
Abstract
This study examines the independent and interactive effects of adverse childhood experiences (ACEs) and positive childhood experiences (PCEs) on adolescent substance use. Guided by resilience theory, we analyze data from the 2024 Florida Youth Substance Abuse Survey, a representative sample of 18,962 high school students. Negative binomial regression models indicate that greater ACE exposure is significantly associated with increased substance use, whereas greater PCE exposure is associated with decreased substance use. Although the interaction between ACEs and PCEs is statistically significant, analyses of predicted counts and average marginal effects suggest that the moderating effect is modest rather than strongly protective. PCEs decrease overall substance use but do not substantially attenuate the association between ACE exposure and substance use. These findings clarify how compensatory and buffering processes operate differently in shaping adolescent health behavior.
Introduction
Adolescent substance use remains an important critical public health issue, linked to numerous short- and long-term adverse outcomes, including physical health problems, academic underachievement, and increased risk of substance dependence in adulthood (Brown and Shillington 2017; Hoffmann and Jones 2022). A comprehensive understanding of the risk and protective factors influencing substance use during adolescence is essential for developing effective prevention and intervention strategies. Two significant concepts addressed in recent research are adverse childhood experiences (ACEs) and positive childhood experiences (PCEs).
ACEs, encompassing various forms of abuse, neglect, and household dysfunction, have been consistently associated with heightened risks for substance use among adolescents (Felitti et al. 1998; Karatekin and Hill 2019). Research reveals a robust, dose–response relationship between the accumulation of ACEs and increased likelihood of substance use, highlighting the cumulative impact of early adversity (Dube 2020; Fothergill et al. 2016; Hughes et al. 2017; Villar et al. 2024). Consistent with this dose–response tradition, the present study employs a cumulative ACE measure to capture the overall burden of childhood adversity. This approach is widely used in ACE research because it both reflects the additive nature of risk exposure and provides a parsimonious way to estimate how boarder adversity patterns relate to adolescent substance use. Conversely, PCEs—including supportive relationships, safe environments, and meaningful social engagement—may be critical protective factors that promote resilience and healthy developmental trajectories (Bethell et al. 2019; Sege and Browne 2017).
Although ACEs and PCEs are usually examined independently, their simultaneous presence and interplay in affecting adolescent outcomes have gained increasing attention (Crandall, Broadbent, et al. 2020; Everett, Jones, and Hoffmann 2026). Recent studies suggest that PCEs may mitigate, although not eliminate completely, some of the risks associated with ACEs (Kim et al. 2024; Moyers et al. 2024). The precise nature and extent of these interactive effects are not well understood, however, especially regarding adolescent substance use. To address this important gap in the literature, the current study employs a resilience theory framework (Masten and Cicchetti 2016; Zimmerman 2013) to explore both independent and interactive roles of ACEs and PCEs in adolescent substance use using data from the 2024 Florida Youth Substance Abuse Survey (FYSAS). By exploring these relationships, our study aims to enhance the understanding of how adverse and positive experiences jointly influence adolescent behavioral health, informing targeted prevention and intervention programs.
Background
Adverse Childhood Experiences
ACEs—first conceptualized in the Centers for Disease Control and Prevention Kaiser study (Felitti et al. 1998)—have substantial public health implications. They include abuse, neglect, household dysfunction, community violence, and perceived neighborhood insecurity (Karatekin and Hill 2019). ACE exposure is highly prevalent: Between one-quarter and three-fourths of U.S. adults report at least one ACE, and about 21% report four or more (Park, Lee, and Han 2021). Research consistently links ACEs to adverse physical and mental health outcomes (Tzouvara et al. 2023), including anxiety and depression (Gajos et al. 2022), suicidality (Jensen et al. 2025; Lensch et al. 2021), bullying involvement (Everett et al. 2026), early neurodevelopmental disruptions (Andrzejewski et al. 2023), and psychiatric symptoms in adolescence (Bomysoad and Francis 2020).
ACEs are also associated with persistent and serious delinquency, chronic offending, and rearrest (Fox et al. 2015; Perez, Jennings, and Baglivio 2018); diminished self-regulation (Meldrum et al. 2020); and poorer neighborhood conditions (Jones, Everett, and Hoffmann 2024). These psychosocial consequences are compounded by neurobiological disruptions, including dysregulation of neurological and endocrine systems (Cooke et al. 2023). Notably, ACE-outcome associations typically follow a dose–response pattern, with greater exposure predicting more severe behavioral, emotional, and developmental impairments (Jensen et al. 2025; Meeker et al. 2021).
ACEs and Substance Use
Scholars increasingly recognize ACEs as significant risk factors for adolescent substance use. Studies consistently show that youth exposed to ACEs are more likely to use substances than those without such exposure (Brown and Shillington 2017; Hoffmann and Jones 2022; Villar et al. 2024). ACEs are also disproportionately common among adolescents receiving treatment for substance use disorders, with meta-analytic estimates indicating that 85.4% to 100% of individuals with substance use disorders report at least one ACE (Chandler, Kalmakis, and Murtha 2018; Leza et al. 2021; Philogene-Khalid et al. 2020).
ACEs rarely occur in isolation; exposure to one type of adversity often increases the likelihood of experiencing others, creating cumulative risk (Baglivio and Epps 2016). A growing body of evidence supports a graded, dose–response pattern, with each additional ACE increasing the likelihood of adolescent substance use (Dube 2020; Hoffmann and Jones 2022; Hughes et al. 2017). For example, Schauss et al. (2020) found that 47.2% of adolescents in a southeastern U.S. residential treatment facility who reported four or more ACEs also reported substance use. Shin, Edwards, and Heeren (2009), using nationally representative longitudinal data, identified a 79% increase in the odds of adolescent binge drinking among youth exposed to multiple ACE categories. Swedo et al. (2020) documented a graded association between ACE exposure and recent opioid misuse among 7th- to 12th-grade students in northeastern Ohio, with adolescents exposed to two to five or more ACEs having substantially higher odds of misuse than those reporting no ACEs. Additional research highlights distinct ACE clusters—particularly those involving family dysfunction and school safety—that exert stronger effects on substance use risk (Jayawardene et al. 2024). Collectively, this evidence underscores the robust, cumulative impact of ACEs on adolescent substance use.
Positive Childhood Experiences
PCEs encompass supportive, enriching, and nurturing environments or events that foster resilience and promote optimal health, psychosocial development, and well-being across adolescence and into adulthood (Bethell et al. 2019; Crouch et al. 2024; Cunha et al. 2024; Han et al. 2023; Sege and Browne 2017). These include stable and supportive relationships, safe home and community environments, opportunities for constructive social engagement, and contexts that encourage emotional growth (Han et al. 2023; Hero et al. 2025). PCEs are widespread: National survey data show that most U.S. youth experience at least one PCE, with specific PCEs ranging from roughly one-quarter to over 90%, depending on the domain (Anderson et al. 2024). Similarly, a population-based Wisconsin study found that over 86% of adults retrospectively reported three or more PCEs (Bethell et al. 2019).
PCEs are robust predictors of positive adolescent outcomes. They are associated with lower rates of depression, anxiety, suicidality, delinquency, bullying involvement, recidivism, and risky sexual behavior (Bergquist, Schmidt, and Thomas 2024; Crandall, Broadbent, et al. 2020; Everett et al. 2026; Kallapiran et al. 2025; Lynne et al. 2025; Novak and Fagan 2022). PCEs also correspond with better physical health, psychosocial functioning, and academic achievement (Crouch et al. 2022, 2024; Han et al. 2023; Sousa et al. 2025). Importantly, PCEs demonstrate a protective, dose-dependent relationship: Greater exposure predicts lower likelihood of adverse outcomes—an inverse pattern to the dose–response trend observed for ACEs (Everett et al. 2026; Lynne et al. 2025; Sousa et al. 2025; Zhang et al. 2021).
PCEs and Substance Use
PCEs have emerged as important protective factors and resiliency resources in reducing the likelihood of substance use during adolescence. Research on the role of PCEs in substance use prevention demonstrates that safe, nurturing, and connected childhood environments can substantially reduce the risk of substance use later in life (Crandall, Miller, et al. 2020; Moyers et al. 2024). Recent longitudinal and population-based studies provide consistent evidence that PCEs are associated with lower rates of substance use. For example, Kosterman et al. (2011) found that during adolescence, PCEs such as strong school engagement and interpersonal connection predicted a reduced risk of substance use disorders in adulthood. Similarly, youth who report higher levels of PCEs demonstrate lower rates of alcohol, tobacco, and illicit drug use, even after accounting for ACE exposure (Crandall, Miller, et al. 2020; Forster et al. 2017). In a nationally representative study of U.S. adolescents ages 12 to 17, Kim et al. (2024) found that each additional PCE increased the likelihood of recovering from a substance use disorder by 35%. Collectively, this body of evidence suggests that PCEs not only promote healthy developmental trajectories but also serve as critical leverage points for preventing and interrupting adolescent substance use—even in the context of early adversity.
ACEs, PCEs, and Substance Use
Since adverse and positive experiences both shape developmental trajectories across the life course (Elder, Johnson, and Crosnoe 2003; Masten and Cicchetti 2016), understanding their interactive effects on adolescent substance use is essential for advancing risk- and resilience-informed prevention. Although ACEs and PCEs are often examined separately, youth rarely encounter risk and protection in isolation. Instead, ACEs and PCEs commonly co-occur across homes, schools, and neighborhoods, jointly shaping behavioral health outcomes (Zimmerman 2013). Emerging evidence shows that PCEs can reduce—but not fully eliminate—the negative consequences of ACEs (Everett et al. 2026; Hinojosa and Hinojosa 2024; Wang et al. 2021).
Resilience theory offers a useful framework for understanding how ACEs and PCEs intersect to influence adolescent outcomes (Masten and Cicchetti 2016). It emphasizes that development is shaped by multiple interacting systems—including individual, family, school, and community contexts—that contribute to resilience over time (Zimmerman 2013). Resilience emerges through promotive factors, including internal assets (e.g., social skills, coping abilities, self-efficacy) and external resources (e.g., family support, school connectedness, community engagement), which enhance adolescents’ ability to navigate adversity (Fergus and Zimmerman 2005; Zimmerman 2013). In its ecological formulation, resilience theory underscores that adaptive capacity is embedded within broader environmental contexts (Fergus and Zimmerman 2005), aligning with ecological models of development (Bronfenbrenner 1994).
Within this framework, PCEs function as key promotive factors through two pathways. In the compensatory model, PCEs exert direct benefits on adolescent outcomes regardless of adversity exposure (Fergus and Zimmerman 2005). For example, strong school engagement or emotionally supportive caregivers may reduce substance use for all youth. In the protective model, PCEs moderate risk by buffering the negative impact of ACEs, weakening their association with behavioral health outcomes such as substance use. PCEs may thus be particularly influential for adolescents with high ACE exposure, helping redirect developmental trajectories toward healthier coping responses. Recognizing these dual pathways highlights the importance of examining both the direct and buffering roles of PCEs in shaping substance use.
Despite growing research documenting the independent associations of ACEs and PCEs on negative health and behavioral outcomes (e.g., Bethell et al. 2019; Crandall, Broadbent, et al. 2020; Hughes et al. 2017), important gaps remain. Although several studies demonstrate that PCEs are associated with improved mental and behavioral outcomes net of adversity exposure (e.g., Bethell et al. 2019; Crouch et al. 2022), fewer have rigorously examined whether PCEs condition the association between ACEs and adolescent substance use in large, statewide samples. Moreover, prior work often treats PCEs as uniformly buffering ACEs, with limited attention to whether their influence varies across levels of ACE exposure. Resilience theory distinguishes between compensatory processes—where promotive factors reduce risk regardless of adversity—and protective processes—where promotive factors weaken the association between adversity and outcomes (Fergus and Zimmerman 2005). Yet empirical tests that clearly differentiate these mechanisms in the context of adolescent substance use remain limited.
Current Study
Guided by cumulative risk and resilience frameworks, this study evaluates whether PCEs modify or simply offset the association between ACEs and adolescent substance use. Using a large, population-based sample of Florida high school students, we test three propositions. First, consistent with cumulative risk theory, ACE exposure will be associated with increased substance use. Second, consistent with promotive models of resilience, PCE exposure will be associated with decreased substance use net of ACEs. Third, we assess whether PCEs moderate the association between ACEs and substance use, thereby distinguishing between compensatory processes—where PCEs are linked to lower substance use across levels of adversity—and protective processes—where PCEs attenuate the strength of the ACE–substance use relationship. By explicitly testing these competing resilience mechanisms within a large statewide sample, this study helps clarify whether PCEs function primarily as promotive influences or as a protective mechanism that meaningfully attenuates ACE-related health and behavioral outcomes.
Data and Methods
Sample
The present study used data from the 2024 Florida Youth Substance Abuse Survey (FYSAS), 1 a large-scale annual survey of youth enrolled in Florida public middle and high schools. The survey employs a two-stage cluster sampling design to produce a cross-sectional, statewide representative sample. In the first stage, separate samples of middle schools (Grades 6–8) and high schools (Grades 9–12) were randomly selected within each of Florida’s 67 counties, with selection probabilities proportional to school enrollment. All educational institutions are eligible except adult education, correctional, vocational, and special education schools. In the second stage, classrooms are randomly selected within participating schools to meet survey quotas; English for speakers of other languages classrooms are excluded from the sampling frame.
Data collection occurred during the first three months of 2024 using paper-and-pencil optical scan forms or, in some schools, an online platform. A total of 48,352 youth completed the survey. Following administration, the FYSAS team removed cases failing any of five validation checks (n = 3,341) and cases administered at an incorrect grade level (n = 256), 2 yielding a final data set of 44,755 respondents. Because middle school students were not asked ACE items, analyses were restricted to the high school sample (n = 22,016). Missing data were handled using multiple imputation (see the following). Descriptive statistics for the nonimputed data appear in Table 1.
Descriptive Statistics: 2024 Florida Youth Substance Abuse Survey.
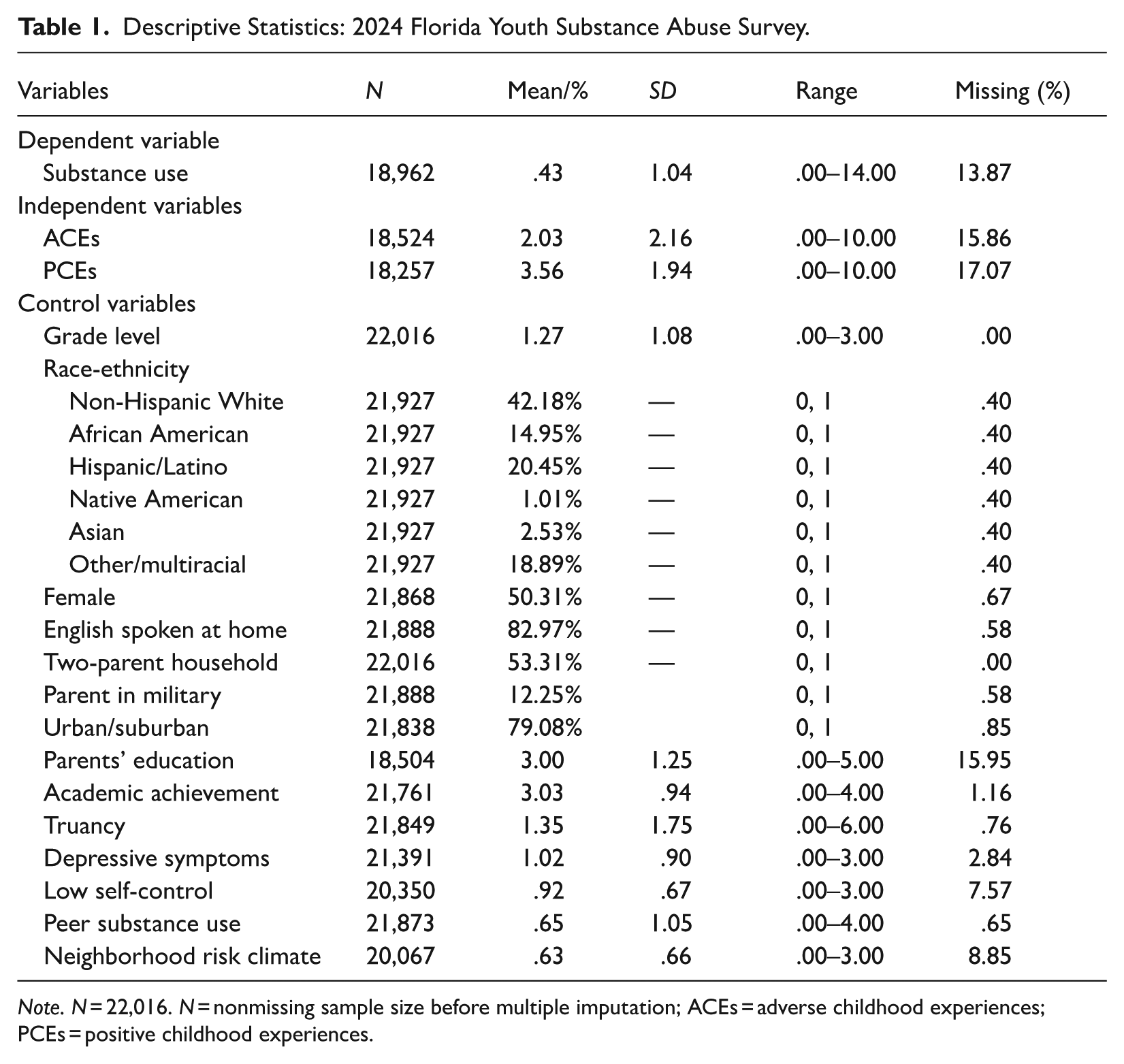
Note. N = 22,016. N = nonmissing sample size before multiple imputation; ACEs = adverse childhood experiences; PCEs = positive childhood experiences.
Substance Use
Substance use was measured with 14 items assessing the number of occasions (if any) participants used the following substances in the past 30 days: (1) alcohol, (2) marijuana/hashish, (3) vape nicotine, (4) vape marijuana, (5) inhalants, (6) methamphetamine, (7) club drugs, (8) LSD, (9) cocaine or crack, (10) depressants, (11) prescription opioid pain relievers, (12) over-the-counter medications purchased or used in order to get high (e.g., cold and cough medications), (13) heroin, and (14) amphetamines (e.g., Ritalin, Adderall). Response options ranged from “0 occasions” (=0) to “40 or more occasions” (=6). Given the rarity of frequent use across many substances, we coded any past-30-day use as 1 for each substance and summed the indicators to create a variety index of substance involvement (α = .70). Psychometric studies indicate that variety scales tend to yield greater validity and reliability than alternative measures (Bendixen, Endresen, and Olweus 2003; Stewart et al. 2023).
Adverse Childhood Experiences
To capture ACEs, we constructed a variety index comprised of the summed scores from 10 dichotomous items. The survey asked respondents a series of “Yes” (=1) or “No” (=0) questions regarding any lifetime experience with (1) emotional abuse by a parent or other adult, (2) physical abuse by a parent or other adult, (3) sexual abuse, (4) parental separation or divorce, (5) parents’ physical abuse of each other, (6) living with someone who has a drinking problem or abuses illicit drugs, (7) living with someone who has mental health issues or has attempted suicide, (8) living with someone who was incarcerated, (9) emotional neglect by family members, and (10) physical neglect by parents (for a full list of items, see Appendix Table A, available in the online version of the article).
Positive Childhood Experiences
According to the healthy outcomes positive experiences framework (Crouch et al. 2022; Sege and Browne 2017), PCEs encompass four broad domains: nurturing and supportive relationships, living in a safe or stable environment, constructive social engagement, and opportunities to develop social and emotional competencies. Guided by this framework, we identified 10 PCE indicators available in the FYSAS data, each representing a distinct dimension of positive experiences. For multiitem PCE indicators, we first constructed compositive scales using the full ordinal response information, with higher values indicating more positive experiences. Consistent with prior PCE research (e.g., Bethell et al. 2019; Lynne et al. 2025), we followed Arthur et al.’s (2007) framework for deriving cut points at the scale level. Specifically, composite scores were dichotomized using a distribution-based threshold defined as the median plus 1.5 times the median absolute deviation. To maintain consistency across all PCE measures, we applied the same distribution-based cut points to single-item indicators; given their limited response range, this threshold typically corresponded to endorsement of the highest response category.
Supportive teachers was measured using three items assessing relational support from teachers, including praise for good work, praise for hard work, and the ability to speak one-on-one with a teacher. Response options ranged from “NO!” (=0) to “YES!” (=3). Quality of parent–child relationships captured relational warmth and accessibility through four items assessing enjoyment of time spent with mother and father, ability to seek help from a parent, and opportunities to engage in fun activities together. Response options ranged from “NO!” (=0) to “YES!” (=3). Items referring to each parent were retained as reported by youth regardless of household structure; family structure was controlled for separately in all analyses.
Supportive parents was assessed with two items measuring parental affirmation, including whether parents notice and acknowledge when the participant does a good job and how often parents express pride in the youth’s accomplishments. Response options ranged from “never or almost never” (=0) to “all the time” (=4). Parent–child collaboration was measured with a single item that asked respondents, “Do your parents ask for your input on family decisions?” The response options ranged from “NO!” (= 0) to “YES!” (= 3). Parental monitoring/discipline was assessed using eight items capturing rule clarity, parental awareness, and perceived likelihood of detection for various forms of misbehavior, including alcohol use, weapon carrying, skipping school, coming home late, and violating family rules about substance use, and whether parents inquire about their homework completion. Responses ranged from “NO!” (=0) to “YES!” (=3).
Youth felt safe at school was measured with a single item assessing perceived safety at school, with response options ranging from “NO!” (=0) to “YES!” (=3). Involvement in extracurricular activities was measured with a single yes/no item that captured participation in organized school or community activities, including school sports, non-school sports, band, and clubs. School connectedness was assessed with four items measuring perceived meaningfulness of schoolwork, effort in school, enjoyment of being at school, and dislike of school (reverse-coded). Response ranged from “never” (=0) to “almost always” (=4). Church attendance was measured by a single item assessing frequency of religious service attendance ranging from “never” (=0) to “about once a week or more” (=3). Prosocial peer association was measured using six items assessing perceived peer disapproval of substance use behaviors, including alcohol use, tobacco use, marijuana use, nicotine vaping, marijuana vaping, and nonprescribed prescription drug use. Response options ranged from “very wrong” (=0) to “not wrong at all” (=3).
Finally, we constructed a cumulative PCE index by summing the 10 dichotomized PCE indicators, yielding scores ranging from 0 to 10, with higher values reflecting exposure to a greater number of PCEs. This cumulative PCE measurement strategy is consistent with prior ACE–PCE research employing additive counts of protective experiences (Bethell et al. 2019; Crandall, Broadbent, et al. 2020; Lynne et al. 2025) and aligns conceptually with resilience theory’s emphasis on the accumulation of supportive resources across ecological contexts (Bronfenbrenner 1994; Fergus and Zimmerman 2005; Masten and Cicchetti 2016; Zimmerman 2013).
Control Variables
The analyses included several control variables. Grade level was coded ordinally (9 = 9th grade to 12 = 12th grade). Race-ethnicity was captured with a six-category measure identifying youth as African American, Hispanic/Latino, Native American, Asian, Other/Multiracial, and Non-Hispanic White (reference). A binary variable identified respondents as female (=1) or male (=0); no alternative gender measure was available. We also included dichotomous indicators for language spoken at home (English = 1) and community context (urban/suburban = 1 vs. rural/farm = 0).
Two-parent household was coded 1 when youth resided with two married or cohabiting biological parents; all other structures (single-parent, stepfamilies, extended family households, etc.) were coded 0. This covariate accounted for differences in parental availability and household composition. Parent in the military was coded 1 if youth reported having a parent or guardian in the military. As a proxy for socioeconomic status, we included parental education, averaging two items assessing each parent’s educational attainment (“grade school or less” = 0 to “graduate or professional school after college” = 5). 3 To account for academic functioning, we included academic achievement (“Mostly Fs” = 0 to “Mostly As” = 4) and truancy (“None” = 0 to “11 or more days” = 6) in the past month.
We also incorporated several risk and protective factors. Depressive symptoms were measured with four items assessing hopelessness, low self-worth, perceived failure, and persistent sadness. Responses ranged from “NO!” (=0) to “YES!” (=3), and items were averaged (α = .91). To capture low self-control, we used six items from the Grasmick et al. (1993) scale—two each assessing impulsivity and anger—with responses from “strongly disagree” (=0) to “strongly agree” (=3). Items were averaged (α = .84). A peer substance use index (five items; α = 0.91) measured how many of youths’ four closest friends had smoked cigarettes, tried alcohol, used marijuana, vaped nicotine, or vaped marijuana in the past 12 months (“none” = 0 to “4” = 4). Neighborhood risk climate was included to account for broader contextual conditions that may confound PCE–outcome associations. This multiitem index captured perceived ease of access to alcohol, cigarettes, marijuana, hard drugs, and handguns (“very hard” = 0 to “very easy” = 3); perceived adult norms regarding youth substance use (“very wrong = 0 to “not wrong at all = 3); and perceived likelihood of police enforcement for youth substance use (“NO! = 0 to YES!” = 3). Items were averaged (α = .86), with higher scores indicating greater perceived availability and weaker informal and formal social control.
Analytical Strategy
We first estimated descriptive statistics for the high school sample. To model the relationship between ACEs, PCEs, and substance use, we estimated negative binomial regression models (Hoffmann 2016), appropriate for overdispersed count variables. ACEs and PCEs were modeled as continuous variables. To assess moderation, we included a continuous interaction term (ACEs × PCEs).
Because interaction terms in nonlinear models cannot be directly interpreted as conditional effects (Breen, Karlson, and Holm 2018; Long and Freese 2014; Mize 2019), we followed recommended practice by examining predicted counts and marginal effects. Predicted substance use counts were presented as average adjusted predictions, with control variables allowed to vary across respondents; standard errors were computed using the delta method. To further interpret the interaction, we estimated average marginal effects (AMEs) of ACEs evaluated at low (–1 SD), mean, and high (+1 SD) levels of PCEs. We also tested differences in marginal effects across PCE levels using slope-difference tests (Long and Mustillo 2021; Mize 2019).
To address missing data, we used multiple imputation (MI) to generate 25 data sets with 250 burn-ins via chained equations (Graham, Olchowski, and Gilreath 2007). Because substance use may not be missing at random, we followed Von Hippel’s (2007) conservative approach: The outcome was used to impute independent variables, but cases with imputed outcomes were excluded. Auxiliary variables (race-ethnicity, grade, gender) were included to reduce bias (Graham 2009). Models were weighted by county to account for FYSAS’s two-stage sampling design. Analyses were conducted pre- and post-MI, with no meaningful differences observed. The final analytic sample included 18,962 Florida high school students. All analyses were conducted in STATA 18.5.
Results
Descriptive statistics for the variables are presented in Table 1. Youth in the sample, on average, used .43 substances within the past 30 days. Regarding exposure to ACEs, youth in the sample had an average ACE score of 2.03, while the average PCE score was 3.56. Table 1 also shows that the sample is diverse with respect to grade level, gender, race-ethnicity, geographical location, and neighborhood context. About 53.3% of youth reported living with their biological parents who averaged some college education.
Main and Interactive Effects of ACEs and PCEs on Substance Use
The results of the negative binominal models designed to estimate the incidence rate of substance use are presented in Table 2. In Model 1, these findings reveal that a 1-unit increase in a youth’s ACE score is associated with a significant higher rate of substance use (4.9%, p < .01). By contrast, a 1-unit increase in a youth’s PCE score is associated with a significantly lower rate of substance use (9.6%, p < .001). Regarding other predictors of substance use, we find that Hispanic/Latino (incidence rate ratio [IRR] = .778, p < .05) and Asian youth (IRR = .486, p < .001) reported lower rates of substance use than non-Hispanic White youth. Furthermore, significantly higher rates of substance use were exhibited among female youth (IRR = 1.190, p < .01) compared to male youth. Additionally, significantly higher rates of substance use were shown among youth who were in higher grade levels (IRR = 1.105, p < .001), had skipped school (IRR = 1.084, p < .001), had low self-control (IRR = 1.260, p < .001), associated with peers who engaged in substance use (IRR = 1.874, p < .001), and lived in neighborhoods with higher levels of antisocial features and behaviors (IRR = 1.589, p < .001).
Negative Binomial Regression: Main and Interactive Effects of ACEs and PCEs on Substance Use (N = 18,962).
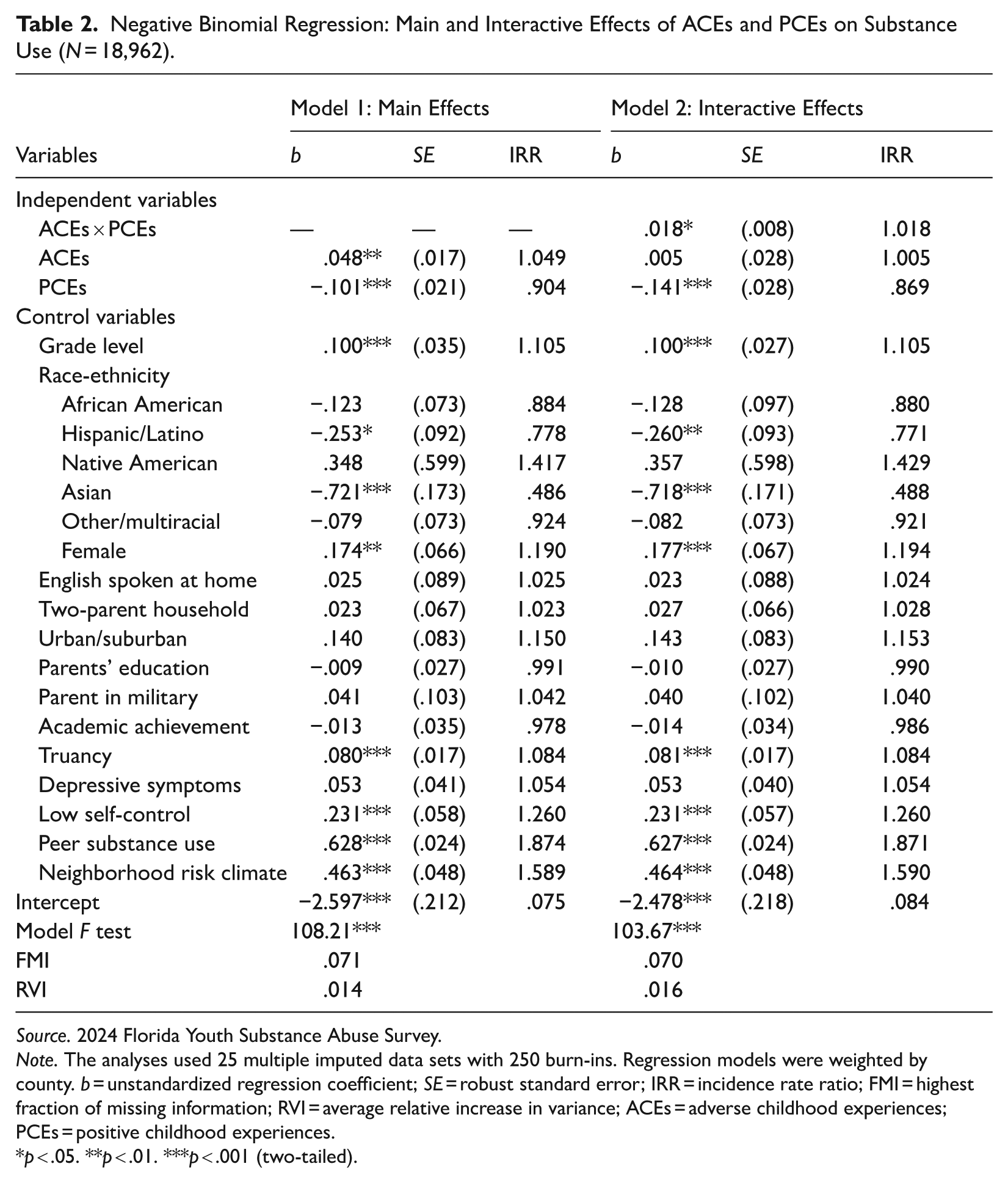
Source. 2024 Florida Youth Substance Abuse Survey.
Note. The analyses used 25 multiple imputed data sets with 250 burn-ins. Regression models were weighted by county. b = unstandardized regression coefficient; SE = robust standard error; IRR = incidence rate ratio; FMI = highest fraction of missing information; RVI = average relative increase in variance; ACEs = adverse childhood experiences; PCEs = positive childhood experiences.
*p < .05. **p < .01. ***p < .001 (two-tailed).
Given the challenges with interpreting interaction coefficients in nonlinear models, Figure 1 plots the predicted counts of substance use across increasing ACE exposure at low (−1 SD), mean, and high (+1 SD) values of the continuous PCEs measure based on Model 2 (Table 2). Table 3 presents the corresponding predicted counts. At lower levels of ACE exposure, predicted substance use is substantially lower among youth with higher PCE scores relative to those with fewer PCEs. However, as ACE exposure increases, predicted substance use rises across the range of PCE values, and the distance between the illustrative PCEs points narrows. This pattern indicates that while higher PCE scores are associated with lower expected substance use overall, their protective association diminishes as ACE scores increase.
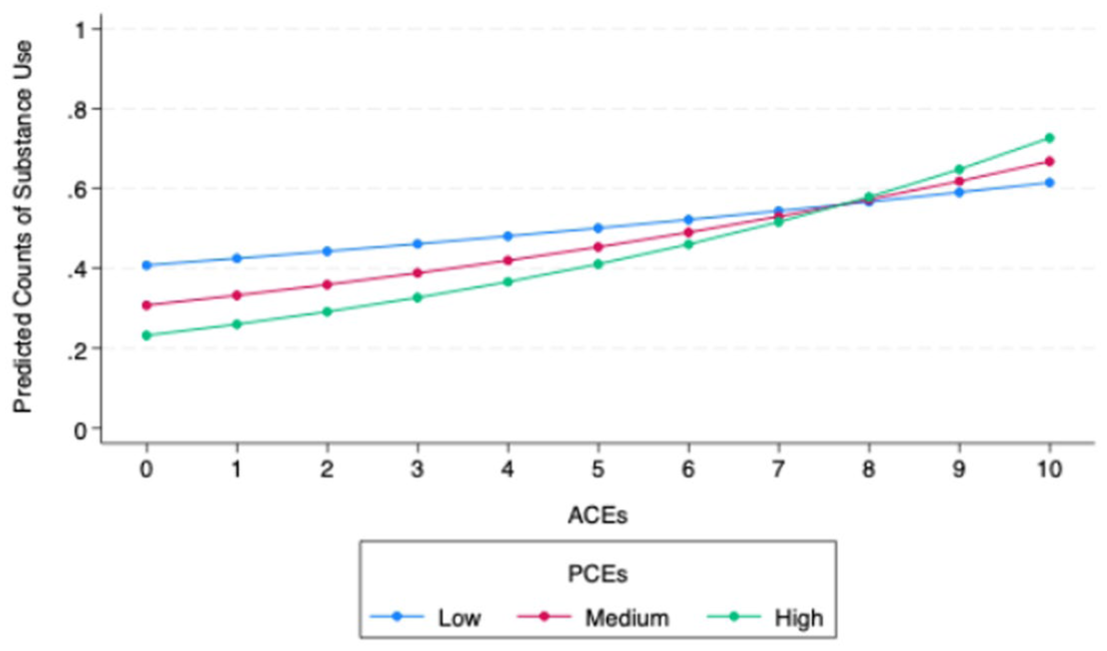
Predicted counts of substance use by ACEs and PCEs (N = 18,962).
Predicted Substance Use across ACE and PCE Levels (N = 18,962).
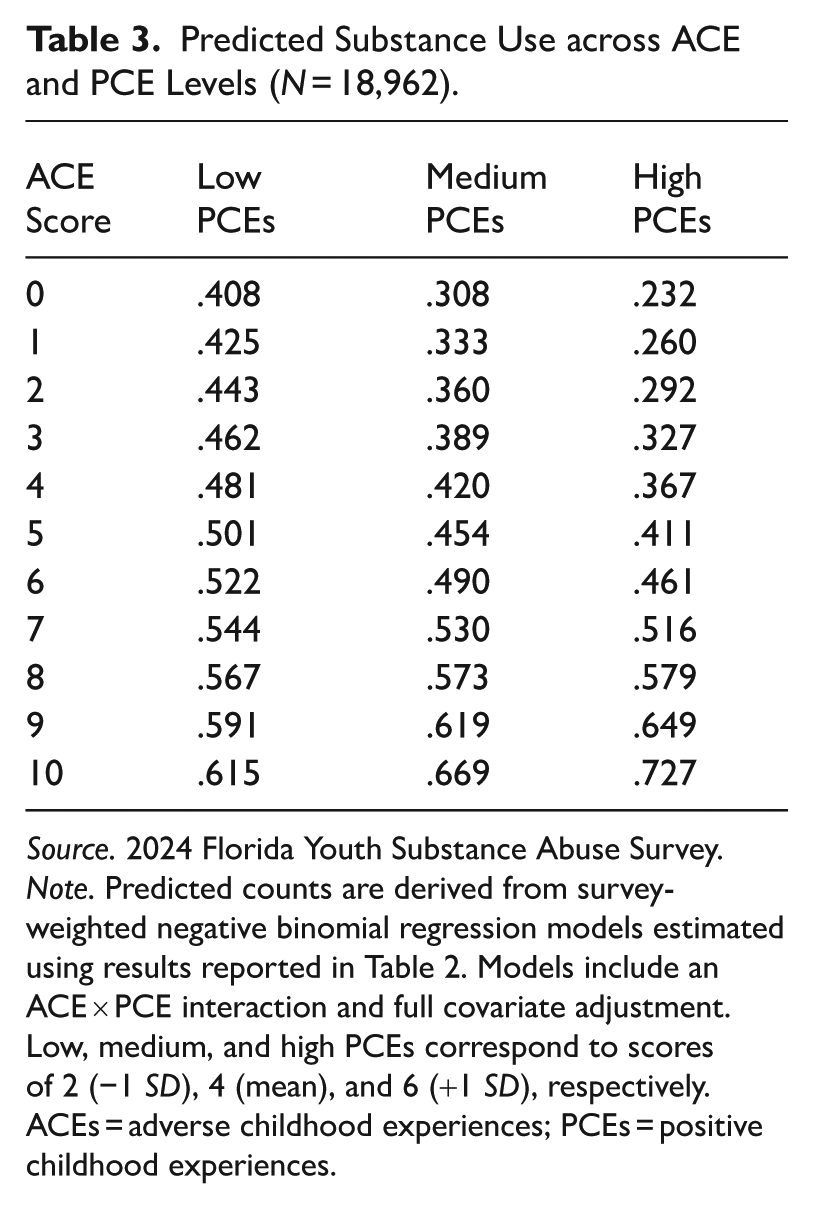
Source. 2024 Florida Youth Substance Abuse Survey.
Note. Predicted counts are derived from survey-weighted negative binomial regression models estimated using results reported in Table 2. Models include an ACE × PCE interaction and full covariate adjustment. Low, medium, and high PCEs correspond to scores of 2 (−1 SD), 4 (mean), and 6 (+1 SD), respectively. ACEs = adverse childhood experiences; PCEs = positive childhood experiences.
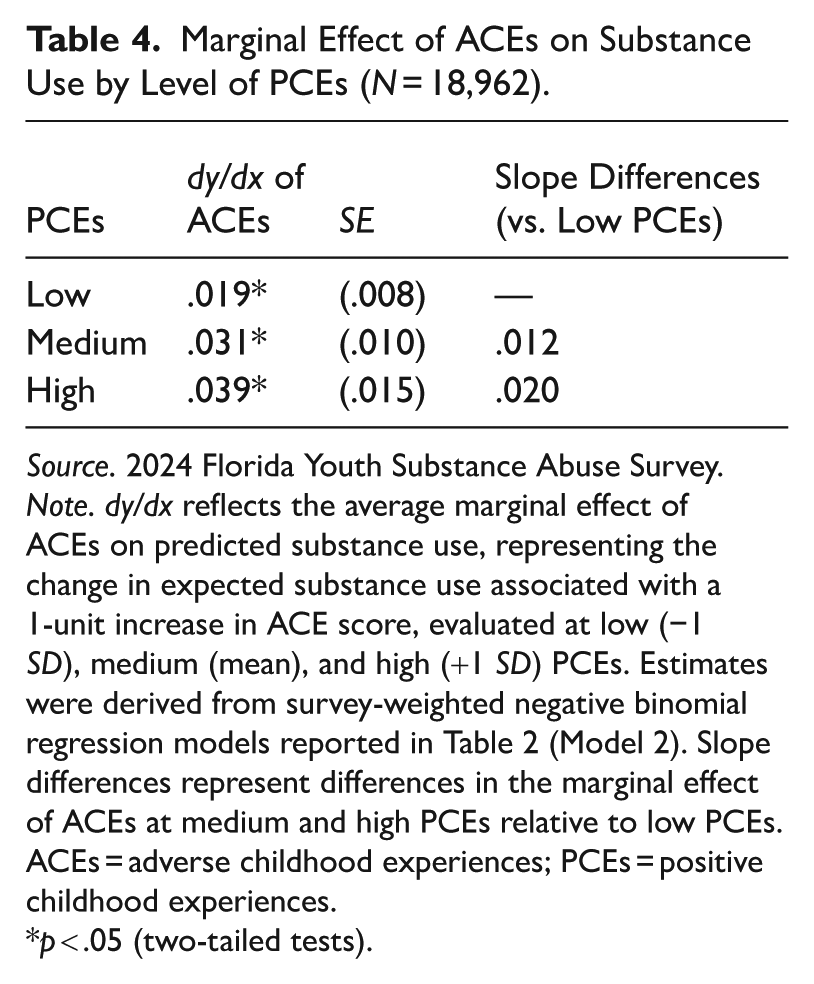
To more formally evaluate moderation, Table 4 presents the AMEs of ACEs evaluated at low, mean, and high values of PCEs. The marginal effect of ACEs is statistically significant at each level of PCEs, indicating that greater ACE exposure is associated with higher substance use across the range of PCE scores. Although the magnitude of the ACE slope increases numerically at higher PCE values, formal tests of slope differences relative to low PCEs are not statistically significant. Taken together, these findings suggest that PCEs are associated with lower overall substance use but do not significantly attenuate the association between ACEs and substance use.
Marginal Effect of ACEs on Substance Use by Level of PCEs (N = 18,962).
Source. 2024 Florida Youth Substance Abuse Survey.
Note. dy/dx reflects the average marginal effect of ACEs on predicted substance use, representing the change in expected substance use associated with a 1-unit increase in ACE score, evaluated at low (−1 SD), medium (mean), and high (+1 SD) PCEs. Estimates were derived from survey-weighted negative binomial regression models reported in Table 2 (Model 2). Slope differences represent differences in the marginal effect of ACEs at medium and high PCEs relative to low PCEs. ACEs = adverse childhood experiences; PCEs = positive childhood experiences.
*p < .05 (two-tailed tests).
Sensitivity Analyses
We conducted several sensitivity analyses to assess the robustness of our findings to alternative measurement and modeling decisions. First, to evaluate whether dichotomizing the PCE indicators influenced the results, PCEs were modeled as a latent construct using confirmatory factor analysis. Empirical Bayes factor scores were derived and used in negative binomial regression models to estimate the ACEs × PCEs interaction. Although coefficients are somewhat larger in the latent specification, the direction, statistical significance, and substantive interpretation of the findings remain the same.
Second, to examine potential nonlinearities in the ACEs–substance use association, we reestimated the interaction model treating ACEs as a categorical variable (0, 1, 2, 3, 4, 5+). Predicted values were nearly identical to those from the linear specification, providing no evidence of distinct threshold effects. Third, to assess whether including psychosocial and academic covariates affected the focal associations, we reestimated the primary models without depressive symptoms, self-control, and academic indicators. Coefficients differed minimally (.01) from the fully adjusted models, and the ACE × PCE interaction results remained substantively unchanged.
Finally, because the substance use measure includes nonmedical use of prescription drugs as well as illicit substances, we estimated models using alternative outcome specifications: (a) a dichotomous indicator of any past-30-day use, (b) a three-category variable distinguishing illegal use from prescription-only misuse (no use, prescription-only use, and illegal substance use), and (c) a count excluding prescription and over-the-counter items. Across all three specifications, the substantive results—including the ACE and PCE main effects and the ACE × PCE interaction—remained consistent. Together, these analyses indicate that the findings are robust to alternative operationalizations of PCEs, ACEs, covariates, and substance use.
Discussion
The current study examined the independent and interactive associations of ACEs and PCEs with substance use in a large, population-based sample of U.S. high school students from Florida. Consistent with prior research, adolescents who reported more ACEs reported higher rates of substance use (Dube 2020; Hoffmann and Jones 2022; Hughes et al. 2017; Shin et al. 2009; Swedo et al. 2020), whereas PCEs were associated with lower predicted substance use (Crandall, Broadbent, et al. 2020; Forster et al. 2017; Kim et al. 2024), even after adjusting for sociodemographic characteristics and our predictors of substance use. These findings align with the cumulative risk and resilience frameworks that posit that adverse experiences elevate behavioral health risks and positive experiences are associated with healthier outcomes (Fergus and Zimmerman 2005; Masten and Cicchetti 2016). In particular, the observed inverse association between PCEs and substance use supports a compensatory model of resilience in which promotive experiences can provide a direct beneficial influence on adolescent outcomes regardless of ACE exposure (Crandall, Broadbent, et al. 2020; Forster et al. 2017; Kim et al. 2024; Zimmerman 2013).
We also evaluated whether PCEs moderated the association between ACEs and substance use. Although the interaction term was statistically significant, closer examination of predicted counts and AMEs revealed a pattern inconsistent with a strong buffering interpretation. Adolescents reporting higher levels of PCE exposure consistently engaged in lower rates of substance use. However, substance use increased as ACE exposure increased across the full range of PCE scores, and formal contrasts indicated that differences in the marginal effects ACEs across levels of PCE exposure were not statistically significant. In other words, while PCEs were associated with lower base levels of substance use, they did not meaningfully attenuate the association between ACEs and substance use. This pattern is consistent with prior research suggesting that the influence of promotive experiences may be constrained at higher levels of adversity (Everett et al. 2026; Hinojosa and Hinojosa 2024; Scholtes and Cederbaum 2024).
Our findings underscore resiliency as a dynamic, context-dependent mechanism rather than a uniform buffering mechanism. Positive and adverse experiences may coexist in ways that generate tension rather than straightforward protection. Youth may encounter “safe” spaces embedded within broader contexts of risk (DaViera et al. 2020) or develop coping strategies in response to environmental unpredictability (Ellis et al. 2022) that simultaneously support adaptation and maintain heightened vigilance. Such “conflicting worlds” suggest that promotive experiences operate within—rather than outside of—broader structural and interpersonal exposures. The same social contexts that foster connection and support may also reproduce stress or constrain the capacity of protective processes to offset cumulative adversity (Bronfenbrenner 1994; Masten and Cicchetti 2016).
Taken together, these findings refine sociological understandings of resilience by distinguishing between compensatory and protective processes. Although PCEs were associated with lower baseline levels of substance use, they do not substantially attenuate the association between ACEs and substance use. This distinction clarifies that resilience may manifest in a patterned reduction in baseline vulnerability rather than overcoming the associated consequences of ACEs. By demonstrating that positive and adverse experiences coexist without necessarily neutralizing one another, this study highlights the layered and structurally embedded nature of adolescent health and behavioral outcomes.
While this study offers several important contributions, it is not without limitations. First, the sample is limited to Florida high school students, cautioning against generalization to other populations. Second, our outcome measure, which captures self-reported use of multiple illicit substances in the past 30 days, is derived from cross-sectional data. This design prevents us from establishing temporal sequencing with certainty. Such limitations are not unique to our study; much of the literature on both ACEs and PCEs similarly relies on cross-sectional approaches, making it difficult to disentangle whether observed associations reflect true consequences or, alternatively, underlying causes (Hughes et al. 2017; Kallapiran et al. 2025). Third, while we can capture several different categories of ACEs, there are other types of ACEs that are not captured in this study that may influence delinquency, such as exposure to the death of a loved one, exposure to community violence, or bullying victimization, which may exert considerable influence on delinquency. Moreover, due to data limitations, we are unable to capture the frequency, severity, or duration of exposure to each ACE.
Fourth, our operationalization of PCEs is constrained by the measures available in the FYSAS. Although our PCE indicators align with prior research and capture relational, school, and peer-based experiences, the data do not include direct measures of neighborhood safety, housing stability, or collective efficacy. While we adjust for neighborhood risk climate—reflecting perceived availability of substances and firearms as well as informal and formal regulation of youth substance use—this measure captures exposure and regulatory context rather than protective environmental conditions. As such, our operationalization does not fully capture the environmental dimension of the healthy outcomes from positive experiences framework. Future research would benefit from incorporating direct measures of neighborhood-level protective processes. Finally, our cumulative PCE measure assumes that each positive experience contributes similarly to protective exposure, limiting our ability to assess the relative influence of specific domains.
In conclusion, this study underscores the importance of examining ACEs and PCEs in tandem when evaluating adolescent substance use. While ACEs elevate substance use, PCEs reduce baseline risk of substance use without fully disrupting the influence of ACEs. These findings suggest that resilience is not simply the attenuation of risk but a contextually embedded process shaped by layered social environments. Future longitudinal research that incorporates more comprehensive measures of environmental stability and protective processes will be essential for clarifying how resilience unfolds across adolescence and how broader social structures shape both risk and protection.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465261457836 – Supplemental material for Two Sides of Childhood: How Adverse and Positive Childhood Experiences Shape Adolescent Substance Use
Supplemental material, sj-docx-1-hsb-10.1177_00221465261457836 for Two Sides of Childhood: How Adverse and Positive Childhood Experiences Shape Adolescent Substance Use by Melissa S. Jones, Ashleigh C. Anderson, Annabelle H. Bailey, Mara J. Erickson and John P. Hoffmann in Journal of Health and Social Behavior
Footnotes
Acknowledgements
The authors would like to thank the Florida Departments of Children and Families, Health, Education, and Juvenile Justice and Rothenbach Research and Consulting, LLC, for making these data available. The analyses, conclusions, views, and opinions presented here are those of authors alone and should not be attributed to any of the organizations that sponsor the Florida Youth Substance Abuse Survey.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.