
Abstract
Early initiation and consistent use of prenatal care is linked with improved health outcomes. American Indian birthing people have higher rates of inadequate prenatal care (IPNC), but limited research has examined IPNC among people living on American Indian reservations. The current study uses birth certificate data from the state of Montana (n = 57,006) to examine predictors of IPNC. Data on the community context is integrated to examine the role of community health in mediating the associations between reservation status and IPNC. Results suggest that reservation-dwelling birthers are more likely to have IPNC, an association partially mediated by community health. Odds of IPNC are higher for reservation-dwelling American Indian people compared to reservation-dwelling White birthers, highlighting intersecting inequalities of race and place.
Nationally, pregnancy-related mortality rates among American Indian/Alaskan Native (AI/AN) people are twice the rate of White people (29.7 vs 12.7 per 100,000 live births; Petersen et al. 2019). Despite declining AI/AN maternal death rates, this gap has widened over time (Kozhimannil et al. 2020). Pregnancy-related deaths are largely considered preventable, with complications related to cardiovascular conditions, hemorrhage, and hypertensive disorders higher among AI/AN people compared to White people (Heck et al. 2021). Likewise, AI/AN infants have higher rates of preterm birth and low birth weight and die nearly twice the rate of White infants (March of Dimes 2022). Accessing health care during pregnancy (prenatal care [PNC]) can lead to the detection and treatment of complications found during pregnancy and improved patient education. AI/AN birthing people experience fewer prenatal visits (Osterman and Martin 2018), enter PNC later in their pregnancy (Sebens and Williams 2022), and report less satisfaction with their PNC timing (National Conference of State Legislatures [NCSL] 2021) compared to their White counterparts. Reservation-dwelling AI/AN people face greater community health obstacles that are known to affect timely and adequate PNC access (Advisory Committee on Infant and Maternal Mortality [ACIMM] 2022; Baldwin et al. 2002).
Access to care is a critical element to improving health; however, disparities exist, with AI/AN birthing people experiencing elevated rates of inadequate prenatal care (IPNC) utilization compared to their non-Hispanic White counterparts (Johnson, Call, and Blewett 2010; Osterman and Martin 2018). Yet little is known on this topic, such as (1) whether living on an American Indian reservation is associated with less adequate PNC, (2) how reservation residence is linked to IPNC for people with different racial identities, and (3) whether dimensions of the community’s health may explain elevated rates of IPNC among AI/AN and reservation-dwelling people. The current study aims to address these gaps in the literature using logistic regression models to predict the odds that a person experiences IPNC. Birth certificate data from the state of Montana are leveraged, with measures of community health integrated to examine mechanisms underlying disparities in PNC utilization facing AI/AN and reservation-dwelling people.
Background
Adequate versus Inadequate Prenatal Care
Healthy pregnancies are key to promoting healthy people, births, and babies. Ideally, PNC is initiated in the first trimester, helping to educate pregnant individuals, identify perinatal risk factors, alleviate preventable risks leading to the dyad’s morbidity and mortality, and treat complications (American Academy of Pediatrics and American College of Obstetricians and Gynecologists 2017). The three-delay conceptual model integrates individual, provider, and system factors to articulate that delay in the provision of timely and appropriate medical treatment is a contributing factor for maternal mortality, with delays occurring across three realms: delay in seeking care, delay in arrival at an adequate health care facility, and delays in receiving adequate care (Thaddeus and Maine 1994). Delays in initiating and maintaining consistent care throughout pregnancy reduce the adequacy of PNC. PNC is said to be adequate when it is initiated during the first trimester and utilization meets the recommended number of care visits following care initiation (Kotelchuck 1994). IPNC has been linked with increased risk of poor birth outcomes, including preterm delivery and infant mortality (Partridge et al. 2012).
Root Causes of Perinatal Disparities
Much of the current knowledge surrounding AI/AN disparities within PNC examines individual factors, including culture, geographic location, and socioeconomic status (Burns, DeAtley, and Short 2023). Emerging scholarship on perinatal health disparities endeavors to understand root causes, largely focusing on Black perinatal health inequities (Davis 2019; Gadson, Akpovi, and Mehta 2017). Root causes of health inequity, including inequitable PNC among AI/AN people, are likely found at the intersections of social determinants of health and structural inequities (structural racism; Baciu et al. 2017). The racist legacy of colonialism that has gravely impacted the AI/AN population historically manifests today through disparate maternal and infant outcomes, as characterized by Palacios and Portillo (2009), wherein daily ongoing disenfranchisement (weathering) and reverberating collective historical atrocities (historical trauma) negatively impact AI/AN perinatal health.
For reservation-dwelling AI/AN people, structural inequities and structural racism are manifested in “place” through historical and contemporary policies and practices that continue to constrain the health of AI/AN people. Underlying structural inequities become “the context in which health inequities exist” (Baciu et al. 2017). Community health encompasses dimensions of the contextual environment of a place that may affect the health and health care utilization of individuals residing in these environments, including socioeconomic resources, access to and quality of health care, and patterns of health behaviors and outcomes in the community (Hillemeier et al. 2003). Integrating information about community health situates individuals within the environments they live in to better understand how intersecting inequities related to place and race impact health. Intersectionality highlights how interconnected, overlapping, and interdependent social identities and social locations shape individual experiences and systematic inequities (Crenshaw 2017). Accounting for place, in this case, reservation residence, reflects the potential of situated intersectionality to understand health inequities (Bambra 2022), including in PNC utilization.
PNC Disparities
Racial disparities exist within the adequacy of PNC. Nationally, AI/AN people enter PNC during the first trimester at lower rates than White people (63% vs. 82.3%, respectively), have higher rates of late PNC (9.2% vs. 3.3%) and no PNC (3.3% vs. 1.1%; Osterman and Martin 2018), and are more likely to report being dissatisfied with the timing of initiation (Sebens and Williams 2022). Between 2017 and 2019, 64.4% of childbearing AI/AN individuals entered early PNC, accounting for the lowest rate of early PNC entrance of U.S. racial groups, including White (82.4%), Asian (80.5%), Hispanic (72.4%), and Black (67.3%) birthing people (NCSL 2021). Nationally, rates of IPNC are twice as high among AI/AN individuals compared to White individuals (44.6% vs. 23.9%, respectively, in 2000 to 2002), with states in the West and Midwest experiencing even larger disparities (Johnson et al. 2010) and AI/AN individuals living in rural areas at greatest risk (Baldwin et al. 2002).
Although adequate PNC is not the panacea for racial disparities found within perinatal outcomes (Thurston, Fields, and White 2021), research suggests that elevated rates of IPNC help to explain higher rates of preterm birth among AI/AN and other racially minoritized people (Sparks 2009). Gadson et al. (2017) suggest that social determinants of health and racism account for lower PNC utilization and poor birthing outcomes among Black birthing people. Structural racism is also believed to account for much of the general poor health outcomes among AI/AN people (Solomon et al. 2022). AI/AN strength and resilience belie their continued presence and striving for thriving family and community health. This resilience is a dynamic, fluid process; evident throughout the life course; and accessed through cultural knowledge and practice (Oré, Teufel-Shone, and Chico-Jarillo 2016) manifesting within social support, cultural engagement, a holistic worldview, navigating dual cultural identities, and avoiding the victim identity through cultural strength (Teufel-Shone et al. 2018). Despite the wealth of resilience and strength, reservation-based AI/AN people face systemic barriers when accessing PNC, including social, economic, political, and geographic factors. IPNC has been linked to individuals who are younger, uninsured, less educated, experience unintended pregnancies, engage in substance use, live in more economically deprived areas, and have previous live births (Gadson et al. 2017; Partridge et al. 2012). AI/AN history is marked by centuries of systemic racism, discrimination, and systematic disenfranchisement from cultural, religious, economic, environmental, and bodily sovereignty that has contributed to heightened rates of poverty and unemployment, lower rates of education, and higher rates of self-medication through substance use (ACIMM 2022; Huyser, Takei, and Sakamoto 2014), thereby elevating their risk for IPNC. Furthermore, AI/AN birthers are more likely to be younger, uninsured, unmarried, have unplanned pregnancies, and less likely to have private insurance (Osterman et al. 2023; Raglan et al. 2016).
Reservations and Systemic Barriers to Prenatal Care
Reservations embody the collective AI/AN history in a physical form and serve as a reminder of historical and political practices aimed at isolating and marginalizing this population. From extermination to assimilation to termination, reservations are the physical expression of a living history that has repercussions today. The historical and contemporary trauma of Indigenous peoples due to colonization, genocide, forced relocation, systemic racism, and cultural erasure has profound consequences for the health of AI/AN people and reservation communities, including through its impact on health care utilization (Palacios and Portillo 2009; Pool and Stauber 2020). For example, the legacy of reproductive control (e.g., forced government-sponsored sterilization) and infant separation policies (infants separated from substance-using parents) contribute to contemporary mistrust between AI/AN people and care providers (Call et al. 2006; Johnson 2020). Empirical research has not examined how residence on American Indian reservations is associated with experiences of IPNC, although research points to several barriers to seeking perinatal care for reservation-dwelling individuals (Hanson 2012; Johnson 2020; Sebens and Williams 2022; Thorsen et al. 2022). Qualitative research has identified several obstacles to PNC for AI/AN birthing people, including lack of reliable transportation, competing economic and/or familial concerns, dissimilar communication styles, provider mistrust, long wait times, inconsistency of providers, and scarce access to culturally congruent care (Brooks-Cleator, Phillipps, and Giles 2018; Hanson 2012; Johnson 2020; Sebens and Williams 2022).
Geographic barriers to perinatal care for AI/AN and reservation-dwelling birthers are substantial across several metrics (Johnson et al. 2010; Rayburn, Richards, and Elwell 2012; Thorsen et al. 2022, 2023). The U.S. government forced relocation of AI/AN peoples onto reservations, lands that were strategically chosen for geographical isolation and low resources, and the continual lack of economic and social development in these areas has contributed to persistent social and economic marginalization of reservation-dwelling AI/AN people residing in these geographically remote areas. Labor market opportunities are limited, unemployment and underemployment abound, wages are meager, and poverty is omnipresent (Davis, Roscigno, and Wilson 2016), which impacts food security, housing, and health coverage. These sources of structural racism manifest in challenges accessing care and experiencing optimal health. Birthing people residing on reservations live within and among these circumstances. These factors converge and compound. AI/AN race and community context (accounting for exposure to social, economic, political, and geographical determinants of health), represented as place, shape access to early and consistent PNC. To understand how place impacts health and health care utilization for AIAN people, a focus on reservation residence is warranted. The current study considers how the context of community health on reservations impedes the adequacy of PNC for people residing on them.
Indian Health Service as a Barrier to Adequate Prenatal Care
In exchange for signing treaties that ceded land to the U.S. government, the Indian Health Service (IHS) was created to provide care for tribally enrolled AI/ANs living within IHS service areas. Yet chronic inadequate funding of IHS clinics and facilities has consistently been cited as a key contributing factor to poor health outcomes among AI/AN people (Warne and Frizzell 2014). Challenges with the IHS health care delivery system erode patient–provider continuity in care and case management support for complex cases (Cromer, Wofford, and Wyant 2019). For those relying on IHS health coverage for PNC, geographic remoteness, dwindling IHS clinic sites, long wait times, provider vacancies, fear of reported substance use in pregnancy, substandard care, and lack of provider accountability likely contribute to later initiation of PNC (ACIMM 2022; Raglan et al. 2016).
Prior research confirms regional differences in rates of IPNC among rural and urban AI/AN populations living within different IHS service areas, and AI/AN individuals residing in non-IHS serving counties were found to have the lowest rate of IPNC (Baldwin et al. 2002). This previous study, however, uses birthers’ county of residence to identify IHS service regions, which includes areas both on and off reservation, and did not examine birthers’ residence on reservation. The current study uses self-reported residence on an American Indian reservation to help identify inequities in the adequacy of PNC for reservation-dwelling birthers, enabling insight into the intersecting inequities of race and place.
Current Study
The current study uses data from Montana to examine how racial identity, rurality, and reservation residence (and their intersections) are associated with the likelihood of experiencing IPNC. Montana is a useful case study to examine PNC inadequacy for these populations. The majority of Montana’s population lives in rural areas (65%), compared to the minority of the U.S. population (14%; United States Department of Agriculture Economic Research Service 2020). Montana has a large AI/AN population (6.7% of the population; 78,000 people) with 12 federally recognized tribal nations and seven American Indian Reservations (Montana Governor’s Office of Indian Affairs n.d.; United States Census Bureau 2020). Many tribally enrolled members (43%–73%) in Montana live on or near their tribal reservation (Montana Governor’s Office of Indian Affairs n.d.).
Perinatal care access in Montana is quite limited and marked by racial inequities. Fifty percent of counties in Montana lack a birth center, obstetric provider, or hospital offering obstetric care, compared to 32.6% of counties across the United States (Brigance et al. 2022). Relative to other states in the contiguous United States, birthing people in Montana drive the farthest on average to access obstetric care (Rayburn et al. 2012), with disparities in access for AIAN and reservation-dwelling people (Thorsen et al. 2022, 2023). Previous research leveraging IHS service region status as a proxy for reservation status identified the Billings service region (which includes Montana) as the area with the highest rate of IPNC (Baldwin et al. 2002). Together, these results situate Montana as a useful site for examining how aspects of place, including rurality and reservation dwelling, intersect with racial identity to shape the utilization and adequacy of PNC. Results from this study may provide insight for scholars, public health policy makers, and practitioners that serve rural American Indian populations and work with reservation communities.
Our study addresses several research gaps. First, limited research has examined IPNC for reservation-dwelling birthers. Prior research has only examined residence in IHS service sites (which cover wide geographic areas that include nonreservation land; Baldwin et al. 2002), whereas this study utilizes self-reported residence on a reservation. Second, our study furthers previous nuanced findings of contributing factors leading to heightened rates of IPNC for AI/AN birthers across different geographic areas (Johnson et al. 2010; Raglan et al. 2016) by considering geographical and maternal factors. Finally, this study integrates data on the health of the community context in which birthers reside to examine whether higher rates of IPNC for AI/AN and reservation-dwelling birthers are mediated by exposure to social, economic, and geographical determinants of health, which has not been examined.
Data and Methods
Data
Montana birth certificates from 2014 to 2018 (n = 60,461) constituted the data on individuals who gave birth during this period. Nonresidents of Montana (n = 964; 1.6%) and those missing values on the dependent or independent variables (n = 2,494; 4.1%) were excluded using listwise deletion for a final sample size of 57,006. Stratified models were further limited to non-Hispanic White (n = 47,408) and AI/AN (n = 6,485) birthers and non-Hispanic White or AI/AN birthers living on (n = 5,305) or off reservation (n = 48,588). County-level data about the health and well-being of birthers’ residential county were derived from the Robert Wood Johnson Foundation (RWJF) County Health Rankings 2018 data set. This data set integrates county-level data from a variety of sources, including the National Center for Health Statistics (NCHS; mortality and natality files), Behavioral Risk Factor Surveillance System, and Area Health Resource File, among several others. For full information on data sources, see Appendix A in the online version of the article and https://www.countyhealthrankings.org/. The sample for models incorporating county-level health metrics was further restricted to those with nonmissing data on county health variables (n = 56,471). County-level data were linked to individual birthing people based on the reported county of residence at the time of the birth.
Measures
Dependent variable
Access to PNC was measured by the Kotelchuck adequacy of prenatal care index, which factors the month PNC was initiated and comparison between the actual number of visits from initiation to delivery with the expected number of visits based on American College of Obstetricians and Gynecologists (ACOG) recommendations; a ratio of less than .5 is considered inadequate (Kotelchuck 1994). The dependent variable, derived from this index, measured whether or not a birther was reported on the birth certificate to have received IPNC (0 = no, 1 = yes). Birthers with a value of 0 for “no PNC” or 1 for “inadequate PNC” on this index were classified as having IPNC. Supplementary analyses were conducted limiting the sample to those who received some PNC. Results were similar and are available on request.
Independent variables
Data for individual-level variables came from birth certificates. Sociodemographic characteristics included self-reported maternal race-ethnicity (AI/AN, non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, and Hispanic), education (less than high school, high school, some college, college graduate or more), and age (in years). Two measures of location were used: whether the mother reported on the birth certificate to be living on an American Indian reservation (0 = no, 1 = yes) and rurality of residence, measured at the county level using the Rural–Urban Continuum Code (RUCC), which classifies counties based on both population size and remoteness. Information on the associated RUCC of the county of residence reported on the birth certificate was derived from the United States Department of Agriculture Economic Research Service (n.d.) RUCC classification data. Six RUCC categories existed in our data and are described in table notes. Two binary measures captured aspects of social support available to the birthers: whether the birther used the Supplemental Nutrition Program for Women, Infants, and Children (WIC) and if they were married at any time during pregnancy or birth. Characteristics of the pregnancy reported on the birth certificate include binary indicators of whether the birther had any pregnancy risk factors (e.g., gestational diabetes) or the birth was to multiples (e.g., twins; 0 = no, 1 = yes) and a continuous measure of the number of previous live births. Payment source for the birth was measured with separate binary indicators of payment source(s) used as reported on the birth certificate (self-pay, private insurance, Medicaid, military insurance, IHS, and other sources [e.g., health care cost-sharing]). A control for the year of birth (2014 to 2018) was included in all models.
To capture information on birthers’ surrounding community, county-level measures of community health were integrated from the RWJF County Health Rankings database. Four county-level measures were used: health outcomes, health behaviors, clinical care, and social and economic environment. The health outcomes index measured both the length and quality of life for the county’s population. The health behaviors index measured the tobacco use, diet and exercise, alcohol and drug use, and sexual activity of the county’s population. The clinical care index measured both access to health care and the quality of care for the county’s population. The social economic environment index measured several dimensions of education, employment, income, family and social support, and community safety for the county’s population. Counties were ranked on these metrics and placed into quartiles. The quartile rankings of a birther’s residential county were used as measures of the health of their surrounding community. Sensitivity analyses produced similar results when using deciles and raw ranking values. For additional information on community health measures, see Appendix A in the online version of the article.
Analytic Strategy
Logistic regression models predicted the likelihood that a birther received IPNC during their pregnancy. These models were conducted first on the overall sample of all birthers and then on stratified samples by reservation status and race (limited to non-Hispanic White and AI/AN birthers). A final set of logistic regression models predicting IPNC incorporated indicators of county-level health. Mediation analyses examining the role of county health indicators as mediators of the association between reservation status, race-ethnicity, and IPNC were tested using the causal mediation approach of Imai, Keele, and Tingley (2010), which enables examination of mediation with nonlinear outcomes.
Results
Most birthers reported having adequate PNC, with only 16.8% reporting IPNC. However, when looking across race and reservation status, clear inequities emerge. A much larger share of AI/AN birthers (46.4%) reported IPNC compared to White birthers (12.6%), Black birthers (17.1%), Asian birthers (13.9%), and Hispanic birthers (20.2%). Many more reservation-based birthers experienced IPNC (43.4%) compared to those living off reservation (14.0%). For additional descriptive information about the sample and racial and reservation status differences in measures, see Appendix B in the online version of the article.
Table 1 presents the results of multivariate logistic regression models predicting the odds that birthers experienced IPNC during their pregnancy (Model 1; odds ratios). AI/AN birthers had significantly higher odds of experiencing IPNC compared to White (59.9% higher odds), Black (55.2% higher odds), Asian (43.0% higher odds), and Hispanic birthers (46.0% higher odds), controlling for all other variables. Compared to birthers residing off reservation, birthers living on reservation had 39.4% higher odds of experiencing IPNC. Those with lower levels of education, younger ages, and residence in more remote rural areas all had significantly higher odds of IPNC compared to birthers who were college-educated, older, and urban-dwelling. Significantly lower odds of IPNC were found among married individuals and those using WIC compared to unmarried birthers and those not using WIC. Compared to individuals financing their birth with private medical insurance, those paying with Medicaid, IHS, military insurance, self-payers, and other payment sources were more likely to have IPNC (86.0% higher odds ratio, 81.9% higher, 51.7% higher, 154.4% higher, and 111.0% higher, respectively). Experiencing at least one health risk during pregnancy (compared to none) translated into 10.3% lower odds of having IPNC, and birthers delivering multiples were marginally less likely to have IPNC compared to singleton births (12.2% less likely). For every additional previous live birth, birthers had 19.1% higher odds of experiencing IPNC in their current pregnancy. Finally, births occurring more recently had lower odds of experiencing IPNC (3.2% lower odds ratio for every additional year later).
Reservation Dwelling and Odds of Inadequate Prenatal Care (Odds Ratios).
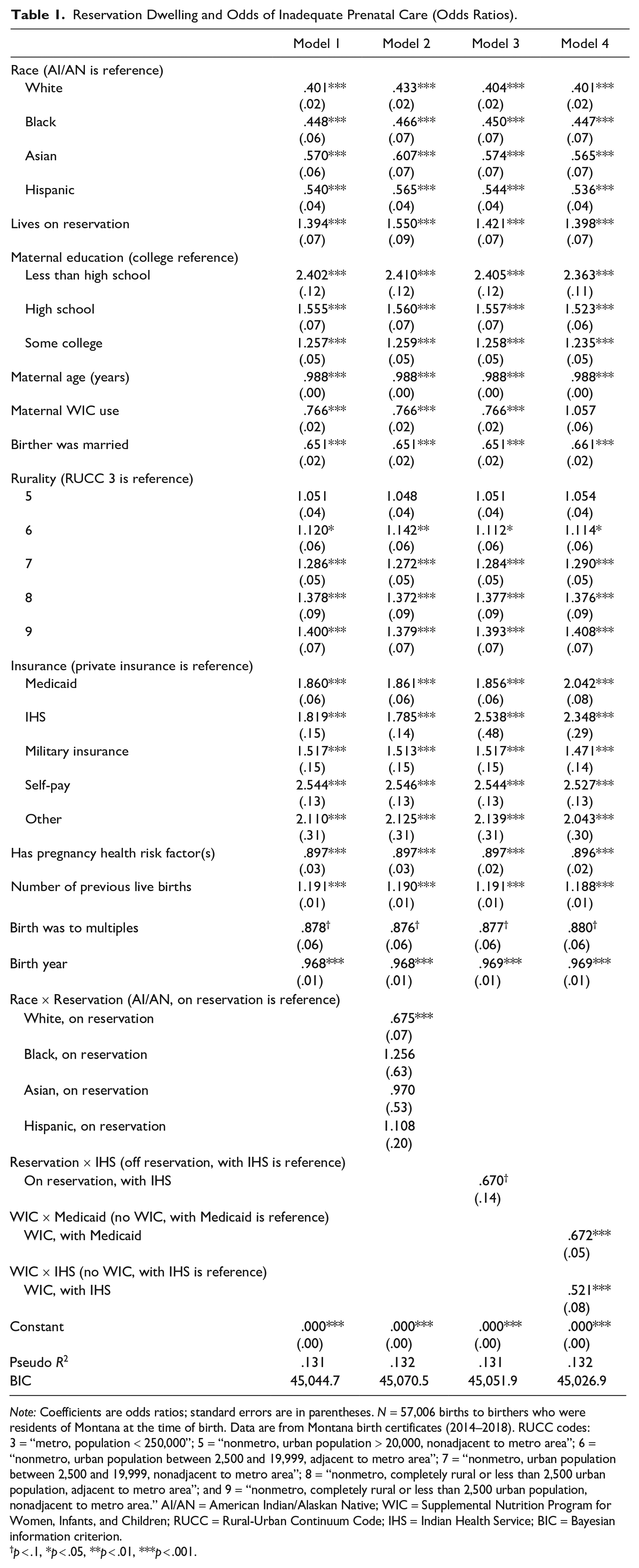
Note: Coefficients are odds ratios; standard errors are in parentheses. N = 57,006 births to birthers who were residents of Montana at the time of birth. Data are from Montana birth certificates (2014–2018). RUCC codes: 3 = “metro, population < 250,000”; 5 = “nonmetro, urban population > 20,000, nonadjacent to metro area”; 6 = “nonmetro, urban population between 2,500 and 19,999, adjacent to metro area”; 7 = “nonmetro, urban population between 2,500 and 19,999, nonadjacent to metro area”; 8 = “nonmetro, completely rural or less than 2,500 urban population, adjacent to metro area”; and 9 = “nonmetro, completely rural or less than 2,500 urban population, nonadjacent to metro area.” AI/AN = American Indian/Alaskan Native; WIC = Supplemental Nutrition Program for Women, Infants, and Children; RUCC = Rural-Urban Continuum Code; IHS = Indian Health Service; BIC = Bayesian information criterion.
p < .1, *p < .05, **p < .01, ***p < .001.
To further explore variation in the odds of IPNC among reservation-dwelling birthers, interaction effects were tested. Results presented in Table 1, Model 2 indicate that the higher odds of IPNC among reservation-dwelling birthers are significantly higher for AI/AN reservation-dwelling birthers compared to White reservation-dwelling birthers. Although most reservation-dwelling birthers are AI/AN (74.1%), White birthers are the second largest racial group to reside on reservations (21.8%). Supplementary postestimation analyses were conducted to estimate marginal effects, the predicted probability of IPNC by reservation and race (Appendix C in the online version of the article). According to these results, White birthers living on reservation (14.4%) and off reservation (13.9%) had a similar predicted probability of experiencing IPNC, whereas AI/AN birthers living on reservation had a significantly higher predicted probability of IPNC compared to AI/AN birthers living off reservation (34.2% vs. 25.9%).
Payment type was also associated with the adequacy of PNC in different ways for birthers living on and off reservation. Results presented in Table 1, Model 3 indicate that the higher likelihood (odds ratio) of experiencing IPNC when using IHS coverage relative to private insurance was more pronounced for birthers who lived off reservation but used IHS coverage to pay for their birth. Supplementary postestimation analyses were conducted to estimate marginal effects, the predicted probability of IPNC by reservation and IHS coverage (Appendix C in the online version of the article). Those relying on IHS coverage living off reservation had a statistically significantly higher predicted probability of IPNC (29.9%) compared to those using IHS living on reservation (29.0%) and birthers paying with private insurance who lived on reservation (20.5%) and off reservation (15.9%). Results rotating the reference group for payment type (Appendix D in the online version of the article) further highlight the higher likelihood of IPNC for birthers using IHS coverage when living off reservation.
Nested regression models (available on request) indicated that the association between WIC receipt and the likelihood of IPNC changed once payment source was controlled for. Further examining this, interaction terms between WIC and payer source were tested. Results presented in Table 1, Model 4 indicate that the receipt of WIC reduced the likelihood of IPNC, but only for those paying with Medicaid or IHS coverage. Supplementary postestimation analyses were conducted to estimate marginal effects, the predicted probability of IPNC by WIC receipt and payer type (Appendix C in the online version of the article). According to these results, birthers who did not have Medicaid had a similarly low likelihood of IPNC whether or not they were enrolled in WIC (14.1% and 13.7% predicted probability of IPNC, respectively). For birthers on Medicaid, using WIC was associated with a lower predicted probability of IPNC (17.9%) relative to those who were not enrolled in WIC (23.0%). A similar pattern emerged in the interaction between WIC and IHS coverage. Birthers without IHS coverage had a lower predicted probability of IPNC whether or not they were enrolled in WIC (15.9% and 18.0%, respectively). However, for birthers using IHS coverage, having WIC was associated with a significantly lower predicted probability of IPNC (18.4%) relative to birthers on IHS who did not have assistance through WIC (30.9%). These findings suggest that WIC receipt is associated with a reduced likelihood of IPNC, but only for those birthers on Medicaid or IHS. This finding may reflect the concentration of WIC receipt among birthers on Medicaid and IHS, with a much larger proportion of birthers paying with Medicaid (59.0%) and IHS (61.1%) enrolled in the WIC program relative to self-paying birthers (13.1%) and those birthers with private (7.9%), military (19.5%), or other insurance forms (22.1%).
Results of multivariate models with the full sample (Table 1) demonstrate distinct differences in the likelihood of experiencing IPNC for White versus AI/AN birthers and birthers living on and off reservation. To further explore these dynamics, stratified models were run by race (White vs. AI/AN) and reservation status (see Table 2; odds ratios). First, focusing on race differences, we see that living on reservation was associated with a higher likelihood of IPNC for AI/AN birthers but not White birthers (Table 2, Models 1 and 2). Larger differences were noted for AI/AN versus White birthers when comparing the likelihood of IPNC for people living in more rural versus urban areas. The likelihood of IPNC rose as individuals resided in more rural counties and nearly doubled among AI/AN birthers (41.3%–76.8% higher odds ratios) compared to White birthers (no differences, 32.4%) among RUCCs 6 through 9. The association between payment type and IPNC also varied for White versus AI/AN birthers. No significant differences were found in the odds of IPNC for White birthers paying with IHS versus private insurance (largely due to the small number of White birthers meeting IHS eligibility requirements; n = 72), while AI/AN birthers paying with IHS coverage had 74.2% higher odds of IPNC compared to AI/AN birthers paying with private insurance. Furthermore, AI/AN birthers paying with military or other insurance did not have elevated rates of IPNC compared to AI/AN birthers paying with private insurance, while the odds of IPNC were 60.8% and 127.9% higher for White birthers paying with these insurance forms, respectively, compared to White birthers using private insurance. White and AI/AN birthers paying with Medicaid had similarly higher odds of IPNC relative to White and AI/AN birthers paying with private insurance (83.4% and 80.2% higher odds ratios, respectively). AI/AN birthers who relied on self-pay compared to private insurance had much higher odds of IPNC (228.9% higher odds) compared to White birthers using self-pay (145.2% higher odds). Enrollment in WIC was more strongly associated with having a lower likelihood of IPNC for AI/AN birthers (42.8% lower odds) than White birthers (15.3% lower odds) compared to their counterparts who were not enrolled in WIC. Having a pregnancy health risk was associated with lower odds of experiencing IPNC for White birthers (11.3% lower) but was not associated with IPNC among AI/AN birthing people. Finally, over the period of study (2014–2018), there is an observed reduction in the likelihood of experiencing IPNC for White but not AI/AN birthers, suggesting that rates of IPNC are improving for White people in Montana but not AI/AN people.
Odds of Inadequate Prenatal Care, Stratified by Race and Reservation Status (Odds Ratios).
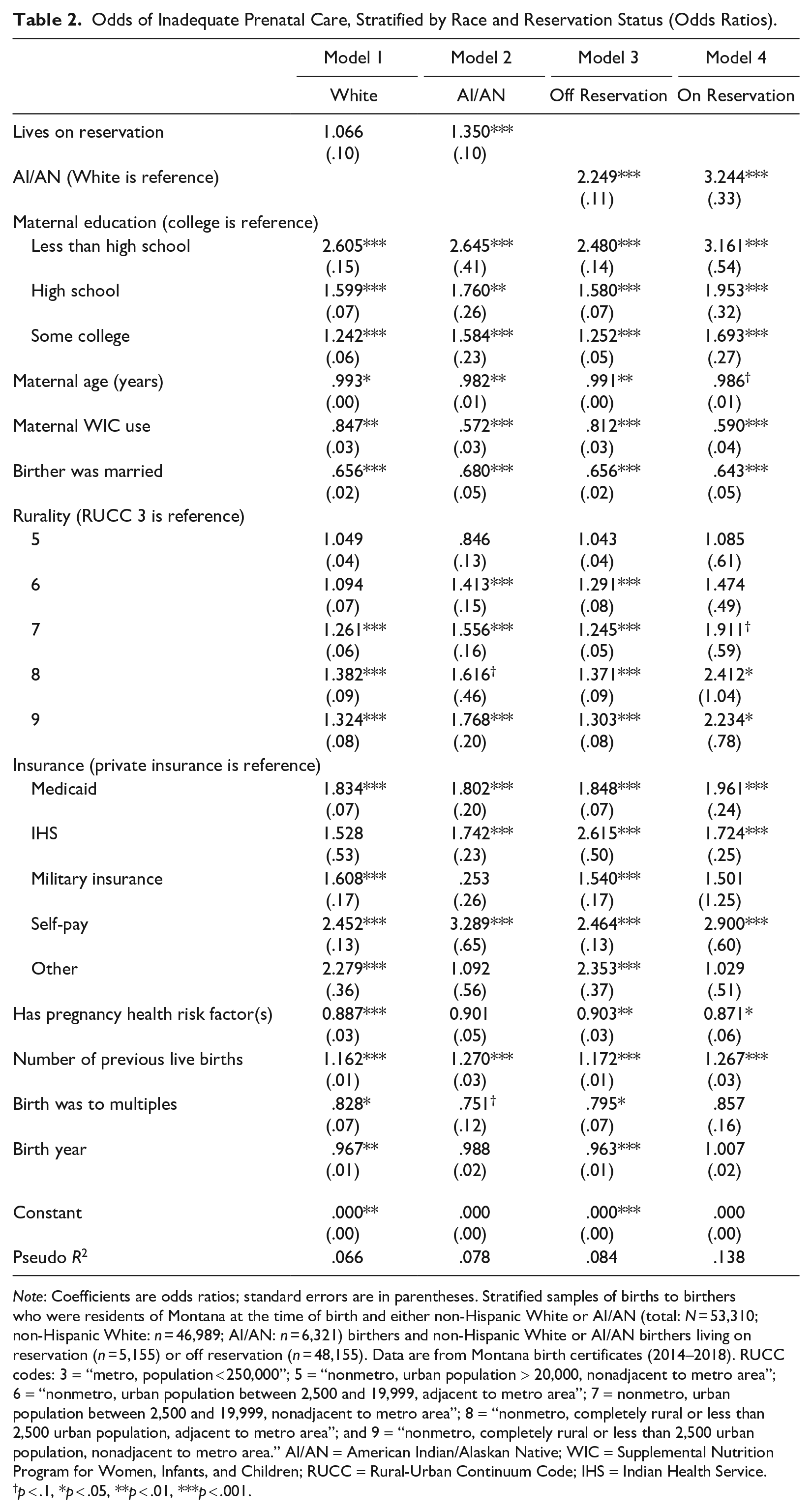
Note: Coefficients are odds ratios; standard errors are in parentheses. Stratified samples of births to birthers who were residents of Montana at the time of birth and either non-Hispanic White or AI/AN (total: N = 53,310; non-Hispanic White: n = 46,989; AI/AN: n = 6,321) birthers and non-Hispanic White or AI/AN birthers living on reservation (n = 5,155) or off reservation (n = 48,155). Data are from Montana birth certificates (2014–2018). RUCC codes: 3 = “metro, population < 250,000”; 5 = “nonmetro, urban population > 20,000, nonadjacent to metro area”; 6 = “nonmetro, urban population between 2,500 and 19,999, adjacent to metro area”; 7 = nonmetro, urban population between 2,500 and 19,999, nonadjacent to metro area”; 8 = “nonmetro, completely rural or less than 2,500 urban population, adjacent to metro area”; and 9 = “nonmetro, completely rural or less than 2,500 urban population, nonadjacent to metro area.” AI/AN = American Indian/Alaskan Native; WIC = Supplemental Nutrition Program for Women, Infants, and Children; RUCC = Rural-Urban Continuum Code; IHS = Indian Health Service.
p < .1, *p < .05, **p < .01, ***p < .001.
Turning to models stratified by reservation status, distinct differences were observed among reservation-dwelling birthers (Table 2, Models 3 and 4). Among those living on reservation, AI/AN birthers had larger differences in the elevated likelihood of IPNC relative to White birthers (224.4% higher odds of IPNC). Off-reservation AI/AN birthers also experienced an elevated likelihood of IPNC relative to White counterparts (124.9% higher odds), albeit a smaller difference. Educational inequities in the odds of IPNC appear larger for reservation-dwelling birthers. Again, the association between WIC receipt and IPNC appears to be substantively stronger for reservation-dwelling birthers. Statistically significant rurality differences in the odds of IPNC were more prevalent among birthers living off reservation when comparing birthers residing in nonmetro, urban areas to birthers from urban areas. However, reservation-dwelling birthers residing in the most remote, rural areas (RUCC 9) had much higher likelihoods of IPNC compared to urban birthers (123.4% higher odds) than the same comparison for non-reservation-dwelling birthers (30.3% higher odds). The concentration of reservation-dwelling birthers in rural regions may be contributing to the lack of observed statistically significant differences in IPNC for this group (Appendix B in the online version of the article). Following results from Table 1, Model 3, findings presented in Table 3, Models 3 and 4 also indicate that birthers using IHS coverage who live off reservation had substantially higher odds of having IPNC relative to birthers using private insurance (161.5% higher odds) compared to birthers living on reservation with IHS coverage (72.4% higher odds). Other payment-type differences by reservation status largely follow the results of racially stratified models, reported above. Finally, birthers residing off reservation experienced improvements in the risk of IPNC over the period, while no such improvements were observed among reservation-dwelling birthers.
Odds of Inadequate Prenatal Care, Mediation of Reservation-Dwelling by County Health Indicators (Odds Ratios).
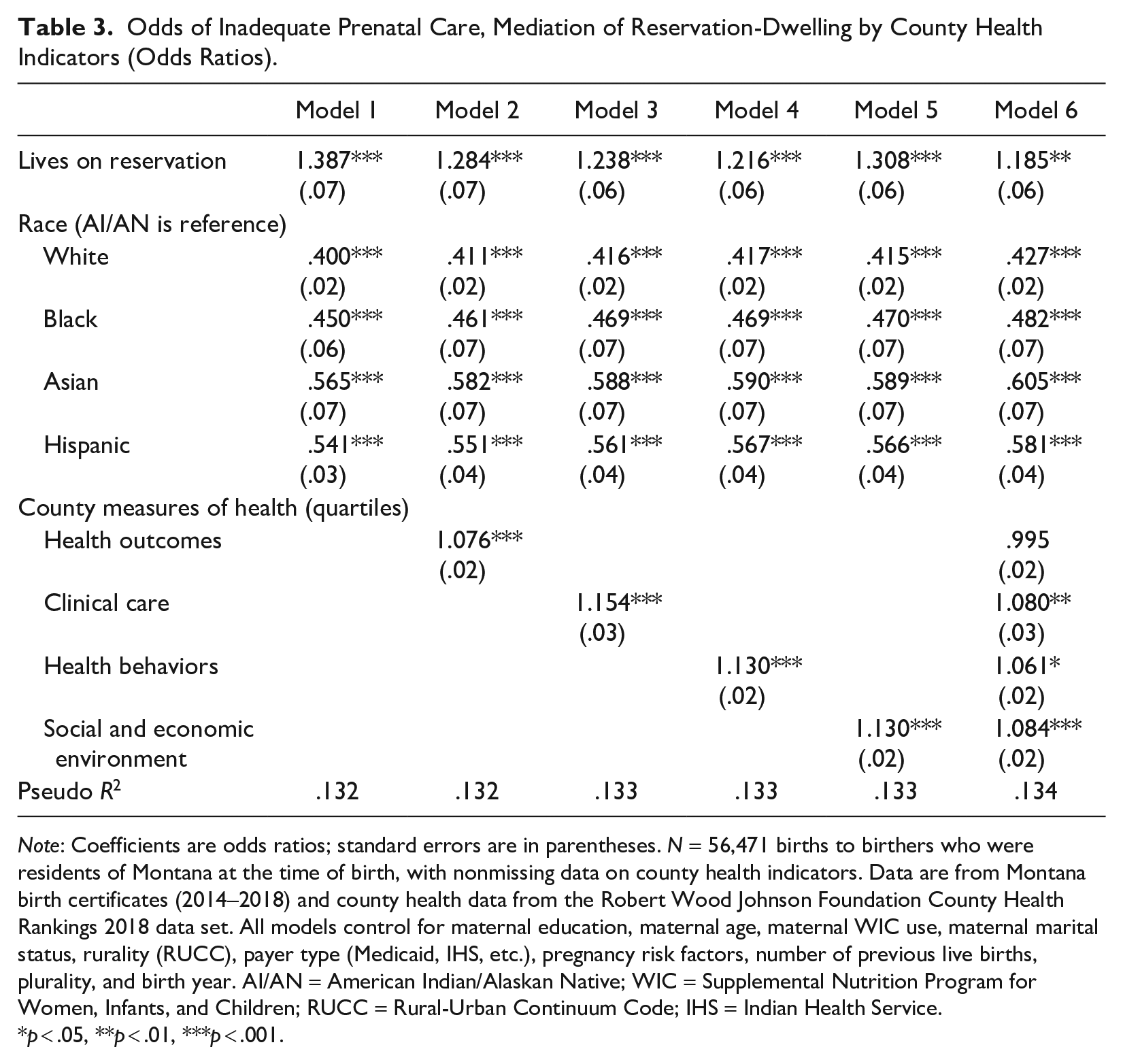
Note: Coefficients are odds ratios; standard errors are in parentheses. N = 56,471 births to birthers who were residents of Montana at the time of birth, with nonmissing data on county health indicators. Data are from Montana birth certificates (2014–2018) and county health data from the Robert Wood Johnson Foundation County Health Rankings 2018 data set. All models control for maternal education, maternal age, maternal WIC use, maternal marital status, rurality (RUCC), payer type (Medicaid, IHS, etc.), pregnancy risk factors, number of previous live births, plurality, and birth year. AI/AN = American Indian/Alaskan Native; WIC = Supplemental Nutrition Program for Women, Infants, and Children; RUCC = Rural-Urban Continuum Code; IHS = Indian Health Service.
p < .05, **p < .01, ***p < .001.
To examine possible mechanisms underlying the elevated rates of IPNC among AI/AN and reservation-dwelling birthers, we examined the role of community health using county-level health indicators. The odds of experiencing IPNC are 38.7% higher for reservation-dwelling birthers, controlling for race, rurality, sociodemographic characteristics, social support, payer type, and pregnancy and birth characteristics (Table 3, Model 1). For AI/AN birthers, the odds of experiencing IPNC are 60.0%, 55.5%, 43.5%, and 45.9% higher compared to White, Black, Asian, and Hispanic birthers, respectively, controlling for reservation status, rurality, sociodemographic characteristics, social support, payer type, and pregnancy and birth characteristics. After controlling for community health factors, these associations were reduced across Models 2 to 6. Tests of mediation (Imai et al. 2010) indicated that these were statistically significant reductions in the association between reservation status and IPNC, mediated by county health factors (results available on request). However, while there were reductions in the magnitude of race coefficients when models included county health indicators, mediation analyses did not find evidence that county health indicators mediated the association between race and IPNC (results available on request).
Birthers residing in counties ranked in lower quartiles for community health were more likely to have IPNC. Birthers living in counties with higher rates of poor health outcomes (Table 3, Model 2), poorer health care access and lower quality clinical care (Table 3, Model 3), elevated rates of unhealthy behaviors (Table 3, Model 4), and more social and economic disadvantage (Table 3, Model 5) were more likely to have IPNC, as indicated by higher odds ratios. After controlling for these four dimensions of community health, reservation-dwelling birthers had only 18.5% higher odds of experiencing IPNC relative to birthers living off reservation (Table 3, Model 6). This is a 52.2% reduction in the association between reservation status and IPNC from Model 1. Mediation analyses examining the individual contributions of county health indicators in mediating the association between reservation status and IPNC (Models 2–5) suggest that county-level health outcomes mediated 45.3%, clinical care access and quality mediated 37.3%, health behaviors mediated 44.1%, and socioeconomic environment mediated 26.6% of the total effect of reservation status on IPNC. Reservation-dwelling birthers are more likely to have IPNC, in part, because they reside in communities characterized by poorer health outcomes, poorer clinical care, elevated rates of poor health behaviors, and more social and economic disadvantage.
Discussion
Race and place matter. Consistent with other studies, AI/AN birthers in our study report the highest rates of IPNC compared to other racial and ethnic groups (Johnson et al. 2010). Among Montanan AI/AN birthing people, our study found that 46.4% received IPNC, higher than historical IHS data ranging from 18.9% to 27.1% among AI/AN individuals (Baldwin et al. 2002). AI/ANs living on and off reservation had significantly higher rates of IPNC versus White people living on reservation (224.4% higher odds) and off reservation (124.9% higher odds). Race is a proxy for the effects of structural racism and is not employed in this article to attribute unique biological differences to one’s ability to access care. Race, in this sense, demonstrates how the reference group, White race, benefits from systemic structures that were created to privilege power and resources in their favor (Braveman et al. 2022). Systematic disenfranchisement and racial discrimination have significant consequences for the health of individuals and their offspring (Williams 2018). In the current study, AI/AN race reflects intergenerational processes and outcomes that have targeted this group to disenfranchise them from power and resources.
Findings from this study demonstrate that considerable disparities exist between AI/AN and White birthers’ PNC use and that residence on American Indian reservations increases the likelihood that AI/AN birthers experience IPNC. This highlights the intersecting inequities of race and place such that the location where people live further contributes to their experience of social, political, economic, and geographical disenfranchisement that leads to IPNC.
Land is sacred. Land holds memories. For many AI/AN tribes relocated from ancestral lands and territories onto reservations, land holds special cultural meaning and can be a repository for ancestral land memory of communal loss. Reservations are, for the most part, concentrated communities of AI/AN people that were geographically selected by the federal government to isolate Indigenous people from White settlers and the growing U.S. economic society onto lands with few resources. Repercussions from segregation policies continue today, resulting in differential education, employment, and health care access—all manifestations of structural racism. As such, health outcomes may reflect those inherited from intergenerational trauma from a brutal colonized and forced assimilation history (Brave Heart et al. 2011) as well as ongoing daily effects of systemic racism (Palacios and Portillo 2009) that have gravely affected AI/AN maternal and infant outcomes (ACIMM 2022).
Living on a reservation was not protective but, rather, was associated with a 3 times higher rate of IPNC (43.4%) compared to those living off reservation (14.0%). All reservations within Montana reside in rural geographically isolated areas. If rurality uniformly affects prenatal access, one might suspect White birthers to have similar rates of IPNC after accounting for rurality; yet very few differences were observed among White birthers’ rates of IPNC who live on reservation (14.4%) or off reservation (13.9%), similar to national rates (14.8%; NCHS 2021). For White birthers, IPNC is stable, suggesting similar underlying social, political, economic, and geographic determinants of health regardless of place. Perhaps geographical separation from resources may help explain the 8.3%-point difference between IPNC among AI/AN birthers living on reservation (34.2%) to those living off reservation (25.9%); however, we believe that disparate systems and structures exist that facilitate one population’s greater ability to access PNC
For low-income pregnant people, WIC is meant to enhance health and nutrition through education, supplemental food, referral to PNC, and support for high-risk pregnancies. Research suggests WIC is related to fewer incidences of late PNC entry (Venkataramani et al. 2022). We found WIC to be protective against IPNC among those using Medicaid or IHS given that when birthers using these payers did not use WIC, they often had the highest rates of IPNC. It is unknown how and when birthers access WIC; however, there is room for standard policies to connect birthers from these payers to WIC. Utilizing WIC fully, including referrals to PNC and specialty services, may improve maternal outcomes.
Reservations uniquely demonstrate the intersection of race and place for AI/AN birthers and the cumulative effects of systemic racism and structural policies that have distanced this population from optimal health. Findings from the current study indicate that the health of the community context and associated exposures to social determinants of health help to explain elevated rates of IPNC among AI/AN reservation-dwelling birthers. Structural barriers in the community environment, such as poverty, education, employment, access to insurance, and access to resources (food security, reliable transportation, etc.), are obstacles that affect PNC access and therefore adequacy of use. While this study finds that aspects of community health help to partially explain elevated rates of IPNC on reservations, future research should continue to explore additional measures of the community context to improve our understanding of these mechanisms. Furthermore, public health offices should consider including a measure of reservation status on birth certificates and other data collection tools monitoring maternal and infant health.
Compounding these structural barriers are reverberations from historical atrocities (e.g., coercive sterilization campaign), malaligned policies (universal drug screening of all childbearing age AI/AN women, regardless of state statutes and consequences for infant/child placement; ACOG 2018), and ongoing frustrations with IHS (ACIMM 2022). At the intersections of an inherited history, place, and race, Hanson’s (2012) qualitative study revealed PNC use among Sioux birthers was affected by mistrust in providers and the health care system, access to reliable transportation, competing priorities, system barriers related to provider continuity, and absent cultural and/or gender congruence. Future research should continue to explore the barriers to PNC use facing AI/AN and reservation-dwelling birthers but also those factors that promote timely and adequate PNC. Grassroots Indigenous organizations such as the Alaska Native Birthworkers Community (2023), Hummingbird Indigenous Family Services (2023), and Changing Woman Initiative (2023), led by AI/AN doulas, midwives, and lactation consultants, are reclaiming health care for AI/AN families and communities by offering services rich in cultural teachings while providing culturally and racially congruent care. In addition to financial and policy support for Indigenous-focused programs, qualitative research is needed to examine both barriers to care and how these programs center AI/AN birthing people to best understand, identify, and create optimal paths to care for reservation-based AI/ANs.
Limitations
There are limitations to self-report on birth certificate data, including inaccuracies in data entry. This is common, especially in the misclassification of race and ethnicity among AI/AN people, where AI/AN people are usually undercounted when not allowed to self-report or counted when they report multiple races (Jim et al. 2014). Our study uses a bridged race methodology that includes self-report single and multiple maternal race and ethnicity (NCHS 2004), a preferred methodological practice to better approximate AI/AN health outcomes (Urban Indian Health Institute n.d.). “American Indian/Alaska Native” is a political term that has legal implications regarding tribal enrollment. In research, this term has been used interchangeably with those meeting strict enrollment criteria to those who self-identify. It is not the focus of this article to debate the term’s use, but we acknowledge that birth certificate data allowed birthers to self-identify, and regardless of meeting specific legal requirements, those who identified as AI/AN still experienced differential health outcomes and experiences. Our study’s measure of health insurance is limited to the payer(s) for delivery. Therefore, we are not able to capture changes in insurance coverage over the course of pregnancy, which may impact engagement with care and adequacy of PNC (Daw et al. 2017). Furthermore, we lack information regarding health care provider type providing PNC for people in our study (e.g., family physician, obstetrician, midwife), and therefore, we cannot statistically control for variation in adequacy of PNC across provider type. Finally, county-level health indicators are the best approximation of how healthy reservations are, although reservations may encompass more than one county, and blending these county-level health indicators may under- or overrepresent health outcomes.
Conclusion
To improve the adequacy of PNC and help address persistent inequities in maternal and infant health, policies must address structural and social determinants of health that impede PNC utilization for AI/AN people. Community-based home visiting programs may improve early initiation or access to PNC (Johnson 2020) and could be a useful intervention to address unmet social determinants of health needs. Increasing the workforce diversity, both in provider diversity and expanding the type of perinatal services offered (e.g., social work, mental health, midwives, doulas, family medicine physicians, lactation consultants, etc.), are considered key strategies to improve patient utilization of perinatal services and improve perinatal health among AI/AN birthing people (ACIMM 2022). Offering racially concordant (racially matched) and culturally congruent (culturally matched) care, like Changing Woman Initiative, Hummingbird Indigenous Family Services, and the Alaska Native Birthworkers Community, allow birthing people options for choosing more familiar providers while improving trust in the health care system (Jeffers et al. 2023).
At a minimum, health care providers and systems must provide culturally safe care, self-reflective care aimed at examining and dismantling power dynamics between providers and patients (Curtis et al. 2019). Qualitative research suggests that asymmetrical power dynamics between providers and patients negatively impact the childbirth process for racially marginalized birthing people (West and Bartkowski 2019). Implicit bias training is a practical tool to help facilitate culturally safe care among clinicians, and evidence demonstrates implicit biases are stronger across intersectional identities, such as a low socioeconomic AI/AN woman (Meidert et al. 2023).
Additionally, integrating novel PNC delivery methods (e.g., telemedicine) and expanding health insurance may improve access to PNC and therefore use (Sebens and Williams 2022). Finally, implementation of group PNC models that integrate peer support along with risk assessment and education may help increase fidelity to PNC for AI/AN populations because group models have been shown to increase PNC utilization among high-risk and racially marginalized populations (Mazzoni and Carter 2017).
The United States is approaching Healthy People 2030, which aims for 84.3% of all pregnant individuals to enter PNC within the first trimester (Healthy People n.d.), and presently, AI/AN birthing people are lagging far behind. Perinatal disparities will persist until existing disparities affecting social determinants of health are addressed, including those that manifest within particular community environments.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465241236448 – Supplemental material for Race and Place Matter: Inequity in Prenatal Care for Reservation-Dwelling American Indian People
Supplemental material, sj-docx-1-hsb-10.1177_00221465241236448 for Race and Place Matter: Inequity in Prenatal Care for Reservation-Dwelling American Indian People by Maggie L. Thorsen and Janelle F. Palacios in Journal of Health and Social Behavior
Footnotes
Acknowledgements
A previous version of this article was presented at the 2023 annual meeting of the Population Association of America.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this article was supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award No. P20GM104417. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Notes
Supplemental Material
Appendices A through D are available in the online version of the article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.