
Abstract
Therapist empathy toward existential concerns might be a critical component of clinical practice. This study aims to explore the psychometric properties of the Existential Empathy Questionnaire (EEQ), a self-report instrument developed to measure levels of existential empathy among mental health professionals. The EEQ was completed by a sample of 393 therapists recruited in Belgium, along with measures of general empathy, experiential avoidance, and existential avoidance. To assess the test–retest reliability, 353 participants of the same sample completed the EEQ a second time 2 weeks later. Clinical experience and therapeutic theoretical background were assessed to inform professional characteristics. The results support the use of the EEQ as a unidimensional measure of existential empathy. It demonstrates good internal reliability and temporal stability. A principal components analysis indicates three components with small to moderate intercorrelations, labeled as “Communication,” “Avoidance and Overwhelming Feelings,” and “Resonance and Presence.” EEQ total scores show a moderate positive association with general empathy and a moderate negative association with experiential and existential avoidance. Furthermore, the EEQ significantly uniquely predicts experiential and existential avoidance after controlling for general empathy. Years of clinical practice and a humanistic-oriented therapeutic approach correlated moderately with high EEQ scores.
Keywords
Therapist empathy has been identified as a primary common factor in the process of psychotherapy and as a robust predictor of therapy outcome across therapeutic orientations (Wampold, 2015). However, the most recent meta-analysis covering 82 independent samples (N = 6,138) showed considerable heterogeneity concerning the effect of empathy, which led the authors to encourage researchers to identify situations in which empathy might be particularly valuable (Elliott et al., 2018). Recently, Vanhooren (2019a) pointed out that empathy could be of specific value when it comes to the existential concerns of clients. Existential concerns refer to people’s questions and worries about human existence and reach beyond people’s concrete, specific issues. Examples include concerns about life’s finitude, the search for meaning and the struggle with meaninglessness, and existential loneliness and the search for connectedness (Yalom, 1980).
During the last decade a stream of research has been showing that existential issues, such as existential distress and search for meaning, are highly prevalent and relevant across patient groups in psychotherapy practice (Arredondo & Caparrós, 2019; Golovchanova et al., 2021). Existential concerns have, for example, been associated with several forms of psychopathology, including eating disorders, depression, anxiety disorders, addiction, and psychosomatic illnesses (Fuchs, 2013; Glaw et al., 2017; Iverach et al., 2014; van Bruggen et al., 2014). Accordingly, different psychotherapy models have underlined the need for mental health professionals to address the existential experiences of their clients (Cooper, 2017; Vanhooren, 2022a). Yet, at the same time several authors have indicated how difficult it can be for mental health professionals to work with clients’ existential concerns (Hill, 2017; Lundvall et al., 2018; Sundström et al., 2018; Ulland & DeMarinis, 2014; Vanhooren, 2019b).
Qualitative studies have recurrently shown how mental health professionals often feel overwhelmed by these existential concerns, feel unequipped to work with existential issues, and how the existential struggles of their clients evoke existential questions and struggles in themselves (e.g., Hill, 2017; Lundvall et al., 2018; Sundström et al., 2018; Ulland & DeMarinis, 2014). However, a recent meta-synthesis of two qualitative studies with 19 mental health workers who were experienced in working with existential concerns has also shown how their capacity to be and empathize with these specific clients’ struggles can grow through their careers (Frediani et al., 2022). In the same line, trainees in existential empathy have recurrently expressed how their empathy to the existential concerns of their clients has grown during their training, although they were already trained in empathy during their previous psychotherapy trainings (Vanhooren, 2018). Therefore, it might make sense to differentiate the capacity for empathy toward existential experiences from a general empathy to help mental health workers expand this specific competence.
This capacity to resonate with the client’s existential experiences, to symbolize, and to communicate this resonance has recently been called existential empathy (Vanhooren, 2019a, 2022a, 2022b). Yet, before we dive into the conceptualization of existential empathy, it is important to first address the concept of “general” empathy.
General Empathy
As Cuff and colleagues (2016) illustrated, presenting a clear definition of general empathy poses a real challenge. In their review study on empathy, they examined 43 distinct definitions and argued that there are eight themes that lead to different conceptualizations of empathy. Examples include whether empathy is considered as a cognitive or affective concept, whether the empathic emotion of the observer needs to be congruent with that of the emotional person, and whether the self/other distinction is maintained (for a full overview see Cuff et al., 2016). Based on their analysis of the empirical evidence on empathy, including neuroscientific studies and the theoretical arguments of the reviewed literature, they concluded that
There are functional differences between empathy and related concepts; empathy includes both cognitive and affective elements; the emotions of the target and observer are similar but not identical; other stimuli, such as imagination, can evoke empathy; a self/other distinction is maintained in empathy, although a degree of merging is necessary; empathy is affected by both trait and state influences; behavioral outcomes are not part of empathy itself; and finally, empathy is automatically elicited but is also subject to top-down controlled processes. (Cuff et al., 2016, p. 150)
In sum, they described empathy as an emotional (affective) response that also relies on the cognitive understanding of what the other person is experiencing, resulting in the experiencing of an emotion that is similar to the other person’s emotion while still recognizing that the source of the emotion is not one’s own (Cuff et al., 2016).
If we apply this conceptualization of empathy to how empathy is generally understood within a clinical setting, then this definition seems to correspond with Rogers’s (1957, 1980) theory on empathy and how it was further elaborated by Barret-Lennard (1993). Rogers’s (1980) description of empathy contains the cognitive and affective processes of the empathic therapist who tries to grasp the meaning of the client’s experiences as well the accompanied feelings and felt senses of the client. Furthermore, Rogers (1980) described how the therapist’s awareness of their own bodily felt experiences is a crucial source of empathy, and how the self/other distinction is important to be maintained. Simultaneously, Rogers (1980) hinted how a certain degree of merging is necessary, as long as therapists can find their way back home to their own experiences. Finally, Rogers (1957, 1980) emphasized that this experienced empathy has also to be communicated by the therapist to be perceived by the client. Barret-Lennard (1993) summarized this process of empathy in three different steps: (a) empathic resonance, (b) the expression or communication of this resonance and empathic understanding, and (c) finally the perceived empathy by the client (Barret-Lennard, 1993).
Perceived empathy refers to the effect of the therapist’s behaviors on the client. In the case of perceived empathy, the therapist’s behaviors—the expressed empathy—are evaluated as empathic (Watson, 2007). It is this expressed empathy and perceived empathy that have robustly been associated with therapy outcome (Wampold, 2015), not the therapist’s empathic resonance. This is why although a behavioral response is not implied in most definitions of empathy (e.g., Cuff et al., 2016), the dimension of empathic communication is still implied when discussing the therapist’s empathy in a clinical setting. Important to note is that this empathic communication is expressed by both verbal and nonverbal therapists’ behaviors as it is not only about “what to say” but also about “how to be” (Riess & Kraft-Todd, 2014). Being empathic is thus not a technique, but a way of being present in relationship to the client (Geller & Siegel, 2017; Rogers, 1980). It is this conceptualization of general empathy, which integrates therapeutic presence, empathic resonance, and empathic communication, that Vanhooren (2022a, 2022b) based his concept of existential empathy on.
Existential Empathy
According to Vanhooren (2022b), the difference with general empathy is that while general empathy is directed toward the client’s particular and concrete life circumstances, existential empathy is directed toward the experience of the human condition, and the typical life questions, struggles, and feelings that accompany this experience. Or in other words, existential empathy touches the macro-dimension of meaning in therapy (the meaning levels that includes one’s ultimate concerns and one’s self-transcendent ontological meanings), whereas general empathy typically stays focused on the ontic micro-dimension of meaning (one’s felt sense about the here-and-now inner experiences and one’s interactional experiences) and the ontic meso-dimension of meaning (one’s self-concept, life narrative, cherished beliefs, world assumptions, and other conceptual meanings; Vanhooren, 2019b). Vanhooren (2022b) also explained that the difference between general and existential empathy should not be understood as simply a difference in content but also in how empathy is experienced. The self-other distinction, for example, that is mostly maintained in general empathy (Cuff et al., 2016), may become more elusive in existential empathy because when it comes down to the human condition the client and therapist share the same existential reality (Vanhooren, 2022a, 2022b). So when clients for example share their anxiety about life’s finiteness, therapists cannot deny they have the same reality to face.
This could imply that empathizing with clients’ existential concerns could more easily be overwhelming for therapists. These overwhelming feelings could hinder their empathy as a certain degree of being grounded in life is considered a prerequisite for being able to stay present with one’s own and another’s existential concerns (Missiaen & Vanhooren, 2021; Vanhooren, 2022a). This is in line with the studies on general empathy that state that empathy implies a regulatory factor, sometimes referred to as emotional disconnection (Carré et al., 2013). This means that although an individual can feel negative emotions similar to the negative emotions of the other person, this person does not experience dysregulating levels of personal distress (Carré et al., 2013). Vanhooren (2022a) argued that when this basic level of groundedness is missing, the therapist might tend to avoid existential themes in therapy.
In sum, existential empathy refers to the therapist’s capacity to resonate with the client’s existential experiences and to symbolize and communicate this resonance while staying grounded within oneself, when the existential reality, which both the client and therapist share, is the focus in the session. It is hypothesized that existential empathy might help facilitate new meaning in life, help bridge existential loneliness, and help develop awe, wisdom, and resilience in clients’ approach to life (Golovchanova et al., 2021; Vanhooren, 2022b). However, empirical research on existential empathy has been missing by the lack of a validated instrument to measure this construct. Assessing therapists’ existential empathy allows for future research to clarify whether and how empathizing with the client’s existential experiences fosters the therapeutic process and impacts therapy outcome.
In this context, the Existential Empathy Questionnaire (EEQ) (or in the original Dutch version the Existentiële Empathie Vragenlijst; EEV) was recently developed as a tool to measure levels of existential empathy in mental health professionals. The construction of the EEQ was based on Vanhooren’s (2019a, 2022a, 2022b) concept of existential empathy. As described above, this definition of existential empathy implies that (a) the therapist is sufficiently grounded in life to be able to face—and not to avoid or be totally overwhelmed by—the existential dimension of life, (b) that the therapist is open toward the client’s existential concerns and is able to stay present and resonate with these concerns, and (c) the therapist is able to communicate their empathy, both verbally and nonverbally. The items of the EEQ were generated to reflect these elements. For example, the item, “I feel that something resonates in me when my clients talk about existential themes” (agree) was chosen to assess the level of empathic resonance. Also negative items that include the therapist’s efforts to avoid resonating with clients’ existential experiences were included, for example, “I change the subject when my clients are talking about existential themes” (disagree). The level of groundedness—or contrary, avoidance, and overwhelming feelings—was assessed by items such as “I feel overwhelmed when my clients talk about existential themes” (disagree) and “I start feeling anxious when my clients talk about existential themes” (disagree). Finally, items reflecting empathic communication were included, for example, “I convey my closeness when my clients talk about existential themes” (agree).
As mentioned before, empathic communication is usually not included in general empathy questionnaires (e.g., Jolliffe & Farrington, 2006) as the therapist’s behaviors are formally not seen as a characteristic of empathy (Cuff et al., 2016). Vanhooren (2022a, 2022b), however explicitly included the dimension of empathic communication in his definition of existential empathy, leading it to be understood as a therapeutic skill that is directly relevant in therapy. This is why we chose to also include empathic communication in our scale. Based on these ideas, a first version of the EEQ with 8 items was compiled by the first author and discussed with two senior supervisors and trainers in existential therapy. Based on their feedback, a second version of the EEQ was made with 51 items by the KU Leuven experiential-existential psychotherapy research team consisting of the first author and four other clinical psychologists who were trained as person-centered, existential, or family therapists. The same group discussed the 51 items and decreased the EEQ to 34 items, omitting items that were too overlapping, idiosyncratic, or confusing. Next, 10 therapists who were not existentially trained and were not part of this research group were asked to complete this version of the EEQ and to provide their feedback on their understanding of the items. Based on their feedback, the EEQ was finally reduced to 21 items. The English version is based on the same 21 items that were originally developed in Dutch. First, the Dutch version was translated into English by the second author. Then, the first and last author, both bilingual and native Dutch English speakers, engaged in a process of back translation and adjusted the English version. Third, the English version was checked by another native English speaker and two translated items were discussed again by the bilingual research members, which led to the final English version.
This study aimed to assess the psychometric properties of the current Dutch EEQ version with its 21 items. Specifically, it explored the instrument’s (a) internal consistency, (b) test–retest reliability, and (c) factor structure. The (d) convergent validity and (e) divergent validity of the instrument were also examined. Finally, the study examined the professional characteristics of the EEQ, specifically years of clinical practice and current therapeutic orientation.
Structural Validity
As Rogers (1980) and Vanhooren (2022a, 2022b) suggested, although empathy might consist of different processes, its existential significance resides in the client feeling deeply understood in their fundamental struggles with their existential concerns. Therefore, the questionnaire has primarily been developed to measure this phenomenon as a whole, and the scale’s latent structure is thought to be unidimensional.
However, as the items reflect aspects that have been defined as essential in existential empathy, such as (a) empathic resonance and presence, (b) groundedness or not having to avoid existential content or feeling overwhelmed by it, and (c) empathic communication, we hypothesized that the questionnaire might show different components and a three-factor structure. However, we also hypothesized that these components might be strongly interconnected. Being able to be present and resonant is, for example, only possible when a therapist is sufficiently open toward the client’s experiences (Rogers, 1957, 1980), instead of being avoidant of them. Therefore, we thought presence and resonance might be negatively associated with avoidance. Also, we expected that feeling overwhelmed could be negatively related to presence and resonance, as being overwhelmed might prevent the therapist to be grounded enough to stay present with the client’s experiences. Moreover, communication of empathy could result from feeling empathy; thus, we expected communication to be strongly related to presence and resonance. Because of the fact that existential empathy is a new concept and other questionnaires on existential empathy do not exist, the questionnaire’s structure and its possible components have been explored in this study. The results of this exploration render a more solid hypothesis for its factor structure to be tested in a future study.
Construct Validity
Given that the EEQ considers the distinction between general and existential empathy and the necessary presence and resonance for existential empathy to occur (Rogers, 1957, 1980; Vanhooren, 2019a, 2022b), it was expected that EEQ scores would have a positive moderate correlation with levels of general empathy. We expected this effect size to be moderate because current self-reported questionnaires measure empathy with specific, concrete experiences, rather than with the existential layer of the client’s experience. A strong correlation would actually question whether there is such a thing as existential empathy. Based on the idea that resonance and presence are necessary before one can communicate existential empathy (Rogers, 1957, 1980; Vanhooren, 2019a, 2022b), we expected a significant negative moderate to strong correlation between existential empathy and experiential avoidance. Likewise, we also expected a significant negative moderate to strong correlation between existential empathy and existential avoidance. Above this, we had expectations concerning the professional characteristics. It has been found that more experienced and humanistic-oriented therapists are more likely to work and feel confident working with their clients’ existential experiences (Hill et al., 2017). We thus expected that more years of clinical practice would be associated with higher scores on the EEQ and that compared with other theoretical orientations, a humanistic-oriented therapeutic background would predict higher scores on the EEQ.
Method
Study Design
This study used a cross-sectional design with two assessment points. As unexpected life events might influence existential empathy, we limited the test–retest period to only 2 weeks. Participants completed all questionnaires at the first assessment (T1) and the EEQ a second time 2 weeks later (T2) to investigate the psychometric properties of the EEQ.
Participants and Procedures
The study sample consisted of therapists and counselors from five major therapeutic orientations: humanistic (including person-centered, existential, gestalt, and humanistic-experiential therapists); marital, and family and systems; psychodynamic and psychoanalytic; cognitive-behavioral; and integrative psychotherapy. Inclusion criteria were (a) practicing psychotherapists and counselors and (b) sufficient proficiency in the Dutch language. Participants were recruited in Flanders (Dutch-speaking Belgium) via social media, newsletters of professional psychotherapy associations, and emails to group practices and mental health care centers. There was no incentive offered for participation. The minimum sample size (N = 333) was determined based on the a priori power calculation using Creative Research Systems’ Sample Size Calculator (Creative Research Systems, 2021) with a 95% confidence level and 5 margin of error. An estimated size of N = 2,500 was considered for the population of Dutch-speaking clinical psychologists and social workers with psychotherapy training in Belgium, based on the latest national report (Luyten & Jeannin, 2021).
Data were collected between October and December 2021. Participants completed both self-report surveys online via the Qualtrics program at two different time points. The first survey (T1) measured age, years of clinical practice, therapeutic orientation, and scores on existential empathy, general empathy, experiential avoidance, and existential avoidance. This survey started with an information letter about the study and an informed consent form, which respondents needed to sign electronically before proceeding with the study. Two weeks after completing this survey at T1, respondents were invited to fill in the EEQ a second time (T2).
Initially, 522 psychotherapists and counselors signed the informed consent, of which 393 (75.3%) completed the first online survey. Martinez-Plumed and colleagues (2021) argue that before missing values are automatically imputed, the characteristics of these missing values should be identified to understand the impact of these values on the sample. To identify these characteristics and its impact on our sample—and therefore our study—we first had a closer look. Of the 129 participants (24.7%) participants who didn’t complete the first survey, 108 (20.7%) only completed their demographic and professional characteristics, which was 9.00% of the entire survey. They did not start to fill in the measures concerning the study variables. The remaining 21 noncompleters (4.00%) filled in the EEQ, but not the other measures. The online system did not allow participants to proceed to the next items or measures if the previous one’s were not completed. As a consequence, the missing values in our sample can be understood as partial completion or attrition instead of other types of missing values, and only exists of “row” missing values (Martinez-Plumed et al., 2021). Martinez-Plumed and colleagues (2021) argue that in general, row missing values do not bias the sample. To test whether this partial completion indeed did not impact the sample’s characteristics concerning its representativeness of the population, we checked for significant differences between completers and partial completers through independent-sample t tests and one One-way ANOVA. However, these tests did not show any statistical differences between completers and noncompleters concerning age, years of clinical practice, or being humanistic-oriented as a therapist or not. Therefore, partial completion seemed to be random and could not be attributed to participant characteristics. The sample of completers still represented the targeted population and the remaining sample size remained adequate. Because of these arguments and the fact that the large majority of noncompleters did even not start to fill in measures concerning our actual study variables, imputing the “missing” values and even entire measures did not seem to be an ethically responsible action.
Only participants who completed the first survey at T1 (n = 393) were automatically invited to participate in the second survey at T2 2 weeks later to study the test–retest reliability of the EEQ. At T2, 325 participants started the survey and they all completed all the questionnaires. In sum, the final sample was constituted of 393 respondents at T1 and 325 respondents at T2.
Additional Ethical Considerations
Data collection followed the ethical approval of KU Leuven’s Social and Societal Ethics Committee (SMEC; G-2021-3541). The study was publicly registered at Open Science Framework (OSF; 10.17605/OSF.IO/KJWHR) prior to any human observation of the data. The preregistration occurred during the start of recruitment because some of the therapy associations contributing to the recruitment issued their newsletters earlier than planned.
Measures
Professional Characteristics
Respondents reported their age, years of clinical experience, and therapeutic orientation. Their years of clinical experience was assessed in units of years. To measure therapeutic orientation, respondents indicated which of the given five major therapies they identified with the most at that moment (i.e., humanistic-person-centered-experiential-existential, marital and family, psychodynamic and psychoanalytic, cognitive-behavioral, or integrative). Then, for the analysis of their therapeutic orientation we coded this variable as a dichotomous variable with all therapeutic orientations other than the humanistic grouped into the level called “other-oriented.”
Existential Empathy Questionnaire
The EEQ is a self-report questionnaire developed by the Experiential-existential Psychotherapy research team to measure therapist existential empathy according to Vanhooren’s (2019a, 2022a, 2022b) conceptualization of the construct. Examples of items are “I feel that something resonates in me when my clients talk about existential themes,” “I avoid existential topics or feelings of my clients (reverse-keyed), and “I articulate how the client might be feeling about these existential themes.” The current study examined the psychometric properties of the 21-item version of the EEQ. Items were rated on a 7-point Likert-type scale ranging from 1 (never) to 7 (always). Total scores were calculated from the sum of all items. Scores range from 21 to 147. The study used the original Dutch version EEV.
General Empathy: Toronto Empathy Questionnaire
The Toronto Empathy Questionnaire (TEQ) is a brief self-report questionnaire used to assess levels of empathy, conceptualized primarily as an emotional process (Spreng et al., 2009). It was developed to represent the common factor detected across several validated questionnaires measuring empathy. The TEQ consists of 16 statements rated on a 5-point Likert-type scale ranging from 0 (never) and 4 (always). Examples of items are “It upsets me to see someone being treated disrespectfully” and “I find it silly for people to cry out of happiness” (reverse-keyed). Empathy is indicated by a unidimensional total score computed by summing the rating of each of the 16 items. Total scores can range between 0 and 64, where higher scores indicate higher levels of empathy. The TEQ has presented good internal consistency, high test–retest reliability, and strong convergent validity (Spreng et al., 2009). In this sample, Cronbach’s alpha coefficient was .76. An unpublished authorized Dutch translation of the TEQ (Vanaken et al., 2018) was used in this study. The process of translation and back translation was discussed with the authors of the original questionnaire.
Experiential Avoidance: Acceptance and Action Questionnaire II
The Acceptance and Action Questionnaire II (AAQ-II) is a 10-item self-report assessment of the levels of psychological inflexibility or experiential avoidance (Bond et al., 2011). Examples of items are “I’m afraid of my feelings” and “It is okay if I remember something unpleasant” (reverse-keyed). Respondents rate the degree to which each statement applies to them on a 7-point Likert-type scale ranging from 1 (never true) and 7 (always true). A unidimensional measure of experiential avoidance is derived by summing the rating of all items. Total scores can range from 10 to 70 where higher total scores indicate higher levels of acceptance and lower levels of experiential avoidance. The AAQ-II has shown high internal reliability, test–retest reliability, and construct validity (Bond et al., 2011; Jacobs et al., 2008). In this sample, Cronbach’s alpha coefficient was .84. The current study used the validated Dutch translation of the AAQ-II (Jacobs et al., 2008).
Existential Avoidance: Existential Concerns Questionnaire—Avoidance Subscale
The Existential Concerns Questionnaire (ECQ) is a 22-item self-report questionnaire. It measures the levels of existential anxiety, defined as the fear toward nonconcrete conditions of human existence, that is, death, meaninglessness, and fundamental loneliness (van Bruggen et al., 2017). Respondents rate the items on a 5-point Likert-type scale ranging from 0 (never) to 4 (always). A total score is computed from the sum of all items, where a higher score indicates a higher level of existential anxiety. Although the ECQ is recommended to be used as a unidimensional scale, the subscale “Avoidance” is found to measure existential avoidance as a different conceptual aspect of existential anxiety (van Bruggen et al., 2017). Therefore, the current study used the sum of the four items comprising the Avoidance subscale separately as a measure of the levels of existential avoidance in the analysis of the divergent validity of the EEQ. These scores can range from 0 to 16. The ECQ has shown good reliability, stability, and construct validity (van Bruggen et al., 2017). In the present sample, Cronbach’s alpha was .90 for the full ECQ and .64 for the Avoidance subscale. The validated Dutch translation of the ECQ (van Bruggen et al., 2017) was used in this study.
Statistical Analyses
Data analyses were carried out using SPSS Statistics Software version 27 (IBM Corp, Released 2020) with significance at p < .05. In all analyses, we used the data of all respondents at T1, except in the test–retest reliability analysis. In this analysis, we only used the data of the respondents who also completed the assessment at T2. Descriptive statistics were obtained to inform the distribution of the professional characteristics in the sample in terms of age, years of clinical practice, therapeutic orientation, and distribution of scores across the EEQ, TEQ, AAQ-II, and ECQ–Avoidance subscale. Internal consistency from all instruments was obtained by running a Cronbach’s alpha reliability test.
To evaluate the internal consistency of the EEQ, a Cronbach’s alpha coefficient was computed for the scores at T1.
To evaluate the temporal stability (test–retest reliability) of the EEQ, an intraclass correlation coefficient (ICC) was carried out using the total scores from the test (T1) and retest (T2) assessments. Respondents who did not complete the survey at T2 were excluded from the analysis. A two-way mixed-effects model (absolute agreement of single measures) was used with a 95% level of confidence. The ICC value was interpreted according to current guidelines, indicating the reliability as poor (<.50), moderate (.50–.75), good (.75–.90), or excellent (> .90; Koo & Li, 2016).
The component structure of the EEQ was identified with a principal components analysis (PCA) on the data at T1. Before performing the PCA, assumption checks were carried out regarding the strength of the intercorrelations (> .35), Bartlett’s test of sphericity (p < .05), Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy (at least .60), and outliers among cases. Direct Oblimin rotation was used with Kaiser normalization and component extraction based on eigenvalues greater than 1, Cattell’s (1966) scree test, and parallel analysis.
The convergent validity of the EEQ was assessed by computing Pearson product-moment correlations between the TEQ total scores and EEQ total scores at T1. The divergent validity of the EEQ was assessed by computing separate Pearson product-moment correlations between the EEQ total scores at T1 and the AAQ-II total scores and the total scores on the ECQ Avoidance subscale. The Pearson correlation effect sizes of these three validity analyses were interpreted as small (r < .10), moderate (.10 – .30), or large (r > .50), following Cohen’s (1988) general guideline. In addition, to explore the incremental validity of the EEQ, two hierarchical regression analyses were conducted to test whether the EEQ would still significantly and uniquely be correlated with experiential (AAQ-II) and existential avoidance (ECQ Avoidance subscale) after controlling for general empathy (TEQ).
For an examination of the professional characteristics of the EEQ, a Pearson-product correlation coefficient was planned to examine the association between years of clinical experience and EEQ total scores. However, a visual inspection of the histogram and Q–Q plot and a Kolmogorov-Smirnov test indicated that years of clinical experience did not follow a normal distribution, D(393) = .12, p < .001). Due to the violation of the normality assumption, a Spearman’s correlation was eventually used instead to calculate the professional characteristics with the EEQ. To examine the difference in levels of existential empathy between humanistic-oriented and other therapeutic backgrounds, an independent-samples t test was performed with therapeutic orientation (humanistic-oriented/ other-oriented) as the independent variable and EEQ total scores at T1 as the dependent variable. A Levene’s test was carried out to check the assumption of homogeneity of variance. The Cohen’s d effect size was used to interpret the output, with values indicating a small (0.20), medium (0.50), or large (0.80) effect (Cohen, 1988).
Results
Sample Characteristics
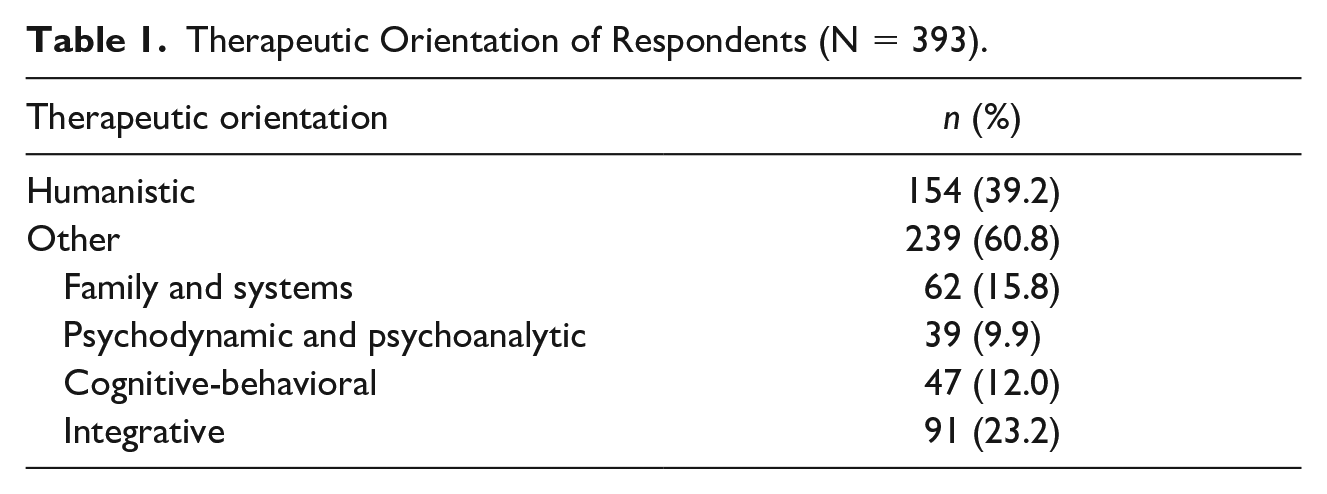
Therapists had a mean age of 45.6 (SD = 11.6) years and a mean of 13.7 (SD = 10.6) years of experience in psychotherapy practice. The distribution of therapeutic orientation of respondents is summarized in Table 1. Over a third of the sample identified with a humanistic-oriented psychotherapy background. Table 2 presents the sample distribution across the scores on existential empathy (EEQ), general empathy (TEQ), experiential avoidance (AAQ-II), and existential avoidance (ECQ–Avoidance subscale).
Therapeutic Orientation of Respondents (N = 393).
Sample Characteristics on EEQ, TEQ, AAQ-II, and ECQ—Avoidance Subscale.
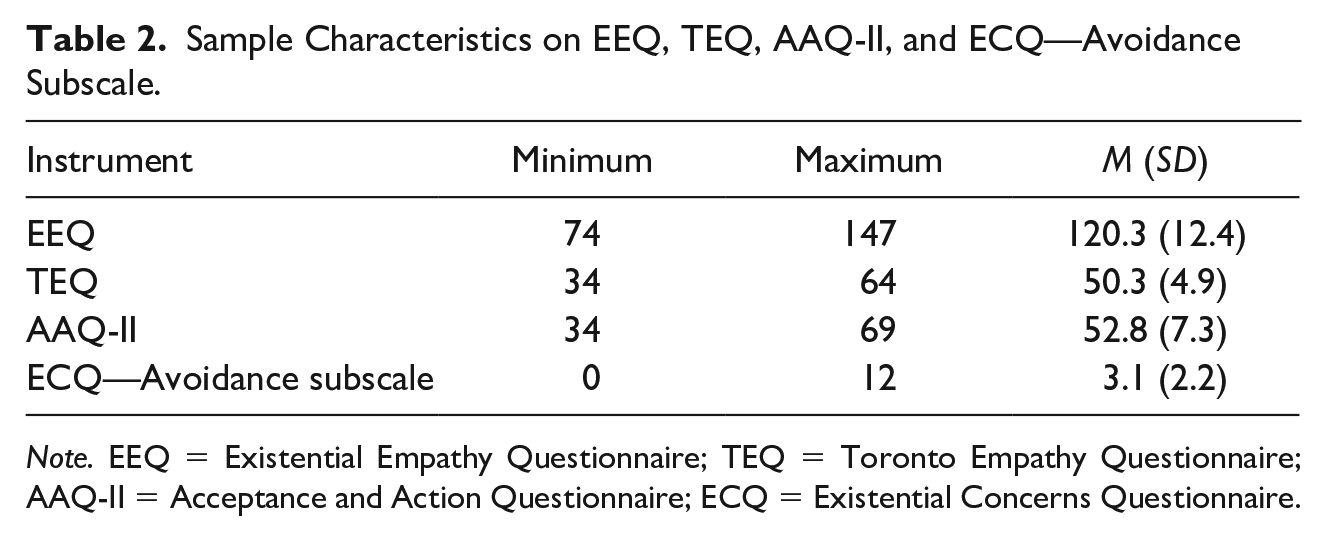
Note. EEQ = Existential Empathy Questionnaire; TEQ = Toronto Empathy Questionnaire; AAQ-II = Acceptance and Action Questionnaire; ECQ = Existential Concerns Questionnaire.
Reliability of the EEQ
The Cronbach’s alpha coefficient of the EEQ was .90. The intraclass correlation coefficient indicated good test–retest reliability of the EEQ scores at T1 and T2, r = .85, 95% confidence interval (CI) = [0.82, 0.88], F(324, 324) = 12.33, p < .001.
Component Structure of the EEQ
A principal component analysis (PCA) was performed on the 21 items of the EEQ. A total of nine values were identified as outliers (i.e., standardized residuals larger than 3.0) in four of the items in the EEQ. The PCA was performed after changing those scores to the nearest value within 3.0 standard deviations from the mean. The KMO value was .91. The Barlett’s test of sphericity was significant, χ2(210) = 4,070.61, p < .001. An inspection of the intercorrelation matrix identified several coefficient values of .35 and above. Four components were identified with eigenvalues exceeding 1.0, which explained 35.0%, 15.9%, 6.4%, and 4.8% of the variance. The scree plot illustrated a clear break after the second and third components. In the parallel analysis, the eigenvalues of three components exceeded the corresponding criterion value based on the randomly generated data matrix of the same size (21 Variables × 393 Respondents). Given that there were at least four items with unrotated loading values above .40 in the first three components, it was decided to retain three components for further investigation.
The three-component solution explained a total of 57.3% of the variance, with Component 1 explaining 35.0%, Component 2 explaining 15.9%, and Component 3 explaining 6.4%. An oblimin rotation was performed to aid in the interpretation. As represented in Table 3, all items related to communication and one item more explicitly related to genuine empathy (16) loaded more strongly on Component 1. This component was labeled “Communication.” All items measuring avoidance of resonance and overwhelming feelings (which are reverse-keyed) loaded more strongly on Component 2, whereas all items designed to reflect resonance and presence loaded more strongly on Component 3. These components were labeled “Avoidance and Overwhelming Feelings” and “Resonance and Presence,” respectively. There was a small positive correlation among the Components 1 and 2 (r = .25) and Components 2 and 3 (r = .17), and a moderate correlation between Components 1 and 3 (r = .50).
Pattern Matrix From Principal Component Analysis With Oblimin Rotation of Three Component Solution of EEQ Items.
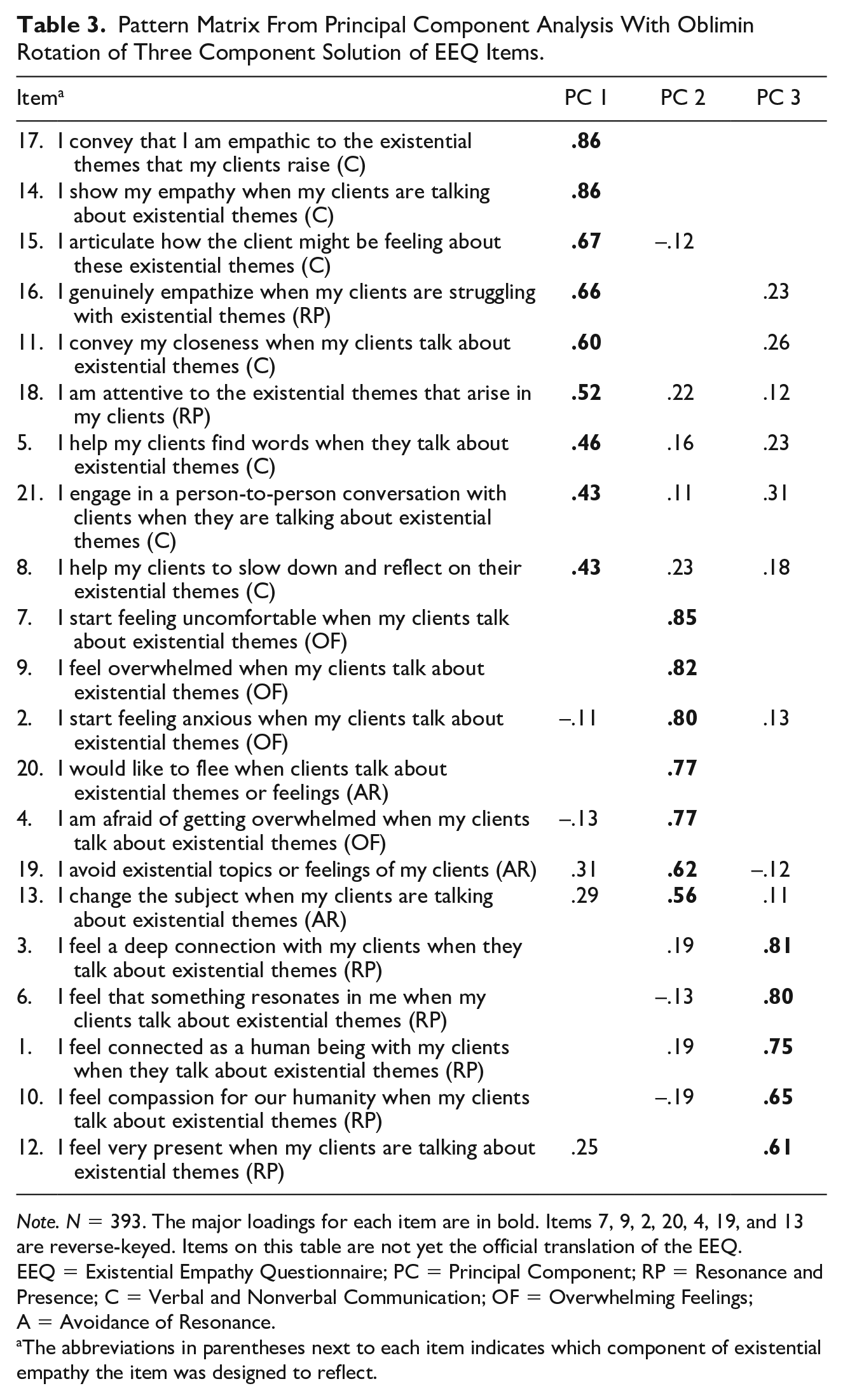
Note. N = 393. The major loadings for each item are in bold. Items 7, 9, 2, 20, 4, 19, and 13 are reverse-keyed. Items on this table are not yet the official translation of the EEQ. EEQ = Existential Empathy Questionnaire; PC = Principal Component; RP = Resonance and Presence; C = Verbal and Nonverbal Communication; OF = Overwhelming Feelings; A = Avoidance of Resonance.
The abbreviations in parentheses next to each item indicates which component of existential empathy the item was designed to reflect.
Validity Analyses of the EEQ
Three Pearson product-moment correlation coefficients were computed to examine the convergent and divergent validity of the EEQ based on the relationship of EEQ scores with levels of general empathy, levels of experiential avoidance, and levels of existential avoidance. There was one outlier among EEQ scores (std residual = −3.73), two outliers among scores on general empathy (largest std residuals = −3.31), and three outliers among scores on existential avoidance (largest std residuals = −3.31). These scores were changed to the nearest value within 3.0 standard deviations from the mean. For each of the analyses, a visual inspection of the normality of residuals with a Q–Q Plot and histogram indicated a somewhat normal distribution of error. The scatterplot illustrated a linear relationship between the variables, and the residual scatterplot indicated moderate to good homoscedasticity. The coefficients are summarized in Table 4. EEQ showed a moderate positive association with general empathy (r = .36, p < .001), and moderate negative association with experiential avoidance (reverse-keyed; r = .27, p < .001), and existential avoidance (r = −.32, p < .001).
Correlation Coefficients Among EEQ Scores and Scores on General Empathy, Experiential Avoidance, and Existential Avoidance.
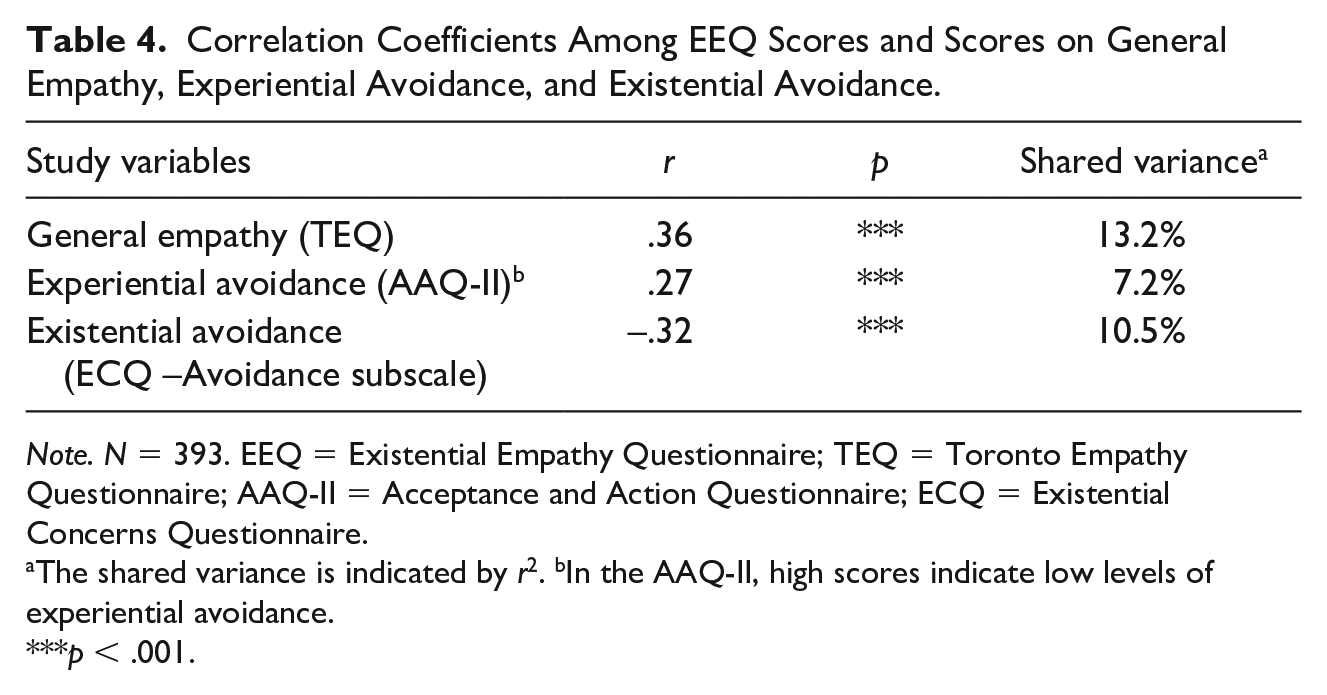
Note. N = 393. EEQ = Existential Empathy Questionnaire; TEQ = Toronto Empathy Questionnaire; AAQ-II = Acceptance and Action Questionnaire; ECQ = Existential Concerns Questionnaire.
The shared variance is indicated by r2. bIn the AAQ-II, high scores indicate low levels of experiential avoidance.
p < .001.
To explore the incremental validity of the EEQ, two hierarchical regression analyses were conducted to test whether the EEQ would still significantly and uniquely be correlated with experiential (AAQ-II) and existential avoidance (ECQ Avoidance subscale) after controlling for general empathy (TEQ). In the first hierarchical analysis, general empathy (TEQ) was entered in Step 1 as a predictor of experiential avoidance (AAQ-II). General empathy predicted experiential avoidance, R2 = .01, F(1, 391) = 3.94, p < .05 (β = .10, p < .05). In Step 2, existential empathy (EEQ) was added, ΔR2 = .06, F(1, 390) = 15.23, p < .001. In this step, experiential avoidance was predicted by existential empathy (β = .27, p < .001) but no longer by general empathy (β = .003, p = ns).
In the second hierarchical analysis, general empathy (TEQ) was entered in Step 1 as a predictor of existential avoidance (ECQ avoidance). However, general empathy did not predict existential avoidance, R2 = .002, F(1, 391) = .77, p= ns (β = −.04, p = ns). In Step 2, existential empathy (EEQ) was added, ΔR2 = .11, F(1, 390) = 24.30, p < .001. Also in this step, general empathy did not predict existential avoidance (β = .08, p = ns), but existential avoidance was predicted by existential empathy (β = −.35, p < .001).
Professional Characteristics of the EEQ
The association between years of clinical experience and EEQ scores was examined with a Spearman correlation coefficient, given that the data showed a highly skewed distribution in the years of clinical experience according to a visual inspection of the histogram and Q–Q Plot of the variable. The violation of the normality assumption was further verified by a Kolmogorov-Smirnov test, D(393) = .12, p < .001). Five outliers (largest std residual = 3.70) were corrected to the nearest value within 3.0 standard deviations from the mean. Scatterplots indicated that years of clinical experience had moderate homoscedasticity and linearity with EEQ scores. More years of clinical experience was moderately associated with higher EEQ scores, rs(393) = .25, p < .001, with a shared variance of 6.5%.
An independent-samples t test was conducted to compare the EEQ scores between therapists with a humanistic-oriented and other-oriented theoretical backgrounds. Therapists with a humanistic orientation scored higher on the EEQ (M = 122.88, SD = 11.57) than therapists reporting other theoretical backgrounds (M = 118.74, SD = 12.57), t(391) = 3.28, p = .001. The effect size was small to medium, d = 0.34, 95% CI = [0.13, 0.54].
Discussion
This study aimed to explore the psychometric properties of the EEQ, a self-report instrument developed to measure levels of existential empathy among mental health professionals. Results indicate that the EEQ items have good internal consistency and that the total scores show good temporal stability. The PCA analysis suggested a three-dimensional structure. The components could be subjectively labeled as “Communication” (CO), “Avoidance and Overwhelming Feelings” (AOF; reverse-keyed), and “Resonance and Presence” (RP). The reverse-keyed subscale AOF showed a small to moderate negative associating with CO and RP, whereas CO had a moderate to strong positive association with RP. The construct validity indices were in accordance with the hypothesized direction and strength: Higher EEQ scores were associated moderately with higher levels of general empathy (convergent validity) and moderately with lower levels of experiential avoidance (reverse-keyed) and existential avoidance (divergent validity). Furthermore, concerning the incremental validity of the EEQ, an additional hierarchical regression analyses showed that the EEQ was uniquely and significantly associated with experiential and existential avoidance after controlling for general empathy. Regarding the professional characteristics, therapists with high EEQ scores tended to have more years of clinical experience and a humanistic-oriented background instead of other therapeutic orientations.
The internal reliability of the EEQ indicates a clear underlying construct homogeneity of the items. This corresponds with the theoretical conceptualization of existential empathy in the psychotherapeutic setting, where resonance, presence, communication, and openness to existential experiences are each necessary elements to reach a therapeutic effect of existential empathy (Rogers, 1980; Vanhooren, 2019a, 2022a, 2022b). Further confirmatory factor analysis (CFA) should verify whether the three identified components (Communication; Avoidance and Overwhelming Feelings reverse-keyed; and “Resonance and Presence”) could be retrieved and confirmed in a different sample. Exploration of their interrelatedness and possible use as subscales could inform the therapist’s particular profile of existential empathy. This way therapists could learn about which aspects they might have to develop more to increase their existential empathy.
Our findings that therapists with more years of clinical experience and with a humanistic-oriented background scored higher on the EEQ might hint to the importance of training, clinical experience, and life experience to develop existential empathy. This association in our study is in line with the evidence that more experienced and existentially oriented therapists appear more comfortable approaching existential issues such as the search for meaning in life (Hill et al., 2017). In this study sample, it is, however, difficult to disentangle the contributions of older age, life experience, clinical training, and clinical experience. Any of these variables might have contributed to the association between clinical experience and EEQ scores. In previous studies, theoretical orientation did not correlate with levels of overall self-reported empathy based on the TEQ (Boulton & Davis, 2019) or with observer ratings of empathy, warmth, and genuineness (Fischer et al., 1975). Interestingly, our study seems to suggest that humanistic and existential therapists might specifically differ in existential empathy compared with other therapists. This is also in line with the qualitative study of Frediani and colleagues (2022) that suggests that person-centered and existentially trained therapists depict more complex and implicit existential themes in their clients’ stories and in the therapeutic relationship. Humanistic and existential therapy trainings typically let the trainees work through their own existential issues, and by doing that—often in a group context—trainees develop not only a larger awareness of existential themes as such (Krug & Schneider, 2016; Vanhooren, 2018). Trainees also learn to make sense of their existence, learn how to communicate their empathy better by having more vocabulary to talk about existential themes, and tend to feel more grounded to resonate with the existential concerns of their clients (Krug & Schneider, 2016; Vanhooren, 2018). With the EEQ, specific research could be performed to delineate whether these and/or other aspects of therapy training indeed contribute to more existential empathy.
Furthermore, the EEQ could be used to study in which clinical settings, client populations, or cultural contexts the existential empathic capacities of therapists or health care workers would particularly contribute to clients’ outcome, well-being, and growth. Different settings, clients populations, and cultural contexts might also ask for a different understanding of the existential concerns and how existential empathy should be communicated. As a result, this might not only lead to a shift in how psychologists, therapists, counselors, and health care workers pay attention to the existential concerns of their clients. Awareness around the importance of the existential layer might also evoke a change in psychotherapy and counseling training as such. The EEQ can help to identify clinical situations where existential empathy might make a difference, as well as training variables that could specifically contribute to existential empathy.
Important limitations need to be taken into account. First, the current sample is restricted to Dutch speakers, so further research is needed to verify the psychometric properties of the EEQ among psychotherapists of other sociocultural backgrounds. Also, the English translation still needs to be validated. Moreover, recruitment was nonrandom and the survey was web-based, allowing for the risk of nonresponse bias and nonrepresentativeness of the target population. However, even within the target population, the results should not be generalized to any other sample of therapists or counselors without caution. As no information was gathered about sociodemographic characteristics (except for age and professional information), gender, and cultural and ethnic background, the sociodemographic composition of the sample is unknown. However, we do have information about the population we recruited from: The group of psychologists and psychotherapists and counselors in Flanders (Belgium) is predominantly Western European Caucasian, 93.4% is born in Belgium, and 83% female (Luyten & Jeannin, 2021). As empathy might be differently understood and expressed in different cultural contexts (Hoffman, 2020), and the experience of existential concerns might also culturally differ (Hoffman et al., 2009), the EEQ should not be automatically used in other cultural populations without considerable reflection and reconsideration.
Because all measures were self-report measures with high face validity, the current findings are also vulnerable to the risk of social desirability bias and to systematic differences in levels of self-awareness across the variables. This might have contributed to spurious correlations among measures as well as among items within the EEQ. Therefore, future research should control for social desirability bias to examine the sensitivity of the EEQ items and the robustness of the current findings (e.g., following King & Bruner, 2000). Finally, the interpretation and labeling of the component solution from the PCA are subjective in nature and therefore other interpretations of the constructs underlying each subscale might also be valid.
It is crucial to note that the current study does not confirm the factor structure of the EEQ. This is only possible in a next step when confirmatory factor analysis (CFA) is performed (Kim, 2008). Therefore, to validate the EEQ, future research should apply a CFA in a different sample to evaluate the fit of the currently defined model and replicate the current results (Cabrera-Nguyen, 2010; Fokkema & Greiff, 2017). To clarify the conceptual interpretation of possible subscales and strengthen the construct validity assessment of the EEQ, future studies should examine the relationship between the separate scores on subscales and levels of personal distress, existential concerns, general empathy, experiential avoidance, and existential avoidance. Research should also investigate the mechanisms through which avoidance and overwhelming feelings might still coexist with high levels of resonance, presence, and communication in therapists. Another suggestion for future research is to explore the EEQ’s predictive validity using correlates of therapist empathy, and therapy outcomes over time with different patient groups (Elliott et al., 2018). Also, it should be noted that the authorized Dutch translation of the used TEQ was not validated. Further research on the EEQ should include (different) validated measures of general empathy.
Conclusion
The initial findings concerning the psychometric properties of the EEQ are promising. The EEQ appears to be a reliable instrument to assess self-reported levels of existential empathy among mental health professionals. However, additional research is needed to verify its psychometric properties and address the questions raised by this study. The clinical applicability of the EEQ lies in the possibility to examine whether and when existential empathy levels are related to treatment outcome, and to study the development of existential empathy during therapy training and throughout therapists’ and counselors’ careers. This could eventually inform clinicians on how to address their clients’ existential concerns and could help improve training programs and supervision.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.