
Abstract
During the COVID-19 pandemic in the United States, the success of public health authorities’ strategies to curb the spread of the virus hinged on individuals’ voluntary compliance with their directives. This study considers how two components of the cultural authority of public health influenced compliance with health guidelines during the pandemic: (1) individuals’ views of public health officials as legitimate and (2) the shared value of health. I also examine the influence of other basic values, alongside health, on pandemic behavior. Data come from an original survey of 1,356 U.S. adults collected online in spring 2022. Findings reveal the pivotal role of perceived legitimacy of public health authorities in motivating compliance, even when considering perceived threat of the virus, political orientation, and other contextual factors. Results provide insight into why people complied with health guidelines by indicating how variation in individuals’ value priorities influenced behavior.
Compliance with authority directives is crucial for authority effectiveness (Johnson, Dowd, and Ridgeway 2006; Zelditch and Walker 1984). Gaining widespread compliance, however, can be “a formidable challenge” (Tyler 2010:252), as seen during the COVID-19 pandemic in the United States. To slow the spread of COVID-19, public health authorities asked individuals to engage in specific behaviors, such as wearing masks, sheltering in place, and quarantining after exposure. Prior to the availability of vaccines, individuals’ behavioral compliance with public health directives was crucial in curbing the spread of the virus, yet compliance varied widely. The importance of behavior during the pandemic stimulated research within medical and other social sciences aimed at understanding what motivated behavior, such as perceived threat of the virus (Folmer et al. 2021), personality traits (Nofal, Cacciotti, and Lee 2020), political affiliation (Kerr, Panagopoulos, and van der Linden 2021), and self- versus others-orientation (Oosterhoff and Palmer 2020). However, little work casts pandemic behaviors as (non)compliance with public health authorities; thus, the role of predictors of compliance with health authorities remains to be investigated.
Work on authority within medical sociology distinguishes between social and cultural authority (Starr 1982). Social authority “involves the control of action through the giving of commands” (Starr 1982:13). Cultural authority is the ability to define reality and impose “judgments of meaning and value . . . as valid and true” (Starr 1982:13). 1 Cultural authority, in theory, precedes and justifies social authority, which is demonstrated when individuals comply with authority directives (Epstein and Timmermans 2021; Starr 1982). The pandemic foregrounded the cultural authority of public health as public health officials provided knowledge about the virus and directives on appropriate measures to combat it, which prioritized the value of health over other aspects of life. Challenges to the cultural authority of public health also arose when individuals (e.g., politicians, activists, or the media) criticized the pandemic response, questioning public health information and guidance.
This study investigates whether and how the cultural authority of public health authorities influenced compliance with their directives during the COVID-19 pandemic. Despite the theoretical importance of cultural authority for effective exercise of social authority, the link between cultural and social authority remains underdeveloped theoretically and largely untested empirically in medical sociology (Epstein and Timmermans 2021). I propose an approach to capture individuals’ perceptions of cultural authority, grounded in Starr’s (1982) definition of the concept and in past social psychological work on compliance with authorities. Cultural authority, according to Starr (1982), stems from perceptions of health authorities as right, proper, and appropriate (i.e., legitimate; Johnson et al. 2006) to define and provide directives relating to health and illness and in the shared value of health. Social psychological work identifies legitimacy and shared values as key drivers of compliance with authorities. Legitimacy motivates compliance because individuals view legitimate authorities as having the right to “dictate appropriate behavior,” contributing to the belief that they should be obeyed (Tyler and Jackson 2014:78). Value alignment with authorities motivates compliance because people want to behave in line with what they think is good and important in life (Miles 2015; Schwartz and Butenko 2014; Tyler 2010). Individuals are less likely to comply with authorities lacking legitimacy or when authority directives contradict their values.
Both public health legitimacy and the shared value of health likely influenced compliance during the pandemic as public health authorities asked individuals to voluntarily adopt and refrain from behaviors that significantly impacted day-to-day life to prioritize health. Here, I investigate how perceptions of the legitimacy of public health authorities and individuals’ values shaped behavioral compliance with public health directives during the pandemic in the United States. In doing so, I heed recent calls for work on cultural authority in the health domain (Epstein and Timmermans 2021). This study contributes theoretically to understanding the cultural–social authority link by drawing on social psychological work on compliance with authorities, which provides theoretical background on why and how Starr’s (1982) conceptualization of cultural authority (comprised of legitimacy and the value of health) shapes behavior. This work also makes a practical contribution to research seeking to understand why people complied (or did not comply) with public health guidelines and provides insights for public health authorities aiming to gain compliance in future health crises.
I examine the role of two sources of authority legitimacy, at the individual and collective levels, that influence compliance: individuals’ personal support of public health authorities (propriety) and their beliefs about others’ support (endorsement; Dornbusch and Scott 1975). Propriety motivates compliance because it entails a personal evaluation of authorities as right, proper, and deserving of their position (Tyler and Jackson 2014). Perceived collective support engenders a felt obligation to obey authorities’ directives, regardless of one’s personal views, because it contributes to a view of authorities as valid and taken for granted by others (Zelditch and Walker 1984). In considering the roles of both propriety and endorsement, this study investigates the extent to which compliance was motivated more by individual versus social sources of legitimate authority, thereby delving into the why behind (non)compliance.
Alongside legitimacy, I consider the relationship between values and compliance with public health authorities. The shared value of protecting health and preventing disease motivates compliance with directives by health authorities given toward that end (Sandelowski, DeVillis, and Campbell 2008). However, as Epstein and Timmermans (2021:250) argue, work on cultural authority “should not treat health as a domain apart” but consider how “the viewpoints of health authorities on the nature of social reality may compete with or be advisory to . . . different epistemologies, values, and goals.” Many directives intended to promote health conflicted with individuals’ ability to pursue other valued goals. Using basic human values identified by Schwartz et al. (2012), I examine how the value of health, alongside other basic values, influenced compliance with recommended health behaviors. Considering the extent to which public health directives aligned with a range of values, in addition to health, can illuminate the role of the cultural authority of public health during the pandemic in contrast to competing values and provide insight into why individuals complied (or chose not to comply).
Data come from a survey of 1,356 adults living in the United States. I examine reported compliance with behaviors recommended by public health officials from the start of the pandemic in the United States (roughly March 2020) until vaccines were available in the respondents’ area because this was arguably when behavioral guidelines were most restrictive and compliance most crucial. 2
Background
Cultural Authority and Compliance
In his work on the rise of the medical profession in the United States, Starr (1982) introduced the distinction between social and cultural authority. Social authority is demonstrated when subordinates comply with authority commands. Cultural authority (also referred to as epistemic authority; see Stivers and Timmermans 2020; Whooley 2013) is the ability to “pronounce and enforce agreement on definitions of the nature of the world and the status of particular facts and values in the world” (Davis 2016:50). For physicians (the focus of Starr’s analysis), cultural authority manifests in their perceived right to delineate between health and illness, diagnose patient health problems, dictate treatments, and position health as a central value, all of which precede their social authority, demonstrated in patient compliance with their directives (Starr 1982). Challenges to cultural authority, arising when individuals look to other sources of knowledge (e.g., alternative medicine, friends, or social media; see Au and Eyal 2022), question physicians’ diagnoses, or prioritize values outside of health, may weaken social authority.
The COVID-19 pandemic highlighted the importance of the cultural authority of public health authorities for population health outcomes. The goals of public health include disease detection and prevention and protection of population health. The cultural authority of public health is thus indicated in the ability of public health authorities to position population health as a central value, define what constitutes health threats and emergencies, and specify strategies and practices to mitigate threats and protect health (see Collier and Lakoff 2010). Public health authorities exercised cultural authority during the pandemic by designating COVID-19 as a health emergency, providing authoritative information about the virus, offering policy recommendations and guidelines on individual behavior, and prioritizing population health as paramount over other concerns. The social authority of public health authorities, then, was revealed in the extent to which individuals complied with their COVID-19 guidelines.
Cultural authority is especially important for public health and other health authorities seeking compliance because, unlike law enforcement, legal, or workplace authorities, they are often unable to gain compliance through use of power or threats of sanctions. For example, many public health directives during the pandemic required voluntary adoption of specific behaviors to curb the spread of the virus, and U.S. government and health authorities could not universally surveil individuals’ behaviors or offer punishments or incentives to encourage compliance. Instead, perceptions that health authorities have the right to define reality and issue directives in the domain of health (i.e., that they possess cultural authority) can enable them to obtain voluntary compliance with difficult to enforce treatment plans, health recommendations, or pandemic guidelines (Starr 1982). Yet, to date, no studies have examined the impact of cultural authority on compliance in the pandemic context.
Much existing empirical work on medical authority focuses on the doctor–patient relationship, examining how physicians verbally express authority in interactions with patients and patients’ responses to them. Conversation analyses of doctor–patient visits indicate how, over time, physicians have become less overtly authoritative in their directives, instead presenting reasoning and evidence behind their diagnoses and decisions (see Heritage 2021), and how patients feel freer to challenge medical authority by asserting their treatment preferences and expressing uncertainty about recommendations (Cox 2023; Stivers and Timmermans 2020). Although resistance or acquiescence to physicians’ expertise implies an influence of cultural authority on patient outcomes (Spencer, Mrig, and Talaie 2022), these studies do not distinguish between cultural and social authority, directly capture whether patients perceive physicians to have cultural authority, or examine how those perceptions influence behaviors. Thus, although the role of cultural authority in gaining compliance has been discussed by Starr (1982) and others (e.g., Whooley 2013), whether it is “still the case, as Starr suggested, that the cultural authority to define prefigures and undergirds the social authority to command” remains an open empirical question (Epstein and Timmermans 2021:250).
This study contributes to research on cultural authority by integrating work in medical sociology and social psychology to propose an approach to measure individuals’ perceptions of cultural authority and empirically investigating the impact of cultural authority of public health authorities on compliance with their pandemic directives. According to Starr (1982), the legitimacy of physicians and their orientation to the shared value of health constitute their cultural authority and contribute to perceptions that they should be obeyed. In what follows, I draw on social psychological work on compliance with authorities, which provides theoretical rationale and empirical evidence for why and how legitimacy and values motivate compliance, to offer hypotheses about how cultural authority of public health authorities influenced compliance with their directives during the pandemic. I augment past work on medical authority by considering cultural authority in the broader health domain, beyond the physician–patient relationship (see Epstein and Timmermans 2021). Figure 1 depicts my conceptual model, illustrating the proposed links between legitimacy, values, and compliance.
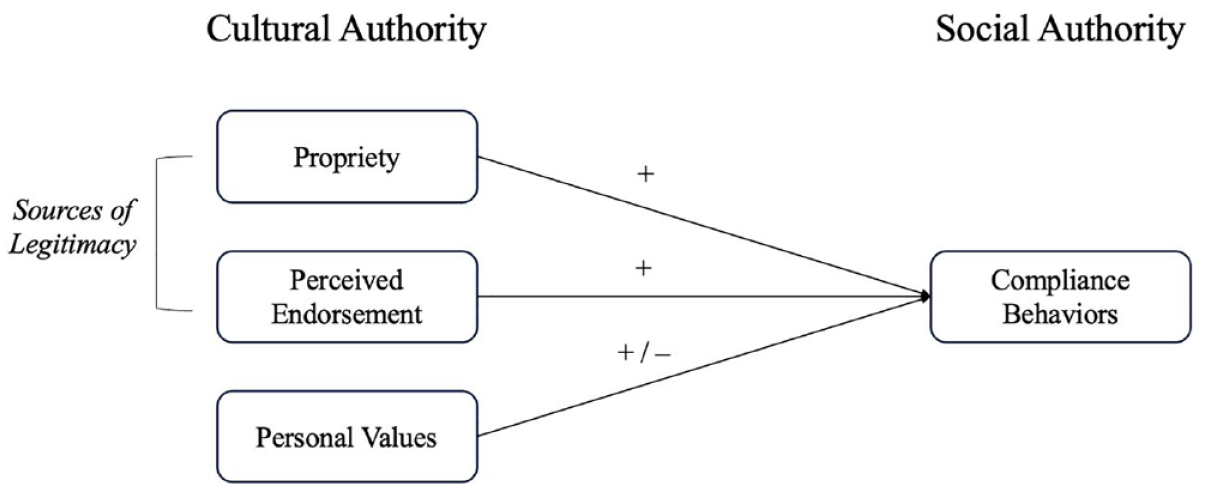
Conceptual Model of Effects of Propriety, Endorsement, and Personal Values on Compliance.
Legitimacy
Central to cultural authority is the view of the authority in question as legitimate (Davis 2016; Heritage 2021; Parsons 1947; Starr 1982; Whooley 2013). Legitimate authorities are viewed as right, proper, widely accepted, and appropriate within their social context (Johnson et al. 2006). Individuals view legitimate authorities as having the right to make decisions and “dictate appropriate behavior” within their area of expertise or governance, which contributes to the belief that they should be obeyed (Tyler and Jackson 2014:78). For health authorities, their expertise, competence, and specialized knowledge contribute to the view that they have legitimacy to offer definitions and directives in the field of health that should be followed (Parsons 1947; Schupmann and Timmermans 2023; Starr 1982). Because health authorities possess expertise beyond that of the general public, they can “claim epistemic primacy” over knowledge relating to health, which validates their interpretations and pronouncements (Cox 2023:538; Whooley 2013). Individuals’ dependence on the expertise of such authorities further boosts perceptions that they are legitimate and enhances compliance with their directives (Starr 1982).
Social psychologists (e.g., Dornbusch and Scott 1975; Johnson et al. 2006) identify two sources of legitimacy, operating at the individual and collective levels, that shape compliance with authorities. First, “propriety” refers to an individual’s personal approval and support of an authority and view that the authority is right and proper. When individuals personally approve of authorities, they are likely to accept their decisions and willingly follow their directives (Dornbusch and Scott 1975; Tyler and Jackson 2014). For example, personal approval and support of police and legal authorities enhance individuals’ likelihood to comply with the law and are more influential in securing compliance than the perceived risk of being caught or punished for breaking the law (Tyler, Goff, and MacCoun 2015).
Second, perceived “endorsement” of an authority by peers or other members of the general public constitutes a collective source of legitimacy that influences compliance. When people perceive an authority to enjoy wide social acceptance and support, they are likely to view it as taken for granted and feel obligated to conform to the social order (Dornbusch and Scott 1975; Johnson et al. 2006; Zelditch and Walker 1984). The belief that others support and follow authority directives encourages individuals to do so as well, regardless of their personal views, to avoid formal or informal sanctions from others (Dornbusch and Scott 1975; Zelditch and Walker 1984). For example, individuals are more likely to accept unfair decisions and feel less intense negative emotions about unfair outcome distributions from authorities who enjoy collective support (Johnson et al. 2016).
Whether motivated by personal approval or perceived collective support, individuals are likely to comply with directives from legitimate authorities because they feel obligated to do so. Thus, legitimacy is crucial for authorities seeking widespread compliance, especially in times of crisis and uncertainty, such as a pandemic, when they may ask individuals to accept difficult decisions or comply with disagreeable or burdensome policies for the greater good. Additionally, legitimacy entails a perceived obligation to obey even when individuals do not understand or agree with authority directives (Huq, Jackson, and Trinkner 2017) due to a personal belief that an authority’s power is justified (propriety) and/or a belief that others think so (endorsement).
The onset of the COVID-19 pandemic in the United States constituted a time of crisis and uncertainty during which the population looked to public health authorities, as experts in disease detection and prevention, for guidance. The novelty of the virus meant that there was uncertainty about how best to curb its spread, accompanied by public disagreement about the effectiveness of public health guidelines. Furthermore, health directives, prior to the availability of vaccines, severely restricted individuals’ ability to pursue normal daily activities and required personal inconvenience and sacrifice. Thus, in the pandemic context, individuals’ personal views (propriety) of public health officials as the right and proper authorities to provide information on the virus, define the severity of the health risks, and dictate behavioral guidelines (i.e., exercise cultural authority) likely enhanced compliance, even with guidelines that were difficult or when individuals were uncertain about the most effective approach. Similarly, perceived acceptance and support from others (endorsement) likely boosted compliance above and beyond individuals’ personal views.
Hypothesis 1: Individuals’ perceived propriety and endorsement of public health authorities are positively related to compliance behaviors.
Values
The shared value of health, according to Starr (1982), provides another basis for the cultural authority of health authorities that enhances compliance with their directives. That health authorities use their expertise in the service of health, “a value of usually unambiguous importance to its clients and society,” theoretically justifies their right to make authoritative claims and commands regarding health and illness (Parsons 1947; Starr 1982:5). People largely profess to value their health (see Sandelowski et al. 2008), especially in the U.S. context (see Davis 2016), which boosts the cultural authority of health experts (Starr 1982). Furthermore, the personal desire to protect and improve health provides motivation to respect and heed the advice and interpretations of health authorities about various health matters (Davis 2016).
Social psychological work demonstrates that perceptions that an authority’s decisions or directives align with one’s values enhance compliance with them. Values represent desirable goals that “serve as guiding principles in the life of a person” (Schwartz 1994:21); thus, individuals seek to embrace or avoid behaviors that enhance or thwart, respectively, pursuit of their values (Hitlin and Piliavan 2004; Schwartz and Butenko 2014). Perceptions that an authority shares one’s values contributes to the view that their authority is justified and should be obeyed, resulting in increased cooperation with them (Hamm, Trinkner, and Carr 2017). For example, individuals are more likely to obey the law and follow organizational rules when they believe that the behaviors that they prescribe are consistent with their values (Tyler and Blader 2005). By contrast, decisions and directives, even by legitimate authorities, are more likely to elicit protest and noncompliance when they contradict individuals’ values than when they are inconsistent with nonmoral beliefs or preferences (see Skitka, Bauman, and Lytle 2009).
During the pandemic, public health authorities provided guidelines and mandates that prioritized protecting population health. Past work demonstrates that valuing health translates into behavior, such as adoption of preventive health behaviors (Sandelowski et al. 2008) and compliance with medical professionals’ directives (Reed et al. 2020). However, the value of health exists alongside other values deemed desirable and important in life, with implications for behavior. For example, individuals who value an exciting life more than health are more likely to engage in risky health behaviors (Kristiansen 1986). During the pandemic, public health directives promoting health also restricted activities and social interactions, thereby obstructing pursuit of other values, outside of health. The importance of alternative values to health may weaken the effect of public health’s cultural authority on compliance with directives that conflicted with those values. Thus, the effect of the value of health on compliance should not be considered in isolation but alongside other, potentially competing, values.
Schwartz’s (1994, 2005) theory of basic values identifies 10 values that express goals relating to fundamental requirements for human survival and flourishing that influence behavior. 3 In addition to health and safety (captured by security), other values include conformity, tradition, benevolence, universalism, self-direction, stimulation, hedonism, achievement, and power (see Table 1). Although all values are desirable, individuals vary in the importance they ascribe to different values. Additionally, the motivational goals underlying specific values may conflict with each other in a given context. Thus, in determining modes of action, individuals engage in trade-offs among values depending on their importance and salience in the situation.
Basic Human Values and Definitions.
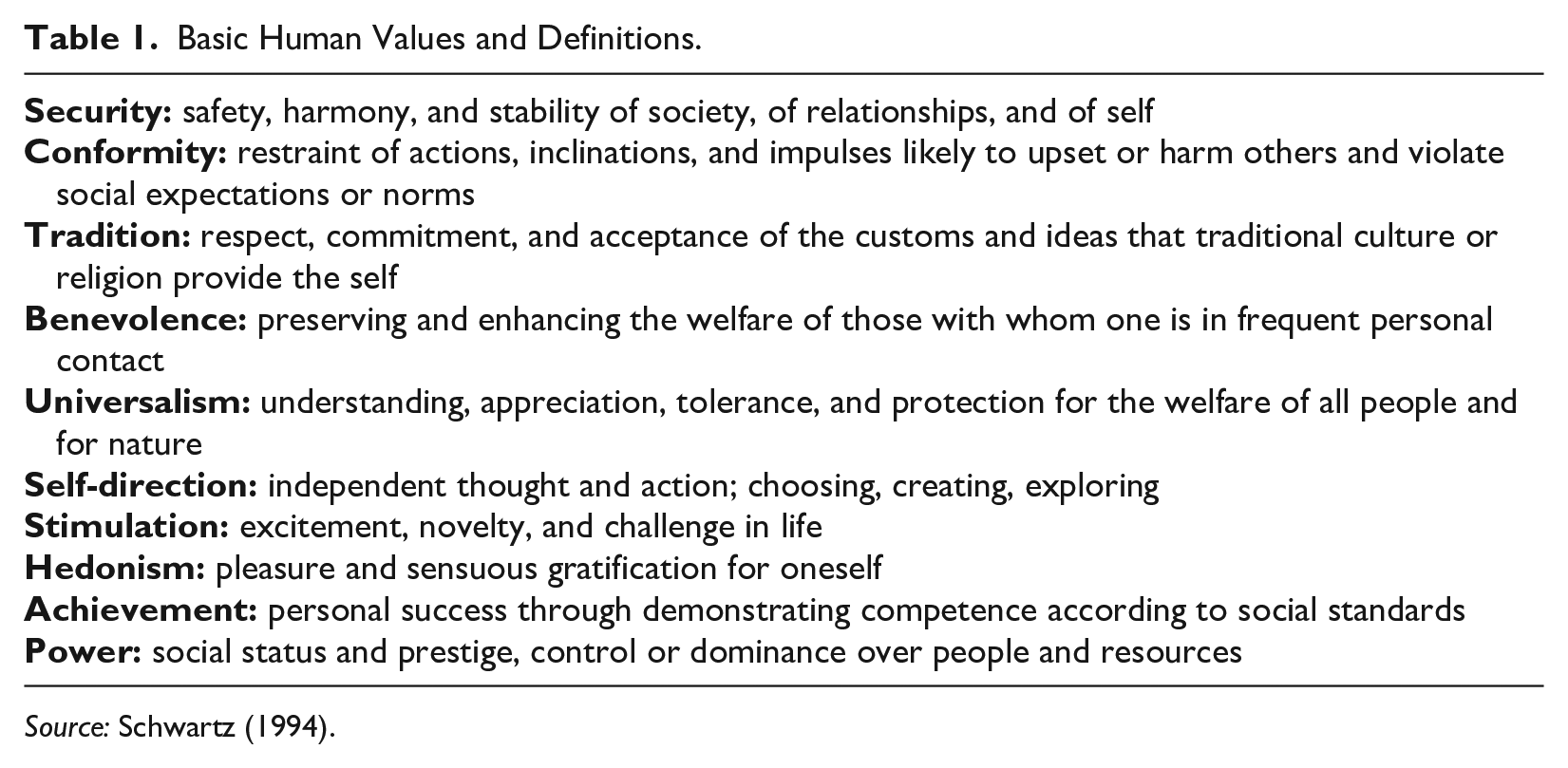
Source: Schwartz (1994).
A circular continuum (see Figure 2; Schwartz 2005) illustrates the relationships among the values, with more compatible values nearer and competing values opposite each other. The orthogonal positioning of the four higher-order values (conservation vs. openness to change and self-transcendence vs. self-enhancement) depicts the tensions between the motivational goals underlying the values. Conservation values, emphasizing health, stability, social order, and preserving traditional customs/ideas (security, conformity, and tradition), oppose openness to change values, emphasizing desires for independence in thought/action and new and varied experiences (self-direction and stimulation). Self-transcendence values, expressing concern for the well-being of friends and family (benevolence) and the welfare of all people (universalism), oppose self-enhancement values, expressing goals related to personal success (achievement) and control over resources and people (power). Hedonism, emphasizing pleasure and enjoying life, overlaps with openness to change and self-enhancement values. The (in)compatibilities among the values help guide predictions about relationships between values and behaviors.
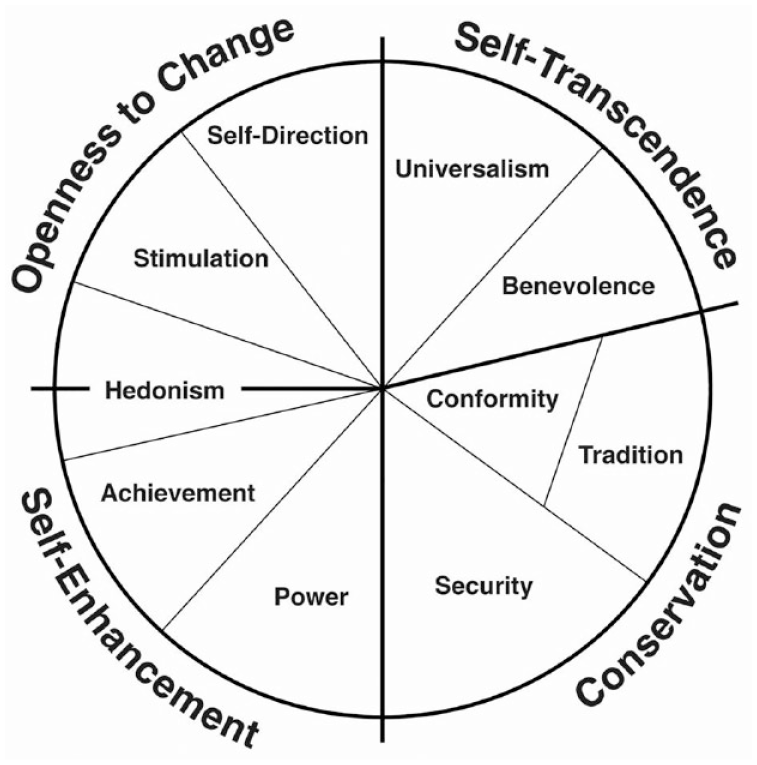
Theoretical Model of Relations among 10 Values.
During the pandemic, the underlying goals of public health directives (to prevent disease and mitigate the health crisis) were most congruent with conservation values of security and conformity. The importance of these values, therefore, should positively relate to compliance with health guidelines. By contrast, health guidelines, such as lockdowns and directives to avoid travel and social gatherings, prioritized conservation values over openness to change values by restricting freedom of movement (self-direction) and hindering opportunities for new experiences, risk-taking (stimulation), and enjoying life (hedonism). Individuals who value self-direction may resist authority commands if perceived to impinge on individual autonomy. Similarly, those who view experiences and pleasure as central to a good life may prefer to risk infection to pursue living life to the fullest. Thus, highly valuing openness to change values likely inhibited compliance with public health directives.
Hypothesis 2a: Conservation values of security and conformity are positively associated with compliance behaviors.
Hypothesis 2b: Openness to change values of self-direction, stimulation, and hedonism are negatively associated with compliance behaviors.
Compliance with public health directives entailed inconvenience and personal sacrifice. Public health officials often appealed to self-transcendent values to encourage compliance by casting directives as aimed at safeguarding the health and well-being of others. Individuals’ concern for the well-being of loved ones (benevolence) and the welfare of the broader population (universalism) may thus have stimulated compliance with directives that were burdensome. Some work indicates that social responsibility values (considering others’ needs) positively related to handwashing among U.S. adolescents (Oosterhoff and Palmer 2020), and social-focused values (as opposed to personal-focused ones) were associated with more social distancing among Australian adults (Lake et al. 2021). By contrast, importance of achievement and power values may be negatively related to compliance with directives that thwart self-enhancement by interfering with work or education.
Hypothesis 3a: Self-transcendence values of benevolence and universalism are positively associated with compliance behaviors.
Hypothesis 3b: Self-enhancement values of achievement and power are negatively associated with compliance behaviors.
Because tradition is a conservation value, its underlying goals are typically compatible with those of security and conformity, which should enhance compliance. However, directives to stay home and avoid social gatherings and nonessential travel prevented observation of many family, cultural, and religious customs (e.g., weddings, holidays, and religious services). Thus, during the pandemic, importance of tradition may hinder compliance.
Hypothesis 4: Tradition is negatively associated with compliance behaviors.
In the absence of situational constraints, values drive behaviors in the direction of the goals that they express and hinder behaviors in opposition to those goals. However, contextual factors may weaken the strength of the relationship between values and behavior (Bardi and Schwartz 2003). Health-related factors likely shaped pandemic behavior, such as perceived threat of the virus, age, underlying health conditions, or living with someone over 65 and/or with underlying conditions. Geographic location may play a role because individuals in rural settings may be less likely to comply with guidelines than those in congested, urban settings. Additionally, many aspects of the pandemic became politicized, with implications for compliance (Kerr et al. 2021).
Individual characteristics also impact compliance with health authorities and may have done so during the pandemic. Racial bias and discrimination in health care contributes to mistrust and negative stereotypes about health systems and providers among racial minorities in the United States, which can diminish adherence to medical treatment and recommendations (see Dovidio et al. 2008). Individuals with higher socioeconomic status are more likely to adopt healthy behaviors and avoid unhealthy behaviors (Pampel, Krueger, and Denney 2010). Education may be associated with recognition of health risks and adoption of behaviors to mitigate those risks (Mirowsky and Ross 2015). I consider the role of contextual and demographic factors alongside propriety, endorsement, and values on compliance behavior.
Data And Methods
Data and Study Participants
Data came from a survey of 1,356 adults collected online in spring 2022. Respondents were U.S. residents, recruited from nonprobability, online panels in partnership with a university-based survey research center and Marketing Systems Group, which maintains a large sampling frame reflective of national census data regarding gender, age, race, and geography. Table 2 provides descriptive characteristics of the sample.
Sample Characteristics, N = 1,356.
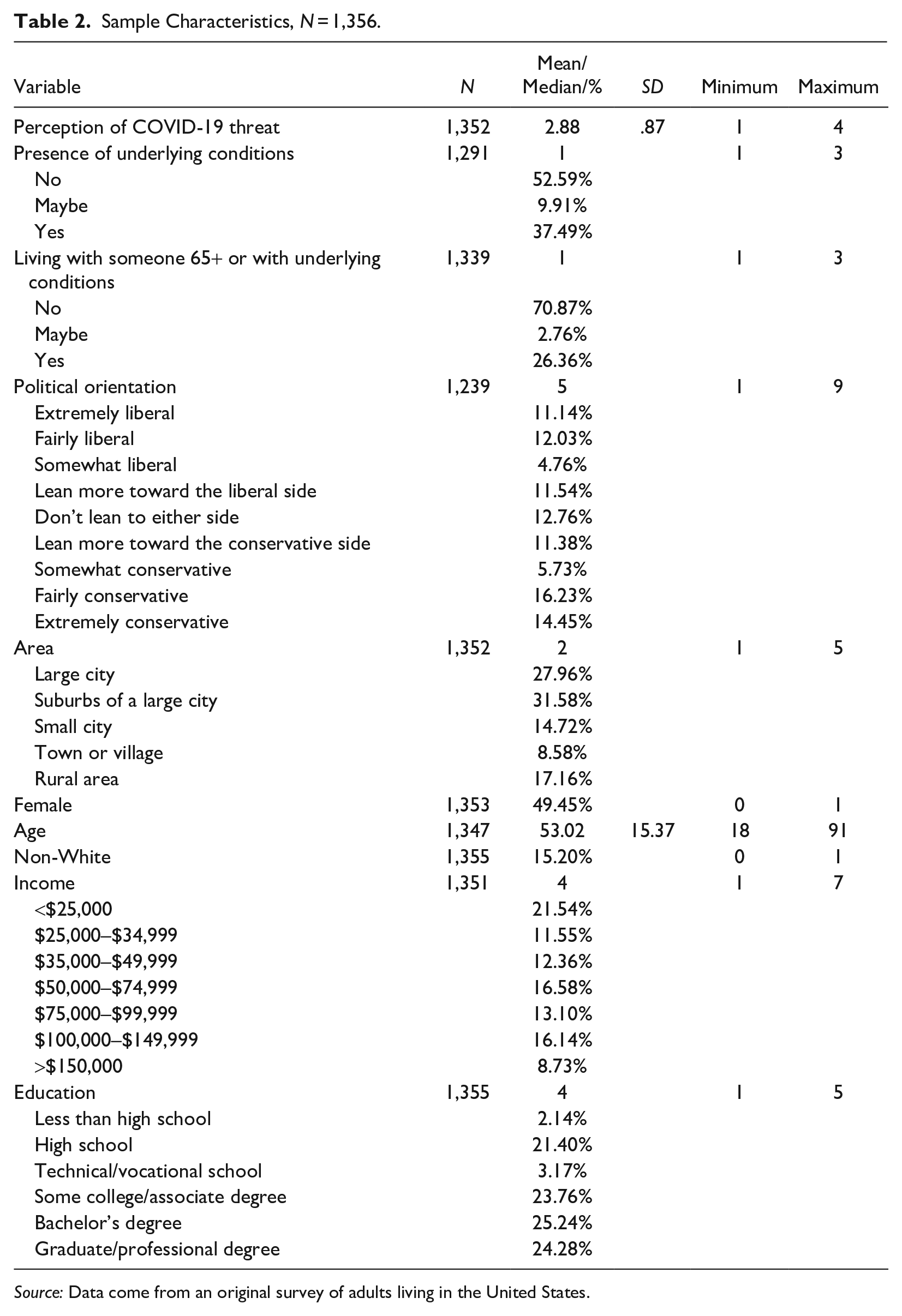
Source: Data come from an original survey of adults living in the United States.
Dependent Variables
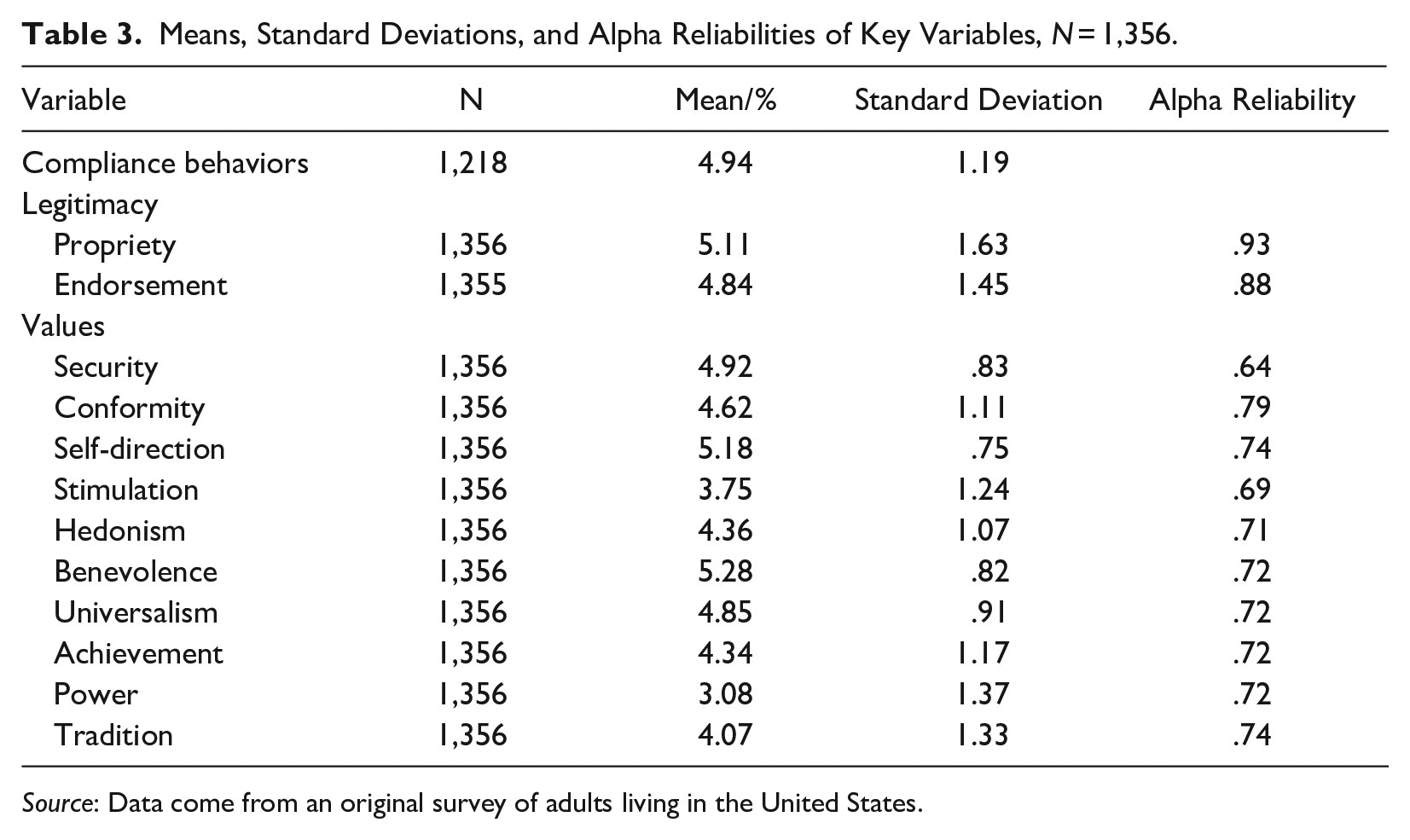
Table 3 includes means (standard deviations) of dependent and independent variables. To capture compliance, I created an additive scale (averaged by number of items) including seven items measuring the frequency of self-reported behaviors over time, following the act-frequency approach (Buss and Craik 1983) often used in work examining relationships between values and behavior (e.g., Schwartz and Butenko 2014). 4 Behaviors constituting the scale were recommended by public health officials. Respondents were asked: “Thinking about the COVID-19 recommendations and mandates, how often did you engage in each of the following from the start of the pandemic to the time that vaccines were available in your area (relative to the number of times that you had an opportunity to do so)?” Respondents reported whether they engaged in the following behaviors never = 1, rarely = 2, sometimes = 3, fairly often = 4, very often = 5, or always = 6: “wearing a face mask,” “practicing social-distancing (staying 6 feet away from other people),” “staying at home as much as possible,” “avoiding going out to bars/pubs/restaurants,” “avoiding social gatherings of more than 10 people,” “avoiding indoor social gatherings,” and “avoiding any non-essential travel.” The alpha reliability for the scale was .92.
Means, Standard Deviations, and Alpha Reliabilities of Key Variables, N = 1,356.
Source: Data come from an original survey of adults living in the United States.
Independent Variables
I used multiple items to capture propriety, endorsement, and values. For each scale, items were added and averaged. Measures of propriety and endorsement were drawn and adapted from social psychological work on legitimacy (e.g., Hamm et al. 2017; Hegtvedt et al. 2022). The following items measure propriety of public health authorities: (1) “To what extent do you see public health officials (such as the Centers for Disease Control and Prevention [CDC] or Health Department) as the right and appropriate people to look after the health and well-being of the population in general?” (2) “To what extent do you support decisions by public health officials even when you don’t understand the reasons?” and (3) “To what extent do you believe that you should comply with directives from public health officials?” Response categories range from 1 = not at all to 7 = a great deal. Alpha reliability was .93.
Items measuring perceived endorsement of public health authorities mirrored the propriety items. Items used the same response scale but asked about respondents’ beliefs about what others think. For example, “To what extent do you believe that other people in general see public health officials as the right and appropriate people to look after the health and well-being of the population in general?” Alpha reliability was .88.
The values measures included 22 items drawn (and adapted) from the Schwartz Portrait Values Questionnaire (PVQ-RR; Schwartz et al. 2012). PVQ items were statements describing an individual’s goals, desires, or preferences that “point implicitly to the importance of a value” and were matched to respondents’ self-identified gender (Schwartz 2005). Sample portrait items included “It is very important to him to avoid disease and protect his health” and “It is important to her to make her own decisions about her life” (see Appendix A for all items). For each statement, respondents indicated, “How much like you is this person?” (from 1 = not like me at all to 6 = very much like me). Respondents’ values were deduced from those of the individuals they rate as similar (or dissimilar) to themselves. For instance, “It is important to him to be the one who tells others what to do” depicts someone who values power, and “It is important to her to be tolerant toward all kinds of people and groups” portrays someone who values universalism.
The 22 items were formed into 10 scales (consisting of 2 to 3 items per scale) representing the 10 values. Alpha reliabilities ranged from .64 to .79, falling within typical ranges received using the PVQ (Schwartz, Sagiv, and Boehnke 2000). In constructing the values, I employed within-person mean centering to eliminate potential bias introduced by social desirability and respondents’ differential use of the response scales. For example, some respondents may rate themselves as similar to most portraits, whereas others may use the middle or lower ends of the scale in assessing their similarity. Regardless, each individual will produce variation across their responses, indicating their value priorities. To get at these priorities, I calculated each respondent’s mean scores across all items and subtracted their mean rating from each of their individual value scores to produce their unbiased value hierarchy (Schwartz 2005).
Contextual Factors
I measured factors during the pandemic likely to influence behaviors. Two items captured perceived threat of the virus (adapted from Folmer et al. 2021). Respondents were asked, “How much of a threat, if any, is the COVID-19 pandemic . . . for your personal health?” and “ . . . for the population in general?” (1 = not a threat, 2 = a minor threat, 3 = a moderate threat, 4 = a major threat). The Pearson correlation coefficient between these indicators was .68. Respondents reported whether they had underlying health conditions that increase the risk of severe illness from COVID-19 and whether they lived with anyone over 65 or with health conditions that increase the risk of severe illness from COVID-19. 5 Respondents indicated their political orientation and their geographic area.
Demographic Controls
Demographic controls included sex, age, race, income, and education (see Table 2 for specific categories).
Analysis Strategy
I first examined Pearson correlations between propriety, endorsement, values, contextual factors, and compliance, following the common analytical approach used to test hypotheses about relationships between Schwartz values and behaviors (e.g., Schwartz and Butenko 2014). Bivariate correlation coefficients revealed the strength and direction of the relationships between each value and compliance, indicating whether values had significant relationships with compliance in the expected directions.
I next performed a series of ordinary least squares regressions (OLS) examining effects of propriety, endorsement, and values on behaviors, including contextual factors and demographic controls. Because the values were interdependent, all 10 values could not be included in a single regression model because the coefficients would have been uninterpretable (regardless of whether multicollinearity is an issue). I ran separate regression models to investigate the effects of each value on compliance. I ran models only for values with significant correlations with compliance.
Results
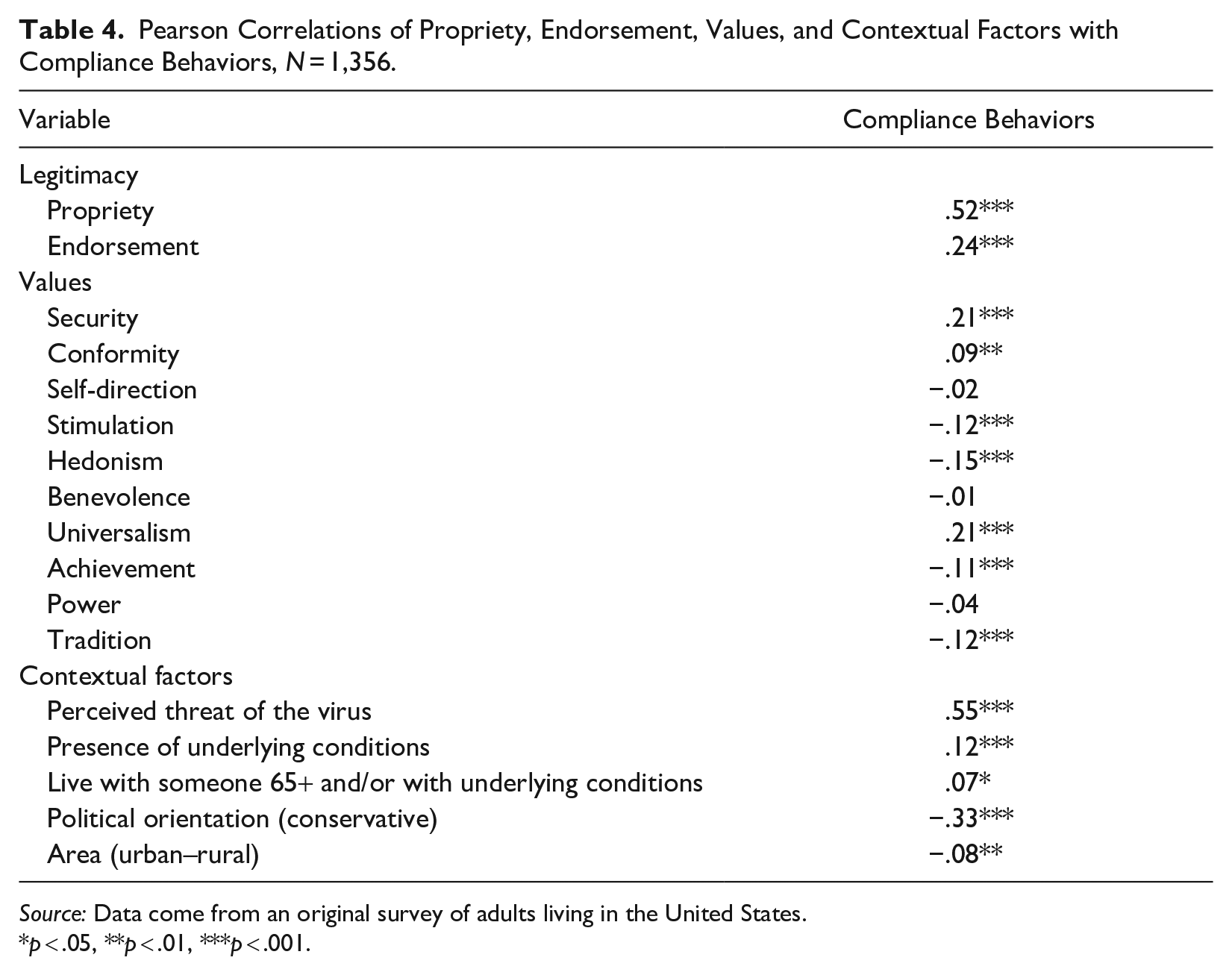
I first report bivariate correlations presented in Table 4, indicating whether they provide preliminary support for my hypotheses. Positive and significant correlations between propriety and endorsement and compliance indicate support for Hypothesis 1. Values also have significant, although weaker, associations with compliance. Security and conformity reveal positive and significant associations with compliance (Hypothesis 2a). Of the openness to change values, self-direction is negatively but not significantly related to compliance, whereas both stimulation and hedonism reveal significant negative correlations (Hypothesis 2b). Among self-transcendent values, universalism positively and significantly correlates with compliance; however, benevolence does not have a significant association (Hypothesis 3a). Self-enhancement values negatively correlate with compliance, but only achievement has a significant correlation (Hypothesis 3b). Finally, tradition has a significant, negative correlation with compliance (Hypothesis 4).
Pearson Correlations of Propriety, Endorsement, Values, and Contextual Factors with Compliance Behaviors, N = 1,356.
Source: Data come from an original survey of adults living in the United States.
p < .05, **p < .01, ***p < .001.
Among contextual factors, perceived threat of the virus, presence of underlying conditions, and the status of living with someone over 65 or with underlying conditions are each positively and significantly correlated with compliance. Living in a rural area (in comparison to urban) and conservative political orientation are both negatively related to compliance.
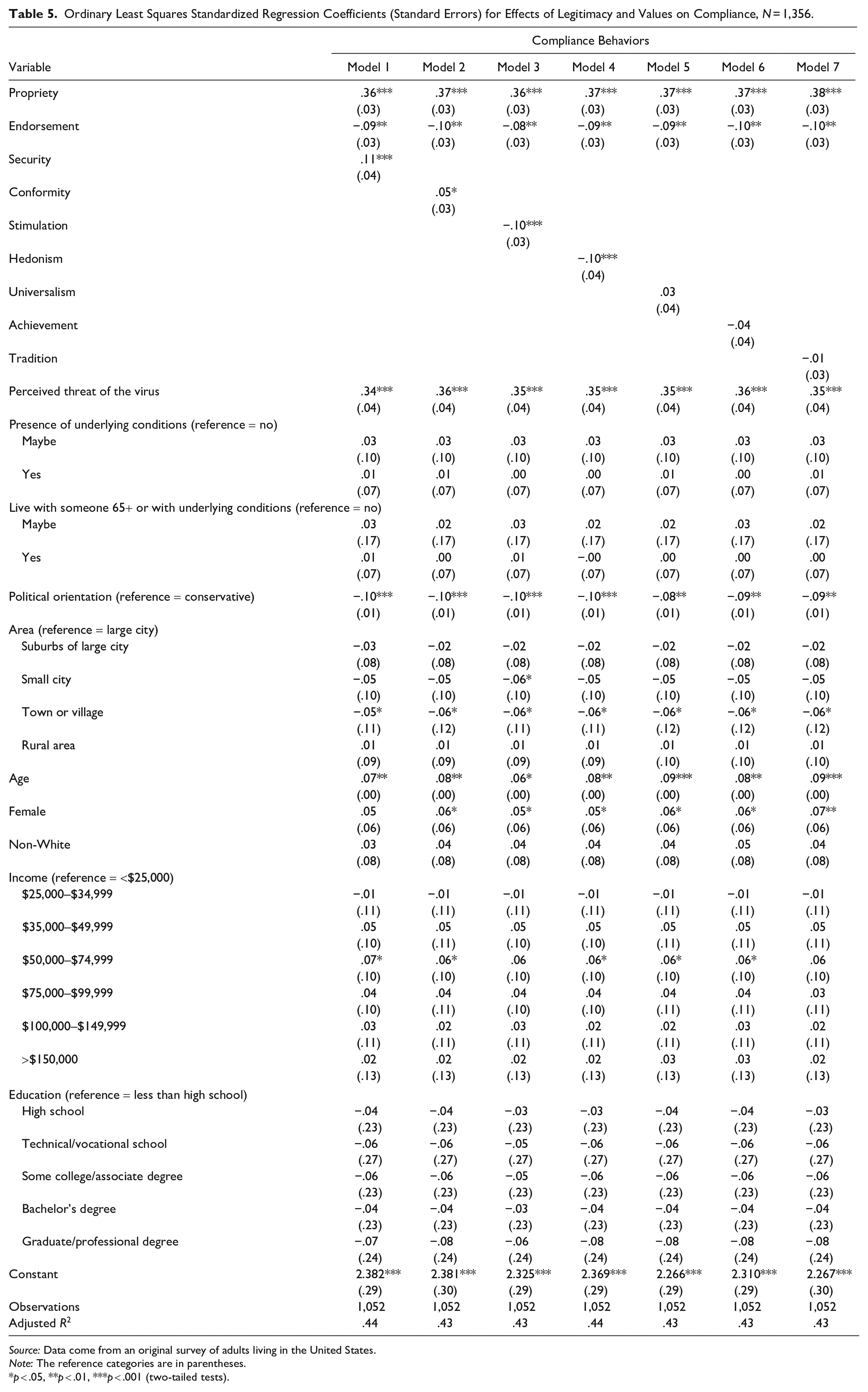
Table 5 presents results of the OLS analysis. In support of Hypothesis 1, propriety positively and significantly affects the frequency of engaging in compliance behaviors. Across all models, effects of propriety range from β = .36 to β = .38 (p < .001). Inconsistent with Hypothesis 1, endorsement has a significant negative effect on compliance (effects range from β = −.08 to β = −.10, p < .01).
Ordinary Least Squares Standardized Regression Coefficients (Standard Errors) for Effects of Legitimacy and Values on Compliance, N = 1,356.
Source: Data come from an original survey of adults living in the United States.
Note: The reference categories are in parentheses.
p < .05, **p < .01, ***p < .001 (two-tailed tests).
When taking legitimacy and contextual factors into account, only a subset of values maintains significant effects on compliance. Additionally, the associations between values and compliance are weaker than suggested by the correlations, as expected (Bardi and Schwartz 2003). Significant regression coefficients reveal which values influenced compliance; however, the magnitude of the effect sizes is much smaller than that of propriety and contextual factors.
As predicted in Hypothesis 2a, importance of conservation values enhances compliance. Security positively affects compliance (Model 1: β = .11, p < .001), and conformity has a weak positive effect (Model 2: β = .05, p < .05). In partial support of Hypothesis 3b, openness to change values of stimulation (Model 3: β = −.10, p < .001) and hedonism (Model 4: β = −.10, p < .001) have negative effects on compliance.
Although I expected that importance of self-transcendence values would enhance compliance (Hypothesis 3a), universalism (Model 5) has no effect. Additionally, achievement does not affect compliance (Model 6), disconfirming Hypothesis 3b predicting self-enhancement values to have a negative impact. Finally, although tradition significantly correlates with behaviors, when considered alongside legitimacy, contextual factors, and demographic controls, tradition has no effect (Model 7), disconfirming Hypothesis 4.
Among contextual factors, perceived threat of the virus has a strong positive effect on compliance (effects range from β = .34 to β = .36, p < .001). Reported presence of an underlying condition and the status of living with someone over 65 or with an underlying condition do not contribute to compliance. Political conservatism negatively affects compliance (effects range from β = −.08 to β = −.09, p < .001). Compared to those living in a large city, respondents living in a town/village were less likely to comply with health authorities (effects range from β = −.05 to β = −.06, p < .05).
Older age is positively associated with compliance (effects range from β = .06, p < .05 to β = .09, p < .001). Women were more likely to report compliance than men (effects range from β = .05, p < .05 to β = .07, p < .01). Compared to respondents earning less than $25,000, those with an annual income of $50,000 to $74,999 were more likely to comply (effects range from β = .06 to β = .07, p < .05). Education and race had no effect.
Discussion
This study contributes to research aimed at understanding individual behavior during the pandemic by examining how the cultural authority of public health authorities shaped compliance with their directives. This work contributes to broader theoretical and empirical questions about the link between cultural and social authority in the health domain by proposing legitimacy and values, both core to Starr’s (1982) definition of cultural authority and measurable constructs grounded in social psychological work on compliance with authorities, as a way to capture individuals’ perceptions of cultural authority and empirically test its effects on behavior. This approach provides insight into how individual (propriety) and collective (endorsement) sources of legitimacy influenced compliance and the relative impact of each. Additionally, utilizing a range of basic values sheds light on how health concerns exist in tension with other values that may compete for cultural authority, with implications for compliance. Findings reveal the importance of the cultural authority of public health for individual behaviors that translate into population health outcomes, providing support for recent calls for work on cultural authority of health generally (see Epstein and Timmermans 2021).
First, individuals’ personal view of public health officials as legitimate (i.e., propriety) strongly shaped compliance, over and above other motivating factors in the pandemic context, such as perceived risk of the virus, personal health conditions, and political orientation (Hypothesis 1). This finding empirically supports Starr’s (1982) and others’ (see Heritage 2021;Whooley 2013) theoretical emphasis on the importance of the belief that health authorities have the legitimate right to provide guidance and directives regarding health as undergirding their social authority. To ensure future compliance, public health authorities should focus on gaining and maintaining propriety. In addition to the competence and expertise that Starr (1982) noted as a basis for legitimacy (an instrumental base), work in social psychology (e.g., Tyler 2010) points to relational and moral bases. Public health authorities might gain propriety on relational grounds by showing concern for individuals’ well-being and on moral grounds by demonstrating integrity and abiding by ethical standards. The specific ways that public health authorities attend to each base will also depend on the social context and level of interaction. For example, an individual public health official could gain propriety on instrumental grounds by effectively administering vaccines, whereas the CDC might do so through demonstrating expertise in research and policy recommendations.
Second, perceived endorsement of public health authorities did not enhance compliance during the pandemic and instead diminished it. This surprise finding contradicts the hypothesized positive effect of endorsement (see Figure 1) and prior work indicating that perceived collective support often has a stronger effect on compliance than propriety (see Johnson et al. 2006). Conflicting opinions about the effectiveness of public health guidelines in the news and social media and a wide array of information (and “misinformation”) about the virus (Pan American Health Organization 2020) may have reduced the weight that people placed on perceived endorsement of public health authorities in determining their own behavior. As multiple voices increasingly vie for cultural authority on health (see Epstein and Timmermans 2021), public health (and other medical) authorities must be wary of taking perceived collective support for granted as a boost to compliance.
Understanding the negative effects of endorsement requires additional research. This finding may reflect a view that others’ support for (and thus assumed compliance with) public health authorities lessens one’s own responsibility to follow health guidelines. Given the negative effects of endorsement, the positive correlation between endorsement and compliance also presents a puzzle. Past work indicates that endorsement enhances perceived propriety of authorities (Yoon and Thye 2011); thus, propriety may mediate positive effects of endorsement on compliance. Future work might investigate this potential pathway. Regardless, results suggest that individuals’ personal perceptions of public health authorities’ cultural authority, rather than perceptions that they have such authority in the broader social context, are what mattered for compliance during the pandemic.
Third, the extent to which public health directives aligned with basic values influenced (non)compliance, in line with past social psychological research on values and compliance with authorities. The value of health and safety (captured by security), central to cultural authority, motivated adherence to public health directives. However, findings indicate that public health authorities must recognize the importance for compliance of other basic values, outside of health. Even during a global pandemic, public health officials cannot assume that individuals will prioritize health over other concerns about what makes life meaningful. Significant correlations between values and behaviors (mostly in the anticipated directions per Hypotheses 2a, 2b, 3a, 3b, and 4) suggest how other value considerations, such as enjoying life (hedonism), experiencing new things (stimulation), pursuing success (achievement), and maintaining customs (tradition), matter even in a health crisis. Public health authorities should recognize that such values are also rooted in basic human needs (Schwartz 1994), which individuals may place above health. Public health authorities should consider how health directives hinder pursuit of other values and attempt to address such tensions head on.
Fourth, values that maintained significant effects on behaviors alongside legitimacy and key contextual factors (e.g., perceived threat of the virus) provide insight into why people complied (or did not comply) with public health authorities during the pandemic that runs counter to some popular explanations. Values that maintain significance are security and conformity (positive) and stimulation and hedonism (negative). This pattern makes sense given the structure of value relations (see Figure 2) and the nature of the directives aimed at protecting health and upholding order during a crisis but necessarily restricting individuals’ ability to experience new things and engage in many activities that make life enjoyable.
By contrast, values along the self-transcendent versus self-enhancement dimension did not affect compliance when taking legitimacy and contextual factors into account. The lack of benevolence, universalism, achievement, and power effects is striking given that adherence to public health guidelines became “moralized” during the pandemic, with compliance cast as demonstrating altruistic concern for the welfare of others and noncompliance as indicating a selfish disregard for others (Bor et al. 2023). Similarly, popular narratives pitting the value of individual liberty against that of preventing harm to others (e.g., Authers 2021) may have been missing the point given that neither self-direction nor benevolence/universalism significantly shaped behaviors when controlling for legitimacy and other contextual factors.
Beyond the pandemic context, this study shows how examining a range of values can provide insight into the relationship between cultural and social authority for health authorities generally. Although the shared value of health boosts cultural authority and motivates adoption of health behaviors, other values may weaken or override the effect of health on behavior depending on the context. Individuals may perceive health authorities as high in cultural authority while still considering other values in determining behavior, complicating the cultural–social authority link. Furthermore, other voices may appeal to other values to justify their own authority and influence behavior in crisis situations. Cultural authority of health authorities then, even when high, may constitute only one among many factors influencing health behavior, especially when health directives affect aspects of life outside of health, as seen during the pandemic.
Despite these important findings, this study also has limitations. The intensity of state-level COVID-19 restrictions likely influenced the strength of propriety/value-behavior relationships. Because state restrictiveness varied throughout the pandemic (see McCann 2021), accounting for situational constraints poses a challenge because (to my knowledge) no longitudinal surveys tracking COVID behaviors also measured legitimacy and values. 6 Additionally, values likely varied in salience throughout the pandemic. Concerns for health and safety (security) may have strongly influenced behavior early on, whereas the effect of hedonism (desire to enjoy life) may have strengthened as the pandemic dragged on. Future work should ideally draw on longitudinal data measuring values, behaviors, and situational constraints over time.
Another limitation stems from the use of survey methods to capture behaviors. Although self-reports can be accurate (Miles 2015), individuals’ verbal accounts do not always align with their behavior, and surveys and interviews do not observe actual behavior, which is shaped by situational factors (Jerolmack and Khan 2014). Future work might employ ethnography to observe behavior in context. Although this quantitative study provides evidence for general patterns, qualitative work could further illuminate how people construe the impact of their perceptions and values on their actions. A sample limitation includes a lack of racial diversity. A more diverse sample may reveal variation in compliance by race (see Dovidio et al. 2008). Furthermore, value priorities may differ based on racial-ethnic group (as well as gender, age, and education; see Schwartz 2005), although relationships between the specific values and behavior would likely remain consistent.
Overall, this study reveals how the cultural authority of public health affected individuals’ compliance with COVID-19 prevention measures. This study also augments work on the social psychology of legitimacy and research in cultural sociology focused on the link between values and action (Miles 2015) by revealing the effect of values on behavior during a crisis. The importance of propriety (over and above the value of health and other factors) may be of particular interest given concerns about a crisis of expertise (Eyal 2019) and the potential decline in the cultural authority of medical and other health authorities (Heritage 2021; Stivers and Timmermans 2020). Although analyses do not capture whether perceptions of public health legitimacy changed during the pandemic, the strong effect of propriety on behavior suggests that whether increasing or decreasing, cultural authority continues to influence individuals’ decisions and health outcomes. Loss of legitimacy, therefore, might have significant consequences in the next health crisis. Future work should investigate antecedents to public health legitimacy, focusing on how public health authorities can gain legitimacy. Work in this area might benefit from examining interrelationships among components of cultural authority, such as the potential effects of values on legitimacy and the role of trust in health authorities as contributing to and/or stemming from cultural authority.
Footnotes
Appendix A
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported with a grant from the American Sociological Association Social Psychology Section Graduate Investigator Award and Emory University Laney Graduate School Professional Development Support Competitive Research Grant.