
Abstract
Considerable attention and legislation are currently focused on developmental dyslexia. A major challenge to these efforts is how to define and operationalize dyslexia. In this article, we argue that rather than defining dyslexia on the basis of an underlying condition, dyslexia is best viewed as a label for an unexpected reading disability. This view fits well with a preventive approach in which risk for reading disability is identified and addressed prior to children experiencing reading failure. A risk–resilience model is introduced that proposes that dyslexia is due to the cumulative effects of risk and resilience factors. Evidence for the multifactorial causal basis of dyslexia is reviewed and potential factors that may offset this risk are considered. The implications of a cumulative risk and resilience model for early identification and intervention is discussed.
Developmental dyslexia is now recognized worldwide as a specific learning disability (Mather et al., 2020). In the United States, grass roots organizations of parents and educators have advocated for state legislation to better address dyslexia (Youman & Mather, 2018). These efforts have resulted in most states passing laws requiring that intervention services be provided to children with this condition, especially in the early school grades. Many states also have legislation that calls for mandatory screening to identify students with dyslexia. A major challenge that states face in implementing this legislation is how to best define and operationalize dyslexia (Miciak & Fletcher, 2020). In this article, we argued that rather than defining dyslexia on the basis of an underlying cause, it is better viewed as a label for an unexpected reading disability. Such a view is consistent with a preventive approach in which risk for reading disability is identified and intervention is provided prior to children experiencing reading failure. To expand on this approach, we introduce a risk–resilience framework that can assist in operationalizing risk for dyslexia and potentially lead to more timely and effective intervention.
Defining Dyslexia
Despite the extensive scientific evidence concerning dyslexia, there is still disagreement of how best to define it (Elliott, 2020; Elliott & Grigorenko, 2014; Protopapas, 2019; Snowling et al., 2020). Most researchers, clinicians, and educators agree that a primary characteristic of dyslexia is a severe and persistent difficulty learning to read (and spell) words despite adequate opportunity and instruction. There is also agreement that children must have adequate vision and hearing acuity, whereas the adequacy of verbal and/or nonverbal intellectual abilities is still under debate. In regard to the latter, research indicates that measures of IQ should not be part of the definition of dyslexia (Francis et al., 2005; Stuebing et al., 2002) but some continue to argue for the use of IQ-achievement discrepancy definitions (e.g., Hammill & Allen, 2020). Also, some have suggested that dyslexia be defined on the basis of a discrepancy between listening and reading comprehension, which could exclude children with low verbal abilities like those with a developmental language disorder (DLD; Wagner et al., 2019).
Another issue in dispute is what role an underlying cognitive deficit should play in defining dyslexia. Historically, such a deficit has been a central component in definitions of dyslexia (Critchley, 1970). According to this view, individuals with dyslexia have a neurologically based disorder that limits their ability to respond to typical reading instruction. Diagnosis of this condition often involves the use of neuropsychological assessments to identify areas of cognitive strengths and weaknesses. Some even believe that assessments can reveal special gifts that many individuals with dyslexia are proposed to have (Davis, 1997; Eide & Eide, 2011). A major problem with defining dyslexia on the basis of an underlying condition is that there is considerable variability in the causal basis of reading difficulties (O’Brien & Yeatman, 2021; Pennington et al., 2012; Snowling, 2008). Research shows that multiple neurological, behavioral, and environmental factors are associated with dyslexia and that these factors may act and interact in complex ways to influence the trajectory of reading development (van Bergen et al., 2014). As a result, there is no single deficit or small group of deficits that are consistently associated with dyslexia that could be used for diagnostic purposes.
Because of these issues, some argue that the term dyslexia is better thought of as a synonym for a reading disability (de Yong, 2017; Elliott, 2020; Protopapas, 2019). According to this view, dyslexia is not considered a discrete condition that underlies a reading disability but rather the name or label for the disability. Furthermore, this disability is unexpected on the basis of adequate opportunity and instruction in reading as well as adequate hearing and visual acuity. Significant intellectual disabilities are also ruled out. This type of definition has been operationalized in the vast majority of studies that have investigated dyslexia. In most studies, individuals with dyslexia have been identified on the basis of poor word reading performance, measured in terms of accuracy and/or fluency, that falls below some expected normative cut-score (e.g., Pennington et al., 2012; Snowling et al., 2019). Such a definition has the advantage of not specifying a distinct causal basis but allows for multiple factors to be involved. It also accommodates the fact that reading ability is on a continuum and dyslexia represents the lower end of that continuum. As such, dyslexia is not discrete in its presentation, but rather part of normal individual variability in reading development.
The latter view of dyslexia also has the advantage of being more easily operationalized in most contexts. In fact, this definition is especially well suited for educational settings and could work well under new state legislation. Most schools have personnel with training in reading development and experience with assessing and evaluating reading performance. Defining dyslexic on the basis of difficulties learning to read provides educators with a clear target for diagnosis and intervention. Of course, decisions still need to be made concerning the severity and persistence of these difficulties along with an evaluation of hearing, vision, and other exclusionary criteria (e.g., severe intellectual disability). But focusing on children’s reading development would take some of the mystery away from dyslexia and offer clearer directions for educational practice.
Defining dyslexia on the basis of reading failure also fits well within a preventive model. Such a model seeks to identify risk factors associated with reading failure as early as possible to provide timely intervention (Catts & Hogan, 2021). There is now a large body of evidence concerning potential risk factors that could guide early identification (Catts et al., 2015; H. Lyytinen et al., 2015; Peterson & Pennington, 2015). Research also demonstrates that early intervention based on the identification of risk can be effective in improving the outcomes of at-risk children (Lovett et al., 2017; Wanzek & Vaughn, 2007). Such an approach to defining dyslexia and identifying risk has the added advantage of using what is known about the causal basis of dyslexia without requiring that it be central to the diagnosis of the condition. That is, causal factors could be considered in risk assessment without any one factor being necessary for diagnosis. Finally, defining dyslexia as reading failure allows for the use of poor response to reading instruction, both general classroom and supplemental instruction, as a potential risk factor for dyslexia (Miciak & Fletcher, 2020).
In the remainder of this article, we expand on the view that dyslexia is best defined on the basis of a difficulty learning to read. Specifically, we consider reading failure in the context of a risk–resilience model that is based on evidence of the multifactorial causal basis of dyslexia. We further argue that this model has implications for the early identification and intervention of dyslexia and could play an important role in meeting the intent of dyslexia legislation.
Multifactorial Causal Models
In many causal models of dyslexia, it has been common to focus on a single causal factor (Snowling, 1998; Vidyasagar & Pammer, 2010). These models have argued that a specific deficit in sensory, linguistic, or cognitive processing (e.g., phonological processing) is the primary cause of unexpected difficulties learning to read. More recently, however, research clearly indicates that single deficit models do not fully account for the variability found in dyslexia. This work shows that not all individuals with a reading disability have the same underlying deficit and no single underlying deficit consistently leads to problems in learning to read (Catts et al., 2017; O’Brien & Yeatman, 2021; Pennington et al., 2012; Snowling, 2008).
The lack of support for single deficit models has led to the proposal of multiple deficit or multifactorial causal models of dyslexia (Catts et al., 2017; McGrath et al., 2020; O’Brien & Yeatman, 2021; Pennington, 2006; van Bergen et al., 2014). These models propose that multiple factors combine and/or interact to cause a difficulty in learning to read. Such a view is consistent with recent arguments that developmental disorders in general are best explained by a constellation of strengths and weaknesses rather than “core deficits” (Astle & Fletcher-Martin, 2020). This would seem to be especially true for disorders involving reading development. Research shows that the development of accurate and fluent word reading abilities rely on a host of linguistic, cognitive, socioemotional, orthographic, and instructional factors that act and interact in various ways (Cain et al., 2017). As such, difficulties in learning to read are likely due to individual differences and experiences across many of the factors.
A multifactorial model also fits well with what is known about the genetic basis of dyslexia. Multiple genes are associated with dyslexia, but none of the candidate genes account for more than a small proportion of the variance in reading ability/disability (Bishop, 2009; Mascheretti et al., 2017). Rather, it appears that multiple genes, some more generalist genes (Plomin & Kovas, 2005), work together to increase the likelihood of dyslexia. Genes also influence the environment and can have a subsequent effect on reading achievement (Cheesman et al., 2020). In addition, environmental factors influence the expression of genes and their impact (Plomin et al., 2013). Because of the varying genetic and environmental influences, multifactorial causal models are probabilistic rather than deterministic. In other words, multiple risk factors work in conjunction to increase the probability of difficulties in learning to read rather than any one factor or combination determining that an individual will have these difficulties.
Risk–Resilience
Whereas multiple risk factors can increase the likelihood of dyslexia, positive factors can decrease this likelihood. A framework that accounts for the impact of such influences is the risk–resilience framework (Fraser & Galinsky, 2004). This framework has been applied in disciplines such as child maltreatment and psychopathology (Masten & Wright, 1998; Rutter, 1985). In these contexts, it has been observed that individuals with very similar risk factors can have very different outcomes. Some individuals seem to show resilience against even the strongest risk factors, while others do not. These differences in resilience have been explained in terms of promotive or protective factors. Promotive factors are those associated with better outcomes for all individuals regardless of risk, whereas protective factors are moderators and have their greatest influence in the context of heightened risk, but have limited influence by themselves (Masten & Barnes, 2018). An example from nutrition sciences may be helpful here. A well-balanced diet is a promotive factor for good health in all individuals, whereas for those with Phenylketonuria (PKU), a metabolic disorder, a diet low in protein and other foods is a protective factor for good health. Within a statistical framework, promotive factors may be viewed as main effects and protective factors as moderators. Although the distinction between promotive and protective factors is often made, one factor may be both promotive and protective depending on the sample. For example, effective parenting may simultaneously promote positive outcomes across all individuals, while also having the greatest protective influence for those most at risk (Masten & Barnes, 2018).
Figure 1 is a graphic representation of a proposed risk–resilience model as it relates to dyslexia. We refer to this model as the Cumulative Risk and Resilience Model of Dyslexia. A similar model has been used in the field of child maltreatment to account for factors that contribute to child abuse (Masten & Wright, 1998). Some components of a risk–resilience model have also recently been considered in relationship to dyslexia (Haft et al., 2016; Yu et al., 2018). In our model, we display risk and resilience factors in terms of a seesaw. On the left side are risk factors that increase the probability of an individual having an unexpected and severe difficulty in learning to read. On the right side, we list examples of resilience factors that can buffer the effect of risk. In both cases, we include influences that can be divided into those that are internal and external to the individual. Taken together, these various risk and resilience factors are proposed to work jointly in a complex and nonlinear fashion to influence children’s trajectories for reading development.
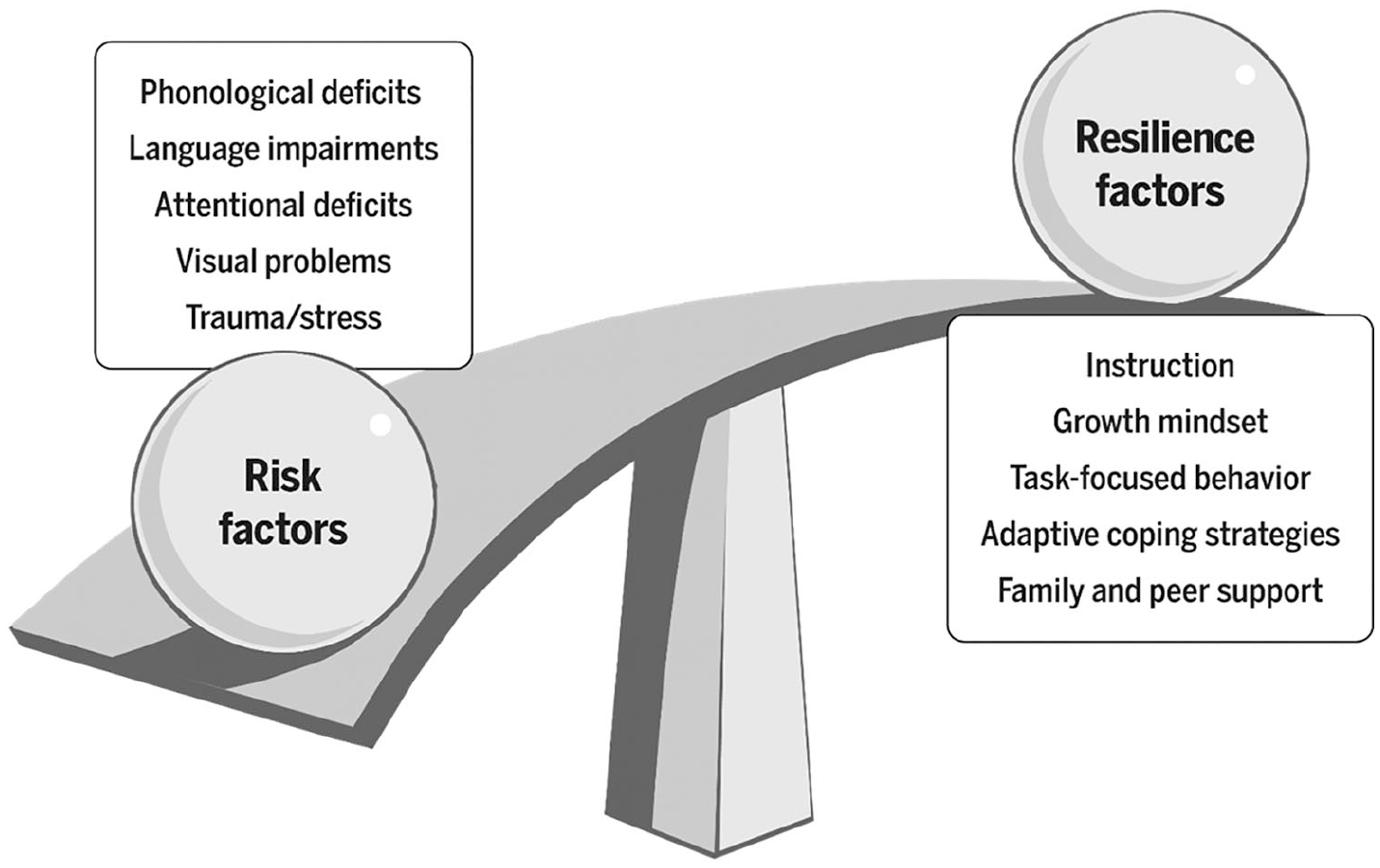
Cumulative risk and resilience model of dyslexia.
Risk Factors
In our model, risk factors are variables that increase the likelihood of severe and persistent difficulties learning to read. Depending on the variable, they can have different degrees of negative impact on reading. It should also be recognized that the positive end of these variables could well serve as promotive factors. Primary among the risk factors associated with dyslexia are deficits in phonological processing. Deficits in storing, retrieving, and/or reflecting on the sounds of language are often reported in individuals with dyslexia. See Melby-Lervåg et al. (2012) and Peterson and Pennington (2015) for full consideration of this work. Whereas evidence is strong for a phonological processing deficit as a causal factor in dyslexia, it does not appear to be a necessary or sufficient cause of a reading disability. For example, Pennington et al. (2012) found that only about half of each of two samples of kindergarten children who later developed dyslexia had a severe deficit in phonological awareness (PA). Somewhat similar results have been reported in other case-based studies of children with dyslexia (Carroll et al., 2016; O’Brien & Yeatman, 2021; White et al., 2006 but see Ramus et al., 2003). Examining the relationship from the opposite perspective, Catts et al. (2017) found that only about half of the children with a severe deficit in PA at the beginning of kindergarten had dyslexia at the end of second grade. This work does not negate the role of phonological deficits in dyslexia, but rather suggests that other factors operate in combination, or sometimes in lieu of these deficits, to lead to severe and persistent deficits in reading development.
There are a number of other potential candidates for risk factors associated with dyslexia. One is slowed performance on measures of rapid automatized naming (RAN). Research has shown a relationship between RAN and reading achievement across numerous orthographies and reading tasks (Araújo et al., 2015). RAN is partly a measure of phonological retrieval but also likely shares many features with the process of reading, including saccadic eye movement, lexical access, cognitive vigilance, and automaticity. As such, poor performance in RAN can be a multifaced indicator of risk for dyslexia (Norton & Wolf, 2012). Furthermore, it has been proposed that children with deficits in PA and RAN or what is called a “double deficit” are more likely to have a reading disability than those with a single deficit (Wolf & Bowers, 1999). However, given the mild-to-moderate correlation between PA and RAN, when both deficits are present, each tends to be more severe in nature than when only one deficit is present (Compton et al., 2001; Schatschneider et al., 2002). Thus, at least part of the double deficit effect may be related to the severity of either deficit rather than the presence of both. Nevertheless, evidence linking slowed rapid naming to a reading disability is strong and of clinical/educational significance.
Another risk factor for dyslexia is a deficit in other aspects of oral language. Numerous studies have shown that deficits in vocabulary, grammar, and discourse are often present in children with dyslexia (Catts et al., 1999; P. Lyytinen et al., 2001; Scarborough, 1990; Snowling, 2008) and that dyslexia is frequently comorbid with a developmental language disorder (DLD; Catts et al., 2005). Also, early identification studies have shown that oral language abilities predict reading success or failure over and above PA, RAN, and other variables (Catts et al., 2001; Thompson et al., 2015). Furthermore, in studies examining children at family risk for dyslexia, preschool oral language problems appear to be among the earliest precursors of later reading difficulties and at school age differentiate those who have dyslexia from those who do not (P. Lyytinen et al., 2001; Scarborough, 1990; Snowling & Melby-Lervåg, 2016).
Like reading, oral language is dimensional in nature and both mild and severe language difficulties can co-occur with a reading disability. When language problems are severe, children may be diagnosed with DLD (Bishop et al., 2016). However, in our model they would still be considered to also have dyslexia if they had a severe and persistent word reading disability. But it is important to note that not all children with DLD have significant difficulties learning to read words. Whereas oral language problems are a risk factor for dyslexia, they alone do not always lead to severe word reading problems (Catts et al., 2005; Snowling et al., 2019).
Non-Linguistic Risk Factors
Another risk factor that has been linked to dyslexia is a deficit in visual processing. Behavioral and neurophysiological evidence has documented an association between dyslexia and problems in visual temporal processing (O’Brien & Yeatman, 2021; Stein, 2001), visual attention (Bosse et al., 2007; Facoetti et al., 2010), and visual crowding (Joo et al., 2018). Whereas there is a converging body of evidence indicating a link between visual processing problems and dyslexia, it remains unclear as to the extent and nature of their causal role (Olulade et al., 2013). Much of this research has examined specific aspects of visual processing in isolation, independent of other risk factors. However, studies have begun to investigate deficits in visual processing in the context of other risk factors. This research indicates that visual processing may make a unique contribution to reading development when considered alongside other risk factors (Facoetti et al., 2010; O’Brien & Yeatman, 2021; van den Boer et al., 2015). For example, van gen Boer and colleagues found that visual attention explained variance in reading and spelling abilities beyond that of phonological awareness, phonological memory, and rapid naming. While these results imply that visual attention deficits could be an additive risk factor for dyslexia, the authors also suggest that non-visual factors (i.e., quality of connection between orthographical and phonological units) may underlie these findings. To better understand the role of visual deficits in dyslexia, large-scale longitudinal studies should examine the co-development of multiple aspects of visual and other risk factors and their relationship to reading.
Deficits in executive function or more specifically attention have also been linked with dyslexia (McGrath et al., 2011; Willcutt & Pennington, 2000). The relationship between these conditions, however, is highly complex and far from being well understood. Research shows that the overlap between dyslexia and attention deficits (25%–40%) is higher than would be expected by chance (Willcutt & Pennington, 2000). Such comorbidity could be taken to indicate that attention deficits are a risk factor for dyslexia. Indeed, Torgesen et al. (1999) reported that attention was a unique predictor of response to intervention in children with dyslexia. An alternative line of research indicates that the comorbidity of attention deficits and dyslexia may be due to shared problems in processing speed (McGrath et al., 2011). If this is the case, then attention deficits may not be a risk for dyslexia but a separate condition that shares a common underlying risk factor.
Exogenous Risk Factors
The above factors are all endogenous or internal to the individual. External or exogenous variables may also play a role in dyslexia. Whereas such variables are not generally considered to be part of dyslexia, and are often used as exclusionary criteria, we choose to include them in our model. We do this because these factors can co-occur with endogenous risk factors and increase the probability of a reading disability. Variables that function in this way have sometimes been referred to as vulnerability factors. These factors are analogous to protective factors in that they are moderators and have their primary impact in the presence of other risk factors (Masten & Wright, 1998). For example, low socioeconomic status (SES) or poverty likely increases the risk for a reading disability when other risk factors are present. Of course, SES is a corollary of a host of associated risk factors, including limited literacy and language experience, poor nutrition, low maternal education, and homelessness. Another risk factor that is related to poverty but can also occur in higher SES families is trauma. Research shows that children who have experienced trauma and other adverse childhood experiences often have difficulties in school performance including problems in learning to read (Blodgett & Lanigan, 2018; Delaney-Black et al., 2002). Given that approximately 60% of adults report having at least one adverse childhood experience (Merrick et al., 2018), it is likely that it is the cumulative effects of multiple experiences and/or the co-occurrence of other factors that place children at the highest risk of severe reading problems. Furthermore, minority (i.e., Black, Hispanic, & multiracial children) experience adverse childhood events at disproportionally higher rates than non-minority children (Merrick et al., 2018) and minority children have higher poverty rates. Consequently, the intersection among these factors produces increased risk for poor academic achievement and behavioral outcomes (Skiba et al., 2008). Finally, whereas adverse childhood experiences may be classified as exogenous factors, these experiences can have neurological consequences, and in this sense, become endogenous (De Bellis & Zisk, 2014).
Before moving on, it is important to acknowledge the role of family history in our model. It is well documented that dyslexia runs in families and has a genetic basis (Bishop, 2009). Other multiple deficit models explicitly address family risk in dyslexia. Specifically, van Bergen et al. (2014) nicely demonstrate how family risk contributes to and supports an intergenerational multiple deficit model of dyslexia. While we do not explicitly include family history in Figure 1, we acknowledge that genetic influences underlie and are responsible for many of the risk and resilience factors in our model. There is also some evidence that family risk may account for variance in word reading ability that is independent from that of the commonly recognized predictors (e.g., PA, RAN, oral language) in our model (Carroll et al., 2014; Puolakanaho et al., 2007; van Viersen et al., 2018). Of course, such a finding is consistent with a multifactorial causal model of dyslexia.
Resilience
Some children appear to avoid reading problems despite having one or more risk factors (Catts et al., 2017; Pennington et al., 2012; van Bergen et al., 2014). In our model, we propose that resilience against poor reading outcomes is the result of protective or promotive factors. Recall, protective factors are moderators and only have an impact in the context of risk. Promotive factors, on the other hand, operate like main effects and can have a positive influence for both those at risk and not at risk. We believe the distinction between promotive and protective factors is important and highlight it when evidence is available. But research is just beginning to examine the role of resilience factors in dyslexia and to determine which factors are better described as promotive or protective in nature. With the appropriate data and statistical analyses, we should be able to more clearly delineate how these factors operate in dyslexia.
Instruction
The most notable factor that can have a positive impact on risk for dyslexia is instruction. Explicit instruction on how to decode and read printed words is critical for promoting word reading abilities in all children not just those at risk for dyslexia (Ehri et al., 2001; Fletcher et al., 2019). By definition, the delivery of appropriate reading instruction is a necessary condition to identify children with dyslexia. Without good instruction, it is not surprising to find large numbers of children who are slow to learn to read words. But when high-quality instruction is provided, we will inevitably find some children who continue to experience difficulties, and when these difficulties are severe and persistent enough, these children may be diagnosed with dyslexia.
While appropriate instruction is a promotive factor for all children, and a defining inclusionary criterion for dyslexia, it may also serve as an important protective factor for at-risk children. Indeed, there is some initial indication that at-risk children may benefit the most from high-quality instruction. For example, Foorman et al. (2003) found that a prescriptive kindergarten curriculum that included phonological awareness instruction differentially raised the letter-naming and phonological awareness skills of the lowest performing students as compared with higher performing students. In addition, Connor et al. (2004) reported that teacher-managed explicit code focused instruction had a significant impact on first graders’ reading skills, and this impact was greater for poor readers than for good readers. Numerous other studies have also documented the special role of good instruction in offsetting the negative outcomes associated with dyslexia (Scammacca et al., 2007; Wanzek & Vaughn, 2007). If instruction does operate as a protective factor, it may have its greatest impact when used within an early intervention program for at-risk children (Lovett et al., 2017). In our model, the risk factors described above, along with initial poor response to instruction (Miciak & Fletcher, 2020), can be used to identify children early and provide them with supplemental reading intervention.
Cognitive Resilience
Beyond instruction, children’s cognitive abilities can serve a compensatory role in risk for dyslexia. Berninger and Abbott (2013) reported that students with dyslexia but with high verbal reasoning skills had better outcomes than less verbally gifted students. Van Viersen et al. (2014) further found that at-risk children with better verbal short-term memory, working memory, and language skills had better reading scores than less verbally gifted children. In addition, van Viersen et al. (2019) reported that among gifted adolescents with dyslexia, those with more strengths in verbal working memory, vocabulary, and grammar were more likely to resolve their reading problems. These results suggest that verbal skills in general might be considered a promotive factor in dyslexia. As noted earlier, this would be the case of the positive side of a risk factor serving as a compensatory mechanism. That is, while language deficits can increase risk for dyslexia, better language skills may reduce this risk. Indeed, Snowling and Melby-Lervåg (2016), in a meta-analysis, found that among children with a family risk for dyslexia, those with better language skills had better reading outcomes.
Another cognitive factor that has been linked to outcome in dyslexia is children’s mindset toward their intelligence. Individuals with a growth mindset broadly believe that intelligence can be attributed to learning, practice, and effort whereas persons with a fixed mindset hold that intelligence is fixed and cannot be changed (Dweck, 2006). Numerous studies have examined the connection between growth mindset and academic achievement including reading achievement. A recent meta-analysis of this work found that, on average, the connection was rather weak (Sisk et al., 2018). However, this relationship might be stronger for children at risk for dyslexia. In support of such a relationship, Petscher et al. (2017) found that growth mindset was moderately related to word reading ability in a sample of children with low reading ability and/or from schools with a large percentage of children from low-income families.
A growth mindset may provide some benefit to those at risk, but success requires more than belief about intelligence. It requires that children put in the effort to achieve better results. Research has begun to examine how this effort is linked with outcomes in children at risk for dyslexia. Specifically, Eklund et al. (2013) examined what they called task-focused behavior in children with a family history of dyslexia. They defined such behavior as the tendency to remain highly engaged in tasks and/or to be persistent in the face of failure. Investigators found that a high level of task-focused behavior in children with a family history was associated with the absence of reading problems irrespective of the presence of a phonological deficit. Whereas task-focused behavior has just begun to be examined in relationship to dyslexia, others have documented its relationship with reading achievement more generally (Hirvonen et al., 2010; Stephenson et al., 2008). In addition, Petscher et al. (2021) showed in a latent profile analysis that effort, a variable similar to task-focused behavior, combined with growth mindset to predict vocabulary and reading achievement.
Socioemotional Resilience
Difficulties learning to read can lead to anxiety, frustration, anger, poor self-concept, and/or depression (Arnold et al., 2005; Maughan et al., 2003; Morgan et al., 2012). However, some at-risk children meet learning challenges without strong negative emotions and consequences. Goldberg et al. (2003) found that students with dyslexia who had developed adaptive coping skills had fewer negative consequences than those who did not develop these skills. The former students tended to be more proactive, set goals, and react to failure with less frustration. Research also shows self-determinism is related to outcomes in students with learning challenges (Zheng et al., 2014). That is, students who see themselves as the origins of their actions, have high aspirations, and take control of their learning have better academic outcomes than those who do not share these resilience factors. Finally, others have argued that hope mediates the connection between risk and resilience factors. Specifically, Idan and Margalit (2014) found that hopeful thinking leads at-risk students to be more goal oriented and to invest more effort in order to achieve their academic goals. Taken together, this research is supportive of a link between socioemotional factors and reading/academic achievement. However, more work is needed that explicitly examines how these factors interact with known risk factors to increase or decrease risk for dyslexia.
Exogenous Factors
Resilience not only resides within the individual but can also result from the context in which dyslexia occurs. Indeed, as mentioned above, instruction can serve this role. But also, the connections that children have with other people and systems can act as protective/promotive mechanisms and reduce the negative consequences of dyslexia. Much of the support for the compensatory role of the context comes from other fields of study where resilience has been examined from a developmental systems perspective (Masten & Barnes, 2018). Research has just begun to examine exogenous factors related to resilience in dyslexia, and this work has primarily focused on adolescents with learning disabilities including some with dyslexia. This research suggests that a student’s teacher can play an especially important role by providing support and encouragement (Al-Yagon & Mikulincer, 2004). Teachers can also mitigate interactions with peers and increase peer acceptance that can reduce the feelings of loneliness and social isolation associated with dyslexia (Connor et al., 2004). Strong parent–teacher partnerships may also influence literacy development in at-risk children (Dearing et al., 2006). Furthermore, nurturing family members and high family cohesion may serve as protective mechanisms in dyslexia (Al-Yagon, 2010; Idan & Margalit, 2014). Future research can add to our understanding of these effects by examining contextual factors within developmental models that better allow for the examination of causal relationships across the school years.
A contextual factor that has been examined from such a perspective is home literacy environment. Research shows that children who have more books and/or whose parents read more often to them have better early literacy skills than children without these experiences (Frijters et al., 2000; Levy et al., 2006). However, the relationship between informal home literacy and children’s reading achievement does not seem to be a direct one. Rather, research suggests that the link between informal home literacy practice and risk for dyslexia is better accounted for by maternal skills and/or genetic influences (Puglisi et al., 2017; van Bergen et al., 2017). This work shows that mothers with higher literacy skills or a genetic predisposition toward higher language/reading skills read to their children more often and pass on their competences/genes that confer good language/reading. Thus, what appears to be an environmental contextual effect may also involve genetic influences.
Early Identification
Our multifactorial risk–resilience model and suggested approach to defining dyslexia have implications for the early identification of children at risk for dyslexia. First, given that multiple factors are associated with dyslexia, it will be necessary to examine a wide range of variables to accurately evaluate risk for dyslexia. These should include both endogenous and exogenous factors. Second, risk will be better viewed as probabilistic rather than deterministic. That is, no single factor or set of factors can determine that a child will have dyslexia. Rather a combination of multiple risk and resilience factors will increase or decrease the probability of dyslexia. Third, by defining dyslexia as a reading disability, slow response to reading instruction can be viewed as an additive factor in early identification.
In health-related professions, it is common to consider multiple factors to evaluate probability of risk. For example, medical personnel typically use multiple indicators to determine risk of conditions such as cardiovascular disease. In fact, a cardiovascular disease risk calculator has been introduced to assist in this identification. This online calculator uses data concerning nine variables to determine the probability of cardiovascular problems in the next 10 years. It can be completed by a practitioner during an office visit or is available to the public online. See http://www.cvriskcalculator.com/. A comparable procedure could be used to assist in the early identification of dyslexia. A prototype of such a calculator was introduced by Catts et al. (2001). This calculator used five kindergarten variables to estimate the probability of reading difficulties in second grade. In an extension of this work, Petscher et al. (2016) developed an automated, online risk calculator (i.e., the Earlier Assessment for Reading Success; EARS) that uses one or more curriculum-based measurements in K–Grade 3 to predict reading comprehension and language risk. Similar to the approach of Catts et al. (2001), the EARS estimates various probabilities of reading and language success based on available curriculum-based measures in K–Grade 3 (https://flassessments.fcrr.org/EARS/uo/).
Besides the above studies, there are numerous other investigations that have provided rich data relevant to a probabilistic approach to early identification (Carroll et al., 2016; Elbro et al., 1998; Landerl et al., 2013; H. Lyytinen et al., 2015; Ozernov-Palchik et al., 2017). However, most of this work has focused on child-level cognitive variables. Whereas screening tools using these variables can provide estimates of risk for dyslexia, they are characterized by limited accuracy. According to the Tools Chart from the National Center for Intensive Intervention (https://charts.intensiveintervention.org/ascreening), most screening tools have sensitivity and specificity below a desirable level (.80–.90). Whereas the risk calculators mentioned above do have more desirable levels of sensitivity and specificity (>.85), we believe that to improve accuracy further the next generation of screening tools and calculators will need to go beyond these child-level cognitive data and include socioemotional risk and resilience data as well as exogenous factors concerning the context in which children are learning to read. Furthermore, in estimating risk, the interactive, as well as the additive, effects of the various risk and resilience factors should be taken into consideration.
Finally, we agree with others (e.g., Miciak & Fletcher, 2020) that early identification of dyslexia risk is best achieved by also considering children’s response to initial reading instruction. Because dyslexia represents a severe and persistent reading disability, initial difficulties in learning to read in the face of good instruction can be an early indicator of the condition. But for this to be the case, it is critical that children be exposed to high-quality reading instruction upon beginning school. Without such instruction, delayed word reading development may be less indicative of risk. Furthermore, high-quality instruction is critical for identifying risk in economically disadvantaged children. These children typically have fewer books in their homes, have parents who read less often to them, and who provide less rich language environments than do children from higher SES families (Aikens & Barbarin, 2008; Neuman et al., 2018). Because of these differences, economically disadvantaged children may initially perform less well on literacy measures and appear to be at risk. However, research indicates that high-quality instruction can considerably reduce the influence of socioeconomic disadvantage on reading achievement (Blachman et al., 1999; Hus, 2001; Romeo et al., 2018). Nonetheless, it may be necessary for screening algorithms to be adjusted initially to take into consideration SES and related variables, such as home environment, so as not to overidentify risk in disadvantaged children. Future research should help us identify which screening measures and/or weighting adjustments are more or less indicative of risk in this population. A similar approach will be necessary for children from homes in which English, or the specific language spoken, is not the majority language. In this case, assessment of children’s minority language and early literacy may provide valuable information about risk beyond initial response to instruction and other screening measures (Language and Reading Research Consortium et al., 2019; Prevoo et al., 2016).
Intervention
Much progress has been made in intervention for dyslexia. Research demonstrates that explicit and systematic skills-based intervention directed at strengthening phonological awareness, letter-sound knowledge, and decoding/spelling abilities is maximally effective for many children with dyslexia (Lovett et al., 2017; Scammacca et al., 2007). Such intervention can be especially impactful when initiated early within a mult-tiered system of supports (MTSS) framework (Al Otaiba et al., 2014). Nevertheless, intervention procedures could be improved especially for a portion of children who respond less well to standard-treatment protocols. A multifactorial risk–resilience model of dyslexia would seem to have implications for how to do this. By identifying specific factors associated with dyslexia, such a model should provide relevant information on how best to intervene. That is, if a child shows a particular set of strengths and weaknesses, a specific intervention approach directed at that profile might prove to be especially effective. However, research has yet to show the efficacy of matching strength and weakness profiles with specific intervention approaches (Burns et al., 2016).
Despite the lack of evidence for interventions based on strengths/weaknesses profiles, interventions that take into consideration multiple risk factors could still prove useful if combined with standard-treatment protocols. For example, Tamm et al. (2017) found that targeting both attention deficits and reading problems in children with comorbid attention-deficit/hyperactivity disorder and dyslexia had more overall effectiveness than either intervention alone. Similar approaches could prove to be effective for children with a different set of risks. For instance, children who have experienced significant trauma in addition to having other known risk factors for dyslexia might benefit maximally from an intervention that addresses academic literacy skills as well as the psychological effects of the trauma. Also, for those children who have suffered significant negative consequences of reading failure (e.g., low self-concept, isolation, depression), an intervention that also addresses these secondary factors may prove to be advantageous.
Beyond focusing on risk factors, our model suggests that interventions might also take advantage of resilience factors. Given that these factors are thought to reduce the risk for dyslexia, addressing them in intervention could prove advantageous. This approach has been shown to be especially effective in other fields involving children at risk. For example, Forgatch et al. (2009) reported that parent management training significantly reduced the negative outcomes of children at risk for conduct disorder. A similar approach could be taken in work with children at risk for dyslexia. Specifically, intervention directed at improving parent and/or teacher support might have a positive impact on reading outcomes, especially when combined with word-level interventions. Alternatively, there has been some initial efforts made to facilitate a growth mindset or increase task-focused behavior in at-risk readers (Credé, 2018; Sisk et al., 2018; Yeager et al., 2019). The results of this work have been mixed but studies have not generally targeted improvement in word reading and/or tested these interventions in combination with standard treatment protocols, which might add to their effectiveness.
Conclusion
We have argued that a multifactorial causal model can best account for dyslexia when defined as an unexpected reading disability. We further have proposed that placing such a model within a risk–resilience framework could be advantageous for the early identification and treatment of dyslexia, which would assist school personnel in meeting state mandates. Currently, there is considerable support for many of the components of the risk–resilience model. There is also emerging evidence for multifactorial causal models that are central to the framework. Case-based studies have been especially informative in this regard (Catts et al., 2017; Pennington et al., 2012; Snowling, 2008). But these studies have mostly examined well-documented risk factors at single points in time. Additional support for multifactorial models could come from investigations that include a wider array of risk and resilience factors examined within a longitudinal perspective. This would better allow us to differentiate possible causal and correlative factors. Of course, other research designs (e.g., intervention studies) would be needed to fully support a causal basis.
Beyond case-based studies, investigations that treat risk and resilience factors as continuous variables could be particularly valuable both from the study of individual differences and causal modeling. This work would allow us to better investigate the additive and interactive effects of these variables. Specifically, exploratory research projects that study the presence of latent risk and resilience factors, including a wide range of exogenous and endogenous variables, would represent an initial step in analyses (e.g., Petscher et al., 2021). Finite mixture models (FMMs) such as latent class or latent profile analysis represent one methodology to look at heterogeneity in risk and resilience factors along levels of categorical latent variables. When combined with latent class regression models (e.g., three-step approaches; Asparouhov & Muthén, 2014), FMMs may both highlight levels of differences in such factors in a nuanced manner and test the extent to which profile differences in risk and resilience factors are predictive of individual differences in distal reading performance. Continuous latent variables of risk and resilience factors may also be used in sets of structural equation models as additive and interactive factors predicting individual differences in either dichotomous variables (e.g., performing below or at/above a cut-point on a selected outcome) or continuous measures of word reading. Moreover, classification accuracy models (e.g., logistic regression, CART analysis, ROC curve analysis) could be extended to not only consider the inclusion of single screener measures or multiple screener measures in an additive model but to look at statistical interactions across multiple screener measures to further study classification accuracy. For example, Petscher and Catts (2021) found that the area under the curve in a multifactorial risk model improved from .88 to .96 by including pairwise interactions among the indicators. Multifactorial risk–resilience models could further gain support from their application to early identification and intervention. For example, studies examining the effectiveness of interventions directed at both risk and resilience factors could be supportive (Masten, 2018). It is through these efforts and others that we may better serve children who are at risk for dyslexia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded in part by the Chan Zuckerberg Initiative.