
Abstract
Although many successful Community Advisory Boards (CABs) are discussed in the literature, some articles report that community members feel they are treated as token participants, or that their voices are not heard. This article describes the initial steps we took in designing an effective and empowered CAB, the underlying group dynamics principles we employed to formulate this CAB, and the structure and processes we instituted. We focused on how to build decision-making procedures that support and enhance the group’s function and effectiveness over the long term. Additionally, we considered how we might intervene when these features become out of balance. Though the literature on CABs often talks about power dynamics, explanations of what is meant by this label are rare. We resolved to explore these dynamics and to design a CAB that would operate successfully in full recognition of power dynamics.
Keywords
Introduction
As part of a nationwide transition toward greater Veteran-centeredness, Veteran and community involvement have become priorities of the Veterans Health Administration (VA), of which research is an important exemplifier (Department of Veteran Affairs, 2019). Although many successful Community Advisory Boards (CABs) are discussed in the literature (Chhatre et al., 2017; Cramer et al., 2018; Frye, et al., 2015; Israel et al., 2001; Morin et al., 2003; Newman et al., 2011; Pinto et al., 2011; Walsh et al., 2011; Young et al., 2019), some articles report that community members feel they are treated as token participants, or that their voices are not heard (Hahn et al., 2017; Ocloo & Matthews, 2016; Pinto et al., 2013; Safo et al., 2016). Like other centers of its size around the country, our center, the VA Center for Health Equity Research and Promotion (CHERP) at the Cpl. Michael J. Crescenz VA Medical Center in Philadelphia (CMCVAMC) elected to create its own CAB to facilitate Veteran input to the design of research studies. However, our Center sought to avoid the above pitfalls by providing us, the authors, with latitude in the design and implementation of an effective, empowered CAB. This article describes the initial steps we took in designing the CAB, the structure and processes we instituted, and the underlying group dynamics principles we employed.
Along with the Civil Rights Movement of the 1960s (Foner, 2016), the growth of the practice of community organizing (Fisher & Defilippis, 2015), and the development of qualitative research (Wertz, 2014) humanistic psychology contributed to the foundational principles and knowledge on which we have built our understanding of how to create and support a CAB. Our work, which takes systemic issues into account, recognizes power dynamics and confronts issues of dependency, owes a great debt to the work of humanistic psychologists over the years. In fact, our determination to avoid the pitfall of tokenism is based on principles clearly articulated by humanistic psychologists in the 1950s and 1960s (DeCarvalho, 1990). More recently, recognition of systemic forces and power dynamics spurred development of empowerment practices (Diaz-Liplante, 2007) and an examination of how to avoid tokenism (Daya et al., 2020; Hoffman, 2012). In addition, by stressing the importance of human agency and responsibility (Bugental, 1967) humanistic psychologists helped build our understanding of autonomy and how to sustain it over time. Moreover, humanistic psychologists focused on the importance of human experience (Bugental, 1967, 1965/1981), emphasized listening (Rogers, 1961, 1951/1965), and made a point of empowering those usually denied a voice (Moustakas, 1959, 1994). These are the basic principles on which we base our work.
Our first step was to determine a formation strategy that specifically addressed how we could avoid common pitfalls, such as patients’ distrust of researchers (Nyden & Wiewel, 1992). From these considerations, we identified three important points: (a) the expectations of the institution or center forming the CAB are often not congruent with what the CAB will require to operate effectively; (b) in ways that overlap with confused expectations, CABs are often not granted the authority or autonomy that they need to have an impact; and (c) the power dynamics between CAB members and principal investigators (PIs), although often named, remain unexplored. Unless these concerns were properly grounded in CAB formation, empowering the CAB to persuade PIs to address the equity needs of vulnerable and marginalized Veteran communities would be jeopardized. Importantly, our decisions were informed by the unique mind-set of Veterans, a perspective based on the group-centered culture of our military.
Initially, we began by seeking out expertise from other CAB coordinators in the Philadelphia area. Next, we convened focus groups composed of both Veterans and researchers to dialogue about expectations, observe interactions, and model what we wanted to achieve. The subjects and questions raised in the focus groups convinced us that we would not be able to detect Veteran-centered changes in CHERP’s research portfolio unless Veterans were engaged in a fashion that we could measure in years. To ensure that CAB members remain motivated to continue long-term engagement with the VA research community, and to establish interpersonal, group and organizational relationships, we focused on how to build decision-making processes that support and enhance the group’s function and effectiveness over the long term. Additionally, we considered how we might intervene when these features become out of balance.
The systems and group literature in organizational dynamics (Ackoff, 1999; Hackman, 1998, 2004; Hackman & Wageman, 2005) emphasizes that in order for a new group, team, task force, department, and so on, to be effective, the context in which the group is embedded needs to be clarified. Thus, in forming the CAB our earliest questions centered on: (a) What motivation is propelling CHERP to develop a CAB? (b) How will the CAB function in relation to CHERP and the larger VA Research institution in which it is embedded? and (c) How do we ensure CAB survival in the larger VA Research milieu?
CHERP’S Motivations
Engaging patients means that they are actively involved in defining and realizing their health-related goals (Wendleton et al., 2019). As a nontraditional component of the research process, patient engagement can be disruptive to traditional patient deference to clinician–researcher authority (Wendleton et al., 2019). Thus, we understood from the outset that an effective CAB was one that would likely disturb the status quo. This factor had implications for the design of the CAB, as organizations often squash efforts that disrupt the usual ways of operating (Argyris, 1976; Edwards & Saltman, 2017).
For CHERP, the CAB was a response to an environment of increased demand for translation of research into practice (Barkin et al., 2013). At the same time, Congressional legislation presented another set of directives. The Veteran’s CHOICE and MISSION Acts (Frakt & Pizer, 2016; Garrido & Pizer, 2019; Kirsh, 2019) introduced imperatives to shorten the timeframe from research publication to clinical application, requiring stakeholder engagement, of which Veterans are an important subgroup. In addition, Veterans Affairs Medical Centers across the country were promoting community engagement (Wendleton et al., 2019), leading to the formation of the nation-wide Community Veteran Engagement Board model to develop and disseminate this work (Veterans Experience Office, 2019). With the arrival of the Patient Centered Outcomes Research Institute on the scene, there was increased spotlight nationwide on patient voices in all stages of the research process (Forsythe et al., 2019).
In June of 2016, a CAB was featured as a component of a CHERP VA Merit Review proposal on the subject of HIV (Gross, 2016). Coincidentally, the then Co-Director of CHERP was also considering how best to include Veteran and community perspectives in CHERP’s multifaceted Health Equity research portfolio. The Co-Director conveyed to staff his view that patient perspectives needed to be included in CHERP’s studies, especially in its research development.
Organizational Context in Which the CAB Would Be Operating
Once we had a better grasp on what was motivating CHERP to develop a CAB, we turned our attention to examining details of the organizational context in which the CAB would operate. We learned about the structure of VA Research administration; we initiated relationships with facility leaders and other stakeholders with an interest in VA health care quality; and we refined our understanding of what Veterans value in their care. From the people we talked to and the literature we read, CABs created merely to satisfy an eligibility requirement or to make a research entity appear to be innovative, were unlikely to be successful (Safo et al., 2016). As we will describe below, to avoid “check-box” CABs such as these, we worked hard to set clear expectations about what the CAB would and could do.
From our discussions and literature review, we identified some key factors that we thought could potentially derail the establishment of an effective CAB. We discussed with leadership some of the ways that the CAB might disrupt business-as-usual in order to test their commitment. We extended invitations to facility leaders to attend CAB meetings for conversations about issues and questions they felt the CAB could help them address (such as Veteran employee concerns, recruitment for studies, justice-involved Veterans, clinical programs, etc.).
Designing a CAB That Could Survive
From our understanding of organizational and group dynamics we knew that power dynamics are central to the operation of a CAB. Although the literature on CABs often talks about power dynamics, it rarely explains what is meant by this label (Becker et al., 2013; Chung, & Lounsbury, 2006; Newman et al., 2011; Safo et al., 2016). Power dynamics that are relevant to a CAB’s functioning involve the differences in power and status between the patients/Veterans and PIs. We resolved to explore these dynamics and to design a CAB that would operate in full recognition of these power differences. Honesty about who in the organization has decision-making power, when decisions have been made, and whether additional input will change a decision is instrumental in determining CAB power (Talley, 2019). Often in organizations, groups and teams are formed to address specific problems without the authority to deal with the issues they uncover (Hackman, 1998, 2004; Hackman & Wageman, 2005), leaving the group with the feeling that their work is futile. Together, we considered the following issues: (a) who authorized the CAB and what the boundaries of this authorization were; (b) PIs typically possess more authority than patients, and how the CAB can navigate this disparity; and (c) how our own authority was to be designated and implemented.
Early CAB Design Considerations: Shifting Expectations
Unless the CAB was clearly authorized, and expectations transparently defined, it was likely to be ineffective when confronted with the authority of other leaders in the VA research community. Not only did the Co-Director of the Center have the authority to form a CAB, but sensing a change in the overall VA research complex, he used his authority and autonomy to steer CHERP toward greater Veteran-centeredness and patient involvement in a transparent fashion. In response, we enshrined the Co-Director’s authority in a memo of understanding with the CMCVAMC (Hyde et al., 2018), which outlined the specific areas where CAB input would be utilized in CHERP’s research. This ensured that all signatories in significant positions of authority in the system had full knowledge of and formally agreed with the authority structure we intended to erect.
Additionally, the Co-Director and other senior leaders attended the first three meetings of the CAB to introduce themselves to the members, and to listen as they clearly stated their expectations and hopes for the CAB. These steps memorialized the authority, autonomy, and expectations of the CAB as well as its interrelationship with CHERP and CMCVAMC leadership.
We anticipated that the CAB would have to make consequential decisions about how to organize itself, how to run its meetings, how to form subcommittees to address specific issues, and, most important, how to interact with PIs. Therefore, we considered social and administrative processes related to authority that were likely to support and enhance the group’s function and effectiveness.
When group or organizational boundaries are unclear or are transgressed without consequences, the group or organization’s functioning can be undermined (Green & Molenkamp, 2005). One aspect of defining boundaries is stating expectations clearly. Consequently, defining and agreeing on the expectations about a group’s boundaries should not be taken for granted, especially as new boundaries are formed as a result of CAB activities. Furthermore, openly and systematically sharing expectations—even periodically revisiting expectations—with all participating groups and leaders facilitates the establishment of goals, objectives and structure, as well as transparency and trust-building across the system. When expectations or established boundaries are disrespected, expressions of futility are likely to result from all stakeholders no matter their position in the system (i.e., “What’s the use of doing this?”). If unaddressed, this situation will precipitate distrust, feelings of being unproductive, and a hardening of the system’s structural encasements (Smith, 1982). Persons at every system level may begin to use stereotypes, may refrain from listening to other perspectives, and may even use their authority to thwart activities of groups at other levels of the system (Oshry, 1995, 1999).
Empowering those who have formerly been passive in an organization involves a shift in expectations. We hoped—rather than assumed—that PIs and leaders at CHERP and at the VA would see the CAB as an enhancement to their work. At the same time, we anticipated that an empowered CAB would be disruptive, but in a positive way. Therefore, we stressed that the CAB would likely slow the research process down and raise questions that would make some PIs uncomfortable. We noted that some researchers might be discomfited with merely seeking Veteran feedback about their research. We raised these expectations in the hope that, when conflicts and disagreements arose, CHERP’s leadership would support the CAB and its members. Nevertheless, we were not naïve enough to believe that engaging Veterans in the research process would not disturb some PIs.
In order to build trust in the CAB among its Veteran members, CHERP’s leadership also committed to being as transparent as possible. In our early briefings with CAB members, we sought to help them understand CHERP’s mission and goals, and to orient them as to their role in the center. At the same time, we solicited feedback regarding specific points where CHERP’s engagement philosophy and strategy needed revision, such as tactics to disseminate information about CHERP’s successes to the Veteran community. Trust is most likely to be broken when group members experience a department or organization being less than honest about how the group’s input will be used, the ways in which the group’s role fits into the larger organization, or potential future difficulties (Becker et al., 2013; Keddem et al., 2017).
Another expectation which CHERP leadership expressed, and which we highlighted with the CAB, was that evaluation of the members’ activities should be measured in years, not months. In order for PIs to integrate Veteran voices into their research in a systematic fashion, it would take time to build trust, as well as for PIs to understand the value that a Veteran perspective could bring.
Focus Groups With Veterans and PIs
Early on it became clear to us that we could not design a CAB without input from those people who might eventually be members of the CAB or who would seek its input. Since our goal was to include Veteran voices in the research process, it would have been antithetical to our philosophy and ethics to exclude Veteran voices in the design phase. In addition, as researchers, it was natural to us to perform some background investigation in order to refine the design of the board. We decided to convene two focus groups in which Veterans receiving care at our facility would come together as equals with CHERP’s PIs to discuss the formation. Running focus groups also allowed us to model the inclusive listening to participants that we hoped the CAB would adopt. We selected researcher participants who had experience with community driven research, as this group would be more likely to value community perspective. Similarly, Veterans were recommended to us by clinicians on account of their willingness to discuss their care in an open and assertive manner. Holding the focus groups with Veterans and PIs allowed us to observe interactions between the groups, and to test what we hoped to achieve with the CAB, that is, a path where researchers’ as well as Veterans’ views would have influence in the kinds of research undertaken by CHERP.
From the focus groups, we learned that the development of a common vocabulary, aiding both Veterans and PIs in understanding each other, would not only facilitate communication but would also build trust (Schulz et al., 2003). Diversity among CAB members was also raised in the focus group conversation, though it was also pointed out that the group should be capable of working together toward a common goal. The ability to raise difficult or controversial issues without judgment was also highlighted. There was agreement that selection criteria should be established for CAB membership, and that members should be oriented toward service and helping CHERP’s work, rather than any personal benefit. Finally, in a manner that mirrors the institutional challenges of communicating with diverse groups of Veterans, the point was made that when communicating and disseminating information, communication needs to go out over multiple channels (web, hardcopy, telephone, etc.) to accommodate those who are not internet savvy. Notably, all the Veterans who attended the focus groups were interested in being members of the CAB.
Early Decisions: Creating an All-Veteran CAB
Although many CABs include members who are PIs and staff of the research center (Cramer et al., 2018; Pinto et al., 2011), to foster solidarity and social cohesion in the group, we decided to make the CAB membership exclusively Veteran. Additionally, during the focus group a Veteran recommended that CAB membership be open also to spouses or caregivers of Veterans. When the CAB met to design its bylaws, this category of member was included. We believed that by restricting the CAB to Veterans and spouses/caregivers, the resulting enhanced cohesion would: (a) help group members experience their own agency, which is more likely to occur when everyone in the group has the same status and power; (b) strengthen the CAB’s ability to challenge power differences between patients and PIs; and (c) enable the entire CAB to confront the PIs’ greater expertise, and reduce the tendency of PIs to dominate conversations about research (Newman et al., 2011). This sense of group purpose, unique to Veterans, mirrors Veterans’ military experience: training, deployment, and demobilization occur in the context of the group (Shay, 1994; R. T. Smith & True 2014). We hoped to avoid the splintering into factions we had witnessed with other advisory boards and committees that included patients and PIs, with the PIs holding the upper hand and the patients’ voices being sidelined (Hahn et al., 2017; Newman et al., 2011; Ocloo & Matthews, 2016; Pinto et al., 2013; Safo et al., 2016).
Based on other CAB models, we decided that the CAB would have a Chair and Vice-Chair, enabling a team-based approach to leadership responsibilities and decision making deepened by the different but overlapping roles, knowledge, and skills the joint leaders possess. Our selection criteria for these posts were that the candidate should have prior community engagement experience, clear grasp of research principles, and extensive connection to the Veteran community at large. The Chair we chose had lengthy experience in leading health-related CABs, while the Vice-Chair was well-versed in the opinions of Veterans who get their care at VA. This representative structure ensured that the CAB would be led by Veterans.
After we selected the Chair and Vice-Chair, they assumed direction over the selection of the other members of the CAB. For budgetary reasons, the CAB could support up to 15 members. Although we were present during the interviews, and we contributed our views and impressions of each candidate as representatives of CHERP, the Chair and Vice-Chair made the final decisions about who was to be invited to be a member. During this selection process, we consciously took a backseat role. This decision was unusual, as research center staff and PIs often make all initial decisions about CAB formation, including membership (Pinto et al., 2011; Wendleton et al., 2019). Our goal was to begin to shift the authority and autonomy for directing the CAB to its members and leaders. This first iteration of the CAB was composed of 11 members.
Drafting the CAB Mission Statement and Bylaws
We believed having Center staff and/or PIs set the direction, mission and bylaws of the CAB would deprive the members of authority and autonomy. An approach such as this may lead to lackluster engagement from participants at best, to at worst participants drifting away in favor of other obligations.
The first test came when the CAB needed its name and mission statement to align with the mission of CHERP, yet also express the CAB’s unique identity and goals (Pinto et al., 2011; Wendleton et al., 2019). The CAB expeditiously decided on a name and a clear mission statement in less than a half hour. For the task of developing bylaws, the CAB decided to form a small subcommittee to draft bylaws attuned to their circumstances (Wendleton et al., 2019). The efficiency and effectiveness of drafting these documents was in our estimation due to the fact that members had the authority and cohesiveness to determine the direction of the CAB within its predetermined limits.
Giving the CAB the authority to create their mission statement and bylaws we believed would contribute to the future empowerment of the CAB and would improve their competency in working on complex tasks as a team. We were also aware that there were risks with creating a CAB empowered to do so. For example, it was possible that the CAB would go off in directions not within the purview of CHERP, or that CAB members would interpret attempts to influence its approach or decisions as invasive. We reasoned that these risks were worth taking given our commitment to listening to the voices of Veterans even if it created some tension, discomfort, or disagreement. The literature reports that some CAB members feel they are brought in as an afterthought, rather than as valued collaborators (Pinto et al., 2013). It seems very likely that these perceptions will arise when CABs are not given the authority to determine their own future within an established framework and expectations (Israel et al., 2001; Safo et al., 2016).
Early in the formation of the CAB, we realized that the Community Engagement Continuum (Clinical and Translational Science Awards Consortium, 2011) as a conceptual framework would give the CAB a broad range of options regarding its activities. The Community Engagement Continuum specifies a number of different ways for a community to be involved in research (i.e., Outreach/Consult/Involve/Collaborate/Shared Leadership; Figure 1).
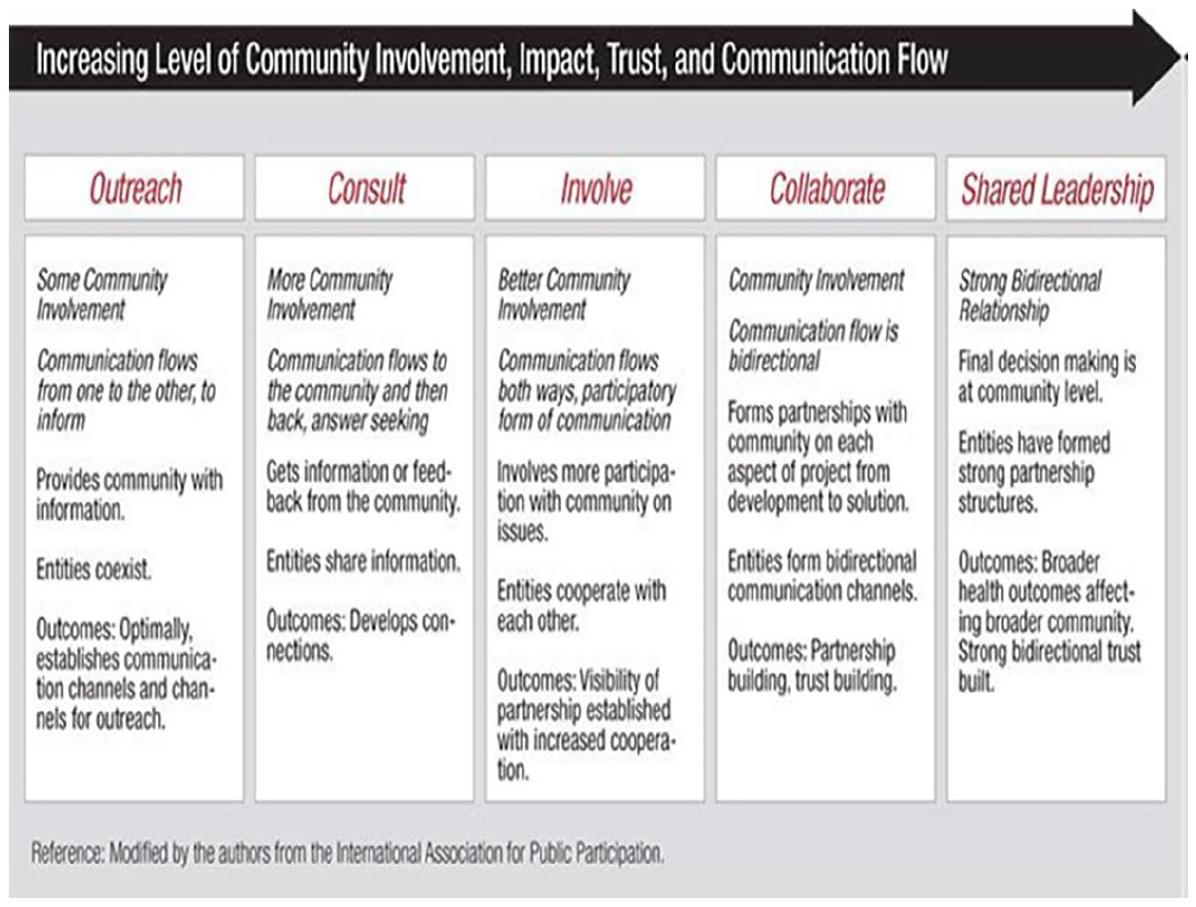
Different Levels of Community Engagement.
The literature on CABs indicates that most are involved at the level of “Consult” (Joosten et al., 2015). This means that PIs come to a CAB with specific questions in mind, answer-seeking typically about recruitment, the wording of surveys, or simplistic patient experience data. This interaction is a one-way, passive encounter in which little institutional status or power is necessary or achieved. We envisioned that an empowered CAB might want to not only Consult but also “Collaborate” or “Share Leadership” with PIs in ways that enhance the engagement in the research process and its results.
Moreover, we realized that if the CAB saw different levels of involvement as possible from the start, it was more likely to develop the agency to take advantage of these options in a fashion that would be transparent to all stakeholders (i.e., setting expectations). We recommended that PIs deeply consider the Continuum before they came to a CAB meeting to discuss their research. This suggestion provided clear expectations and terminology to both the CAB and PIs about the specific level of engagement.
Using the Continuum to set expectations for the CAB and for PIs signaled to both groups that the CAB was authorized and could flex to work with PIs in a number of ways at a variety of intensity levels (Chung, & Lounsbury, 2006). Some of the levels, such as Collaborate and Shared Leadership, indicated complicated ways of working with PIs, crossing traditional boundaries that previously limited the way CAB members were seen and treated. Other levels, such as Outreach, comprise the one-sided communication of information that has defined engagement with patients for decades. This is not to say the Outreach level and associated techniques are not appropriate at times. What is important to note is that the Continuum depicts the ways in which a CAB may be flexible according to its circumstances. Using the Continuum also made it clear to PIs and CAB members that this was not a token endeavor, and that CHERP was committed to involving Veterans in research that was meaningful, and potentially game changing.
Stabilizing the Relationship Between CAB and PIs
From reading the literature and from previous experience, it was clear to us that stable relationships between the CAB and PIs were crucial to the success of the CAB. An atmosphere in which PIs treated the CAB in as an afterthought or as another bureaucratic hurdle would doom the CAB from the start. Equally problematic was a relationship where CAB members treated PIs as superior or as the enemy (Nyden & Wiewel, 1992). We therefore spent a lot of time during the group’s formation working out ways to instill collaboration and equality between the CAB and PIs. It is to facilitate these relationships that many CABs have research center PIs and staff serving as members (Pinto et al., 2011), but it was our early assessment that this configuration sidestepped the difficult issue of how these two groups with very different forms of power and status would learn to work together. We also reasoned that if PIs were members of the CAB, they might dominate the discussions—even unwittingly—because of their training and knowledge, resulting in a muting of CAB members’ voices and ideas.
Power Dynamics
The literature on CABs often raises the issue of unequal power dynamics, but rarely discusses it in any depth (Becker et al., 2013). We began with the premise that there was an unequal distribution of power (Becker et al., 2013; Newman et al., 2011; Safo et al., 2016), status and resources between PIs and CAB members. CAB members would be asked to provide feedback to PIs about research in which PIs had a very substantial “home court advantage.” Moreover, in addition to PIs’ training and experience in conducting medical research, they also hold status and power in the VAMC system which Veterans do not have. Although we have heard many PIs proclaim, in effect, “We are all equal,” hidden power dynamics influence relationships and are often ignored in relationships of unequal status and power (Mansbridge, 1973). Only by recognizing and acknowledging these differences could we hope to navigate them in a way which does not undermine the CAB authority and autonomy, nor treat PIs unfairly (Chung, & Lounsbury, 2006).
In order to deal with these unequal power dynamics, we put a number of features in place to avoid a destructive collision. First, we decided to brief every PI before they attended a CAB meeting. This briefing emphasized that PIs should treat the meeting with the CAB as though they were speaking informally to a colleague or acquaintance about their research. By emphasizing informality and collegiality, we hoped to set a tone for collaboration. Also, before meeting with the CAB, we asked PIs for a brief summary of the research they wanted to discuss, what kind of involvement they wanted with the CAB vis-a-vis the Community Engagement Continuum, and five questions they wanted to ask. Furthermore, we requested that the PIs not come with a PowerPoint presentation, since this would put the PI in the role of lecturer or teacher, which could effectively disempower the CAB members.
We also discussed with the CAB how to treat PIs when they came to meet with them. To establish the issues around authority, autonomy and expectations, we enumerated differences in power and status, and some of the worries PIs might have. For example, we thought that some PIs might view the CAB negatively, as if it were another type of IRB. To avoid this type of interaction, we encouraged the CAB to treat PIs like colleagues, to be respectful and friendly without being differential. The question arose about whether the CAB had the autonomy and authority to decide not to support a PI’s research. We made it very clear to the CAB that they could decide, for example, not to write a letter of support, or to ask PIs to make changes to their research design in order for the CAB to comfortably support the research. In other words, the CAB was not a rubber stamp. However, we also took great care to inform the CAB of the consequences of not supporting a PI’s work: the damage to the trust and longevity of the relationship could be irreparable.
Dependency
Research into intergroup dynamics in which groups with unequal power and status are involved indicates that unwanted feelings of dependency are often responsible for derailing collaboration and collegiality (Bornstein, 1998; Smith & Berg, 1987). PIs are not used to feeling dependent on patients or Veterans, as they often see themselves as having superior status and power. However, PIs have to depend on funding agencies, supervisors, and administrators in order to conduct their research, relationships that often evoke negative feelings (Bornstein, 1998; Edwards & Saltman, 2017; Smith & Berg, 1987). Therefore, for a PI to attend a CAB meeting in which he or she is asking the CAB for feedback or guidance could easily activate unwanted feelings. We reasoned that if difficult feelings were activated, PIs would be more likely to respond to CAB members’ involvement defensively. For example, unwanted feelings of dependency can evoke a superior affect on the part of the person who does not want to feel dependent (Bornstein, 1998; Smith & Berg, 1987), leading, in turn, to conversations that are patronizing, condescending or in which others’ views are invalidated. In other words, tokenism. This situation can become deleterious and difficult for the CAB to recover from. When these conversations occur, it is important for facilitators to redirect the conversation towards restating the reasons for the PI’s visit: obtaining Veteran perspectives. What this does is reinforce the authority and autonomy of the PI, while also preventing the PI from dominating the conversation.
The members of the CAB were likely to have different issues with dependency: CAB members were likely accustomed to relating to physicians and researchers from a dependent position. For example, since many of the members received their care at the VA, and they were used to relating to physicians as patients, we worried that this submissive and passive posture would carry over to the CAB. We were therefore alert for CAB members who acted in subservient ways toward PIs in order to intervene with conversations that build the confidence of the members and directly validate their views. Also, we alerted CAB members to the possibility that, because PIs were not familiar with feeling dependent on patients, they might react, as noted above, in defensive ways. We suggested that a remedy might be to remind the PI in a respectful way that issues being raised are ones they may not have considered. Also possible was that CAB members might do the opposite and act defensively with PIs. For example, to avoid feelings of dependency and inferior status, members might act self-righteous, or overly aggressive with PIs in order to compensate for these unwanted feelings. When this occurs, a tactic that may work to reestablish equanimity among the CAB members is to listen to their views without judgment and to affirm the value of their perspective, while also preventing the member experiencing defensive feelings from dominating the conversation. Therefore, to equalize the status between PIs and CAB members, we established that part of a CAB member’s job was to help create a safe and collaborative atmosphere for PIs during CAB meetings by being welcoming to the PI throughout the entire meeting, setting clear expectations for the interaction, and indicating their interest in the PI’s research.
We paid a great deal of attention to balancing and navigating these psychological and social issues, as we believed they could reinforce the authority and autonomy of the CAB or, if these forces became unbalanced, would undermine it. Negotiating unequal power dynamics and dependency are crucial to creating an effective and empowered CAB and need to be part of the design and execution of all CABs.
Effectiveness Snapshot
In keeping with the importance of measuring CAB members’ views of engagement activities, we designed a very brief survey to learn whether they felt actively involved in defining and realizing CAB goals (see Table 1). We surveyed the members annually from 2017 to 2019, anonymously asking members’ feelings about their participation. When asked whether they felt the meetings were productive, the average score, on a scale of 1 to 4, displayed an improving trend from 2.5 to 3.6 (ca. 50% response rate).
Member’s Views of CAB Effectiveness & Empowerment.
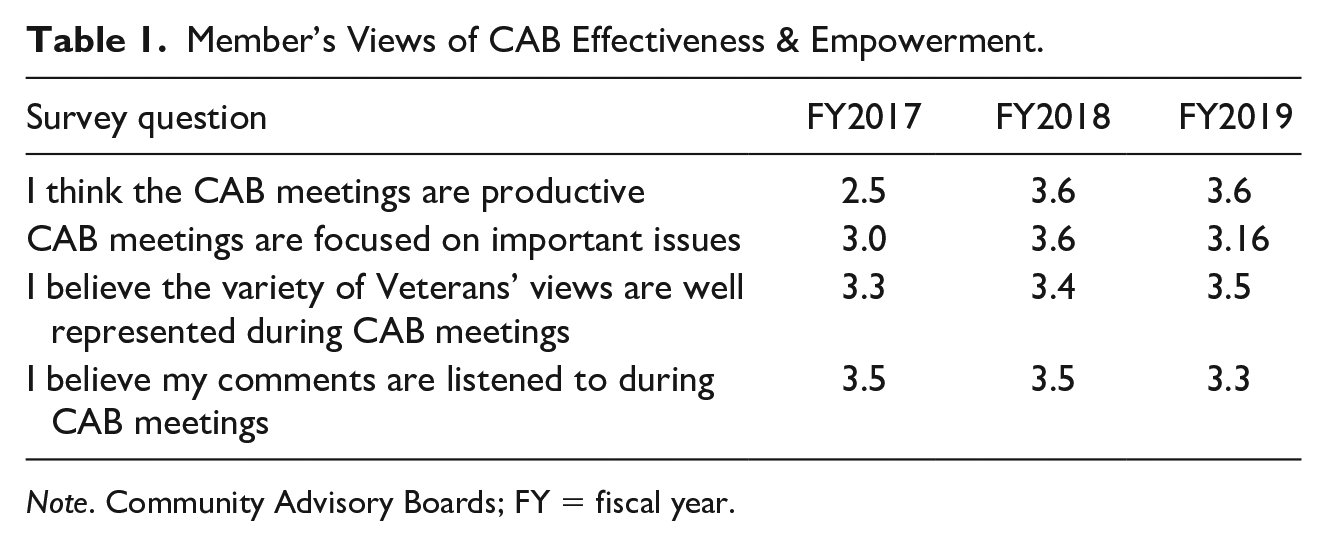
Note. Community Advisory Boards; FY = fiscal year.
When asked whether the CAB was focused on important issues, there was variation in their response. Initial assessment in 2017 indicated an average rating of 3.0, rising to 3.6 in 2018, and falling back to 3.16 in 2019. We surmise that this range may be related to the emphasis and quality of the activities presented to the members in these years. In Year 1, there were foundational tasks related to establishing procedures and norms for interactions with PIs. The second year’s score may reflect the newness of reviewing CHERP’s Pilot Program applications along with increased evidence of contributions to improving Veteran Health. The lowered score in 2019 may reflect the increased workload of a fuller scope of engagement: guidance on recruitment tactics, public outreach events about VA Research, meeting with VA leaders, and so on. Though important to engagement and CAB agency, these are areas which are tangential to the central mission of reviewing health equity research proposals.
When asked if the variety of Veterans’ views were well represented in CAB meetings, the data show an escalating trend beginning at 3.3 in 2017, rising to 3.5 in 2019. Finally, when asked if the members felt their voices were being listened to in the meetings, the scores ranged from 3.5 in 2017 rising slightly to 3.6 by 2019. Because most respondents gave a score of 3 or above (i.e., agree) to these questions every year, we have a consistent picture that members experience the board as effective and empowered.
In practice, an empowered CAB is one that freely questions PIs assumptions and surpasses their expectations of Veteran engagement in research. CAB members question PIs about their data gathering, about their outcomes of interest, and often raise issues of disparity that the research fails to address. Furthermore, the CAB may see fit to pursue its own topics and interests outside of those presented to them by PIs. If the CAB is not pressing PIs to consider or include member identified issues or concerns, this is evidence the CAB does not feel empowered to go beyond the status quo.
Conclusions
In sum, differing expectations are often the cause of a derailed group or CAB. Especially in large systems, it is easy for different people at different levels of a hierarchy to have disparate expectations for a CAB. Our experience led us to prioritize among each of the stakeholders the clarification of expectations for an effective and empowered CAB. We did this through multiple discussions with CHERP’s leadership, Veterans and PIs; with medical center leaders; and through formally chartering the CAB with a mission and by-laws.
The issue of authority looms large in groups containing members that have unequal status. It remains important to track the pathways of authority in order to illuminate its structure, and in order to build an effective CAB within it. We encourage research center leaders to first consider who authorizes the formation of the CAB, and to ensure that this authorization and decisions resulting from it will not be undermined. Furthermore, creating a Veteran CAB in which all the members shared the same status promoted the cohesiveness and solidarity that mirrored the group-centered culture of their military experience. This enabled the members to exercise their own agency, prevented them from experiencing a lesser status than researchers, and consequently, being and feeling isolated or split off from the group in the face of complex tasks. Forming a CAB with members of equal status enabled them to use their decision-making power to challenge status differences in a group-centered way.
Autonomy always has its limits, and this is especially true in large bureaucratic systems like the VA. Discussing limits to a group’s autonomy with the CAB is another way we ensured that expectations were clear. We also sought to ensure that the CAB acted with appropriate power, while not transgressing organizational boundaries, and yet at the same time confidently exercised the power and authority it did possess. In terms of equity, structuring the CAB in this fashion insured that the CAB could raise tough questions with PIs when equity issues are missing or marginalized in their work. Using the Community Engagement Continuum illustrates the range of ways that the CAB could apply its autonomy to equity questions.
Unless power dynamics are acknowledged, tracked and explicitly discussed, they can easily turn a CAB into a rubber stamp, or CAB members into feeling like tokens. We sought to embrace equal distribution of power and status by addressing issues of authority and autonomy, and by taking specific steps to equalize the distribution. We attribute the CAB’s success in no small part to the fact that we directly addressed the issue of dependency and worked to interrupt the submissive and passive dynamic that patients often enact toward medical research PIs (who are often physicians). We simultaneously made PIs aware of their own feelings of dependency that might be engendered when they attended a CAB meeting, and what to do about it.
The literature on CABs repeatedly emphasizes the issue of trust (Barkin et al., 2013; Becker et al., 2013; Safo et al., 2016; Schulz et al., 2003). Although we have discussed the issue of trust here, we have not emphasized it because we believe it is a byproduct of positively managing the issues we chose to prioritize—expectations, authority, autonomy, power dynamics, and dependency. We also would note that emphasizing trust in CAB discussions can subvert a clear understanding of the hidden group dynamics inherent in CABs. Research organizations that want to introduce an effective, empowered CAB would do well to clarify expectations and consider the ways in which they are going to authorize and provide the CAB with autonomy. Research organizations that need to address a CAB that has become fragmented, ineffective or disempowered might revisit the expectations that led to the creation of the CAB, while also tracking down the points where authority and autonomy have gone awry.
Footnotes
Acknowledgements
We thank Dr. Said Ibrahim for his vision of increasing Veteran engagement when he was Co-Director of the HSR&D Center for Health Equity Research and Promotion and Heather Johnson for helping us to realize that vision when she was Associate Director of the HSR&D Center for Health Equity Research and Promotion. We thank Dr. Judith Long (HSRD& Center for Health Equity Research and Promotion and the University of Pennsylvania) for her support and courage in continuing to advocate for Veteran engagement.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.