
Abstract
Despite decades of research, psychiatric pharmacotherapy remains limited in its clinical effectiveness and understanding of therapeutic mechanisms. Dominant approaches, rooted in symptom-scale-driven randomized controlled trials (RCTs) and biological reductionism, often fail to capture the complex, subjective, and context-dependent nature of psychotropic drug effects. In this article, we outline a novel methodology – First-Person Psychopharmacology (1PPP) – which integrates the rigor of RCTs with qualitative, idiographic methods to explore the lived experience of medication use. 1PPP centers on how psychoactive substances alter consciousness, emotion, and behavior in real-life contexts, with attention to personal meaning, social situation, and narrative frameworks. The method employs a mixed-design with multiple experimental groups, semi-structured interviews, and interpretative and quantitative analyses. By emphasizing subjective experience and its interaction with set and setting, 1PPP offers a more ecologically valid and person-centered alternative to current paradigms. We discuss the epistemological, methodological, and practical challenges of implementing 1PPP, while highlighting its potential to improve drug evaluation, clinical guidelines, and psychiatric care. We argue that putting the psyche back into psychopharmacology is essential for advancing a humanistic, context-sensitive, and scientifically robust understanding of psychiatric medications.
Introduction
Rose (2016) argues that the crisis in which psychiatry is currently mired has three core aspects:
Diagnosis: the unsatisfactory reliability, validity, and coherence of the nosological entities by which the profession chooses to describe the suffering of the people whom they treat;
Explanation: the attempt to understand why a particular person suffers in a particular way;
Therapeutics: The effort to alleviate people’s suffering, with maximum effectiveness and minimum side effects.
These three aspects are interrelated and shape each other: the heterogeneity of diagnostic categories feeds the failure of the search for reliable neurophysiological explanations or biomarkers for specific diagnostic categories, which drugs or other therapeutic interventions could then address. In turn, while the number of people using psychiatric drugs is growing, their effectiveness remains low and has probably not improved in the past 70 years (Hyman, 2012; Leichsenring et al., 2022). We may be dealing with a treatment-prevalence paradox (Ormel at al., 2022), where, despite growing access to and utilization of supposedly effective treatments, the number of people dealing with mental health problems has not diminished and may even be growing (Davies et al., 2023; Jorm et al., 2017; Mulder & Jorm, 2023). In the case of people diagnosed with schizophrenia, despite more treatment, and “[a]s we become better at detecting and treating the core symptoms of schizophrenia,” the mortality gap may actually be growing, a troubling paradox indeed (Saha et al., 2007, p. 1129).
Thinking in terms of matching the “right” DSM or ICD diagnosis with the “right” medication assumes a neurobiological and categorical paradigm, which harks back to late 19th century Kraepelinian approaches, and continues to underlie much contemporary research and practice, may be hampering clinical progress (Belmaker & Lichtenberg, 2023; Campolonghi & Orrù, 2023; Deacon, 2013; Dumas-Mallet & Gonon, 2020; Ghaemi, 2022; Van Os & Guloksuz, 2022). The dominant reductionist approaches to the role of neurobiology in psychiatry prioritize the analysis of brain mechanisms, at the expense of an understanding of the whole living organism in its milieu, and the interpersonal, social or even economic processes which shape neurobiology from the moment of conception (Breggin, 2003). Likewise, in the dominant approach to psychopharmacology, the pharmacological agent and its effects are usually understood and explained as neurophysiological changes at the level of the transmitter, which eventually may be expressed as a change in results on measurement scales supposedly addressing symptoms of specific disorders.
Some of the problems inherent in the current paradigm are highlighted by the current “psychedelic renaissance” that is, the revival of interest in using various substances labeled as psychedelics for therapeutic purposes in institutional psychiatry. These problems include lack of control groups, spin, outcome switching, multiple testing, financial conflicts of interest, lack of proper reporting standards for adverse events, small samples, statistical problems, lack of long-term outcomes, breaking the blind and placebo effect. Methodological and measurement problems are also aggravated by the fact that the therapeutic mechanisms of these drugs are poorly understood (Van Elk & Fried, 2023).
This situation is associated with the controversies regarding the approval of esketamine or MDMA-assisted therapy (Horowitz & Moncrieff, 2021; Lemarchand et al., 2024; Turner, 2019). The impact of the therapy component on the efficacy of psychedelic drugs, the inseparable connection between the patient, the pharmacological agent and the context in which it is used (or “set and setting” and broadly defined placebo effect and other non-specific factors), proves to be a difficult theoretical, methodological and practical problem to solve, and may suggest that, in fact, research and practice regarding other drugs used in psychiatry faces similar problems as these effects may substantially alter efficacy of pharmacological treatments (Pronovost-Morgan et al., 2023). The “psychedelic renaissance,” while highlighting these problems, may create a window of opportunity to rethink psychopharmacology and psychiatry (Stupak, 2025).
The disappointing results of the dominant paradigm, and other methodological problems outlined above, may suggest that a reconsideration of psychopharmacology is necessary. Even though the effects of psychoactive substances are undeniably mediated by their biological mechanisms of action, a better method for advancing our understanding of drug action and harnessing their potential might be to shift the attention toward the subjective (first-person) experiences of the person receiving the medication (Belmaker & Lichtenberg, 2023). In this context, we’d like to propose a tentative outline of a First-Person Psychopharmacology (1PPP) that could provide results informing guidelines and clinical practice and lead to a more effective and safer utilization of drugs.
We will first outline the main problems with the dominant paradigm in psychopharmacology, then briefly present some qualitative evidence regarding the effects of psychiatric drugs, and sketch the program and methodology of 1PPP next. We will then discuss possible limitations and challenges of the proposed approach.
Problems With the Dominant Approach
One source of the disappointing outcomes and lack of progress in psychopharmacology and psychotherapy might be the insufficient quality of many randomized controlled trial (RCT) studies. As with the prevailing response to the replication crisis, the solution would then be to increase the methodological rigor of the studies, use preregistration, counteract questionable research practices or use different statistical approaches in order to better adhere to the RCT logic (Damen et al., 2023; Fidler & Wilcox, 2021; Hengartner, 2018; Stahl & Pickles, 2018; Studart et al., 2025). This response suggests that the prevailing paradigm is correct and we simply need to implement it better. On the other hand, as with the replication crisis, one could argue that the problems are more fundamental than that and are related to some of the basic epistemological assumptions of the model (Brailas, 2025), so that “more of the same” or “doing the same, but better” won’t address them properly.
Although RCT design relying on symptom scales is usually presented as the best available method of studying drug efficacy in psychopharmacology, there are many problems and biases inherent in such an approach that limit the generalizability and transportability of the results outside of the study conditions, for example, low external validity (Harrer et al., 2023; Healy, 2009; Moncrieff, 2009; Mulder et al., 2018). Heterogeneity of studied populations, related to the heterogeneity of diagnostic categories, as well as heterogeneity of treatment effects or the impossibility of distinguishing between a drug’s action on the “disorder” and its supposed mechanisms and the subjective state the drug produces regardless of the supposedly underlying disorder, may be some of the most important problems in the context of psychopharmacology.
Similar problems may be present in relation to psychotherapy outcome research. RCT design in psychotherapy assumes, as with pharmacological research trials, a nomothetic approach, whereby one seeks general laws common to the varied individuals to whom these laws are applied. This approach relies on the assumption of ergodicity (homogeneity between and within individuals), while data suggest that that group-derived estimates are not accurate proxies of individual processes (Fisher et al., 2018) and it may be more sensible to view lived experience (i.e., the actually lived-through states and experiences) as non-ergodic (Speyer & Ustrup, 2025). Precision psychiatry, which in fact relies on many of the same fundamental assumptions of the dominant psychiatric paradigm and employs a nomothetic approach, may be unable to overcome these problems (Van Os & Kohne, 2021). An idiographic approach, which focuses on the unique individuals who suffer and seek succor, might be the more appropriate method to understand outcomes (Dunlop & Medeiros Da Frota Ribeiro, 2022; Erwin, 2006; Gupta, 2007; Hayes et al., 2022; Seligman, 1995; Shean, 2014). The nomothetic approach is traditionally associated with natural sciences, while the idiographic one is closely related to humanistic psychology (Gross, 2023).
Moreover, statistically significant differences between groups may not translate to clinically meaningful ones (Hengartner & Plöderl, 2018). As there is no way to assess the severity or improvement through an objective laboratory analysis, and in light of the many limitations of the scales, some researchers propose shifting to “hard outcomes” such as suicide attempts, hospital admissions, employment status, criminal convictions, reliance on social benefits, or educational completion (Juul et al., 2024). However, these outcomes, though crucially important, may be hard to tie down to specific drug effects or mechanisms and/or difficult to disentangle from many other social circumstances or individual factors.
The quantitative nature of the outcomes produced by symptom scales is another major limitation related both to the purely statistical level of analysis, for example, the supposedly additive and continuous nature of variables, as well as to the question of whether numerical values, often assigned in a social situation from a subjective second-person perspective or a supposed third-person one, can adequately represent the experience and the meaning of the first-person phenomena (i.e., not accessible directly by anyone else) they purport to measure (Gupta, 2007; Ingleby, 1980; Kępiński, 1978; Stupak & Dobroczyński, 2021; Uher, 2003). This problem is related to the many scientific, epistemological, methodological and conceptual problems related to psychometrics and “measuring the mind” (Borsboom, 2005). Thus, imposing the logic of numbers and defining change in quantitative terms may create a false sense of knowledge and obscure or even undermine the actual importance or quality of the patient’s experience (Gupta, 2007). What’s more, the numerical sum of items on a scale may consist of completely different elements, so the same numerical value for two different research subjects, though interpreted as an identical outcome, may in fact represent completely different experiences and severity (Stupak, 2025). This crucial qualitative difference is lost in a quantitative statistical analysis, which may hamper the validity of the finding.
The measurement scales are also somewhat arbitrary and may put undue weight on “symptoms” considered to be important by clinicians, relatives or society and undervalue or even completely overlook aspects of the experience or functioning that actually matter to patients themselves (Russo, 2018; Stupak & Dobroczyński, 2021). Emphasis on symptom change of predefined disorders in RCTs may thus inappropriately focus the attention and treatment goals away from those that actually matter to patients, such as improvements in quality of life, interpersonal relations and functional status (Zimmerman et al., 2012). Still, drug approval relies mostly on scales such as Positive and Negative Syndrome Scale, the Montgomery-Asberg Depression Rating Scale or the Hamilton Depression Scale (Ahn-Horst et al., 2025).
Mechanisms of action of psychiatric drugs, especially as they translate to beneficial clinical effects, are unknown, but the fact that drugs used in psychiatry have psychoactive effects that sometimes may be perceived as beneficial seems unquestionable. Since we are unable to precisely explain these effects mechanistically, especially in particular individuals, a more promising area of research may be to focus on studying the subjective states produced by drugs and if or how could these states offer relief or support when facing and overcoming different aspects of distress and difficult situations, and how these effects might translate into clinical benefit.
Some Qualitative Evidence to Date
Some qualitative evidence about the subjective effects that psychiatric drugs may produce already exists. The studies usually rely on qualitative methodology, interviews or surveys. Even though clinical qualitative research faces a biomedical discourse that constrains what counts as evidence, and accordingly the kind of research that gets funded, conducted, and published, the legitimacy of qualitative research seems to be slowly growing, also in the clinical and psychiatric contexts (Harper, 2017). Some of this research relates directly to studying the lived experience of people diagnosed with mental disorders and/or receiving pharmacological treatments (Fusar-Poli et al., 2022, 2023).
The action of neuroleptic drugs, beyond the neurophysiological level, may be described as a modification of cognition, emotion and motivation. A person is administered a medication, whether orally or parenterally. Some users will describe a distinctive state of lethargy, sedation, cognitive slowing, diminished concentration and clarity of thinking, emotional blunting, fatigue and reduced motivation. These may be associated with a variety of physical effects, which together are often described as profound, unpleasant, debilitating, and impaired functioning. Still, many of the same effects may be perceived as beneficial, reducing some of the distressing experiences or helping with insomnia (Thompson et al., 2020). The distinction between a “side effect” or “adverse effect” and a “therapeutic effect” is thus largely contextual, dependent on the framework employed (Stupak & Dobroczyński, 2021).
These effects are reflected by statements such as “I remember taking my first depot . . . and it absolutely knocked me out . . . I couldn’t even lift a dustpan and brush in that I didn’t have any movement in my arms, in my legs . . . I didn’t have any thoughts in my head. I couldn’t do anything . . . I was like a zombie” (Thompson et al., 2020, p. 117), or “On a personal note, ‘I hate my meds’. It makes me fat, depressed, lethargic. It strips my life and soul away.” (Salomon & Hamilton, 2013, p. 163). Other self-descriptions include “dopey,” “zonked,” “feeling like a cabbage” or “being hit by a truck” (Thompson et al., 2020).
Similarly, in the case of antidepressants, a number of users reported feeling “like a zombie” (Gibson et al., 2016). The emotional, motivational or cognitive blunting was reflected also by statements such as: “They don’t make the problems go away. They just make me numb enough to not give a shit” (Gibson et al., 2016, p. 3). Some described effects that were positive on the one hand, but on the other could be interpreted as undesirable changes in personality, for example, “I am a considerate and selfless person and while on the antidepressants I was the complete opposite” (Gibson et al., 2016, p. 4).
The first-person descriptions of drug effects can be grouped and categorized, and a number of themes, describing physical, cognitive, emotional and spiritual harm hindering recovery can be distinguished (Hagen et al., 2010). In the same way, qualitative data on drug effects could be grouped within themes and sub-themes resembling beneficial experiences. Some users report that reduction in symptoms helped them in restoring a sense of normality and autonomy, but many express a sense of resignation, endurance or loss of autonomy (Gibson et al., 2016; Maroun et al., 2018; Thompson et al., 2020). At the same time, some statements by the patients represent directly what they’ve been taught by medical professionals, even if it concerned controversial hypotheses that may negatively affect treatment, for example, “[Its] just like diabetes – a chemical shortage . . . I need serotonin uptake inhibitors – simple!”, or “My GP said that if I had diabetes I would need to take insulin forever, so not to worry that I appear to need to continue to take anti-depressants forever.” (Gibson et al., 2016 p. 3; Schroder et al., 2025). This example shows that it may be difficult to disentangle the first-person perception of drugs and their effects from socially shaped beliefs about drugs. This presents a challenge to be addressed in the methodology of 1PPP, also in the context of the placebo and nocebo effects and placebo control (Cundiff-O’Sullivan et al., 2023).
A somewhat similar problem concerns phenomenologically oriented research on the experience of “disorders” where the effects of drugs, the reified “disorders” and the convictions about them may be conflated. A phenomenological approach to psychopharmacology has been already proposed (Lopes & Messas, 2023), however, paradoxically, phenomenology comes with its own set of theoretical and epistemological assumptions, also regarding psychopathology. Moreover, there are rich and different phenomenological traditions, so rather than one phenomenology, we are dealing with different schools of phenomenology or different phenomenologies with lively debates about key issues and concepts (Stanghellini et al., 2019; Švec & Čapek, 2017; Thoma et al, 2022; Zahavi, 2015). Thus, rather than delving into these nuanced debates, it may be better, for the purpose of psychopharmacology, to side-step them and focus on actual first-person accounts analyzed from a relatively theory-free position.
Qualitative studies, such as those briefly presented above, seem to have little impact on real-world clinical practice influenced largely by guidelines based on “gold standard” evidence of RCTs relying on quantified symptom scales and educational, training and lobbying initiatives of drug manufacturers and Key Opinion Leaders (Amsterdam et al., 2017; Murayama et al., 2024; Whitaker & Cosgrove, 2015). 1PPP would need to overcome this problem by adopting some of the methodological assumptions and solutions of the EBM paradigm and thus produce evidence that could be incorporated into guidelines and gain practical clinical relevance.
1PPP – Outline of the Approach
The problem, then, is that we have a task at once nomothetic and ideographic. We need to assess the results of treatment in a way that could eventually inform practice and be translated into broad recommendations or guidelines, while at the same time we seek to both understand and alleviate the subjective suffering of particular individuals. Objective measurement of subjective states is implausible and a violation of the positivistic demands of scientific investigation (Ingleby, 1980). The study of first-person experiences is often associated with qualitative methods and interviews, and has produced a rich literature about applying such methods in the context of psychology, psychiatry and medicine (Galasiński, 2021; Janusz et al., 2010; Palinkas, 2014; Willig & Rogers, 2017). However, in order for such data to have practical clinical utility, qualitative methods would need to be imposed on a modified RCT with a double or triple blind design that would allow for causal interpretations to be made. 1PPP could then, at the fundamental level, be described as a qualitative RCT.
Methodological rigor is necessary, and insofar as possible, 1PPP should avoid any kind of presuppositions. This could allow for a sort of grounded approach (Chun Tie et al., 2019), where data on lived experience, instead of the authority of clinicians or a particular theoretical or philosophical stance, would guide the process of description of drug effects and their utility. Still, some assumptions are unavoidable in order to decide what kind of questions should be asked or what kind of phenomena should be studied. 1PPP assumes that we need to focus on several general aspects of experiences related to psychiatric drugs and their clinical use.
Firstly, we should be interested in persons in situations, that is, how particular drug effects experienced by particular people can have a positive or negative influence on them and their situation, and how their situation may be related to the drug effect. This would resemble the assumption that the set and setting may influence the action of a psychoactive agent – however, both the set (as “self” influenced by cultural narratives but also specific motivations, traits and problems people may face) and the setting should be understood broadly, encompassing the wider interpersonal, occupational and social context of a person.
Secondly, since 1PPP focuses on the effects of drugs, relying on specific DSM or ICD diagnoses as inclusion criteria would be rendered superfluous, so that participants diagnosed with different conditions could be included in the same trials, and the specific problems people face and the interactions of these problems with drug effects should be reflected in interviews. Still, this does not exclude content analysis in relation to diagnoses, which may be an important part of people’s experience of self and their problems, and thus a part of the set and setting.
In terms of design, similarly to RCT studies, four study groups could be used: (1) drug (D), (2) placebo (preferably active placebo) (P), (3) placebo – drug, with the drug introduced halfway into the trial (PD), (4) placebo – drug – placebo, with the drug introduced after a third of the trial and switched back to placebo in the last third (PDP). A trial should assess the effects of one specific substance. Blinding should be routinely assessed. Such design could have several advantages that we will discuss later in the context of data analysis.
Data collection would rely on interviews that could have a semi-structured character and start with basic general questions such as “Could you describe your current situation and problems?”, “Could you describe the effects the drug has on you?” or “Do this drug’s general psychoactive effects help you manage your distress at the moment? How?” and “Do this drug’s general psychoactive effects contribute to your distress at the moment? How?”. These could be followed by some more specific questions regarding the drug’s influence on different aspects of life, relations or experience of self. These kinds of questions should be able to capture both the general drug effects, in a drug-centered model of action (Moncrieff, 2018), as well as their beneficial and harmful influence on people’s problems and their lives, while avoiding presuppositions about benefits and harms. A general framework for the interview could be based on the Power Threat Meaning Framework (PTMF) (Boyle & Johnstone, 2014; Johnstone & Boyle, 2025; Stupak & Johnstone, 2024), which should allow for the inclusion of a wider cultural, interpersonal and social context and their meanings in relation to drug effects and people’s challenges.
The qualitative data obtained this way could be supplemented with a Visual Analogue Scale asking about a drug’s “general positive impact” and “general negative impact” to provide a simple and easier-to-interpret quantified score, which could be useful in ranking different agents, comparing them to placebo and assessing general outcome in relation to qualitative effects. This mixed-methods approach could provide a semblance of objectivity, which could be important for some practitioners or when including such data in treatment guidelines.
As for data analysis, the qualitative and quantitative data would need to be analyzed in relation to the RCT groups. On the one hand, qualitative data interpretation could follow the Interpretative Phenomenological Analysis approach (Pietkiewicz & Smith, 2014), informed by the PTMF, in order to uncover nuanced meanings and possibly experiences related to selfhood, embodiment, temporality or affective vitality. On the other hand, a thematic analysis (Braun & Clarke, 2006), preferably with coding coproduced by people with lived experience of psychiatric drug use and services, could provide themes that could be analyzed in terms of similarities or differences of codes in different groups. A summative content analysis (Hsieh & Shannon, 2005) could then be used to analyze their frequency in relation to the study group and phase, different aspects of functioning or situations and other factors, providing a sort of network analysis that could uncover patterns between them.
The inclusion of the PD and the PDP group, resembling an “ABA design” (Byiers et al., 2012), could have several advantages. First, it could allow for better control for placebo effects. For example, if participants reported the same effects in the D, P and placebo phase of the PD and PDP groups, it would be highly unlikely that the effect could be attributed solely to the drug and would most likely be mainly an effect of expectations or other factors. Conversely, an effect reported only in the D group and the drug phase of the PD and PDP groups, but not in placebo phases of groups, could be attributed to drugs with high certainty. Additionally, an effect reported in the second placebo phase of the PDP group, but not in the first one and not in the P, PD or D group would likely be a withdrawal effect.
The inclusion of PD and PDP groups could also provide data about effects related to the duration of use. For example, if some drug effects become more common or pronounced with time, they should be observed first in the D group, then in the PD group (which would have half the duration of use of the D group) and be rare in the D phase of the PDP group (as in this group, the duration of use would be the shortest). Inclusion of an additional “no intervention” group could be considered to account for natural remission and the role of expectations in shaping the placebo response in P and D groups. Thus, the additional groups could provide additional data that could help in distinguishing between drug effects and other factors and allow for better identification of adverse and beneficial effects.
This kind of between-groups analysis of data could be complemented with a within-subject or a type of “single subject” trial (Bąbel et al., 2018; Byiers et al., 2012). For example, if some adverse effects diminish with time, it could be observed in the D group within-subjects and on the overall level of the D group. This could be compared to the PDP group (there should be no adverse effects related to drugs initially there, as the drug would be introduced after the first third of the trial, but these effects should appear later in the trial and would have less time to diminish before the switch to placebo) and the PD group (where these effects should appear last, as drugs would be introduced halfway into the trial). The combination of within-subject analysis within groups and a between-groups analysis could help to distinguish potential different reactions to the same drug or establish different “types” or “classes” of predominant reactions in general and in relation to specific problems. For example, for people speaking about difficulties related to initiating and/or maintaining sleep, some people may react to the same drug with worsening of problems, some may observe beneficial effects, some may report initial beneficial effects followed by worsening, while others could report worsening followed by improvement. At the same time, some may report better sleep and overall benefit, while others could report better sleep but worsened functioning during the day or other negative effects on motivation, cognition, emotions or other areas of life.
The analysis should also take into account the relation between the circumstances people face and the drug effects, thus this should be reflected in coding and pattern analysis. For example, effects could be different or perceived and valued differently depending on the context: a person facing a stressful work situation and high job demands may react differently to the same drug than an unemployed person struggling with social isolation and financial difficulties. Similarly, the same effect, for example, sedation, may be valued differently depending on the situation, as it may be beneficial in some circumstances for some people and impede social functioning and recovery for others in another situation. For this reason, demographic data should be collected, which could enable the discovery of different patterns for different groups (i.e., related to age, gender, education, occupation, economic status etc.). This may be related to the General Patterns distinguished by the PTMF (Johnstone, 2022). This kind of evidence could be very helpful for practitioners when suggesting treatment.
However, for such a fine-grained analysis to be possible and in order to capture different aspects of drug effects and users’ situation (or the interaction between drug and set and setting), 1PPP would need to rely on a large sample sizes and the interviews would need to be conducted relatively often. The length and the frequency of the interviews would need to be predetermined and possibly also dependent on the class of drug studied. The interviews could be conducted on the day of first dosing, the days of switching assignment to placebo or drugs, the day after assignment or switch, and then weekly for the remainder of the trial.
The four groups design would also require relatively long trials. For example, for SSRI or SNRI trials, instead of the usual 8 to 12 weeks period (Ward et al., 2025) they should ideally last for at least 36 weeks, preferably a year, and include a longer follow-up with monthly interviews. This would be closer to real-world practice, help with spotting different emerging patterns, especially effects depending on the duration of use and the impact of drug effects on particular problems and situations (Figure 1).
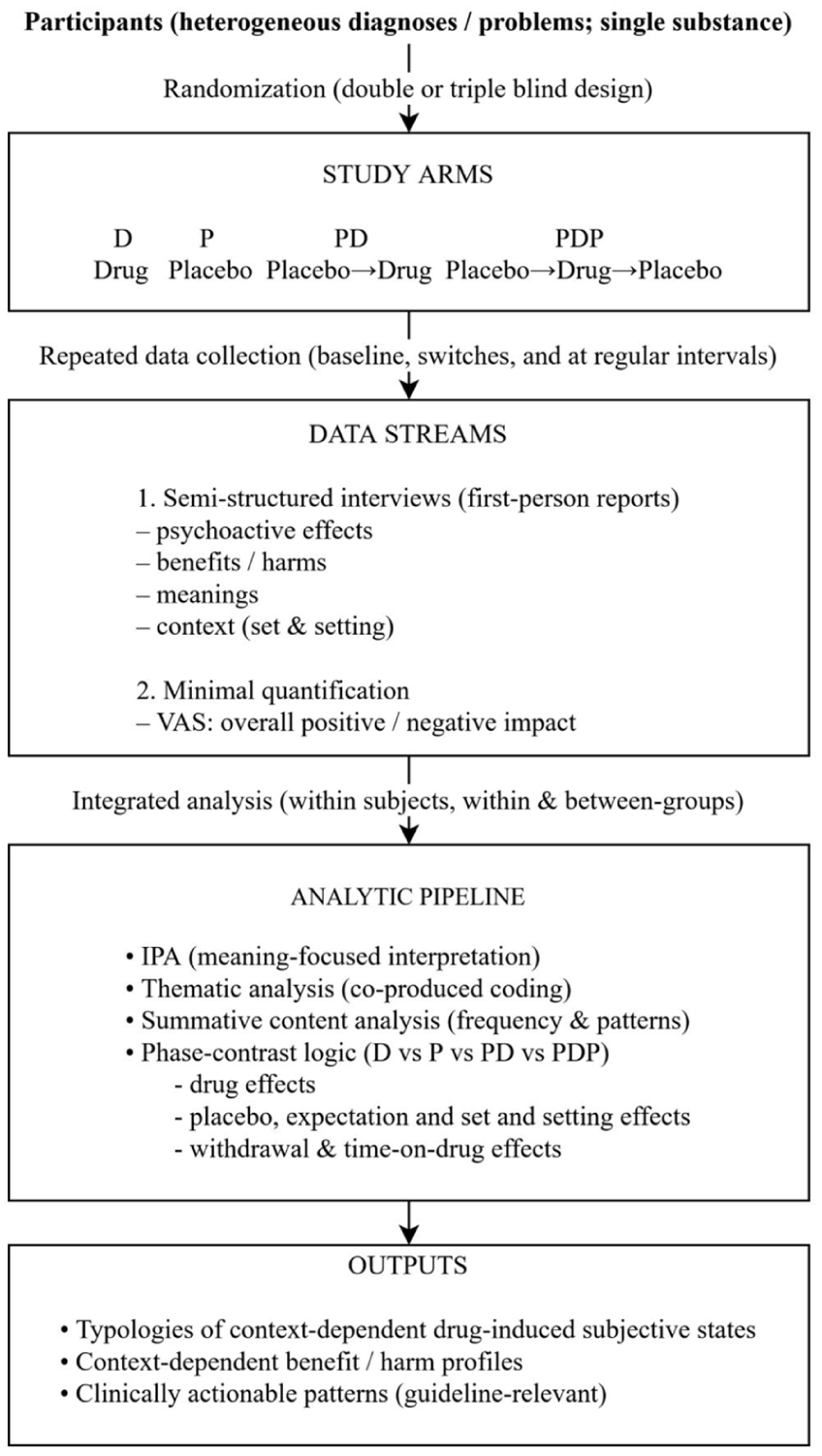
Schematic figure summarizing the 1PPP design and analytic flow.
Limitations and Challenges of the 1PPP
The 1PPP approach must overcome hurdles both theoretical and practical. These include, among others, cross-cultural validity, the impact of interviewers on the content of interviews, and the amount of time and resources needed to conduct such complex clinical trials and, crucially, to properly analyze the data.
Most importantly, if the first-person effects of drugs are mediated or moderated by set and setting, including wider economic, social and cultural contexts (Dupuis, 2022; Pronovost-Morgan et al., 2023), this will limit the generalizability of findings. Data and patterns from one region may not represent accurately the experiences of people in other regions or cultures. However, the problem of cross-cultural validity plagues much of psychiatric knowledge and practice (Mills, 2017; Bhugra & Bhui, 2018), and is certainly not specific to 1PPP. If anything, the methodology we suggest above could be better suited than psychopharmacological RCTs to studying cultural influences on drug response.
Though the controlled trial method of 1PPP could allow for causal interpretations, there are still deeper problems related to the nature of causality of mental states understood as meaning-imbued phenomena (Moncrieff et al., 2024). As Maslow (1970, p.7) noted, “[t]he fact that humans live in the natural world does not mean that their rules and laws need to be the same. (. . .) Wishes, fears, dreams, hopes, all behave differently from pebbles, wires, temperatures, or atoms.”
The proposed 1PPP methodology will require considerable resources, since it would, among other factors, require many interviewers engaged in conducting a single trial. Appropriate training of the interviewers would require substantial investment of resources. The data analysis will likely prove to be costly and time consuming. Perhaps AI could be used to assist the analysis of the data (Christou, 2024; Zhang et al., 2025), in order to facilitate coding and the discovery of patterns, which could reduce costs and workload. However, caution is needed especially regarding risks related to data privacy and algorithmic bias (Cabanillas-García et al., 2025). Obtaining funding for this kind of research could prove to be a major obstacle as funding agencies or industry would first need to be persuaded of the feasibility and potential clinical benefits of such an approach. If regulatory agencies or guidelines required qualitative evidence, that could help in the implementation of this approach. Scaled down implementation of some of the propositions and/or the addition of qualitative methods to regular psychiatric drugs RCT could constitute necessary first steps for the successful adoption of the 1PPP program.
Another point that needs to be taken into account is the unintentional influence of the interviewers upon patients’ reports of subjective states. Careful training and design of the interviews could offset that to a degree, and if several interviewers are employed in one trial, this should be taken into account in the data analysis (e.g., as interviewers nested in groups), in order to control for the effects of the interviewers. At the same time, conducting interviews, and especially relatively frequent ones, may itself have a placebo or nocebo effect on the treatment outcomes and patient experiences. A similar problem arises in the context of current RCT trials requiring frequent assessments by clinicians in order to produce a score on a rating scale. On the other hand, this kind of setting, with patients describing their situation and effects of drugs every week or two may be closer to actual, or ideal, psychiatric practice. The similarity of this kind of situation to regular check-ups with a prescribing clinician may thus be an advantage, as the research situation in 1PPP could more closely reflect real-world practice. If different frequencies of interviews is used in different trials or in relation to different drugs, this should be taken into account in the data analysis.
It could be argued that this kind of research would be inappropriate for people who are less psychologically minded and less able to articulate themselves. However, in regular RCTs all patients still need to describe their experiences to clinicians, which are then transposed to a rating on a scale, possibly leading to distortions. In the absence of direct access to an individual’s mind, this is and will remain a problem with any research depending on self-reports.
Another limitation of 1PPP could lie in the extent of the actual first-person nature of the results. It could be argued that the first-person data, when subjected to analysis by the researchers, would no longer accurately reflect first-person experience or that the goal of finding general patterns contradicts the stated first-person nature of the approach. This could lead to the usurpation of experiential knowledge by experts. Again, this is a problem far broader than 1PPP, and as elsewhere can be at least partly ameliorated by employing users with lived experience in the process of data analysis and interpretation of the results (Rivera Prince et al., 2025; Soklaridis et al., 2024).
We hope that we have shown that though qualitative research and randomized clinical trials may seem incorrigible approaches, nevertheless, with some modifications and creative adaptations, merging of these two traditions can produce valuable insights and knowledge, with the potential to significantly reshape and improve clinical practice.
Summary
Even though historically psychiatric drugs were first seen as mind altering substances and not curative agents (Scull, 2022), to this date, psychopharmacological research has not given sufficient attention to the subjective patient experience produced by these drugs, both positive and negative (Belmaker & Lichtenberg, 2023). Despite decades of primarily neurobiologically-oriented research on the psychopharmacological properties of psychiatric drugs, their effectiveness remains limited, their effects can at times be deleterious, and we still do not understand why they may be effective for one person in one context, but not in others (Cosgrove et al., 2020).
There have been calls to “fix the E in the EBM” (Heneghan et al, 2017). For psychopharmacology, we have gone even further by trying to develop a method for producing another kind of evidence. We focus on the study of drug-induced subjective states in relation to individuals’ problems in order to better understand the potential benefit and harm of psychiatric drugs.
A 1PPP will focus on the subjective experiences of taking psychotropic drugs and the quality of their psychoactive effects as they relate to their potential clinical utility. It will also examine the influence of different factors, internal and external, personal, situational, cultural and cross-cultural, influencing these effects. These kinds of factors have been widely discussed and considered in humanistic and existential psychotherapy, but largely neglected in the case of psychopharmacology. Even though the main focus of the 1PPP is on clinical trial design, data collection and interpretation with the aim of providing better clinically relevant psychopharmacological evidence, 1PPP could indirectly facilitate a real turn toward a personalized, person-centered approach to mental health care and drug prescription. A proper recognition of the perspectives of service users with lived experience may also allow for a better reporting of adverse effects of drugs or withdrawal effects and the development of effective ways of supporting people in these kinds of circumstances.
Putting the psyche back into psychopharmacology could mean understanding psychiatric drugs as psychoactive substances that exert their influence through changing subjective states of the mind in a process mediated by personal and situational circumstances, and not primarily via their action on the biology of a person. This is not meant to imply dualism. A more productive conceptualization would be that we assess a drug’s effects with a “top-down” rather than a “bottom-up” perspective, similarly to what can be done in understanding the placebo effect (Lichtenberg et al., 2004). This also doesn’t mean that biology doesn’t play a crucial role or that biological research is not important; quite the contrary, we are suggesting an approach which has heuristic value for biological research, in an attempt to better understand the link between subjective states and neurochemical drug action.
The idea of 1PPP presented here is preliminary and many details still need to be addressed, potentially with variations for each trial that we might try to design. This might eventually lead to the development of a stable framework to be reliably used in different settings in a reproducible way. The data obtained through 1PPP research could also change the way we understand the action of psychiatric drugs and the way we use them, perhaps leading to a more cautious approach when prescribing or toward using drugs on a more short-term and as-needed basis, which could prevent some of the iatrogenic effects of long-term or unnecessary use.
Recently, there have been important calls to include qualitative studies in the development of psychotherapy guidelines (Levitt et al., 2025), and many of the problems and arguments raised in the context of the study of psychotherapy effectiveness in the dominant paradigm apply as well to psychopharmacology. Conversely, the basic design of 1PPP proposed here could also be implemented in studies concerning psychotherapy. These kinds of studies could reveal effects and phenomena related to psychopharmacology or psychotherapy that are otherwise unnoticed, with important clinical ramifications (Conneely et al, 2025).
Regardless of how exactly 1PPP, or the program of qualitative studies in psychopharmacology, is realized, we believe that the need for such research is urgent. Research on first-person experiences for people taking psychiatric drugs may yet facilitate hitherto elusive progress in psychopharmacology, to the benefit of our patients.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.