
Abstract
Professionals increasingly encounter tools aimed at rationalizing and standardizing their work. Existing research largely conceptualizes their responses to these tools on a continuum from professional resistance to managerial control. But the institutional logics perspective and emerging empirical evidence suggest more varied responses and diverse, possibly non-zero-sum, outcomes. Using survey data from 1,116 physicians in China’s public hospitals, we systematically examined physicians’ reactions to pathway implementation and the impacts on clinical autonomy and job satisfaction. Cluster analysis identified four response types: (a) ignoring, where physicians avoided pathways and maintained autonomy; (b) coerced, where imposed pathways reduced autonomy and satisfaction; (c) decoupling, where pathways were adopted superficially, preserving autonomy; and (d) embracing, where physicians actively participated in pathway implementation and enforcement, experiencing high satisfaction and autonomy. The findings help broaden the conceptualization of professionals’ reactions to rationalizing tools, uncover multiple pathways to clinical autonomy, and illustrate how professionals navigate institutional complexity in ever-evolving environments.
Control over a task area is a defining characteristic of a profession. A key aspect of this control is professionals’ abilities to take possession of their work process (Abbott 1987). In contemporary societies, as professionals increasingly work in large formal organizations and as powerful stakeholders, such as clients and payers, escalate their accountability demands, the control over professional work has become contested (Gorman and Sandefur 2011). Against this backdrop, stakeholders both within and outside of professions have rallied behind tools to standardize and rationalize professional work, although often with differing motivations (Adler and Kwon 2013; Armstrong 2002; Timmermans and Kolker 2004). In medicine, clinical guidelines and pathways are primary examples (Timmermans and Oh 2010). These tools have quickly proliferated during recent decades, often becoming key sites of contestation. It is therefore essential to understand professionals’ experiences with the growing presence of these tools: how they cope with the standardization and rationalization of their work, whether and how they retain their autonomy, and how these dynamics shape their overall work experience, thereby influencing their job fulfillment and satisfaction.
Conventional theoretical approaches typically interpret professionals’ responses to standardization and rationalization through the lens of conflicts between professionalism and bureaucracy. These two are seen as competing modes of organizing work: Professionalism emphasizes expertise, commitment, and autonomy of individual professionals, whereas bureaucracy relies on rules and hierarchical commands (Freidson 2001). In this vein, most empirical studies that examine professionals’ reactions to rationalizing tools were motivated by concerns for professional autonomy and largely focused on how professionals circumvented or resisted these tools (Timmermans and Kolker 2004).
Over recent decades, the institutional logics perspective, primarily developed within organizational studies, has become an influential contender for understanding how diverse social forces shape organizational structures and the work within organizations (Lounsbury et al. 2021; Thornton, Ocasio, and Lounsbury 2012). Scholars of professions have started to apply this perspective to characterize how multiple stakeholders interact in complex ways to configure professional work (Alvehus 2018; Goodrick and Reay 2011; Noordegraaf 2015). It has been argued that as an institutional logic, professionalism may coexist or collaborate with other institutional logics, such as those of the bureaucracy, market, and state, in addition to competing with them (Goodrick and Reay 2011; Reay and Hinings 2009).
This emerging approach holds promise for broadening our understanding of professionals’ responses to rationalization and standardization and the implications of such responses for work autonomy and broader work experience. It suggests that professionals’ coping strategies can potentially be diverse and complex rather than necessarily a zero-sum battle between professionals and their organizations (Reay et al. 2017). Indeed, a few ethnographic studies have found cases where professionals deployed a wider range of strategies than conventionally thought. Beyond rejecting or resisting rationalizing tools, they may adapt, co-opt, or make productive use of them (Allen 2014; Martin et al. 2013, 2015; Wilhelm, Bullinger, and Chromik 2020). These empirical observations are compatible with the implications of the institutional logics perspective and offer a valuable, nuanced understanding of professionals’ experiences. However, systematic and comparative assessments of the diverse patterns of professionals’ responses and their impacts on work autonomy are limited. Key questions remain: What are the major types of professionals’ responses to rationalization and standardization? How prevalent are these responses? How do they influence professionals’ work autonomy and job satisfaction?
In this study, we investigate these questions by leveraging the recent large-scale implementation of clinical pathways, a standardized protocol that provides step-by-step guidance to diagnose and manage specific diseases, in China’s public hospitals (He and Yang 2015). A survey of 1,116 physicians from 23 public hospitals in four cities in China was conducted. We applied cluster analysis, a data-driven approach, to empirically classify physicians’ responses to clinical pathways and then assessed their effects on clinical autonomy and job satisfaction. Our analysis revealed four major response types, which we named “ignoring,” “coerced,” “decoupling,” and “embracing.” The ignorers disregarded the pathways, and their clinical autonomy was unaffected, which suggests professional control. The coerced had clinical pathways imposed on them and reported the lowest autonomy and satisfaction, which indicates managerial dominance in their work. Notably, two response types went beyond the zero-sum struggle between professionalism and managerialism. The decouplers actively engaged in pathway implementation but sidestepped effective enforcement, making the pathways more of a formality than a real constraint on their practice. By contrast, the embracers actively participated in pathway design and helped install strict enforcement, suggesting that the pathways had a real impact. Yet they reported high autonomy, similar to the ignorers and decouplers, and the greatest job satisfaction among all groups. The pathways appeared to have enhanced the embracers’ work experiences without diminishing their autonomy.
By identifying major types in professionals’ responses and revealing multiple pathways to autonomy, this study answers calls to go beyond the single-dimensional approach to conceptualizing professionals’ relationships to rationalization and standardization (Noordegraaf 2015; Numerato, Salvatore, and Fattore 2012). It sheds light on how professional workers can maintain their autonomy and interact with work environments increasingly shaped by formal organizations and external demands for transparency and accountability.
Background
Multiple Institutional Logics and Professionals’ Responses to Rationalizing Tools
Control over the work process is central to maintaining professional jurisdiction and authority (Abbott 1987). In recent decades, this control has faced growing pressure due to rising consumerism, the increasing integration of professionals into bureaucratic organizations, and the expanding role of the state as both regulator and payer (Armstrong 2002; Timmermans and Oh 2010). Within this shifting landscape, various stakeholders have turned to rationalizing and standardizing tools, such as protocols, guidelines, and pathways, that seek to codify and structure core professional tasks. For external actors, such as payers and clients, these tools promise cost containment and quality assurance. For professionals, they are often problematic because they are readily appropriated for managerial purposes as technologies of surveillance and control, raising concerns about reduced discretion and autonomy (Numerato et al. 2012; Timmermans and Epstein 2010). At the same time, some professionals recognize potential benefits, such as enhancing the legitimacy of professional control, bringing practice closer to scientific ideals, and buffering more invasive oversight (Armstrong 2002; Timmermans and Kolker 2004). Professionals’ responses to rationalizing tools and the broader implications for professional autonomy and work experience have become the subject of ongoing debates.
Sociological theories of professions have been largely concerned with explicating and adjudicating the dominance and privileges of professions. Influential theoretical perspectives, such as professional dominance, proletarianization of professions, and countervailing powers, regarded professionalism as competing with other models of organizing work (Gorman and Sandefur 2011; Timmermans and Kolker 2004). Along this line, discussions of professionals’ responses to rationalizing tools have often focused on potential conflicts between bureaucracies and professions. The professional model emphasizes autonomous workers applying technical expertise, whereas the bureaucratic model prioritizes hierarchical control and formal rules (Freidson 2001). Professionals in bureaucratic organizations are often seen as vulnerable to organizational encroachment, with their work at least partially subjected to hierarchical control (Epstein 2014; Ritzer and Walczak 1988). On the other hand, it has been argued that even when professionals cannot fully control the terms and context of their work, their exclusive technical expertise protects the substantive content of their work from external intrusion (Abbott 1987). From the conflict perspective, professionals can either successfully resist these tools and retain their control or are dominated by the bureaucratic organization.
Rationalizing tools have grown especially quickly in medicine. Since the early 1980s, many Western countries have witnessed a movement toward standardizing clinical practice (Timmermans and Kolker 2004). This movement, known as “evidence-based medicine,” is centered on clinical practice guidelines that summarize scientific findings on specific diseases or treatments and offer step-by-step guidance. Clinical pathways are developed on the basis of practice guidelines: A pathway incorporates several guidelines and outlines the process for managing a given disease; it also specifies the roles of different health care professionals (Martin et al. 2017). For example, a pathway on the initiation of hemodialysis for end-stage renal disease, issued by the National Health Commission 1 of China, specifies diagnostic criteria, treatment options and goals, intervention steps, and possible complications. It assigns tasks to different professionals (e.g., nephrologists, nurses, dietitians) at each stage of care, offering detailed and standardized guidance (National Health Commission 2020).
Implicitly informed by the conflict view between professionalism and bureaucracy, most empirical research on such rationalizing measures was concerned that they may constrain clinical autonomy and lead to “cookbook medicine.” The findings tended to focus on how physicians resisted and undermined these measures by questioning their applicability in complex and uncertain clinical situations, discrediting their scientific basis, and highlighting the ulterior motives for their implementation (e.g., they serve cost control more than quality improvement; Timmermans and Oh 2010).
In this article, we approach this issue by drawing on the insights provided by the institutional logics perspective, developed in the field of organizational studies since the early 1990s (Friedland and Alford 1991; Lounsbury et al. 2021; Thornton et al. 2012). Institutional logics refer to “the socially constructed, historical patterns of cultural symbols and material practices, including assumptions, values, and beliefs, by which individuals and organizations provide meaning to their daily activity, organize time and space, and reproduce their lives and experience” (Thornton et al. 2012:2). From this perspective, professionalism is conceptualized as a societal-level institutional logic that shapes behavior alongside other logics, such as the bureaucracy, the market, and the state (Currie et al. 2012; Thornton et al. 2012). In the ideal-typical logic of professionalism, professionals draw on specialized, abstract knowledge to carry out their work independently or collaboratively with their peers, maintaining control over their work area. By contrast, the bureaucratic or managerial logic structures work through rational rules, standardized routines, and hierarchical oversight by managerial authority (Goodrick and Reay 2011; Olakivi and Niska 2017; Tuohy 1999). The market logic centers around consumer preferences and the competition for profit among producers, whereas the state logic emphasizes the central role of government in regulating and organizing work activities (Goodrick and Reay 2011).
Early empirical work in this tradition focused on the conflicts among different logics and how dominant logics shifted over time (Lounsbury et al. 2021; Thornton and Ocasio 1999). Later research came to highlight the idea of institutional complexity. That is, multiple logics may coexist and interact in complex and context-dependent ways; in addition to being antagonistic, their interplay can also take cooperative, non-zero-sum forms (Ocasio, Thornton, and Lounsbury 2017). Most empirical studies tended to assess the consequences of institutional complexity at the field and organizational levels (Ocasio et al. 2017). For example, Goodrick and Reay (2011) traced the evolution of U.S. pharmacy through the dynamic interactions among multiple logics, showing that one logic may dominate, support, or simply coexist with others, depending on the historical context.
Building on this foundation, recent scholarship has begun to emphasize the agentic possibilities that institutional complexity affords (Reay et al. 2017; Skelcher and Smith 2015). Although logics are collectively understood and offer “guideposts for action” (Ocasio et al., 2017:524), they are not deterministic; rather, they allow for local adaptation, individual interpretation, and multiple forms of enactment (Kirby 2021; Ocasio et al. 2017; Streeck and Thelen 2005; Tuohy 2023). Moreover, the copresence of multiple institutional logics in actors’ environments provides different sets of resources and constraints, potentially enriching actors’ repertoire (Ocasio et al. 2017; Reay et al. 2017). This agentic turn has given rise to a growing body of empirical work on how professionals navigate competing institutional demands to construct meanings and identities (e.g., Martin et al. 2021; Reay et al. 2017), manage emotions (e.g., Vedi, Korczynski, and Bishop 2025), and maintain collaborations (e.g., Gøtzsche-Astrup et al. 2023). Although the perspective has yet to be systematically applied to the study of professionals’ engagement with rationalizing tools, it opens promising avenues for thinking about this issue. Instead of seeing a tug-of-war between professionalism and managerialism, it suggests that professionals may employ a broader array of strategies. Besides resistance or capitulation, they may “borrow” or “hijack” elements across different logics; use “separating,” “interweaving,” or other tactics; and develop a variety of relationships with rationalizing measures. The patterns of responses and the outcomes may well transcend a zero-sum game between professional autonomy and managerial control.
Indeed, findings from a small body of qualitative research, although not explicitly grounded in the institutional logics perspective, resonate with this notion of diverse responses. These studies examined how professionals interacted with various rationalizing measures, such as checklists, guidelines, pathways, and reporting systems. They found that in some contexts, professionals successfully circumvented these measures (Allen 2014; Waring and Currie 2009), whereas in others, they were constrained by them (Martin et al. 2015). In certain cases, they selectively adopted elements of these measures, especially when minimal changes to practice were required (Martin et al. 2015; Waring and Currie 2009). Notably, in a few cases, professionals were effectively involved in decision-making processes, and the measures achieved some desirable outcomes, such as facilitating knowledge transfer and challenging entrenched hierarchies (Levay and Waks 2009; Martin et al. 2013, 2017; Wilhelm et al. 2020). Terms such as “organizational professionalism” and “hybrid professionalism” were coined to describe professional practices that integrate elements of managerialism (Evetts 2016; Noordegraaf 2015). Although these concepts highlight the evolving nature of professional work, considerable ambivalence remains about the implications of such integration. Some viewed the relationship as synergic, such that a “new professionalism” emerges to adapt to a changed social environment. Some, however, cautioned that as more elements of surveillance and control are incorporated into professional work, professionalism may “lose its soul” (Evetts 2011; Martin et al. 2015).
This ambivalence reflects important empirical and theoretical gaps in our understanding of professionals’ autonomy and work experiences in the context of increasing rationalization and standardization. Empirically, although previous case studies provided rich details and nuanced insights, it remained unclear whether the varied patterns of responses observed, particularly those involving constructive or positive engagement, represented typical reactions or rare and isolated instances. A related question concerns the prevalence of different types of responses, which remains largely unexplored. Moreover, most qualitative studies are not designed to systematically compare professionals’ sense of autonomy and satisfaction across response types. Consequently, we have a limited understanding of how responses to rationalization influence autonomy and broader work experiences. Scholars have underscored the need for more quantitative and comparative research to provide robust evidence and complement qualitative findings (Martin et al. 2017; Noordegraaf 2016; Numerato et al. 2012).
Theoretically, how professionals cope with rationalization and standardization continues to be largely conceptualized within a single-dimensional “hegemony/resistance framework” (Numerato et al. 2012:637), albeit with finer gradation and more in-between categories (Numerato et al. 2012; Waring and Currie 2009). A comprehensive review found that in existing studies, professionals’ responses can be thought of as falling into categories such as managerial hegemony, co-optation, negotiation, adaptation, and professional resistance. These categories remain positioned on a single-dimensional continuum from bureaucratic dominance on one end to professional control on the other, with the intermediate categories representing varying degrees of trade-offs between the two (Numerato et al. 2012). This linear framing, however, does not adequately capture the plurality of dynamics of professionals’ engagement with rationalizing tools. As the institutional logics perspective suggests, when multiple logics coexist, they can offer rich sets of resources and ample space for agents to formulate their responses—collaborative and antagonistic strategies may both emerge. Scholars have called for moving beyond the single-dimensional scheme (Noordegraaf 2015; Numerato et al. 2012).
Nevertheless, the institutional logics framework has yet to fully systematize how actors combine or navigate multiple logics in practice (Lounsbury et al. 2021; Ocasio et al. 2017) and as it stands, does not offer strong predictive claims about how professionals’ responses will unfold. Therefore, an inductive and ground-up approach would be especially productive at this point. In this article, we employ cluster analysis, a data-driven method that identifies empirical patterns from complex and multidimensional data without a priori assumptions, to classify physicians’ reactions and uncover potential heterogeneity. We apply this method to a large-scale survey of Chinese physicians to inductively develop a typology of physicians’ responses to the implementation of clinical pathways. We then link the response types to physicians’ clinical autonomy and job satisfaction. We begin with an overview of the Chinese medical profession and the rollout of clinical pathways in China.
Clinical Pathways in China’s Public Hospitals
In 2009, the Chinese government laid out plans to reform public hospitals, and a key element is to implement clinical pathways (Cheng 2013). Public hospitals, which deliver most of the care in China, faced serious challenges, such as suboptimal care quality and resource misuse (Jin and Ye 2021). Echoing trends in many Western societies, clinical pathways were expected to help rein in health care costs and improve quality of care. Pathways were also linked to payment reforms that introduced reimbursement based on disease groups, creating financial incentives for adoption (Cheng 2013; Jin 2017). To support implementation, the National Health Commission compiled manuals and guidelines and used the coverage of pathways as criteria in assessing hospital performance (Guo, Han, and Dong 2018). Hospitals responded by setting up committees and appointing staff to oversee pathway implementation (He and Yang 2015). By 2017, clinical pathways became widespread in China’s public hospitals (Guo et al. 2018).
Chinese physicians, like their Western counterparts, practice in an environment shaped by the interplay of multiple institutional logics, in particular, those of professionalism, bureaucracy, and the market. The logic of professionalism is prominent: Physicians undergo standardized training and are granted exclusive licensure by the state to provide medical care. Clinical expertise and ethical commitment are central to doctors’ professional identity (Hu et al. 2014). At the same time, the bureaucratic logic is influential. Doctors in China’s public hospitals are salaried employees, relying on their clinical departments and hospitals for income and career advancement opportunities (Jin and Ye 2021). Public hospitals themselves also embody institutional complexity. Although highly bureaucratic, they are typically led by senior physicians in key administrative roles (Mei and Kirkpatrick 2019). In addition, the market logic is firmly entrenched in hospital operations. With limited direct government funding, public hospitals in China face strong financial pressure to generate revenue, which incentivizes profit-seeking behavior at both the organizational and individual levels (Jin and Ye 2021). As a result, Chinese physicians must continuously navigate the interplay of multiple institutional logics in their practice.
Previous research has indicated structural differences between Chinese physicians and their Western counterparts. In China, physicians are deeply embedded within the bureaucratic structures of public hospitals and operate under the oversight of a strong and centralized state (Jin and Ye 2021; Yao 2019). Despite the differences, we argue that our study holds broader relevance. First, China’s situation may serve as a conservative case for observing the plurality of professional responses to rationalization, one in which organizational and state influence is especially pronounced, imposing strong constraints. Moreover, physicians in many Western countries have been increasingly incorporated into complex organizations (Lin 2014). Our findings can therefore be a point of reference for future research on physicians in those settings.
The large-scale implementation of clinical pathways in China offers a lens to observe the varied patterns in how physicians cope with rationalizing tools when faced with institutional complexity. Existing studies on clinical pathways in China have primarily focused on assessing their impacts on patient care and costs (e.g., Cheng 2013; Zhao et al. 2016). Little research has taken a theoretically motivated and comparative approach to assessing physicians’ responses and experiences.
Physicians’ Responses to Clinical Pathways and Their Autonomy and Satisfaction
In this article, we aim to develop a typology of professionals’ responses to rationalizing tools. Motivated by the institutional logics perspective, we ask whether physicians exhibited diverse patterns of responses to clinical pathways. We apply cluster analysis to survey data of Chinese physicians to inductively classify physicians’ reactions. We seek to empirically uncover the major types of physicians’ strategies without imposing a priori assumptions of antagonism between professionalism and managerialism.
We then assess how physicians’ responses to clinical pathways are linked to their clinical autonomy and job satisfaction. The conflict view suggests that physicians’ autonomy and satisfaction correlate positively with their ability to reject these tools: Those who successfully resist such tools are expected to experience the highest levels of autonomy and satisfaction, whereas those compelled to adopt them would experience the lowest. Physicians positioned between these extremes would exhibit intermediate levels of autonomy and satisfaction. By contrast, the institutional logics perspective acknowledges the possibility that there may be multiple paths through which physicians retain their autonomy. Moreover, physicians’ satisfaction may not correlate linearly with how much they distance themselves from the pathways. Those who productively engage with pathways may also be highly satisfied.
Data and Methods
Data
This study drew on survey data from 1,159 physicians across 23 hospitals in four major Chinese cities. Conducted between April 2018 and April 2019, the survey focused on physicians’ experiences with and attitudes toward clinical pathway implementation. The cities, two megacities and two provincial capitals, were selected for their geographic diversity (north, southeast, and central China) and their status as national or regional medical hubs. In each city, four tertiary and two secondary hospitals were targeted because pathways were initially promoted in tertiary hospitals before expanding to secondary ones. Except in one city, where one secondary hospital did not cooperate with the data collection, six hospitals were surveyed per city. In each hospital, we chose 10 specialties that were included in the government-sponsored pilot programs for implementing pathways (see Appendix A in the online version of the article). On the days of data collection, five to six physicians were surveyed per specialty in tertiary hospitals and four to five in secondary hospitals. Forty-three respondents were excluded due to missing data on key items, yielding a final analytical sample of 1,116 physicians.
Variables
Physicians’ responses to clinical pathways
We assessed physicians’ experiences in the entire process of pathway implementation. First, the respondents reported their involvement in four steps of designing pathway implementation: choosing the disease, drafting or modifying the pathway, creating the noncompliance form, and establishing evaluation and sanction measures. Response options included a lot, some, none, and did not want to be involved. A lot of and some involvement were counted as being involved, and a variable was constructed to indicate the number of steps involved (ranging from zero to four). For the robustness of cluster analysis, as explained later, the variable is dichotomized to indicate whether the respondents participated in three or more steps.
Next, physicians were asked if their hospital or department solicited feedback during pathway rollout, if they provided input regardless whether feedback was solicited, and if changes followed. Three dummy variables were constructed: feedback was solicited, input was given and modifications were made, and input was provided, but no modifications were made.
Finally, we assessed how pathway adherence was monitored and sanctioned. Hospitals and departments may monitor pathways using process measures (e.g., completion of forms, regular review meetings), compliance levels (e.g., patient coverage, completion rates, deviations from specified treatments), and patient outcomes (e.g., costs, length of stay, adverse events). Respondents reported which criteria were applied, yielding a variable indicating the number of criteria (ranging from zero to eight). In cluster analysis, this variable was dichotomized to reflect six or more criteria. Financial incentives and public profiling are common motivational strategies. The former was measured by whether 5% or more of a physician’s income was tied to pathway compliance and the latter by whether physicians’ compliance statistics were publicized and compared. Moreover, patients may receive informational materials about pathways, implying that they could monitor adherence. A dummy variable indicated whether such materials (patient pathways) were introduced.
Clinical autonomy, job satisfaction, and perceived outcomes of pathway implementation
Perceived clinical autonomy was measured by physicians’ agreement with the statement that they could control the diagnosis and treatment of their patients, using a 4-point scale from strongly disagree (1) to strongly agree (4). Job satisfaction was measured by asking how satisfied physicians were with their jobs, using a 5-point scale from very dissatisfied (1) to very satisfied (5).
We examined physicians’ replies to three survey questions about the perceived outcomes of pathway implementation to help shed further light on physicians’ responses to pathways. Physicians rated their agreement with the following statements: (1) “In my department, the use of clinical pathways was often merely a formality”; (2) “In my department, most people strictly followed and complied with the clinical pathways that have been introduced”; and (3) “The clinical pathways implemented in my department took into account the practical reality of our work.” All were measured on a 4-point scale, with higher scores indicating more agreement.
Control variables
When we assessed how physicians’ response types related to their clinical autonomy and job satisfaction, we controlled for both individual and hospital characteristics that previous studies have shown to influence such outcomes (Lin 2014; Zhang et al. 2009). Individual characteristics included gender, seniority (≤5, 6–10, 11–15, and >15 years), professional ranks (junior, middle-level, deputy chief, and chief), levels of education (bachelor’s, master’s, and doctoral), income (≤¥5,000, ¥5,001–¥10,000, ¥10,001–¥20,000, and ≥¥20,000), and specialty (surgical vs. nonsurgical). Hospital features included size (number of beds) and hospital rank (elite, tertiary and secondary). 2 City-level dummy variables were also included to capture differences in regional health care systems, administrative cultures, and policy environments.
Analytical method
Our analysis proceeded in two stages. First, we performed cluster analysis on the eight variables describing physicians’ involvement and experiences during clinical pathway implementation, aiming to identify distinct experience types. Because cluster analysis is sensitive to variable scales, we followed common practice and dichotomized all nonbinary variables by coding the values above the median as 1 and those below as 0 (Garip 2012). Cluster analysis consists of three steps: choosing a clustering algorithm, selecting a similarity measure, and determining the optimum number of clusters. We used the K-means algorithm, a classical clustering algorithm that minimizes within-cluster variance. For the similarity measure, we employed a measure known as the “city-block distance,” which evaluated similarity based on the number of shared attributes in physicians’ implementation experiences (Garip 2012; Waggoner 2020). Finally, we identified the optimal number of clusters using three validation measures alongside substantive interpretation of the clusters. As detailed in Appendix B in the online version of the article, the three measures corroborate with one another and are also consistent with the substantive interpretation, which led us to identify four clusters. The analysis was conducted in Matlab.
In the second stage, to examine the link between physicians’ responses to clinical pathways and their subjective experiences, we regressed perceived clinical autonomy and job satisfaction on the four identified clusters, controlling for individual physician and hospital characteristics. Because clinical pathways are implemented primarily at the department level and hospital-level policies are typically interpreted within departments, we applied multilevel linear regression models with the clinical department as the grouping variable. To check for the robustness, we also ran multilevel ordinal logistic regressions, treating autonomy and satisfaction as ordinal variables. These models yielded qualitatively similar results. For simplicity and ease of interpretation, we presented the results from the linear models. Results from the ordinal models are available on request.
Results
Select Sample Characteristics
Table 1 displays respondent characteristics and the features of their hospitals. Around 40% were women, and 39% practiced in surgical departments. Physicians with 5 or fewer years, 6 to 10 years, 11 to 15 years, and 16 or more years of experience made up 26%, 31%, 21%, and 21% of the sample, respectively. Regarding education, 26% held college degrees, 41% held master’s degrees, and 33% held doctoral degrees. Professional ranks were distributed as follows: junior (30%), middle-level (39%), deputy chief (24%), and chief physicians (6%). About 42% worked in elite tertiary hospitals, 33% worked in regular tertiary hospitals, and 25% worked in secondary hospitals.
Descriptive Statistics (N = 1,116).
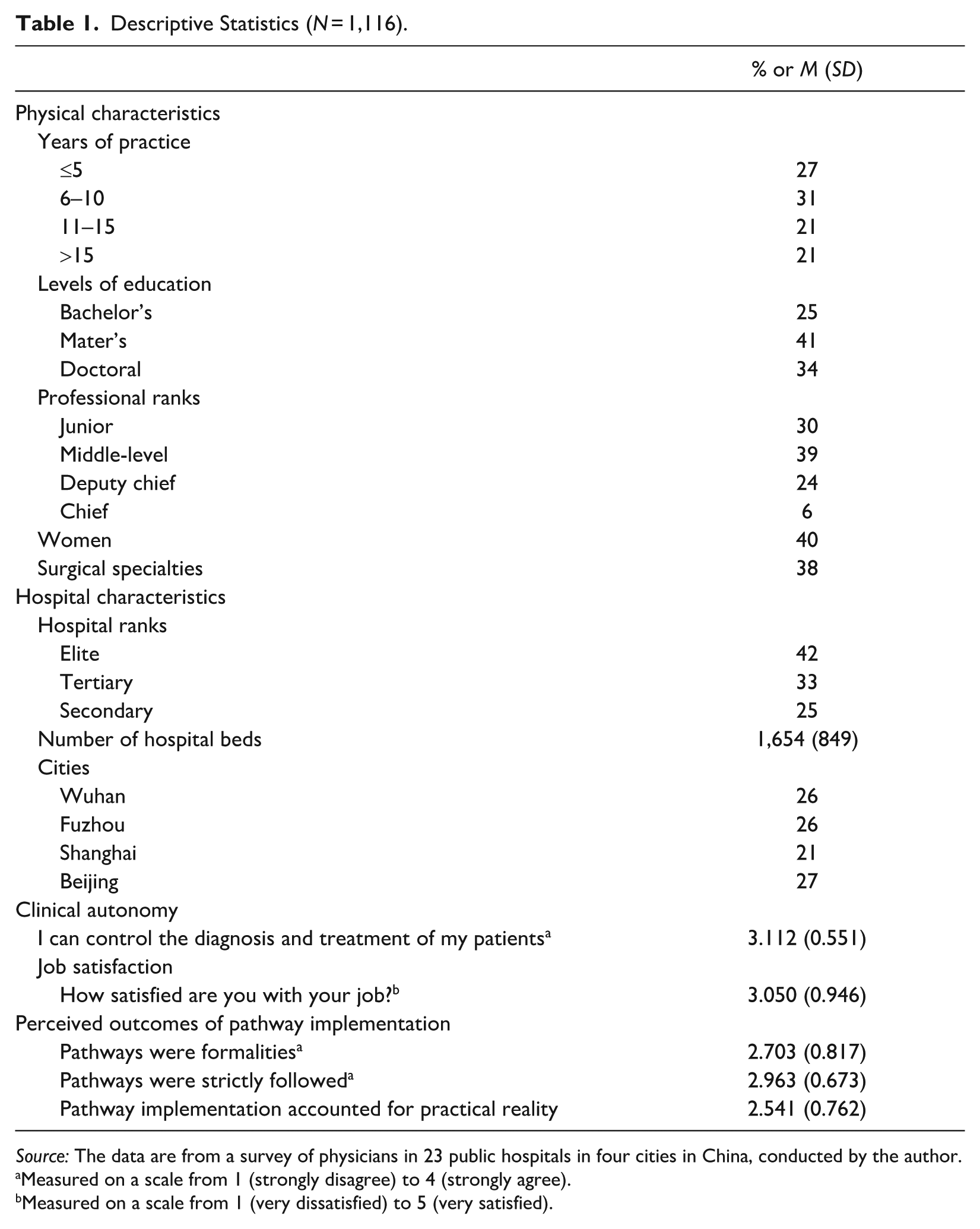
Source: The data are from a survey of physicians in 23 public hospitals in four cities in China, conducted by the author.
Measured on a scale from 1 (strongly disagree) to 4 (strongly agree).
Measured on a scale from 1 (very dissatisfied) to 5 (very satisfied).
Developing a Typology of Physicians’ Responses to Clinical Pathways
Descriptive statistics of variables about the implementation process
The first column of Table 2 presents the descriptive statistics on physician involvement in pathway implementation and the monitoring practices. Around 49% of physicians were involved in three or more steps of pathway implementation (out of four). Approximately 70% reported that their hospitals/departments sought their feedback on clinical pathways. Regardless of whether their feedback was solicited, 56% provided their input. Of these, 77% reported that changes were made, and 23% said that no changes were made. Regarding monitoring and incentives, 43% of physicians reported encountering six or more evaluation criteria (out of eight), and 46% indicated that simplified pathways were provided to patients. Moreover, 43% had five percent or more of their income linked to pathway adherence, and 24% reported that adherence statistics were publicly shared within their organizations.
Physicians’ Experience of Pathway Implementation.
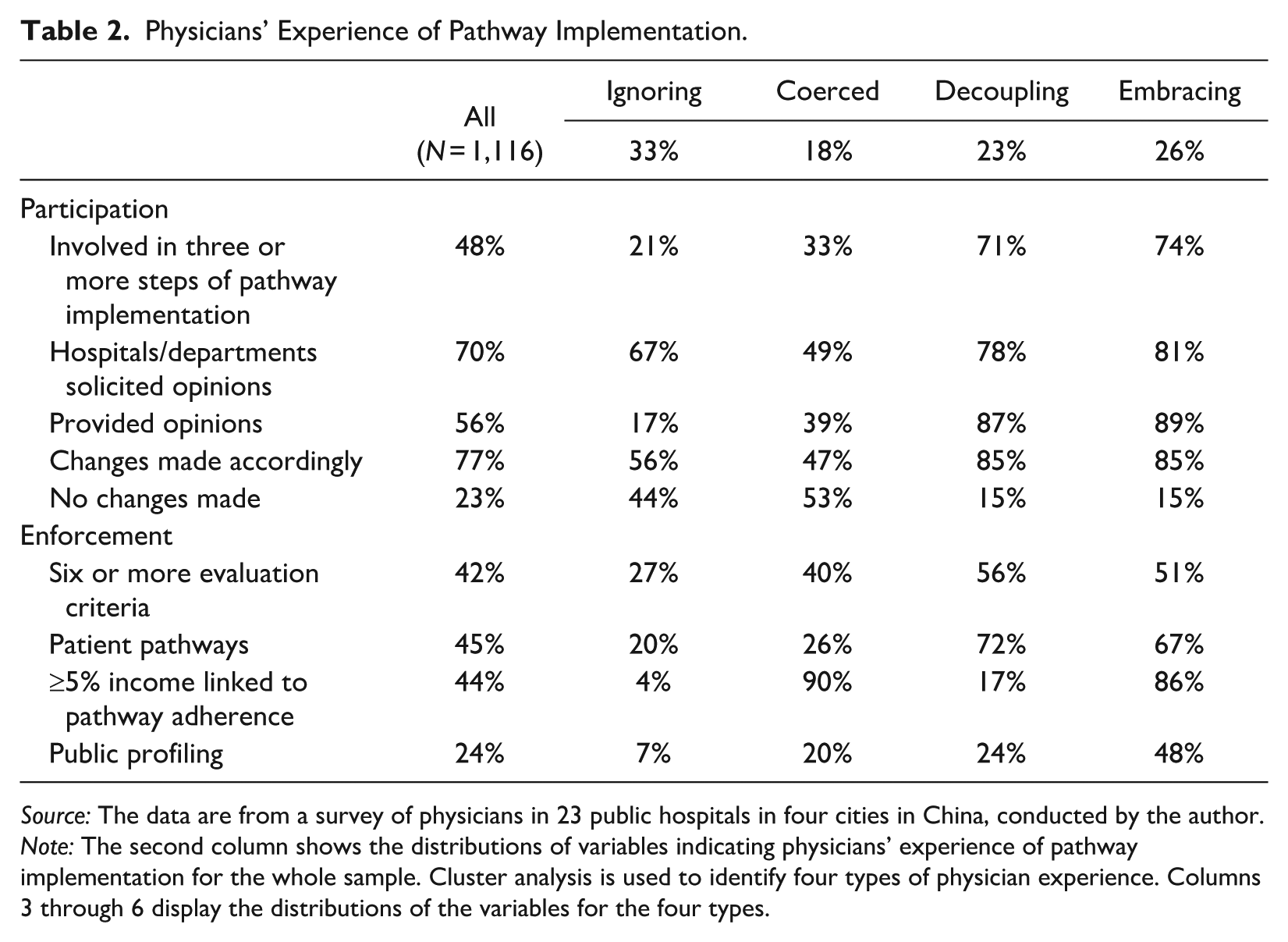
Source: The data are from a survey of physicians in 23 public hospitals in four cities in China, conducted by the author.
Note: The second column shows the distributions of variables indicating physicians’ experience of pathway implementation for the whole sample. Cluster analysis is used to identify four types of physician experience. Columns 3 through 6 display the distributions of the variables for the four types.
Physicians’ response types
Cluster analysis identified four distinct response types, which we term “ignoring,” “coerced,” “decoupling,” and “embracing.” In the following, we outline the characteristics of the four clusters and discuss the reasons for and meaning of the labeling. Columns 3 to 6 in Table 2 present the statistics of the four types of physicians’ experiences in pathway implementation.
Physicians in the first cluster (column 3 in Table 2) were largely able to keep their distances from clinical pathways. Only 21% were involved in three or more implementation steps. Although 67% were asked for input, most (83%) did not respond. Of the 17% who did, 56% said changes were made based on their feedback. The level of monitoring in this group was well below the sample averages: 27% encountered six or more evaluation criteria, and 20% indicated that simplified pathways were provided to patients. Only 4% had five percent or more of their income tied to pathway adherence, and 7% experienced public profiling. With minimal involvement and weak enforcement, these physicians effectively ignored the pathways, hence the label “ignoring.”
Physicians in the second cluster (column 4 in Table 2) were somewhat more involved in pathway implementation than those in the ignoring cluster: 33% participated in three or more implementation steps, and 39% provided feedback, higher than the ignorers’ respective 21% and 17%. But their organizations were less responsive; only 49% were asked for input (vs. 67% among the ignorers), and of those who gave feedback, just 47% saw changes made. In terms of enforcement measures, this group faced strong financial incentives: 90% reported that five percent or more of their income was tied to pathway adherence, the highest among all clusters. Other monitoring measures, such as encountering six or more evaluation criteria or using patient pathways, were more common than among ignorers but not the highest overall. Because financial incentives directly affect physicians’ economic well-being and have been found to be highly effective, they clearly signaled stringent enforcement (Martin et al. 2017). For this cluster of physicians, their organizations were the least responsive, and they experienced the most stringent financial sanctioning. Therefore, we term this group “coerced.”
Clusters 3 and 4 showed similarly high levels of engagement in the clinical pathway implementation (columns 5 and 6 in Table 2). Around 75% of physicians in cluster 3 and 71% in cluster 4 participated in three or more steps. Their organizations were receptive: 81% in cluster 3 and 78% in cluster 4 were asked for feedback. A high percentage of physicians in both clusters offered their opinions (89% in cluster 3 and 87% in cluster 4), and in both clusters, 85% of those who offered suggestions said that changes were made, demonstrating strong organizational responsiveness.
On the other hand, enforcement was substantially higher in cluster 4, especially regarding financial incentives and public profiling: 86% had five percent or more of their income tied to pathway adherence, compared to only 17% in cluster 3; 48% reported public profiling versus 24% in cluster 3. Other monitoring measures were similar across the two clusters. As discussed previously, financial incentives were a strong indicator of strict enforcement. Public profiling fosters social comparison and competition, and previous research has shown that it was also an effective enforcement measure (Martin et al. 2017). Thus, enforcement was clearly more rigorous in cluster 4. It is worth noting that given their active engagement and organizational responsiveness, physicians in both clusters likely played a key role in shaping enforcement practices. These mechanisms may have emerged through negotiation or even physician initiative rather than being imposed top-down.
The results thus far suggest that although both clusters were highly engaged in pathway design and rollout, enforcement was considerably stronger in cluster 4. To further understand whether pathways were used differently across the two clusters, we compared responses to two survey items. The first assessed agreement with “In my clinical department, pathways were just a formality” and the second with “People in my department strictly followed and complied with the pathways.” Cluster 3 physicians were more likely to view pathways as just a formality (mean score: 2.581 vs. 2.451; p = .063) and were less likely to report strict adherence (mean score: 2.927 vs. 3.035; p = .065) compared with those in cluster 4.
These findings suggest that cluster 3 physicians tended to perceive pathways as more of a ceremonial exercise than an actual constraint on their work behavior. This aligns with the concept of decoupling, where formal procedures are adopted for legitimacy concerns, but with weak enforcement, they do little to affect workers’ actual practice in the technological core (Meyer and Rowan 1977). We therefore name cluster 3 “decoupling.” By contrast, for cluster 4, active engagement with pathway implementation was paired with effective enforcement. With meaningful incentives and consequences, the pathways may be substantively integrated into physicians’ practice. Because cluster 4 physicians took an active part in pathway design and implementation, likely also in shaping these enforcement mechanisms, we term this cluster “embracing.”
To summarize, our analysis revealed four clusters of physicians, each representing a distinct response to clinical pathway implementation: (1) ignoring—physicians maintained a distance from pathways, with minimal involvement and little monitoring, allowing them to deflect the pathways in practice; (2) coerced—physicians experienced pathway implementation as imposed, with limited responsiveness from their organizations but significant financial penalties tied to adherence; (3) decoupling—physicians engaged extensively in the implementation process, but weak enforcement rendered pathways largely ceremonial; and (4) embracing—physicians helped design and implement pathways with effective sanctions, indicating a high degree of pathway integration in practice.
Physicians’ response types and their clinical autonomy and job satisfaction
We then examined how the four types of responses to clinical pathways are linked to physicians’ clinical autonomy and job satisfaction. Table 1 presents the descriptive statistics of the two measures. Table 3 presents the coefficients for the response types from multilevel linear regressions. For results for the control variables, see Appendix C in the online version of the article.
Physicians’ Responses to Clinical Pathways and Their Clinical Autonomy and Job Satisfaction.
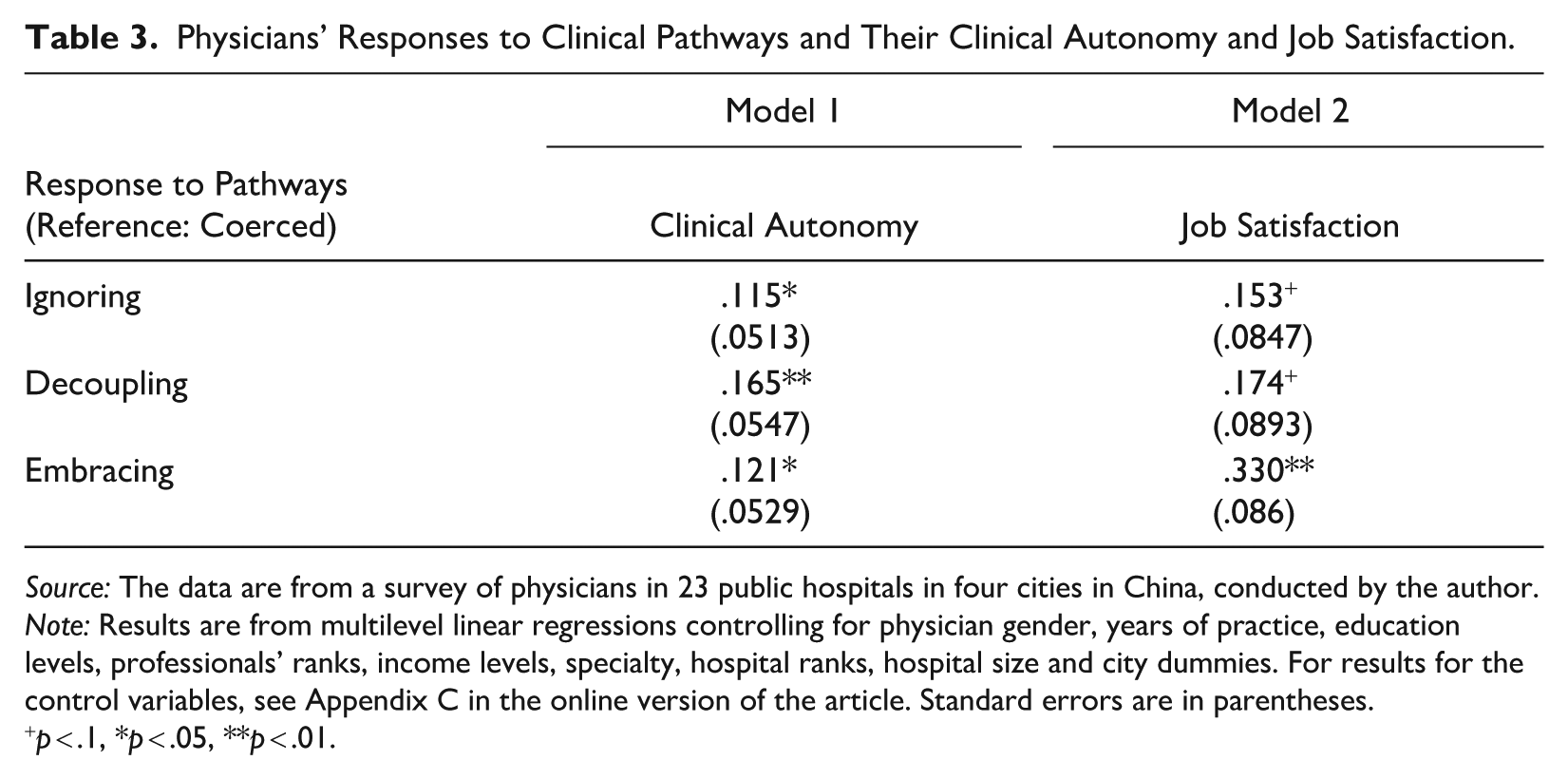
Source: The data are from a survey of physicians in 23 public hospitals in four cities in China, conducted by the author.
Note: Results are from multilevel linear regressions controlling for physician gender, years of practice, education levels, professionals’ ranks, income levels, specialty, hospital ranks, hospital size and city dummies. For results for the control variables, see Appendix C in the online version of the article. Standard errors are in parentheses.
p < .1, *p < .05, **p < .01.
Model 1 in Table 3 shows the differences in perceived clinical autonomy across the four groups. Compared with the coerced, the ignorers (β = .115, p = .024), decouplers (β = .165, p = .003), and embracers (β = .121, p = .023) all perceived significantly greater clinical autonomy. The coerced reported the lowest autonomy, suggesting that when forced on physicians, pathways may curb autonomy.
Further analysis shows that there were no significant differences in autonomy among the ignorers, decouplers, and embracers (ignorers vs. decouplers: β = .049, p = .332; ignorers vs. embracers: β = −.005, p = .918; decouplers vs. embracers: β = .044, p = .353). This suggests that physicians can maintain their autonomy through more than one route, challenging the zero-sum view that the more physicians can banish pathways, the better they are able to maintain their autonomy. The ignorers, who disengaged from clinical pathways, enjoyed greater autonomy than the coerced. But the decouplers and embracers, although both highly engaged with pathway implementation, retained similarly high autonomy via different strategies. The decouplers insulated their practice from pathway influence by dissociating formal procedures from actual behavior. The embracers, operating under rigorous enforcement, likely maintained autonomy by helping design flexible pathways suited to their clinical needs and local conditions. To examine this possibility, we compare responses to a survey item on whether pathways accounted for physicians’ actual work conditions; the embracers reported higher agreement than all other groups (mean scores: embracers vs. the coerced: 2.775 vs. 2.505, p < .001; embracers vs. ignorers: 2.775 vs. 2.328, p < .001; embracers vs. decouplers: 2.775 vs. 2.641, p = .032). This match between pathway design and practical reality likely contributed to the embracers’ high perceived autonomy.
Model 2 investigates the relationship between the physicians’ response types and their job satisfaction. Compared with the coerced, the ignorers (β = .153, p = .071) and decouplers (β = .174, p = .051) reported greater job satisfaction, and the differences are marginally statistically significant. The embracers reported significantly greater job satisfaction than the coerced (β = .330, p < .001). Further analysis shows that the ignorers and decouplers were similarly satisfied (β = −.021, p = .800), whereas the embracers were more satisfied than both the ignorers (β = .177, p = .032) and decouplers (β = .156, p = .045). Thus, the embracers reported the highest satisfaction, the coerced the lowest, with the ignorers and decouplers in the middle.
The low job satisfaction among the coerced is unsurprising given that clinical pathways were imposed without much of their input. More interestingly, although the ignorers and decouplers effectively dealt with pathway implementation and maintained their autonomy, they were less satisfied than the embracers. The latter may have benefited from pathways being functional tools adapted to their practical needs and local conditions, facilitating rather than impeding their daily work. These findings again challenge the prediction of the zero-sum view that physicians are more satisfied as they move further away from pathways. Consistent with the institutional logics perspective, we found that actors developed diverse responses to standardization requirements and achieved non-zero-sum outcomes.
Discussion
In this article, we took advantage of the large-scale implementation of clinical pathways across China’s public hospitals to examine how physicians cope with these measures and how their experiences relate to perceived clinical autonomy and job satisfaction. We aim to advance the understanding of how professionals respond to rationalizing tools, such as clinical pathways, and more broadly, how professionals as agents navigate institutional complexity.
We identified four major types of physicians’ responses. The first group, the ignorers, avoided pathway engagement, faced limited monitoring, and maintained high clinical autonomy. By contrast, the coerced had little influence over pathway implementation and experienced stringent enforcement; they reported the lowest clinical autonomy and job satisfaction. Past research has largely emphasized the tension between bureaucracy and professionalism, framing professionals’ responses to rationalizing tools as a zero-sum struggle between professional resistance and managerial control (Numerato et al. 2012; Timmermans and Oh 2010). We found evidence for the conflict given that these two groups reflect the dominance of professionalism and managerialism, respectively. On the other hand, contrary to the prediction of the zero-sum view that the ignorers, who were the most able to distance themselves from the pathways, would enjoy the greatest job satisfaction, we observed that their satisfaction was only intermediate.
More importantly, our analysis revealed two other groups that went beyond the single-dimensional framework. One group of physicians decoupled formal pathway implementation from actual clinical work, preserving autonomy and reporting job satisfaction comparable to that of the ignorers. These physicians actively shaped pathway implementation but did not help put in place effective sanctioning procedures to ensure adherence. So the pathways were more ceremonial than functional in their everyday clinical activities. Decoupling thus offers physicians an alternative path to safeguarding autonomy when encountering rationalizing tools. In organizational studies, the new institutionalism literature has long viewed decoupling as an effective strategy to cope with external demands for transparency and accountability, allowing organizations to obtain legitimacy from key stakeholders while preserving efficiency in core operations or protecting internal constituents’ interests (DiMaggio and Powell 1983; Meyer and Rowan 1977). Despite its potential relevance, this concept has not been widely applied to research on professionals’ responses to rationalizing tools. Our study provides evidence of decoupling as a key professional strategy, thereby linking the institutional theory on organizations and the study of professions.
The final group, the embracers, played an active role in pathway implementation and helped install rigorous financial and administrative measures to ensure compliance. Importantly, despite strict enforcement, these physicians reported high clinical autonomy, comparable to that of the ignorers and decouplers, and the highest level of job satisfaction. They were also the most likely to see pathways as genuinely reflecting their clinical context, adhere closely to them, and reject the notion that they were mere formalities. This suggests that when physicians are substantially involved in designing and enforcing pathways, these tools can be made flexible and match actual clinical needs, potentially enhancing care quality and work experience. The case of the embracers dovetails with the emerging qualitative evidence suggesting that well-implemented rationalizing tools can deliver meaningful benefits. For instance, Wilhelm et al. (2020) found that junior physicians used clinical pathways as stabilizing reference points amid inconsistent treatment decisions by senior colleagues, thus aiding knowledge transfer. Levay and Waks (2009) observed that involving physicians in designing quality registries fostered constructive competition and reframed performance comparisons as opportunities for improvement. Rationalizing tools may also reconfigure existing power dynamics. Martin et al. (2017) reported that junior members leveraged them to challenge entrenched hierarchies and improve their own clinical performance. Our findings add to the evidence that codeveloped and contextually adapted rationalizing tools can enhance physicians’ work experience without undermining their autonomy.
In summary, we identified four responses that Chinese physicians developed in contexts of institutional complexity, where different institutional logics, most notably, those of professionalism, bureaucracy, and market, overlap. The logic of professionalism emphasizes expert autonomy, the bureaucratic logic stresses hierarchical control, and the market logic prioritizes profit-making. The recent “agentic turn” in the institutional logics scholarship highlights that competing yet coexisting logics generate spaces of tension and abundant opportunities, in which agents may creatively select, modify, and combine elements from different logics (Ocasio et al. 2017). Agentic responses thus draw on the sets of resources afforded by institutional complexity, but they are more than the mechanical permutations of distinct logics. Taking this agent-centered view, we adopted a data-driven approach to discern the major types of strategies actors actually used on the ground. The responses we identified resonate with some existing accounts of how different logics interact. For example, decoupling appears to align with the tactic of segmentation whereby different logics affect separate aspects of professional work, whereas embracing reflects a form of cooperative interweaving where adopting elements of one logic facilitates the functioning of others (Ocasio et al. 2017). At the same time, given the generative possibilities offered by institutional complexity, we do not claim that these responses represent an exhaustive mapping. Rather, they provide a starting point for further theoretical development and empirical inquiry.
Our findings intersect with the research on intraprofessional and interprofessional dynamics. Although the conflict view often regards rationalizing tools as sites of professional struggles, our results suggest that when such tools are collaboratively developed and tailored to local needs, they can potentially become sites of negotiated alignment among professionals operating in different domains. Within the profession, codeveloping pathways may foster shared norms and practices among diverse actors, such as senior and junior physicians, thereby fostering a more inclusive professional culture (Wilhelm et al. 2020). Across professions, coproduced standardization can serve as a common platform for collaboration with administrators, nurses, and other health workers (Gøtzsche-Astrup et al. 2023).
More broadly, the results prompt us to rethink what standardization and rational rules can offer to professionalism. Much prior research focuses on their constraints on professionals’ discretionary decision-making (Timmermans and Epstein 2010). But some scholars have argued that standardization can also benefit professionals, depending on the types of standards and the contexts in which they are enforced. For example, it can promote consistency in practice (Abbott 1987) and help preempt favoritism and foster democracy in the workplace (Timmermans and Epstein 2010:82). Our study contributes to illuminating the potential positive value and encourages a more balanced and nuanced view about standardization and rationalization. It also invites a reexamination of what autonomy means for professionals. Echoing Kant ([1797] 1996), true autonomy may not lie in the absence of constraints but in self-governance through abiding by rational rules that are made by the actors themselves.
If physicians’ responses to standardization are diverse, a natural follow-up question, albeit beyond the scope of this article, is why physicians reacted differently to pathway implementation. Existing literature has yet to systematically theorize the factors that shape professionals’ strategic choices, although both the sociology of professions and organizational theory offer useful leads. For instance, scholars have highlighted intraprofessional stratification, such as differences across specialties or between research elites and rank-and-file clinicians, that may produce divergent orientations (Freidson 2001) and the influence of institutional structures, power balances, and organizational cultures (e.g., Besharov and Smith 2014). Future research should utilize multilevel data and investigate the professional, institutional, and organizational antecedents of these response patterns.
This study has several limitations. First, our ability to obtain a fully representative sample was constrained by the absence of a comprehensive sampling frame, a common challenge in research on physicians in China. To mitigate this, we designed the study to ensure diversity across key dimensions relevant to pathway implementation, including geography, hospital type, and specialty. Second, due to the cross-sectional nature of our data, we cannot draw definitive conclusions about the causality between physicians’ coping strategies and their autonomy and satisfaction despite extensive control of possible confounders. Future research employing longitudinal data can be helpful to more rigorously assess causality and the temporal dynamics of professional responses.
This article draws on data from physicians in China’s public hospitals. Although clinical pathways were centrally mandated and Chinese physicians were closely embedded in their hospitals, most were able to employ diverse strategies to maintain clinical autonomy. Although China may represent a relatively constrained context for analyzing the spectrum of professional reactions, the distinction between “Western” and “Chinese” physicians should not be overstated. Research has highlighted transnational linkages in medical education, training, and hospital governance, challenging any simple binary distinctions (Baum 2020). We view China not as an outlier but as a site where globally circulating rationalizing tools interact with local institutional configurations. Given the widespread trend that physicians increasingly operate in large and complex organizations, the dynamics observed in China may offer valuable insights into how medical professionals globally navigate similar institutional pressures.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465261419783 – Supplemental material for Pathways to Autonomy: Chinese Physicians’ Responses to Clinical Pathways amid Institutional Complexity
Supplemental material, sj-docx-1-hsb-10.1177_00221465261419783 for Pathways to Autonomy: Chinese Physicians’ Responses to Clinical Pathways amid Institutional Complexity by Lei Jin and Lin Tao in Journal of Health and Social Behavior
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge the funding support of the Research Grant Council of Hong Kong (GRF-14612415).
Notes
Supplemental Material
Appendices A to C are available in the online version of the article.