
Abstract
A defining characteristic of humanistic psychotherapy is its focus on the therapeutic relationship. This could position it as a preferred approach for treating trauma symptoms, but scientific evidence detailing its benefits in this regard is still limited. The aim of this review was to identify the most relevant contributions of the humanistic model’s main therapies to the treatment of trauma-related issues. Following PRISMA guidelines, a systematic review of studies published in Scopus, Web of Science, PsycINFO, and PubMed was conducted. Empirical studies and reviews published in Spanish or English that applied humanistic psychotherapy to trauma-related symptoms were included. Twenty-three out of 392 studies were selected for the review. They were classified according to the specific humanistic therapy used: emotion-focused, Gestalt, person-centered, existential, focusing-oriented, or other. Most empirical studies showed lower dropout rates, significant reductions in symptoms, and efficacy comparable to cognitive-behavioral therapies. Although more research is required, the specific characteristics of humanistic psychotherapies may make them effective treatments for patients with trauma-related symptoms, potentially offering advantages in terms of treatment adherence and patient wellbeing.
Keywords
Introduction
Psychological trauma refers to the emotional wound that remains after a person experiences a situation that overwhelms their processing capacity and threatens their survival. This wound can be manifested at the emotional, physiological, behavioral, as well as cognitive levels, and impact the brain’s executive functions, a person’s self-esteem, and the way one relates to oneself and others (Van der Kolk, 2014). The Diagnostic and Statistical Manual of Mental Disorders (DSM-V-TR; American Psychiatric Association [APA], 2022) includes post-traumatic stress disorder (PTSD) as a diagnostic label for individuals who have been exposed to a traumatic event through direct experience, witnesses, exposure to repeated or extreme details, or knowledge that the event occurred to a close family member or friend. After the exposure, they manifest several characteristics from four symptom clusters (intrusion, avoidance, negative alterations in cognition and mood, and hyperarousal) for at least 1 month. Nevertheless, a person may exhibit trauma-related symptoms and require specialized psychological treatment even without meeting all the criteria for a PTSD diagnosis.
Moreover, a person may experience a single traumatic event or face an accumulation of traumatic events. Repeated exposure to traumatic experiences has been shown to increase the complexity of PTSD symptoms (Cloitre et al., 2009). Some authors argue that there should be a separate diagnostic category for this phenomenon currently referred to as complex trauma, because traumatic situations are more diverse, and the resulting effects on the individual are deeper due to the cumulative harm and the need to develop adaptive survival strategies in a traumatizing context (Nieto Martínez & López Casares, 2016).
In addition to PTSD and complex trauma, other authors speak to the existence of attachment trauma. Based on Bowlby’s attachment theory (1989), this refers to psychological harm experienced by an individual after suffering episodes of hostility from their attachment figures during childhood (Bowlby, 1989). Such episodes can range from physical aggression to verbal or physical rejection, emotional abandonment, neglect, or devaluation. This type of trauma can lead to diverse forms of psychological harm (Lahousen et al., 2019), as well as to the development of pathologies in childhood (Haliburn et al., 2011) and the emergence of somatic symptoms in adulthood (Sansone et al., 2009).
Due to the magnitude and breadth of the damage caused by experiencing one or more traumatic situations, individuals with PTSD or trauma-related symptoms often develop other conditions such as depression, anxiety, behavioral, or substance abuse-related disorders (APA, 2022), among others. In terms of treatment, the main goal is to help the person regain control over their mind and body, as well as their ability to self-regulate (Van der Kolk, 2014). This might be divided into four sub-goals (Van der Kolk, 2014): (a) achieving a state of calm and focus; (b) maintaining this calmness when confronted with stimuli that trigger memories of the traumatic event; (c) fully living in the present and interacting with the environment; (d) no longer needing to hide aspects of oneself, the traumatic event, or survival strategies, thus freeing oneself from shame and guilt.
According to a recent meta-analysis (Mavranezouli et al., 2020), the psychological therapies with the most empirical support received to date for treating PTSD in adults are Cognitive Behavioral Therapy (CBT) and Eye Movement Desensitization and Reprocessing (EMDR). Both are trauma-focused, directive therapies which share a common technique, exposure to trauma-related stimuli, with the aim of reducing the distress they cause in the individual (Jericho et al., 2021; Morris et al., 2021). Moreover, Trauma-Focused Cognitive-Behavioral Therapies (TF-CBT) have proven to be more effective than pharmacological interventions in reducing PTSD symptoms and comorbid psychopathologies (Coventry et al., 2020). Within TF-CBT, the National Institute for Health and Care Excellence (NICE, 2018) more specifically recommends Cognitive Processing Therapy (CPT), Narrative Exposure Therapy (NET), and Prolonged Exposure Therapy (PET) as first-line treatments. EMDR is considered a second-line option when a patient does not adhere to or benefit from the previous therapies.
However, one of the limitations of these therapies is the high dropout rate among patients. Research has evaluated the efficacy of CBT for victims of gender-based violence with PTSD and recorded a 24% dropout rate (Santandreu & Ferrer, 2014). Similarly, a systematic review of effective treatments for adults suffering PTSD as a result of terrorist attacks has shown dropout rates in CBT groups ranging from 0% to 53%, with an average of 22.7% (García-Vera et al., 2015). Additionally, one study testing the efficacy of TF-CBT for victims of terrorism with PTSD reported a 28.6% dropout rate (Gesteira et al., 2018). Later, research specifically focused on dropout rates in PTSD therapies found that, on average, 16% of patients discontinued therapy (Lewis et al., 2020). When focusing only on cognitive-behavioral and EMDR therapies, this figure rose to 19.9%. This phenomenon was explored in a group of patients aged 7 to 17 who were receiving TF-CBT, and a 26.8% dropout rate was found (Yasinski et al., 2018). It was concluded that avoidance symptoms and difficulty establishing a therapeutic alliance in the early sessions were predictors of therapy dropout.
Establishing such a therapeutic alliance right from the outset is crucial when working with any patient. However, for individuals who have experienced traumatic situations, it becomes especially important to create a secure and trusting bond with the therapist, as fear, shame, and guilt are often prominent emotions. This can be achieved by validating the victim’s narrative, maintaining an open attitude, and ensuring the person feels understood and validated (Nieto Martínez & López Casares, 2016). It is noteworthy that humanistic psychotherapy focuses on the therapeutic relationship as a tool for change. However, the evidence supporting the effectiveness of this model for trauma treatment is still limited, albeit promising, highlighting the need to further examine its potential contributions to this field.
Humanistic psychotherapies claim that people naturally tend to develop their potential, and that the therapeutic space should be an environment of trust and empathy which facilitates self-exploration and encourages this development, thereby fostering the acquisition of resources to live in a more adaptive way (Cain et al., 2016). Therapies from a humanistic approach take into account the subjectivity of patients and seek to understand them from their perception of reality rather than from a diagnostic label. These therapies have a greater focus on emotions and the ‘self’, understood as self-concept, self-knowledge, and self-efficacy. Moreover, they understand the person holistically, as an indivisible organism in constant interaction with its environment (Cain et al., 2016).
One of the greatest challenges of the humanistic approach since its beginnings has been to adjust to the methodology of academic research, marked by behavioral and later cognitive-behavioal models. Humanistic psychology has opted for a research methodology that responds to the complexity and openness of human phenomena, taking into account the unique characteristics of each individual and their capacity for creativity (Polkinghorne, 1992). In this approach, therefore, qualitative or single-case research takes priority over empirical studies with large samples where all possible variables are operationalized and controlled, and whose aim is to generalize results and establish structured therapeutic protocols. This makes it difficult for certain institutions to propose humanistic procedures as treatments of first choice.
It is understood that one of the reasons why cognitive-behavioral models have a high dropout rate in the treatment of PTSD is because of a less pronounced focus on the therapeutic relationship (Yasinski et al., 2018). It is also known that one of the basic pillars of psychological intervention in humanistic therapies is the establishment of such a relationship (Cain et al., 2016). It is critical, therefore, to improve our understanding of how such therapies may contribute to the improvement of the symptomatology associated with trauma. To this end, this study conducted a systematic review of the literature aimed to explore the contributions of humanistic therapies to the psychological treatment of patients with a history of trauma. The handbook of research and practice of the humanistic approach was used to select the main therapies within this model (Cain et al., 2016), which are described below.
Person-Centered Therapy
Person-centered therapy (PCT) is widely recognized as one of the approaches that has most significantly contributed to the development of the concept of the therapeutic alliance, which is currently regarded as a key predictor of success in psychotherapy. By emphasizing empathic dialogue, unconditional positive regard, and the therapist’s authenticity, PCT establishes a safe therapeutic environment that fosters the patient’s self-support and self-regulation (Rogers, 1951).
Gestalt Therapy
Gestalt therapy (GT) emphasizes authentic contact and dialogical exchange, providing an experiential framework that promotes awareness in the ‘here and now’. This approach assists patients in identifying present emotions and unmet needs, while also offering a wide range of practical contributions through a variety of therapeutic techniques (Perls, 1976).
Focusing-Oriented Therapy
This therapy highlights the intrinsic connection between bodily experience and emotional processes. It supports patients in becoming aware of bodily sensations that, once processed, can give rise to profound psychological change. Focusing-oriented therapy (FOT) thus offers a valuable pathway for accessing implicit material and fostering experiential transformation at a somatic level (Gendlin, 1996).
Existential Therapy
Existential therapy (ET) integrates a philosophical perspective on human existence, emphasizing the search for meaning as a central dimension of psychological well-being. Its major contribution lies in providing patients with a framework to confront existential anxiety and to transform it into an opportunity for personal growth and resilience. This approach is particularly relevant in the context of borderline situations, drawing primarily on experiential strategies (Yalom, 1980).
Emotion-Focused Therapy
Emotion-focused therapy (EFT) offers a powerful framework for the processing and transformation of maladaptive emotional responses learned from past experiences, enabling patients to reconstruct more adaptive self-narratives. Its primary contribution resides in the integration of a strong therapeutic alliance, with specific tasks aimed at facilitating emotional processing, thereby fostering change both at the level of subjective experience and within interpersonal relationships (Rice & Greenberg, 1984).
Objective
Like the literature reviewed above, the aim of this systematic review was to identify the different contributions made by the main humanistic models to the psychotherapeutic treatment of PTSD or symptoms associated with traumatic experiences. This could provide evidence of the efficacy of the humanistic approach in this context and thus establish the basis for more effective intervention proposals.
Method
Search Strategies, Data Sources, and Selection Process
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA, Page et al., 2021) statement for the search and selection of articles. The databases consulted were Scopus, Web of Science, PsycInfo, and PubMed. The search terms were grouped into the following six formulas, requesting that they appeared in the title and/or abstract of the articles: ‘person-centered therapy’ AND ‘trauma’; ‘gestalt therapy’ AND ‘trauma’; ‘focusing-oriented therapy’ AND ‘trauma’; ‘existential psychotherapy’ AND ‘trauma’; ‘emotion-focused therapy’ AND ‘trauma’; and (‘humanistic therapy’ OR ‘humanistic psychology’ OR ‘humanistic psychotherapy’) AND ‘trauma’. The search process was conducted between January and April 2024. The search, screening, and study selection were conducted by the first author and, whenever doubts arose, discussed with the second author.
Eligibility Criteria
The inclusion criteria were: empirical studies or reviews in which trauma was treated using a humanistic psychological approach; publications from scientific journals written in English or Spanish. No limit was set on the date of publication so as not to overlook studies that might be relevant.
Data Collection and Synthesis of Results
The articles were divided according to type of study -empirical or reviews- and were analyzed by summarizing the main characteristics, the participants and evaluation instruments (in the case of empirical research), the objectives, and the main results or conclusions. Then, a narrative synthesis of the most relevant results of each article was performed.
Results
Study Selection
The selection process is displayed in the PRISMA flow diagram (Figure 1), which details the reasons for exclusion where applicable. The initial search generated 392 results from the four databases. After eliminating duplicated documents, 215 articles were left for a first screening of titles and abstracts, 150 of which were excluded. Ten of the remaining 65 articles could not be retrieved, so the remaining 55 were downloaded for full-text reading. Finally, 32 articles were discarded applying the above-mentioned inclusion criteria, and 23 articles were included for review (Figure 1).
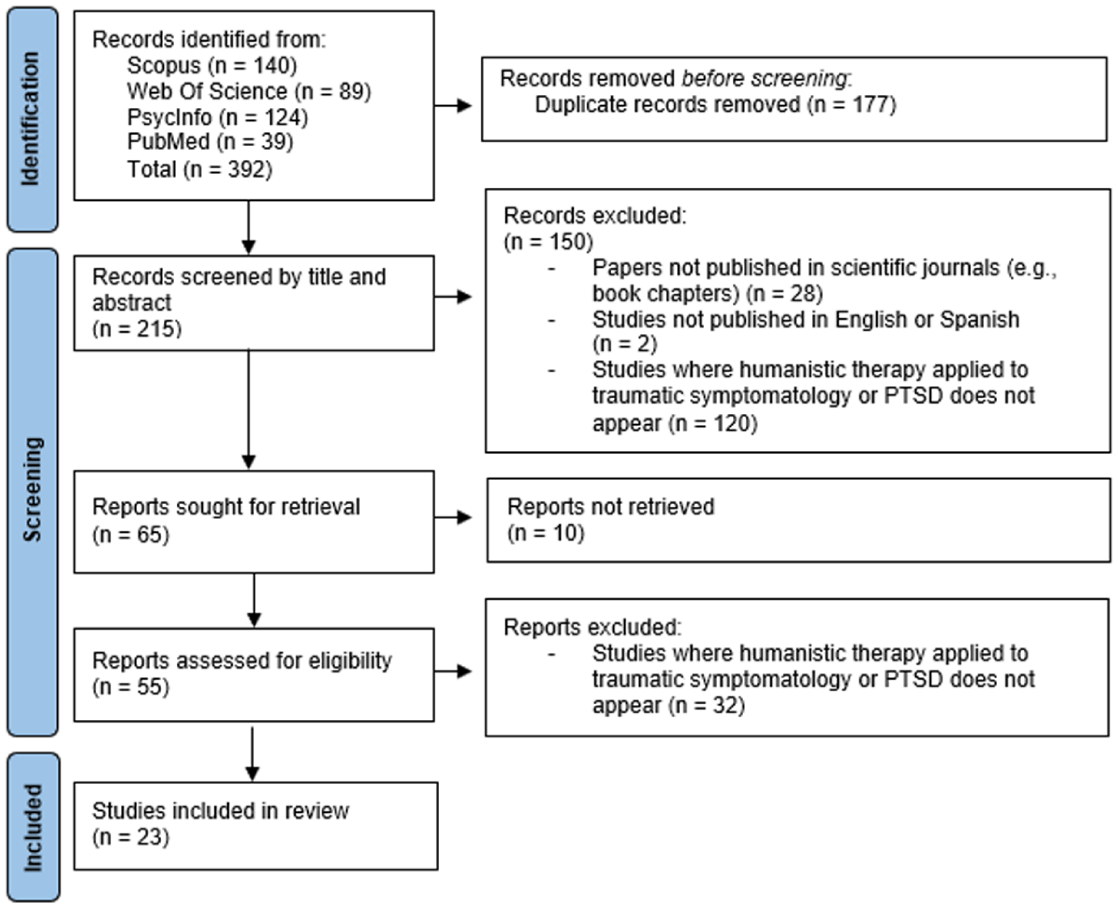
PRISMA flow chart of the selection process.
Seventeen of the included articles were empirical studies, and six were reviews. As for the type of therapy analyzed, EFT was most frequent (n = 8), followed by GT (n = 6), PCT (n = 5), ET (n = 1), and TOF (n = 1). Some articles referred to other humanistic therapies without specifying any of the above categories (n = 3).
Characteristics of the Studies Included
Regarding the type of trauma treated, 11 studies focused on PTSD without specifying the traumatic event. In the others, traumatic symptoms were caused by child abuse (n = 6), sexual abuse (n = 3), intimate partner violence (n = 1), interpersonal violence (n = 1), or loss of a partner after war (n = 1). As for the gender of the participants, six of the empirical studies focused exclusively on women and seven included participants of both genders, although women represented a higher percentage (ranging from 53.3% to 81.9%). Four studies did not specify the gender of the participants. The studies were conducted in Canada (n = 6), the United States (n = 7), Germany (n = 4), the United Kingdom (n = 2), Poland (n = 1), Bosnia and Herzegovina (n = 1), Chile (n = 1), and Israel (n = 1). As for the date of publication, nine studies (39.13%) were published in 2014 or before and 14 (60.87%) after 2015, that is, within the last 10 years of the period under review. Tables S1 and S2 (Supplemental Material) present the main characteristics of the articles analyzed, including the most relevant objectives and results with regard to the purpose of this article, and are ordered according to the type of humanistic therapy studied for ease of reading. EFT and PCT share one article, which has only been included in the EFT section.
Narrative Synthesis of Results
Emotion-Focused Therapy
Within the humanistic approach, emotion-focused therapy (EFT) is the most studied therapy style and is positioned as an empirically supported treatment for PTSD, which makes use of the therapeutic alliance and emotional processing of trauma as its main tools for patient recovery (Lee et al., 2022). In their case study (n = 4), Murphy et al. (2019) point out four therapeutic principles of EFT (shared with PCT) that would be essential in the early stages of treatment of PTSD: (a) Generating a therapeutic alliance from the outset, so that a safe and trust-based environment is established; (b) Facilitating the narration of the traumatic event, as it is often not the main reason for consultation and can be dominated by emotions of shame, guilt and fear; (c) Helping identify and explore the traumatic sources of current problems and distress, as EFT is not only about working on past events but also about understanding how they can affect the present moment; (d) Offering empathic responses focused on self-support and autonomy, and thereby facilitating emotional regulation.
As for empirical studies demonstrating the efficacy of EFT in working with trauma, significant improvements were observed in PTSD symptoms caused by child abuse after treatment with EFT (15.9% dropout rate, Holowaty & Paivio, 2012). In addition, patients undergoing this therapy perceived the useful elements to be related to a greater focus on the event and on emotional expression. One example, among other applications, is the empty chair technique, taken from GT, which allows patients to interact symbolically with the abuser or with damaged parts of themselves. Within emotional expression, the emotion found to be the most useful to work with was anger in terms of experience, legitimization, and expression.
Similarly, a significant reduction in PTSD symptoms related to intrusions and hyperarousal after treatment, and avoidance 3 months post-treatment, has been observed in female survivors of sexual assault (7.1% dropout rate, Anderson et al., 2010). Furthermore, a comparison was made of two versions of EFT applied to adults who had suffered child maltreatment (Paivio et al., 2010); one in which confrontation in imagination is used, and the other in which the problem with the aggressor is resolved exclusively through interaction with the therapist. The findings revealed significant improvements with regard to trauma symptoms, and maintenance of these improvements 1 year after treatment in both versions. Nevertheless, the dropout rate was significantly lower in the therapist interaction group (7%) compared with the imaginative confrontation group (20%).
However, two studies in which participants had experienced childhood abuse did not find significant results for the reduction of PTSD symptoms after EFT treatment, although EFT was effective in improving marital satisfaction (Dalton et al., 2013), in decreasing expressions of distress, as well as in increasing primary adaptive emotions (Khayyat-Abuaita et al., 2019). In addition, a direct relationship was observed between this increased access to and experience of primary adaptive emotions and positive therapy outcomes (Khayyat-Abuaita et al., 2019).
When applied in the context of complex trauma, the following general characteristics of EFT have been identified as a result of a systematic review (Mlotek & Paivio, 2017): (a) emphasis on generating a therapeutic alliance from the outset as a tool for change, because a safe interpersonal experience like this could be generalized to other relationships; (b) facilitation of emotional regulation through the therapist’s empathic response, which helps modulate the intensity of emotions, rather than by training in self-regulation skills; memory work and emotional reprocessing through techniques based on imaginal exposure, such as the empty chair; (c) development of new adaptive meanings in relation to the narrative of the traumatic event and the perception of self and others; (d) modification of maladaptive emotions such as fear and shame, and access to inhibited basic adaptive emotions such as sadness and anger; (e) focus on the patient’s experience rather than on directed psychoeducation, as exploring the patient’s feelings and meanings in vivo is understood to be more effective than talking about them on a theoretical level; (f) focus on current difficulties as well as on resolving past problems that have become entrenched and are a source of distress and maladaptive behaviors.
The capacity of EFT to work with inhibited emotions and to reframe traumatic experiences makes it clinically valuable. However, some methodological limitations and the heterogeneity of procedures may make it difficult to determine which components of the approach are most decisive for improvement in trauma treatment.
Gestalt Therapy
The second-most researched humanistic therapy is Gestalt Therapy. The results of the systematic review conducted by Cohen (2003) postulated it as an effective approach for working with patients affected by PTSD. According to this author, PTSD is, at the theoretical level, defined by the term ‘unfinished business’, which explains the appearance of symptoms as an attempt to assimilate an event that exceeds the organism’s processing capacities and threatens its survival. As a result, the ‘experience cycle’ of a healthy organism is left unfinished. At the strategic level, GT is based on the therapeutic alliance, the I-Thou dialogue, and phenomenology as fundamental therapeutic elements. The I-Thou dialogue includes presence, engagement, and confirmation between therapist and patient, while the phenomenological approach focuses on examining the traumatic experience moment by moment, allowing for its correct assimilation. Finally, at the tactical level, the technique par excellence of the Gestalt approach is the ‘empty chair’ described above. Other techniques such as narration and awareness in the here and now, or attention to body movements are also useful for the resolution of trauma (Cohen, 2003).
Dialogical Exposure Therapy (DET), derived from GT, has been applied to adult patients diagnosed with PTSD (16% dropout rate), and significant symptom improvements between pre- and post-treatment assessments were found (Butollo et al., 2014). The dialogical exposure has also been used with a group of women who had lost their husbands in the war in Bosnia and Herzegovina (5.8% dropout rate), finding significant improvements in overall trauma symptoms, with changes being more pronounced in avoidance when compared to the control group (Hagl et al., 2015). When comparing this therapy model with CPT, no differences were found in terms of efficacy in PTSD symptom reduction, dropout rates (DET = 12.2%; CPT = 14.9%, Butollo et al., 2016), and maintenance of improvements 2 years after therapy (König et al., 2018). Nevertheless, certain advantages were observed for CPT in reducing post-traumatic cognitions, and for dialogical exposure in reducing interpersonal problems (König et al., 2018). In a later study (König et al., 2020), it was concluded that patients in the DET group found in-session exercises and emotion work helpful, whereas patients in the CPT group perceived cognitive work, psychoeducation, and the structured approach as especially helpful.
By emphasizing the ‘here and now’ and the processing of blocked emotions, GT allows the patient to re-integrate fragmented experiences. Its integration into DET illustrates its flexibility and allows for a comparison with standardized models. The variability in dropout rates and the limited control of external variables constrain the validity of the studies included in this review.
Person-Centered Therapy
According to the case study by Murphy et al. (2019) previously discussed, PCT and EFT share the focus on the therapeutic alliance, the facilitation of the narration of the traumatic event, the identification of the elements of the traumatic event that are currently generating problems and discomfort, as well as the therapist’s attitude of empathy and encouragement of self-support. In recent years, although CBT remains the most commonly accepted approach for trauma-related therapy, the use of PCT is growing in countries such as the United Kingdom, as there is a need to tailor treatment to the particularities of each patient (Murphy et al., 2012). When compared with CBT and PET, all three therapy models successfully improved post-traumatic stress symptoms in patients who had suffered interpersonal violence and, in addition, achieved a dropout rate that was significantly lower for the PCT group (41.75%) when compared to CBT (56.82%) and PET (49.64%, Ghafoori et al., 2019). These results were associated with the non-directive therapeutic style and the focus on the therapeutic alliance characteristic of PCT.
However, for more specific populations, such as adolescents with PTSD following sexual assault, they seemed to perceive a greater alliance with therapists who apply PET than with those who apply PCT (Capaldi et al., 2016). Nevertheless, both therapies significantly reduced PTSD symptoms (Capaldi et al., 2016; Zandberg et al., 2016). Performing a deeper analysis of the different effects of these two therapies for this population, research has found that there were no differences in the reduction of internalizing problems (as measured with scales of anxiety, depression, withdrawal, and somatic complaints), but there was greater reduction in externalizing symptoms (aggressive and defiant behavior) when receiving PET (Zandberg et al., 2016).
PCT offers a non-directive and safe space that is particularly valuable for patients with histories of victimization and relational mistrust. Its strength lies in enhancing adherence and building a therapeutic alliance, making it highly applicable in clinical practice. However, the variability in implementation and evaluation criteria makes it difficult to identify active mechanisms of change and draw solid comparisons with more structured approaches for now.
Existential Therapy and Focusing-Oriented Therapy
No empirical studies have been found concerning ET and FOT, although two review articles explored their contributions to working with patients with trauma issues (Fisher, 2015; Rappaport, 2010). According to Fisher’s review (2015), ET is especially useful for patients who suffered sexual abuse in childhood, as it allows them to build a relationship of authenticity and trust with their therapist and exposes them to interactions they are not used to in their daily lives, as the rest of their relationships with their environment were formed based on fear and mistrust. In addition, the therapist helps the patient unlearn the survival strategies that were once integrated to cope with the abuse, and that now hinder their personal development and limit their capacity for self-support.
As regards FOT, its fusion with art therapy has been investigated as an effective clinical approach to work with trauma (Rappapport, 2010). By supporting the patient’s narrative through the creation of images, empathy and understanding are promoted beyond the therapist’s active listening, as both can visualize the same elements. In addition, it facilitates the separation of the traumatic event or aggressor from the person. This approach also promotes a climate of trust and generates an environment that facilitates the patient’s catharsis, as it enables them to detect and give voice to the wounded parts of themselves. Furthermore, through visual art, the patient can develop their creative intelligence and document their process of change.
Although the principles of ET appear clinically useful, the lack of standardized protocols and controlled studies prevents a solid assessment of its effectiveness in trauma for now. FOT might be an original path to facilitate emotional expression and self-knowledge in patients with trauma-related issues that may enable the externalization of the traumatic experience and support the integration of wounded inner parts. However, the available research is still preliminary and mostly descriptive.
Other Humanistic Therapies
Finally, two other humanistic therapies were identified from the search process whose contributions were of interest to the research question. These are Testimonial Therapy (Lakshmin et al., 2018) and Present-Centered Therapy (Kowalski et al., 2023). Testimonial Therapy descends from a method developed in Chile in the mid-1970s to gather information in legal proceedings (Lakshmin et al., 2018). Since then, it has been used to help populations that might not fit the traditional Western models of psychotherapy, such as immigrants or refugees. It consists mainly of facilitating the narration of a traumatic event, as well as the implications of that event for the person, after which certain ‘rituals’ adapted to their beliefs and culture are performed, such as singing, dancing, or prayers. In one study (Lakshmin et al., 2018), patients (n = 3) remained clinically stable throughout the therapeutic process, and reported that therapy had enabled them to give meaning to past suffering, reduce feelings of shame and guilt, and increase community reconnection.
Regarding Present-Centered Therapy, it emphasizes generating a safe and functional relationship between the patient and the therapist, who uses empathic responses to construct meaning from the patient’s experiences, without exposing the patient to any trauma-related stimuli (Kowalski et al., 2023). A comparison of this approach with CBT and EMDR revealed that Present-Centered Therapy was effective in the treatment of PTSD, but CBT and EMDR showed significantly greater efficacy. According to the results of this review, which could be explained because the specific technique that shows the best results for the reduction of PTSD symptoms is exposure to trauma-related memories and stimuli, a technique that Present-Centered Therapy dispenses with. Finally, one study conducted with patients who had suffered child abuse revealed that the therapeutic process, when working from a humanistic framework, is gradual, dynamic, and personal, and that patients progress in an ascending circular manner (Manríquez-Reyes, 2023). In other words, they return to the same conflicts, but each time from a different perspective and with a ‘healthier’ outlook.
Testimonial Therapy might be beneficial for the resignification of suffering, but the strong dependence on cultural and contextual factors and the unavailability of methodologically sound studies limit the generalization to other populations and the strength of the results. Present-Centered Therapy offers a non-directive approach focused on the therapeutic alliance without resorting to exposure, which may be clinically relevant for patients who do not tolerate more confrontational interventions. However, the absence of specific techniques may limit its effectiveness compared to more structured interventions.
Discussion
The aim of this systematic review was to identify the ways in which the humanistic approach has contributed to the treatment of PTSD and symptoms associated with traumatic experiences, as a way to provide scientific evidence of its efficacy in this context. According to the results of this study, at least the main humanistic psychotherapies have proven to be useful for the treatment of PTSD and trauma-related symptoms thanks to their non-directive therapeutic style, their focus on the patient’s subjective experience, and on the therapeutic relationship as a tool for change.
In most of the empirical studies reviewed in which the reduction of PTSD symptoms after the application of humanistic psychological therapy is evaluated, this reduction was clinically significant (e.g., Anderson et al., 2010; Butollo et al., 2014; Hagl et al., 2015; Holowaty & Paivio, 2012; Paivio et al., 2010). Furthermore, the results revealed that their efficacy may be comparable to that of cognitive-behavioral treatments proposed by NICE (2018) as a first choice for treating PTSD. In the studies that compared therapies from the two models, the reduction in PTSD symptoms was significant in both groups, and no major differences in treatment efficacy were found (Butollo et al., 2016; Capaldi et al., 2016; Ghafoori et al., 2019; König et al., 2018, 2020; Zandberg et al., 2016). Patients related positively to different treatments and perceived useful elements in both therapeutic approaches (König et al., 2020). Nevertheless, some advantages of cognitive processing therapy over dialogical exposure therapy were detected in reducing traumatic cognitions (König et al., 2018), as well as a markedly greater reduction of externalizing symptoms with PET versus CPT (Zandberg et al., 2016). In contrast, advantages of dialogical exposure therapy compared with cognitive processing therapy were observed for the reduction of interpersonal problems (König et al., 2018), as well as a lower dropout rate in the CPT versus CBT and PET groups (Ghafoori et al., 2019).
While the dropout rate of papers reviewed here has ranged between 5.8% and 20% when humanistic psychotherapies are used for the treatment of PTSD or associated symptoms, a notable anomaly exists in one study, which reported a rate of 41.75% (Ghafoori et al., 2019). This impacts the range by 21.75%. The dropout rate for CBT, however, exceeded that number and reached 54.82% in the same study. This high rate of therapy dropout might be related to what has been referred to in the scientific literature as the difficulties of CBT in generating a strong therapeutic alliance (Yasinski et al., 2018). According to previous research, the dropout rate of CBT ranges from 19.9% to 28.6%, figures that are above those found when applying humanistic psychotherapy. Moreover, due to the characteristics of patients with PTSD or symptoms associated with traumatic events, the need for a bond of trust and security with the therapist in order to adhere to treatment is even greater (Nieto Martínez & López Casares, 2016). Therefore, and in light of the results of this review, humanistic psychotherapies could represent an alternative that might lead to a decrease in dropout rates, as one of the fundamental pillars of the humanistic model is the therapist-patient relationship (Cain et al., 2016). However, in one of the studies reviewed, it was observed that if the patient profile is adolescent women who have been victims of sexual assault, a greater alliance could be perceived with therapists using PET than with those employing PCT (Capaldi et al., 2016). Given these contradictory results, it is necessary to investigate whether humanistic psychotherapies are effective in generating a strong therapeutic alliance with all types of populations or, considering the scarcity of available evidence for PCT in this context, if any of these therapies are superior to others in generating a strong therapeutic relationship.
In sum, the results of this study suggest that, although humanistic therapies are often perceived as having less empirical support – potentially leading to the assumption that they are unsuitable for certain psychological problems – existing research, though comparatively limited relative to approaches that have received more attention in the academic context such as CBT, nonetheless provides additional evidence of their benefits. As Hoffman and Lac (2025) recently highlighted, existential-humanistic therapy has a solid empirical foundation, meets the standards of evidence-based practice in psychology and can be at least as effective as other therapeutic approaches.
For the purpose of compilation, the following common aspects may summarize the specific contributions of humanistic therapies to the treatment of PTSD or trauma-related symptoms.
Therapeutic Alliance
Generating a therapeutic bond that serves as a tool for change is one of the main characteristics of humanistic psychotherapies, which is vital to create a safe and trusting environment for patients with a history of trauma. This, together with the therapist’s attitude of listening, empathy, and openness, facilitates the narration of the traumatic event and its implications in the person’s current situation. In addition, creating and experiencing this relationship with the therapist serves as training for the creation of new relationships in their environment which are based on trust, in contrast to the ones created since the traumatic event, which are commonly based on fear.
Empathetic Dialogue
As in all other psychological therapies, dialogue is the therapist’s basic technique to get to know the patient, guide them towards change, and make them feel understood. This is essential in treating trauma issues since this helps them feel that they matter and that the therapist is able to see and understand them. In addition to facilitating the patient’s openness, the therapist’s own empathic responses function as a channel of emotional regulation, as they provide the patient with a model for identifying sensations that they are unable to name on many occasions.
Experiential Focus
This is perhaps the point at which humanistic psychotherapies differ the most from other psychological models. Their focus on the patient’s experience in the present moment involves dedicating a large part of the therapy to encouraging the patient to identify and legitimize their emotions, to give permission to experience and express them, so they become aware of how the trauma affects them here and now in order to be able to transcend that pain. The space of the sessions is a living space, where the therapeutic process let the patient transform their emotions and beliefs to become more adaptive.
Use of Exposure
This is the psychological technique with the most scientific support in terms of efficacy, and which could be a common ground between humanistic therapies and CBT. Specifically for patients with PTSD, exposure to trauma-related stimuli is very useful for emotional reprocessing and the subsequent development of new meanings. This is mainly obtained by exposure in imagination, using the patient’s own narration or the therapist’s presentation of possible scenarios, where they assist the patient in identifying and living through their emotions. Little by little, emotions such as fear, shame, or guilt are transformed into basic adaptive emotions such as sadness and anger, which need to be experienced and expressed in order to close the wound and move forward. It should be noted that, although the use of exposure is shared with various psychological models, humanistic psychotherapies focus much more on the patient’s emotional process, intertwine this exposure with the experiential approach, apply the technique in a non-directive and flexible way, and respect the time needed by the patient at all times.
Although these four points are transversely present in the different humanistic therapies reviewed, the use of exposure has been found more explicitly in EFT and GT. In both therapies, the empty chair technique is used, also called dialogical exposure therapy. The gestalt empty chair technique combines exposure in imagination with an experiential approach, allowing the patient to establish a symbolic dialogue with external (e.g. the person who perpetrated the aggression) or internal (e.g. one’s own repressed anger, or the child who felt guilty despite being the victim of the abuse) elements related to the trauma, in order to access and experience associated emotions in the present (Butollo et al., 2014, 2016; Cohen, 2003; Hahl et al., 2015; Holowaty & Paivio, 2012; König et al., 2018, 2020; Lee et al., 2022; Mlotek & Paivio, 2017; Paivio et al., 2010).
These contributions of humanistic therapies should be reflected in the day-to-day clinical practice. First, understanding the importance of the therapeutic alliance, clinicians intervening in trauma contexts may wish to pay sustained attention to and continually assess the therapeutic relationship during the entire therapeutic process, ensuring that it is established and maintained in an adequate manner and grows over time. It would also be useful to employ empathetic dialogue and to communicate verbally and nonverbally with patients in a way that shows them that they matter, that they are truly understood, and not being judged. This type of interaction with the therapist could also make it easier for patients to identify, express, and integrate their emotions related to the trauma. Their growing ability to regulate emotions would, in turn, enable them to face exposure to traumatic content. It is particularly relevant to allow gradual exposure to trauma-related content. Professionals must, however, respect the patient’s pace and attend to their needs. Lastly, raising the patient’s awareness of the ‘here and now’ of thoughts, emotions, and bodily sensations would not only help patients stay connected, but also serve therapists as a source of information, helping them assess patients’ ongoing processing and integration of trauma.
Limitations and Future Research
As for the limitations of this study, firstly, 10 articles that met the inclusion criteria in the first screening could not be retrieved for full reading, so valuable data for this review may have been omitted. One possible explanation might be that these were older papers (published between 1985 and 2009), and so the means for retrieval are limited. Secondly, several of the empirical studies had a rather small sample size, limiting the generalizability of their results. Thirdly, in all the articles reviewed, the traumatic events are interpersonal in nature, but no evidence was found that humanistic therapies are effective in intervening with people who have been the victims of natural disasters or serious traffic accidents, for example. More research into the efficacy and usefulness of humanistic psychotherapies in treating PTSD is required, which takes into account the type of trauma experienced. Finally, a noteworthy fact regarding the patient profile of the empirical studies reviewed is that the percentage of women significantly exceeds that of men, representing the total sample in many cases. This would suggest there is a need to carry out research with a gender perspective in this field in order to take into account the maximum number of characteristics and particularities of the patients, and to better adjust the treatments.
For future research, as mentioned above, more studies are needed on the efficacy of humanistic psychotherapies for people with a history of trauma, factoring in specific variables such as gender, age, or type of trauma. Furthermore, future studies should analyze other variables outside the therapy modality that may influence the establishment of the therapeutic relationship, such as the characteristics of the therapist and the patient, the type of problem, or the context (Bárez Palomo, 2020). In addition, further research could be aimed at identifying the specific mechanisms beyond the therapeutic alliance that contribute to a lower dropout rate in humanistic psychotherapies. The present systematic review may contribute to the future development of a specific intervention proposal for PTSD from a humanistic therapeutic approach, which would integrate the useful aspects of each therapy in a single protocol and would allow for empirical assessment of its efficacy with different populations. This could lead to greater scientific support for this psychological model, and more widespread implementation in the practice of clinical psychology and psychotherapy.
Conclusion
Humanistic psychotherapy may contribute positively to the treatment of psychological trauma, probably thanks to the specific characteristics of this model. CBT and EMDR continue to be the psychological therapies with the strongest empirical support for treating individuals with PTSD; however, the available research examining humanistic therapies indicates promising outcomes, emphasizing that a lack of extensive evidence does not imply ineffectiveness. Moreover, a growing number of professionals acknowledge the effectiveness of humanistic psychotherapies for people with a history of trauma and are increasingly adopting this approach to better accommodate the unique needs of each patient. A humanistic framework, which emphasizes flexibility, respect for the patient’s rhythms and needs, and the creation of a safe and supportive therapeutic environment, may enhance treatment adherence, addressing the high dropout rates often observed in cognitive-behavioral approaches and potentially benefiting a larger population. Key contributions of humanistic psychotherapies for the psychological treatment of trauma-related issues as highlighted by this review include: (a) the therapeutic relationship as a vehicle for change; (b) the use of empathic dialogue; (c) an experiential focus that enables patients to identify, experience and express their emotions within the session; and (d) the application of imaginal or symbolic exposure to traumatic stimuli. Future research should aim to develop specific humanistic interventions for PTSD and empirically evaluate their efficacy. Such work would not only strengthen the evidence base for humanistic therapies but also expand their role within the scientific community and general clinical practice.
Supplemental Material
sj-docx-1-jhp-10.1177_00221678261462960 – Supplemental material for Contributions of Humanistic Psychotherapy to the Treatment of Post-Traumatic Stress Disorder or Trauma-Associated Symptoms: A Systematic Review
Supplemental material, sj-docx-1-jhp-10.1177_00221678261462960 for Contributions of Humanistic Psychotherapy to the Treatment of Post-Traumatic Stress Disorder or Trauma-Associated Symptoms: A Systematic Review by Clara Vélez and Rosario Castillo-Mayén in Journal of Humanistic Psychology
Footnotes
Acknowledgements
The authors would like to thank Joachim Peter Hubner for proofreading this article. His efforts are very much appreciated.
Ethical Considerations
The nature of the manuscript does not require ethical approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.