d just give her Robitussin”) were less likely to get resistance from parents than recommendations against treatment (e.g., “We can’t give her stuff like Sudafed”). We similarly show how the format of a recommendation can condition patient resistance. However, our work extends current knowledge in two ways. First, we demonstrate how doctors can condition resistance through the embodiment of presuppositions about what the patient already knows. Second, we identify mechanisms by which doctors can play a role in not only establishing patient resistance but also sustaining it over the course of a conversation, even in the face of nonalignment.
Ideally, an informed medical decision should involve interactants who have access to the same information before a decision is made to avoid problems like the ones that arise in our analysis. Yet this ideal may be a challenge given research demonstrating not only the persistence of asymmetry in doctor–patient interactions (Pilnick and Dingwall 2011) but also the lack of space in oncology to talk about what results mean (Singh et al. 2017). Our results underscore the importance of the diagnostic moment in serious illness (Jutel 2011) and the intimate interactional relationship between diagnoses and treatments.
Because this is a cross-sectional data set, we do not know the ultimate outcome of this patient’s treatment. At the very end of the interaction, the doctor closes the visit by asking the patient to call the radiation oncologist so she can get more questions answered. The patient responds “okay” and is reminded of the time-sensitive nature of the treatment—ideally, she should begin treatment in three weeks. The doctor also reminds the patient about an appointment to follow up in two weeks. Because of the unusual nature of this case, the first author followed up with the doctor six months later about this patient, who she learned did not return to this doctor or the radiation oncologist for treatment. She could have later decided to pursue treatment with this doctor, found another doctor to administer treatment, or decided to not treat. The doctor’s adversarial approach to advocating for treatment could have served to alienate the patient and may have contributed to the patient not following up with this doctor.
At the very least, this case demonstrates a delay in treatment uptake in the context of aggressive cancer, which could have implications for this patient’s morbidity and/or mortality. Such measures are relevant outcomes in large clinical data sets, evaluating treatment efficacy on the population level. Yet the origin of that outcome, the fundamental source of treatment delay, begins with understanding what happens when two people—a patient and the expert from whom she seeks help—enter a decision-making exchange.
In such an environment, where days or weeks may matter to intervene before disease potentially spreads and prognosis potentially worsens, consequences for resisting pose challenges. Doctors may be particularly invested in ensuring patients accept their proposed plan. Yet patients are being asked to undergo an extraordinary amount of treatment, one with substantial side effects that will likely render them temporarily disabled and doing so in an era of increased engagement. This sort of tension lays bare the co-constitution of resistance, in which both interactants are likely to be strong advocates of their own agendas. Although other scholars have established physicians’ authority and strategies to condition patient compliance, this work underscores that doctors can also condition patient resistance, even in life-or-death scenarios. This paradox, in which the doctor can both recommend life-prolonging care and condition resistance to it, has broad relevance beyond cancer treatment; it also can help us understand other doctor–patient decisional conflicts, for instance, medication nonadherence, delaying emergent care, and vaccine refusal.
Footnotes
Appendix A
Acknowledgements
We offer many thanks to Tanya Stivers and Rebecca Schut for their invaluable feedback in the early stages of this work and to the anonymous reviewers that made this work stronger. We would also like to express our gratitude to the doctors who allowed us to collect video data in their clinics and to the patients who welcomed us into often challenging and vulnerable treatment experiences.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by a National Institute on Aging grant (5P30AG066619-03).