
Abstract
Most disability research originates from high-income countries, masking important cultural variability in how disability is conceptualized. Through 199 interviews with people living in Sierra Leone, we investigated the following research questions: (1) What are the experiences of community members with people with disabilities? (2) What employment options or other resources are available for people with disabilities? (3) How do community members perceive people with disabilities? We used a mixed-method approach to data analysis by quantitizing the qualitative responses to further examine whether participants’ responses differed by urbanicity, age, or level of education. The results of this study provide insight into how disability is understood in a low-income country and reveal important directions for future research.
Keywords
Nearly 80% of the one billion people with disabilities worldwide live in low- and middle-income countries (LMICs; World Health Organization, 2011). Despite the heavy concentration of people with disabilities living in these areas, research suggests that the majority of what is known about disabilities comes from high-income countries. For example, Saxena and colleagues (2006) found that among mental health research, 94% of studies came from high-income countries and this trend was stable over a 10-year period. Similarly, in a review of worldwide autism research, Franz and colleagues (2017) found that nearly 80% of the research on autism originated in the United States and Europe, despite less than 15% of the world’s population living there. This clear disparity in disability research is concerning, given that research is linked to capacity building and the provision of evidence-based practices (Durkin et al., 2015).
As intervention research can help remediate the lack of access to vital services and supports experienced by many people with disabilities living in LMICs (Durkin et al., 2015), it stands to reason that an increase in intervention research is needed in these areas. However, conducting cross-cultural disability research can be ineffective, or even detrimental, if it is approached without a culturally responsive framework, meaning that the researcher actively seeks to understand the values and culture of the population being studied (Ford et al., 2008). Although there are many aspects to conducting culturally responsive research, two important considerations are (a) the relevancy of the research problem to the local community members’ interests and needs, and (b) the alignment of the intervention to the participants’ experiences and preferences (Trainor & Bal, 2014). Furthermore, it is important to ensure that any adaptations to interventions designed for use in a different culture incorporate the local cultural group’s values and norms (Clark, 2012). With disability research, this translates to ensuring the researcher has a deep understanding of the local culture’s perception of what it means to have a disability.
Disability is characterized differently in countries around the world, with different definitions of disability available. Although there are different views on disability, two prevailing perspectives are the deficit perspective and the cultural perspective (Bryant et al., 2020). The deficit perspective, also termed the medical model, posits that people with disabilities have inherent weaknesses that are in need of remediation (Kirby, 2017). The deficit perspective is the prevailing view in the United States, as evidenced by the criteria used to diagnose disabilities outlined in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013). A second perspective on disability is the cultural perspective, which states that disability is defined by a culture and that there is no universal definition of disability (Bryant et al., 2020). People engaged in cross-cultural research understand disability as an “evolving concept that is embedded within culture and society . . . and reflects an interaction between a person with an impairment and their environment” (Mckenzie et al., 2013, p. 1751).
The way in which people and cultural groups understand disability affects their interactions with people with disabilities, which in turn impacts the outcomes for people with disabilities (Bryant et al., 2020); therefore, it is critically important to understand how a culture defines disability before attempting to conduct cross-cultural research. In many low-income countries, there is a widespread belief that disabilities are caused by supernatural forces (Hashimi et al., 2020). This belief is shared by many cultural groups, including those living in Indonesia and India, but is especially prevalent throughout sub-Saharan Africa (Mckenzie et al., 2013). Prior research suggests that many African people believe that disabilities are caused by witchcraft or angered spirits, resulting in ostracization and the practice of infanticide in some countries when a child is suspected of having a disability (Koszela, 2013; Rohwerder, 2018). These beliefs have implications for people wishing to conduct disability research in low-income countries as they often lead to barriers to service access and willingness to engage in treatment or interventions (Hashimi et al., 2020).
Despite some prior research on disability perspectives in low-income countries, more research is needed, particularly in West Africa. Much of the previous work on disabilities in sub-Saharan Africa has focused on Nigeria and South Africa, with significantly fewer studies being conducted in other countries. Sierra Leone, in particular, has a paucity of disability research. According to a recent large-scale meta-synthesis of qualitative disability research in West Africa, a mere 11 studies had been conducted in Sierra Leone compared to 212 studies conducted in other West African countries (Blasko et al., in review). What little information is known about disabilities in Sierra Leone often comes from national census data, which are self-report measures, and focuses on quantitative measures of disability, such as frequency, employment rate, and educational attainment (Kabia & Tarawally, 2017). Additional research that does not confine participants to a preselected set of options is needed to determine if the spiritual beliefs on disability, prevalent in many other African countries, also characterize the beliefs of people living in Sierra Leone. Furthermore, additional research on people’s perceptions of disabilities in Sierra Leone will contribute to a deeper understanding of how disability is perceived in different cultures, which may benefit cross-cultural researchers wishing to conduct research in these contexts.
When examining perceptions on disabilities, it is important to use constructs that are familiar to the people being studied. In Sierra Leone, disabilities are often characterized dichotomously, as either physical or mental, with a deeper understanding of physical disabilities. For example, during the 2015 census, physical disabilities were separated into 13 different categories (e.g., polio, amputee, blind, deaf), whereas mental disabilities were included in only three categories (i.e., mental difficulties, psychiatric disability, and other; Kabia & Tarawally, 2017). Part of the reason for this dichotomous characterization of disability stems from Sierra Leone’s history and the social and political policies in place (Sesay, 2020). Sierra Leone was part of a decade-long civil war (1991–2002) that resulted in many people losing limbs and acquiring physical disabilities. Furthermore, the war exacerbated the challenges associated with being a low-income country, namely draining already limited resources and damaging already limited infrastructure (Sesay, 2020). In addition, postwar policy has focused more on physical impairment and trauma, and there is a significant lack of support for, and focus on, mental disabilities. For example, despite having a population of more than 7 million people, Sierra Leone only has one psychiatric hospital and two psychiatrists in the entire country (Harris et al., 2020). This disparity in access to mental health care likely contributes to the limited understanding of different disability types and may lead to distinct views and beliefs about these two categories of disabilities. As such, this study sought to investigate beliefs and perceptions about disabilities using the broader categories of mental and physical disabilities.
This study also sought to examine differences in perceptions of disabilities between community members from rural and urban areas as previous studies have indicated that actions taken toward individuals with disabilities may vary depending on the area where the people live. For example, children born with impairments in rural areas in Guinea, Niger, Sierra Leone, and Togo were more likely to be ritually killed than those born in cities (Njelesani, 2019), which the authors posited may be due to ritual killings being more likely to be detected by officials when they occurred in or around cities. Furthermore, previous studies have indicated that beliefs about disabilities, particularly mental disabilities, vary immensely between urban and rural areas (Alem et al., 2008; Monteiro & Balogun, 2013). Currently, there is a lack of knowledge about perceptions and beliefs of disabilities in all areas of Sierra Leone. Therefore, this study recruited respondents from several urban and rural settings to gain a more holistic view of how people perceive disabilities and to examine how these perceptions may differ based on location.
The purpose of this study was twofold: (1) to understand the perspectives of Sierra Leoneans regarding physical and mental disabilities in the community and (2) to understand what supports or resources are available for people with disabilities living in Sierra Leone. Furthermore, we aimed to determine whether people’s responses differed by urbanicity, education, or age. Gaining a deeper understanding of how disability is conceptualized in Sierra Leone facilitates cross-cultural intervention research by informing researchers of the beliefs of a culture. This information can then be used to design more effective, sustainable interventions that overcome the cultural barriers in place. By designing or adapting existing interventions based on a culture’s beliefs and values, researchers can increase the likelihood that their research will be sustained and ultimately lead to an improvement in the quality of life of people with disabilities by reducing stigma. Specifically, the research questions that guided our study included:
Method
To gain an understanding of the perspectives of Sierra Leoneans regarding disability, interviewers traveled to Sierra Leone and asked community members living in rural and urban areas of Sierra Leone 11 questions encompassing three broad themes: (a) experience with people with disabilities, (b) resources and employment options for people with disabilities, and (c) perceptions about people with disabilities. To answer our first research question and gain an understanding of the first theme, experiences with people with disabilities, interviewers asked community members the following questions: (a) Do you know someone with a physical disability, (b) Do you know someone with a mental disability, (c) What are some common disabilities in the community, and (d) How did you learn about disabilities? To answer our second research question and address the second theme, resources and employment options for people with disabilities, interviewers asked the following questions: (a) What are some treatments for people with disabilities, (b) What are some resources for people with disabilities, and (c) Do you know anyone with a disability who has a job? To answer our final research question and learn about our third theme, interviewers asked the following questions: (a) What are some causes of physical disabilities, (b) What are some causes of mental disabilities, (c) How do you feel interacting with people with disabilities, and (d) Do people with disabilities deserve their disability? In addition to these questions, interviewers also gathered the following demographic data: urbanicity, education, age, and sex.
Respondents
A total of 199 Sierra Leoneans participated in this study. Of these, 120 respondents (60%) were male and 79 respondents (40%) were female. The average age of the respondents was 40 years old, with a range of 18 years old to 85 years old (19% ages 18–24, 55% ages 25–49, 26% ages 50+). Most respondents had some form of education; however, a large number reported not having any formal education (n = 58; 29%). Of those who reported some form of education, 24 respondents had a primary school education only (i.e., typically attended between the ages of 6–12 years old; 12%), 50 respondents had a junior secondary school education (i.e., typically attended between the ages of 12–15 years old; 25%), 18 respondents had a senior secondary school education (i.e., typically attended between the ages of 15–18 years old; 9%), 42 respondents had a college education (21%), six respondents reported attending an Arabic school (3%), and one person reported attending a technical training school (0.5%). The respondents were fairly evenly divided between urban (n = 96; 48%) and rural (n = 103; 52%) areas.
According to the latest census report, Sierra Leone had a total population of 7,092,113 people (Statistics Sierra Leone, 2017). Of this, approximately 51% of the population is female and 49% male. Sierra Leone has a very young population, with nearly 41% of the population between birth and 14 years old, 22% between 15 and 24 years old, 25% between 25 and 49 years old, and 12% 50 years old and older. A total of 59% of the population lives in rural areas, whereas 41% lives in urban areas. Among employed individuals ages 15 years old and older, approximately 64% of the population reported no formal education, 21% reported their highest level of education as basic school (i.e., primary and junior secondary school), 9% as senior secondary school, 3% as vocational/technical/nursing/teaching school, and 3% as college. There were notable differences in educational attainment between males (56% reported no formal education) and females (72% reported no formal education), as well as for those living in rural areas (77% reported no formal education) versus urban areas (23% reported no formal education).
Procedure
When developing the questions in the interview protocol, research team members conducted a review of the literature to determine what knowledge gaps existed and developed a set of initial questions based on this review. Team members then distributed these initial questions to experts in the field and local community members in Sierra Leone to gain feedback and establish content validity. Team members revised the protocol based on expert review and used cognitive interviewing techniques to further refine the protocol (Peterson et al., 2017).
Research team members trained in interviewing techniques traveled to Sierra Leone and used the finalized protocol to conduct the interviews using convenience sampling. More specifically, local interpreters accompanied interviewers and suggested rural villages and one city in the Northern Province of Sierra Leone (Bombali District) in which to conduct the interviews. Interviewers and the interpreter traveled door-to-door to collect data. All interviews were audio recorded for later transcription and lasted approximately 15 to 30 min. The interviews followed a semistructured format (Galleta, 2013), meaning that interviewers allowed for a free-flowing conversation and took notes on ideas or thoughts that the respondents brought up that were not part of the original questions.
Design and Data Analysis
To answer our research questions, we employed a mixed-methods research design. Mixed-methods research is traditionally grounded in pragmatism, meaning that quantitative and qualitative methods may be used in different combinations, depending on what is needed to best answer the research questions (Corr et al., 2021). Owing to this pragmatic approach, it is ideally suited for special education research (Klinger & Boardman, 2011). A defining feature of mixed-methods research is data integration, or the meaningful combination of multiple methods during data collection, data analysis, and/or interpretation of the results (Corr et al., 2021). In this study, we integrated qualitative and quantitative methods during data analysis by quantitizing the qualitative interview responses into quantitative data for use in quantitative analyses. Quantitizing data involves assigning numerical values to textual responses and is a hallmark of mixed-methods research (Creamer, 2017; Sandelowski et al., 2009). By quantifying our qualitative data, we were able to gain additional insight into our data by determining whether there were statistically significant differences between respondents’ answers based on age, urbanicity, and education level.
Research team members transcribed the interview data and provided the transcript to the local community members who acted as interpreters to ensure the accuracy of the transcription. To analyze the data, research team members organized responses by question in Microsoft Excel and used an iterative process that involved identifying themes in responses both within and across questions (Galleta, 2013). We used a three-stage approach to coding, aligned with grounded theory, with codes developed inductively. More specifically, we began with an open-coding stage where we created broad codes for each response based on overall themes in the data. During this stage, we also included an “other” category where we noted responses of interest that did not fit with our initial codes. Next, we used axial coding where we grouped initial related codes, deleted irrelevant codes, and added additional codes based on responses in the “other” category. We conducted a final round of qualitative coding where all responses were recoded based on the new categories. Throughout the coding process, the first author met weekly with research team members and regularly reviewed codes to establish consistency in coding (Carter et al., 2014). Once all responses were coded qualitatively, they were quantitized and recoded a final time for use in quantitative analyses. Specifically, experiences with disabilities answers were coded into dichotomous responses (1 = Yes, 0 = No) for use in regression analyses. We also recoded education to include three categories (none, primary/secondary, and college) and age to include two categories (<30 and >30 years of age). We used both descriptive statistics and logistic regression for the quantitative analyses. For a list of codes with examples of responses that were applied to each code, please see the online supplemental materials.
Results
Experiences With People With Disabilities
Disabilities are common in Sierra Leone, especially in rural settings, with most people knowing at least one person with a disability; however, there are cultural differences in how disability is understood. Although schools were cited less frequently than other ways of learning about disabilities, the results of statistical analyses suggest that some groups of people benefit from school as a source of information more than others.
Do you know someone with a physical or mental disability?
A total of 135 people responded to the question related to physical disability and 121 people responded to the question related to mental disability (see the online supplemental materials). The remaining respondents declined to answer these questions. Of the people who responded, most people did know someone with a physical or a mental disability; however, more people knew someone with a physical disability (83%) than a mental disability (69%).
Logistic regressions were performed to examine whether there were differences in responses for physical disability and mental disability by age, education level, and urbanicity. For physical disability, the logistic regression was statistically significant, χ2(4) = 11.00, p = .03. The model explained 13.5% (Nagelkerke R2) of variance in knowing someone with a physical disability and correctly classified 82% of responses. Urbanicity was the only significant predictor of knowing someone with a physical disability. Individuals in rural settings were 7.43 times more likely to know someone with a physical disability than individuals in urban settings, B = 2.01, SE = .77, p = .01. For mental disability, the logistic regression was statistically significant, χ2(4) = 28.42, p < .001. The model explained 31.3% (Nagelkerke R2) of variance in knowing someone with a mental disability and correctly classified 68% of responses. Urbanicity was the only significant predictor of knowing someone with a mental disability. Individuals in rural settings were 33.1 times more likely to know someone with a mental disability than individuals in urban settings, B = 3.58, SE = 1.05, p = .001.
What are some common disabilities in the community?
Respondents were asked to identify common disabilities found within their community to determine which types of disabilities are prevalent within Sierra Leone. A total of 171 people responded to this question (see the online supplemental materials). Of the individuals who gave examples of disabilities present within the community, the most common disabilities cited were (a) vision, hearing, and speech impairments (78%), and (b) physical disabilities, such as a stroke, handicap limitations, or paralysis (75%). Psychological disorders such as “madness,” “mental disability,” and “abnormal behavior” were also frequently cited as common disabilities (64%), with many people using terms such as “crazy” and “lunatic” to describe people with these conditions. Notably, diseases (e.g., malaria, typhoid, gonorrhea, Ebola, leprosy) and acute illnesses (e.g., chicken pox, rash, cough, fever, headaches) were cited as disabilities by more than half of the respondents who responded to this question (54%), indicating a different cultural understanding of what constitutes a disability. Less commonly cited disabilities were neurological or intellectual disabilities, such as epilepsy or Down syndrome (33%), with the majority of respondents specifically citing epilepsy (26%; n = 51).
When analyzing responses by age, education, and urbanicity, overall logistic regression models were not statistically significant (see Table 1). Education was a significant predictor in physical disabilities, psychological disabilities, and disease. Respondents with secondary/postsecondary education were 50% less likely to report psychological disabilities as disabilities commonly found in the community than respondents with no formal education. Respondents with a college education were 172% more likely to report physical disabilities and 66% less likely to report disease as disabilities commonly found in the community than respondents with no formal education.
Summary of Logistic Regression Analyses for Age, Urbanicity, and Education Predicting Types of Common Disabilities Reported in the Community.
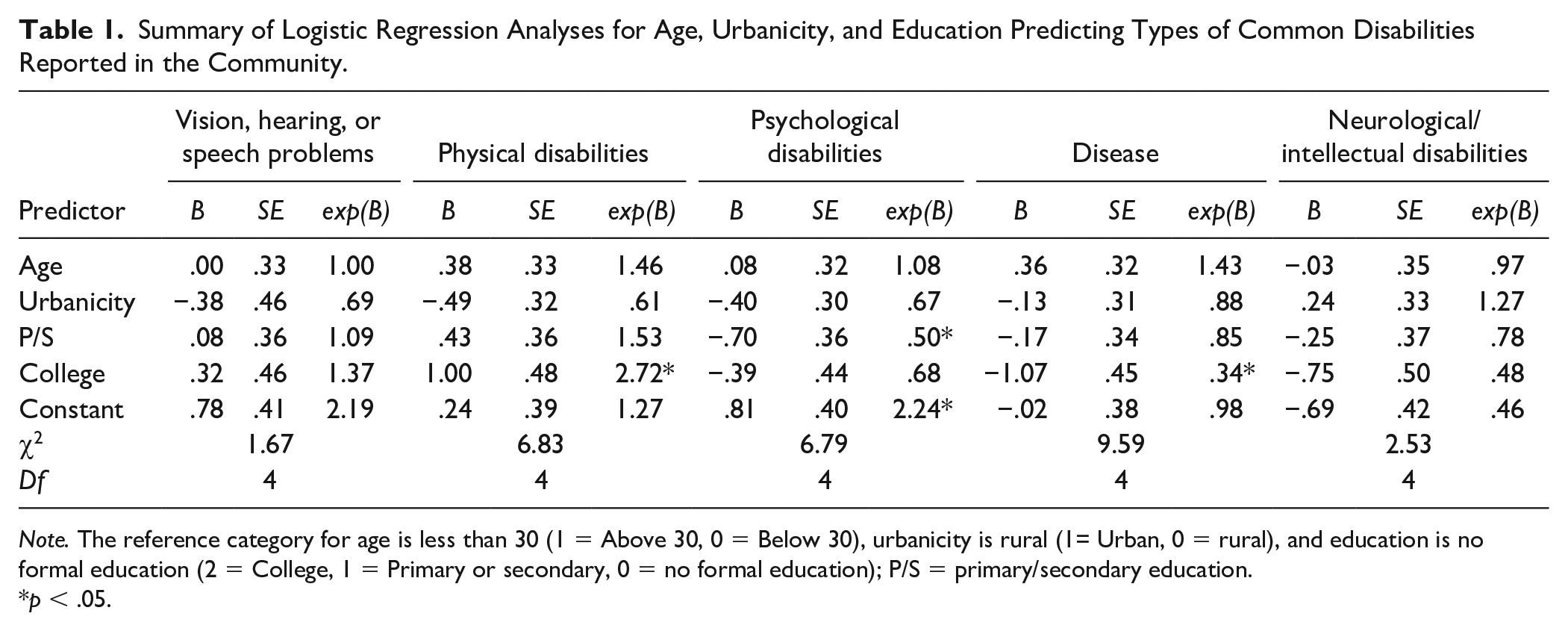
Note. The reference category for age is less than 30 (1 = Above 30, 0 = Below 30), urbanicity is rural (1= Urban, 0 = rural), and education is no formal education (2 = College, 1 = Primary or secondary, 0 = no formal education); P/S = primary/secondary education.
p < .05.
How did you learn about disabilities?
To determine how information regarding disabilities is disseminated within various communities in Sierra Leone, respondents were asked to recall how they learned about disabilities. A total of 132 people responded to this question. Of the people who answered this question, a large percentage cited personal experience (45%) or the community (44%) as a means of learning about disabilities. Notably, nearly one in five respondents also indicated that they learned of various disabilities in a school setting (18%). Less common methods of learning about people with disabilities were through (a) hospitals or community health workers (8%), trainings or workshops (7%), and the media (5%).
Logistic analyses were performed to examine responses by age, urbanicity, and education level. The overall logistic regression model was significant for citing schools as a source for learning about disabilities, χ2(4) = 43.8, p < .001. The model explained 38.8% (Nagelkerke R2) of variance in citing school as a source for learning about disabilities and correctly classified 91% of responses. Age, urbanicity, and education were significant predictors of school. Respondents over the age of 30 were 77% less likely to report learning about disabilities in school than those ages 18–30, B = −1.48, SE = .57, p = .01. Urban respondents were 4.27 times more likely than rural respondents to report learning about disabilities in schools, B = 1.45 SE = .62, p = .02. College-educated respondents were 19.03 times more likely than respondents with no formal education to report learning about disabilities in schools, B = 2.95, SE = 1.09, p = .01. The overall logistic regression model for hospitals was statistically significant, χ2(4) = 16.60, p = .002. The model explained 23.4% (Nagelkerke R2) of variance in learning about disabilities from a hospital or from community health workers and correctly classified 94% of responses. However, no individual predictors were statistically significant. There were no statistically significant logistic regression models for personal experiences, community, training or workshops, or through TV, media, and radio. Although the overall logistic regression was not significant, age was a significant predictor of citing community as a source for learning about disabilities. Respondents over the age of 30 were 52% less likely to report learning about disabilities in the community than those ages 18–30, B = −.74, SE = 3.4, p = .3.
Employment Options and Available Resources
Medical and cultural treatments were both commonly cited as possible treatments for people with disabilities, especially among people living in rural communities; however, the specific treatment suggested differed based on the person’s disability type. Although medical resources were commonly cited as available to people with disabilities, there may be barriers to access, especially among people living in rural communities. Unfortunately, most people did not know anyone with a disability who had a job, but participants’ responses to this question did differ based on urbanicity and education level.
What are some treatments for people with disabilities?
A total of 149 people responded to this question. Of those who responded, most people cited medical treatments as available to people with disabilities (69%); however, more than half also responded that cultural or traditional treatments, such as those provided by herbalists or traditional healers, were available as possible treatments (54%). Notably, approximately one in six people reported not knowing any treatments for people with disabilities (17%). Less commonly reported were community or family supports as possible “treatments” for people with disabilities (9%).
Logistic analyses were performed to examine differences among responses by age, urbanicity, and education. The overall logistic regression model was significant for citing medical treatments as available to people with disabilities, χ2(4) = 12.9, p = .02. The model explained 8.3% (Nagelkerke R2) of variance and correctly classified 63% of responses. Urbanicity was the only significant predictor. Urban respondents were 64% less likely than rural respondents to report medical treatments as available to people with disabilities, B = −1.02, SE = .31, p = .001. The overall logistic regression model was significant for citing cultural or traditional treatments as available treatments, χ2(4) = 23.2, p < .001. The model explained 15.5% (Nagelkerke R2) of variance and correctly classified 65% of responses. Urbanicity was the only significant predictor. Urban respondents were 75% less likely than rural respondents to report medical treatments as available to people with disabilities, B = −1.39, SE = .32, p <.001. There were no differences by age, urbanicity, or education level for family support.
When examining participants’ textual responses, community members often differentiated between treatments available to people with physical versus mental disabilities, stating that hospitals were a possible treatment for people with physical disabilities, whereas the “cultural way” or the “mental doctor” was a possible treatment for people with mental disabilities. Some community members elaborated on common cultural treatments, describing herbalists who boiled herbs into a tea and gave it to people with disabilities to drink. Although some people expressed confidence in cultural treatments, stating that they worked at least some of the time, most people indicated that they were ineffective and that “curing mental is impossible.” In addition to differences in treatments for people with disabilities, there were also disparities in access. Although medical resources and treatments were frequently cited as being available to people with disabilities, many people elaborated on this response by clarifying that this option was expensive and that many people could not afford it. In addition, people in rural communities commented that the hospitals and other medical resources or treatments were far away, thus serving as a barrier to access.
What are some resources for people with disabilities?
Respondents were asked whether they knew of any resources for people with disabilities. Out of 199 respondents, 151 individuals responded to the question. Of the people who responded to the question, the most commonly cited was medical resources, such as hospitals, clinics, doctors, community health workers, or crutches and wheelchairs (49%); however, a large percentage of people reported not knowing of any existing resources or cited a lack of available resources for people with disabilities (39%). Other prominent responses were community and family resources, such as local and household support, nonprofits and civil society, state resources, and disability specific schools and centers (30%). Less-frequently cited responses were cultural and traditional resources (10%). Interestingly, eight people mentioned that begging was a resource or source of support for people with disabilities.
Logistic analyses were performed to examine differences among responses by age, urbanicity, and education. The overall logistic regression model was statistically significant for respondents selecting no resources available, χ2(4) = 19.50, p = .001. The model explained 13.8% (Nagelkerke R2) of variance in stating that there are no available resources for individuals with disabilities and correctly classified 73.2% of responses. Urbanicity and age were significant predictors. Urban respondents were 52% less likely to indicate there were no resources available for those with disabilities than individuals from rural communities, B = −.74, SE = .35, p = .04. Individuals above the age of 30 were 66% less likely to indicate there were no resources available for those with disabilities than individuals under the age of 30, B = −1.08, SE = .35, p = .002. There were no statistically significant predictors of medical resources, community/family support, or traditional/cultural support.
Do you know any people with disabilities who have jobs?
A total of 136 people responded to this question. Of those who responded, the majority of people did not know of any people with disabilities who had a job (58%). The overall logistic regression model examining age, urbanicity, and education was significant, χ2(4) = 16.71, p = .002. The model explained 16.3% (Nagelkerke R2) of variance in knowing people with disabilities who have jobs and correctly classified 67% of responses. Urbanicity and education were significant predictors. Urban respondents were 2.67 times more likely than rural respondents to report knowing someone with a disability with a job, B = .98, SE = .41, p = .02. Respondents with postsecondary school education were 68% less likely than respondents with no formal education to report knowing someone with a job, B = −1.15, SE = .50, p = .02. College-educated respondents were 89% times less likely than respondents with no formal education to report knowing someone with a job, B = −2.19, SE = .62, p < .001.
Several respondents gave examples of disabilities that they believed could work and those they believed should not work, although there was some discrepancy in their responses. Although most people who provided examples believed that people who were blind could work (n = 13), three respondents believed they could not work. More people (n = 7) also believed people with polio could work; however, two respondents disagreed and said people with polio should not work. Additional discrepancies occurred related to epilepsy and people with amputations. A few respondents mentioned that people with leprosy or minor disabilities such as broken bones could work, while other respondents believed people who were paralyzed or severely disabled could not, or should not, work. A final follow-up question was answered by some of the respondents (n = 84), where they listed jobs that people with disabilities can do, and 48% of jobs that were listed required no formal training (petty jobs, office jobs, shop workers, and trading) compared to 31% that required on the job training (blacksmith, carpentry, mechanical work, and construction) and 21% that required formal education (teaching and medical work).
Perceptions of People With Disabilities
Overall, most respondents reported feeling uncomfortable interacting with people with disabilities but did not believe people deserved their disability. Furthermore, multiple causes of disabilities were suggested. However, for each of these responses, qualitative differences were found in respondents’ answers, depending on whether they were referring to someone with a physical or mental disability. In addition, statistically significant differences were found for responses to most questions based on participants’ age, urbanicity, and/or education level.
What are some causes of physical disabilities?
A total of 164 people responded to this question. Of the people who responded, the most commonly cited causes were disease or illness (51%), such as fever, polio, malaria, high blood pressure, and measles; however, accidents were also cited by nearly half of the respondents (49%). Hereditary causes (e.g., “they were born with it”) was cited as a cause of physical disabilities by nearly one in three respondents (35%), as were spiritual or cultural causes (e.g., witchcraft or “cultural mischiefs”; 32%). More than one in five people attributed the cause of physical disabilities to issues related to being in poverty, such as lack of access to clean water, scarcity of food, and lack of money for, or access to, medical care (23%). Less commonly cited causes of physical disabilities were drugs or alcohol (4%) and psychological causes, such as stress or family conflict (2%).
When comparing responses across respondents, differences were found only for poverty-related causes across age, urbanicity, and education level. The overall logistic regression model for poverty-related causes was statistically significant, χ2(4) = 16.82, p =.002. The model explained 13.8% (Nagelkerke R2) of variance and correctly classified 81.6% of responses. Urbanicity was the only significant predictor. Urban respondents were 72% less likely to report poverty-related causes of disability than rural respondents, B = −1.27, SE = .44, p = .003. There were no significant differences in responses for hereditary, drugs or alcohol, accidents or unintentional injuries, disease, spiritual, or psychological causes of physical disability across age, urbanicity, and education level.
What are some causes of mental disabilities?
A total of 125 people responded to this question. Of those who responded, spiritual or cultural causes (e.g., “devils,” God, witchcraft, “cultural methods,” punishment for stealing or “misbehavior”) were the predominant response, with nearly half of all respondents attributing mental disabilities to this cause (49%). Drugs or alcohol were also cited frequently as causes of mental disabilities (42%). More than one in five respondents cited the following as causes of mental disabilities: hereditary (28%), psychological (e.g., frustration, stress, family conflict, and disappointment; 22%), and disease/illness (21%). Less frequently cited as causes of mental disabilities were poverty-related (11%) and accidents (10%).
The overall logistic model for drugs or alcohol was statistically significant, χ2(4) = 19.70, p = .001. The model explained 14.4% (Nagelkerke R2) of variance and correctly classified 76% of responses. Age, urbanicity, and education were significant predictors of citing drugs or alcohol as a cause of mental disabilities. Individuals older than 30 were 2.35 times more likely to report drugs or alcohol as a cause than individuals 30 and younger, B = .86, SE = .40, p = .03. Urban respondents were 2.62 times more likely to report drugs or alcohol as a cause than rural individuals, B = .96, SE = .36, p = .008. College-educated individuals were 3.56 times more likely to report drugs or alcohol as a cause than those with no formal education, B = 1.28, SE = .49, p = .01. The overall logistic model for psychological causes was statistically significant, χ2(4) = 11.07, p = .03. The model explained 10.5% (Nagelkerke R2) of variance and correctly classified 87% of responses. Urbanicity was the only significant predictor. Urban respondents were 3.68 times more likely to report mental trauma causes of disability than rural respondents, B = 1.30, SE = .51, p = .01. There were no significant differences in responses for hereditary, poverty related, accidents or unintentional injuries, disease, or spiritual causes of mental disability across age, urbanicity, and education level.
Overarching themes across responses to questions related to causes of disability
Community members were much more likely to attribute physical disabilities to heredity, accidents, or disease/illness, whereas mental disabilities were more likely to be attributed to psychological causes or drugs/alcohol. Spiritual or cultural causes were cited at approximately the same frequency for both mental and physical disabilities, supporting the belief that disabilities are caused by spiritual forces. When examining community members’ textual responses, there was a common theme of retaliation through curses as a cause of disability. For example, one person mentioned, “If you steal, the victim will impose madness on you.” Another person elaborated by stating that “punishment is imposed by others through magical actions.” This theme of disability as a result of wrongdoing is pervasive and not limited to mental disabilities, although it was more prevalent among this disability category. Elephantiasis was frequently cited as a type of physical disability as it causes swelling or enlargement of the legs, arms, or genitalia. Despite being caused by a parasitic worm that enters the body through a mosquito bite, one respondent attributed it to stepping on a spell cast by an enemy. Furthermore, multiple community members attributed the cause of deafness to an infant getting breast milk in their ear.
Another interesting result was found when comparing those that declined to respond: 39.1% of all primary and secondary educated, 29.3% of uneducated, and 16.7% of college-educated respondents declined to provide a possible cause for mental disabilities, signifying a stronger confidence in knowledge surrounding disability among people with more education. The 32 respondents who declined to respond or did not know of a cause of physical disabilities pales in comparison to the 71 who declined to respond or did not know the cause of mental disabilities, indicating a knowledge gap when it comes to physical versus mental disability.
How do you feel interacting with people with disabilities?
A total of 160 people responded to this question. Of those who responded, most people indicated they felt bad or uncomfortable when interacting with people with disabilities (44%); however, more than one in three people indicated they felt good or comfortable around people with disabilities (36%). Approximately one in five people indicated they felt the following emotions when interacting with people with disabilities: fear (20%), pity or sadness (18%), and sympathy or empathy (18%). Interestingly, more than one-third of respondents (35%) indicated they felt differently depending on whether the person had a mental or physical disability, with most people feeling good or comfortable around people with physical disabilities as opposed to mental disabilities. The overwhelming majority of people who indicated they were fearful of people with disabilities were referring to people with mental disabilities, with many people making comments such as “the mentally disabled are dangerous” and “mental (people) can kill” (see the online supplemental materials). Although there was a general theme of feeling more comfortable around people with physical disabilities as opposed to mental disabilities, many community members did not feel comfortable around anyone with a disability, with one person mentioning that “disabilities are transferred by interaction.”
The overall logistic regression model was statistically significant for individuals reporting feeling good or comfortable around individuals with disabilities, χ2(4) = 11.61, p = .03. The model explained 8.2% (Nagelkerke R2) of variance and correctly classified 72% of responses. Urbanicity was the only significant predictor. Urban respondents were 2.39 times more likely to report feeling comfortable than rural respondents, B = .87, SE = .34, p = .01. The overall logistic regression model was statistically significant for individuals reporting discomfort or bad around individuals with disabilities, χ2(4) = 10.78, p = .03. The model explained 7.6% (Nagelkerke R2) of variance and correctly classified 64% of responses. Education was the only significant predictor. College-educated respondents were 67% less likely to report feeling discomfort or bad around people with disabilities than those with no formal education, B = −1.12, SE = .50, p = .03. There were no significant differences for feelings of sympathy or empathy, pity, or fear by age, urbanicity, or education level.
Do people with disabilities deserve their disability?
Over half of the respondents (n = 111) did not feel comfortable responding to this question, and an additional two respondents provided answers that were uninterpretable (i.e., “Some don’t share knowledge of disabilities”; “Only God knows why”). Of those who respond to this question, only two believed that people with disabilities deserved them. An additional 33 respondents (38%) believed that some people with disabilities deserved their disability but not others; however, the majority of respondents (59%) believed that people with disabilities did not deserve their disability. Of those who believed some deserved their disability but not others, the majority (i.e., 70%) believed that people who engaged in socially unacceptable behaviors deserved their disability (e.g., drugs, alcohol, crime, or misbehavior), and nearly one-third of respondents (i.e., 30%) believed that people with physical disabilities did not deserve them but people with mental disabilities did. This response is reflective of community members’ perceived causes of disabilities as physical disabilities were often attributed to causes beyond the person’s control (e.g., heredity, accidents, disease/illness) whereas mental disabilities were frequently attributed to causes within the person’s control, such as using drugs or alcohol, fighting (i.e., psychological causes), or failing to follow cultural norms and societal laws (i.e., spiritual/cultural causes). When analyzing responses across age, urbanicity, and education, there were no statistically significant differences.
Discussion
As a result of interviewing nearly 200 community members living in Sierra Leone, we gained insight into the perceptions of disability. Specifically, we learned there are many differences in how disability is conceptualized in Sierra Leone as compared to high-income countries, such as the United States, and that these differences are consistent with the way disability is conceptualized in many other low-income countries (Hashimi et al., 2020). The findings from this study have several implications. First, it is critically important to spread awareness of the true causes of disability. As long as the community believes that disability is caused by spiritual forces or a perceived wrongdoing by the person with a disability, people with disabilities will continue to be stigmatized and have a poor quality of life. These beliefs also negatively affect researchers’ ability to conduct effective intervention research as previous research has demonstrated that cultural beliefs about spiritual causes of disability present barriers to health care and intervention access (Hashimi et al., 2020). Cross-cultural researchers wishing to conduct research in low-income countries where beliefs about spiritual causes of disability prevail will need to incorporate a knowledge dissemination plan into their protocol. Failing to do so will likely result in barriers that reduce the effectiveness or sustainability of the research.
To ensure knowledge dissemination efforts are effective, it is imperative that they match cultural norms. When asked how they learned about disabilities, most people responded that they learned about them through personal interactions or from seeing people with disabilities in the community. Sierra Leone, similar to other countries in West Africa, has a very social, communal culture. As such, the most effective way to spread information is likely by training local leaders who can then share information with other community members. This is, in fact, the strategy that was used to spread information about Ebola during the 2013 outbreak, effectively ending the outbreak (Gillespie et al., 2016). A similar approach is likely to be effective at spreading awareness of disabilities and ending the stigma surrounding them. An important consideration, however, is who should be trained and the format of the training. Nearly one in five people responded that they learned about disabilities in schools, indicating that this could be an effective mode of dissemination.
Although few people indicated they learned about disabilities through trainings or workshops, hospitals/community health workers, or the media, this does not necessarily mean they are ineffective. Rather, it could be an indication that no one has attempted to spread knowledge of disabilities through these modes because no one had the knowledge of disabilities to spread. Currently, there is only one psychiatric hospital and two psychiatrists in the entire country (Harris et al., 2020). This scarcity of professionals with specialized knowledge of disabilities is likely a significant contributing factor to the misinformation surrounding disabilities. However, it is important to note that people in rural communities rarely have access to smartphones or media, such as televisions or radios. In addition, in community members’ textual responses, many indicated that hospitals were inaccessible due to prohibitive costs and lack of transportation. As such, dissemination through these modes may be limited. Future research should examine the most effective methods of dissemination to reach the widest audience possible.
One way that knowledge of disabilities can be disseminated on a larger scale is through regular screening. Currently, there is not a way to screen or diagnose developmental disabilities, such as autism spectrum disorder, and the screeners we use in the United States are not culturally appropriate and may produce invalid results (Bauer et al., in press). As such, community members are unaware of these disabilities. If children were screened at an early age, then parents and others would come to realize that behavioral characteristics, such as restrictive and repetitive behavior and deficits in social communication, were due to a disability with a medical cause as opposed to a spiritual one. Future research should focus efforts on developing culturally appropriate screeners for developmental disabilities to spread awareness of the characteristics of these disabilities and combat misinformation. Similar knowledge dissemination efforts have been effective for combating misinformation about epilepsy. Epilepsy is a seizure disorder that also used to be thought to have spiritual causes and was not well known in low-income countries (Diop et al., 2003). As a result of efforts, such as the Global Campaign against Epilepsy (Diop et al., 2003), people living in low-income countries are now more knowledgeable about this disability. For example, prevalence studies have demonstrated prevalence rates of .02% to 5.8% for epilepsy in developing countries (Diop et al., 2003). Despite this low prevalence, more than one in four people in our sample specifically named epilepsy as a disability, indicating that knowledge dissemination efforts were effective. This finding is even more significant, given that the only other types of disabilities that community members in this study were able to name were ones related to physical disability or disease. It stands to reason that similar knowledge dissemination efforts will be effective at spreading awareness of specific developmental disabilities and mental health disorders.
Finally, efforts should be made to bolster resources and supports for people with disabilities. Knowledge dissemination may help to promote acceptance for people with disabilities, but without resulting supports in place, it is unlikely that people with disabilities’ situations will improve. Many community members indicated that people with disabilities did not have any treatments or resources available to them, with begging as the only source of support being a common theme. Despite community support being cited frequently as a resource for people with disabilities, examining individuals’ textual responses reveal that there is no system in place for this support, leading to a lack of consistency. As one person mentioned, “The community shares what they have when they are able to—when stuff comes in or there is excess.” Given that Sierra Leone is a low-income country, with the majority of the population living on less than $1.50 per day (World Bank, 2019), it is probably safe to assume that there is rarely ever an excess. Partnering with existing local organizations, such as World Hope International, the Sierra Leone Autistic Society, the St. Joseph’s School for the Hearing Impaired, and the Browne-Penn Special Education School, in an effort to strengthen and expand existing services is likely the best way to effect lasting change.
Limitations
There are several limitations to this study that should be considered when interpreting the results. First, despite our efforts to establish the content validity of the interview questions, it is possible that some community members may not have understood the questions as we intended. Similarly, because we used an interpreter for the interview, it is possible that the questions or the participants’ responses were not translated exactly as stated. Second, we used convenience sampling to obtain participants for the interviews, which can sometimes lead to bias and may have contributed to over- or under-representation of participants with certain demographics in our sample. Finally, our entire sample came from the Northern Province of Sierra Leone, which has the largest percentage of people with disabilities in the country (35% in the Northern Province, 24% in the Southern Province, 28% in the Eastern Province, and 13% in the Western Province; Statistics Sierra Leone, 2017). As such, it is possible that the results reported in this study are not representative of all individuals living in Sierra Leone.
Conclusions
Through this study, we sought to gain insight into the perspectives of community members living in Sierra Leone regarding physical and mental disabilities and to understand what supports and resources are available for people living with disabilities. Through nearly 200 interviews, we were able to gain a better understanding into how disability is perceived by individuals living in a low-income country. These results were consistent with prior research on perceptions of disabilities in other low-income countries and provide important information for cross-cultural researchers wishing to conduct intervention research in these areas. They also highlight the need to disseminate accurate information to reduce barriers to service access and eliminate stigma toward people with disabilities, particularly those with mental disabilities. By understanding how disability is conceptualized and perceived by people in other parts of the world, researchers are better positioned to design and implement intervention studies and knowledge dissemination plans that are meaningful, overcome cultural barriers, and produce lasting change.
Supplemental Material
sj-docx-1-sed-10.1177_00224669211065051 – Supplemental material for Perspectives on Disabilities in Sierra Leone
Supplemental material, sj-docx-1-sed-10.1177_00224669211065051 for Perspectives on Disabilities in Sierra Leone by Kristi L. Morin, Brianne R. Tomaszewski, Kathleen Bauer, Alyssa M. Blasko, Grace B. Enriquez, Emily J. Tasik and Khanjan Mehta in The Journal of Special Education
Footnotes
Acknowledgements
The authors would like to thank Emma Hebert, William Ferguson, Spencer McCullough, Margaret Chan, Arsen Drobakha, and Sarah Ritter for their work on developing the interview protocols and conducting the interviews in Sierra Leone. This work was not possible without the support of World Hope International, a nonprofit organization that has been working in Sierra Leone for the last 20+ years and has developed very strong community relationships across the country.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by an Inquiry to Impact Project Initiation grant from the Office of Creative Inquiry at Lehigh University.
Supplemental Material
Supplemental material is available on the Journal of Special Education webpage with the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.