
Abstract
The results of a survey exploring counselor attitudes toward the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) are presented. The survey revealed that counselors have mixed attitudes toward the DSM. They view DSM positively and see it as both beneficial to their profession and important in determining treatment. They also believe that DSM-5 revisions reflect the best science available. Counselors worry that the DSM prioritizes diagnosis over treatment, have concerns about proposed DSM-5 revisions, and support developing alternatives to the DSM.
The Diagnostic and Statistical Manual of Mental Disorders (DSM), hailed by its authors as the “standard reference” in both practice and research settings (American Psychiatric Association, 2013), is an important tool employed by counselors and other mental health professionals. However, despite counselors’ widespread use of the DSM, there has been little research on their attitudes toward it. The few existing studies imply that counselors have mixed feelings about the DSM (Mead, Hohenshil, & Singh, 1997; Patureau-Hatchett, 2008; Strong, Gaete, Sametband, French, & Eeson, 2012). After briefly reviewing the existing literature, we present new survey data reaffirming counselors’ mixed feelings about the DSM. While they appreciate the scientific status and practical uses of the DSM and see it as beneficial to their profession, counselors also worry about its impact on clients and are interested in seeing alternatives to it developed.
Counselor Attitudes Toward the DSM
Mead et al. (1997) conducted the only published quantitative study on counselor attitudes toward the DSM. They found that clinical mental health counselors consult the DSM regularly, with over 90% citing it as their most frequently used professional reference and rating themselves as usually making accurate diagnoses. Just over half of respondents said they would use the DSM even if it was not required. Billing was rated most highly as an advantage of the DSM, but case conceptualization, treatment planning, and communication were also seen as advantages. Perceived disadvantages were bias in labeling and difficulty in use; the latter finding is interesting given that over 90% of respondents also indicated they usually diagnose accurately. Counselors saw intentional underdiagnosis or overdiagnosis as common and problematic, while also finding the DSM unsatisfactory for use in couples and family counseling. Despite their concerns, a little more than 70% of respondents agreed that the advantages of the DSM outweighed its disadvantages.
Mead et al.’s (1997) findings are largely supported by Patureau-Hatchett (2008), whose dissertation found that counselors (a) identified billing as the most important reason for diagnosing, (b) expressed concern about underdiagnosis and overdiagnosis, and (c) felt conflicted about having to diagnose one partner in order to bill insurance for couples therapy. Additionally, while counselors self-identified as multiculturally competent, they did not see this or their counseling identity as inconsistent with using the DSM (Patureau-Hatchett, 2008). The only other published study of counselor attitudes toward the DSM is a qualitative study by Strong et al. (2012). They mapped counselor attitudes toward the DSM, finding them complex and influenced by circumstances; nonetheless, some of the same themes found in other studies seemed to emerge—namely, that the DSM can be useful and helps people access services, but can also medicalize problems.
Other Professionals’ Attitudes
Psychologists
A recent study of ours suggests that psychologists’ attitudes toward the DSM have changed little since the early 1980s (Raskin & Gayle, 2016). We found that psychologists value the DSM for providing diagnoses and streamlining reimbursement through its inclusion of diagnostic codes. However, psychologists are concerned that the DSM pathologizes clients and medicalizes psychosocial problems. In our study, psychologists’ overall view of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) was more negative than neutral. They were interested in seeing alternative approaches to DSM-5 diagnosis developed, but did not wish to see diagnosis abandoned entirely. These findings are mostly consistent with the only previous research on psychologist attitudes toward the DSM, conducted over 30 years ago—the main difference being that unlike now, psychologists back then supported nondiagnosis (Miller, Bergstrom, Cross, & Grube, 1981; Smith & Kraft, 1983). The DSM has changed, but psychologist attitudes toward it have remained consistently skeptical at best (Raskin & Gayle, 2015).
Psychiatrists
Past research on psychiatrists’ attitudes toward the DSM found that psychiatrists were more positive about the manual than counselors or psychologists (Smith & Kraft, 1989)—not surprising given their authorship of the manual. This is consistent with other research showing that psychiatrists generally support the DSM (Jampala, Zimmerman, Sierles, & Taylor, 1992; Junek, 1983; Kortan et al., 2000; Maser, Kaelber, & Weise, 1991; Setterberg et al., 1991; Someya, Takahashi, & Takahashi, 2001).
Social Workers
Social workers see few advantages to the DSM, though they value it as a tool for third-party billing (Frazer, Westhuis, Daley, & Phillips, 2009; Kutchins & Kirk, 1988; Newman, Dannenfelser, & Clemmons, 2007; Probst, 2012). They tend to differentiate diagnosis from the DSM, viewing the former as a way to comprehend client experience and the latter as a practical tool for labeling clients and billing (Probst, 2012).
Studying Counselors’ Attitudes Toward the DSM-5
Given how much controversy surrounded the DSM-5 revision process (Frances, 2013; Greenberg, 2013) and how few studies have been done on counselor attitudes toward the manual, we thought it timely to undertake a new survey of counselor attitudes toward the DSM. Our survey of counselors parallels the one we did with psychologists (Raskin & Gayle, 2016); in both surveys, many of the items were adopted from the earlier surveys conducted by Smith and Kraft (1983) and Miller et al. (1981). Just as Miller et al. (1981) did in relation to DSM-III 35 years ago, we collected our data immediately prior to the publication of the DSM-5 when interest in the manual among counselors and other health care professionals was high.
Method
Participants
One hundred and fifty-four anonymous counselors participated. Data from the 121 participants who completed at least 75% of the nondemographic survey items and were licensed in or reported a primary professional identification in counseling were analyzed. Of these, approximately 96% of the sample (n = 116) provided information regarding their primary professional identification, which included (clinical) mental health counseling (n = 101); counselor education and supervision (n = 6); marriage, couple, and family counseling (n = 3); career counseling (n = 1); school counseling (n = 1); student affairs and college counseling (n = 1); sex and gender counseling (n = 1); addictions counseling and supervision (n = 1); and rehabilitation counseling (n = 1). A summary of the remaining demographic data is provided in Table 1.
Summary Demographic Characteristics of Sample.
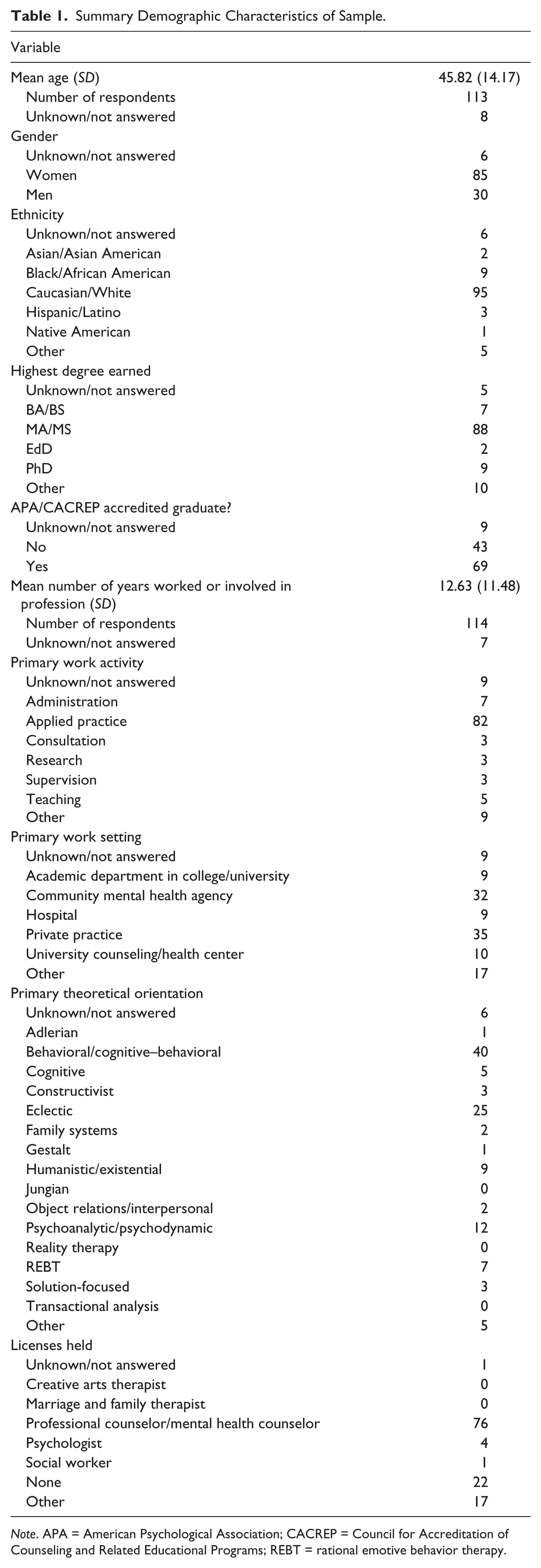
Note. APA = American Psychological Association; CACREP = Council for Accreditation of Counseling and Related Educational Programs; REBT = rational emotive behavior therapy.
Materials
The survey questionnaire was adapted from the one we used in our earlier study of psychologist attitudes toward the DSM (Raskin & Gayle, 2016). The adapted 50-item online survey was created to examine (a) current DSM-IV-TR usage patterns (3 items), (b) attitudes/beliefs about the DSM-IV-TR (3 items), (c) attitudes and beliefs about the DSM-5 (6 items), (d) attitudes about the DSM-IV-TR versus the proposed DSM-5 (13 items), (e) attitudes toward diagnosis and the development of a non-DSM diagnostic system (7 items), (f) general attitudes about diagnosis and the DSM (6 items), (g) demographic information (11 items), and (h) an optional final open-ended item for general comments. The survey utilized structured fill-in response, forced choice, multiple response, and Discrete Visual Analogue Scale (DVAS) items. All DVAS items were displayed as 15 evenly spaced horizontally oriented radio buttons that were sequentially labeled from left to right with consecutive integers from 1 to 15 placed above each button. Verbal labels were used as terminal anchors above the 5th and 11th radio buttons. For example, the following labeling scheme was used for several 15-point DVAS items: 1 (strongly support), 5 (support), 11 (oppose), 15 (strongly oppose). Consequently, scale labeling was symmetrical around the unlabeled scale midpoint (i.e., 8). This research project was institutional review board approved.
Procedure
Participants were recruited via an announcement posted to the Listserv of the New York Mental Health Counselors Association. They clicked a hyperlink that directed them to the survey. The survey was hosted and administered online using SurveyMonkey. Participants were informed that the survey was examining attitudes about diagnosis and the DSM. They were also informed that voluntarily answering survey items constituted consent. Participants were explicitly informed that they were not required to complete all survey items and that they could stop at any time. Data were collected from May 14 to June 22, 2012.
Results
We organized our analyses based on the six main categories the survey assessed (i.e., current DSM-IV-TR usage patterns, attitudes and beliefs about the DSM-IV-TR, attitudes and beliefs about the DSM-5, attitudes about the DSM-IV-TR versus the proposed DSM-5, attitudes toward diagnosis and the development of a non-DSM diagnostic system, and general attitudes about diagnosis and the DSM). In cases of unanswered items, the data point was excluded from the specific analysis. As such, across analyses sample sizes sometimes vary. For clarity, sample sizes are reported for each analysis. We treated nondemographic data obtained from forced choice and multiple response items as categorical-level measurement or frequency data and analyzed it using relevant nonparametric tests. DVAS survey items were treated as ordinal-level measurements and were also analyzed using nonparametric tests. Family-wise Type I error was controlled within each main category using the Holm–Bonferroni correction (Holm, 1979).
Use of DSM-IV-TR
Monthly Use
Using two separate structured fill-in response format items, participants were asked to approximate the number of times per month they relied on the DSM-IV-TR manual directly (e.g., for classifying clients and/or communicating their diagnosis) and indirectly (e.g., to form hypotheses or conceptualize a client). Counselors (n = 120) reported using the DSM-IV-TR directly approximately 10 times per month (M = 10.32, SD = 14.55) and indirectly approximately 14 times per month (M = 13.71, SD = 24.90), t(119) = 1.716, p = .089.
Reasons for Use
Participants were asked “Why do you use the DSM-IV-TR?” One multiple response item with 13 response options was provided and participants were instructed to select all that applied. Participants were also provided with an “other” option and were able to explain their reason. For the 121 counselors, “to help make a differential diagnosis” and “to help conceptualize a case” were reported as the two primary uses of the DSM-IV-TR with 66.1% of the sample selecting each of these reasons for use. Beyond these two reasons, from most to least frequently endorsed reasons, counselors selected “I find it useful” (60.3%), “required by third-party payers” (52.9%), “to help determine treatment” (43%), “because it is the only classification system presently available” (37.2%), “to help determine prognosis” (34.7%), “required by employer” (24.8%), “because of its validity” (19.8%), “because of its reliability” (19%), “because it is required by law” (16.5%), “other” (11.7%), “because psychiatrists use it” (9.1%), and “to aid in research” (6.6%).
Attitudes and Beliefs About DSM-IV-TR
General Satisfaction
Participants were asked “Overall, what best describes your attitude toward DSM-IV-TR?” Participants responded using a single 15-point DVAS item anchored at 1 (very unsatisfied) and 15 (very satisfied). Results of one-sample Wilcoxon signed-rank tests revealed that the counselors’ attitude toward the DSM-IV-TR (n = 121) was significantly more positive (Mdn = 10) than neutral (i.e., Mdn = 8), z = 4.418, p < .001.
Perceived Advantages
Participants were asked “Which do you see as advantages of the DSM-IV-TR?” One multiple response item with nine response options was provided and participants were instructed to select all that applied. Participants were also provided with an “other” option and were able to explain their reason. From most to least frequently endorsed advantages, counselors (n = 121) selected “helps identify pathology” (62%), “diagnostic codes” (55.4%), “diagnostic classification often leads to most appropriate treatment” (50.4%), “multiaxial approach” (48.8%), “has direct bearing on treatment” (33.1%), “is reliable” (28.1%), “is valid” (20.7%), “atheoretical stance regarding etiology of disorders” (20.7%), “strong scientific basis” (19.8%), and “other” (7.4%).
Perceived Disadvantages
Participants were asked “Which do you see as disadvantages of the DSM-IV-TR?” One multiple response item with nine response options was provided and participants were instructed to select all that applied. Participants were also provided with an “other” option and were able to explain their reason. From most to least frequently endorsed disadvantages, counselors (n = 121) selected “places more emphasis on diagnosis than treatment” (65.29%), “obscures individual differences” (60.33%), “labels distort one’s perception of a client” (52.06%), “applies medical labels to psychosocial problems” (42.98%), “places too much emphasis on pathology” (42.15%), “has little bearing on treatment” (22.31%), “diagnostic classification often leads to inappropriate treatment” (15.7%), “not reliable” (9.09%), “other” (9.09%), and “not valid” (8.26%).
Attitudes and Beliefs About DSM-5
Familiarity With Proposed Changes
Participants were asked “How familiar are you with proposed changes for the forthcoming DSM-5?” Participants responded using a single 15-point DVAS item anchored at 1 (very unfamiliar) and 15 (very familiar). The results of a one-sample Wilcoxon signed-rank test revealed that counselors’ familiarity with the proposed changes (n = 120, Mdn = 8) did not differ significantly from neutral, z = −0.766, p = .444.
Satisfaction With Proposed Changes
Participants were asked “How satisfied are you with the changes being proposed for DSM-5?” Participants responded using a single 15-point DVAS item anchored at 1 (very unsatisfied) and 15 (very satisfied). The results of a one-sample Wilcoxon signed-rank test revealed that counselors’ satisfaction with the proposed DSM-5 revision (n = 109, Mdn = 8) was significantly more negative than neutral, z = −2.337, p = .019.
Intention to Use DSM-5
Participants were asked “Do you expect to use DSM-5 when it is published?” and responded using a yes/no forced choice. Over 98% of our sample (n = 119) responded to this item. Despite the tendency toward dissatisfaction, approximately 97.5% of the respondents (n = 116) reported an intention to use the DSM-5 on its publication.
Reasons for Use
Participants were asked “Why do you expect to use the DSM-5?” One multiple response item with 13 response options was provided and participants were instructed to select all that applied. Participants were also provided with an “other” option and were able to explain their reason. For the 121 counselors, “required by third-party payers” (60.33%), “for help with differential diagnosis” (59.5%), and “to help conceptualize a case” (53.72%) were reported as the three primary uses of the DSM-5. Beyond these three reasons, from most to least frequently endorsed reasons, counselors selected “I find it useful” (43.8%), “to help determine treatment” (38.84%), “to help arrive at a prognosis” (33.88%), “because it is the only classification system presently available” (33.05%), “required by employer” (24.79%), “because it is required by law” (14.05%), “because of its validity” (14.05%), “because of its reliability” (14.05%), “to aid in research” (10.74%), “because psychiatrists use it” (7.44%), and “other” (5.79%).
Effect on Diagnosis
Participants were asked “In your professional opinion, what will be the most likely effect on diagnosis of implementing DSM-5?” Participants responded using a single 15-point DVAS item anchored at 1 (significantly improve) and 15 (significantly hinder). Results of one-sample Wilcoxon signed-rank tests revealed that the counselors predicted that DSM-5 would improve diagnosis (n = 104, Mdn = 7), z = −3.841, p < .001.
Effect on Clinicians
Participants were asked “How you think DSM-5 will affect counselors?” Participants responded using a single 15-point DVAS item anchored at 1 (significantly harm) and 15 (significantly benefit). Results of one-sample Wilcoxon signed-rank tests revealed that counselors predicted that the DSM-5 implementation would significantly benefit their profession (n = 106, Mdn = 9), z = 3.974, p < .001.
Comparing DSM-5 With DSM-IV-TR
Based on their familiarity with the proposed changes in the DSM-5, participants were instructed to compare the DSM-5 with the DSM-IV-TR on 13 individual DVAS items, each using a 15-point scale anchored at 1 (much worse) and 15 (much better). Results of one-sample Wilcoxon signed-rank tests revealed that counselors expected the DSM-5 to be significantly better than the DSM-IV-TR regarding the “multiaxial approach” (n = 82, Mdn = 8.5, z = 3.897, p < .001); “reflection of current scientific knowledge” (n = 83, Mdn = 9, z = 3.434, p = .001); and “information supported by empirical data” (n = 80, Mdn = 8, z = 3.027, p = .002. See Table 2 for results of analyses of all 13 items that compared the DSM-5 with the DSM-IV-TR.
Sample Size, Median, and Results of One-Sample Wilcoxon Signed-Ranks Tests for Comparison of DSM-5 With DSM-IV-TR and General Attitudes About Diagnosis and DSM.
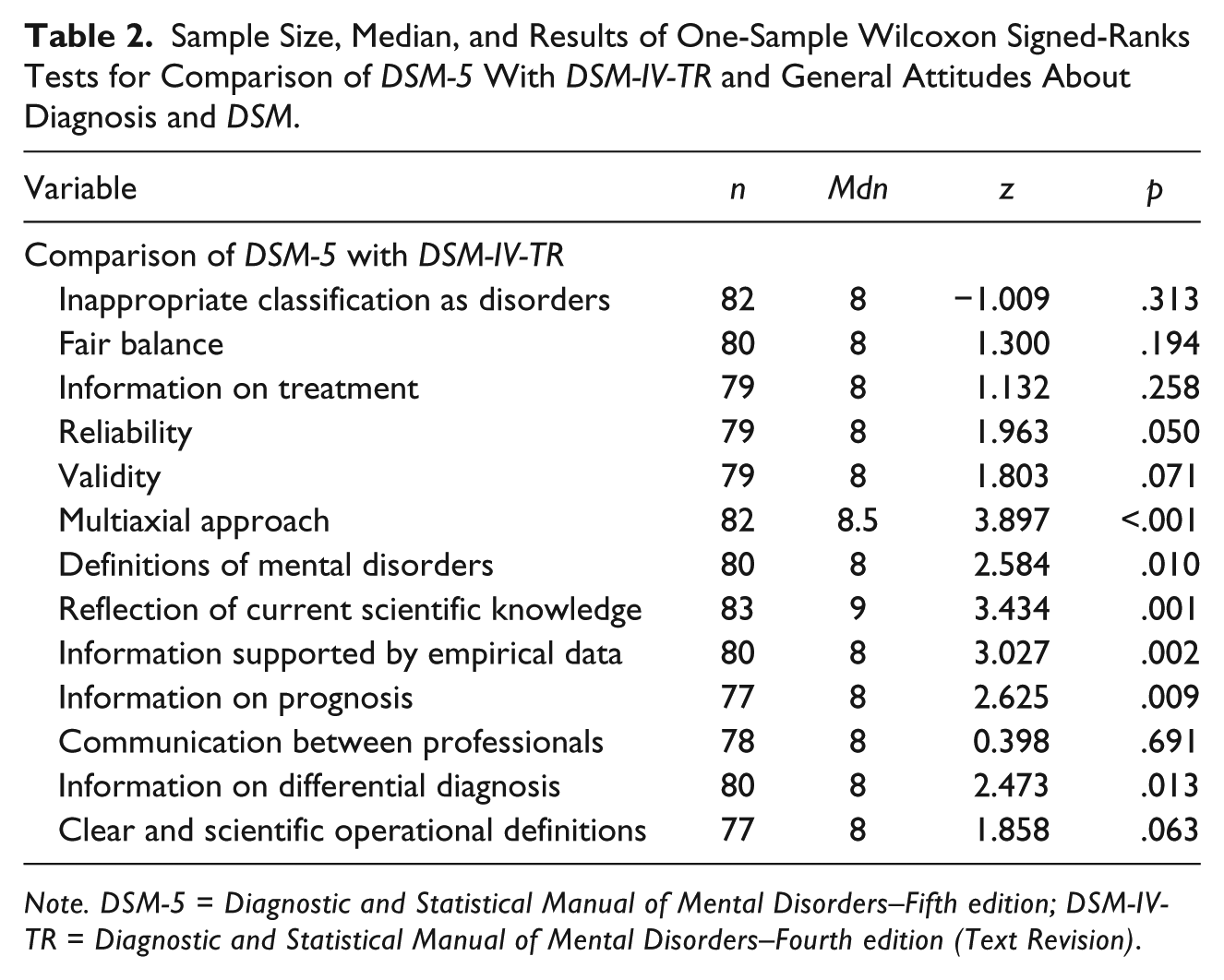
Note. DSM-5 = Diagnostic and Statistical Manual of Mental Disorders–Fifth edition; DSM-IV-TR = Diagnostic and Statistical Manual of Mental Disorders–Fourth edition (Text Revision).
Attitudes and Beliefs Regarding Development of an Alternative Diagnostic System
Interest in Alternatives
Participants were asked “Would you support seeing an alternative diagnostic system to the DSM developed?” Participants reported their degree of support using a single 15-point DVAS item anchored at 1 (strongly support) and 15 (strongly oppose). A one-sample Wilcoxon signed-rank test found that participants were supportive of the development of an alternative diagnostic system (n = 117, Mdn = 5, z = −5.637, p < .001).
Types of Alternatives Preferred
To examine the types of approaches participants would support in the development of an alternate, non-DSM diagnostic system, participants were instructed to rate their degree of support of six individual DVAS items, each using a 15-point scale anchored at 1 (strongly support) and 15 (strongly oppose). Rather than reporting neutrality (i.e., Mdn = 8), one-sample Wilcoxon signed-rank tests revealed that participants supported the development and use of “social–interpersonal diagnosis” (n = 107, Mdn = 5, z = −7.880, p < .001); “mapping developmental and personal meanings” (n = 103, Mdn = 5, z = −7.228, p < .001); “behavioral analysis” (n = 104, Mdn = 5, z = −7.514, p < .001); “assessment of faulty beliefs/cognitions” (n = 103, Mdn = 5, z = −7.298, p < .001); and “nondiagnosis” (n = 96, Mdn = 6.5, z = −2.359, p = .018). The final item used to examine the types of approaches participants would support in the development of an alternate, non-DSM diagnostic system was “none of the above, prefer the DSM instead.” In hindsight, we judged this item as poorly worded and, because it was double-barreled, determined that the findings could not be clearly interpreted. Nevertheless, as a group, participant responses to this item did not differ from neutral (n = 51, Mdn = 8, z = −0.128, p = .898).
General Attitudes About Diagnosis and the DSM
To examine participant beliefs and attitudes regarding diagnosis and the influence of the DSM, participants were instructed to rate their level of agreement to six individual DVAS items each using a 15-point scale anchored at 1 (strongly disagree) and 15 (strongly agree). Results of one-sample Wilcoxon signed-rank tests revealed that participants agreed that “too little has been done to promote a scientific alternative to the DSM” (n = 113, Mdn = 10, z = 3.827, p < .001) and disagreed that “mental disorders are a subset of medical disorders” (n = 115, Mdn = 5, z = −5.320, p < .001). There was a trend toward disagreement that “counselors have lost their autonomy because of widespread use of the DSM” (n = 112, Mdn = 7, z = −2.491, p = .013). However, due to family-wise error correction, this finding was not statistically significant. Participant attitudes did not differ from neutral on the remaining three items (i.e., “DSM relies too heavily on medical semantics,” n = 112, Mdn = 8, z = 0.825, p = .409; “client’s welfare would be better served by abandoning the medical model in training and practice,” n = 114, Mdn = 7, z = −0.581, p = .561; and “most conditions that DSM labels as mental disorders can best be described as nonmedical problems in living,” n = 113, Mdn = 8, z = 0.151, p = .880).
Discussion
General Attitudes Toward the DSM
Mixed Attitudes, Widespread Use
Counselors expressed mixed attitudes toward the DSM, holding views that at times seemed contradictory. They were satisfied with the DSM-IV-TR and thought the DSM-5 would improve diagnosis and benefit their profession—yet at the same time, they were dissatisfied with the proposed DSM-5 revisions. It is difficult to reconcile these seemingly incompatible views. What especially stood out was that despite mixed attitudes toward the DSM-5, almost 98% of counselors intended to use it.
Advantages and Disadvantages
The DSM’s ability to help identify pathology and its assistance in helping counselors choose the most appropriate treatment were ranked highly as advantages. More practically, counselors saw the DSM’s provision of diagnostic codes as beneficial, which makes sense given its central role in their collecting health insurance reimbursements. Another advantage counselors liked about the DSM was the multiaxial approach to diagnosis—an interesting finding given that multiaxial diagnosis has been removed from the DSM-5. As for disadvantages, counselors worried that the DSM overemphasizes diagnosis at the expense of treatment and obscures individual differences, while also expressing the view that labeling distorts understanding clients. Counselors expressed a mixed view of the DSM, liking its ability to discern pathology in a manner that helps determine treatment while simultaneously showing concern that too much emphasis on diagnosis potentially detracts from treatment. Once again, these conflicting attitudes are difficult to reconcile and suggest that, at the very least, counselors are ambivalent about aspects of the DSM.
Attrition
Approximately 33% of the counselors surveyed did not complete items asking them to compare DSM-IV-TR and DSM-5. It is not clear why these items were left out or whether those who did not answer them differed from those who did. High-attrition rates for these items may have influenced the results. Response rates to the rest of the survey were consistently high.
Development of Alternatives to the DSM
Support for Alternatives
Despite believing that the DSM-5 would be scientifically better than the DSM-IV-TR and would benefit their profession, counselors nonetheless supported developing alternatives to it. Four alternative approaches to diagnosis were asked about—social interpersonal diagnosis, behavioral analysis, assessment of faulty beliefs and cognitions, and mapping developmental and personal meanings. Counselors favored developing all of them. They also favored nondiagnosis. Despite seeing the DSM-5 as improved and as beneficial to treatment and to the counseling profession, counselors still see not using diagnosis as a viable option. In this way, they differ from psychologists, who support developing alternative diagnostic approaches, but are not supportive of nondiagnosis (Raskin & Gayle, 2016).
Counselors Versus Psychologists
Both Have Concerns, Support Alternatives
The present study on counselors’ attitudes toward the DSM asked the same questions as our previously published study of psychologists’ attitudes (Raskin & Gayle, 2016). In comparing results from the two studies, there were many commonalities: both psychologists and counselors had concerns about the DSM-5 revision process and both supported developing alternative, non-DSM types of diagnosis—with counselors even expressing support for forgoing diagnosis all together, something psychologists did not support.
Counselors More Positive
It was the differences between counselors and psychologists that most surprised us. Overall, counselors had a positive view of the DSM, while psychologists had a generally negative view. For instance, counselors rated the DSM-IV-TR positively, while psychologists did not. Counselors were also positive about proposed DSM-5 changes—even feeling it would benefit their profession; psychologists were negative about DSM-5 changes and neutral about its potential to benefit their profession. Finally, when asked about the effect of the DSM-5 on diagnosis, counselors indicated that DSM-5 would better reflect scientific knowledge and be better rooted in empirical data, while psychologists worried that DSM-5 would inappropriately classify some behaviors as disorders.
Why the Differences?
What accounts for the tendency of counselors to feel more positive about the DSM than psychologists? Comparing results across both studies reveals that psychologists used the DSM-IV-TR more than counselors to aid in research, whereas counselors used it more than psychologists to make prognoses. This could have made psychologists more aware of the DSM’s scientific limitations than those using it exclusively in practice. At the same time, counseling is an emerging profession, only recently licensed in a number of large states such as New York and California—something worth noting given that participants in this study were recruited through the New York Mental Health Counselors Association. Newly licensed counselors collecting insurance reimbursements for the first time might be especially attuned to the DSM-5 as an important development critical to enhancing their profession’s visibility and improving its economic potential.
Conclusion
Counselors show mixed attitudes toward the DSM. They rate it positively and believe it can be helpful in making diagnoses and conceptualizing cases. They like its inclusion of diagnostic codes (which they can use to get paid) and see the DSM-5 as beneficial to their profession. At the same time, counselors express attitudes consistent with counselor education’s historic emphasis on wellness rather than pathology (Remley & Herlihy, 2014). They worry that DSM diagnosis can overshadow treatment, distort perceptions of clients, and lead to stigmatizing labeling. They also support developing alternatives to diagnosis—even nondiagnosis, which psychologists do not (Raskin & Gayle, 2016).
Counselors’ mixed attitudes might reflect the various pressures the counseling profession currently faces. One way that counseling has established its identity as an emerging profession distinct from psychology and other mental health professions has been by successfully advocating for mental health counseling licensure throughout the United States, which makes licensed counselors capable of diagnosing and treating mental disorders. Doing so has resulted in counselors having to utilize DSM diagnosis. In some respects, this marks a shift away from counseling’s traditional emphasis on wellness (Remley & Herlihy, 2014) toward a more pathology-oriented approach.
The results of the current survey may reflect the impact of this shift. On the one hand, counselors see the DSM-5 as benefitting their profession because they are increasingly using it in professional settings and getting paid by insurers as a result. In these settings, the DSM is helping counselors to make diagnoses and plan treatment, with the general feeling among counselors being that the recent DSM-5 marks the latest, most improved and scientifically up-to-date version of the manual. At the same time, counselors remain committed to the wellness approach they have long practiced. Thus, they worry that DSM diagnosis has a number of drawbacks. This potentially explains why counselors support developing alternative diagnostic systems and see nondiagnosis as a viable option in many counseling settings.
Future research should look at how counselor attitudes toward the DSM-5 are evolving as the manual becomes more familiar and more integrated into professional practice. Given counselors’ mixed attitudes, future research might also examine how counselors balance the wellness-focused assumptions of their profession with the more pathology-oriented DSM-5 system. Finally, future research might explore the extent to which counselors would be willing and practically able to incorporate non-DSM diagnostic alternatives into their professional practice. After all, the only way this is likely to happen is if it can be done in a manner that counselors feel benefits their profession as much or more than DSM diagnosis does. Regardless, diagnosis in general—and the DSM in particular—will likely continue to play a significant role in counselors’ work lives. Therefore, tracking counselors’ changing attitudes toward the DSM is an important area of inquiry that warrants continued attention as both the DSM and the counseling profession evolve over time.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
![]() .
.