
Abstract
With most scholarly attention directed toward understanding the stigma experiences of individuals with mental illness, less attention has been given to associative stigma: an understudied form of social exclusion and devaluation experienced by the social ties of stigmatized individuals. This study advances scholarly understanding of associative stigma by drawing on social network methods to better illuminate how the quantity and quality of social relationships with those dealing with mental illness impact experiences of perceived discrimination. Using a nationally representative sample from the General Social Survey, I find that (1) knowing more people with mental illness, (2) having more core (friends and family members) versus peripheral ties, and (3) having ties who are most at risk of facing public stigma themselves (e.g., stereotype-confirming ties) are associated with greater perceived discrimination experiences. Taken together, these findings shed light on how pervasive associative stigma truly is.
During their lifetime, nearly everyone will either be diagnosed with or be socially connected to someone diagnosed with a mental illness (Jorm 2000). Receiving a mental illness label or being socially tied to someone who receives a label is theorized to confer social devaluation and exclusion processes (Goffman 1963; Pescosolido and Martin 2015). Most researchers and policymakers interested in understanding these processes focus on the direct stigma experiences of individuals with mental illness and the negative consequences of public stigma (see Pescosolido 2013). Although most scholarly attention is given to public stigma, some studies also confirm the deleterious effects of stigma on the people they associate with (e.g., Karnieli-Miller et al. 2013; Östman and Kjellin 2002; Verhaeghe and Bracke 2012). Mental health scholarship examining stigma by association has primarily focused on public perceptions of a specific familial role (i.e., parent) and the qualitative experiences of family members (Angermeyer, Schulze, and Dietrich 2003; Larson and Corrigan 2008; Yin, Li, and Zhou 2020). Individuals, especially female relatives, are often blamed and shamed for their family member’s mental health issues (Corrigan and Miller 2004; van der Sanden et al. 2016).
Yet less is known about the associative stigma experiences of other relevant social ties, such as friendship ties, and the potentially cumulative effect of having multiple social ties with mental illness. There is great variation in terms of how many relationships and what types of relationships (e.g., family member, friend, acquaintance) people have with those contending with mental health issues (Felix and Lynn 2022; Perry et al. 2022). Does this relationship variation translate to variation in associative stigma experiences? Given that friendship ties play an important social support role for people with mental health issues (Bjornestad et al. 2017) and given that each additional social relationship theoretically produces more opportunities for associative stigma to occur, examining the various interpersonal experiences people have could highlight previously overlooked populations contending with mental health stigma.
Drawing on social network methods, this study uses nationally representative egocentric network data to comprehensively measure the quantity and quality of social relationships with stigmatized others to elucidate who is at risk of experiencing associative stigma. Findings reveal that having more meaningful connections to valued ties (both friends and family members), as well as being embedded in networks containing stereotype-confirming social ties, is associated with greater perceived discrimination. These findings have implications for how we conceptualize associative stigma targets.
Background
Stigma by Association
In his groundbreaking work on social stigma, Goffman (1963) argued that a marked individual is someone who experiences prejudice and discrimination from the general public. In the face of stigmatization, these individuals can turn to sympathetic others for support, including the “wise”: “the individual who is related through the social structure to a stigmatized individual—a relationship that leads the wider society to treat both individuals in some respect as one” (Goffman 1963:30). The wise (social ties without a mark) can theoretically experience social devaluation and exclusion due to their association with a marked individual, a phenomenon referred to as courtesy stigma or stigma by association (Goffman 1963). Given that mental illness labels act as marks that confer social devaluation and exclusion, individuals who do not have mental illness themselves but who are tied to individuals with an illness label are at risk of facing prejudice and discrimination as well (Pescosolido and Martin 2015).
Associative stigma is a distinct concept from caregiving burden. Whereas the caregiving literature posits, for example, that family members of individuals with mental illness may experience objective and subjective “burden,” such as allocation of time and resources toward treatment (Baronet 1999), the associative stigma literature focuses on how those family members are perceived and treated by others. Due to social proximity, the associates of the stigmatized individual, such as family members, may experience stigma in the form of shame, blame, and contamination (Corrigan and Miller 2004; Corrigan, Watson, and Miller 2006; Pescosolido and Martin 2015). For example, individuals may avoid potential romantic partners who have family members with mental health issues for fear of it being “passed on” to future children (contamination), or teachers, coworkers, and medical professionals may view parents as responsible for their child’s mental health issue and assume poor parenting practices (shame and blame). The latter are more closely related to culpability or responsibility and are often considered moral forms of associative stigma (Davis and Manago 2016).
With most scholarly attention given to public and self-stigma, the limited research focusing on stigma processes beyond the labeled individual find that stigma by association is also present, albeit to a lesser extent than public stigma. Vignette studies find that the siblings and children of vignette characters with mental illness are perceived to be at risk of developing a similar problem and are socially avoided, particularly by respondents who endorse genetic attributions of mental illness (Phelan 2005). Parents are often blamed for a child’s mental illness, with over 80% of General Social Survey (GSS) participants agreeing that a child’s depression is due to the way they were raised (Perry et al. 2007). More specifically, participants perceive childhood depression as very serious, unlikely to improve with treatment, and due to parenting practices, suggesting that parental blame is not only prevalent but also strong (Pescosolido 2013). Experimental studies also find that the public stigmatizes parents of children with mental illness, with participants expressing more associative stigma toward mothers of children with autism compared to mothers of children with asthma (Thibodeau and Finley 2017).
Studies focusing on the experiences of family members of those with mental illness highlight both the prevalence and consequences of stigma by association (Francis 2012; González-Torres et al. 2007; Koro-Ljungberg and Bussing 2009; Larson and Corrigan 2008; Sheehan et al. 2018). Many individuals with familial ties with mental illness report experiencing associative stigma via social distancing in interpersonal interactions, and over one-quarter report experiencing structural discrimination (Angermeyer et al. 2003). Familial targets of associative stigma are more likely to suffer from psychological distress and employ a variety of coping mechanisms (e.g., selective disclosure) to navigate experiences of discrimination (Karnieli-Miller et al. 2013; Östman and Kjellin 2002; Verhaeghe and Bracke 2012).
Whereas mental health scholarship examining stigma by association has primarily focused on public perceptions of a specific familial role (i.e., parent) and the qualitative experiences of a family member, less attention has been given to other relevant social ties. Yet individuals can (1) know multiple people with mental illness and (2) have interpersonal experiences beyond familial ties (i.e., close friends, coworkers, and neighbors with mental illness). Goffman (1963:30) himself suggested that courtesy (associative) stigma can be experienced across multiple types of social relationships and is not restricted to familial relationships, emphasizing that “the loyal spouse of the mental patient, the daughter of the ex-con, the parent of the cripple, the friend of the blind, the family of the hangman are all obliged to share some of the discredit of the stigmatized person to whom they are related.” This study draws on networks theory and methods to extend the existing research on associative stigma by examining the potentially cumulative effect of knowing multiple individuals with mental illness and discerning which types of social relationships are most likely to be accompanied by experiences of associative stigma.
Applying a Social Network Approach to Associative Stigma
In networks research, every individual (ego) is embedded within a social network: a set of actors (alters or nodes) that are connected by a set of relations (ties). Network effects emerge when the alters’ behaviors or practices affect the ego. Network scholars examine network characteristics, such as network size (number of egos’ alters), and tie characteristics, such as emotional closeness, to better understand potential network effects (Perry, Pescosolido, and Borgatti 2018; Smith and Christakis 2008). In the context of mental illness, individuals (egos) may report having no social ties with mental illness (no alters). Alternatively, individuals may report having several social ties with mental illness (multiple alters), referred to hereafter as their “mental illness networks.”
Studies employing an egocentric network approach have revealed variation in the quantity of social contact when eliciting alters who have received a mental illness diagnosis (Perry et al. 2022) or alters perceived to have mental health issues regardless of diagnosis (Felix and Lynn 2022). These studies reveal that the size of mental illness networks (i.e., all contacts with mental illness that an individual knows) can vary greatly: Some may think they do not know anyone with mental illness, some have a single friend or family member with mental illness, and others report several meaningful relationships with persons dealing with mental health issues. Do individuals with multiple family members with mental illness have a greater likelihood of facing stigma and discrimination compared to individuals with a single family member? Although individuals who list one social tie with mental illness can certainly experience associative stigma, those with multiple relations to stigmatized others may be at an especially increased risk given that each additional social relationship comes with more opportunities for associative stigma to occur.
Hypothesis 1: Network size is positively associated with perceived discrimination such that knowing more people with mental illness has a cumulative effect on associative stigma experiences.
Network composition: kinship, friendship, and peripheral ties
Mental illness networks likely vary in terms of both size (i.e., quantity) and composition (i.e., type of tie). In general, people are embedded in social networks consisting of both a small set of core ties and a larger set of peripheral ties. Core ties, such as family members, romantic partners, and close friends, are usually stable and provide a variety of social support functions (Morgan, Neal, and Carder 1997). Compared to core ties, noncore or peripheral ties (e.g., coworkers, neighbors, and acquaintances) tend to be weak, unstable, temporary, and less likely to provide social support. For example, people contending with mental health issues report that their core ties provide valuable social support, whereas their peripheral ties are more likely to be sources of stigma (Perry 2011).
Although social networks research has studied both core and peripheral ties more generally, most research examining associative stigma has focused on a particular type of core tie: family members of those with mental illness. This focus is understandable given the key role that familial ties play in the recovery outcomes of individuals with mental illness, and studies do in fact find that familial ties are often blamed and shamed for their family member’s mental health issues (see Corrigan and Miller 2004). Thus, in line with previous research, I expect that family members of individuals with mental illness will report greater levels of discriminatory experiences compared to individuals with peripheral ties (i.e., coworkers, neighbors, or acquaintances with mental illness) or no ties at all and that having more family members with mental illness will have a potentially cumulative effect on perceived discrimination.
However, the associative stigma experience of core ties outside of the family is less established. Friends play an important role in providing social support for individuals experiencing mental health issues. Among adolescents, for example, friendship ties influence recovery outcomes to an even greater extent than family members do (Bjornestad et al. 2017). In fact, Bjornestad et al. (2017:213) suggest that “one possible intervention could include systematically involving friends at an early stage of treatment by asking them to commit to regularly meet with the person.” Although this perspective conveys the benefits of having friendship ties that can provide social support for individuals experiencing social stressors and/or psychological distress (Thoits 2010), it also highlights the perceived culpability that friendship ties may face in alleviating or exacerbating mental illness. Just as the public shames and blames parents and siblings for their family members’ mental illness (Corrigan and Miller 2004), the public may perceive individuals as bearing responsibility for their friend’s mental illness and subsequently attribute negative characteristics to them (shame and blame).
Furthermore, given that individuals tend to form friendships with others who are similar to themselves in some regard, the public could infer friendship-based homophily (i.e., birds of a feather flock together) and engage in social distancing upon assuming that friendship ties also have mental illness that could be “passed on” (contamination). Homophily, or ego–alter similarity, is one of the most robust findings in social network research and has been detected along the lines of various demographic variables, attributes, interests, behaviors, and attitudes (see McPherson, Smith-Lovin, and Cook 2001). In the context of mental illness, people with depression are more likely to be friends with others also experiencing depression compared to their nondepressed peers (Schaefer, Kornienko, and Fox 2011). Although it is certainly not the case that all friendship ties of those contending with mental illness are experiencing similar mental health issues, the public could infer a person’s mental health status based on their close friendships. Thus, friendship ties may experience stigma by association through similar mechanisms as familial ties (i.e., shame, blame, and contamination) and may report significantly more stigma experiences compared to those with peripheral ties or no ties at all. Similar levels of stigma and discrimination between friendship and familial ties would suggest that network theory (i.e., core vs. periphery ties, strong vs. weak ties; Granovetter 1973, 1983) could inform our sociological understanding of associative stigma, and empirical research should expand who it examines as potential targets.
Hypothesis 2: Having more meaningful ties with mental illness (kinship and friendship) but not peripheral ties with mental illness (coworkers, neighbors, acquaintances) is associated with greater perceived discrimination.
Network characteristics: stereotype-confirming ties and network undertreatment
In addition to network size and tie composition, relevant network characteristics could also inform the stigmatization process. Given that individual-level characteristics, such as treatment status, impact the likelihood that a person with mental illness will face public stigma (see Pescosolido 2013), network-level characteristics (i.e., network undertreatment or perceived dangerousness of social ties) may influence the likelihood that a person experiences associative stigma. This study investigates the qualitative nature of mental illness networks to understand if being tied to those most at risk of experiencing public stigma increases the risk of experiencing prejudice and discrimination by association.
First, treatment status influences public stigma. A nationally representative survey reveals that adolescents and young adults display significantly higher levels of stigma toward vignette characters with untreated depression compared to vignette characters described as having treated depression (Romer and Bock 2008). Meanwhile, a randomized experiment using nationally representative data found that respondents exposed to a vignette character with mental illness (i.e., schizophrenia) experiencing successful treatment and long-term recovery were significantly less likely to desire social distance from and less willing to discriminate against people with mental illness compared to respondents exposed to a vignette character with symptomatic and untreated schizophrenia (McGinty et al. 2015). Thus, millions of individuals with mental illness are at increased risk of facing stigma related to undertreatment: Approximately 40% of individuals with mental health issues do not receive adequate treatment (National Institute of Mental Health 2021), and over 30% of individuals who do seek treatment do not maintain care over time (Kreyenbuhl, Nossel, and Dixon 2009). Given the important role that social ties play in treatment seeking (McConnell 2017; Pescosolido, Gardner, and Lubell 1998) and recovery outcomes (Perry and Pescosolido 2015; Perry, Pullen, and Pescosolido 2017) for people with mental illness, friends and family may be blamed or shamed when their social ties with mental illness do not successfully seek or maintain treatment. Thus, individuals embedded in undertreated mental illness networks may report more perceived discrimination compared to individuals with a greater proportion of social ties receiving treatment.
Second, public stigma is also reinforced through stereotype confirmation. For example, the negative cultural belief that mental illness is associated with violence and dangerousness has persisted for decades (Martin, Pescosolido, and Tuch 2000; Pescosolido 2013; Pescosolido, Manago, and Monahan 2019). Experimental studies find that exposure to fictional news articles or narratives that confirm dangerousness stereotypes (e.g., highlight a link between mental illness and violence) exacerbates public stigma towards individuals with mental illness (McGinty, Webster, and Barry 2013; Wilson, Ballman, and Buczek 2016). Furthermore, having interpersonal experiences with the minority of people with mental illness who exhibit violent behavior also reinforces public stigma, increasing the likelihood of endorsing dangerousness stereotypes and desiring social distance from individuals displaying mental illness symptoms (Perry et al. 2022). Although individuals embedded in mental illness networks with stereotype-confirming ties may exhibit more public stigma themselves, they may also be at greater risk of experiencing associative stigma: Others may be even more likely to blame them, shame them, or socially avoid them for fear of contamination.
Hypothesis 3: Being tied to people with mental illness most at risk of experiencing public stigma (stereotype-confirming ties or untreated individuals) is associated with greater perceived discrimination.
Current Study
The current study employs a social network approach to conceptualize and operationalize mental illness networks to more comprehensively understand experiences of stigma by association. Specifically, I examine how the number, quality, and content of social ties to people with mental illness are associated with perceived discrimination. First, I hypothesize that network size (i.e., number of ties with mental illness) is positively associated with the likelihood of reporting perceived discrimination (Hypothesis 1). Second, I expect that having kinship and friendship ties, but not peripheral ties, with mental illness exacerbates the likelihood of experiencing perceived discrimination (Hypothesis 2). Third, having social ties that are most at risk of experiencing public stigma themselves (e.g., knowing more people who confirm negative stereotypes or knowing more untreated people) will be associated with reporting more perceived discrimination (Hypothesis 3).
Data and Methods
Data
This study analyzed data from the 2018 General Social Survey (GSS). The GSS is the longest running nationally representative survey of noninstitutionalized adults. Conducted by the University of Chicago’s National Opinion Research Center and with funding largely from the National Science Foundation, the GSS used a cluster sampling design of households. Trained interviewers collected GSS data using a face-to-face, computer-assisted approach. The GSS consisted of core survey questions (e.g., respondent age) given to all respondents and specific modules assigned to a subsection of respondents. This study focused on the subsection of respondents who were assigned two specific modules: the National Stigma Study module (i.e., assigned to Ballots B and C) and the Everyday Discrimination module (i.e., assigned to Ballots A and C). As discussed in more detail in the following section, the National Stigma Study module (NSS-R II) employed network methods to elicit information about each respondent’s social relationships with those contending with mental illness, and the Everyday Discrimination module included items capturing perceived discrimination.
This study focused on the subsection of GSS respondents who self-rated their mental health as good, very good, or excellent and who completed both the Stigma and the Everyday Discrimination modules (N = 572). Although people with poor mental health can certainly experience both public stigma related to their own mental health status and discrimination related to the mental health of their social ties, this study only includes respondents with good mental health in order to align with Goffman’s (1963) original conceptualization of the wise (i.e., people who do not have a “mark” themselves but are socially tied to a stigmatized individual). Sensitivity analyses (see Appendix C in the online version of the article) were conducted on the full sample (i.e., respondents who completed the stigma module and answered the perceived discrimination items).
Furthermore, given that the 2018 GSS Everyday Discrimination module includes general perceived discrimination items but not mental health-specific items, supplemental data were also collected using a custom-designed egocentric network survey that included mental illness-specific perceived discrimination items and a blame-specific item. Studies have implemented the everyday discrimination scale (EDS) with (e.g., Gee, Pavalko, and Long 2007) and without assessing respondent attribution or identification of mistreatment (e.g., Lee and Turney 2012). The supplemental data were specifically collected to verify if similar patterns emerge when assessing identification of mistreatment (i.e., substantively similar results would suggest that the GSS nonspecific items and the supplementary mental health-specific items are capturing similar perceived experiences among the social ties of people with mental illness). Similar to the GSS Stigma module, respondents completed a name generator that was designed to elicit social contacts with mental health issues and responded to name interpreter questions about each social tie (e.g., family member vs. friend) or ego–alter relationship. Respondents who reported knowing people with mental health issues were also asked about experiences of perceived discrimination due to their relationships. The sample consisted of 308 respondents recruited and compensated through Prolific Academic, a web-based data source company. Respondents were invited to participate in a survey hosted by Qualtrics. During data collection, 39 respondents did not complete the study due to failing an attention check question. Results from the supplemental survey are displayed in Appendices A and B in the online version of the article.
Dependent Variable
Analyses examined perceived discrimination: a dependent variable created using items from the EDS, a methodological tool that assesses the occurrence and frequency of an individual’s perceived chronic interpersonal discrimination (Williams et al. 1997). The EDS is a commonly used measure in discrimination research (Paradies et al. 2015; Williams et al. 2019) and has high reliability (Reeve et al. 2011; Shariff-Marco et al. 2011) and construct validity (Krieger et al. 2005; Taylor, Kamarck, and Shiffman 2004). Scholars have also applied the EDS to capture the discriminatory experiences of parents of individuals with physical disabilities (Song, Mailick, and Greenberg 2018).
In line with previous research, this study utilized items from the EDS to assess general perceived discrimination and unfair treatment among individuals with social ties to stigmatized others. The GSS included five items from the EDS that were measured on a 6-point scale (1 = almost everyday, 6 = never). Respondents were asked, “In your day-to-day life how often have any of the following things happened to you?” in relation to the following items: (a) you are treated with less courtesy/respect than others, (b) you receive poorer service than other people at restaurants or stores, (c) people act as if they think you are not smart, (d) people act as if they are afraid of you, and (e) you are threatened or harassed. Items were reverse-coded (0 = never, 5 = almost every day) so that higher scores indicate a higher level of perceived discrimination. A scale was constructed by calculating the sum of the values for each of the five items. Additional analyses examined each of these items as separate binary dependent variables (1 = has experienced at least a few times a year, 0 = never).
Supplemental data included mental health-specific stigma and perceived discrimination items. Respondents were asked, “In your day-to-day life how often have any of the following things happened to you as a result of knowing someone with mental illness?” in relation to everyday discrimination items found in the GSS and an additional item that aligns with traditional conceptualizations of associative stigma: “People have blamed you for your social ties’ mental health issue.”
Key Independent Variables
Mental illness network
The key independent variables in these analyses focused on egocentric social network measures. A mental illness network consisted of a respondent’s social ties who have mental illness (range = 0–5 in the GSS). To capture the mental illness network, GSS respondents were asked an egocentric name generator question, “Leaving yourself aside, have you ever known someone personally who has been diagnosed with a mental health problem?,” and then were instructed to “Please name up to
Mental illness relationship type
The name generator was then followed by several name interpreter questions that gather additional information about each alter listed. The first name interpreter question asked the nature of each ego–alter relationship. Alters were then classified into three relationship types: family members, friends, or other ties. With the GSS data, each relationship type will have between zero and five alters, and combined, they equal a respondent’s mental illness network size.
Mental illness network characteristics
Additional name interpreters were used to create two aggregate ego-level network characteristic measures: perceived dangerousness and network undertreatment. Maximum perceived dangerousness represented the highest value reported when respondents were asked how dangerous each alter in their mental illness network is (1 = not at all dangerous, 10 = very dangerous). Proportion in treatment represented the proportion of social ties who have received treatment for their mental illness compared to the total number of social ties with mental illness and can range from 0 to 1 (0 = no social ties have received treatment, .5 = half of social ties have received treatment, 1 = all social ties have received treatment).
Control Variables
Several respondent characteristics were included in each model to address potential endogenous confounding factors in terms of who would be more likely to know people with mental illness. Age was coded in number of years. Race was coded as two dichotomous measures, one for Black-identifying respondents and one for participants of another race (reference: White). In the GSS, gender is still measured as binary sex (1 = female, 0 = male). A continuous variable measuring socioeconomic status (SES) was also included using the GSS socioeconomic index (sei10). Sexual minority status was coded as a dichotomous measure (1 = homosexual or bisexual, 0 = heterosexual). Finally, self-report surveys are susceptible to social desirability biases in which respondents may underreport attitudes they perceive to be socially undesirable (Singleton et al. 1988), and this study incorporated a measure that has been used in other stigma studies (e.g., Perry et al. 2022) to address this concern. A social desirability bias variable was created using true/false items (e.g., “I have never deliberately said something that hurt someone’s feelings”; Stöber 2001) from a standard scale (0 = low potential bias, 7 = high potential bias).
Analytic Approach
Several key analytic steps were taken to test all hypotheses. First, to determine if there were any potential model violations, I computed histograms, inspected correlations between variables, examined variance inflation factors, and compared sample demographics. Second, I used survey-weighted linear regression to model the relationships between social network measures and perceived discrimination (Table 2). More specifically, these models examined mental illness network size, network composition (e.g., kin, friendship, peripheral ties), and network characteristics (stereotype-confirming ties, proportion receiving treatment), adjusting for control variables (i.e., gender, age, race, sexual minority status, SES, and social desirability) and for sampling weights provided by the GSS. Third, I used survey-weighted logistic regression to conduct similar analyses that focused on each everyday discrimination item separately (Table 3). Fourth, I examined average marginal effects for various models and determined predicted probabilities for various models (Figure 1). Fifth, I conducted supplementary analyses using mental illness relationship-specific perceived discrimination items (Appendices A and B in the online version of the article). Linear models display coefficients and robust standard errors, and logistic models display odds ratios (ORs) and 95% confidence intervals.
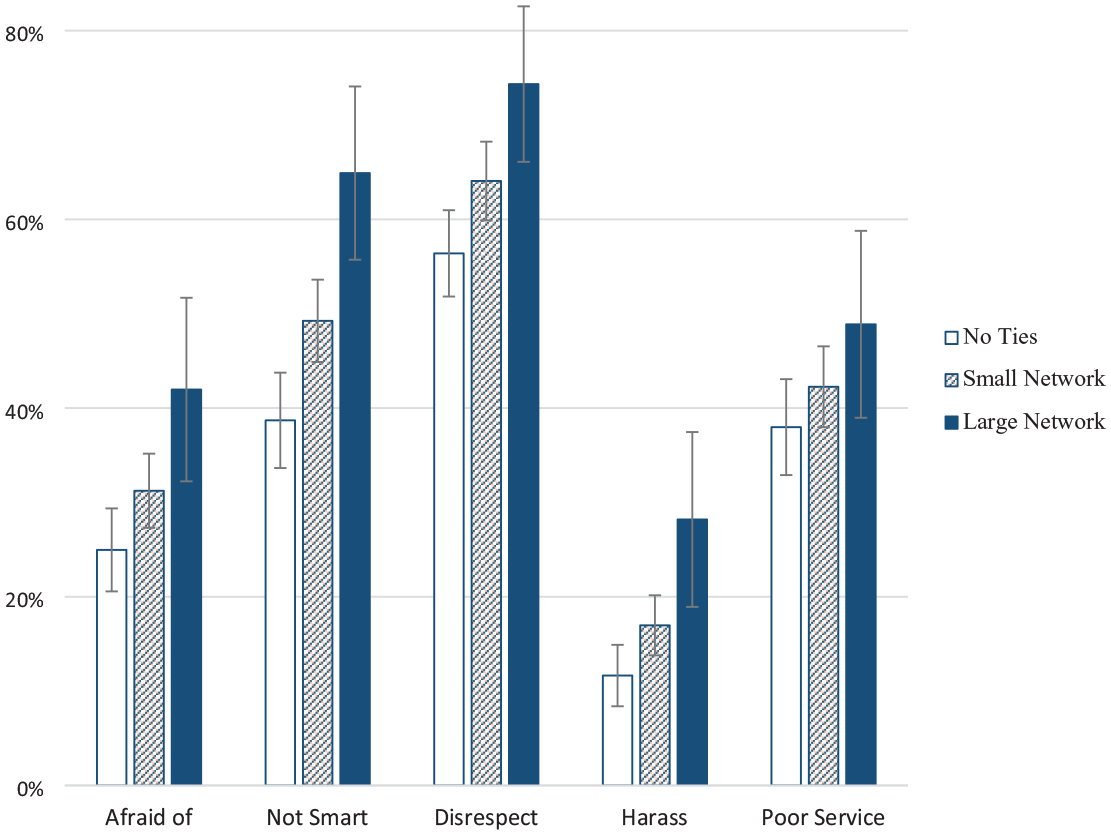
Predicted Probability of People with No Social Ties, a Few Social Ties, or Many Social Ties with Mental Illness Reporting Perceived Discrimination.
Results
Descriptive statistics for the subsection of GSS 2018 respondents who were assigned both the Stigma module and the Everyday Discrimination module are shown in Table 1. Over half of respondents are female (54%), with approximately 76% identifying as White, 14% as Black, and 9% as a different race. Approximately 7% of respondents identity as sexual minorities. The average age or respondents is 46.6 (SE = .73), and the average social desirability score is 3.69 (SE = .07). The dependent variables used in these analyses are also shown in Table 1. Approximately 29% of respondents report that people act as if they are afraid of them at least a few times a year. Almost half of respondents (46%) report that people act as if they are not smart at least a few times a year, over half of respondents (61%) report being treated with less courtesy and respect than others at least a few times a year, and approximately 15% of respondents report being harassed or threatened at least a few times a year. Approximately 41% of respondents report receiving poor service or restaurants at least a few times a year.
Descriptive Statistics, General Social Survey 2018.
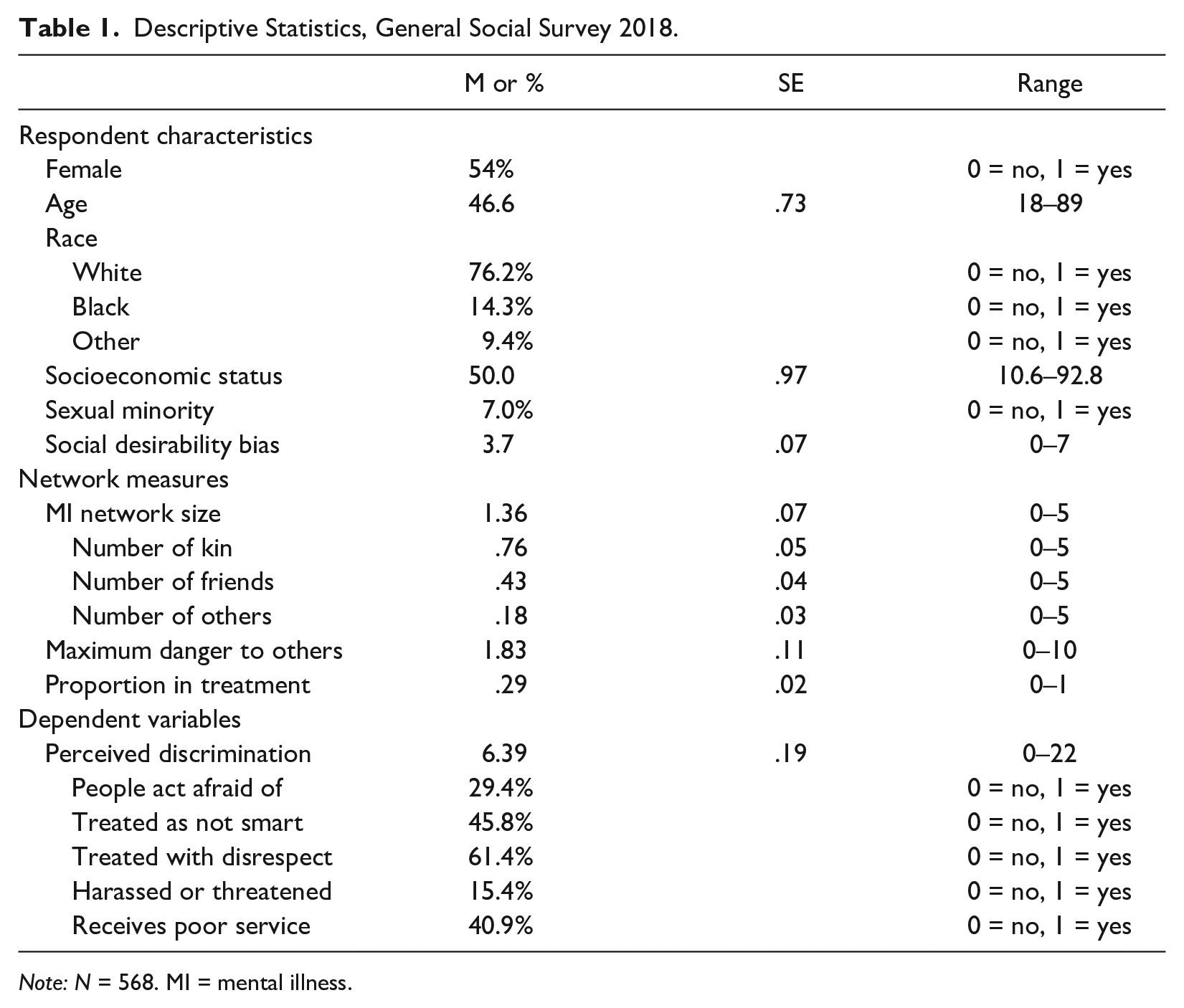
Note: N = 568. MI = mental illness.
Table 2 displays findings regarding the association between mental illness network variables and perceived discrimination. More specifically, Table 2 estimates survey-weighted linear regression models predicting perceived discrimination experiences among all respondents with good mental health. As Model 2 in Table 2 shows, the size of a mental illness network matters; a 1-tie increase in network size is associated with a .67-point increase in perceived discrimination experiences (p < .001). Although the quantity of contact matters, the type of contact is also important to consider. As Model 4 in Table 2 suggests, having more core ties (i.e., family and friends) but not peripheral ties (i.e., acquaintances and coworkers) with mental illness is associated with greater perceived discrimination. In line with previous research, having family members with mental illness is associated with a greater likelihood of experiencing chronic discrimination (b = .50, p < .05). This patterning extends to friendship ties (b = .62, p < .01) but not to peripheral ties.
Survey-Weighted Linear Regressions Predicting Perceived Discrimination Experiences.
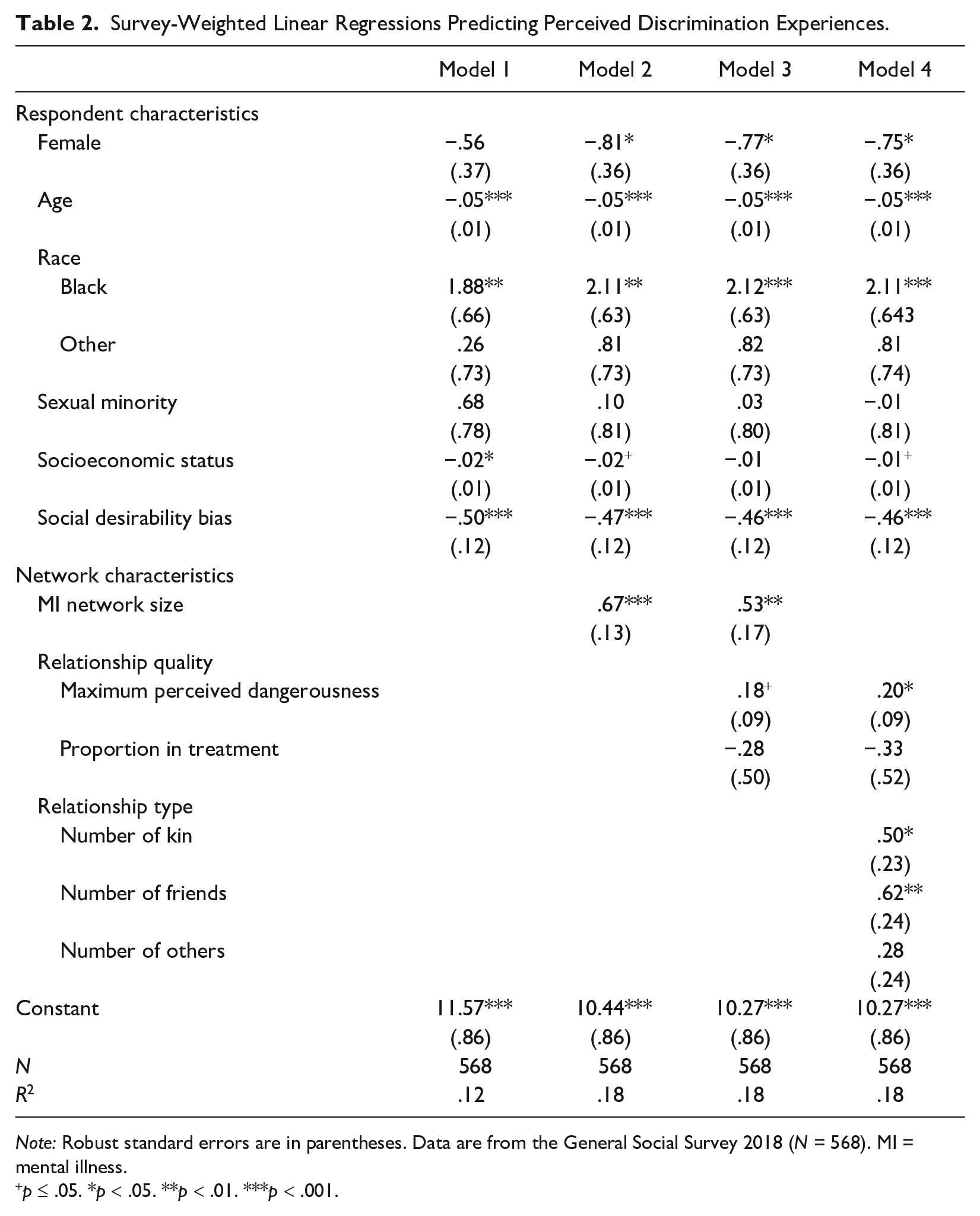
Note: Robust standard errors are in parentheses. Data are from the General Social Survey 2018 (N = 568). MI = mental illness.
p ≤ .05. *p < .05. **p < .01. ***p < .001.
In addition to network size and network composition, certain network characteristics are also associated with perceived discrimination experiences. 1 As Model 4 in Table 2 indicates, as the maximum perceived dangerousness of the mental illness network increases, so too does an ego’s experience of perceived discrimination (b = .20, p < .05). Although, being embedded in mental illness networks with less alters receiving mental health treatment does not appear to increase the likelihood of reporting higher levels of discrimination. Thus, Table 2 conveys how the quantity and quality of contact with individuals with mental illness are correlated with an ego’s experiences with associative stigma and perceived discrimination. Taken together, results support Hypotheses 1 and 2 and partially support Hypothesis 3: Examining mental illness network size, composition, and characteristics reveals significant variation in associative stigma experiences.
Table 3 displays the relationship between network measures and each form of perceived discrimination separately. Respondents’ odds of being treated as someone to fear (OR = 1.20, p < .01), treated as not smart (OR = 1.26, p < .001), treated with less courtesy or respect (OR = 1.20, p < .01), and harassed or threatened (OR = 1.27, p < .001) increase with the more social ties with mental illness that they report. Yet having larger mental illness networks is not significantly associated with greater odds of receiving poor service in restaurants and stores. These results also provide further support for Hypothesis 2: Having core ties, but not peripheral ties, increases the odds of experiencing various forms of perceived discrimination. Having more family members with mental illness increases the odds of being treated as someone to fear (OR = 1.22, p < .05), treated as not smart (OR = 1.24, p < .01), treated with less courtesy or respect (OR = 1.24, p < .05), and being harassed or threatened (OR = 1.21, p < .05). Having more friends also increases the odds of being treated as not smart (OR = 1.34, p < .01) and of being harassed or threatened (OR = 1.37, p < .01).
Survey-Weighted Logistic Regressions Predicting Perceived Discrimination in Concealable versus Nonconcealable Contexts.
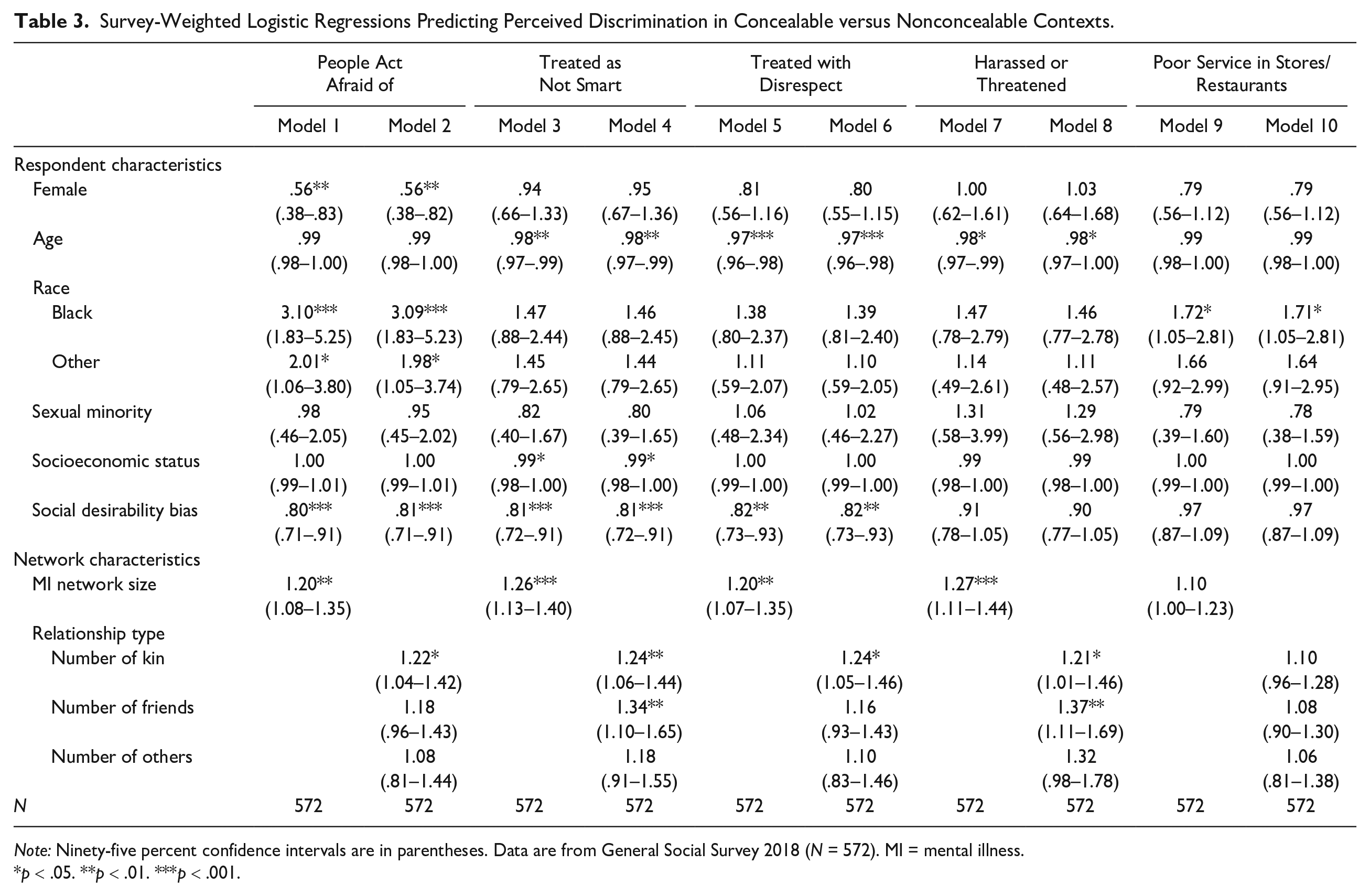
Note: Ninety-five percent confidence intervals are in parentheses. Data are from General Social Survey 2018 (N = 572). MI = mental illness.
p < .05. **p < .01. ***p < .001.
As Figure 1 demonstrates, respondents have greater predicted probabilities of being feared, treated as not smart, treated with less respect, and harassed or threatened as their mental illness network size increases, although the increase and significance vary by type of perceived discrimination. The predicted probability of being feared increased by 17 points, while the predicted probability of being treated as not smart and treated with disrespect increased by 26 points and 18 points, respectively. Taken all together, results suggest that having more social relationships with those experiencing mental illness, especially among family and friends, increases the likelihood of experiencing discrimination.
Supplemental Analyses
Additional analyses (Appendices A and B in the online version of the article) estimate logistic regression models predicting the ORs of reporting perceived discrimination using items specific to having relationships with people with mental health issues. Results provide additional support for several hypotheses and validation for the GSS measures, as well as directly test blame processes. The odds of experiencing any type of discrimination (OR = 1.24, p < .001), being treated as not smart (OR = 1.17, p < .01), and being treated with less courtesy or respect (OR = 1.15, p < .01) increase with the more social ties that a respondent reports; being treated as someone to fear marginally increases (OR = 1.19, p = .05). Furthermore, the odds of being blamed for a social ties’ mental illness (OR = 1.18, p < .01) increase with the more social ties that a respondent reports. Meanwhile, having core ties, but not peripheral ties, with mental illness increases the odds of reporting any perceived discrimination (family: OR = 1.28, p < .001; friends: OR = 1.26, p < .01) and being blamed for their social ties’ mental health issue (family: OR = 1.17, p < .05; friends: OR = 1.21, p < .05).
Discussion
In his important work on stigma, Goffman (1963:30) originally suggested that “the problems faced by stigmatized persons spread out in waves, but of diminishing intensity.” This study implements a social network approach to better understand what social factors (e.g., relationship type and network characteristics) may exacerbate or diminish the intensity of these proverbial waves. Although social network methods have contributed to our understanding of public stigma (Felix and Lynn 2022; Perry et al. 2022), I know of no studies that have applied social network methods to the study of associative stigma. Thus, this study contributes to the literature by comprehensively examining how variation in social relationships with stigmatized others is associated with variation in stigmatizing experiences.
Findings reveal that having more social connections with mental illness is associated with greater perceived discrimination, as is having meaningful connections to valued ties (both friends and family members) and being embedded in mental illness networks with stereotype-confirming social ties. Additionally, having more social ties with mental illness, especially more core ties, significantly increases the odds of reporting non-context-specific social devaluation experiences (e.g., being disrespected, feared, harassed, or treated as unintelligent) but not of reporting poor service in a store or restaurant. Supplementary analyses validate results using mental illness-specific discrimination measures and find that having more core ties also increases the odds of being blamed for their social ties’ mental illness.
These findings have theoretical implications for how we conceptualize associative stigma. Integrating a network approach into the study of associative stigma sheds light on the extent to which stigma is experienced within a given population and expands our understanding of potential stigma targets. Although qualitative approaches that focus on a single familial relationship are important, social network methods can provide researchers with the tools to capture previously unaccounted for variation in the quantity and quality of social relationships. First, the majority of respondents who know someone with mental illness know multiple people with mental illness, and findings suggest that having more robust mental illness networks increases the likelihood of experiencing associative stigma. Thus, when Goffman (1963:30) elicited the “loyal spouse of the mental patient” to exemplify a stigma target, it is important to situate this marriage within the spouse’s broader social network. A spouse who is embedded in a robust mental illness network (i.e., has several friendship and familial ties contending with mental illness) will experience associative stigma more acutely than a spouse who does not have additional social ties contending with mental illness. This study advances stigma theory by highlighting the consequential role that network positioning plays in the associative stigma process and by conveying the cumulative effect of interpersonal contact with stigmatized others on stigma experiences. Although this study focuses on mental illness in particular, this approach can be applied to a variety of devalued marks or identities (i.e., physical illness, criminal record, LGBT identity).
Second, this study suggests that shame, blame, and contamination processes (Corrigan and Miller 2004; Pescosolido and Martin 2015) are not limited to kin ties and should be extended to other core ties. Theorizing exclusively about familial stigma does not account for the experiences of the 30% of respondents who know at least one person with mental illness but do not have familial ties. Having more friends with mental illness is associated with greater levels of perceived discrimination in general and with being blamed for their social ties’ mental health issues in particular. Just as the public shames and blames some parents and siblings for their family members’ mental illness, results suggest that the public perceives some individuals as bearing responsibility for their friend’s mental illness (e.g., due to inadequate provision of social support). People may also avoid social relationships, such as romantic relationships, with both the kin and friendship ties of stigmatized individuals for fear of contamination (i.e., belief that mental illness will be “passed on” to offspring). Although existing studies posit that genetic causal attributions of mental illness contribute to the social avoidance of siblings and children of people with mental health issues (e.g., Phelan 2005), this study suggests that contamination processes may also emerge due to perceived friendship-based homophily. Just as the public may make assumptions regarding the genetic susceptibility of the daughter of someone with clinical depression, the public may infer a person’s mental health status based on the depression diagnosis of their best friend and socially avoid or devalue them as a result. Thus, this study sheds light on the processes of shame, blame, and contamination through the application of two important network concepts: tie strength (i.e., Granovetter 1973; Morgan et al. 1997) and homophily (i.e., McPherson et al. 2001).
Third, results suggest that experiencing associative stigma may be less prevalent in certain social contexts compared to others. In contrast to some conspicuous “marks” or devalued social identities that are immediately visible during social interactions, mental illness is regarded as concealable under certain circumstances (Pescosolido and Martin 2015). In fact, individuals with mental illness report concealing their mental health status in some social situations, a stigma resistance effort that people use to counter the negative effects of perceived stigma on well-being (Thoits 2011). Deflection occurs when individuals with mental illness distance themselves from a mental illness label and therefore reduce the potential of prejudice and discrimination (Thoits 2011; Thoits and Link 2016). This study suggests that the wise may also engage in similar stigma resistance efforts. The social ties of people with mental illness do not appear to have significantly greater odds of experiencing discrimination in contexts where social interactions are brief (e.g., service in a store or restaurant). Yet these social relationships are bound to be more conspicuous in other social contexts: The mother of a child with mental health issues does not conceal this relationship from her child’s doctor, and the close friend of someone who is open about their depression cannot always conceal their friend’s mental health status even if they wanted to. Core ties of people with mental illness may report being disrespected, feared, harassed, or treated as unintelligent by the public when their associations with stigmatized others cannot be concealed but may engage in stigma resistance efforts, such as deflection, in more concealable contexts.
In addition to substantive and theoretical implications, this study has important policy implications. First, this study suggests that when negative cultural stereotypes about mental illness and dangerousness (Martin et al. 2000; Pescosolido et al. 2019) are confirmed on an individual basis, they may reinforce both public and associative stigma. Thus, the consequences of these negative cultural beliefs may be more extensive than policymakers and researchers would surmise if focusing exclusively on public stigma measures, and initiatives aiming to reduce dangerousness stereotypes have the potential to not only ameliorate public stigma but also diminish associative stigma. For example, the recent Surgeon General’s advisory on mental health that provided best practices for the media, such as “avoiding harmful stereotypes about mental illness, such as the idea that people who have a mental illness are prone to violence or that mental illness causes violence,” could reduce both public and associative stigma if taken into consideration (Office of the Surgeon General 2021).
Second, results reaffirm that resources and advocacy should be directed towards the family members of those with mental illness and suggest that these resources should also be extended to friendship ties. Given that approximately one-third of people who have social relationships with people with mental illness do not have familial ties, strategies and policies aiming to support family members are not reaching the thousands of friendship ties at risk of experiencing associative stigma and should more explicitly target friends as well. Third, anti-stigma campaigns addressing public stigma through an epidemiological approach or campaigns encouraging interpersonal contact and social disclosure should consider how they may inadvertently impact associative stigma. These results suggest that some anti-stigma campaigns that are designed to alleviate public stigma by increasing interpersonal contact and social disclosure could unintentionally exacerbate stigma by association. For example, an anti-stigma campaign strategy that encourages social disclosure as a stigma reduction mechanism implicitly suggests friendship-based homophily that may exacerbate associative stigma when it explicitly states “chances are, your friends won’t find it weird at all. They might even be going through something similar” (Bring Change to Mind 2018). More research is needed to explore if these types of messages impact stigma by association in the process of combatting public stigma.
Although this study is an important first step toward more comprehensively understanding associative stigma, it is not without limitations. First, associative stigma is measured with the everyday discrimination scale (EDS), which is not mental illness-specific. Scholars contend that the EDS can be effectively implemented without assessing respondent attribution or identification of mistreatment (e.g., Lee and Turney 2012). Supplementary results using mental health-specific items also validate key findings (see Appendices A and B in the online version of the article). Even so, future research should verify if similar patterns emerge when using nationally representative social network data to examine mental illness-specific stigma and discrimination measures. Additionally, this study relies on only one perceived discrimination item (i.e., receiving poor service at a restaurant) to indicate concealable contexts, and it is possible that this measure differs from the other perceived discrimination items in multiple ways. Future studies should examine additional measures to capture concealable versus nonconcealable contexts more comprehensively. This study also focuses on the associative stigma experiences of people with good mental health. Future research should also investigate potential additive effects of having poor mental health and having various social ties with poor mental health. I also cannot disentangle whether these perceptions stem from felt stigma or enacted stigma. Although the consequences of felt (perceived) stigma are powerful (Scambler 2004), measuring enacted stigma through experimental approaches could validate these findings further.
Finally, the name generator used in the GSS to elicit egocentric network data was truncated, and only a few follow-up questions about each alter (i.e., name interpreters) were asked. Network scholars commonly limit the number of ties and name interpreters asked in egocentric network surveys to reduce respondent burden. However, this methodological strategy also underestimates some respondents’ mental illness network size and limits potentially relevant information about the ego–alter relationship (Perry et al. 2018). Future research should explore other potentially relevant network characteristics and focus on social ties who may be experiencing mental health issues but have not received an official diagnosis.
Nonetheless, this study is an important step in deepening our knowledge of an understudied form of stigma: the social exclusion and devaluation experienced by the social ties of stigmatized individuals. This research advances our understanding of associative stigma by drawing on social network methods to comprehensively measure the quantity and quality of social relationships with people with mental illness to elucidate which types of social relationships are associated with greater stigma by association and under what circumstances is it more likely to occur. Interpersonal experiences with stigmatized others vary greatly, and social network methods are a valuable tool to capture how this variation shapes stigma by association.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465241261711 – Supplemental material for Marked by Association(s): A Social Network Approach to Investigating Mental Health-Related Associative Stigma
Supplemental material, sj-docx-1-hsb-10.1177_00221465241261711 for Marked by Association(s): A Social Network Approach to Investigating Mental Health-Related Associative Stigma by Elizabeth Felix in Journal of Health and Social Behavior
Footnotes
Supplemental Material
Appendices A through C are available in the online version of the article.
Notes
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.