
Abstract
This paper offers a phenomenological and epistemic account of a particular configuration of depressive experience, conceptualized as Gödelian Depression. Such states are marked by internal coherence, recursive self-reinforcement, and epistemic closure: truths vital for healing (hope, trust, worth) may be cognitively grasped but remain affectively unreachable. Drawing on Gödel’s incompleteness theorems as a structured metaphor, the paper explores how the self may function as a logically consistent yet incomplete system that is unable to validate, from within, the very truths that would be required for a reorganization of its own structure. Rather than proposing a therapeutic model, the paper introduces the existential stance of Inkohärenzakzeptanz, the capacity to accept the depressive mind’s incoherence without collapse, as a form of holding. This stance does not resolve closure but adds a meta-level from which it can be borne or affirmed. Grounded in philosophical analysis and first-person narrative, the paper shows how recursive entrapment is not merely conceptual but lived. In doing so, it contributes to humanistic psychology by reframing depression not merely as distortion and suffering but as a structurally intelligible form of consciousness. It also offers a vocabulary for how epistemic limits can be inhabited when healing is not provable, but still possible.
Keywords
Introduction
Depression is often described as emotional pain or cognitive distortion. Yet some depressive states exhibit a deeper structure: they remain internally coherent while resisting the kind of experiential reorganization that would allow new meanings about the self to take hold. This paper examines such configurations through the lens of Kurt Gödel’s incompleteness theorems. The aim is not to offer a general theory of depression, but to introduce a specific conceptual figure – Gödelian Depression – that captures particular internally coherent patterns of interpretation that close off new meanings about the self.
This construct arose from my own lived experience and has evolved from a loose metaphor into an epistemic‑phenomenological model with clearly defined boundaries. Gödelian Depression, however, is likely not a universal category. Rather, it applies to a particular configuration of depressive experience in which core self-evaluations become self‑sealing and resistant to revision, often in the context of early relational trauma or disruptions of ontological security (Benjamin, 2017; van der Kolk, 2015).
Gödel’s first incompleteness theorem demonstrates that within any consistent formal system powerful enough to encode arithmetic, there exist true statements that cannot be proven within the system itself (Franzén, 2005; Gödel, 1931; Smith, 2007). His second theorem goes further: such a system cannot demonstrate its own consistency from within. Originally formulated in the realm of mathematical logic, these theorems have inspired philosophical and interdisciplinary reflections (Angeler, 2025; Nagel & Newman, 2008; Raatikainen, 2025), including explorations of recursion and undecidability in human consciousness (Lucas, 1961; Penrose, 1989, 1994).
Gödelian Depression extends this insight metaphorically. It describes a depressive configuration in which the self operates as a coherent yet incomplete system: certain truths (“I am lovable,” “Life can change”) may be cognitively recognized but cannot be affectively validated. Supportive words are understood but remain inert. Attempts to counter negative self-beliefs are reinterpreted in ways that preserve the original axiom; that is, the underlying conviction about the depressive self. The result is not simple irrationality but a form of structural self-sealing.
Here, coherence is meant in a structural and systemic sense. The depressive self-system remains internally consistent in the way it interprets experience and preserves its underlying axioms, even when lived experience itself may feel fragmented, contradictory, or empty. Coherence in this context therefore refers to the logical stability of the system, not to psychological harmony. Later in the paper, the concept of Inkohärenzakzeptanz will refer to a different level: not the coherence of the system, but the capacity of the person to accept experiential incompleteness without immediately restoring internal consistency.
The analogy used here is not literal. Depression is not a formal axiomatic system, and this paper does not attempt to reduce clinical complexity to logic. Rather, Gödelian Depression functions as a rigorously defined metaphor that clarifies why certain depressive states resist change that cannot be generated from within their own closed interpretative logic. Clinically, this framing resonates with findings on treatment-resistant depression, where remission often remains elusive despite sustained intervention (Oliveira-Maia et al., 2024). Gödelian Depression suggests that such cases may reflect not mere noncompliance but a deeper form of self-reinforcing structural rigidity.
This account resonates with philosophical and psychological work on recursion, self‑reference, and opacity. Philosophers of mind have long noted limits to introspective transparency (Chalmers, 1996; Dennett, 1991; Searle, 1992) while phenomenological psychiatry describes depression as a disturbance of world‑relation and affective attunement (Fuchs, 2005; Ratcliffe, 2008). The present contribution integrates these strands into a structured account of epistemic closure.
In this paper, recursion refers to a specific process in which the output of a mental operation becomes its own input, reinforcing prior conclusions. In Gödelian Depression, the loop can be schematized as follows: (1). Core axiom: “I am fundamentally unworthy.” (2). Encounter with care or affirmation originating outside the depressive system. (3). Reinterpretation of the encounter in ways that preserve the underlying conviction: “They are mistaken, obligated, or deceived.” (4). Reinforcement of the axiom. (5). Return to the starting point. Through such recursive reinterpretation, the system maintains internal coherence by absorbing contradiction rather than revising itself.
The first‑person dimension is integral to this account. I write as someone who has inhabited such closure, not to claim authority through disclosure, but to acknowledge that insight into self-sealing systems may emerge only from within their lived constraints. This orientation aligns with the humanistic-existential tradition, which approaches suffering as an intelligible mode of being rather than mere malfunction (May, 1953; Schneider, 1990; van Deurzen, 2012). In this sense, the text enacts what Blanchot (1995) calls a form of negative presence, where something becomes present precisely through its structural inaccessibility.
This paper addresses three questions:
How can certain depressive states be understood as recursively self-sealing epistemic systems?
In what sense does recursive closure differ from ordinary self-reference or rumination?
What form of existential stance remains possible within such closure, and what are the limits of what can be achieved from within it?
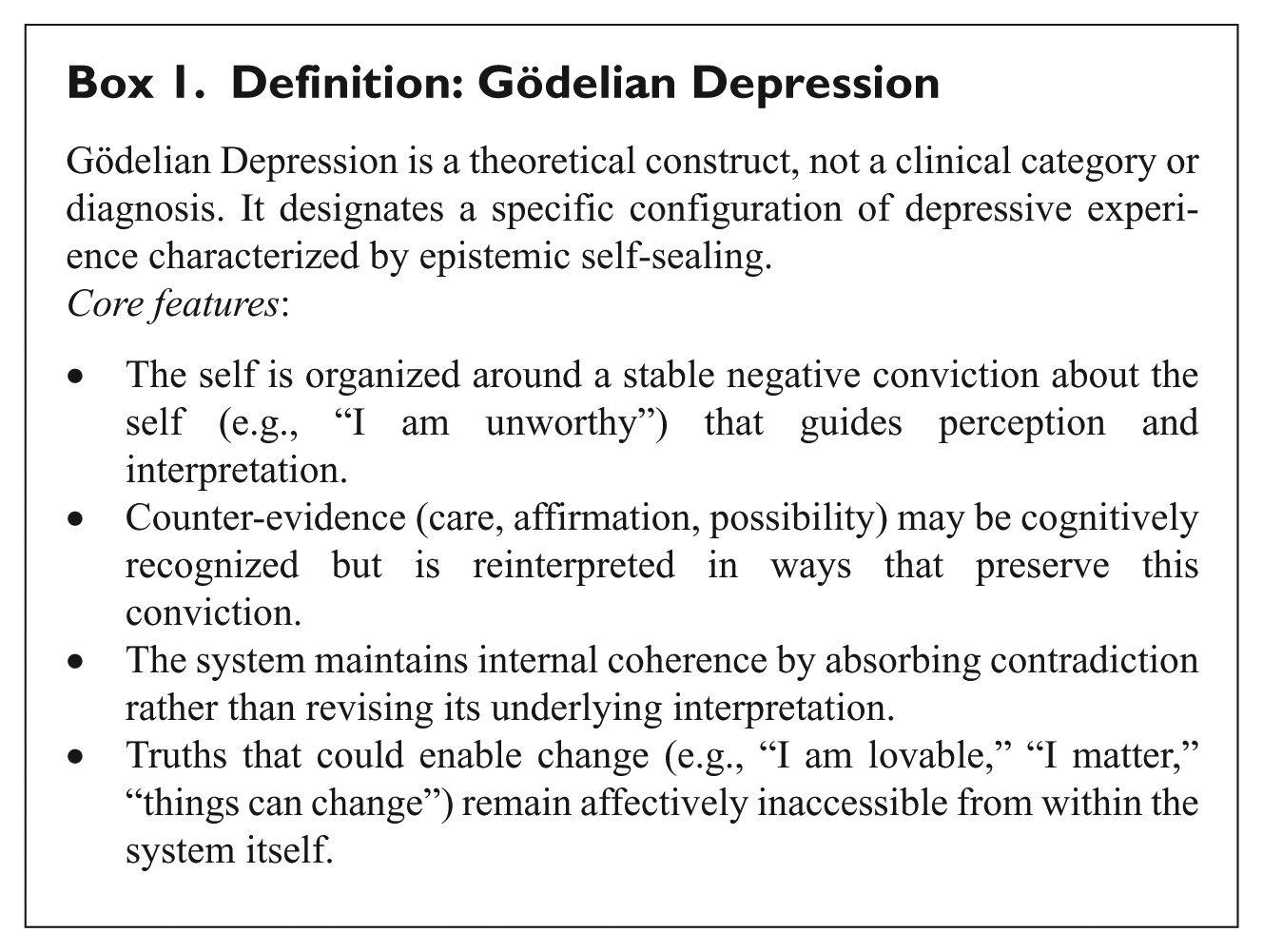
To address these questions, I first revisit Gödel’s incompleteness theorems, not as clinical explanations but as philosophical metaphors that illuminate structural limits of self-knowledge. I then situate Gödelian Depression within psychiatric, phenomenological, and psychodynamic contexts. The analysis introduces Inkohärenzakzeptanz as an existential stance that expands internal elasticity without dissolving the depressive mind’s closure. Finally, I examine the conditions under which rupture (an interruption of recursive self-sealing) may become possible. Box 1 formalizes the concept.
Definition: Gödelian Depression
Recursive Closure, Self-Reference, and the Limits of Self-Knowledge
Recursive self-awareness is not inherently pathological. It underlies reflection, moral deliberation, and narrative identity. It becomes problematic only when the recursive process ceases to generate revision and instead stabilizes prior conclusions. In such cases, self-reference no longer expands perspective but narrows it. In the present account, recursive closure refers not to self-reference as such, nor simply to repetitive rumination, but to a form of self-reference in which the underlying evaluative premises of the system can no longer be revised from within. What would ordinarily allow reflection to correct itself instead preserves the existing structure.
The Gödelian metaphor clarifies this distinction. Gödel showed that a system can be internally consistent while unable to establish certain truths about itself. Transposed metaphorically into the phenomenology of depression, this suggests that the self may preserve coherence while remaining unable to validate meanings essential for change. The issue is not ignorance, but internal limitation.
In depressive configurations of this kind, individuals often report a striking disjunction between cognition and lived conviction. They may understand that others care or that change is possible, yet this recognition does not alter the felt structure of selfhood. The barrier is not a lack of information but a mode of reinterpretation that reabsorbs contradiction into an existing evaluative frame. Care can be recoded as pity, affirmation as politeness, encouragement as obligation. The system thus maintains coherence without revising its underlying conviction about the self.
Philosophers of mind have long emphasized that self-transparency is limited. Dennett (1991), Searle (1992), and Chalmers (1996) each, in different ways, underscore the opacity of conscious processes. Hofstadter’s (1979, 2007) concept of “strange loops” illustrates how self‑reference constitutes subjectivity while also exposing it to circularity. What is normally a generative structure of reflection can, under certain affective conditions, harden into closure.
Phenomenological psychiatry provides complementary descriptions. Fuchs (2005) characterizes depression as a disturbance of embodied attunement and world‑relation, while Ratcliffe (2008) documents how meaningful speech may be semantically grasped yet experientially empty. Benjamin (2017) further shows how relational recognition can fail when the self lacks a stable ground from which to receive it. These accounts converge on a shared insight: the depressive subject may register external gestures without being able to take them in as experientially real.
From this perspective, Gödelian Depression does not denote irrationality but a particular configuration of epistemic limitation. The self recognizes propositions that it cannot existentially authorize. The recursive structure that ordinarily enables self-correction instead preserves coherence of the depressive system by preventing revision. The result is not cognitive distortion alone, but a form of lived incompleteness in which change may be conceivable yet cannot take hold within the structure of experience. The following section examines how this epistemic structure intersects with psychodynamic and relational theories of self-organization.
Consciousness, Recursive Closure, and the Limits of Self-Access
If Gödel’s incompleteness theorems illuminate structural limits within formal systems, their metaphorical relevance here concerns the limits of self-access. The previous section described how depressive meanings can become self-sealing. The present section addresses the second question posed in the introduction: how the structure of consciousness itself allows such closure to persist. Depression, in this framing, does not simply distort reality; it constrains the conditions under which certain meanings can be experienced as real.
The notion of “strange loops,” introduced above, helps clarify how self-awareness can become caught within its own operations. Under ordinary conditions, such loops allow reflection to revise itself by shifting perspective. In depressive states of the kind described here, however, self-reference ceases to generate reorganization. Instead, reflection repeatedly returns to the same evaluative position. What should function as self-correction becomes stabilization.
Phenomenological psychiatry allows this limit to be formulated more precisely. Fuchs’s (2005) account of depression as a disturbance of embodied attunement, together with Ratcliffe’s (2008) analysis of the gap between semantic comprehension and experiential conviction, shows how meaning may be understood without becoming affectively or existentially real. Read in this context, these accounts point to a limit of self-access: the subject can register meaning without being able to inhabit it. One may hear “I am here for you” and understand its propositional content, yet remain untouched by its relational force. What is revealed here is not a lack of knowledge, but a limit in the subject’s capacity to let meaning alter the structure of experience.
Zahavi (2005) emphasizes that subjectivity is inherently first-personal yet not fully transparent to itself. Selfhood contains opacity. In depressive configurations, this opacity intensifies: reflective awareness circles around evaluative conclusions without altering them. The self becomes entangled in its own interpretive operations, unable to reposition its underlying conviction.
Empirical research on rumination provides convergent support. Nolen-Hoeksema (2000) identified repetitive abstract self-reflection as a sustaining factor in depressive episodes, while Watkins (2008) demonstrated that abstract rumination (“Why am I like this?”) predicts poorer outcomes than concrete engagement with experience. These findings suggest that the problem is not reflection per se, but a mode of reflection that reinforces rather than revises previous conclusions. The recursive process preserves coherence at the cost of flexibility. In this sense, recursive closure in Gödelian Depression differs from ordinary self-reference or rumination: it does not merely repeat thoughts, but stabilizes the underlying evaluative premises of the system so that revision from within becomes increasingly difficult.
In this way, the first question posed in the introduction can be answered: certain depressive states constitute instances of epistemic entrapment. Consciousness does not lack content; what it lacks is the capacity to revise itself. As McGinn (1999) describes cognitive closure, some truths about mind may remain inaccessible to the mind itself. In depression, this manifests as a paradoxical awareness: recognition without integration, acknowledgment without experiential change. The following section turns to psychodynamic and relational accounts to examine how such epistemic rigidity may be developmentally anchored and interpersonally sustained.
From Logical Structure to Relational Organization in Gödelian Depression
The preceding analysis described the epistemic structure of Gödelian Depression. The present section situates that structure within relational and developmental frameworks. The focus shifts from logical form to psychic organization.
Psychodynamic Anchoring: Projective Identification
From a psychodynamic perspective, the Gödelian depressive system is not only cognitive‑affective but also relational and intersubjective. Projective identification (Bion, 1962; Ogden, 1994) provides one mechanism by which the system maintains coherence. Intolerable states (helplessness, futility, or unreliability) may be unconsciously disowned and attributed to the other, so that the therapeutic relationship becomes organized around what the self cannot tolerate as its own experience. The therapist can then be experienced as unreliable, intrusive, or controlling, rather than as a stable source of recognition. In this way, relational contact becomes reorganized in accordance with the system’s internal logic. What appears externally as support may be subjectively registered as destabilizing. Stolorow et al. (2002) emphasize that such defensive structuring is not arbitrary but protective. The depressive subject does not reject care out of defiance; care threatens to reorganize a structure built for survival.
False Self Organization
Winnicott’s (1965) concept of the false self further illuminates this dynamic. Where early relational environments were inconsistent or intrusive, adaptation may take the form of functional compliance. Emotional authenticity is replaced by performance. The false self sustains survival by substituting functionality and role compliance for authentic affective expression.
In such cases, a stable negative conviction can become the organizing principle of identity. Perfectionism, social role performance and emotional withdrawal may function as stabilizers. The cost of this stability is permeability. Relational openness becomes risky because it exposes what the self was designed to conceal.
Lived Experience and Epistemic Closure
I have lived this system from the inside. Even the most caring gestures often felt unreal, as though refracted through an internal logic that stripped them of credibility. A statement like “I am not bad” was intellectually comprehensible but experientially unprovable. Accepting it would have undermined the structural coherence of my self‑system, which was anchored in the silent conviction “I am unworthy.” In these moments, no insight, no rational argument, no emotional appeal could penetrate. The world outside continued, but the self existed in epistemic quarantine, intact in its logic, yet unlivable in its isolation.
Jaspers’ (1963) notion of “Unverständlichkeit,” a psychic state that remains phenomenologically coherent while eluding external comprehension, captures part of this condition. It also aligns with Gallagher and Zahavi’s (2007) account of first-person subjectivity as a lived structure, not reducible to third-person explanation. From this perspective, the depressive system reflects not a distortion of reality but a change in the structure of self-experience, where epistemic closure is not chosen but inhabited. Gödelian Depression thus reframes what appears as resistance into a form of existential logic. It depicts a protective stance that guards the self’s internal order against intrusion, even at the cost of remaining unreachable.
Origins of Recursive Closure: Structural Predisposition or Symptomatic Formation?
A further question concerns developmental trajectory. Does recursive closure arise as a symptom of depressive episodes, or does it reflect a prior structural disposition? Cognitive models (Beck, 1967; Teasdale, 1983) emphasize schema consolidation through repetition into self‑reinforcing belief loops. Psychodynamic and structural theories point to earlier and deeper predispositions in the context of early relational trauma, chronic misattunement, or internalized shame (Fonagy et al., 2002; Kernberg, 1992; McWilliams, 2011). Individuals with schizoid, narcissistic, or obsessive‑compulsive (anankastic) organizations often exhibit self‑structures that rely on epistemic withdrawal and relational detachment for survival. Erskine (2021) shows how, in complex trauma or schizoid patterns, depressive symptoms frequently emerge as secondary expressions of a more fundamental structural closure.
Conversely, cognitive and phenomenological models (Fuchs, 2005; Sass, 1992) suggest that recursive closure can also develop progressively during sustained depressive states, as rumination and affective constriction narrow the experiential field. Such processes can lead to hermetic self‑reference, even in the absence of strong biographical predisposition.
This distinction is clinically significant. If rigidity reflects structural self‑protection rather than episodic distortion, change may not rely solely on cognitive reframing or insight. It must proceed through relational experiences that acknowledge the self’s logic without prematurely intruding upon it.
Clinical Reframing: Implications for Therapeutic Stance
Under this lens, resistance or non‑compliance in therapy is not willful negativity but the expression of a logically consistent system protecting its own existence. Therapeutic gestures that appear hopeful from the outside are often experienced as ontological breaches from within. The Gödelian analogy becomes especially poignant where affective defenses are not simply reactive but structurally necessary: truths that could reorganize the self are experienced as threatening because they would collapse the logic holding the self together.
In formal logic, incompleteness invites the possibility of new axiomatic frames (Berto, 2009). Similarly, in depression, change may be possible only from a relational “outside,” yet the system lacks any intrinsic mechanism to trust or integrate that perspective. From a clinical point of view, this suggests that therapeutic work cannot rely solely on correction, reassurance, or reinterpretation. When closure reflects a structurally coherent organization, attempts to introduce new meanings may be experienced as destabilizing rather than helpful. The task of therapy may then shift from trying to overcome the system to sustaining a relational space in which it can remain intact without becoming more rigid.
Such a stance requires tolerating the limits of what can be changed from within the system at a given moment. What appears as resistance may mark the boundary of what the self can currently allow without collapse. Clinical progress may therefore consist not in immediate structural reorganization but in the emergence of flexibility, the capacity to remain with contradiction, or the possibility of approaching previously excluded meanings without losing coherence.
It is at this point that the attitude described here as Inkohärenzakzeptanz becomes relevant. Rather than attempting to eliminate incoherence, this stance allows the self to remain within its structural limits without forcing premature resolution. Here, incoherence does not refer to a breakdown of the system’s internal logic, but to the tension that arises when lived experience exceeds what the closed system can validate. In this sense, therapeutic work does not necessarily overcome the Gödelian closure of the depressive system. Rather than producing change, it may provide a relational context in which that closure can be affirmed without complete withdrawal from relational life. Within such a context, an attitude such as Inkohärenzakzeptanz may become possible, not as a technique or skill that can be taught, but as an existential shift that cannot be forced from within the system itself.
Inkohärenzakzeptanz and the Limits of Change Within Recursive Closure
If change cannot arise from within a self-sealing structure, the question arises whether relief is nevertheless possible without altering that structure. This addresses the third question posed in the introduction: what form of existential stance remains possible within recursive closure, and what its limits are. Inkohärenzakzeptanz (Box 2, Figure 1) addresses this question. It designates an existential stance in the phenomenological-experiential sense rather than a therapeutic method. It refers to the capacity to develop a lived attitude that confers elasticity within the self-system marked by Gödelian closure, so that incoherence is no longer experienced as immediately threatening, but can, to some extent, be affirmed.
Definition: Inkohärenzakzeptanz
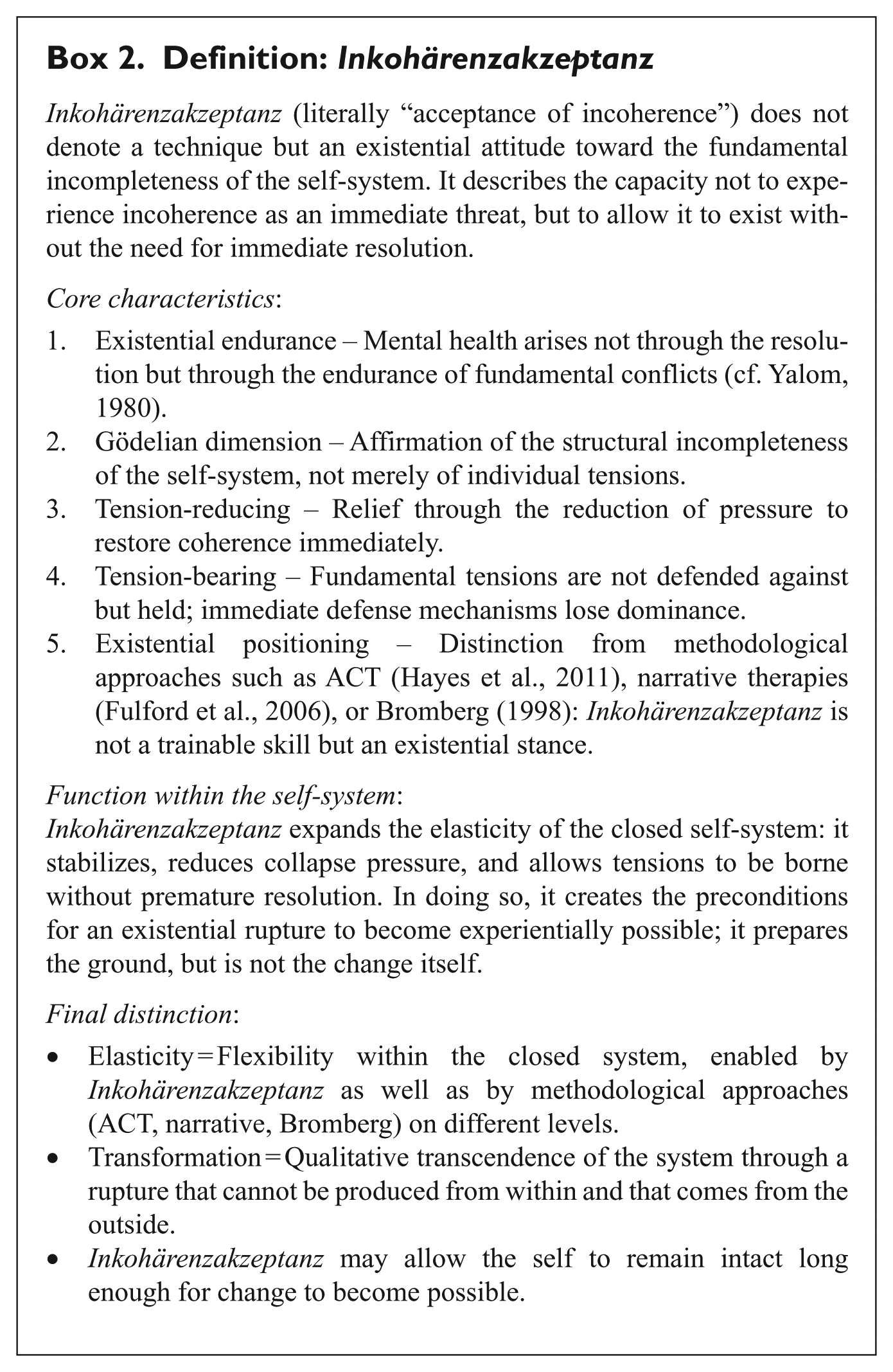
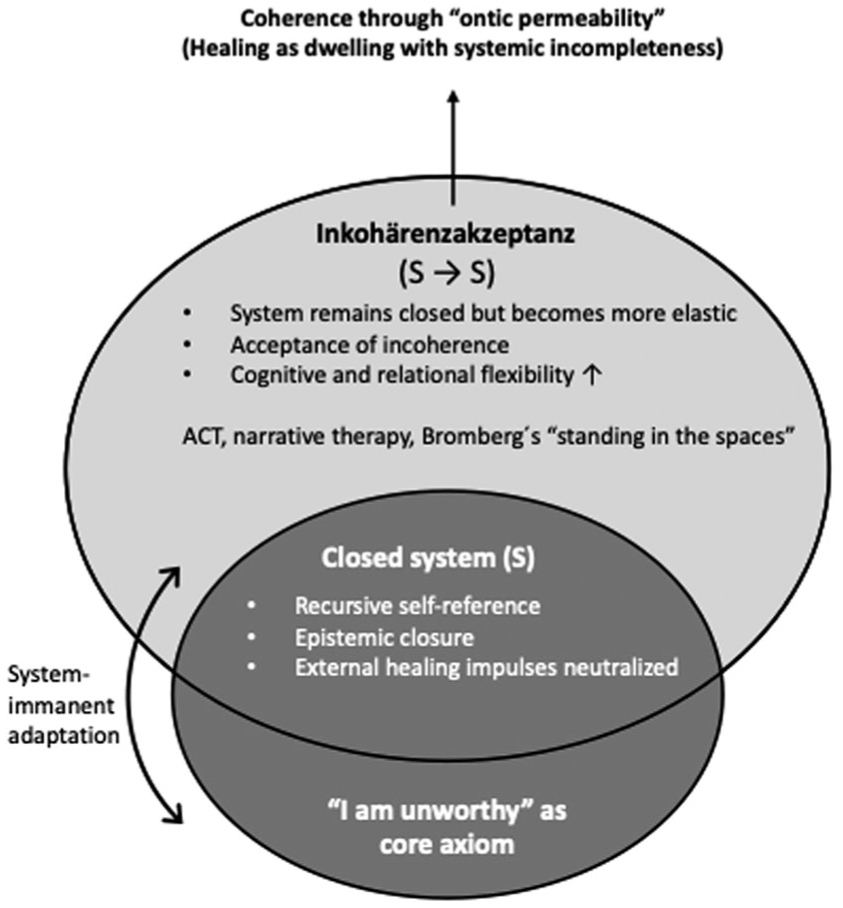
Gödelian Depression as a closed system in which Inkohärenzakzeptanz operates as an existential stance that increases the system’s elasticity, allowing incoherence to be borne without collapse and making coherence possible without structural revision.
The concept aligns with existential psychotherapy as articulated by Yalom (1980), where mental health is not defined by the elimination of existential tension but by the capacity to endure it. Inkohärenzakzeptanz stands in this tradition but takes it one step further: it does not merely tolerate anxiety, despair, or uncertainty, but affirms the fact that one’s own inner order is inherently incomplete. Unlike therapeutic strategies that aim to increase one’s tolerance of difficult experiences, Inkohärenzakzeptanz is not a coping technique but a stance toward being. It does not seek to neutralize incoherence but to dwell within it without collapse. In this context, verbs such as accept, affirm, or bear witness more accurately express its ontological depth than instrumental terms like tolerate or endure, which often imply symptom management. The emphasis here is not on enduring discomfort until relief arrives, but on inhabiting a structurally incomplete self-system without needing to resolve or close it.
Several therapeutic approaches engage similar terrain. Acceptance and Commitment Therapy (ACT; Hayes et al., 2011) encourages commitment to values in the presence of distress. Narrative approaches reframe self-stories (Fulford et al., 2006). Bromberg (1998), with his concept of standing in the spaces, emphasizes that multiple and even contradictory self-states can coexist without needing to be prematurely integrated or harmonized. In doing so, he strengthens the capacity to live with inner incoherence, albeit within a clinical framework.
All of these approaches operate within the system: they open space for reflection, make it more elastic, and expand the range of possible actions. From the perspective developed in this paper, however, the basic organization of the system remains unchanged. Inkohärenzakzeptanz can thus be conceived as a new meta-level within the closed self-system: it provides a layer of self-reflection that allows the system to relate differently to its own contradictions without replacing its underlying conviction. Therefore, meanings that come from outside the depressive system may still fail to become experientially real within it. Existentially, this means: relief, yes; structural opening, no.
A personal aside clarifies the difference between ACT, narrative approaches, Bromberg’s ideas and Inkohärenzakzeptanz: for me, approaches such as ACT initially seemed theoretically conceivable and less threatening precisely because they did not force an immediate opening. This may have allowed my system to accept them at first in contrast to approaches that explicitly sought to introduce a new truth, such as the idea that therapy will help. However, their long-term effectiveness remained limited because my depressive system fundamentally interpreted therapeutic offers as external intrusions. Consequently, they did not change anything fundamentally about the closure and were eventually rejected like all other approaches.
This experience points to a more fundamental question: How can Inkohärenzakzeptanz be situated in relation to other theoretical concepts? Antonovsky (1979, 1987), through his concept of the Sense of Coherence, describes coherence as a central resource that makes life appear comprehensible, manageable, and meaningful. Complete coherence is unattainable for any individual, yet as a resource, it acts salutogenically as it supports and strengthens health. Inkohärenzakzeptanz goes further: it does not merely mean living with limited coherence, but rather affirmatively embracing the structural incompleteness of the self-system.
Whereas coherence in Antonovsky’s framework functions as a resource that sustains adaptation, Inkohärenzakzeptanz describes a different dynamic: coherence is not restored directly, but may emerge as the closed self-system gains elasticity and becomes less rigid in the face of its own incompleteness. Paradoxically, this can give rise to a renewed sense of coherence. It becomes not a salutogenic resource, but a consequence of an attitude that dwells affirmatively within incompleteness.
Inkohärenzakzeptanz does not deny that every self-system inevitably strives for coherence. Yet it shifts the focus: coherence is not produced as a resource, but emerges secondarily from the stance of affirmatively inhabiting incompleteness. Thus, Inkohärenzakzeptanz is not a technique in the usual sense, but an existential attitude toward the fundamental incompleteness of the self-system. But what practical implications does such an attitude have for the depressive system? In lived experience, Inkohärenzakzeptanz does not manifest unidimensionally, but in two distinct directions of effect, each with its own function. The two directions of effect can be distinguished as follows:
Tension-reducing: Inkohärenzakzeptanz provides relief by reducing the pressure to restore coherence immediately. Incoherence thereby appears less threatening, and the risk of collapse decreases.
Tension-bearing: Inkohärenzakzeptanz dampens immediate defense mechanisms (intellectualization, denial, projection, etc.) and allows the underlying tension to persist without being prematurely warded off or neutralized. The tension is not suppressed but held.
From the perspective developed here, however, one limit remains: a closed system cannot complete itself from within. It may develop greater elasticity by introducing new levels of reflection, yet every movement that remains immanent to the system still operates within its existing convictions or axioms. It therefore lacks the structural means to initiate its own reorganization.
In this sense, Inkohärenzakzeptanz marks an important expansion of internal flexibility. It increases the system’s elasticity, enabling it to bear witness to internal contradictions without disintegrating under their weight. In this respect, the function of Inkohärenzakzeptanz resembles what resilience theory describes as adaptive capacity: the ability of a system to absorb disturbance and maintain its organization without undergoing a structural transformation (Angeler et al., 2019). Yet, just as adaptive capacity does not itself produce a regime shift toward a novel ecosystem state, Inkohärenzakzeptanz cannot generate the step beyond the system’s own logic. It remains an immanent attitude that creates the conditions under which further unfolding can be borne at all.
The Epistemic Significance of Rupture and the Limits of Internal Transformation
This leads to the theoretical necessity of a rupture. By “rupture” here, what is meant is not a technique or planned intervention, but an existential event in which the system’s closure is breached. A Gödelian rupture denotes the moment when the internal logic reaches its limit and something enters from the outside that cannot be derived from within the system itself. It cannot be produced or guaranteed; it is experienced as a break in recursion, one that can lead the self out of its closed circularity. Such a rupture does not arise from argument, insight, or reinterpretation alone, but from an encounter with a reality that the system cannot fully assimilate and yet cannot dismiss. In this paper, “transformation” does not refer to symptom improvement in a clinical sense, but to a structural reorganization of the self-system that cannot be produced from within its existing recursive logic.
Inkohärenzakzeptanz does not constitute the opening itself but allows the system to approach its limits without immediate defensive closure. It does not produce structural transformation, but reduces the pressure toward collapse and makes tolerable the contact with what exceeds the system. In this sense, it functions like a firebreak: not the source of change, but the condition that prevents rigid defense or disintegration when the system encounters what it cannot assimilate.
A look at the psychoanalytic tradition makes this clearer. Binswanger (1963) describes mental health not as the absence of contradictions, but as the ability to persist amid incompleteness. Fuchs (2005) emphasizes the importance of embodied integration, which enables a self without syntactic closure. Winnicott’s (1960) concept of the holding environment shows how tensions can be held relationally without needing to be resolved. Bromberg (1998) highlights that multiple, discontinuous self-states can coexist without the immediate demand for integration. Finally, Tedeschi and Calhoun (1995, 2004) describe post-traumatic growth not as the result of linear healing, but as the capacity to remain agentic in the face of unprovable truths. Across these approaches, transformation becomes possible not only through internal reorganization, but through relational situations in which the self encounters something that cannot be reduced to its prior meanings.
Inkohärenzakzeptanz adds its own dimension to this tradition: it shares with these approaches the capacity to hold tension, yet it is not a therapeutic holding function in the usual sense. It designates an existential stance in which structural incompleteness is neither resolved nor neutralized, but allowed to persist without collapse. This also has consequences for the present model itself. As Merleau-Ponty (1968) reminds us, no philosophical or clinical description is written from a position of pure neutrality. The account developed here is shaped by the same recursive structure it seeks to describe. The movement between phenomenological closeness and theoretical distance is therefore not a stylistic inconsistency but an expression of that very condition: reflection cannot fully step outside the system it analyzes. For this reason, the model reaches a limit at precisely the point where the question of transformation arises. From within a closed system, no argument can produce the perspective required to revise its own premises. The analysis can therefore only indicate that transformation, if it occurs, must involve a standpoint that the system itself cannot generate.
Thus, the circle closes – from the formal incompleteness of Gödelian logic to the existential incompleteness of lived experience. Inkohärenzakzeptanz describes the inward stance that, in a sense comparable to adaptive capacity in resilience theory, allows the self-system to remain viable under tension without yet undergoing structural transformation. In ecological resilience theory, such adaptive capacity enables a system to absorb disturbance while remaining within the same regime, whereas qualitative change occurs only when thresholds are crossed and the system reorganizes into a new state (Angeler & Allen, 2016; Holling, 1973). In an analogous way, the depressive self-system may gain elasticity without yet leaving its recursive closure. Transformation in the true sense, however, presupposes an outside that makes an unprovable truth experientially available.
The precise nature of this relational “outside,” and the way in which it may become effective without forcing the system open, requires a more detailed phenomenological analysis than can be developed here. Karin Schaffer (personal communication) explores this dimension further by examining forms of presence and witnessing that remain with the closed self without attempting to overcome it, thereby making rupture possible without producing it.
In this sense, rupture cannot be manufactured, only prepared for. Inkohärenzakzeptanz marks the limit of what the system can achieve from within. What lies beyond that limit belongs to the domain of encounter.
Conclusion
This paper has proposed a reframing of certain depressive states as Gödelian systems: internally consistent yet structurally incapable of validating the very truths, such as hope, trust, and self-worth, that could enable a structural reorganization. Drawing on Gödel’s incompleteness theorems as a philosophical metaphor, the argument does not aim to pathologize or universalize, but to illuminate how some depressive minds sustain themselves through recursive self-reference and epistemic closure, a form of self-reference that stabilizes its own evaluative premises rather than revising them. These systems do not merely resist help; they are constituted precisely by their incapacity to affirm truths that lie outside their axiomatic logic. Seen from within such a system, what appears from the outside as obvious or reassuring may remain experientially unreal, not because it is rejected, but because the structure of the self cannot yet authorize it.
Rather than advancing a clinical typology, this model articulates a phenomenological, epistemic, and humanistic configuration. It describes how depressive closure may emerge as a functional architecture of psychic survival, often grounded in early disruptions of relational security. In such configurations, openness itself is experienced as destabilizing. What appears from the outside as resistance or avoidance may in fact reflect a structurally coherent strategy to preserve internal consistency under conditions of existential threat. This perspective aligns with the humanistic-existential tradition that views suffering not as pathology but as an intelligible mode of being (May, 1953; Schneider, 1990; van Deurzen, 2012). By framing Gödelian Depression as a structurally coherent, though epistemically closed, form of consciousness, the paper extends this tradition’s call to encounter rather than correct existential suffering. Clinically, this implies that therapeutic work may at times require less emphasis on changing the patient’s convictions and more on sustaining a relational field in which the system can remain intact without becoming more rigid.
Within this closure, the paper has introduced the concept of Inkohärenzakzeptanz – the existential stance of affirming incoherence without immediate resolution. Unlike therapeutic methods that seek integration, this stance does not aim to resolve tension but to bear witness to it, and to affirm its presence. It expands the system’s inner elasticity, creating conditions under which rupture might become possible. Notably, Inkohärenzakzeptanz is not a technique, but a lived epistemic attitude that permits the self to remain intact in the face of its own incompleteness. In this context, verbs such as “accept,” “affirm,” or “bear witness” more accurately reflect its ontological depth than instrumental terms like “tolerate” or “endure.” Its significance lies not in producing change directly, but in allowing the self to remain in contact with what exceeds it without immediate defensive closure.
This framework also reorients how coherence itself is understood, in line with the distinction introduced earlier between systemic coherence and existential openness to incompleteness. It shifts from the pursuit of cognitive closure to a deeper form of ontological coherence, or Stimmigkeit, that arises through contact, relation, and existential endurance. This echoes Antonovsky’s (1979) notion of Sense of Coherence, but moves further: coherence becomes not a resource to be restored, but a consequence of affirmatively inhabiting what cannot be resolved. In this sense, coherence is no longer the opposite of conflict, but the capacity to remain with conflict without losing the sense of being.
Importantly, the potential for structural transformation – if it occurs – does not arise through rational persuasion or cognitive reframing, but through rupture: moments in which the system’s recursive loop is interrupted by something it cannot generate or fully assimilate. Such moments may take the form of relational presence, witnessing, or meanings that cannot be proven within the system’s own logic. They cannot be produced by technique, but may become possible when the system no longer needs to defend itself against every contradiction. This suggests that the Gödelian model points beyond itself toward relational dimensions that cannot be fully articulated from within a theory of closure alone.
Finally, the Gödelian framing also has normative implications for how depressive experience is interpreted. As Foucault (1965) observed, psychiatric regimes of truth often marginalize non‑normative experiences by defining them as errors or deficiencies. Kidd et al. (2025) further elaborate this problem as one of epistemic injustice, where structurally intelligible but non-normative forms of subjectivity, such as the recursive logic of Gödelian Depression, are dismissed as irrational or uncooperative simply because they do not align with dominant therapeutic expectations. By conceptualizing certain depressive states as structurally intelligible, self‑sealing systems rather than as flawed or deficient cognition, this paper resists the pathologizing impulse. It illuminates recursive despair as a logically coherent survival strategy and opens conceptual space for forms of help that do not seek to refute the system but to meet it where it cannot complete itself. In this sense, the Gödelian perspective does not offer a cure, but a way of understanding the limits within which change, relation, and meaning may nevertheless become possible.
Footnotes
Acknowledgements
The author wishes to express deep gratitude to Karin Schaffer, MSc, for her generous discussions and invaluable feedback, which significantly strengthened this work.
Author Contributions
DGA conceived the study and wrote the paper.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.