
Abstract
Magnesium regulates myocardial depolarisation, vascular tone, neuromuscular function and provides analgesia. This study examined its analgesic and haemodynamic effects, comparing the effects of intravenous saline 0.9% (NaCl; control n = 8) and magnesium (n = 7) infusions in minipigs undergoing thoracotomy. Preoperative single-housed activity was recorded for 1 h. Intraoperatively, arterial blood pressure (BP) and heart rate (HR) were recorded once telemetry was established; data from the final 60 min of anaesthesia were compared between groups. Postoperative activity, HR and BP were recorded continuously using in-pen CCTV and telemetry, respectively. Indicators of pain, including HR and BP were sampled after tracheal extubation (TTE) at +0.5, +2.5, +4.5, +6, +8.5, +15.5, +17.5, +19.5, +20, +23, +25.5, +26 and +29 h. Changes in HR and BP before and after analgesia at TTE +6, +17.5, +23 and +29 h, and pre- and post-pain assessments at TTE +2.5, +6, +17.5, +20, +23, +26 and +29 h were compared using a paired t-test. During anaesthesia, no electrocardiography derangements were noted. There was no difference between groups in the area under the curve for any cardiovascular variable. Magnesium-treated animals had an increased incidence of hypotension during anaesthesia. Postoperatively, activity decreased significantly for both groups for duration (all time points) and frequency (TTE +0.5, +4.5, +8.5, +15.5 h), but no treatment effect was observed. Pain scores were comparable between groups. Following pain assessment and analgesia administration at TTE +17.5, Group NaCl had significant increases in HR and mean arterial pressure The magnesium dose evaluated produced no harm nor obvious benefit.
Introduction
Pain management is required for all animals subjected to noxious experimental procedures, for legal, ethical, medical, scientific and practical reasons (Animals (Scientific Procedures) Act 1986). Nevertheless, analgesic administration in pigs is reportedly insufficient. 1 The underlying reasons are not understood; however, research investigating veterinarians’ attitudes to animal pain and analgesic selection suggests that concerns regarding adverse drug effects are a principal reason for withholding analgesics. 2 Employing a multimodal approach to perioperative analgesia can mitigate the risk of undesirable side effects. 3 This strategy uses combinations of analgesics from different pharmacological classes (and targeting various points along the nociceptive pathways) at lower dosages. In achieving effective analgesia through additive or synergistic drug interactions the likelihood of side effects associated with any single drug class is minimised.
Magnesium enhances analgesia and mitigates central pain sensitisation by antagonising N-methyl-D-aspartic acid receptors in the spinal dorsal horn. 4 This mechanism suppresses hyperalgesia and allodynia,5,6 as demonstrated in human studies where perioperative magnesium infusion reduced postoperative pain and analgesic requirements.6,7 In dogs undergoing abdominal surgery, 8 magnesium infusions have anaesthetic-sparing effects; however, improved postoperative analgesia was not demonstrated. 9 Calcium channel antagonism by magnesium has been shown to directly decrease vascular smooth muscle tone, causing vasodilation. 10 Consequently, magnesium is used in humans to reduce intraoperative blood pressure (BP), 11 while its antiarrhythmic properties are used perioperatively to manage specific cardiac arrhythmias. 12
Magnesium can alter neuromuscular function. Elevated plasma magnesium concentrations inhibit presynaptic acetylcholine release, impairing neuromuscular transmission and promoting skeletal muscle relaxation.13,14 Studies in terminally anaesthetised pigs have confirmed that magnesium administration leads to neuromuscular blockade via this mechanism.15,16
The analgesic and cardiovascular effects of magnesium have not been investigated in laboratory-housed minipigs undergoing noxious procedures. This study aimed to compare perioperative haemodynamic, analgesic, anaesthesia-sparing, muscle relaxant and activity variables in Gottingen minipigs receiving either magnesium or saline infusions during thoracotomies.
Materials and methods
The surgical procedure described was conducted under Home Office (UK) Project Licence Safety Pharmacology PA952F011, and the magnesium infusion trial, as a potential refinement of the procedure, was approved by the Facilities Animal Welfare and Ethics Committee.
Animals
Sixteen 18-week-old Gottingen minipigs (eight males, eight females; Ellegard, Denmark) underwent surgical implantation of a five-channel telemetry system (L21, DSI). During a 4-week acclimation period, pigs were handled and rewarded with fruit treats, housed indoors in same-sex pairs under a 12:12 h dark:light cycle in 2.0 × 2.6 m enclosures that could be subdivided equally for single housing (Figure 5, Supplemental material). Daily food (300 g SDS Mini-pig 127 in two portions plus fruit) and water (municipal supply) were provided ad lib via Lixit® nipples. Ambient temperature was kept at 18°C–23°C and humidity at 40%–70%. Veterinary examinations, haematology, biochemistry, coagulation testing, nasal bacteriology and electrocardiography (ECG) confirmed that all pigs were fit for surgery within 2 weeks of the procedure.
Baseline video recordings of the pigs were collected between the acclimation and surgical periods (see Figure 1). All pigs were simultaneously and individually penned in their subdivided home pen for 1 h and video recorded.

Study plan and analyses: schematic showing timings of behavioural and physiological variables recorded perioperatively in minipigs receiving (treatment: Mg) or not receiving (control: NaCl) magnesium.
Anaesthesia
Pre-anaesthetic medication consisted of midazolam (Hypnovel® Neon Healthcare) 0.5 mg kg-1, ketamine (Ketamidor® 100 mg ml-1 Chanelle Pharma) 5 mg kg-1, methadone (Comfortan® 10 mg ml-1 Dechra) 0.2 mg kg-1, and dexmedetomidine (Dexdomitor®0.5 mg ml-1 Zoetis) 2 μg kg-1, administered together into the brachiocephalicus muscle. After 5–10 min, once adequate sedation was achieved, the marginal auricular vein was cannulated, and anaesthesia was induced with intravenous (IV) propofol (PropoFlo Plus® 10 mg ml-1 Zoetis) at 0.5–1.5 mg kg-1. Following topical administration of 40 mg lidocaine (Lidocaine Hydrochloride 2%, Hamlen Pharma) using a 10 cm mucosal applicator device (MADgic® Laryngo-Tracheal Mucosal Atomization Device; Teleflex), the trachea was intubated with a cuffed endotracheal tube. Anaesthesia was maintained with isoflurane vaporised in oxygen delivered via a circle breathing system. Fresh gas flows were initially set at 1–2 L min-1 and reduced to 0.5 L min-1 after approximately 15 min for the remainder of the procedure. The vaporiser (Vaportec Series 3) setting was adjusted to maintain an appropriate surgical plane of anaesthesia, assessed by palpebral and corneal areflexia, jaw relaxation and the absence of autonomic nervous responses linked to surgery. Intermittent positive pressure ventilation (IPPV) was provided using a Nuffield Penlon 200 ventilator with a paediatric valve. Peak pressures for tidal ventilation were maintained between 10 and 20 cmH2O. Ventilation rate and tidal volume (V
Treatments
Pigs were randomly assigned to treatment or control groups by sealed-envelope selection. Group Mg received 50 mg kg-1 magnesium IV (Magniject 25% Norbrook Laboratories, diluted for infusion with saline 75 mg ml-1) over 15 min before or during surgery, followed by a 15 mg kg-1 h-1 infusion (infusion pump Medfusion 4000, Smiths Medical). Group NaCl was given equivalent volumes of 0.9% saline (Baxter Healthcare) at identical rates (Figure 1). Only the surgeon knew the group assignments.
Surgery
A lateral thoracotomy incision was made at the left 5th intercostal space. The body of the telemetry device was secured in an intermuscular pocket between the left external and internal oblique abdominal muscles. The BP probe was placed in the caudal abdominal aorta via the left femoral artery; the left ventricular pressure (LVP) probe and ECG leads were tunnelled from the abdominal muscle pocket into the pleural cavity. The LVP probe was inserted into the left ventricular apex. The negative ECG electrode was sutured to the left lateral aspect of the aortic arch and the positive electrode sutured at the ventral aspect of the 5th intercostal space. Measures taken to minimise surgical trauma included removal of the 5th rib to increase surgical access to the pleural space. The intercostal neuro-vascular bundle was elevated from the caudal aspect of the 4th rib and the rib retractors positioned to avoid intercostal nerve compression injury. The thorax was closed and incorporated a wound soaker catheter (15 cm, 20G (Recatho®)) in the serratus dorsalis and serratus ventralis muscle layers, exiting approximately 3 cm dorsal to the thoracotomy incision. Other incisions were closed using standard techniques, cleaned, and covered with sterile dressings for up to 48 h after surgery.
Intraoperative analgesia
Pigs in both groups received perioperative analgesia in the form of preoperative meloxicam (Metacam 5 mg ml-1 Boehringer Ingelheim), 0.4 mg kg-1 IV and intraoperative ketamine infusions of 0.6 mg kg-1 h-1. Alfentanil (0.5 mg ml-1 Hamlen Pharma Ltd) 0.25–1 μg kg-1 min-1 was infused to effect, that is, all pigs initially received alfentanil at 0.25 μg kg-1 min-1 at the onset of surgery, but this was increased stepwise by 0.25 μg kg-1 min-1 when signs of noxious stimulation were encountered (e.g., increases in BP > 20% from previous value). Blind landmark guided intercostal nerve blocks were placed preoperatively at ribs 2–7 using levobupivacaine (Chirocaine ® 5 mg ml-1 AbbVie Ltd) 0.5 ml per rib. Rib locations of non‑palpable dorsal ribs 2–7 were predicted by extrapolating measured intercostal spacings of the caudal thorax.
Intraoperative study variables
Heart rate (HR), systolic- (SAP), mean- (MAP), and diastolic- (DAP) arterial pressures were measured non-invasively (NIBP) at baseline (t = 0) and at 15-, 30-, and 60-min post loading dose (LD) administration of magnesium or saline (Figure 1). Once the telemetry implant was secured, systemic BPs (SAP/DAP/MAP), HR, and left ventricular pressures and performance (peak systolic, early and end-diastolic pressures; contractility and relaxation (change in pressure over time +δP/δT)), were recorded every 30 s throughout surgical closure, tracheal extubation and recovery. During the 60 min preceding extubation, HR and IBP were compared between groups (Figure 1). The transition time from NIBP to IBP monitoring was documented.
Recovery
The interval from cessation of IPPV to the first spontaneous breath was recorded as the return of spontaneous ventilation. To avoid hypoxia during this period, single breaths approximating V
Post-recovery: analgesia and other medications
Pigs were housed individually for 30 h after recovery from anaesthesia. Buprenorphine and levobupivacaine (BL) were administered at TTE +6, +17.5, +23, and +29 h, independent of pain assessment score (Figure 1). The second buprenorphine dose (B2; TTE +6 h) was given IV before cannula removal; subsequent doses were delivered intramuscularly (IM). Meloxicam (M; 0.4 mg kg-1) was administered IM at TTE +21 h. Cephalexin (Ceporex®180 mg ml-1 MSD Animal Health) 20 mg kg-1 was continued IM every 12 h postoperatively (08:00, 20:00) until all cannulae and catheters were removed.
Post-recovery: pain assessment
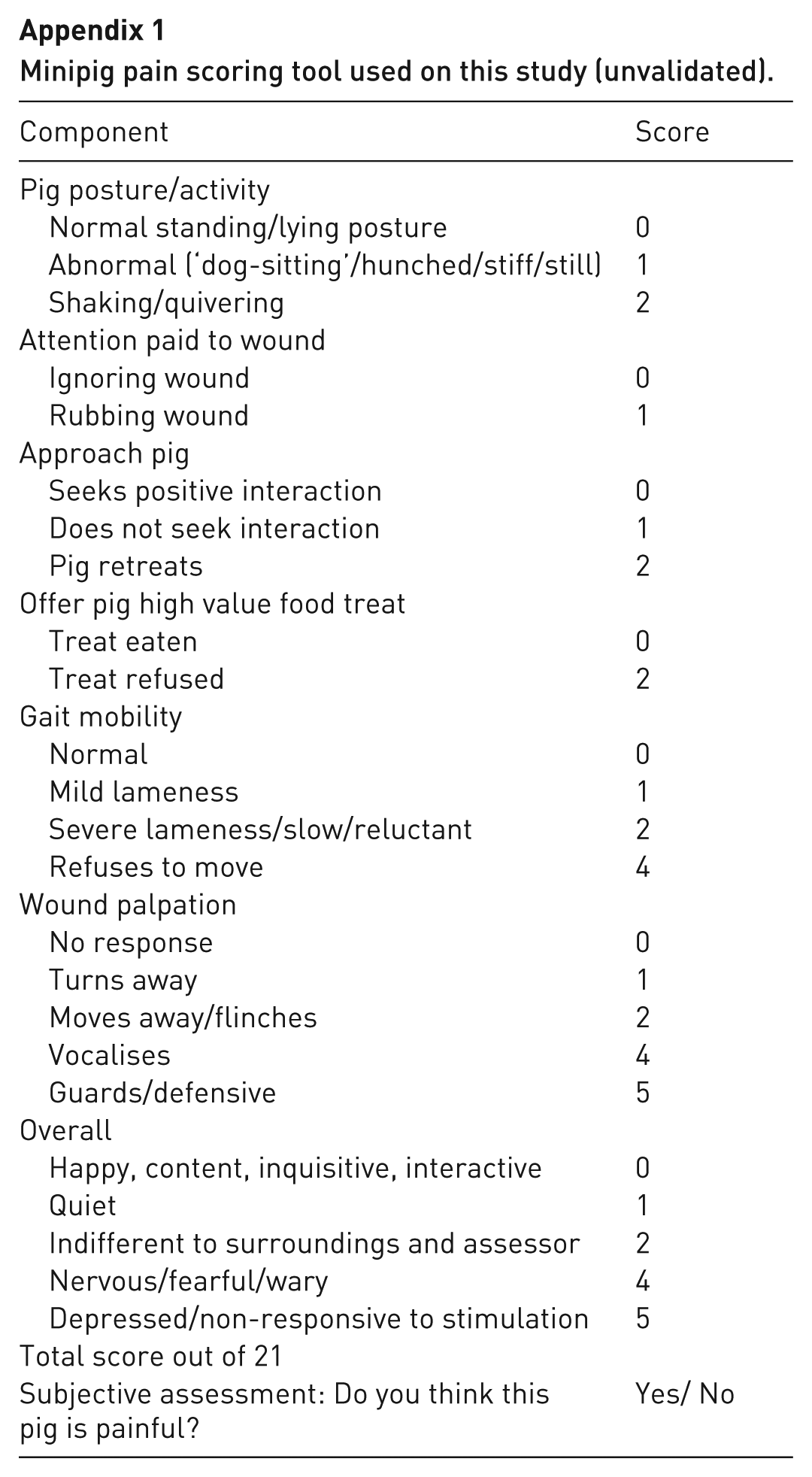
Pain was scored using a custom, non-validated composite scale for minipigs (Appendix Table 1) immediately before and 2–3 h after each administration of BL and meloxicam (TTE +2.5, +6, +17.5, +20, +23, +26, and +29 h). Intervention thresholds using this system had not been established at the time of the current study and so rescue analgesia (morphine 10 mg ml-1 Hamlen, 0.2 mg kg-1 IV or IM) was administered if the pigs were subjectively considered to be painful (based on their condition or appearance) and scheduled planned analgesia was not imminent.
Post-recovery: activity assessment and food intake
Continuous video monitoring was conducted for 30 h during single housing. Pre-surgery baseline and post-recovery activity analyses were conducted on 20-min epochs of the video footage taken from the baseline period and at TTE +0.5, +4.5, +8.5, +15.5, +19.5, and +25.5 h. Video assessment was conducted by an assessor unaware of treatment group. Food intake was measured by providing daily rations in bowls rather than scatter feeding.
Post-recovery: telemetry recording and sampling
Telemetry data for HR, SAP, DAP, MAP, and core temperature (t°C) were collected continuously for 30 h following TTE. Data were sampled in 20-min intervals aligned with activity assessments, and additionally during undisturbed periods immediately before and 20–40 min after analgesia administration. Further telemetry sampling was conducted for 5 min before and after pain evaluations. Area under the curve (AUC) and mean values for HR, SAP, MAP, DAP, and t°C were calculated for all periods. Event timing is outlined in Figure 1.
After 30 h post-surgery, the pigs were rehoused in established pairs, with treatments synchronised. Buprenorphine (10 μg kg-1) was administered three times daily for 2 days, and meloxicam was given orally once daily for 6 days. Animals were used in pharmacological studies upon their full recovery
Activity analysis
Video sequences were analysed using continuous focal sampling with COWLOG software. 17 This was quantified by dividing the home pen into four equal zones (Figure 5, Supplemental material) and continuously recording the frequency and duration of each animal’s location (i.e., the zone they occupied throughout the sequence).
Statistics
Data were analysed using Minitab 21. Normality of continuous variables (physiological measures, body mass, food intake, isoflurane percentage) was assessed via the Anderson–Darling Test. Non-normally distributed data were log10-transformed; if normality was not achieved, the Kruskal–Wallis test was used on raw data. Two-sample t-tests were used for group comparisons (natural or transformed data), with p < 0.05 as the significance threshold.
AUCs for cardiovascular (CVS[AUC]) variables, sampled both non-invasively and invasively, were calculated in GraphPad Prism 4. AUC data were tested for normality and compared between groups using two-sample t-tests at each time point.
Repeated measures (NIBP, HR, and pain scores pre- and post-LD) were analysed using general linear models with Bonferroni correction. Paired t-tests or Wilcoxon signed rank tests (for non-normally distributed data) compared pre- and post-analgesic CVS and pain measurements.
Pen utilisation was assessed with the Spread of Participation Index (SPI), calculated from frequency and duration in the four zones at each time point using a method adapted from Traylor-Holzer and Fritz. 18 SPI values (range: 0 to 1, with lower values indicating greater utilisation) were compared across time points and treatments using the Friedman test (within-subjects factor). Where time effects were significant, Wilcoxon matched-pairs tests with Bonferroni adjustment compared each postoperative time point against baseline. Mann–Whitney U tests assessed between-treatment effects at each time point.

N = total number of observations made on a subject,
M = mean frequency of observations in all sections,
nb = number of sections with frequency less than M,
na = number of sections with frequency greater than M,
Fa = total number of observations with a frequency greater than M, and
Fb = total number of observations with frequency less than M.
Results
Fifteen pigs (eight male and seven female; mean body mass 11.89 ± 0.85 kg) underwent surgery. There were no adverse events. One female did not undergo surgery and was excluded due to persistent leucocytosis. No significant differences were observed between groups for body mass, anaesthesia duration, transition from NIBP to IBP, surgery duration, or magnesium infusion duration. Anaesthesia and surgery were uncomplicated. Most procedures occurred in the morning; 2/8 Group NaCl and 3/7 Group Mg animals had afternoon surgeries.
Intraoperative pre-telemetric (NIBP) phase: loading dose and first 60 min of treatment
Baseline HR and NIBP did not differ significantly between groups (Table 2, Supplemental material). In most pigs (5/8 NaCl; 5/7 Mg), surgery began after LD administration; in the remainder, surgery started 2–3 min before completion of LD or simultaneously with LD in one NaCl pig. Treatment had no significant effect on HR or BP. No ECG abnormalities were observed in either group during the 60-min period after infusions were begun.
Intraoperative telemetric (IBP) phase: terminal 60 min before tracheal extubation (TE)
No significant differences were observed between groups in AUCs for HR, arterial BP, LVP, or left ventricle (LV) contractility (+δP/δT). Group Mg exhibited a higher incidence and longer duration of hypotensive episodes (MAP < 60 mmHg) in five out of seven animals, compared to Group NaCl; the effect of this on group data can be seen in Figure 2.
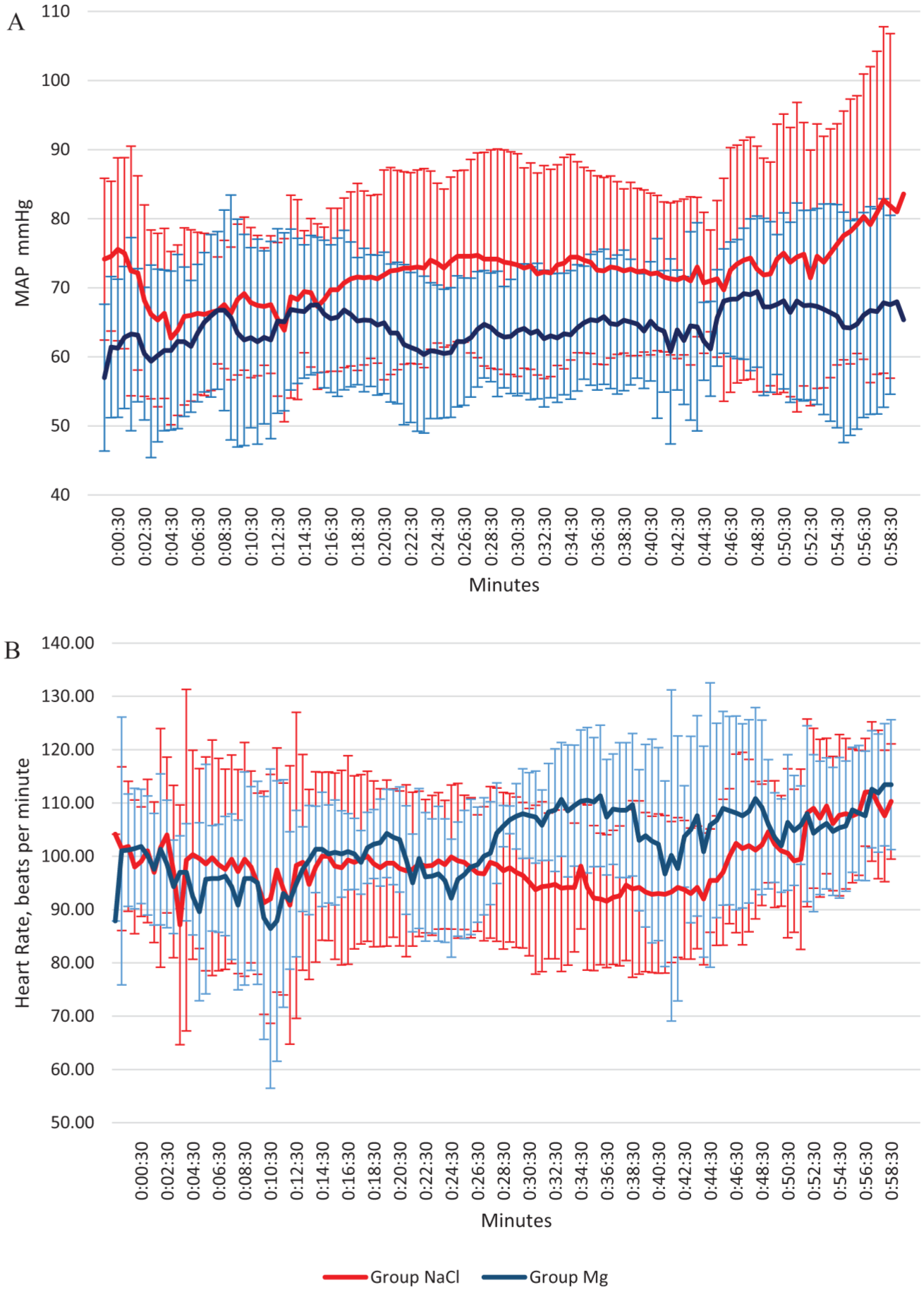
(a) Mean arterial pressure, and (b) heart rate in last 60 min of anaesthesia before recovery and extubation. Error bars represent standard deviation.
Intraoperative telemetric period: ECG effects
Ventricular premature complexes (VPCs) were recorded in all animals during pericardial incision and cardiac manipulation associated with LVP probe insertion. One animal receiving NaCl developed atrial fibrillation during cardiac manipulation, which resolved spontaneously when manipulation ceased.
Intraoperative period: anaesthesia-sparing effect
Mean isoflurane vaporiser settings during surgery did not differ significantly between groups (Group NaCl: 1.39% ± 0.40; Group Mg: 1.60% ± 0.30; p = 0.264). Alfentanil dose rates were not significantly different (Group NaCl: 0.48 ± 0.19 μg·kg−1·min−1; Group Mg: 0.51 ± 0.18 μg·kg−1·min−1; p = 0.744). During the 60 min before extubation, mean isoflurane settings remained comparable (p = 0.726).
Anaesthetic recovery
Resumption of spontaneous breathing after IPPV cessation did not differ significantly between Group NaCl and Group Mg (6.06 vs. 4.0 min, p = 0.177; Table 1). Tracheal extubation times were also comparable (6.38 vs. 7.29 min, p = 0.757). The difference in mean body temperatures at recovery onset was also non-significant (36.50°C vs. 36.86°C, p = 0.431; Table 1).
Summary data of anaesthesia and surgery. Data presented as mean ± SD or non-normal data presented as median [range]. There are no significant differences between groups.
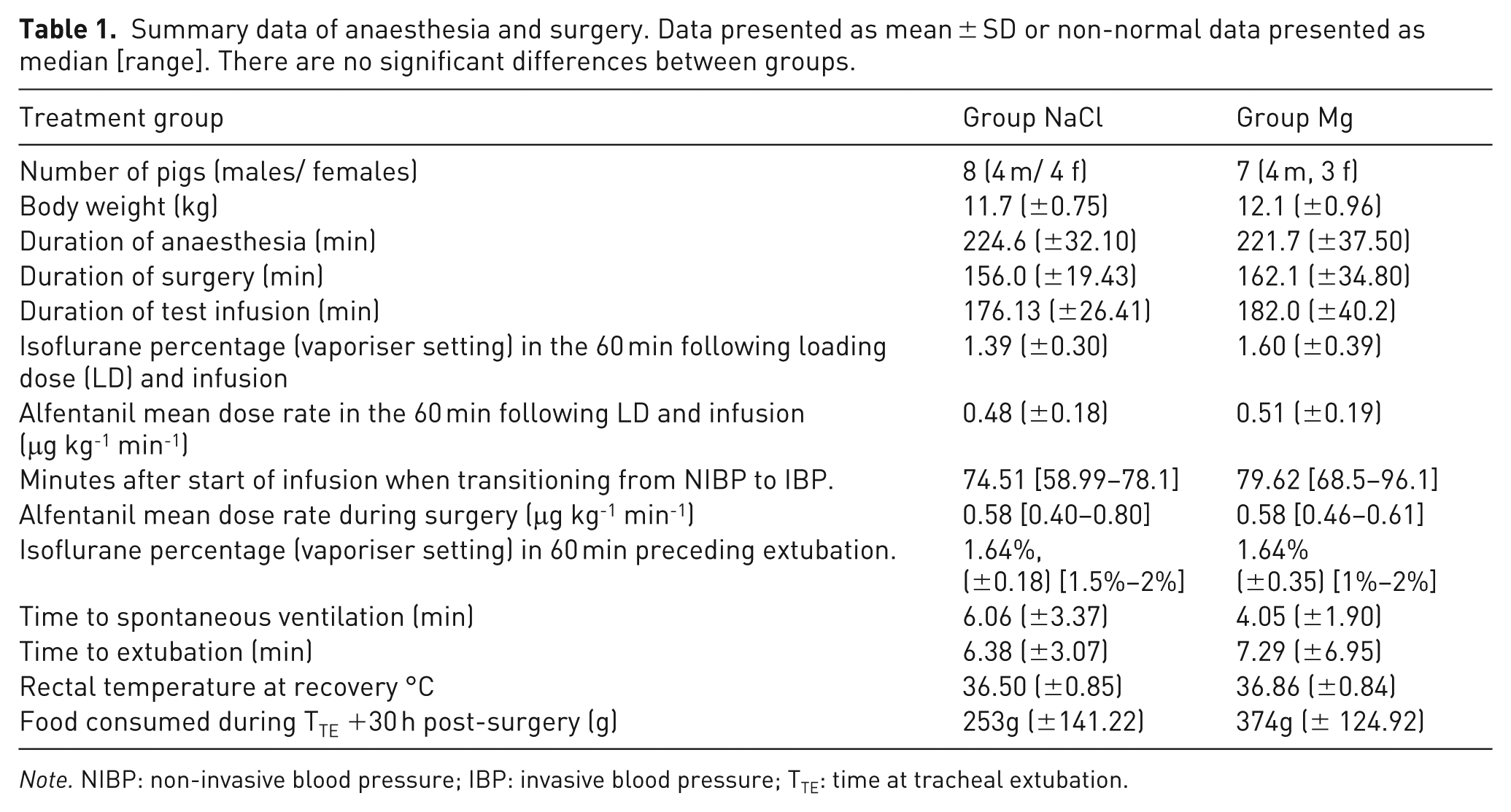
Note. NIBP: non-invasive blood pressure; IBP: invasive blood pressure; TTE: time at tracheal extubation.
Post-recovery: pain assessment, activity assessment and food intake
Composite pain scores and the number of animals classified as painful at each time point are presented in Figure 3. Group NaCl pigs were scored as painful on 17 of the 56 recording sessions, while Group Mg pigs were painful on 9 of the 48 recording sessions (Table 3, Supplemental material). Timepoint significantly affected pain scores (p < 0.0001), but no treatment or interaction effects were observed.
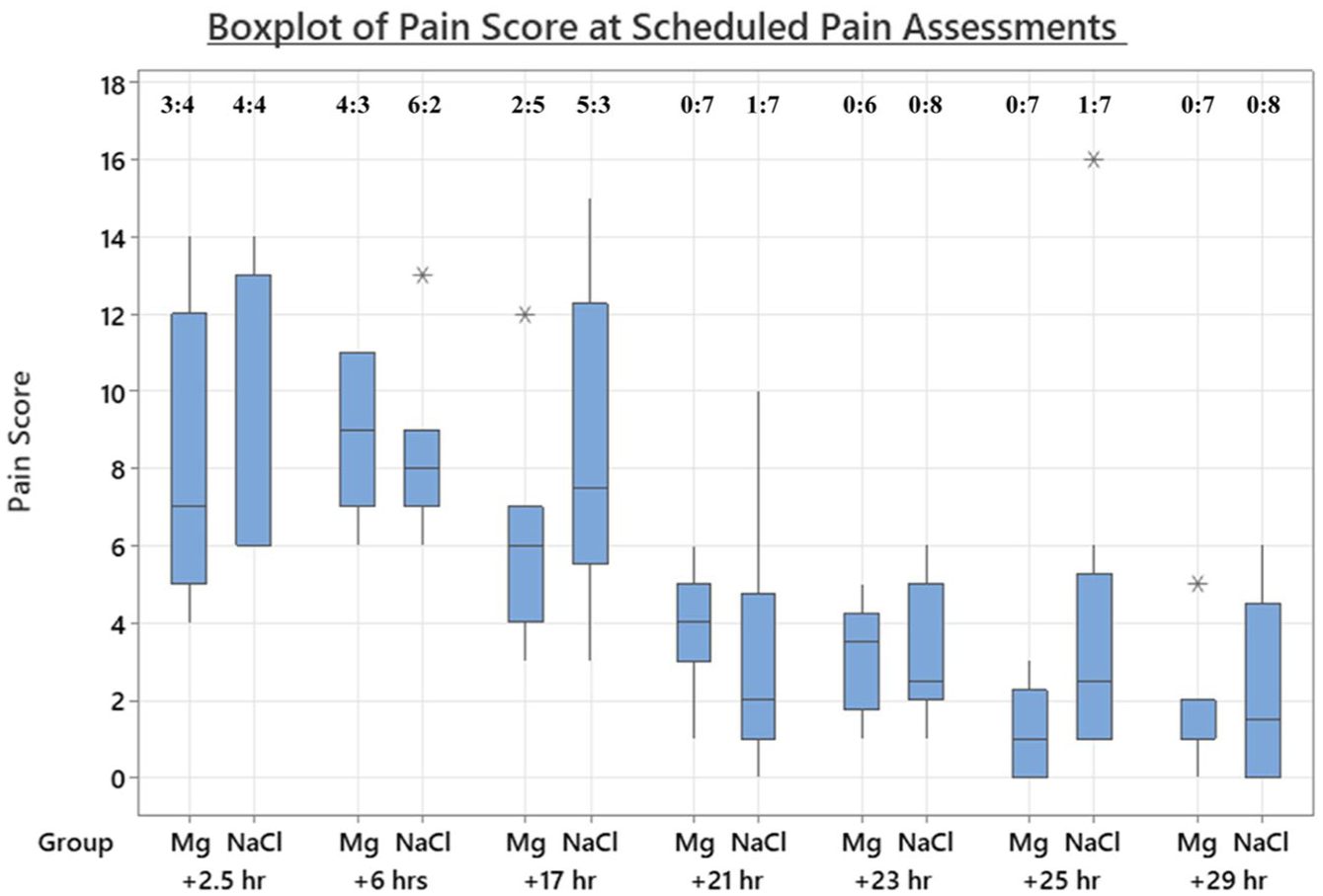
Pain scores at scheduled assessment times postoperatively. Subjective assessment of number painful: comfortable included above.
In Group NaCl, five of the eight pigs received a total of nine morphine doses postoperatively, with four doses administered on the day of surgery and five on the following day. Notably, one pig received three doses, and two pigs received two doses each. In Group Mg, three of the seven pigs received a total of five morphine doses, with only one administered on the day after surgery (Table 3, Supplemental material).
There was a significant effect of time point on the frequency and duration of pen utilisation (p < 0.001 and p < 0.001, respectively). All postoperative time points had significantly lower pen utilisation (i.e., higher SPI values) than at baseline, both in frequency and duration (Figure 4). Treatment did not significantly influence either the frequency or duration of pen utilisation at any time point.
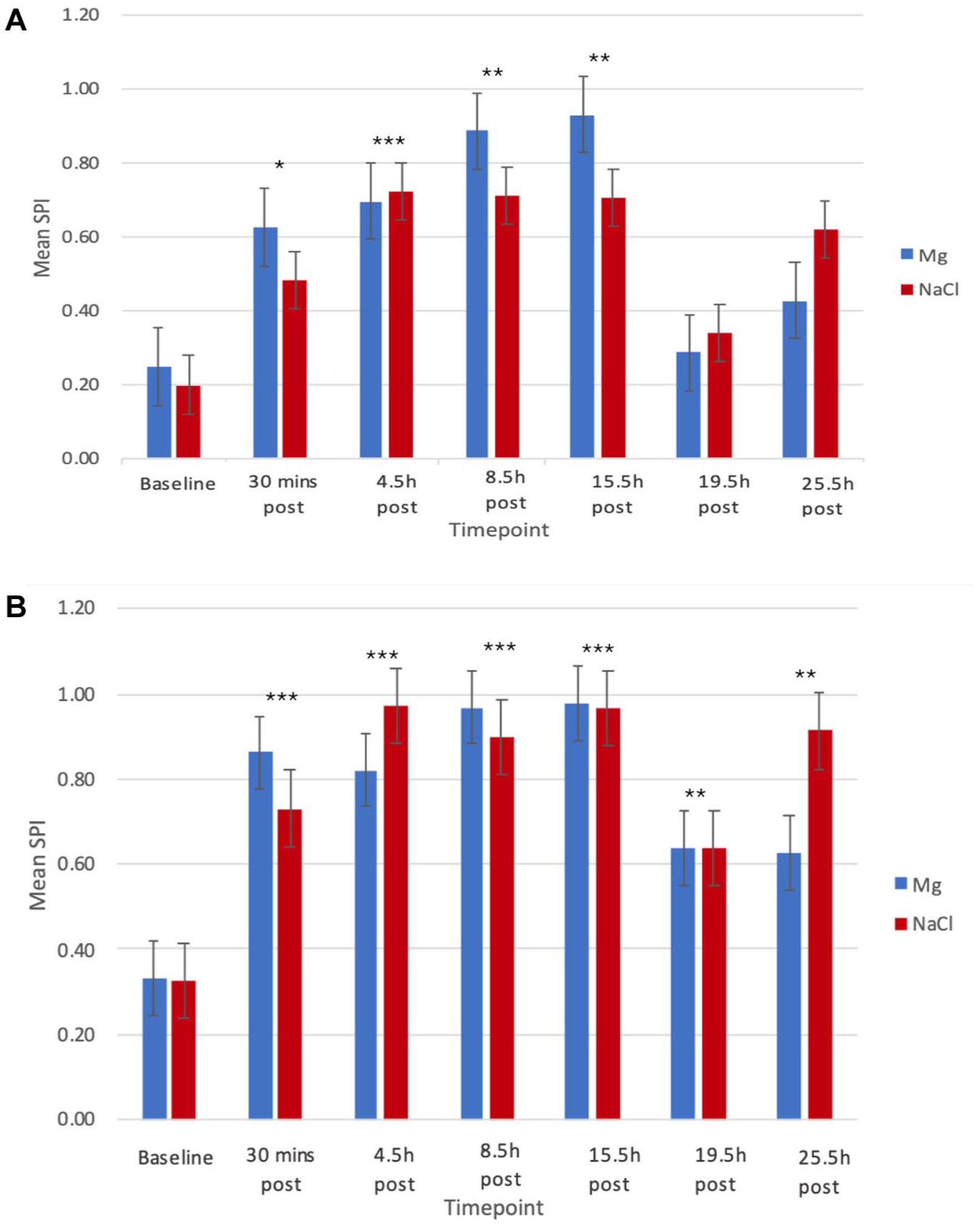
Mean SPI values (±1 SD) for the frequency (A) and duration (B) in each zone of the home enclosure before surgery (baseline) and at each post-surgery time point.
Food consumption did not significantly differ between groups.
Post-recovery telemetry: pain indicators (cardiovascular variables)
A telemetry connection malfunction resulted in incomplete data sets for five pigs during the early recovery period. The collected data were sampled and analysed despite this.
Post-recovery, within-group analysis revealed that Group NaCl exhibited significant increases in MAP, DAP, and HR following pain assessment at TTE +17.5 h (p = 0.049, p = 0.031, p = 0.022, respectively), and in HR at TTE +20 h (p = 0.022). Group Mg showed elevated HR[AUC] after pain assessment at TTE +6, +20, and +29 h (p = 0.028, p = 0.001, p = 0.031, respectively). No other significant within-group differences were noted.
Pre-analgesia (BL and meloxicam), no between-group differences were observed in CVS variables at any time point. Post-analgesia, Group NaCl had increased DAP at TTE +17.5 h (p = 0.033). A within-group difference found Group NaCl had increased SAP at BL3[POST] (TTE +17.5 h; p = 0.036) and MAP approached significance (p = 0.054). Meloxicam[POST] at TTE +20 h increased HR and MAP (p = 0.035 and p = 0.014) for Group NaCl. Group Mg showed non-significant pre- vs. post-analgesia differences.
Between groups, at TTE +17.5 h, Group NaCl showed elevated MAP (p = 0.044), and HR (p = 0.040) post-analgesia compared to Group Mg; no differences were observed at other time points.
Discussion
In the current study, magnesium infusions in minipigs did not confer apparent benefit in terms of reducing i) anaesthetic requirement (antinociceptive effect); ii) the need for rescue analgesia; or iii) postoperative pain. Similarly, the addition of magnesium infusion to a multimodal analgesia regimen did not appear to cause any haemodynamic effects, either adverse or beneficial.
During the intraoperative and post-treatment phases, a 15-min magnesium LD produced minimal cardiovascular effects compared with NaCl. Unlike studies with rapid magnesium boluses (>30 mg kg-1), which reduced BP in anaesthetised dogs,12,19 no significant BP changes were observed here, consistent with Rioja et al.’s findings. 9
Magnesium at the studied dose is administered perioperatively in cardiac surgery to decrease the incidence of perioperative atrial and ventricular arrhythmias.20,21 Real-time ECG monitoring showed no notable alterations during magnesium LD infusion. Akazawa et al. 12 reported that faster infusions (10 s) at higher doses (30, 60 and 90 mg kg-1) led to decreased HR and conduction changes in dogs. The rate of magnesium administration (slow vs. rapid) may be important in eliciting ECG changes. Incision of the pericardium and cardiac manipulation in the pigs induced transient VPCs and, in one NaCl-group animal, brief atrial fibrillation, but no severe arrhythmias occurred.
During the final hour of anaesthesia, no significant differences in cardiovascular parameters were observed. However, the magnesium group showed an increased incidence of hypotension despite having equivalent body temperatures, procedural duration, and fluid administration (Figure 2). This is consistent with findings in anaesthetised humans receiving magnesium infusions during surgery 22 and aligns with magnesium’s role as a calcium channel blocker, which lowers BP via vasodilation and reduced cardiac output. 19 Despite this, no negative inotropic effects were detected at the administered dose, possibly due to concurrent isoflurane and alfentanil use.23,24
Isoflurane requirements, as indicated by vaporiser settings, did not differ between treatment groups during the final hour of anaesthesia. End-tidal anaesthetic agent monitoring was unavailable; thus, an anaesthetic-sparing effect of magnesium cannot be excluded. Anaesthesia was maintained at a stable surgical depth by an experienced anaesthetist, who was ignorant of treatment. Similar studies in sevoflurane-anaesthetised dogs with equivalent magnesium dosing also reported no anaesthetic-sparing effect.9,25
Hypermagnesaemia can manifest as respiratory depression through reduced contractility of inspiratory muscles.26,27 However, the magnesium-treated pigs in this study showed no difference in latency to resume spontaneous respiration or in extubation time compared to Group NaCl. This is consistent with findings in human patients. 28
In a human trial of 100 thoracotomy patients, intraoperative magnesium infusion was associated with lower postoperative pain scores (both postoperative and 30-days post-surgery) and reduced patient-controlled analgesic use, 6 but findings in paediatric patients and dogs receiving an otherwise multimodal perioperative analgesia regime remain inconclusive.9,29 –31 Morphine at 0.2 mg kg-1 was administered as rescue analgesia, based on published effective doses and its full mu-opioid agonist effect. 32 However, it is conceivable that its maximal effect may have been reduced by the prior administration of buprenorphine. 33 Being a long-acting partial μ-agonist with high receptor affinity, buprenorphine may have limited the extent of morphine agonism. However, morphine’s clinical analgesic effect was consistent with expectations, that is, was additive and sufficient, and fulfilled the criteria for effective rescue analgesia. 34 It was not considered possible nor practical to infuse highly potent opioid agonists (e.g., alfentanil, to treat pain with buprenorphine present), since we did not have the necessary ambulatory pumps and jackets, and had no means of mounting a pump safely within the home pen and preventing pig interference with the drug administration set. In any case, morphine proved effective. Morphine rescue analgesia was provided to some pigs in both groups during the 30-h post-surgical period, potentially confounding subsequent pain and cardiovascular variable assessments. However, in accordance with governing ethics and legislation, withholding analgesia for suspected pain was not permissible. Acute pain scores and rescue analgesia requirements did not differ significantly between groups, likely due to the difficulty of recognising pain behaviour in minipigs and the lack of validated assessment tools for this species. 2 At the time of data collection, the piglet grimace score had not yet been developed.2,35 Small sample size and robust analgesia in the control group probably limited the ability to detect group differences.
Pen utilisation decreased from pre- to post-surgery for both frequency and duration. This reduction in movement is routinely observed in many species after surgery,36 –39 as animals are reluctant to move due to post-surgical pain and malaise. The treatments did not alter the reduction in movement observed post-surgery compared to pre-surgery, nor did they alter movement between treatments, suggesting that both treatments were ineffective at treating post-surgical pain and malaise.
Pre-surgical food intake was not recorded, representing a study limitation. Postoperative food consumption within 30 h of extubation was highly variable across groups, with no significant differences observed. Reduced food intake following surgery is routinely accepted as an indicator of pain and impaired well-being in a range of species.2,40
Assessment of autonomic nervous system responses to noxious stimuli, particularly via HR and BP measurements, is well established in both conscious and anaesthetised animals.41,42 Telemetry cardiovascular data from mice suggest increases in HR and HR variability are associated with increased pain following laparotomy without analgesia, compared to groups treated with flunixin or carprofen. 42 In this study, postoperative cardiovascular variables did not differ significantly between groups at 14 out of 16 time points. Notably, within Group NaCl, AUC analysis revealed cardiovascular differences at the TTE +17.5-h pain assessment and following the third dose of BL analgesia. These findings likely reflect reduced analgesic coverage, as BL2 was administered at TTE +6 h and buprenorphine’s half-life in minipigs is 2.4 h, with anticipated analgesia lasting 6–8 h. 43 Additionally, two of the eight pigs in Group NaCl required unscheduled pain assessments and morphine administration around TTE +14 h (8 h after BL2), having undergone afternoon surgeries and thus not receiving their scheduled TTE +17.5 h BL dosing until 10:00 the next morning. In accordance with facility protocols, these pigs were assessed early in the morning and received prompt treatment when pain was observed. Elevations in HR, MAP, and DAP AUCs after pain assessment suggest increased nociception or stress in Group NaCl at this time. This is in contrast to the magnesium-treated group, which did not demonstrate significant cardiovascular changes. Additionally, at TTE +17.5 h, five of the eight Group NaCl pigs were subjectively assessed as painful (compared to 2/7 for Group Mg). Cardiovascular responses and pain scores at this time may have been influenced by external factors such as environmental stimuli or circadian effects, although a major effect of magnesium on cardiovascular function was not expected. Cardiovascular data of all animals indicated a circadian pattern was present. This temporal variation, alongside perioperative magnesium infusion, may have contributed to improved postoperative comfort in Group Mg at TTE +17.5 h. Additionally, inconsistent timing of TTE +17.5 h assessments and BL dosing between groups – due to varying surgery schedules – may have confounded results. In Group Mg, three of the seven pigs had mid-to-late morning assessments (09:30–12:00), while others were assessed earlier (06:30–07:00). This aligns with evidence from systematic reviews indicating human postoperative pain peaks at 08:00 h that subside throughout the day, unless consistent opioid analgesia is provided. 44 Therefore, variability in assessment times may have masked true differences in pain intensity.
Finally, no sustained decrease in BP was observed in Group Mg following the transient reduction noted during the final hour of anaesthesia, and once recovery was achieved.
Limitations and relevance
Several factors may explain the lack of observed differences between treatment groups in this and other studies. First, the magnesium dose selected, which was based on efficacious levels in adult humans,5,7 may not have produced a pharmacological effect for at least three reasons: i) the doses used did not produce analgesic plasma magnesium concentrations because the cation may have accelerated clearance in pigs; ii) equi-analgesic plasma magnesium concentrations may be greater in pigs than humans; iii) both of these. While knowledge of plasma magnesium concentrations would have thrown light on this, the required serial blood sampling was not authorised on the project’s licence. Comparing the pharmacodynamics and pharmacokinetics of magnesium in humans 45 and pigs deserves consideration for further research. Second, any potential analgesic effect was likely masked by the robust multimodal analgesic protocol provided. Third, the use of alfentanil, administered in response to cardiovascular indicators of nociceptive stimulation (tachycardia and hypertension) likely reduced both intrinsic HR and the extent of nociceptive responses, thereby minimising differences between groups. Additionally, morphine provided as rescue analgesia postoperatively would have further limited group differences.
Technical limitations also affected the study: incomplete telemetry data sets resulted from technical problems, but all available data were analysed due to the limited sample size. Furthermore, not all animals were acclimatised to single housing before the study, and the timing of surgery (morning or afternoon) introduced additional variability.
Improvements in future studies
Further investigations are warranted, as the potential benefits of magnesium in reducing postoperative pain represent a significant refinement for research animals, if benefits can be detected. Greater infusion doses of magnesium should be evaluated, alongside pharmacokinetics, since it is possible that the dose of magnesium was too low or that doses of other analgesics masked its effect. However, since detection of pain in minipigs remains challenging, the authors would not in good conscience recommend pursuing an “opioid free” approach in further work involving research animals.
Behavioural analysis could be improved by implementing more specific assessments at set times, for example, using grimace scales before analgesia administration.
Conclusions and relevance
This study shows that perioperative magnesium sulphate infusion at the tested dose caused modest, transient hypotension but few other adverse cardiovascular effects during anaesthesia. Magnesium did not reduce anaesthetic requirements, nor improve postoperative analgesia. Recovery was not delayed. Magnesium at the dose tested brought neither benefit nor harm to the anaesthetic technique described.
Supplemental Material
sj-docx-1-lan-10.1177_00236772261441113 – Supplemental material for The effects of magnesium infusions on haemodynamic and nociceptive variables in minipigs undergoing thoracotomy
Supplemental material, sj-docx-1-lan-10.1177_00236772261441113 for The effects of magnesium infusions on haemodynamic and nociceptive variables in minipigs undergoing thoracotomy by Bryony Few, Scott Burgess, Matt Leach and R. Eddie Clutton in Laboratory Animals
Footnotes
Appendix
Minipig pain scoring tool used on this study (unvalidated).
| Component | Score |
|---|---|
| Pig posture/activity | |
| Normal standing/lying posture | 0 |
| Abnormal (‘dog-sitting’/hunched/stiff/still) | 1 |
| Shaking/quivering | 2 |
| Attention paid to wound | |
| Ignoring wound | 0 |
| Rubbing wound | 1 |
| Approach pig | |
| Seeks positive interaction | 0 |
| Does not seek interaction | 1 |
| Pig retreats | 2 |
| Offer pig high value food treat | |
| Treat eaten | 0 |
| Treat refused | 2 |
| Gait mobility | |
| Normal | 0 |
| Mild lameness | 1 |
| Severe lameness/slow/reluctant | 2 |
| Refuses to move | 4 |
| Wound palpation | |
| No response | 0 |
| Turns away | 1 |
| Moves away/flinches | 2 |
| Vocalises | 4 |
| Guards/defensive | 5 |
| Overall | |
| Happy, content, inquisitive, interactive | 0 |
| Quiet | 1 |
| Indifferent to surroundings and assessor | 2 |
| Nervous/fearful/wary | 4 |
| Depressed/non-responsive to stimulation | 5 |
| Total score out of 21 | |
| Subjective assessment: Do you think this pig is painful? | Yes/ No |
Acknowledgements
Thanks to Katie Odlin for the analysis of the activity, Anthony Webb for his surgical contribution and Jamie Fogarty for practical assistance in recording video and telemetry data.
Author contributions
Bryony Few: Collection and analysis of data, manuscript contributions.
Matt Leach: Design of the activity analysis, manuscript contributions, statistical advice.
Scott Burgess: Statistical advice.
Eddie Clutton: Overall study design and manuscript contributions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Surgical procedures were conducted under Home Office Project Licence PA952F011. The Facility Animal Welfare and Ethics Committee approved this study as a potential refinement.
Data availability
Study data and additional information are available through contact with the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.