
Abstract
The understanding of psychosis has changed over time to consider the impact of trauma on people’s experiences. The Power Threat Meaning Framework (PTMF) highlights the role of adverse life experiences on subsequent distress and has been used to guide team formulation meetings within the NHS for almost a decade. The study aimed to explore clinicians’ experiences of PTMF team formulation meetings and how this may influence their subsequent understanding of psychosis. Ten staff participants from mental health services supporting those experiencing psychosis were recruited and interviewed. Narrative analysis methodology was employed. Within the narratives, most participants spoke of having previously held a medical model understanding of psychosis, reflecting its dominance. The PTMF featured in the narratives and often illuminated the role of adversity and power in clinicians’ understandings. Participants narrated how the PTMF formulation meetings helped to humanise clients, alongside personal stories of loved ones’ experiences of psychosis. Clinical implications and recommendations for future research are discussed.
Introduction
The phenomenon referred to as “psychosis” encompasses a range of experiences, such as hearing voices, seeing, smelling, feeling, or tasting things others do not, and holding beliefs that others may find unusual. The concept of psychosis was brought into psychiatric literature by Carl Canstatt in 1841 and at the time, it was considered a “disease of the brain” (Bürgy, 2008, p. 1201). The biomedical model has subsequently dominated the narratives surrounding psychosis and has guided its treatment (Bentall, 2004), despite the association between adverse life events and psychosis being well known (Read & Larkin, 2008). For example, there is strong evidence suggestive of a dose–response relationship with trauma: people who have experienced three traumas are 18 times more likely to develop psychosis, whereas those who have experienced five traumas are 193 times more at risk (Shevlin et al., 2007).
Narratives of Psychosis
Dominant narratives are produced and reproduced within society and have an influence on both group and individual narratives (Mankowsi & Rappaport, 2000). The medical model is the primary discourse of psychosis in society (Lawrence et al., 2021), mental health services (Chadwick & Billings, 2022), and amongst individuals (Naeem et al., 2016). Medical narratives have the potential to place the blame within the individual and increase stigma (Read et al., 2004), whereas alternative narratives may offer different possibilities. For example, May (2004) commented that his own diagnosis of schizophrenia was unhelpful, instilling a belief that he would always be ill. He argued that a focus on psychological recovery would have been beneficial. Due to the dominance of the medical model, reinforced by the explanations often provided to service users by clinicians and interventions delivered (Corcoran et al., 2007), an illness narrative embeds itself within the personal stories of people who have experienced psychosis (Naeem et al., 2016). As such, it is beneficial to consider clinicians’ understanding of psychosis and how these can be shaped by different team practices, including team formulation meetings.
Team Formulation Meetings
Team formulation meetings have been defined as “the process of facilitating a group of professionals to construct a shared understanding of a service user’s difficulties” (Johnstone & Dallos, 2013, p. 5). They aim to facilitate collaborative working amongst team members and have become increasingly popular (Division of Clinical Psychology [DCP], 2011). There are multiple benefits of team formulations, including a greater understanding of risk (Ramsden et al., 2014), increased psychological thinking (DCP, 2011), more confidence in treatment plans (Hartley, 2021) and improved relationships between staff and clients (Berry et al., 2015). Team formulations also allow staff members to put forward their own ideas, subsequently allowing others to learn from these ideas, and may influence their personal narratives of emotional distress. For example, in a qualitative study, a clinician described seeing clients more as “people” and less as “patients” after attending team formulation meetings (Murphy et al., 2013, p. 444).
The Power Threat Meaning Framework
The Power Threat Meaning Framework (PTMF) developed by Johnstone, Boyle and colleagues (2018) offers a non-pathologising approach to understanding mental distress. It serves as a comprehensive framework for identifying patterns of emotional distress, unusual experiences and troubling behaviour. It proposes an alternative approach to psychiatric diagnosis and moves the question from “what is wrong with you?” to “what has happened to you?” The focus of the framework is to provide a lens to view the role power and adversity plays in people’s difficulties and stories. The PTMF is summarised into four key questions:
“What has happened to you?”
“How did it affect you?”
“What sense did you make of it?”
“What did you have to do to survive?”
Two additional questions are set out to help facilitate conversations about strengths and resources, and how to bring this together to create a narrative. These are:
5. “What are your strengths?”
6. “What is your story?”
The PTMF has been applied in a range of settings, including service design (Nikopaschos & Burrell, 2020), therapeutic work (Sapsford et al., 2023), group formats (Reis et al., 2019) and staff support in a multidisciplinary team (MDT) setting (Akande & Bland, 2023).
The PTMF and Team Formulations
The use of the PTMF within team formulation meetings is growing (Makwana et al., 2022). A recent study found benefits of using formulation meetings underpinned by the framework in an inpatient setting (Nikopaschos et al., 2023, 2025), including: fewer restraints and seclusion measures; clients learning new and helpful ways of managing their mental health; and staff developing a better understanding of the relationship between trauma and distress. Taking into account Seery et al.’s (2021) findings comparing the impact of describing an individual’s difficulties using the medical model and PTMF, where the former was associated with increased stigma, the benefits of the PTMF are becoming increasingly established.
By allowing time to consider parts of the client’s narrative that may typically be missed during other clinical meetings, PTMF team formulation meetings are likely to lead to a shift in a team narrative about psychosis (please see Supplemental Material A for an example of a complete PTMF diagram following a team formulation meeting). To the research team’s knowledge, there has been no research on the utilisation of PTMF in team formulation meetings in secondary mental health care community services or on the potential influence that this may have on clinicians’ understanding of psychosis within these settings.
Research Aim
The study aimed to explore clinicians’ experience of attending PTMF team formulations meetings and how this may influence their subsequent understanding of psychosis. To achieve this aim, five research questions were developed:
Within the participants’ stories, how was their earliest understandings of psychosis depicted?
Did the dominant illness narrative feature in the narratives? If so, how?
Did the PTMF feature in the narratives? If so, how?
Did the participants’ narratives depict a change in their understanding of psychosis since attending formulation meetings using the PTMF? If so, how?
Did the participants’ narratives depict any change in their practice with clients?
Method
Theoretical Framework
The underlying epistemology employed was critical realism, which focuses on the analysis of structures that underlie social phenomena, such as power relations, community and cultural norms and adversities (Pilgrim, 2022). Critical realism also argues that a deeper, underlying reality exists outside of our subjective experiences (Bhaskar, 1978) and acknowledges the material reality of: the lack of services for people in emotional distress; the restrictive nature of interventions; and the way in which services can cause harm. The PTMF itself also employs a critical realist stance and critiques the privileging of “scientific” knowledge and “psychiatric” models to incorporate what has happened to the person and privileges the meaning of their story.
Design and Narrative Analysis
A qualitative research design was employed, guided by narrative analysis. Narrative analysis allows the contextualisation of individual experiences within their own social, historical, and cultural context (Bruner, 1991) and has the potential to hear multiple voices making up an individual’s story (Frank, 2012), thus allowing the reproduction of the wider MDT’s words or other influencing voices to be heard. In line with a narrative approach, all participants were asked the same single open-ended question, which invited them to tell their story without interruption: “Tell me the story of your understanding of psychosis from as far back as you can remember.” Prompts were used to further explore areas associated with the study’s research questions. The average interview length was 59 min.
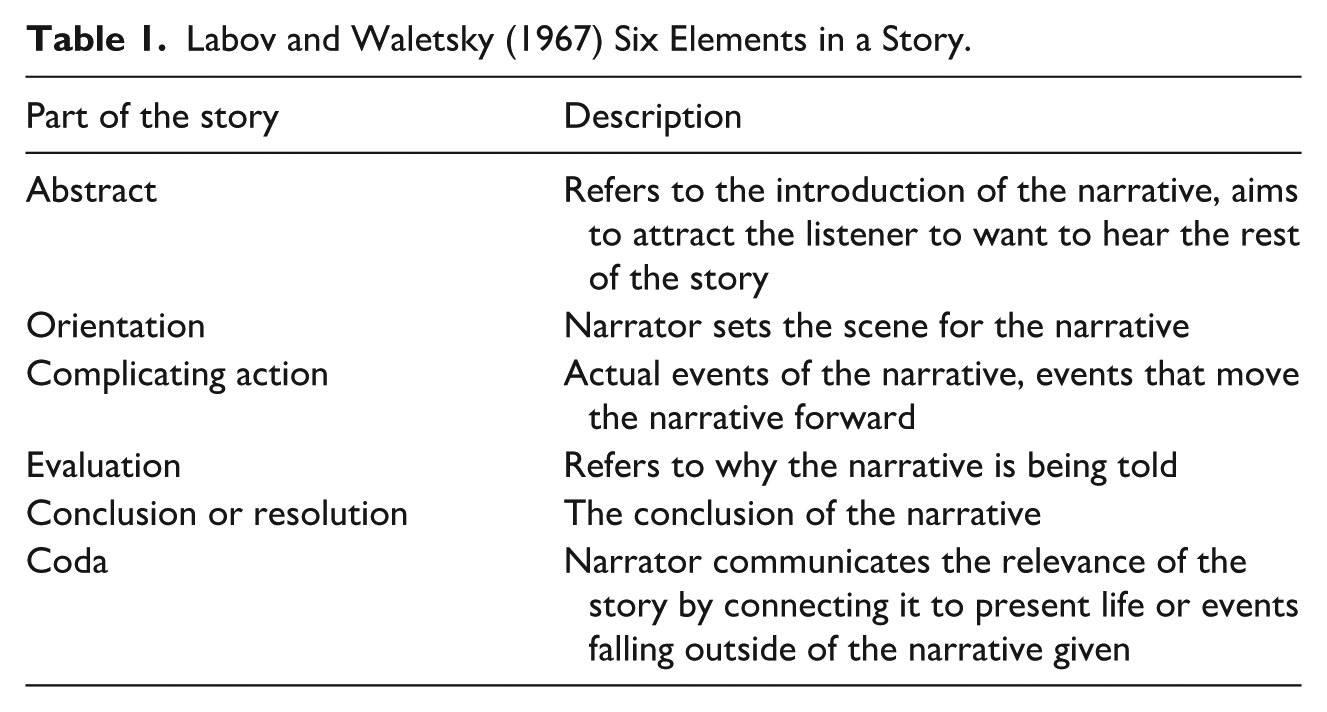
There are no set guidelines for narrative analysis, thus enabling a bespoke analytical approach best suited to answer the research question (Butina, 2015). The present study incorporated structural (Labov, 1972: see Table 1), content (Riessman, 2008) and dialogical (Mankowsi & Rappaport, 2000) narrative analysis approaches. Structural narrative analysis addresses how the person is telling their story, focusing on structural features such as evaluations and turning points (Wieslander & Löfgren, 2023). Content narrative analysis focuses on core themes within and across the participant stories. Finally, dialogical narrative analysis focuses on the relationship between the participant’s personal story and wider societal narratives.
Labov and Waletsky (1967) Six Elements in a Story.
Reflexivity and Quality Assurance
The first author, Meg, is a white British female clinical psychologist, in training at the time of the study, who conducted all 10 interviews. She has experience co-facilitating PTMF formulation meetings and delivering teachings on the PTMF. The second author, Susannah, is a white British female clinical psychologist and academic, with experience of using the PTMF both clinically, and as a framework for research into psychosis. The third author, Isaac, is a Black British male clinical psychologist with experience of using the PTMF in team formulation meetings, reflective practice groups and therapeutic work.
To enhance the quality of the study, the first author sent a synopsis of each participants’ interview to them to check for accuracy. Two participants asked for minor amendments, which were incorporated into the analysis. A process more aligned with narrative analysis may have been iterative narrative conversations alongside member-checking, however due to time restraints this was not possible. During the analysis, reflexive conversations took place within the research team, examining the lens through which the data were being examined and exploring potential biases.
Participants
Purposive sampling was employed, and staff members who had supported clients experiencing psychosis and attended PTMF team formulation meetings were sought and included. An email was sent to MDTs in a mental health NHS trust, where some services conducted PTMF team formulation meetings, and potential participants were invited to contact the researcher. Participant demographic information is shown in Table 2. The participant inclusion criteria were clinicians, previously or currently working with individuals with psychosis and having attended PTMF team formulation meetings.
Participant Demographics.
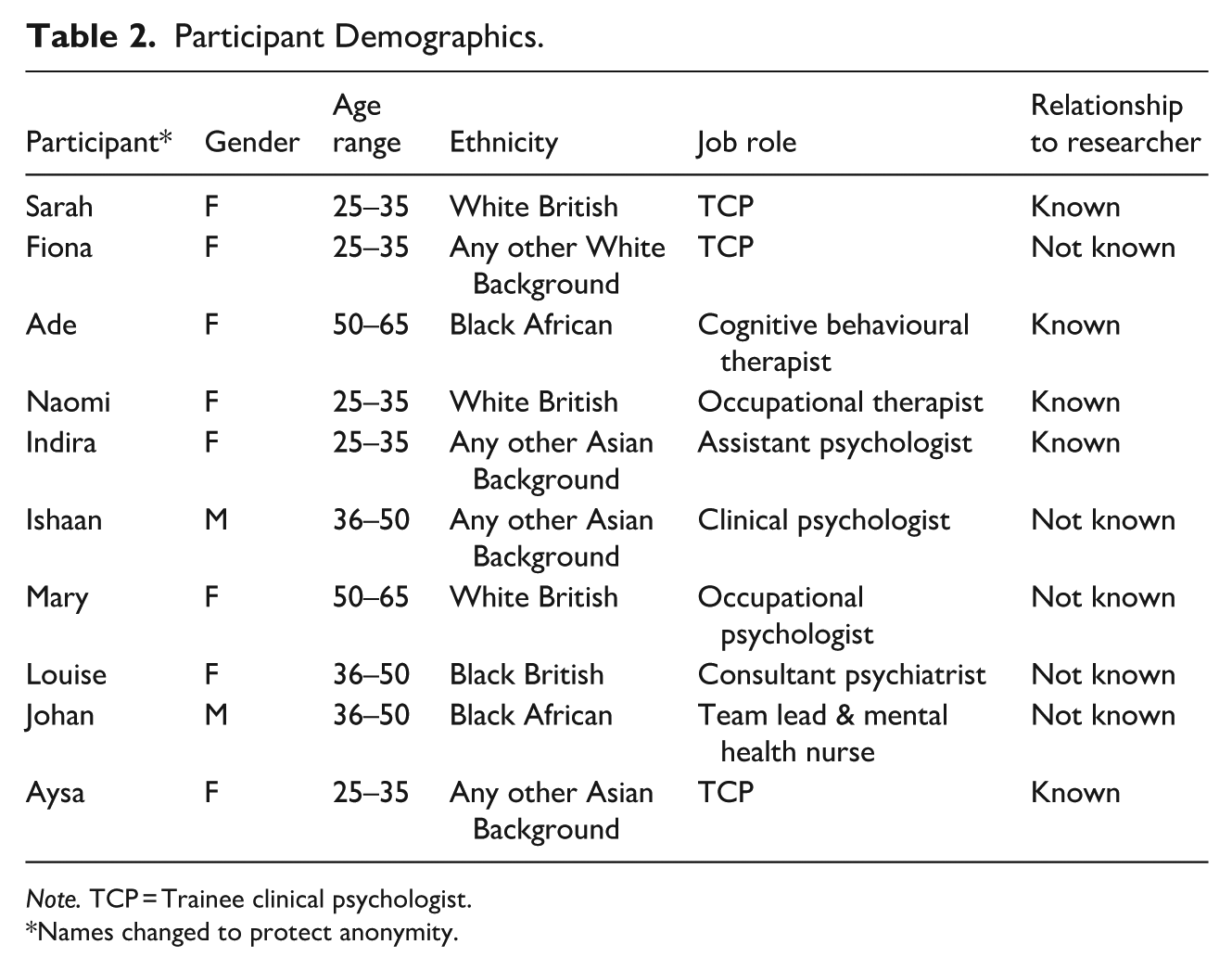
Note. TCP = Trainee clinical psychologist.
Names changed to protect anonymity.
Ethics
The study was reviewed by an NHS Research Ethics Committee and granted approval on May 25, 2023. Each participant read an information sheet and provided written consent. Transcripts were generated from audio recordings using transcription software, following which identifiable features were anonymised and any inaccuracies were manually corrected.
Results
The results have been displayed below with insights from content, structural and dialogical narrative analysis approaches. Please see Supplemental Material B for synopses of the participant narratives.
Within the Participants’ Stories, How Was Their Earliest Understanding of Psychosis Depicted?
The earliest understandings of clinicians tended to serve as the abstract of the narrative and orientated their stories. They varied from a medical model, stories of people they had known personally who had experienced psychosis, a trauma-informed understanding, or understandings based on cultural or religious frameworks.
Four narratives were initially based on medical models. For example, Sarah, a trainee clinical psychologist, began by sharing:
I think the like biological explanations that more prominent hmm mm hmm . . . Or kinda like drug induced explanations for why some cases was kind of more understandable at first. (Sarah)
As her narrative continued, this changed: “I connect a lot more now with just traumatic experiences.” Sarah concluded:
So yeah, I think it’s definitely shifted from where I thought it was, which is probably more biologically mm hmm before. (Sarah)
Her narrative being summarised in this way emphasised her journey and highlighted how her understanding had shifted. This shift was also seen in the narratives of others from a psychology training background and suggested that the further training may have been significant in this development.
Three participants began their narratives with stories from their personal lives. Mary began by talking about a friend:
My first experience of um psychosis um was a close friend who I’d been who’d I’d grown up with and who I was at school. (Mary)
Where personal life stories orientated the narratives, empathy and compassion were a common feature:
It just seemed really sad and, like, and being very aware that they had had a um such a hard life (Fiona)
This was especially apparent when comparing to narratives with a medical understanding. Medically based narratives tended to focus on intellectualising psychosis and holding an emotional distance to participants’ understanding:
When I did my undergraduate in psychology that I may have paid attention to a little bit . . . Umm yeah, I think maybe it was then where I and start to sort of notice that word (Aysa).
Ade started her story by suggesting mental health professionals only diagnose psychosis if they do not agree with what the client’s perception of “normal” is:
If the majority and the patient themselves agree what has happened is normal there will be no psychosis. If our view, especially the professionals, if what we think is different from the patient’s view about their feelings we will call that psychosis so it seems that whatever we don’t understand has to be illness and so we diagnose that. (Ade)
Her narrative encompassed a trauma-informed understanding from the very beginning. Ade conveyed passion throughout her narrative and used examples of clients’ distress mirroring traumas they have encountered:
She’s hearing voices and these voices are those people, the relatives who made her leave the marriage, and because she’s hearing these voices, we are calling it psychosis. (Ade)
It was striking that Ishaan was the only participant to share his initial understanding of psychosis as being based on cultural and religious frameworks. He said these influences would be “a good place to start,” which acted as a strong abstract to his narrative and set the scene. He spoke about the word “Fagol” which, in his first language, refers to “someone who’s mentally unwell but it essentially means crazy person” and how this would be used rather than terms such as psychosis. He compared his religious understanding of psychosis to his cultural understanding of psychosis.
we understand it as Islamically like they've been possessed. Uh so somebody’s happened to them kind of like a jinn has possessed them (Ishaan)
In contrast, Ishaan’s account of his cultural understanding of psychosis has some parallels with the PTMF, particularly in challenging the dominant illness narrative in services and wider society by being curious about adverse life experience:
We think about it it’s like differently, kind of like if someone very stressed out or something’s going on in their life, we we kind of asked like what’s happened to this person, which is quite interesting. Instead of saying what’s wrong with the person, be like, oh, what’s happened to this person? What’s happened in their life? That’s got to this point, that this person is like this, I’m so, yeah. So that’s the contrast between the two (Ishaan)
Did the Dominant Illness Narrative Feature in the Participants’ Narratives? If So, How?
The dominant illness model of psychosis frequently featured in participants’ narratives of psychosis. Seven participants commented on holding, or previously holding, a medical model understanding of psychosis, which served to orientate the narrative. The dominance of this model had mostly stemmed from early education or training:
then I had a more and medicalised understanding of like hearing voices and looking at new brain images and I guess very basic neuroscience around it (Naomi).
The explanations within the narratives varied from the dopamine hypothesis, genetics, neurological and drug-induced psychosis. For example:
Like an imbalance of chemicals in the brain umm whether they might have thought it was drug related or something like that (Louise).
Participants commented on the simplicity of the dominant medical model: “the very medicalised context of psychosis that was a lot easier to understand” (Aysa). Mary similarly implied that the medical model was simple and that it pointed to an obvious intervention: “Then we just called it mental illness and that person had been sectioned.” This may suggest the participants found it easier to submit to a simpler dominant narrative rather than forging their own ideas. Aysa spoke of being younger when she held the medical model:
I think when I was younger and I and learning about psychosis, then I didn’t see a problem with that before . . . Uh . . . Working within very medicalised frameworks not accounting for difference you know. (Aysa)
This again may speak to it feeling easier to accept learnt explanations of psychosis and working within frameworks associated with it.
Some participants showed anger towards the medical model after further exposure to it in services. Aysa spoke of medical interventions being forceful and restrictive:
then this history of being hospitalised and and sectioned and and and, you know experience like it’s lots of restrictive and quite oppressive services. (Aysa)
Fiona also commented on the restrictive interventions used when working with psychosis within medical model frameworks:
I had like a big thing of like, oh, this is wrong, this is over medicalised and it was hard seeing people being restrained, seeing people being put in seclusion. (Fiona)
The emphasis on it being hard to see illustrates Fiona’s emotional response to such interventions. She went so far as to describe professionals diagnosing psychosis as “brandishing it a medical problem.” “Brandishing” implies a weapon, suggesting that there may exist understandings that view the medical model as potentially threatening and harmful to clients. This anger often served as the complicating action element of the narratives by moving it forward. Following a conversation with a “holistic therapist,” who commented on their language preferences in client notes, Naomi said she was careful of what she wrote in clinical notes and avoided using medicalised language:
I’ve really stopped and paused before I’ve written like delusions and hallucinations because I find it quite like . . . umm, I suppose I I do kind of question like how almost like the fairness of me to kind of come to that conclusion. (Naomi)
Ishaan, Ade, and Indira did not depict any influence of the medical model on their understanding of psychosis. For example, Ishaan said that, despite learning about the medical model, he had not felt like he understood it:
I remember being taught about schizophrenia and psychosis as a brain disease and I remember we had a lecture and they were showing the brain, and it was talking about dopamine. And then it became this biological, physical entity, and I could never really understand it, to be honest with you. (Ishaan)
It seemed that alternative understandings, away from the medical model, were only offered in higher education. While this was mostly seen to be offered on psychology trainings, Louise also spoke of later trainings in psychiatry offering different perspectives. Fiona spoke of learning about the significance of trauma and being encouraged to question dominant models during her clinical psychology doctorate training:
I feel like the ideas around psychosis that we had in training were very much. Umm, you know this is seeing it in a way as a response to life events and to trauma. Umm and to experiences, experiences of exclusion and discrimination and racism. Umm and questioning that medical model. (Fiona)
Did the PTMF Feature in the Narratives? If So, How?
The PTMF appeared in eight narratives. Participants articulated having been on a gradual journey with regards to their understanding of psychosis. It seemed that participants came across different influences throughout their lives that shaped how they conceptualised psychosis. However, the influence of the PTMF formulation meetings seemed to be a turning point in six of the narratives. In Mary’s narrative, she positioned the PTMF as the reason her understanding shifted and conveyed a passion for it by commenting that it was why she wanted to participate in the study:
The power threat meaning framework, I do know that that has changed my understanding . . . That’s partly why I agreed to make time for this interview . . . Understanding that psychosis is more a reaction to life and and trauma and life the experiences in life. (Mary)
Similarly, Louise commented on the influence of the PTMF:
I think that’s where the power threat meaning framework have been really helpful just to give a full context of who is this person, what have their experience has been, what has happened to them umm and what has contributed to umm some of their experiences now that we might label as psychosis. (Louise)
The PTMF tended to appear towards the end of most participants’ narratives acting as the conclusion. In comparison to other understandings presented, participants provided examples connecting the PTMF to present life, which operated as a coda to their story. This was often an example of a client who had been discussed during a PTMF formulation meeting, and how the way clinical staff made sense of the client’s experiences had changed through the process. For example, Louise shared an example of a client who was described as “verbally aggressive” and by using the PTMF, the team could see how this client’s experience of childhood abuse may have led her to behave in this way:
almost reinstate themselves and let others know actually you can’t just walk all over me, you can’t bully me. (Louise)
The PTMF often featured in participants’ concluding statements. However, Ade used the PTMF to orientate her narrative. It set the scene for her story, which focused solely on the trauma lens of psychosis. The PTMF featured in her Labovian complicating action, evaluation and conclusion. Sarah and Indira did not directly mention the PTMF, however similarly reported a journey and felt that they presently held a trauma-informed understanding of psychosis. Johan felt the PTMF formulation meetings could be improved with the inclusion of a client:
Maybe what will would also benefit the discussion or enrich the discussion will be to get to the service user if he or she agrees to be part of the discussion would have been to be very, very good, unfortunately, we don’t have them, but we bring their voice alive. (Johan)
Did the Participants’ Narratives Depict a Change in Their Understanding of Psychosis Since Formulating Using the PTMF? If So, How?
Where the PTMF featured in narratives, it was depicted as a catalyst for a change in understanding of psychosis or a framework that supported or consolidated a change in participants’ understanding.
Five participants commented on the PTMF as a team formulation tool, facilitating an appreciation for the humanity of the clients. Johan spoke of the PTMF formulation meetings allowing an individual’s “flesh” to develop from their “bare bones” and that the conversations gave clients a “human face.” This metaphor provided a strong image of a client being rehumanised during the PTMF formulation meetings, following the potentially dehumanising effects of the medical model. Later in his story, Johan described the humanising of clients as being a unique feature of the PTMF:
Oh wow was it this person you know in humanises the patient in a way that was in the way that I I I think would be different with the other tools. (Johan)
In this way, the participants depicted a change in their understanding of psychosis as a human response to adversity and trauma, which challenged the dominant medical model. Additionally, in multiple stories, there was a development in the language used. Participants moved away from labelling clients as a “patient,” or grouping them as “people,” to using humanising and individuating language such as “person” or “human being.”
Ishaan further emphasised the naturalness of having responses to trauma as human beings: “we as human beings have experiences and some of those experiences can be quite distressing.” He later spoke about being able to relate to experiences that would be labelled as “paranoia” in services:
There’s times when I become very suspicious when I’m in white spaces in sense of harm that could come to me as well. Is that paranoia, is that psychosis? It’s not. It’s a . . . it’s a mechanism in a way, to kind of let me know that potentially I could be in danger, physical danger or some kind of social danger . . . Is it helpful for me? Yeah. (Ishaan)
This striking comment, on the power relationship between white dominance and minoritised ethnicities in society, came after discussing the implementation of the PTMF in his team. Conversations around power seemed to emerge during the PTMF team formulation meetings as teams took the time to consider the significance of power throughout clients’ lives and the influence of living in a society that created the need for strategies to keep themselves safe. These conversations also allowed for a consideration of the role of power in their own lives. This resonated with Naomi, who commented on the freedom she held as a white British woman: “Yeah, I guess I didn’t realise how much freedom maybe I perceive I have.” Thus, the PTMF was depicted as not only influencing participants’ narratives of psychosis, but their own life stories as well, and how they related to themselves alongside their clients.
Did the Participants’ Narratives Depict Any Change in Their Practice With Clients?
Some participants shared concerns about how the PTMF team formulation meetings may not have led to changes in how they, or the team, would support the client. Fiona shared her difficulty with moving the work with clients beyond the formulation meeting:
My own struggles to move on to more like move on beyond that kind of formulation stage, I didn’t necessarily feel like I knew or had much more of a clearer understanding of how to support people and how to yeah work with people going beyond this. (Fiona)
While the PTMF formulation may indicate psychological and social approaches to working with psychosis, the dominance of the medical model in determining treatment may mean staff find these alternative approaches as less accessible. This reflection came at the end of Fiona’s narrative, which may mirror the process in team formulation meetings, that implementing the PTMF formulations into care planning remained an afterthought. In contrast, Johan, who was a service team lead, spoke highly of the PTMF informing clients’ care plans:
The objectives of the formulation is to give us insight you know and to to be able to sort of think through, uh, different approaches in caring for the patient effectively so there’s a direct relationship with what what is considering formulation and how that is fed into the care plan. (Johan)
Discussion
The current research used narrative analysis to explore clinicians’ experiences of PTMF team formulation meetings and how this may have influenced their understanding of psychosis. Participants’ initial understanding of psychosis often reflected a medical model, shaped by education, culture, religion, and other life experiences. The dominant illness narrative was prevalent, particularly among those with early medical training. However, engagement with the PTMF was noted to shift perspectives, fostering a more trauma-informed and humanising understanding of psychosis. While some participants felt that the PTMF led to a more compassionate approach to client care, others expressed concerns about translating these insights into practical changes in the support provided to clients. These findings will be discussed alongside the study’s strengths and limitations, clinical implications, and suggestions for future research.
Seven participants said they had previously held a medical understanding of psychosis, reflecting the dominance of this narrative. This resonates with the findings of Bentall (2004) that the medical model dominates how psychosis is understood and influences the subsequent interventions offered by services. In the narratives, this understanding stemmed from early education or training, and many medical influences on the development of psychosis were discussed. However, two participants did not mention the medical model, and one stated they had never understood the significance of it. These participants held understandings shaped by religious, cultural and/or trauma and adversity frameworks. This aligns with literature highlighting the growth in the understanding of the role of trauma, adversity and discrimination in psychosis (Read & Larkin, 2008). These three participants came from a psychology background, which may have meant that their training emphasised the role of trauma in mental health. Two participants spoke about the restrictive interventions the medical model can lead to, which contrasts Nikopaschos et al. (2023) who found a reduction in the use of restraints and seclusion measures on a ward following the introduction of the PTMF in formulation meetings (alongside other changes to embed trauma-informed care approaches). This demonstrates possible benefits of implementing the PTMF in other services, particularly around shifting interventions offered and the reduced use of restrictive practices.
Some participants commented on the PTMF leading clients to be discussed in a way that brought out their humanity. There was a development in the language used in the narratives, which moved away from labelling clients as a “patient” or grouping them as “people,” to using humanising language, such as “person” or “human being.” This is consistent with previous research exploring team formulation meetings, which found that they influenced participants to view clients as more of a “person” and less of a “patient” (Murphy et al., 2013). Additionally, Geach et al.’s (2018) review reported increased empathy towards clients following team formulations. It’s however important to note that there are some concerns about team formulation meetings within the literature, for example, some staff described them as an excuse for a client’s behaviour (Summers, 2006).
Johan commented on how the PTMF formulation meetings could be enhanced by the presence of the client. In a first-person account of psychosis, Fox (2021) commented on the value of “user-led models of care” (p. 1516), which highlights the importance of accessing the lived experience of the service user through their own knowledge and relationship to their experiences. By including the client in formulation meetings, clinical team may benefit from a more holistic understanding of the person’s experiences and needs.
Six participants referred to having known friends and family members who had experienced psychosis, thus showing the development of an understanding of psychosis arising from personal experiences, as well as professional. There was an observed contrast of the presence of empathy and compassion when the narratives started with personal life stories compared to a medicalised understanding, which tended to focus on intellectualising psychosis and holding emotional distance. Yakeley et al. (2014) identified a focus on memorising knowledge and “facts” as a potential mechanism through which this emotional distancing from clients can occur. Early education, such as A-levels and undergraduate degrees, narrowed understandings of psychosis as being mostly medical in nature and providing an explanation, rather than allowing prospective clinicians to see the whole person. Encouraging people to think outside of professional or educational boundaries seemed to enable the endorsement of trauma as an explanatory model.
Some participants reflected upon the power in their professional roles and how this influences clients. These comments seem to have been a result of the attending PTMF formulation meetings and subsequently considering their professional power and the role this can play in people’s difficulties and stories (Johnstone & Boyle, 2018). Despite this reflection on professional power being shown to be useful in the participant narratives, the PTMF has itself been critiqued for failing to acknowledge the power inherent in a framework that makes interpretations about individuals’ experiences (Morgan, 2023).
Although the PTMF formulation meetings were described in a broadly positive manner by participants, some clinicians mentioned that they rarely led to a change in the intervention clients received. Similarly, Geach et al. (2018) found that team formulation meetings did not always lead to subsequent changes in the clients’ care plans. Furthermore, due to an increased awareness of systemic factors beyond their control impacting on clients, team formulations can lead to staff experiencing powerlessness or hopelessness (Buckley et al., 2021). It is plausible that these feelings may contribute to the experience of team formulation meetings being ineffective from a practical perspective. Buckley et al. (2021) advised that facilitators should prepare staff for the possibility of these complex feelings arising and provide support to work through them. In contrast however, more recent research has shown changes in practice following the implementation of PTMF formulation meetings (Nikopaschos et al., 2023, 2025). Similarly, Johan spoke of the meetings translating into clients’ care plans, which mirrors findings from previous research (Hartley, 2021).
Given that participants in the study mostly came from a psychology background and the fact that team formulation meetings promote psychological thinking (DCP, 2011) and are often facilitated by clinical psychologists (Health and Care Professions Council, 2015), the broadly positive view of PTMF team formulation meetings may be a result of bias. This vested interest may be amplified given the study was specifically looking at the PTMF as a formulation tool, which has received growing interest within psychological professions (Makwana et al., 2022). The literature shows that staff from different disciplines may have alternative perspectives on team formulation meetings, for example perceiving them as a space where colleagues seek to seem powerful or have the right answers (Summer, 2006).
Strengths and Limitations
The study has both strengths and limitations. The narrative style of the interviews allowed participants to tell their own story freely, which may have been restricted if a structured interview approach was used. The use of content, structural and dialogical narrative analysis approaches allowed for an in-depth analysis of the data and provided extensive insights.
There were limitations with the gender diversity within the sample, with only two male participants. Narratives of empathy and compassion were emphasised in the study, which aligns more with societal conceptions of femininity and caregiving approaches towards emotional distress (Smith, 2025). It is likely that narratives more fitting with traditional views of masculinity, such as holding back emotions, may have been missed. Secondly, most participants from the study had a psychology background, which may have led to the overemphasis of trauma-informed understandings of psychosis.
Clinical and Research Implications and Recommendations
The study findings suggest that the PTMF can support clinicians in developing an alternative understanding of psychosis. What the formulation meetings might be lacking is how to translate these understandings into care plans. Additionally, the narratives showed that allowing staff to think outside of their professional or educational relationship with psychosis may open possibilities with regards to endorsing a more trauma-informed narrative.
Future studies should look to include clients who have been the focus of a PTMF formulation meeting, to explore their experience of care within their service and any changes in their own understanding of distress. To the research team’s knowledge, there are limited PTMF team formulation meetings that take place with the client present. Services may wish to work towards enhancing the client voice and move towards collaborative formulations, providing a meaningful care plan that holds the client’s strengths and goals in mind. Additionally, due to the over-representation of participants with a psychology background, it would be beneficial to gain a wider understanding of other MDT clinicians’ narratives of psychosis following their attendance at PTMF formulation meetings.
Conclusion
This study used a narrative analytic approach to explore clinicians’ experiences of PTMF team formulation meetings and how they influenced their subsequent understanding of psychosis. Overall, the study found positive stories from using the PTMF as part of a team formulation and illustrated how this shaped how clinicians understood psychosis. Future research may wish to focus on clients’ understandings of psychosis to gain a deeper understanding of the PTMF’s influence on psychosis narratives.
Supplemental Material
sj-docx-1-jhp-10.1177_00221678261462068 – Supplemental material for The Stories of Staff Members’ Understanding of Psychosis With the Use of the Power Threat Meaning Framework
Supplemental material, sj-docx-1-jhp-10.1177_00221678261462068 for The Stories of Staff Members’ Understanding of Psychosis With the Use of the Power Threat Meaning Framework by Meg Bland, Susannah Colbert and Isaac Akande in Journal of Humanistic Psychology
Footnotes
Ethical Considerations
This study was approved by the HRA and Health and Care Research Wales Ethics Committee (approval number 319009) on May 25, 2023. Each participant read the information sheet and provided informed written consent to conduct and publish the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available from the corresponding author upon reasonable request, until 2032, when they will be deleted as an Ethics Committee requirement.*
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.