
Abstract
A consumer’s personal attribute (e.g., disease, body weight) can assume the qualities of a stigma (i.e., become a source of devaluation by others) in the presence of certain audiences, which can affect consumption and represent a major hurdle to marketers in many industries (e.g., health care). Two field experiments manipulating the marketing communications sent to 1,453 consumers diagnosed with 87 diseases of varying stigma potential, as well as two Amazon Mechanical Turk studies, reveal that consumers with potentially stigmatizing attributes distinctly decode aspects of marketing communications as audience cues, to infer how (un)favorable observers of their consumption will be in light of the potential stigma. When consumers possess potentially stigmatizing attributes, audience cues influence social devaluation inferences, which influence their beneficial consumption (program enrollment, long-term engagement in health care program; e.g., 64% click-through decrease) and their interest in detrimental consumption (products that promise to alleviate the stigma but are associated with considerable risks). Anticipated empowerment may increase beneficial consumption among consumers managing stigmatizing attributes.
A stigma occurs when others judge an attribute of a person as negatively deviating from what they consider normal and devalue the person because of this attribute (Goffman 1963). Personal attributes such as health conditions (e.g., HIV, obesity) or financial status (e.g., poverty) can manifest as stigmas (Goffman 1963). Even new diseases (e.g., COVID-19) can quickly become stigmatizing (Centers for Disease Control and Prevention 2020). We propose that marketers need to understand that consumers with potential stigmas often feel they are constantly “on stage” and are unable to be themselves, for fear of being “reduced to the stigma itself” by unfavorable audiences (Hebl, Tickle, and Heatherton 2000, p. 289). We theorize that a stigma uniquely transforms consumers’ judgments of and responses to marketing communications, by making consumers more vigilant in identifying and reacting to audience cues—facets of the communication that inform consumers’ inferences about others they may encounter during consumption (e.g., other consumers) and how these others might judge them. For example, consumers with stigmatizing body weights may perceive seemingly neutral information such as the aspirational, fit models in typical gym ads as cues of an unfavorable, potentially threatening audience (e.g., due to social devaluation), rendering the marketing communication ineffective or even detrimental. The same cue may be a positive signal to consumers with nonstigmatizing body weights. 1 This research examines how and when stigma shapes consumer responses to marketing communication, including responses that likely bolster their well-being (e.g., join a health program), and those that undermine it (e.g., pursue offerings that promise to reduce the stigmatizing attribute quickly at considerable risk, such as bariatric surgery for weight loss).
Subtle and often ignored aspects of marketing communications can inadvertently serve as audience cues. Because stigma can dramatically affect consumers’ presentation of self in front of others (Goffman 1963), we focus on three aspects of ads that enable self-to-other comparisons: a demographic description of co-consumers, visual imagery, and an identified source of the communication. We use these aspects to determine the breadth of cues that trigger consumers to anticipate an unfavorable (socially devaluing) versus favorable (benevolent) audience, and how this affects their consumption.
We examine our conceptual model with four experiments in health care settings (potential stigma: disease and body weight). In these contexts, we observe personal attributes with low or no stigma (e.g., anemia, normal body weight) relative to high stigma (e.g., HIV, obesity) and manipulate audience cues in marketing communications. Study 1 is a longitudinal field experiment, conducted in collaboration with a health care firm, that includes 483 consumers diagnosed with 87 diseases and tests the effect of stigma on consumers’ immediate (click-through) and enduring (e.g., consumer posts, likes over time) responses to audience cues in marketing communications. Study 2’s experiment, conducted using Amazon Mechanical Turk (MTurk), then examines consumers’ anticipated social devaluation as an underlying mechanism mediating the effect of stigmatizing attributes on consumption. Studies 3 and 4 validate consumers’ inferences about a potential audience’s intentions toward them (anticipated devaluing or benevolent audience intentions) as key processes through which marketing communications differentially affect consumer responses among those with potentially stigmatizing versus nonstigmatizing attributes.
Our work offers multiple contributions to the marketing literature. First, we show that a personal attribute can take on the qualities of a stigma (i.e., consumers fear it as a source of devaluation) and affect consumption in relation to specific anticipated audiences. Integrating across our studies, we find evidence that consumers estimate threats related to a potentially stigmatizing attribute along a continuum that ranges from minimal threat (anticipated benevolent audience intentions) to high threat (anticipated devaluing intentions) depending on the degree to which consumers can accurately assess whether the stigmatizing attribute is shared or unshared with the audience, which signals a favorable or unfavorable power differential between the consumer and the audience. Thus, when managing potential stigmas, consumers’ threat assessments vary across audience attribute cues, from no information about the audience relative to the stigma, to a shared cue (e.g., HIV patient with an audience of other HIV patients), to an ambiguous cue (e.g., Type 2 diabetes customer with an audience of people suffering from various diseases), to a contrasting cue (e.g., obese consumer with an audience of thin people). Both ambiguous and contrasting cues allow inferences that the potentially stigmatizing attribute is not shared with the audience; we describe these as “unshared cues.” This continuum (from no information, to shared cues, to unshared ambiguous cues, to unshared contrasting cues) is crucial because it reveals insights into how consumers managing stigmatizing attributes screen for and respond to threats. To prevent unwanted effects and effectively target consumers with potential stigmas, marketers must understand where communications fall along this continuum (e.g., in Study 4, failing to refine communications in light of a stigma reduced click-through rates for a beneficial offering by 41%).
Second, we find that certain audience cues can inadvertently hinder beneficial and encourage detrimental consumption outcomes, illustrating the dangers of stigma in consumers’ decision making and their future well-being. For example, in Study 1, across 87 diseases ranging in their level of stigma, ambiguous audience cues reduced consumers’ participation in beneficial health programs relative to shared audience attribute cues. Moreover, among consumers managing a potential weight stigma, Study 2 demonstrates that the commonly used marketing tactic of aspirational images (e.g., thin models in ads for fitness centers) can signal an unfavorable audience (contrasting along the stigmatizing attribute of body weight); moreover, these aspirational images increase overweight consumers’ interest in offerings that promise to alleviate the stigma quickly (e.g., weight loss surgery) but that often come with high physical risks (e.g., malnourishment, even death) and financial costs. Thus, our research can help organizations and policy makers design more effective communications that prevent (unintentionally) nudging consumers who are managing stigmas away from beneficial and toward harmful consumption (e.g., Chaney, Sanchez, and Maimon 2019).
Third, we find that consumers prioritize the stigmatizing attribute in their definition of self, such that other typically more dominant indicators of similarity (e.g., gender, race) are subordinate to it (Study 2), thereby providing deeper insights into how people prioritize multiple dimensions of homophily (e.g., Block and Grund 2014; Lin and Lundquist 2013). Further, we find that consumers managing potential stigmas may operate with the assumption that all “others,” even those that might even be similar to them, may be a threat unless there are cues that the stigmatizing attribute can be concealed (Study 3) or cues that directly signal the audience’s benevolent intentions (Study 4). These findings identify theoretical insights and managerially relevant factors when similarity does not produce expected homophily effects.
Fourth, we discover (Study 3) that consumers managing a stigma make not only inferences about anticipated audiences, but also stigma-relevant assessments of (1) the offering and (2) the marketer. In terms of the offering, we find that, when consumers possess a potential stigma, they respond particularly favorably to beneficial offerings they perceive as opportunities for their empowerment in that the offering may help them overcome the adversities associated with their stigma (Shih 2004). However, in terms of the marketer, Study 3 shows a detrimental spillover effect: not only do consumers managing a stigma consider their consumption audience to be unfavorable toward them, but they also make detrimental inferences about the organization that promotes the focal consumption. Overall, our findings suggest that marketers need to better understand the relevance of seemingly benign cues in their marketing communication, which may signal audience characteristics and intentions to consumers managing stigmas, thereby reemphasizing the need for paradigms of positive marketing (Mick et al. 2012).
Stigma, Consumers, and Inferred Audiences
A stigma is an attribute of a person that negatively deviates from what others consider normal in a particular social context; it can be “deeply discrediting,” to the point that its possessor is vulnerable to global devaluation by others (Crocker, Major, and Steele 1998; Goffman 1963). However, by definition, not all deviant attributes are stigmas, and no attribute in isolation can be a stigma (Goffman 1963). Rather, stigma implies a social hierarchy in which the stigma possessor is in last (or a lower) place; they are assigned to this position by dominant others (i.e., an audience) in the focal social context. It is this audience that defines what is “normal,” determines acceptable tolerance around this standard, and assesses what is deviant and valued (Lin and McFerran 2016; Wooten 2006). For example, extreme intelligence can be a source of pride in certain social circles but, in others, may be “taken as a sign of social ineptitude” and ridiculed (Wooten 2006, p. 189). Thus, an attribute’s status as a stigma depends on the audience to which any person is exposed in a given (consumption) setting.
In consumption settings, stigma can influence the acquisition, use, and disposal of possessions (Wooten 2006). It can act as a “psychic boundary” that motivates consumers to hide consumption practices (Kozinets 2001), avoid participation in promotions (Tepper 1994), limit their consideration sets, ignore being cheated, or refrain from consumption altogether (Adkins and Ozanne 2005) to avoid stigma-associated risks. To understand the nature of the audience and how consumers sense its favorability toward them, we review extant marketing research, primarily ethnographic studies, that investigate consumption practices that can be sources of stigma (Argo and Main 2008; Kozinets 2001; Muniz and Schau 2005; Tepper 1994) or consumption as a means to manage stigmas (Adkins and Ozanne 2005; Coskuner-Balli and Thompson 2013; Hill and Stamey 1990; Kates 2002) (see Table 1 for summary).
Stigma and the Ever-Present Audience: Themes and Evidence from Extant Marketing Research.

Stigma and Consumers’ Inferred Audiences: Social, Economic, and Physical Consequences
Across diverse consumption contexts, prior research hints at the idea of an implied boundary between people who possess a stigma and those who do not, with the latter manifesting as an ever-present, potentially threatening audience for whom the consumer managing the stigma performs (Kates 2002; Kozinets 2001). The audience can be family or friends, but in the marketplace, it consists of other consumers and service providers too (Sandikci and Ger 2009). Importantly, audience reactions can vary widely from benevolent and empowering to devaluing and threatening (Shih 2004). Consumers search for those who are sympathetic or empathetic to the stigma often by finding those who share it. However, the extreme variance in audience reactions makes stigma management a volatile and dynamic process in which consumers (must) learn to anticipate conditions in which the potentially stigmatizing attribute will be problematic (Dovidio, Major, and Crocker 2000).
Revealing a stigmatizing attribute to an audience might be associated with real or imagined social consequences (e.g., “they treat you like you’re nobody”; stigma: homelessness; Hill and Stamey 1990, p. 312), economic consequences (e.g., “not entitled to the same services”; stigma: senior citizens; Tepper 1994, p. 505), or physical consequences (e.g., bodily harm by others in the marketplace; stigma: sexual orientation; Kates 2002). Thus, for consumers managing potential stigmas, others present at the time of consumption can range from merely irrelevant bystanders or empathetic co-consumers with benevolent intentions to audiences that might challenge their very existence, question their worth to society and entitlement to certain economic benefits, or even inflict physical harm.
Underlying each of these varied threats is the notion that certain audiences may socially devalue the stigma possessor by reducing the person’s worth from “a whole and usual person to a tainted, discounted one” (Goffman 1963, p. 4). Once an audience devalues a consumer based on a personal attribute, it creates psychological conditions that allow them to exclude this consumer from basic human protection, “making it permissible to treat [her] in a way that would be morally objectionable if [she] were fully human” (Goff et al. 2014, p. 527). Thus, fear of harm tends to outweigh expectations of benevolence and appears to be warranted, because social devaluation removes the person from the moral confounds of human rights, in the eyes of that focal audience.
Stigma and Sensing the (Un)favorability of an Audience: Audience Cues
Real and imagined threats related to possessing a stigma coincide with evidence that consumers constantly and vigilantly attempt to protect themselves from the harm an unfavorable audience may inflict on them (Kates 2002). Because it is impossible to know with certainty another’s intentions, consumers with potential stigmas learn to sense and interpret subtle cues and develop context-sensitive judgments to estimate the nature of an anticipated audience (Kates 2002). As a proxy, consumers use their stigma to filter visible markers or subtle behaviors that signal another person shares the focal or similar stigma (i.e., audience attribute cues) and use these signals to divide the world into those who are presumably sympathetic or empathic to the stigma with benevolent intentions toward them and those who are not (Adkins and Ozanne 2005; Frable, Platt, and Hoey 1998). Yet, attribute similarity is an imprecise proxy accompanied with a high risk of inaccurately estimating others’ intentions. Consumers often look for more explicit cues of benevolent intentions (i.e., audience intention cues), such as body language (e.g., smile; Hill and Stamey 1990) or overheard conversations about someone possessing the stigma (Coskuner-Balli and Thompson 2013), to supplement risky inferences made by attribute cues alone.
In summary, stigmatized consumers use cues in their environment such as visible similarities, behavioral subtleties, and observations as an audience member themselves, to sense the (often hidden) intentions of potential audiences, which can range along a continuum from benevolent to devaluing. Indicators of safe versus threatening audiences provide an important frame of reference for consumers’ stigma management and related consumption decisions.
Stigma and Consumer Responses to Audience Cues in Marketing Communication
Extant research generally examines the methods consumers use to infer others’ favorability toward a stigmatizing attribute in their immediate interactions with them (Crockett 2017; Kates 2002). Yet, consumers often need to use marketing communications to predict how future consumption encounters might unfold, on the basis of limited available information and cues in the communication, along with their memory of prior social encounters (Hoch and Deighton 1989). This is crucial for marketers to note, as these predictions typically emerge before the consumer has any social interactions with the focal company; thus, these predictions might inherently deter consumers from engaging with the company in the first place.
For consumers with potential stigmas, the consumption featured in marketing communication can be seen as an unknown, threatening social encounter (Adkins and Ozanne 2005). Their history and knowledge of the consequences of inaccurately reading a situation (e.g., experiencing social devaluation) can motivate them to go beyond merely considering whether an offering fits their economic needs, as is typical (Hoch and Ha 1986), and also consider their consumption audience and how they can ensure self-preservation in front of this audience. We propose that consumers managing stigmas use audience cues (e.g., visual stimuli) in marketing communication to infer where along the continuum of intentions (from benevolent to devaluing) a potential audience might fall, with implications for their consumption (see Figure 1).
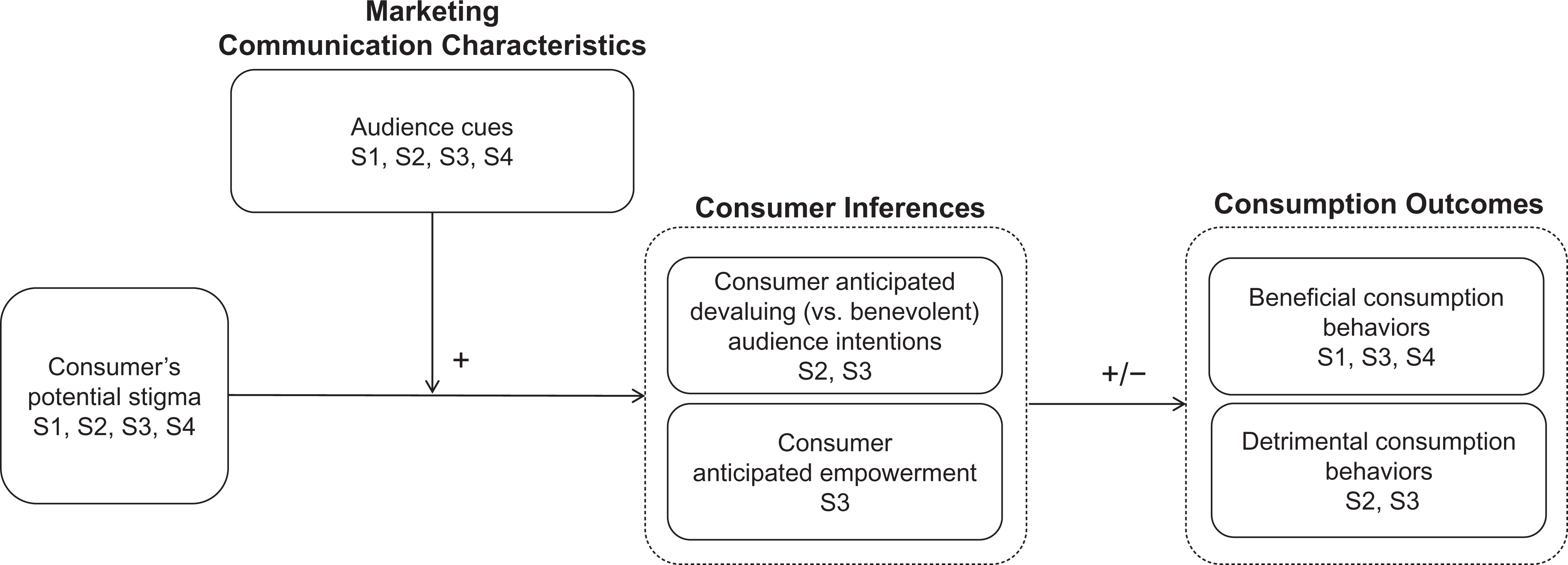
Effects of stigma on consumer responses to marketing communications.
If audience cues are unshared (i.e., either ambiguous with regard to the focal attribute, or contrasting relative to the consumer on the focal attribute), the apprehension that coincides with managing the stigma in unknown social encounters may cause the consumer to anticipate more negative audience-related effects (e.g., increased risk of social devaluation) (Crocker and Major 1989). In general, ambiguous cues allow inferences that range from very positive to very negative (Norton, Lamberton, and Naylor 2013). However, for consumers managing stigmas, communications for offerings that might improve their well-being (e.g., wellness programs) that include ambiguous audience cues may allow negative inferences to dominate, making them less responsive. Similarly, for consumers managing stigmas, unshared cues that are contrasting might elevate interest in high return–risk offerings that they otherwise might consider unnecessary or undesirable (Schouten 1991) (e.g., weight-loss surgery). In these conditions where social devaluation threats are high, consumers may adopt “nothing to lose” mindsets, such that they may believe others assign little worth to their current self (Brough et al. 2016) and discount risks of products that might cause physical harm (e.g., surgical procedures). If the focal cues signal that the audience shares the potentially stigmatizing attribute (e.g., health conditions), consumers should derive more favorable inferences about this audience’s intentions and possible effect on their well-being (e.g., decreased risk of social devaluation, increased inferences of benevolent intentions), enabling more beneficial response to the marketing communication.
In contrast, consumers without the potential stigma typically do not harbor concerns about social devaluations and thus do not attend to cues in marketing communication to check for threats as vigilantly as consumers with the stigma do (Chaney, Sanchez, and Maimon 2019). Taken together, unshared (i.e., ambiguous or contrasting) audience cues may evoke the idea of unfavorable audiences that elicit greater fear of social devaluation and reduce consumers’ likelihood to engage in beneficial consumption behaviors but increase their interest in detrimental consumption. We hypothesize the following effects:
Although we hypothesize the role of audience inferences (ranging from benevolent to socially devaluing) in influencing consumption decisions, we note that there might be characteristics related to the offering in which a seemingly negative attribute could be transformed into a source of empowerment (Conrad and Caldwell 2006; Shih 2004). Experiences and knowledge that can be acquired only through a history of stigma-related devaluation can create a unique expertise related to successfully navigating challenging social situations; this expertise might have value in certain consumption contexts. Providing consumption opportunities that allow stigmatized consumers to use and share their unique knowledge with others might help them feel empowered and motivate more positive responses. We therefore also explore the role of empowerment (in Study 3).
Empirical Overview and Research Context
We conducted four experiments in a health care context, including two field experiments (Studies 1 and 4), with an online health community provider. Health conditions—the main reason consumers seek health care products and services—are deviations from what is considered normal, though only some of them (e.g., HIV, obesity) are potentially stigmatizing. The marketing of many health care offerings makes salient the consumer’s health condition, exacerbating the associated stigma’s effects and discouraging consumption (DiMatteo 2004).
In the studies, we use offers of health care products and services, such as an online health care program, a platform for consumers to share health-related content about symptoms, treatments, and outcomes (Frost and Massagli 2008). An invitation to a new online program is an unknown social context, requiring consumers to estimate the risks and rewards of responding. Online health care platforms are widely used yet remain poorly understood (Wang, Zuo, and Zhao 2015; Young 2013). Thus, health care and online health programs offer managerially relevant contexts in which to rigorously test our theory. Table 2 summarizes the four studies.
Overview of Empirical Studies.

Study 1: Field Experiment Testing Stigma and Response to Marketing Communications
Using a longitudinal field experiment and a sample of consumers diagnosed with a wide variety of diseases (e.g., HIV, cancer, rheumatoid arthritis; see Web Appendix A), we analyze whether the degree to which consumers’ diseases are stigmatizing determines whether they click through on marketing communications that vary in their audience cues. We also test these effects on actual consumer engagement behaviors (e.g., likes, comments, friend requests) over a two-week period following their initial acquisition. Specifically, we examine the interaction between audience attribute cues (ambiguous vs. shared attribute cue) and disease stigma on consumers’ likelihood to join a wellness program and longer-term activity within that program.
Study 1: Design, Participants, and Procedures
The study employed a 2 (audience attribute cue: ambiguous, shared) × measured (disease-related stigma) design. Participants (N = 483) were consumers who agreed to be contacted by the collaborating health care firm about their disease and opened the invitation from the firm. Participants were randomly assigned to conditions, using stratified random sampling by disease, so each disease was equally likely to appear in each condition. An email with the company name and logo invited participants to join either a general health group (ambiguous audience attribute cue) or a group of others sharing the same disease (shared audience attribute cue), as follows: “Thanks for signing up to learn about opportunities to connect with others about your personal health experiences with (health condition)! You may think your story is ordinary, but to someone who is struggling with the uncertainty and fear of a health-related issue, hearing from someone who has been there can make all the difference. The [ambiguous group / shared disease group] in the [Company Name] community offers many ways—such as chats, polls, and blogs—for you to relate and empathize with people about what you’re going through. As a member living with a chronic condition, I hope you’ll sign up. By joining [Company Name] community and the [ambiguous group / shared disease group], you can shape the experience and create a community of people who care about (health condition). Getting started is easy—just click
Manipulation test
We used a sample of 69 U.S. MTurk participants (MAge = 35.78 years, 37 women) to test the effectiveness of our audience attribute cue manipulations. We described the skin illness psoriasis and asked participants to imagine having it, then randomly assigned participants to read either the unshared (ambiguous) or shared email message from the main study. Next, they indicated the extent to which the audience reflected the group with a shared illness (“like a generic-health group/like a specific psoriasis group”; “comprised of people with diseases other than psoriasis/comprised only of people with psoriasis”; “not at all similar to me/very similar to me”; “not specific to psoriasis/very specific to psoriasis”; “distant to me/close to me”; “not like me/just like me”; “a general health group/a health group focused on psoriasis”) on seven-point bipolar scales (α = .90). Participants in the shared audience cue condition perceived the group as having a shared illness (MShared = 5.79, MAmbiguous = 4.81; F(1, 67) = 11.41, p < .001).
Study 1: Results and Discussion
Click-through behavior
We conducted a logistic regression analysis on click-through behavior as a function of disease-related stigma, audience attribute cues, and their interaction. The audience cue main effect is marginally significant (Wald χ2 = 2.93, p = .09), but the stigma main effect is not (Wald χ2 = .68, p = .41). More important, these effects are qualified by the predicted significant two-way interaction (Wald χ2 = 10.20, p < .001; Figure 2, Panel A). In support of H1a, a Johnson–Neyman (JN) analysis reveals that consumers with highly stigmatizing diseases are significantly less responsive if the audience cue is unshared (ambiguously defined) versus shared (possessing the same disease as the recipient), (stigma level ≥ 4.08; z = 1.96, p < .05). This effect reverses for consumers with low-stigma diseases (stigma levels ≤ 1.83; z = −1.96, p < .05).

Study 1 (longitudinal field experiment): Johnson–Neyman analysis of audience attribute cues by stigma.
Long term engagement behaviors
We conducted an analysis of variance (ANOVA) on long-term engagement behaviors in the health care program as a function of the audience attribute cue factor. The audience cue main effect is significant (F(1, 479) = 8.76, p = .003), and the stigma main effect is not (F(1, 479) = .86, p = .35). Importantly, these effects are qualified by a significant two-way interaction (F(1, 479) = 6.70, p = .01; Figure 2, Panel B). Providing further support for H1a, the JN analysis reveals that consumers with highly stigmatizing diseases engage in fewer activities in response to an unshared (ambiguous) versus shared (one that signals they share the same disease) audience cue (stigma level ≥ 5.45; z = 1.96, p < .05). This effect reverses for consumers with low-stigma diseases (stigma levels ≤ 1.74; z = −1.96, p < .05).
In a field study, using unobtrusive measures of stigma and real, observable consumer behaviors (e.g., joining an online health program, customer engagement behaviors), Study 1 provides evidence that audience attribute cues alter consumers’ behaviors when they have a potentially stigmatizing disease. Specifically, we show that consumers whose diseases are more stigmatizing are less interested in engaging in beneficial consumption (e.g., online health program) when audience cues are ambiguous versus specified as sharing a stigmatizing attribute with other consumers; when stigma is low, this effect is attenuated. An invitation with unshared (vs. shared) audience attribute cues decreased click-through rates among consumers with highly stigmatizing diseases (+1SD) by 64%. Moreover, those who joined the program after receiving an invitation with an ambiguous (vs. shared) audience cue completed 52% fewer engagement activities over two weeks. Importantly, these effects cannot be explained by homophily, as we would expect only a main effect of audience cues and no interaction by stigma.
Study 2: Stigma, Audience Cues, and Anticipated Social Devaluation
We theorize the effects observed in Study 1 are caused by inferences made by consumers with highly stigmatizing diseases, anticipating that others in the ambiguous (vs. shared disease) group observing their consumption may devalue them, due to the disease. However, messages may have audience cues that contrast the stigmatizing attribute with a nonstigmatizing one (e.g., using an ad with a thin model when marketing to obese consumers). In Study 2, we test the mediating role of anticipated social devaluation and examine contrasting audience attribute cues using a controlled experiment involving marketing communications for a full-service health facility (e.g., fitness, medical weight loss, spa services). Study 1 tested verbal audience attribute cues. Study 2 tests a visual audience attribute cue. We use body mass index (BMI) as a potential source of stigma, because it is associated with a nationally communicated standard for “normal” and deviant categories (overweight, obese, and morbidly obese) and is linked to pervasive societal stigma (Puhl and Brownell 2006). 3 Thus, BMI provides theory-based levels at which stigma effects are expected to occur (CDC 2019), as compared with nonstigmatizing levels of the same attribute.
Study 1 focuses on a beneficial choice: actual program enrollment behaviors. However, stigma also may influence potentially detrimental purchase decisions. Stigmatized consumers may seek alternatives that (promise to) offer high rewards—physically substitute the stigma for a desirable attribute in its place, but also entail high risk, because it might be irreversible, painful, or dangerous (Puhl and Brownwell 2006; Schouten 1991). Therefore, with Study 2 we test whether audience cues in marketing messages influence consumers’ interest in high return–risk products (e.g., surgical procedures) that promise to quickly alleviate the stigma by reducing excess weight—but come with risks of bodily harm (Chang et al. 2014).
Study 2: Design, Participants, and Procedure
We employed a 3 (audience cue: control vs. shared vs. unshared, contrasting) between subjects × measured (BMI: stigma source) design. Participants (396 U.S. MTurk participants; 200 women; MAge = 40.93 years; MBMI = 27.89)
4
completed a two-part study. We use BMI as an indicator of the degree to which participants’ body weights are stigmatizing and test anticipated devaluation as a mediator. First, participants indicated their weight in pounds and height in inches, which we used to calculate their BMI (703 × weight (in pounds) / [height (in inches)]2). Two days later, participants were randomly assigned to one of the three audience attribute cue conditions: a heavy, thin, or no image of a woman (images adopted from McFerran et al. 2009) who was featured in a health facility testimonial, as follows: “Customer Testimonial: I recently joined [Company]. When I first came to the gym and looked around, the equipment looked great and the trainers were friendly. Most of the members were in the same shape that I am in. —Jessica B., [Company] Member”
The outcome variable was consumers’ interest in a high return-risk offering by the health facility (i.e., sleeve gastrectomy surgery) (H1b). To better disguise the focal offering and reduce demand artifacts, we intermingled it among six other products designed to manage the stigmatizing attribute (BMI) with a brief description of each, in random order (e.g., weight loss acupuncture, cool sculpting, body firming detox; see Web Appendix C for descriptions and stimuli tests). Participants indicated their purchase interest for each product on five-point scales (1 = “Not interested at all,” and 5 = “Extremely interested”). We included anticipated social devaluation as a mediator: “If I met other people at this gym, I think they would be mortified to meet me; If I met other people at this gym, I think they would be disappointed to meet me” (seven-point, “strongly disagree” and “strongly agree”; randomized; α = .67; Shrauger and Schoeneman 1979). The woman in the images from McFerran et al. (2009) was of Asian descent, so we controlled for gender and race. 5
Study 2: Results and Discussion
Interest in high return–risk product 6
An analysis of covariance (ANCOVA) on interest in the high return-risk product indicates significant BMI (F(1, 388) = 4.32, p = .04) and audience cue (F(2, 388) = 4.68, p = .01) main effects. Importantly, the predicted two-way interaction also is significant (F(2, 388) = 6.13, p = .002), see Figure 3A. An omnibus groups regions of significance (OGRS) analysis locates significant JN regions for the effect of a multicategorical variable and continuous variable interaction (Hayes and Montoya 2017). The OGRS JN point is at BMI ≥ 29.12 (p = .05), a point within the overweight category that is approaching the obese category (see Figure 3, Panel A). To examine the two-way interaction further, we use PROCESS Model 1. Notably, the effect of BMI on interest in the high return-risk product is only significant in the unshared, contrasting weight condition (Contrasting: β = .04, t = 3.62, p < .001; Shared: β = .02, t = 1.58, p = .11; Control: β = –.02, t = −1.39, p = .16) supporting H1b. To look at this another way, we ran spotlight analysis using planned contrasts (control vs. shared; control vs. contrasting; contrasting vs. shared). When BMI reaches the CDC designation of obese (BMI = 30), the shared (F(1, 388) = 3.56, p = .06) and contrasting (F(1, 388) = 7.57, p < .01) condition produce greater interest in the high return–risk product, relative to the control condition. At higher levels of the obese category (BMI = 37.5), the contrasting condition produces greater interest in the high return–risk product than the shared condition ((F(1,388) = 2.87, p < .09; see Figure 3).
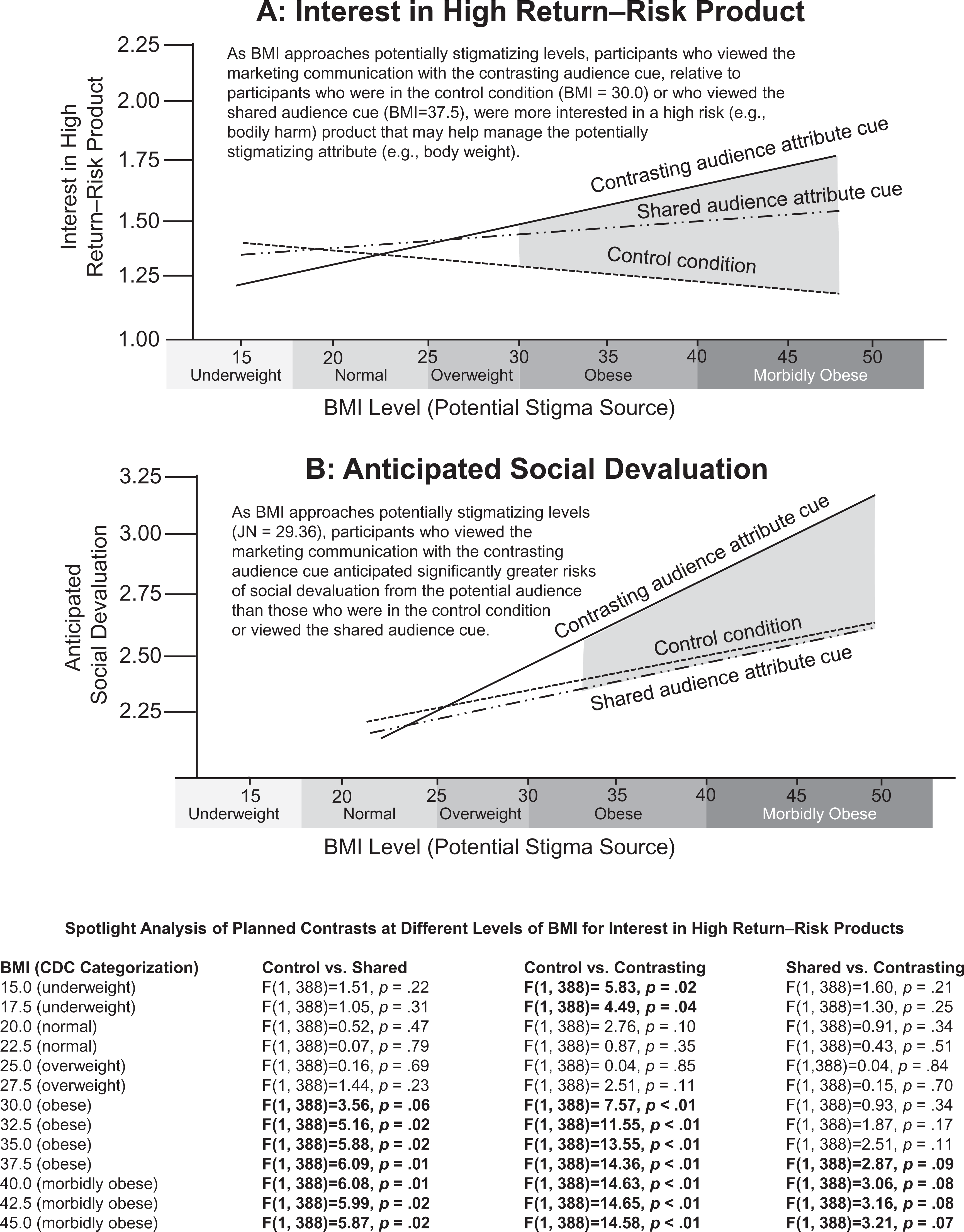
Study 2 results: Johnson–Neyman analysis of audience cues by BMI (stigma source).
Anticipated social devaluation
An ANCOVA on anticipated social devaluation indicates a significant BMI main effect (F(1, 388) = 18.46, p < .001); the audience cue main effect is not significant (F(2, 388) = 1.79, p = .17). The two-way interaction is marginally significant (F(2, 388) = 2.91, p = .06); see Figure 3, Panel B. For this interaction, the OGRS JN point (p = .05) occurs at BMI ≥ 29.36, in the overweight range. Exploring the interaction, PROCESS Model 1 shows effects of BMI on anticipated social devaluation in the contrasting (β = .07, t = 4.35, p < .001) and shared conditions (β = .02, t = 1.75, p = .08); it is not significant in the control condition (β = .02, t = 1.32, p = .19). Looked at another way, when BMI is low (−1SD), the conditions are not significantly different from each other (contrasting vs. control, t = −.37, p = .71), (shared vs. control: t = −.15, p = .88), (contrasting vs. shared: t = −.22, p = .83). When BMI is high (+1SD), the shared and control conditions are not significantly different (t = −.04, p = .97); the contrasting condition is significantly greater than the control (t = 2.54, p = .01) and shared (t = 2.84, p = .005) conditions.
Moderated mediation
We examine the mediating role of anticipated social devaluation on interest in the high return–risk product (Process Model 107; Hayes 2015). The independent variable is BMI, the moderator is audience attribute cues, the mediator is anticipated social devaluation, and the dependent variable is interest in the high return–risk product. Supporting H1c, when the audience cue features a consumer with an unshared, contrasting body type to the participant, anticipated social devaluation mediates (a × b = .0105, 95% confidence interval [CI]: .0041, .0189). It does not mediate when the audience cue signals a shared BMI (a × b = .0036; 95% CI: −.0007, .0094) or in the control condition (a × b = .0032, 95% CI: −.0012, .0119).
The findings in Study 2 suggest that, when consumers’ BMIs are potentially stigmatizing, a popular approach that firms use to advertise health facilities (i.e., depicting thin, aspirational models), may increase their interest in risky products that promise to alleviate their stigma (e.g., weight-loss surgery). In Study 1 we test ambiguous audience cues, which potentially enable inferences about onlookers that vary from anticipating others who share or who contrast their stigmatizing condition (Einhorn and Hogarth 1985); in Study 2 we provide a contrasting audience cue that should clarify these inferences. Study 2 also provides evidence that a potential stigma can make consumers more sensitive to visual as well as verbal (Study 1) audience cues.
Study 3: Manipulating Exposure of the Potentially Stigmatizing Attribute to an Audience
In Study 2, the shared audience attribute cue produced more interest in detrimental consumption than when the visual audience attribute cues were removed (i.e., the control condition), suggesting any information about the focal attribute (even information suggesting attribute similarity with audience members) may elicit inferences of threats. An audience implies some degree of public exposure to others. Yet, our theory suggests it is not general visibility to onlookers that affects behavior, but exposure of a consumer’s stigmatizing attribute to others. Thus, factors that reduce exposure of this attribute could render an audience irrelevant and eliminate the effects. In Study 3, we manipulate exposure of the potentially stigmatizing attribute while holding the audience cue constant to test our theory. We focus again on online health care offers, a context in which typically nonconcealable attributes (e.g., body weight) become concealable. Thus far, we have focused on negative inferences (social devaluation), but when managing stigmatizing attributes, consumers may also make positive inferences, with implications for consumption behaviors. In Studies 3 and 4 we look for evidence of more positive inferences (e.g., anticipated empowerment and benevolent intentions, respectively) as consumption drivers.
Study 3: Design, Participants, and Procedure
In Study 3, again using BMI to capture the level of stigma associated with participants’ body weight, we test whether marketing messages that signal body weight exposure will alter consumers’ responses when their weight is potentially stigmatizing, as a means to corroborate the prioritization of stigma-relevant audience information among these consumers. With a 2 (body weight exposure: yes, no) between × measured (BMI: stigma source) design, holding audience cues constant, we test anticipated social devaluation and anticipated empowerment as mediators. We manipulated body weight exposure as follows [exposed/not exposed]: We would like your opinion on a new online health workshop. Below are the instructions for how individuals sign up for the program. To Join the Program: The website will use [a full body photo of you to create an exact silhouette (outline) of your body to serve as your avatar / an image you select to serve as your graphic logo]. To protect your identity and anonymity, this is used instead of showing the actual photo of you. The software will use [your full body photo to create a silhouette of your body / this line art image], to represent you when you interact with other members of the community. To join: Please upload your photo, then enter the following: [Weight, Height, Age, Gender. /Age, Gender.] The other people in the community will see your: [Silhouette of your body based on your photo, Height, Weight, Age, Gender. / Line art graphic of you, Age, Gender.] [A corresponding graphic with “Support Group” in the header, also showed a red arrow with either “Your Photo Here. Upload a photo of you…” or “Get Started. Create an account…” to begin sharing and receiving support in a nurturing setting. See graphic in Web Appendix D.]
Manipulation test
As a test of our manipulations, we randomly assigned 80 paid U.S. MTurk participants (48 women, MAge = 35.53 years) to view stimuli from one of the two conditions (exposed vs. not exposed). Next, they responded to items designed to measure how exposed they would feel: When interacting with people in this group: “…people could see my body”; “…people would know my weight; my weight would be visible and exposed”; “…other people in the group could see what physical shape I am in”; “…people could judge my weight” (α = .96). We also examined effort to join: “It would take a lot of effort / time / energy / work for me to join this group” (α = .95): anonymity: “People would not know exactly who I am”; similarity: “People in this group are likely very similar to me”; and effectiveness: “Joining this group would be an effective means of managing my weight” (all seven-point scales anchored by “strongly disagree and strongly agree”; random order). The results show that the exposed condition results in significantly greater feelings of weight exposure (MExposed = 5.48, MNotExposed = 2.86, F(1, 79) = 62.34, p < .001). We observed no difference in perceptions of the effort involved (MExposed = 3.82, MNotExposed =3.56, F < 1), effectiveness (MExposed = 4.78, MNotExposed = 5.08, F < 1), or level of anonymity (MExposed = 4.70, MNotExposed = 4.98, F < 1), which rules out the possibility that participants perceived one workshop required more effort to join than the other, one was more effective than the other, or one was more anonymous than the other. There was no difference in perceived similarity (MExposed = 4.55, MNotExposed = 4.56, F < 1); thus, we effectively held the audience constant.
Procedures
Over the course of three days, 389 paid U.S. MTurk participants (196 women, MAge = 39.16 years; MBMI = 26.47) participated in the experiment. 8 First, participants provided demographics and their body weight and height, which we used to calculate their BMI. Two days later, the participants were randomly assigned to assess marketing communications about a health care program (here, a workshop) that focused on benefits to the participants. The audience cues remained constant across all conditions, indicating “people similar to you.”
After reviewing the marketing communication, participants indicated their likelihood to enroll, on the following items: “I would like to enroll in this program,” “I would like to join this program,” and “I would like to sign up for emails from this program” (seven-point scale anchored by “strongly disagree” and “strongly agree”; α = .96). We further isolated how much risk participants are willing to assume to quickly alleviate the stigma by directly measuring their comfort with a given level of risk for a particular return on products recommended through the workshop. To this end, we asked the following questions: “Imagine you could have an Outpatient Medical Procedure (Daily Medication for Three Months). The procedure (medication) is designed to get you your ideal body. Please indicate which option you prefer…(0) I would not try this product, (1) 10% chance of success, 5% chance of minor side effects, 1% chance of serious side effects – (9) 90% chance of success, 45% chance of minor side effects, 9% chance of serious side effects” (at each scale point, all percentages were increased by 10%, 5%, and 1%, respectively; α = .84; e.g., Tversky and Kahneman 1981). We captured anticipated devaluation using the following items: “Thinking about what it would be like to join this group, I feel that I will be negatively judged,” “If I joined this group, I would feel embarrassed about my weight,” If I joined this group, I would be humiliated by my weight,” and “If I joined this group, I would feel distressed about my weight,” (seven-point scale anchored by “strongly disagree” and “strongly agree”; α = .91, Blair and Roese 2013). They also indicated anticipated empowerment: “My experiences with my weight could be a source of insight for other people in this group,” “I could really help others in this program by sharing my personal experiences with my weight,” and “My personal history with my weight gives me a unique advantage to help others in this program” (seven-point scale anchored by “strongly disagree” and “strongly agree”; α = .91, based on Shih 2004).
Consumption decisions involve a mix of inferences that include how consumers feel others will judge them, how the offering may benefit their self-concept, and how they perceive the marketer’s intentions and their persuasion attempts (Friestad and Wright 1994). We capture the former in our measures of anticipated devaluation and empowerment, but it may be that when consumers anticipate devaluation by others, they may also become more skeptical of the ad. Therefore, we also capture consumers’ assessments of the manipulative intent of the ad: “The advertiser tried to manipulate the audience in ways I don’t like,” and “I was annoyed by this flyer because the advertiser seemed to be trying to inappropriately control the consumer audience” (seven-point scale anchored by “strongly disagree” and “strongly agree”; α = .89, Campbell 1995). We also included exploratory measures of guilt and shame; see Web Appendix D for the results and Web Appendix E for list of variables measured.
Study 3: Results and Discussion
To test both beneficial consumption (joining a wellness program) and detrimental consumption (interest in high risk–reward products) while also modeling both proposed mechanisms (anticipated devaluation, empowerment), we simultaneously estimated a model in AMOS. This method (1) accommodates multiple mediators and dependent variables, (2) enables us to estimate the complex relationships in the model simultaneously, and (3) is robust to the nonnormality of multiplicative terms for testing interactions. As a first step, we conducted confirmatory factor analyses for all multi-item constructs in our empirical model. The results indicated good overall fit (χ2(38) = 70.49, p = .001; comparative fit index = .99; incremental fit index = .96; Tucker–Lewis index = .99; root mean square error of approximation = .05; standardized root mean square residual = .02). All standardized factor loadings were .64 or greater and statistically significant at p < .001. The model exhibited high internal consistency, with average variances extracted (AVEs) from .70 to .92. The AVE for each factor was greater than its squared correlation with any other factor, in support of discriminant validity (see Web Appendix D for descriptives).
To determine the statistical significance of the parameter estimates, we simultaneously estimated the joint effects using maximum likelihood estimation in AMOS. Our overall structural model exhibited high goodness of fit (χ2(92) = 171.49, p < .01; comparative fit index = .98; incremental fit index = .98; Tucker–Lewis index = .97; root mean square error of approximation = .05; standardized root mean square residual = .05). The moderating effect of body weight exposure cues is positive and significant on the relationship between BMI and anticipated devaluation (β = .11, p = .04). The path between anticipated devaluation and likelihood to enroll was not significant (β = .05, p = .26) but was significant for interest in high risk-reward products (β = .24, p < .001). The path between anticipated empowerment and likelihood to enroll (β = .52, p = .001) was significant. It was also significant for interest in high risk–reward products (β = .16, p = .01) (see Table 3 and Figure 4).
Study 3 Results: Effects of Stigma and Audience Cues on Beneficial and Detrimental Consumption.
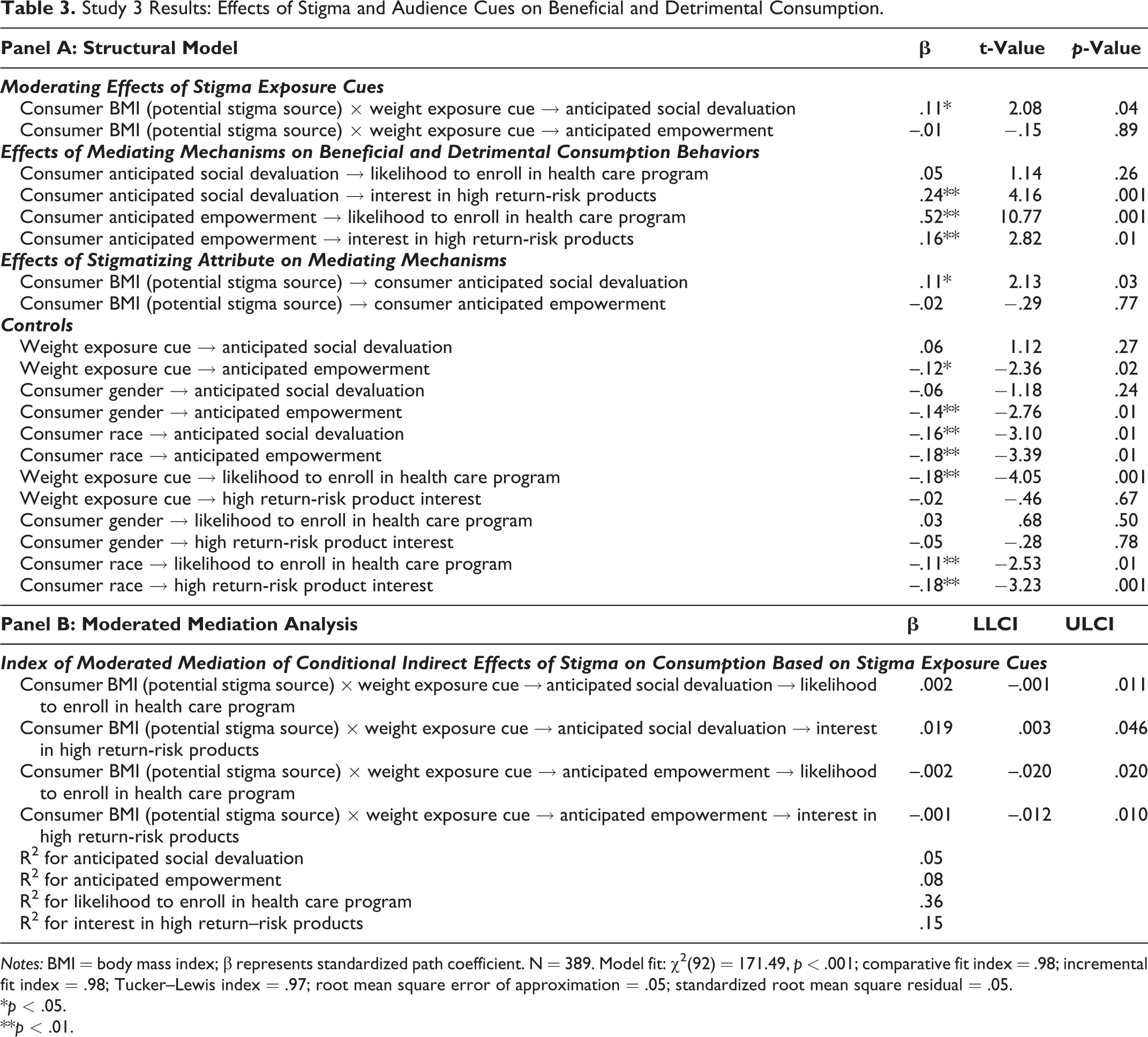
Notes: BMI = body mass index; β represents standardized path coefficient. N = 389. Model fit: χ2(92) = 171.49, p < .001; comparative fit index = .98; incremental fit index = .98; Tucker–Lewis index = .97; root mean square error of approximation = .05; standardized root mean square residual = .05.
*p < .05.
**p < .01.

Study 3 results: effects of stigma on consumers’ beneficial and detrimental responses to marketing communications.
Moderated mediation analysis
To test whether the BMI by exposure cue interaction on consumption is mediated by anticipated devaluation and/or anticipated empowerment, we estimate conditional indirect effects in AMOS using Hayes’s (2015) recommendations. This allows us to test the indirect effect of BMI (stigma source) through social devaluation dependent on whether the participant’s weight was exposed while simultaneously estimating the effect of anticipated empowerment (and vice versa), which is essential when investigating simultaneous mediators with proposed opposing effects. When BMI is at potentially stigmatizing levels (+1SD, BMI = 34.32), weight exposure (versus no exposure) increases anticipated devaluation, which then increases interest in high risk–reward products (a × b = .74, 95% CI: [.139, 1.69]). At low levels (−1SD BMI = 18.62), the effects are weaker (a × b = .44, 95% CI: [.092, 1.02]), providing evidence for H1c. The other mediation effects are nonsignificant (see Table 3).
Exploring the role of manipulative intent as a distal mediator
In this study, anticipated social devaluation does not reduce likelihood that participants would join the wellness program. One possibility for this surprising finding is a spillover effect, such that consumers’ beliefs that the audience will be unfavorable toward them spill over to create suspicion of the advertisers’ intentions, which then might impact their likelihood to join. We tested this explanation with an alternative model that includes participants’ assessments of manipulative intent of the ad as a distal mediator such that, conditional on the presence of body weight exposure cues in the advertisement for the wellness program, BMI is expected to influence anticipated social devaluation, which then influences perceptions of the marketer’s manipulative intent to ultimately affect likelihood to enroll. Indeed, we find a significant moderated mediation effect for the highest-order interaction for likelihood to enroll (a × b × c = −.004, 90% CI: [−.011, −.001]). Body weight exposure is more relevant to consumers’ likelihood to enroll when consumers’ BMIs are highly stigmatizing, and this effect is mediated by anticipated devaluation, which impacts their assessments of manipulative intent of the ad (+1SD, BMI = 34.32) (a × b × c = .22, 90% CI: [.021, .681]). This effect is significantly weaker at low levels (−1SD, BMI = 18.62) (a × b × c = .13, 90% CI: [.013, .396]). 9
This study provides further validation that the effects we observe are not just audience effects, but “stigma audience” effects, which require exposure of the potentially stigmatizing attribute to others. When we hold the audience cue constant, consumers with potentially stigmatizing BMIs respond less favorably to marketing communications that signal their body will be exposed to an audience during consumption, relative to those that are not exposed. Consumers with weights at levels that are not stigmatizing respond indifferently to weight exposure or no weight exposure.
The results provide additional support for our theorizing and a more holistic view of consumers’ decision-making processes that includes assessments of both opportunities and threats relative to the stigmatizing attribute. Consumers with potentially stigmatizing weight generate audience inferences, which in Study 3 were amplified when their weight was exposed to others; the main requirement for an “audience” to exist. This finding cannot be explained by homophily alone, which would predict consistent effects across all conditions since similarity is held constant (Naylor, Lamberton, and Norton 2011). It provides evidence that anticipated social devaluation mediates the effect of a stigma on consumer responses to marketing communications. Although empowerment seemed unaffected by whether the focal attribute was visible to others, it emerged as the primary determinant of enrollment intentions.
Study 4: Test of Process by Moderation, Manipulating Audience Intentions
Audience attribute cues—explicitly defining the potential audience as possessing the same disease or not (Study 1), photos of a thin or heavy co-consumer (Study 2)—provide a baseline from which consumers can estimate an audience’s intentions in light of the stigmatizing attribute. These inferences inherently contain some level of uncertainty that likely affects decision making. As demonstrated in Study 2, if a consumer is managing a stigmatizing attribute, even if an audience cue signals a shared attribute, they may show greater interest in detrimental behaviors. This may be due to the remaining ambiguity associated with potentially hidden intentions of the audience. In each of the previous studies, all audience attribute cues were accompanied by word choices (Study 1: “community of people who care…I look forward to welcoming you”; Study 2: “friendly” staff members; Study 3: “Support Group,” “Get help…,” and “support in a nurturing setting”) that may have guided participants’ inferences about the benevolence of the audiences’ intentions toward them. Theoretically, this would have skewed consumers to infer more benevolent intentions of the potential audience than if these words were not present. Yet, even with these benevolent words we find consistent evidence that consumers inferences of social devaluation vary based on the audience attribute cue they view.
In Study 4, we examine our proposed process further by testing whether more direct audience intention cues (i.e., benevolent words vs. neutral word choices) are necessary for consumers to make favorable assessments of audience attribute cues. If removing these direct intention cues in conditions when the attribute cue would signal a more favorable audience (shared attribute cue) reduces consumers positive response, then this suggests that for consumers managing stigmas, their main priorities for identifying similarity to the audience is to estimate people’s intentions of them, providing further support of H1c.
Study 4: Design, Participants, and Procedure
In Study 4 we partnered with the same health care firm from Study 1 that provided access to consumers diagnosed with a variety of diseases (e.g., HIV, cancer, rheumatoid arthritis). We analyze the click-through effectiveness of various marketing communications, contingent on the degree to which a consumer’s disease is stigmatizing. We employed a 2 (audience attribute cue: shared vs. unshared, ambiguous) × 2 (audience intention cue: benevolent vs. neutral) × measured (disease-related stigma) design. For the field experiment, we assigned participants to conditions using stratified random sampling by disease, to ensure each disease was equally likely to appear in each experimental condition. The sample includes all 970 consumers who received and opened an email solicitation from the company that promoted the online health care program.
Field study participants received an email with the company name and logo, in which we manipulated audience attribute cues (email sender as either a community member suffering from a disease (shared) or a manager of the health care program (unshared, ambiguous). We manipulated audience intentions cues as benevolent or neutral. We manipulated audience attribute cue [shared / unshared, ambiguous] shown here with italics and audience intention cue [benevolent/neutral] shown here in square brackets. The email read: Thanks for signing up to learn about opportunities to [connect with others / exchange information] about your personal health experiences. As [a member of the / the Community Manager for] (Company) community, I’m excited to announce that the new (Company) online [platform / community] is now up and running! The online [community / platform] is a place where people can [connect with a supportive community / exchange information and insights on how] to treat, manage, and cope with (recipient’s condition). The [community / platform] offers many ways—such as groups, chats, polls, blogs, and more—for you to connect with people who [can relate and empathize with / have experience and information about] what you’re going through. As [a member myself / the Community Manager] I wanted to personally invite you to join. By being among the first to join (Company) community, you’ll have the opportunity to shape the experience and create a [community of people who care / platform for learning from others]. In sum: (Company) Community is a [supportive community focused on / great source for the inside scoop about] (recipient’s condition). Getting started is easy—just click here or on the button below. I look forward to getting to know you! (Name), [(Recipient’s condition) Patient / Community Manager]
Manipulation test
To test our manipulations, we randomly assigned 101 participants (MTurk, MAge = 36.91 years, 59 women) to one of the four conditions and asked them to “imagine you are suffering from an illness that you feel impacts your life in a meaningful way. At your doctor’s office, you provided your email address to join a mailing list about the condition. You receive the following invitation on email.” After reading the email (from the main study), participants indicated the extent to which they perceived the audience intention cue to be benevolent (“The people in this group seem more focused on” “…a selfish intent / a benevolent intent”; “…what they can get out of the group / what they could give to others in the group”; “…caring for themselves / caring for others”; “…helping themselves / helping each other”; “…learning from others / connecting with others”; and “…exchanging insider information / providing support and encouragement”; randomized, nine-point bipolar; α = .87). Participants also responded to the audience attribute cue scale (“The person sending the email seems: “…like a person who has the same illness”; “…like someone with the same condition”; “…like a company expert” (R); “…like someone who works for the company” (R); randomized, 1 = “strongly disagree,” and 7 = “strongly agree”; α = .84).
An ANOVA on the audience intention cue index reveals an intention type main effect (MBenevolent = 7.25, MNeutral = 6.07; F(1, 97) = 14.94, p < .001). The audience attribute cue main effect and the interaction are not significant (Fs < 1). An ANOVA on the audience attribute cue index reveals an audience attribute main effect (MShared = 4.37, MAmbiguous = 3.38; F(1, 97) = 16.15, p < .001). The audience intention cue main effect (p = .25) and the interaction (F < 1) are not significant.
Study 4: Results and Discussion
A logistic regression analysis of click-through behaviors includes stigma, audience attribute cues, audience intention cues, and their higher-order interactions. We find the predicted three-way interaction (Wald χ2 = 4.76, p = .03; Figure 5); the other effects in the model are not significant (ps > .59). As expected, for low stigma diseases (−1 SD), the audience attribute × audience intention simple interaction effect is nonsignificant (a × b = .11, z = .53, p = .60). For highly stigmatizing diseases (+1 SD), the audience attribute × audience intention simple interaction is significant (a × b = .67, z = 2.69, p = .007).
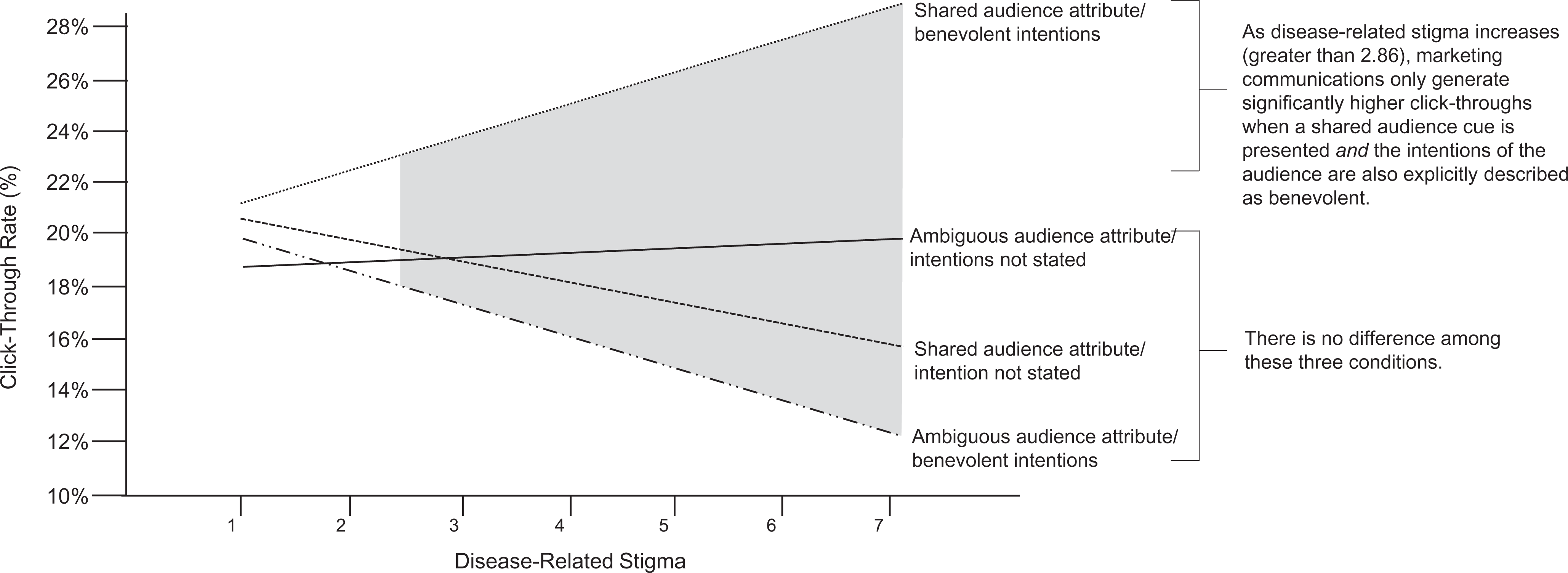
Study 4 results (field experiment): analysis of audience attribute cues and audience intention cues by stigma.
We test the interaction between the four combinations of audience-based communications (shared–benevolent, shared–neutral, ambiguous–benevolent, ambiguous–neutral) and stigma. We identify the point at which the omnibus interaction becomes significant, namely, when stigma ≥ 2.86 (Hayes and Montoya 2017). Consumers with highly stigmatizing diseases (+1 SD) who receive shared–benevolent audience cues (M = 26.67%) click significantly more often than the other groups (average M = 15.66%; z = 2.69, p = .007), as shown in Figure 5. These results emerge from a highly conservative test, because we only changed 9 of 193 words in the audience attribute cue manipulation in this real-world field experiment, and actual patients used their own email accounts, which provides additional support for H1c.
Consumers with stigmatizing diseases click on a marketing communication more when the message source (1) also possesses a stigmatizing disease (shared audience cue) and (2) provides cues of the benevolent intentions of the potential audience; rather than the same benevolent intention cues associated with an ambiguous audience and shared audiences associated with neutral intentions. We find no effects for consumers with less stigmatizing diseases. These findings provide additional support that the effects we observe are due to consumers’ inferences of audiences’ intentions and not similarity alone. These findings also illustrate a “zero miss” strategy for estimating intentions of anticipated audiences among consumers managing potential stigma in which ambiguity in cues (e.g., ambiguous–benevolent) “trigger vigilance for discrimination” (Major and O’Brien 2005, p. 403). They provide guidance to managers on how to improve responsiveness among consumers managing potential stigmas.
General Discussion
Our studies illustrate a robust interactive effect between a consumer’s potentially stigmatizing attribute and audience cues in marketing communications: certain cues fuel fears of social devaluation, which decreases beneficial consumption (e.g., click-throughs, enrollment intentions, engagement within a wellness program) and increases detrimental consumption (high reward–risk products). These findings point to the need for more nuanced theorizing to explain consumer-marketing concepts that may operate differently among consumers managing potentially stigmatizing personal attributes; as such, they enrich marketing theory on stigma, inform managers, and offer avenues for further research.
Theoretical Contributions
Our findings directly respond to recent calls for marketing research on stigma (e.g., Chaney, Sanchez, and Maimon 2019; Lamberton 2019; Mirabito et al. 2016; Wooten and Rank-Christman 2019). They also contribute to research on power, status, and the judgments of others in the marketplace (Ratner and Hamilton 2015); homophily (McPherson, Smith-Lovin, and Cook 2001) and consumer empowerment; and customer engagement (Harmeling et al. 2017).
Stigma, consumer power, and status
Prior work often focuses on how consumers improve their status and power (e.g., Dion and Borraz 2017) but overlooks the inferior status that stigma can impose on them (Coskuner-Balli and Thompson 2013). By definition, stigma implies an undesirable position as “the other” in a social hierarchy, and power rests with those without the stigma (i.e., the audience). Integrating our findings across studies, we identify a continuum of threat inferences that consumers managing stigmas make, based on the cues available to deduce the power differential between them and a potential audience. This continuum ranges from low threat, shared audience attribute cues to high threat, unshared (ambiguous or contrasting) audience attribute cues. It shows how distinct audience cues might (inadvertently) undermine consumer well-being, and it helps reveal a process by which consumers aim to manage power differentials in the marketplace: they first use stigma-relevant audience cues to infer their status relative to a potential audience and then avoid or approach consumption encounters. This is important for marketers to understand, as marketing communications often deliberately emphasize negative deviations in stigma-related campaigns (see Web Appendix F for examples).
Stigma, inferred audiences, and homophily
Homophily suggests that people tend to seek out those who are “similar” under the assumption of a reciprocal sense of “liking” (McPherson, Smith-Lovin, and Cook 2001). We see some evidence of this, but instead of the expected main effects of audience cues that homophily would predict, we observe an interaction by the stigma potential of a given attribute (e.g., disease, BMI). We find systematic distinctions between consumers who (do not) have a potentially stigmatizing attribute in how they assess similarity and how that affects decision making. Consumers prioritize the potential stigma over other typical sources of similarity (e.g., gender, race) (Studies 2 and 3); notably, the same attribute (e.g., BMI) does not seem to provide a relevant point of similarity when the attribute is not stigmatizing. Thus, we contribute to research on the multidimensionality of homophily (e.g., Block and Grund 2014; Lin and Lundquist 2013) by showing that similarity must be calibrated to a highly prioritized attribute—in this case, the stigmatizing attribute.
We also identify a boundary condition in which mere similarity, even along the prioritized attribute, does not produce the intended effects: in Study 2, we find that a shared attribute cue produces more detrimental consumption than the control condition in which the visual attribute cue was removed, counter to homophily research. This, and the observations in Study 4 in which we separate similarity (i.e., shared attribute cues) and favorability (i.e., benevolent intention cue), suggests an important distinction from homophily. When consumers possess potential stigmas, their primary concern may be to reduce threats rather than maximize benefits, and similarity is just a proxy for assessing potential threats.
Stigma, empowerment, and consumer engagement
Stigmatizing attributes might be a source of empowerment (Corrigan, Kosyluk, and Rüsch 2013; Shih 2004). Findings in Study 3 suggest that empowerment can affect consumption decisions. Study 1 also supports the idea that empowerment triggers downstream effects: we found that consumers with stigmatizing diseases who joined the health program after receiving a marketing communication that featured an ambiguous (vs. shared stigma) audience attribute cue completed 52% fewer engagement behaviors (e.g., likes, posts, comments) in the two weeks after the invitation. Although more research is needed, these initial insights point to stigma-related empowerment as a potential platform for a desirable win-win situation that benefits both stigmatized consumers and firms.
Managerial and Policy Contributions
Explicit descriptions of co-consumers, promotional images, and the message source in marketing communications all can function as audience cues relative to a potential stigma. Therefore, our findings offer direct applications to marketing management and public policy.
Stigma-related marketing and policy communications
Our findings suggest three possible communication strategies for alleviating the negative effects of stigma on consumption. First, as illustrated in Study 2, marketers can attempt to remove audience attribute cues. Even ambiguous audience cues might lead consumers managing stigmas to inferring greater threats, in stark contrast to consumers not managing stigmas, who are likely to use ambiguous cues about co-consumers to infer that an audience will be similar to them (Naylor, Lamberton, and Norton 2011). Second, because audience cues are often unavoidable (e.g., referral programs, group-based offerings), marketers can provide signals that the stigmatizing attribute will be concealed (Study 3). Third, marketers can combine shared audience attribute cues with benevolent audience intention cues (Study 4). This is particularly important because it counters the prevalent use of aspirational images in marketing campaigns, which may inadvertently signal a contrasting audience (Study 2). For example, a Google image search of “templates for gym advertisements” produces 502 images on just the first page, 95% of which feature a physically fit model (see Web Appendix F), which in our studies motivated consumers with BMIs at stigmatizing levels to pursue potentially detrimental treatments that promised to quickly alleviate the stigma. This illustration suggests not only that our findings are nonintuitive, but that managers also should consider carefully which information appears in their marketing communications.
Designing offerings and policies with regard to stigma
Study 3 shows that requesting consumers to reveal their otherwise concealable stigma, even to an audience that is presumably similar to them, can create detrimental effects. This has implications for product and policy design. The more consistently a particular cue is tied to a stigma, the greater the risk that it becomes a stigma marker (Goffman 1963). This insight is crucial for products, consumption practices, and policies designed to reduce or manage stigmatizing attributes, which might get systematically linked to that stigma (Adkins and Ozanne 2005). For example, redeeming coupons or participating in public welfare programs might signal impoverishment, thereby insinuating a stigma of poverty, whether it exists or not. The threat of being assigned a stigma, even if it does not apply, might reduce consumers’ motivation to engage in that consumption (Argo and Main 2008). Marketers should consider the potential for their product to become symbolic of a stigma, its visibility to others, and whether exposing stigmatizing personal attributes is necessary. They might seek to reduce a product’s visibility (e.g., Invisalign for orthodontic issues; Wahl 2005) or minimize its association with the stigma (e.g., birth control pills disguised in cases that look like cosmetic compacts; Gibbs 2010). Alternatively, marketers could use stigma symbols strategically, to signal acceptance in subtle ways that are undetectable by consumers without the stigma (Chaney, Sanchez, and Maimon 2019; Shavitt 2019). Our findings lend support to the idea of having service staff (e.g., health care workers) who possess the same stigma as consumers in a focal program (e.g., HIV patients may prefer programs where some health workers are also HIV positive; www.positiveimpacthealthcenters.org).
Stigma and public policy communications
Our results are relevant for institutions that influence, communicate, and apply public policies related to stigma. These institutions (e.g., CDC, World Health Organization) are particularly legitimizing, and communications emanating from them can quickly influence beliefs of what is “normal” (Humphreys and Latour 2013). This standard is the prerequisite for stigmas to emerge. We see evidence of this in Studies 2 and 3, in which the effects emerge in line with the categories set by the CDC for abnormal BMIs. Therefore, policy institutions might (inadvertently) affect whether and when a stigma emerges. Our research suggests that a requirement of a stigma is an audience that identifies those bearing the stigma as the “other.” Clarifying misconceptions of links between a disease and other categorizations of people (e.g., HIV/sexual orientation, HPV/women) may be an effective means of alleviating people’s assessments of “other” and reducing stigma.
Limitations and Research Directions
Our studies have limitations that point to opportunities for further research. First, Study 1 showed an unexpected positive effect of an ambiguous audience cue among consumers with less stigmatizing diseases. This might imply a U-shaped relationship between stigma and specific targeting (e.g., with no or high stigma, specific targeting is more effective, but with low stigma, generic targeting is more effective); an intriguing idea for further research. Second, Studies 2 and 3 point to another important topic: high-risk consumption by people with a stigmatizing attribute. From a consumer well-being lens, our finding that a single advertising image can nudge stigmatized consumers toward high-risk choices (e.g., surgical procedures) is noteworthy, and more research on such negative implications is needed. Third, Study 4 suggests that service providers are crucial audiences. Research should assess how service employees respond to consumer stigmas. A related path is to investigate what makes a particular piece of information a “stigma marker” for different audiences (e.g., co-consumers, service providers). This notion relates back to managerial decisions about product design and branding (e.g., might “unbranding” a product help reduce a product–stigma association?). Fourth, because stigma inherently entails power, studying how consumers estimate power differentials in new encounters and how it shapes their decision to pursue the encounter is important. 10 Fifth, our studies investigate various forms of ambiguity (e.g., along the focal attribute, unspecified similarity) in which a single cue could produce wide variations in inferences. The degree and nature of ambiguity in audience cues and its impact on consumption decision making warrants further investigation. Sixth, we study consumers who bear a stigma, but others (e.g., their caregivers, family, friends) could be affected by mere association (Argo and Main 2008). These close others may be more acutely aware of discrediting conditions and more sensitive in their responses on behalf of the stigmatized. More research is needed to understand such stigma-by-association. Finally, we narrowed our theory to a single attribute (disease, weight), but people may simultaneously possess multiple potentially stigmatizing attributes, and their interplay indicates a fruitful area for further research. In this context, beyond social devaluation by an audience, self-devaluation by stigmatized consumers also may be relevant.
Supplemental Material
Supplemental Material, sj-pdf-1-mrj-10.1177_0022243720975400 - Marketing, Through the Eyes of the Stigmatized
Supplemental Material, sj-pdf-1-mrj-10.1177_0022243720975400 for Marketing, Through the Eyes of the Stigmatized by Colleen M. Harmeling, Martin Mende, Maura L. Scott and Robert W. Palmatier in Journal of Marketing Research
Footnotes
Associate Editor
Katherine White
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.