
Abstract
Expectancy effects for many psychoactive substances appear to play a role in consumption, problematic use, subjective responses to acute administration, and subsequent effects. Expectancies of psychedelics have received little attention in published research despite their reputation for creating dramatic changes in subjective state. Psilocybin-assisted treatment (PAT) improves depression, but details of associated expected effects remain incomplete. Previous work suggests that PAT-induced changes in depression and other forms of well-being covary with specific subjective effects of psilocybin. Self-reports from over 500 psilocybin-using individuals revealed correlations with relevant subjective effects that appeared to mediate antidepressant effects in previous work (e.g., Mystical Experiences, Ego dissolution, and Emotional Breakthrough). Correlations with demographic variables, current depressive symptoms, and general hallucinogen involvement were markedly smaller. Expectancies on specific depressive symptoms also paralleled retrospective reports of other psychedelic-induced antidepressant effects. Regression revealed that current depressive symptoms, ego dissolution, and emotional breakthroughs accounted for unique variance in expected antidepressant effects, but expectancies on mystical effects did not. Although limitations suggest cautious interpretation, psilocybin-using individuals appear to hold relevant expectancies about subjective and antidepressant effects, which might play a role in treatment outcomes worthy of monitoring in clinical trials.
Keywords
Introduction
Psilocybin-assisted therapy has established antidepressant effects (e.g., Davis, Barrett, May, et al., 2021; see Goldberg et al., 2020; Luoma et al., 2020; Romeo et al., 2020 for reviews). Clinical depression, characterized by hopelessness, worthlessness, and loss of joy or interest in activities, can have alarming costs for affected individuals and their loved ones. The disorder is common and difficult to treat. Worldwide prevalence estimates approach 300 million (World Health Organization [WHO], 2017). Lifetime prevalence in the United States is approximately 20% (Hasin et al., 2018), and global incidence has increased by nearly 50% in the last three decades (Liu et al., 2020). The conceptualization of depression as a medical problem leads to a narrow framework for treatment, notably antidepressant medications and cognitive-behavioral psychotherapy (Berra, 2021; Elkins, 2009). The most successful therapies frequently combine pharmacological and psychological interventions, with recovery rates of approximately 65% (Cuijpers et al., 2020), leaving definite room for improvement and highlighting the limitations of the medical model of depression and associated treatments (Cosgrove et al., 2020; Davies et al., 2010). Critics of available treatments often emphasize problems related to treatment adherence, side effects, attrition, and compliance. Many also stress that statistically significant improvements are often not clinically meaningful, and the impact on symptoms that matter most to clients often remains unknown (Earleywine & De Leo, 2020). In contrast, humanistic approaches emphasize outcomes related to developing self-actualization, personal insight, and acceptance that could mitigate suffering (Davies et al., 2010).
This predicament and other increases in mental health problems inspired a re-emergence of research on psilocybin-assisted therapy, which appears to evoke improvements in depression through relational and insightful processes consistent with humanistic frameworks (see Carhart-Harris et al., 2016, 2018; Penn et al., 2021; Schenberg, 2018). This treatment often includes preparatory sessions to build rapport with facilitators, followed by the repeated administration of a psychoactive dose. Clients ingest the drug in a comfortable, soothing physical space accompanied by the facilitators (or “guides”), wear eyeshades to block distractors and listen to music. Follow-up sessions address making sense of the drug’s subjective effects to enhance benefits (see Johnson et al., 2019, for a detailed review). Initial trials show considerable promise (see Luoma et al., 2020), but criticisms remain. Most have been designed to establish safety and feasibility rather than provide generalizable estimates of effect sizes. Historically samples are small and potentially limited, though notably, recent investigations have recruited or pooled larger samples (Goodwin et al., 2023; Vargas et al., 2020). Some long-term follow-ups are evident, yet many studies do not have follow-up data after the completion of the study or report on outcomes less than a year following the study (Agin-Liebes et al., 2020; Carhart-Harris et al., 2018; Majić et al., 2015; Ross et al., 2016). A clearer understanding of the mechanisms underlying the improvement might help enhance the treatment.
Psilocybin-assisted therapy’s antidepressant effects likely arise from multiple factors. Findings underscore a path between the treatment and relief from symptoms: the subjective effects of psilocybin. Mystical experiences (characterized by mystical-type experiences, positive mood, transcendence, ineffability), ego dissolution (dissolution of self, self-importance, and identity), and emotional breakthroughs (overcoming negative affect and challenging memories in a way that leads to a sense of closure) all precede improvements apparently induced by psychedelics (e.g., Barrett et al., 2015; Carhart-Harris et al., 2017; Garcia-Romeu et al., 2019; Nour et al., 2016; Roseman et al., 2018, 2019). Note that changes in other subjective states fail to predict improvements in depression, supporting the validity of mystical, ego dissolution, and emotional breakthrough experiences. For example, acute ketamine-induced dissociation, though a novel change in subjective experience, does not predict subsequent antidepressant effects in other substance-assisted treatments (Mathai et al., 2020).
Given the inherent costs of clinical trials, a first step toward addressing potential mechanisms might benefit from work with large samples addressing expectancies. Expectancies are beliefs about a substance’s effects (Rauch & Bryant, 2000). Extensive work in both drug-related and psychotherapy research supports the import of relevant expectations. Classic and modern research reveals that alcohol expectancies covary with real-world drinking behavior (Brown et al., 1980) and reactions after acute administration (King et al., 2019). Expected effects of prescription stimulants (as well as cannabis) covary with relevant use and negative consequences as well (Holt & Looby, 2018; Waddell et al., 2021). The role of expectancies in psilocybin-assisted treatments is presently unclear. In addition, expectancies for therapy can contribute to outcome. Expectations related to efficacy and credibility of treatments account for meaningful variance in progress in diverse areas. Research on placebo responses supports the importance of expectancies in psychotherapy outcomes, particularly in depression (e.g., Renaud et al., 2013). Generally, clients who believe a treatment will work show the greatest gains (Wampold et al., 2005). Meta-analytic results suggest that patient outcome expectancies predict improvement (Constantino, Coyne, & Boswell, 2018; Constantino, Visla, et al., 2018). Years of comparable work have inspired a model of psychotherapy that relies upon enhancing expectations of outcome to facilitate treatment (Doering et al., 2018). In a sense, the impact of some psychoactive drugs and psychotherapy experiences stem, in part, from individual expectations about their effects, much like other learning experiences and behaviors, which have proven relevant in animals and humans (e.g., Bolles, 1972; Tolman, 1932). Importantly, psychological insight derived from psychedelic use may also be linked to improvements such as psychological flexibility and quality of life (Davis, Barrett, So, et al., 2021).
Ideally, expectancies for PAT would function in ways that parallel established findings in the field. Links with the expected subjective effects mentioned above might support their validity. In addition, symptom-specific expectancies might offer additional support. Although most work on the impact of psychedelics on depression focuses on total scores of established measures of symptoms, at least one study linked another 5-HT psychedelic, ayahuasca, to specific symptoms, suggesting that people experience more relief for some symptoms than others. Participants who participated in ayahuasca ceremonies retrospectively reported that the brew created more of an impact on affective symptoms like hope and depressed mood than vegetative symptoms like motivation and sleep (Gilbert, Earleywine, Mian, et al., 2021). By extension, specific PAT expectancies might help rule out alternative explanations related to a general positive attitude toward psilocybin, hopes related to current depressive symptoms, or a history of involvement with psychedelics more broadly. Those who view psychedelics as some sort of panacea might claim that these drugs alter all depressive symptoms rather than some but not others. Furthermore, expectancies of psychedelics might differentially impact the subjective effects related to their use. For example, mystical experiences may be a product of neurally derived networks with some potential to be modulated by benefit enhancement strategies, while other effects such as emotional breakthrough might be more susceptible to expectancies (Barrett & Griffiths, 2018; Lancelotta & Davis, 2020).
Thus, we examined expected effects of PAT on individual self-reported depressive symptoms and for relevant psilocybin-induced subjective effects like mystical, ego dissolution, or emotional breakthrough responses. We also examined lifetime psychedelic use, depression, and various demographic measures. While we did not have specific hypotheses regarding which depression symptoms might specifically be expected to be improved by PAT, we hypothesized that psilocybin’s expected effects on depression would vary across symptoms and covary strongly with subjective effects but show less covariation with lifetime psychedelic use, current depressive symptoms, and demographic measures. We chose subjective effects based on previous work supporting the import of mystical experiences, ego dissolution, and emotional breakthroughs (Carhart-Harris et al., 2017; Nour et al., 2016; Roseman et al., 2018, 2019).
Method
Participants
We recruited from MTurk, Amazon’s work platform, where individuals volunteered for the study and completed an informed consent to participate. A total of 551 (268; 48.6% Female) participants had used psilocybin at least once, consented, had unique IP addresses, and passed attention check items, potentially improving the quality of data from this source (Agley et al., 2022; Mellis & Bickel, 2020). The survey appeared on Qualtrics. Ages ranged from 18 to 73 (Mean = 34.84; SD =10.67). Skew for age was above acceptable standards (.90; Osborne, 2013), but a log transformation corrected skewness to .56. Most participants identified as White (423; 76.8%), followed by Latinx (41; 7.4%), African descent (40; 7.3%), Asian/Pacific Islander (27; 4.9%), multiracial (9; 1.6%), Native American (8; 1.5%), and other (3; 0.5%). The modal educational status was a Bachelor’s degree (208; 37.7%) with some College (142; 25.8%), Associates degree (68; 12.3%), High School Diploma (58; 10.5%), Advanced degree (49; 8.9%), some graduate school (14; 2.5%) and some High School (12; 2.2%) also represented. All procedures were in accordance with and approved by the university's Institutional Review Board.
Procedures
Participants who consented to participate went on to complete the survey (measures detailed below). Briefly, participants self-reported their depression symptoms (CES-D) and lifetime use of psychedelics. Participants then responded to a brief vignette on PAT and responded to an adapted version of the CES-D framed to provide their expectancies of how PAT could affect different symptoms of depression. Finally, participants completed inventories for emotional breakthrough, mystical experiences, and ego dissolution for their own personal experiences with psilocybin.
Measures
Current Depression
Participants completed the 10-item short form of the Center for Epidemiological Studies-Depression scale (CES-D 10; Andresen et al., 1994), an index of symptoms in the previous week rated on a scale from 0 “Rarely or none of the time (Less than 1 day)” to 3 “All of the time (5–7 days).” Psychometric properties were comparable to other samples (González et al., 2017; Cronbach’s alpha = .71. Mean = 15.499, SD = 5.736; Range: 4–30; Skew = .165).
Expected Antidepressant Effects of Psilocybin-Assisted Psychotherapy
Development of vignette followed comparable methods assessing perceived credibility and antidepressant effect of various treatments, including psychotherapy and psychedelic-assisted therapy, which provide a low-burden and convenient assessment of substance use beliefs (Altman et al., 2022; Earleywine et al., 2022; Gilbert, Earleywine, & Mian, et al., 2021). Participants responded to this item: “Recent research used psilocybin, the active ingredient in hallucinogenic mushrooms, as part of a treatment for depression. The clients got to know the support team, learned what to expect from the psilocybin experience, and discussed any concerns to prepare. Then they came to the laboratory for the two psilocybin sessions, which were one week apart. Clients wore eyeshades and stretched out on a comfortable sofa to listen to music while the psilocybin took effect. The support team was there to offer reassurance, emphasize safety, and encourage clients to look inward and attend to their experience. Then clients met with the support team to discuss their experiences, share insights, and talk about ways to cultivate changes in their outlook and lifestyle.” Clients then rated how much impact they thought this approach would have on depression on adapted version of CES-D with the stem: “How much do you think a psilocybin session could affect each of the following?” Participants rated expected impact on each CES-D item from −50 (“Affects very negatively”) through 0 (“No effect”) to +50 “(Affects very positively”). Items were adapted to be framed as expectancies (e.g., “feeling fearful”; “feeling bothered by things that don’t usually bother someone.”) Internal consistency across the 10 items (Cronbach’s alpha) was .88 and would not increase if any items were deleted. Skew was –.23. Average scores per item ranged from −50 to +50, with a mean of 16.64 (SD = 15.50).
Lifetime Hallucinogen Involvement
All participants endorsed using psilocybin at least once. Participants estimated the number of times they had used LSD, MDMA, Psilocybin, DMT, Salvia, Peyote, Mescaline, PCP, MDMA, Ketamine, Ibogaine, DOT, and Ayahuasca across their lifetime as a measure of familiarity with drugs like psilocybin. The sum across all drugs ranged from 1 to 3,060 (Mean = 46.31; SD = 190.32) with a high positive skew (13.05) that decreased to an acceptable level (.424) with a log transformation (Osborne, 2013). Comparable analyses focusing on psilocybin exclusively showed even smaller effects than those reported here.
Subjective Effects
We used multiple indices (mystical experiences, emotional breakthrough, and ego dissolution) as detailed below.
Mystical Experiences (MEQ)
The MEQ has been revised since its original conception and now includes 30 questions (MacLean et al., 2011) with an accepted four-factor structure in English (MacLean et al., 2012). The MEQ asks participants to respond with the following scale: 0—none; not at all, 1—so slight cannot decide, 2—slight, 3—moderate, 4—strong (equivalent in degree to any other strong experience), or 5—extreme (more than any other time in my life and stronger than 4). Internal consistency was acceptable (Cronbach’s alpha = .97) and would not improve meaningfully by deleting an item. The average item score ranged from 0–5 (Mean = 3.12, SD = 1.07; skew = −.58). Typical items included a sense of being at a spiritual height and a sense that the experience cannot be described in words or was an experience of ecstasy.
Emotional Breakthrough (EB)
Participants rated the 6 items of the Emotional Breakthrough Scale, which account for unique variance in psychedelic-induced changes in well-being (Roseman et al., 2019) from 0 (“not at all”) to 100 (“very much”). Typical items include: “I achieved an emotional release followed by a sense of relief,” and “I faced emotionally difficult feelings that I usually push aside.” Cronbach’s alpha was .93. Average score per item ranged from 0 to 100 (Mean = 62.50, SD = 23.51; skew = −.43).
Ego Dissolution Inventory
Participants rated the 8 items of this scale (Nour et al., 2016) from 0 (“not at all”) to 100 (“very much”), including “I lost all sense of ego” and “I experienced a decrease in my sense of self-importance.” ED predicted greater improvement in depression in previous work (e.g., Carhart-Harris et al., 2017; Garcia-Romeu et al., 2019). Cronbach’s alpha was .91. Average scores per item ranged from 0–100 (Mean = 56.86, SD = 22.96; skew = −.25).
Data Analytic Plan
Given the large sample and numerous analyses, we designated p < .001 to interpret statistical significance. Visual inspection as well as P–P plots suggested normal distributions, so we focused on parametric approaches. We used Welch’s t-tests for independent two-group comparisons to sidestep potential problems with unequal variances (Delacre et al., 2017) and paired t-tests for dependent two-group comparisons. To examine the symptom specificity of psilocybin, we computed index variables of most and least affected symptoms based on previous work (Gilbert, Earleywine, Mian, et al., 2021) and examined correlations between ranks of symptoms in these data and those reported previously. Univariate outliers did not appear after corrections for skew. Three multivariate outliers (detected based on Mahalanobis Distance) were omitted for regression analyses.
Results
Demographic Effects
We examined links among Age, Sex, Education, and Ethnicity with the dependent and independent variables. Transformed Age showed small (<|.17|) but significant correlations with Hallucinogen Involvement and Mystical Experiences (see Table 1). Men (n = 278) and women did not differ significantly on any measures, Cohen’s d’s < .10. Those with a Bachelor’s degree or more (n = 271) did not differ significantly from others (n = 280) on any measure, Cohen’s d’s < .22. The small number of people of color required a split between White (n = 413) and non-White groups. No comparisons between these groups reached statistical significance, all Cohen’s d’s < .21.
Correlations Among Age, Hallucinogen Involvement, Subjective and Expected Antidepressant Effects.
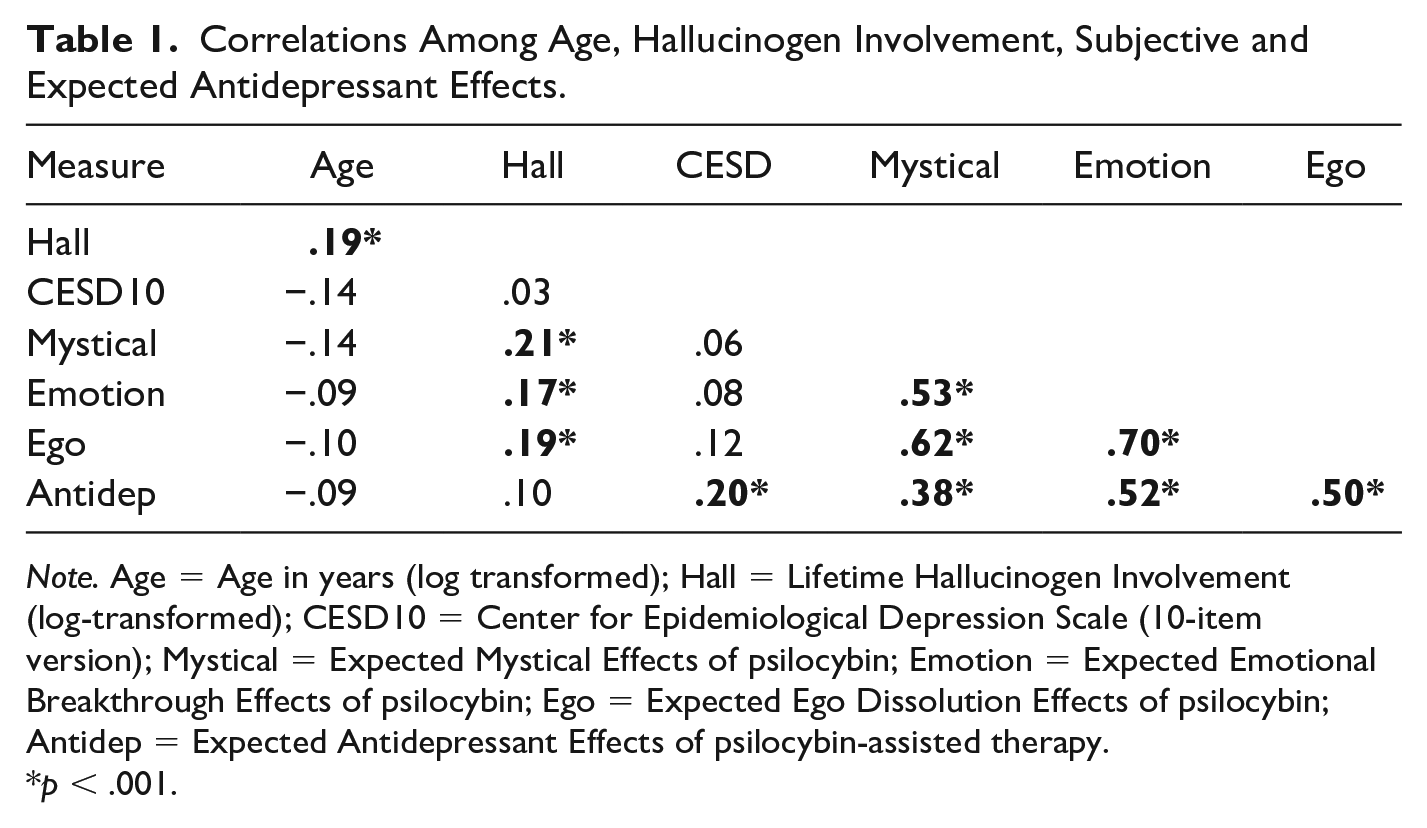
Note. Age = Age in years (log transformed); Hall = Lifetime Hallucinogen Involvement (log-transformed); CESD10 = Center for Epidemiological Depression Scale (10-item version); Mystical = Expected Mystical Effects of psilocybin; Emotion = Expected Emotional Breakthrough Effects of psilocybin; Ego = Expected Ego Dissolution Effects of psilocybin; Antidep = Expected Antidepressant Effects of psilocybin-assisted therapy.
p < .001.
Correlations
Correlations among all variables (transformed when appropriate) appear in Table 1. Hallucinogen Involvement showed small (r < .22) but statistically significant links to subjective and expected antidepressant effects. Subjective effects generally correlated with each other (r = .53 to 78) more than with expected antidepressant effects of psilocybin (r = .38 to .52) and still less with hallucinogen involvement (r = .17 to .21). For example, a comparison among the correlated correlation coefficients (Meng et al., 1992) revealed that the smallest link between expected antidepressant effects and a subjective effect (Mystical; Pearson’s r = .38) exceeded the largest correlation with any other variable (current depressive symptoms; Pearson’s r = .20), t (547) = 3.31, p < .001.
Symptom Specificity of Expected Antidepressant Effects
Using two discrete methods, we examined how expected antidepressant effects might differ for specific depressive symptoms. For our first approach, we conducted a paired t-test to compare the average of the depressive symptoms most expected to be impacted by psilocybin compared to symptoms expected to be least impacted. We formed two indices based on the individual items that were most and least affected in previous work on psychedelic (ayahuasca) and depression (Gilbert, Earleywine, Mian, et al., 2021). Their data suggested that respondents reporting about an ayahuasca experience expected five CES-D items to improve most, including Hopeful (reverse scored), Depressed, Happy (reverse scored), Fearful, and Effort. In addition, they expected less impact for the five others: Bothered, “Get going,” Focus, Lonely, and Sleep disturbance. We formed indices using the same items and found that they differed in our sample as well: mean difference = 7.80, SD =11.80; Paired t (550) = 15.51, p < .001; Cohen’s d = .66.
For our second approach, we compared the present data with previously published ranked expectancies of antidepressant effects using an ordinal correlation. That is, the most impacted item (Hope—reverse scored) in the previous paper (Gilbert, Earleywine, Mian, et al., 2021) received a rank of one, the second-ranked symptom (Fearful) received a two, and so on. Spearman’s rho for the rank order of symptoms was .733, which did not reach statistical significance given our focus on p < .001 (p = .016), likely due to the small number of symptoms, which served in the computation of degrees of freedom (10). Nevertheless, the ranks accounted for 53.78% of the variance in the previous ranks (Cohen’s classic classification of effect sizes lists any r over |.5| as large (Cohen, 1992)).
Predicting Expected Antidepressant Effects
Participants reported on their depression severity through the CES-D and then reported on their belief of psilocybin’s impact on each depression symptom through an adapted version of the CES-D. Average scores per item on adapted CES-D ranged from −50 to +50 with a mean of 16.64 (SD = 15.50. d = 1.07), indicating the average expected antidepressant of psilocybin. We regressed the significant covariates (age and hallucinogen involvement) and expected subjective effects on expected antidepressant effects. After the removal of the multivariate outliers, outlier diagnostics were all acceptable (all VIFs < 2.4, and no Tolerance < .42). Standardized coefficients and associated t-tests appear in Table 2. Only Emotional Breakthrough and Ego Dissolution remained significant among the predictors.
Antidepressant Expectancies of Psilocybin Regressed on Depression Symptoms, Emotional Breakthrough, Ego Dissolution, and Mystical Experiences.
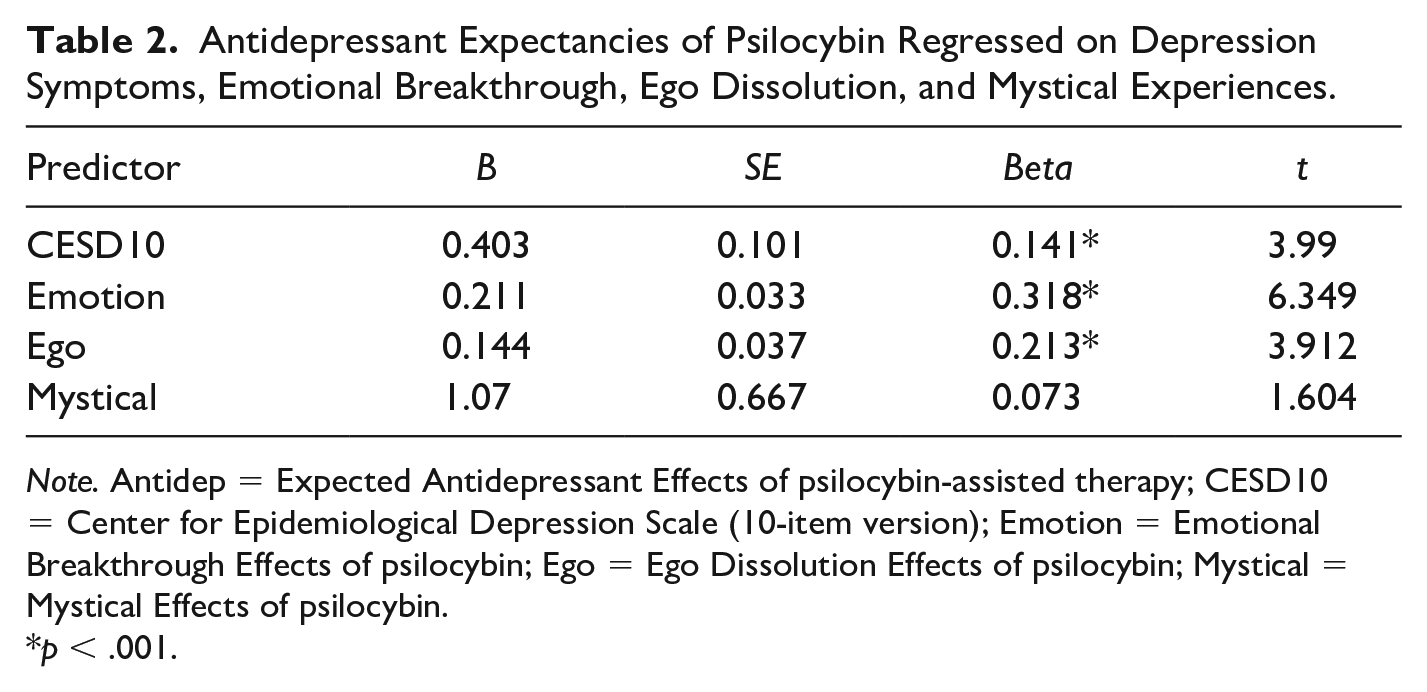
Note. Antidep = Expected Antidepressant Effects of psilocybin-assisted therapy; CESD10 = Center for Epidemiological Depression Scale (10-item version); Emotion = Emotional Breakthrough Effects of psilocybin; Ego = Ego Dissolution Effects of psilocybin; Mystical = Mystical Effects of psilocybin.
p < .001.
Discussion
Clinical depression is ubiquitous (WHO, 2017) and on the rise (Liu et al., 2020). Available treatments often leave at least one third of clients without meaningful improvement (Cuijpers, 2017). Psilocybin-assisted therapy for depression has shown considerable promise in multiple clinical trials, even with clients labeled “treatment resistant” because two or more interventions failed to help them decrease their symptoms sufficiently (see Goldberg et al., 2020; Luoma et al., 2020; Romeo et al., 2020). Most trials include extensive support from trained guides, multiple meetings with staff, and multiple psilocybin-administration sessions. The quest to understand the underlying mechanisms has generated support for important contributions from the subjective effects of psilocybin, particularly experiences involving contact with facets of the mystical, a dissolution of the ego, and emotional breakthroughs. As these experiences increase, so do the ameliorative effects (Carhart-Harris et al., 2017; Nour et al., 2016; Roseman et al., 2018, 2019). In contrast, empirically validated cognitive behavioral or pharmacological interventions for depression rarely address potential mechanisms related to mystical experiences, ego dissolution, or emotional breakthrough, often related to the medical conceptualization and treatment of depression (Cuijpers, 2017; Davies et al., 2010).
We assessed expected antidepressant effects of psilocybin-assisted therapy as well as demographics, lifetime hallucinogen involvement, and alterations on mystical, ego dissolution, and emotional breakthrough effects. Over 500 individuals who used psilocybin responded to a vignette of PAT followed by a scale of depression symptoms adapted for assessing expectancies of psilocybin’s antidepressant effects. Participants reported anticipating that PAT’s antidepressant effects would exceed effect sizes established as clinically significant (1.07 vs. the .875 established cut-off), which also exceeds meta-analytic summaries of the impact of antidepressant medication (.3; see Hieronymus et al., 2020) and psychotherapies that do not include a psychedelic component (.58 to .83; see Cuijpers, 2017). Their expected antidepressant effects also covaried with psilocybin-induced changes in subjective effects, including mystical, ego dissolution, and emotional breakthrough reactions. A regression revealed that only effects on ego dissolution and emotional breakthroughs accounted for unique variance in expected antidepressant effects when all variables appeared in the equation. The significant link between mystical experiences and expected antidepressant effects dropped to nonsignificance with ego dissolution and emotional breakthrough in the equation. Perhaps the covariation between mystical experiences and antidepressant effects stems from associated opportunities to express emotion or take one’s ego less seriously.
Although the data have meaningful limitations addressed below, these results suggest that expected antidepressant effects vary with subjective effects in ways that parallel established work in clinical trials. At least in the minds of psilocybin-using individuals, the impact of mystical experiences on depression might be mediated by other subjective effects. Limitations in the current data underscore the need for more research on the expected effects of psychedelics on subjective experience and various forms of human suffering, including maladaptive consumption of alcohol and nicotine, anxiety, and depression (see Thomas et al., 2017) and angst related to end-of-life concerns (Yu et al., 2021). The current study focused on only three forms of psilocybin-induced changes in subjective state (mystical, ego dissolution, and emotional breakthrough), but not promising additional subjective changes related to psychological insight (Davis, Barrett, So, et al., 2021) and awe (Hendricks, 2018), among others. Debate about the necessity of these subjective changes for therapeutic effects continues (D. E. Olson, 2021; Yaden & Griffiths, 2021), but expectancies covary such that previously-using individuals who expect larger subjective changes also expect greater antidepressant effects. An examination of a broader set of potential subjective effects could prove illustrative. In addition, mystical experiences, ego dissolution, and emotional breakthrough might have conceptual overlap or contribute to overlapping constructs, such as positive affective changes. These likely contribute to the antidepressant effects of PAT and warrant both further research and consideration in the conceptual understanding of these processes. Extending from antidepressant effects to expected impacts on the symptoms of other disorders or measures of well-being might also reveal more about the way people expect subjective and therapeutic effects to covary.
Limitations
Limitations related to sampling and data collection are also worthy of note. Replication with a large, diverse sample would help establish the generalizability of these results. We chose MTurk sampling given its advantages in recruiting nationally-representative individuals who endorse higher rates of depression (Walters et al., 2018) and who use substances that typically have lower base rates in the community (Mellis & Bickel, 2020; Strickland & Stoops, 2019), and Mturk’s use in prior similar work (Altman et al., 2022). Alternative data collection procedures might have different limitations but might provide access to more underrepresented groups. We had few people of color in our current sample, which was nearly 3/4 White. Poor diversity has plagued psychedelics research, particularly in investigations of therapeutic potential (Williams & Labate, 2019). Alcohol expectancies and their links to drinking behaviors can vary with ethnicity (Banks et al., 2020). In the United States, consumption of psychedelics appears more often in White and Mixed-Race groups compared to those who report Black/African American descent (Jahn et al., 2021), suggesting that perhaps these groups hold different expectancies of psilocybin’s subjective and therapeutic effects. Examination of this study in a clinical sample of individuals screened for depression might also prove useful; given the novelty of this current work, recruiting from a convenient community sample provided preliminary findings that will be useful for this kind of future work.
Individuals who have more experience with psilocybin might hold different expectancies for PAT, though past use had only weak associations with subjective effects and no association with antidepressant expectancies. We focused only on those who had used psilocybin at least once, but those who did not use psilocybin might also have expectations about psilocybin’s impact as well. People appear to develop expectancies about alcohol’s effects prior to consumption, potentially based on various aspects of social learning. These expectancies appear to account for links between established predictors and subsequent use of alcohol (Smit et al., 2018). Expectancies of prescription stimulant effects also appear in those who have never consumed the drugs and distinguish between those who are at risk for misuse (Holt & Looby, 2018). Individuals who do not use psilocybin might have varied exposure to other individuals who use, related media depictions, personality differences, or different personal histories with comparable drugs, which might explain their expected effects. This consideration also highlights the long-standing challenges around placebo controls currently facing clinical trial work with psychedelic therapies. The role of expectancies in the placebo effects of psychedelics is not fully understood. Expectancies have the potential to drive therapeutic outcomes, and given the difficulties with developing robust controls in clinical trial work, other methods of assessing expectancy effects are much needed.
The current methodology asked participants to report expectancies of psilocybin based on a hypothetical experience with PAT, which offers a preliminary understanding of the role of psychedelic expectancies in treatment and is consistent with similar work examining the role of perceived effects of substances and psychotherapy (Altman et al., 2022; Earleywine et al., 2022; Gilbert, Earleywine, & Altman, 2021). Given the limitations of this method, which is consistent with any self-report measure, future work is needed to extend these findings beyond self-report and examine expectancies in acute states in the context of PAT.
We also do not know the actual correlations between effects and genuine experiences after acute administration, suggesting that drug administration trials might assess expectancies prior to an assessment of drug responses. Expected and pharmacological effects correlate significantly with stimulant and sedative properties of alcohol (King et al., 2019), but comparable data with other drugs and other effects have not received much attention in the published research literature. Psilocybin’s effects might be less dose-dependent or correlated with gender (Garcia-Romeu et al., 2021), but the legendary links between set, setting, and reactions to psychedelics might suggest vast ranges in expectancies as well (Hartogsohn, 2017). Set and setting factors invariably play a role in both forming expectations and experiencing the subjective effects of psilocybin and other psychedelics (Gukasyan & Nayak, 2022; Hartogsohn, 2016; J. A. Olson et al., 2020). Future work is required to examine the role of set and setting alongside the nuanced links between expectancies, (which speak generally to formed beliefs about a substance’s effects), and predicted effects, (which would be specific to those who are in an active state of use). Despite the limitations emphasized above, these data suggest that psilocybin-using individuals do hold expectancies for subjective effects of the drug as well as for psilocybin-assisted therapy’s impact on depression.
Footnotes
Author Contributions
ME collected the data, designed this research, analyzed the data, and drafted the original manuscript. MNM collected the data and reviewed and edited the manuscript. JDL designed the research, reviewed analyses, and reviewed and edited the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Mian is supported by the National Institute on Drug Abuse, Award Number T32DA007250.