
Abstract
Temporomandibular disorders affect about 12% of the industrialized population, and their complex management often results in recurrence or treatment failure. Among animal models, the pig is particularly relevant owing to its anatomical similarity to humans, although specific differences in the zygomatic arch and mandibular fossa require adapted surgical approaches. We describe and validate a standardized surgical approach to the porcine temporomandibular joint (TMJ) suitable for translational research. Eleven cadavers of Sus scrofa domestica were dissected to identify key anatomical structures. A high condylectomy was performed to establish a reproducible surgical pathway, and the caudal intra-articular injection technique was tested using methylene blue to assess its feasibility. The pig’s TMJ area consists of superficial muscles such as the platysma and parotidoauricularis, with deeper structures such as the parotid gland, facial nerve and major vessels, while the bony anatomy includes a large condylar head and a superficial zygomatic arch. The proposed surgical approach to the pig TMJ involves a retromandibular incision with preauricular extension, subperiostal dissection to expose the zygomatic arch and articular capsule, followed by an incision to access the condyle, disc and mandibular fossa, allowing for condylectomy with careful preservation of the facial nerve and surrounding structures. This study highlights the anatomical differences with humans, such as the presence of the parotidoauricularis muscle, which lies superficially to the facial nerve and serves as a useful landmark for a safe dissection. The described approach provides a reliable and reproducible technique for future TMJ surgical studies in the pig model.
Introduction
Temporomandibular disorders (TMDs) are common myoarthropathies of the temporomandibular joint (TMJ), affecting approximately 12% of the industrialized population. 1 Their management remains challenging, with a high rate of therapeutic failure or recurrence. In recent years, minimally invasive strategies (such as arthrocentesis, arthroscopy, intra-articular injections of biomaterials and regenerative approaches) have gained increasing attention as alternatives to more invasive procedures.2,3 These techniques require reliable preclinical models to assess safety, feasibility and efficacy before clinical translation. Consequently, small animal models, including mice, rats and rabbits, are commonly employed in preclinical TMD research.4,5 However, their craniofacial anatomy, the joint size and masticatory physiology differ considerably from humans, limiting the direct applicability of experimental findings in the clinical practice.
The pig is one of the most suitable larger animal models owing to its anatomical and physiological similarities to the human TMJ. 6 Similar to in humans, the pig TMJ demonstrates both translational and rotational movements during mastication, as both species are omnivorous. Nevertheless, important anatomical differences exist, particularly the presence of a broad zygomatic arch and limited caudal bony coverage of the condylar head, which distinguish the porcine TMJ. 7 These features alter joint exposure compared with humans and necessitate adapted surgical approaches.
Although several studies have described porcine TMJ anatomy, no standardized method has been reported for surgical access, particularly for minimally invasive procedures. We hypothesize that a reproducible surgical approach can be developed in swine to facilitate future translational TMJ research. Therefore, the aim of this study was to investigate the anatomical landmarks of the porcine TMJ and develop a reliable surgical approach enabling both surgical procedures and intra-articular therapeutic applications to facilitate future surgical research.
Material and methods
Ethics and animal selection
The study was conducted in the Département Hospitalo-Universitaire de Recherche et d’Enseignement (Dhure) of Lille University Hospital. Eleven cadavers of Sus scrofa domestica were included within 12 h postmortem.
All procedures complied with European regulations for the protection of animals used for scientific purposes (Directive 2010/63/EU). Since the study was conducted exclusively on cadavers of pigs previously euthanized for unrelated research projects, no additional animals were used. Ethical approval was therefore not required.
The included pigs were used after euthanasia at the end of those projects with a dose of 200 mg/kg of pentobarbital (Doléthal, Vetoquinol S.A.Ⓡ). Prior to their use in this study, animals were monitored daily, and their health was supervised by a veterinarian during housing. The animals received specialized pig feed (coopérative UnéalⓇ) with unlimited access to water.
Seven minipigs (Göttingen-like) and four farm pigs were used. The minipigs were approximately 1–2 years old, while the farm pigs were 4–5 months old. Weights ranged from 35 kg to 51.7 kg for the minipigs and 42 kg to 50 kg for the farm pigs. Detailed characteristics of each pig are summarized in Supplemental material Data 1 online.
Experimental procedures
To investigate different approaches to the TMJ and validate potential translational applications, several complementary procedures were performed on the cadaveric specimens.
Anatomical dissection
A systematic dissection of the TMJ region was performed on all specimens in order to expose the main anatomical landmarks encountered during surgical access. The dissection was conducted in a stepwise fashion, beginning with the removal of skin and subcutaneous tissues to identify the platysma muscle, followed by careful separation of the superficial muscular and fascial layers. Intravascular injection of saline followed by diluted betadine solution was carried out to enhance the visualization of vascular structures and facilitate their identification during dissection. The parotid gland and the facial nerve were then dissected in detail, and the course of the main vascular and nervous branches was documented. This approach allowed precise mapping of vascular, nervous and muscular structures in relation to the TMJ capsule and condylar head.
3D reconstruction of bony anatomy
To complement the anatomical dissections, a 3D reconstruction of the porcine craniofacial skeleton was generated. A high-resolution computed tomography (CT) scan of a minipig head was performed using bone window settings. The dataset was processed with 3D Slicer software (version 5.7.0-2025-01-0), which allowed segmentation and reconstruction of the osseous components of the TMJ, including the condyle, mandibular fossa and zygomatic arch. The resulting Standard Triangle Language (STL) file was exported and printed with a Ultimaker S5 using PLA filament material. The physical model was used to validate the findings from dissection and to provide a reproducible visual aid for surgical planning. It also served as a training tool to anticipate surgical access and evaluate bone relationships prior to cadaveric interventions.
Caudal injection technique
The feasibility of intra-articular access to the porcine TMJ was tested using the caudal injection technique described by Wang et al. 8 A 22-gauge needle was introduced at the caudal border of the zygomatic process, oriented rostro-medially at approximately −10° in the sagittal plane and −80° in the coronal plane, according to the published method. A solution of methylene blue was injected and correct intra-articular positioning of the needle was confirmed by applying a distraction movement to the mandible: passive needle movement indicated successful placement. After injection, the joint was dissected to verify intra-articular diffusion of the dye. This technique was repeated on three specimens to assess reproducibility.
Surgical approaches (retromandibular/subangular)
Finally, surgical access to the condylar region was performed in order to standardize an approach suitable for experimental and translational purposes. Both a retromandibular incision, corresponding to the pretragic approach commonly used in humans for condylar exposure, 9 and a subangular (modified Risdon) approach providing access to the subcondylar region 10 were tested. By using both approaches, a condylectomy was performed. These procedures were carried out with the aim of defining reproducible anatomical landmarks and assessing potential risks related to surrounding neurovascular structures.
Results
Anatomic description of the pig TMJ area
Superficial structures
The skin and subcutaneous fatty tissue covered the underlying platysma muscle, which extended from the chest to the mandible, with some fascicles reaching the ventral edge of the orbit. The fascicles were oriented in a cranio-caudal direction. The platysma muscle covered the ventral part of the neck but tapered off in the dorsal region, leaving the upper part of the mandibular ramus and the zygomatic arch exposed. In the same plane, behind the mandibular ramus, the dorsal portion of the parotidoauricularis muscle was identified. This muscle was attached at the base of the auricular cartilage and extended ventrally to pass beneath the platysma.
Deep structures
Removing the platysma exposed the deeper structures, including the parotid gland. The gland was challenging to dissect owing to the surrounding fatty tissue and the absence of a distinct capsule. The previously described parotidoauricularis muscle continued beneath the parotid gland and was divided into two heads. The first head was attached to the deep surface of the parotid gland, while the second continued to insert onto the deep surface of the platysma muscle along the midline. Upon removal of the parotid gland, the mandibular ramus, the maxillary/lingofacial vein, the submandibular gland, and the dorsal and ventral buccal branches of the facial nerve were identified (Figure 1). These structures were covered by the superficial layer of deep cervical fascia. The facial nerve innervated the gland with multiple small branches on its deep surface. The main trunk of the facial nerve emerged at the mid-point of the mandibular ramus, approximately 1 cm below the palpable pterygoid process, before dividing into several branches. Among these, the auriculopalpebral, the dorsal and ventral buccal branches of the facial nerve were consistently identified, together with a cervical branch coursing toward the neck. Several facial nerve branches ran vertically near the TMJ, partially overlying the posterior and caudal aspects of the condylar head and the joint capsule. Owing to the variability of distal branching patterns, these branches could not be reliably individualized and were therefore described according to their topographical distribution, corresponding to rostral auricular and zygomatic facial nerve branches. The auriculopalpebral branch ran vertically, positioned ventro-caudally and deep relative to the TMJ. The dorsal buccal branch followed a vertical course, crossing the mandibular ramus at its midpoint. The ventral buccal branch (also referred to as the marginal mandibular branch in classical anatomical descriptions) ran along the ventral border of the mandible a few millimetres below it, while the cervical branch coursed caudally behind the buccal branches toward the neck (Figure 2).
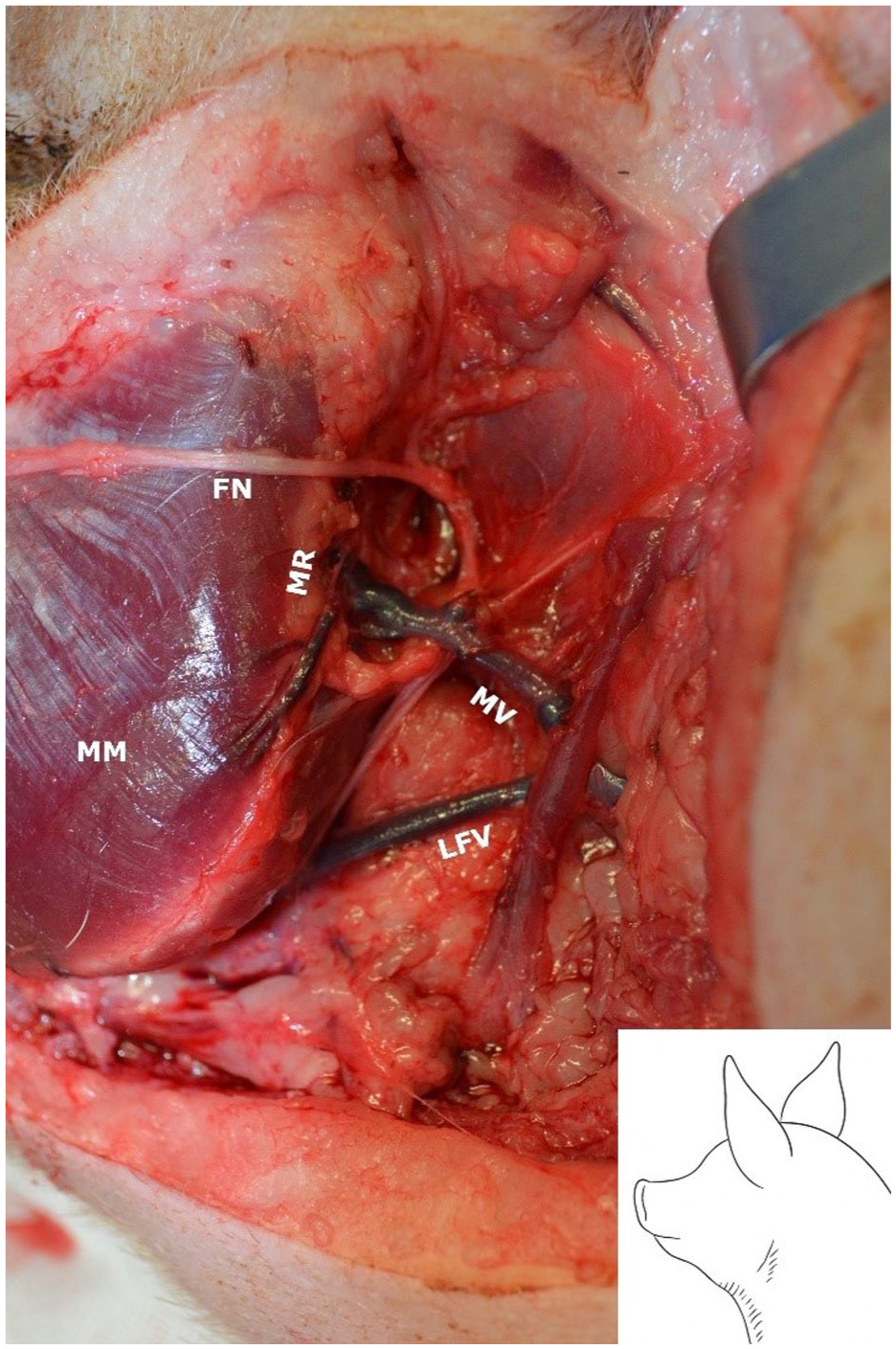
Removal of parotid gland, allowing exposure of the masseter muscle (MM), the mandibular ramus (MR), the maxillary and linguofacial vein (MV and LFV) and the buccal branches of the facial nerve (FN).
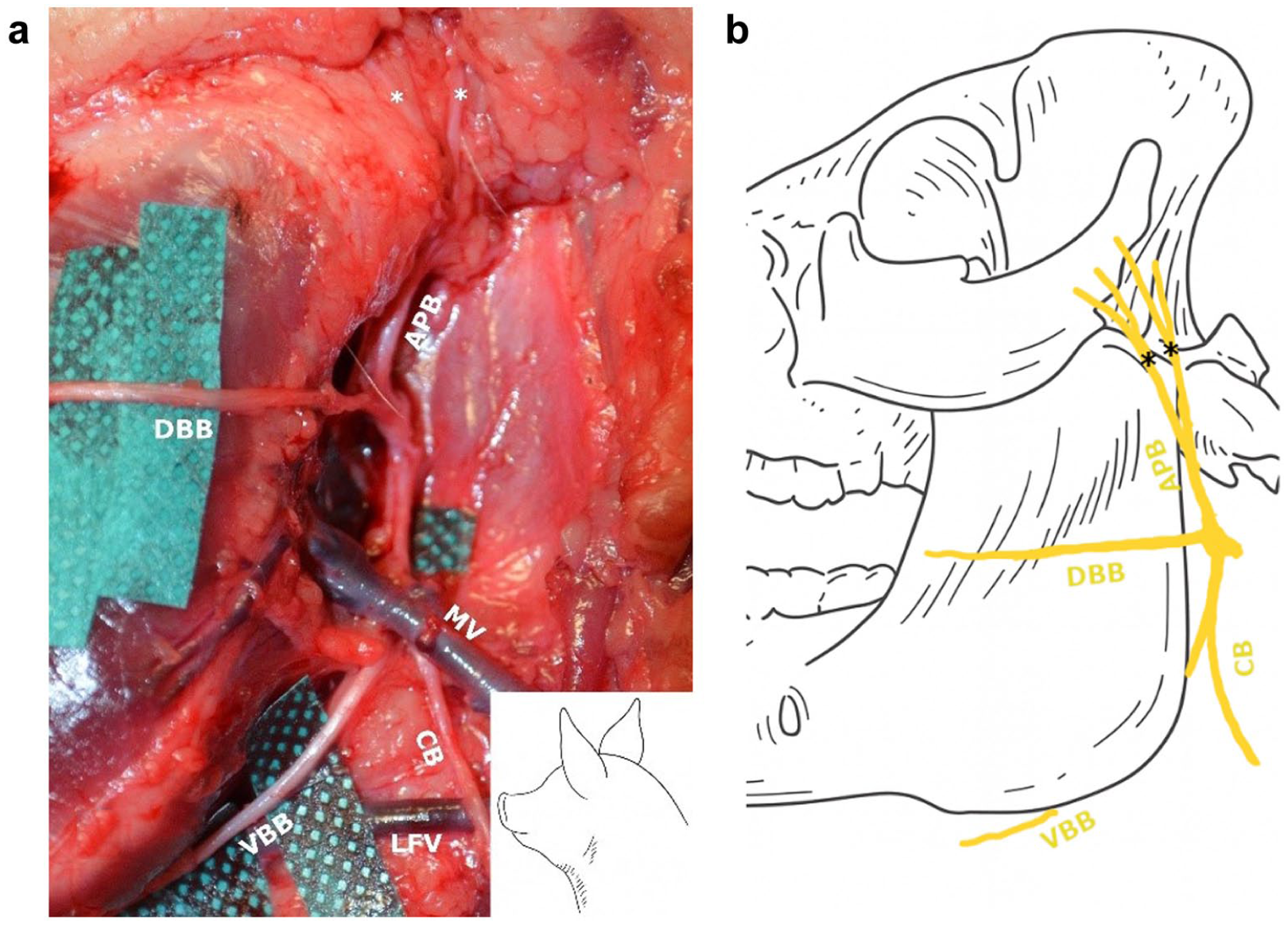
Deep structures of the temporomandibular joint (TMJ) dissection and schematic representation of the facial nerve.
Two arteries were in proximity to the TMJ (Figure 3): the superficial temporal artery, rostrally, which is one of the two terminal tributaries of the external carotid artery, and the caudal auricular artery, caudally, which is collateral tributary of the external carotid artery. At the venous level there is a network modelled on that of the arteries: the superficial temporal vein and the caudal auricular vein, ended in the proximal segment of the maxillary vein (also referred to as the retromandibular vein in classical anatomical descriptions), which is a tributary of the external jugular vein.
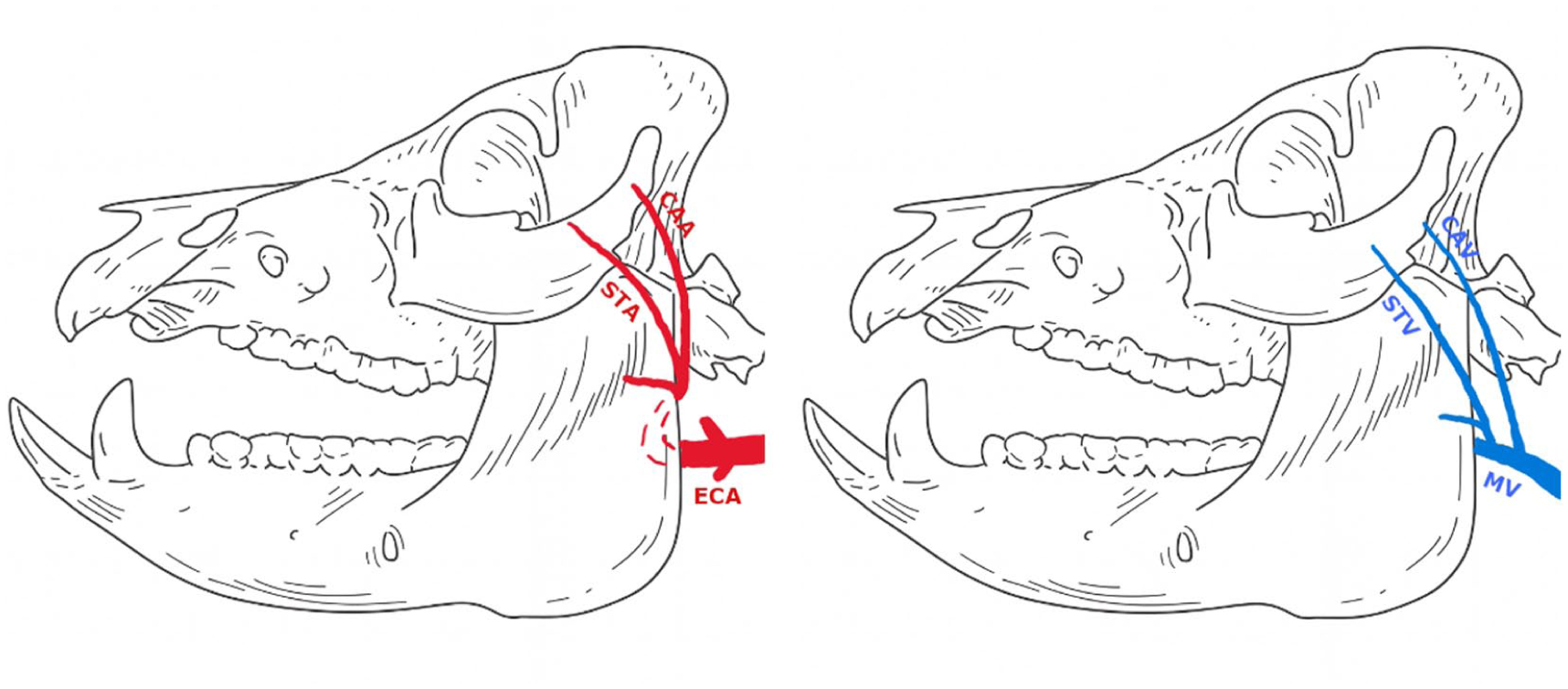
Vascular structures around the TMJ.
Bony structures
No relevant differences were observed between the 3D-printed models, the CT-based reconstructions and the anatomical landmarks encountered during TMJ dissection. The zygomatic arch was broad and relatively superficial. After the skin and subcutaneous fatty tissue were removed, the bone was covered only by a fibrous layer. The TMJ capsule was attached at the ventro-caudal edge of the zygomatic arch and the dorso-caudal extremity of the mandibular ramus, concealing the condylar head. Opening the capsule revealed the condylar head. The retroarticular process was underdeveloped, and the retro-TMJ area was filled with fibrous tissue. The condylar head was large and convex, connected to the mandibular ramus by a short neck. A 3D-printed model of the bony structures is shown in Figure 4. The TMJ discs were oval and biconcave, with both rostral and caudal attachments
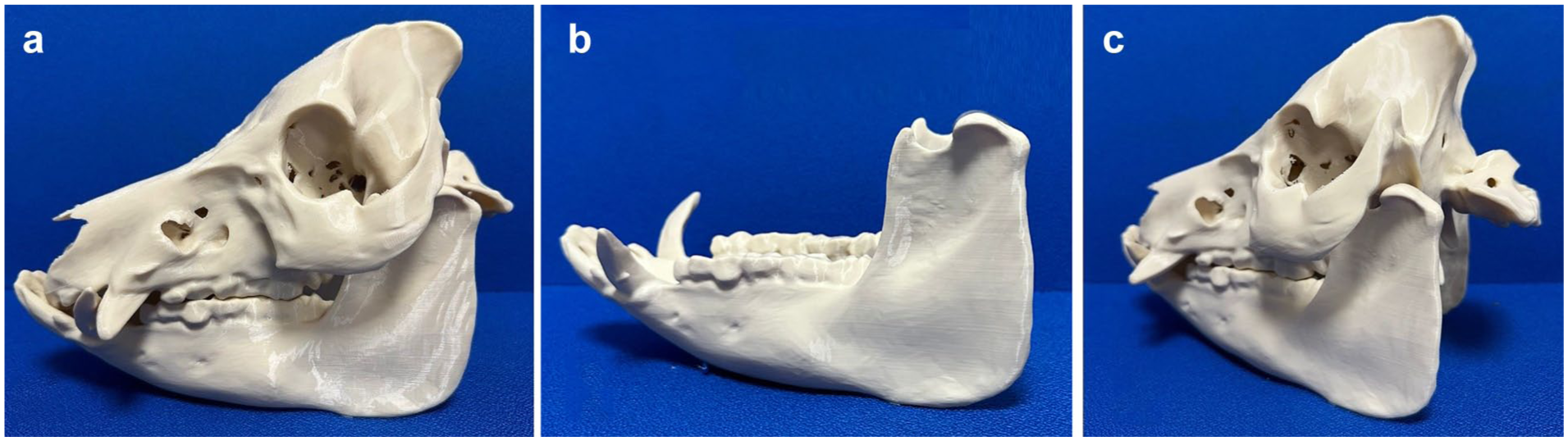
3D-printed model showing bony structures of the temporomandibular joint (TMJ). Differences between the bone structure of pigs and that of humans. (a) Lateral view: broad zygomatic arch forming a lateral wall over the TMJ. (b) Mandibular view: larger condylar neck and smaller coronoid process. (c) Caudal view: absence of a well-defined mandibular fossa due to the absence of retroarticular process.
TMJ injection
Intra-articular injection using the caudal approach was successfully achieved in all three tested joints. In each case, methylene blue was confined to the TMJ cavity, with homogeneous diffusion observed after dissection. The passive displacement of the needle during mandibular distraction confirmed correct intra-articular positioning, demonstrating the reproducibility and reliability of this technique in the porcine model. A schema of the technique and the result post-injection are presented in Figure 5.
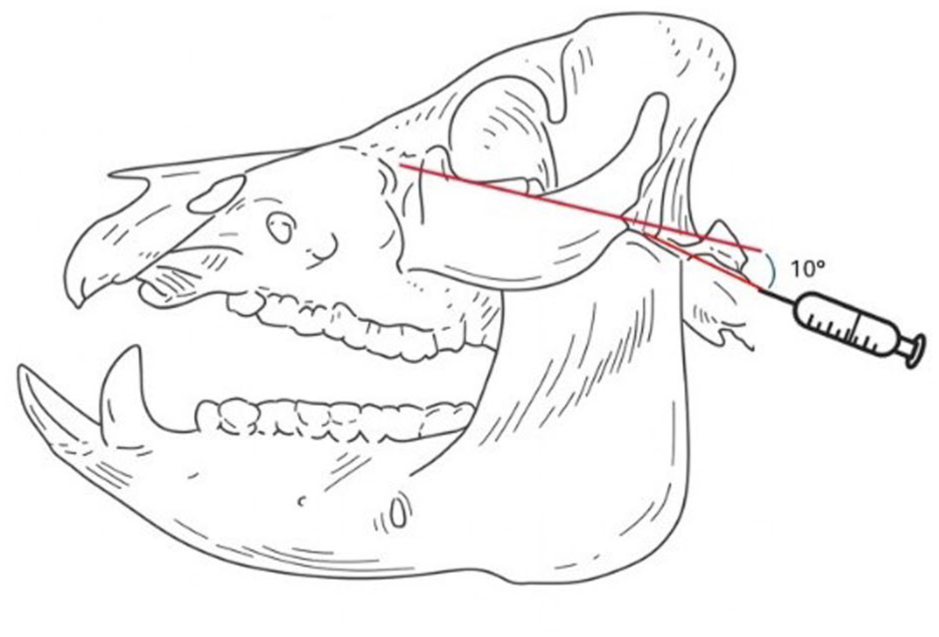
Injection of the temporomandibular joint, according to the technique of Wang et al. 8
Surgical approach of the pig TMJ
Retromandibular approach
The pig was positioned in lateral decubitus, with the head aligned with the body. A retromandibular incision with preauricular extension was made, creating an rostral hinge. The incision was performed through the skin and subcutaneous fatty tissue, followed by a subcutaneous dissection to expose the platysma layer and the parotidoauricularis muscle. The platysma muscle was gently retracted downward with a retractor. The zygomatic arch was easily identified by palpation. Bony contact could be felt in the caudal third of the zygomatic arch with the tip of the scissors through the fibrous pad covering the bone. A small incision could be safely made here, as no critical structures were present in this area. A subperiosteal dissection was then performed toward the TMJ to expose the articular capsule, taking care to avoid entry into the orbit, which was nearby. The capsule was then opened on its posterolateral part with an X-shaped incision, allowing exposure of the condylar head, the disc and the mandibular fossa. The subperiosteal dissection could be extended along the mandibular ramus as needed for further exposure. Two malleable blade retractors were placed on each side of the condylar neck to enable a controlled caudal translation, thereby facilitating lateral exposure. The bony section was performed using a saw or burr. The condyle was pulled with forceps but remained attached by the lateral pterygoid muscle, which was then cut to allow condyle removal. Closure was performed layer by layer. After the procedure, the initial incision was extended to perform a facial nerve dissection to verify its integrity, with no nerve or vessel damage observed. The technique is illustrated in Figure 6.
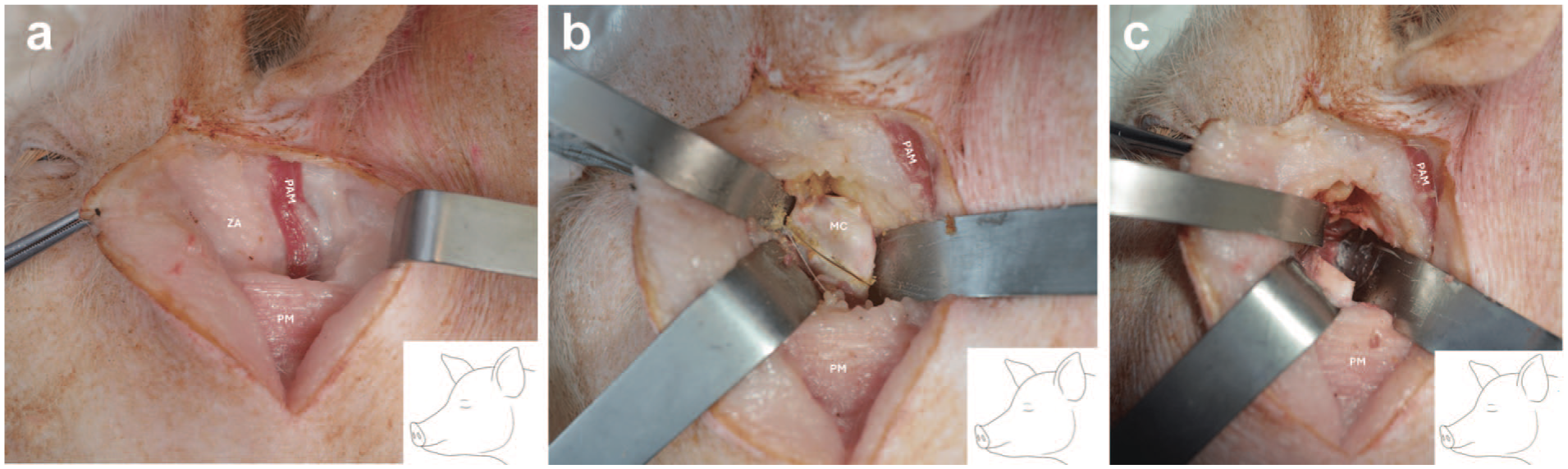
Surgical approach of the temporomandibular joint. (a) Subcutaneous dissection exposing the caudal part of the zygomatic arch (ZA), the platysma muscle (PM) and the parotidoauricularis muscle (PAM). (b) View of the mandibular condyle (MC) after surgical section following capsular opening. (c) Operative view after the condylectomy.
Mini-invasive retromandibular approach
The initial retromandibular incision could also be made shorter for minimally invasive procedures. The condylectomy was completed without any complications.
Subangular approach
The animal was positioned as previously described. A skin incision was made 1 cm below the palpable margin of the angular region, and the underlying platysma muscle was identified through a subcutaneous dissection. The platysma was then incised above the mandibular angle, exposing the fascia of the masseter muscle. The masseter was sharply dissected with scissors down to the bone surface. The cortical bone of the mandibular ramus could then be easily exposed using a raspatory. This approach provided full access to the mandibular ramus. The approaches are summarized in the Supplemental Data 2.
Discussion
This study provides the first standardized and reproducible description of a surgical approach to the porcine TMJ. Our results confirm the feasibility of intra-articular access and condylar exposure while preserving key neurovascular structures. By characterizing the anatomical specificities of the pig model, this work establishes a reliable framework for translational applications ranging from minimally invasive procedures to reconstructive surgery.
The porcine TMJ displays several differences from human anatomy. The skin and platysma are thicker, and the parotidoauricularis muscle (absent in humans) serves as a reliable superficial landmark since all critical structures lie beneath it. 11 Unlike in humans, the facial nerve does not traverse the parotid gland but runs along its deep surface, facilitating gland removal. 12 Bony differences, including the absence of a retroarticular process and a broad zygomatic arch providing lateral coverage, necessitate a caudal rather than lateral surgical access to the condyle. 13 Recent veterinary anatomical work has described the porcine TMJ as being reinforced by three individualized capsular ligaments (lateral, caudo-medial and caudo-lateral), with insertions involving the zygomatic process of the temporal bone and the mandibular neck. Although a ligamentous apparatus is also present in humans, including the lateral, stylomandibular and sphenomandibular ligaments, stabilization of the human TMJ is more commonly described as relying on a complex capsulo-discal system associated with a retrodiscal tissue zone that plays a major role in disc–condyle coordination during mandibular translation. 14 Concerning the TMJ disc, Kalpakci et al. 15 also reported that the pig represents the closest animal model to humans in terms of morphology, biochemical composition and mechanical properties. Regarding minipigs and farm pigs, no major differences in surgical exposure or anatomical landmarks were observed between the two groups. Despite differences in age and breed, overall body size and mandibular dimensions were comparable. The main noticeable difference concerned the thickness of subcutaneous adipose tissue and soft tissues, which was more pronounced in farm pigs, without impacting the feasibility or safety of the surgical approach.
Minimally invasive approaches to the TMJ are increasingly relevant for both clinical and experimental purposes owing to their potential to reduce surgical morbidity, preserve anatomical structures and promote faster functional recovery. Intra-articular injections enable evaluation of novel therapies such as drug delivery systems, injectable hydrogels, or regenerative biomaterials. 16 They also enable the development of pathological models; for example, osteoarthritis induction via intra-articular injection of monoiodoacetate has been successfully performed in rats and could be adapted to minipigs to create reliable large-animal models. 17 Our successful use of the caudal injection technique with methylene blue demonstrates that intra-articular access is both feasible and reproducible in pigs, supporting future therapeutic and disease-induction protocols, including osteoarthritis models.
The surgical procedure described here offers a safe and reliable approach for TMJ condylectomy, a procedure integral to several surgical techniques, including TMJ prosthesis replacement. This method allows for a systematic approach from the skin surface to the deep bony structures, making it a robust option for a range of TMJ surgeries. The facial nerve branches near the TMJ are safely accommodated in the initial steps of this approach, which remains above the platysma muscle. This ensures protection for the dorsal buccal branch, which runs beneath the platysma, several centimetres below its upper edge. The rostral auricular and zygomatic branches, located caudally to the TMJ, are also preserved owing to the rostral approach at the zygomatic arch and subsequent subperiosteal dissection. Additionally, our description of the vascular structures near the TMJ allows for an approach that avoids vein or artery ligation. The subangulomandibular and retromandibular approaches described here can be combined to provide wide exposure of the mandibular ramus. While such a combination is not necessary for a simple condylectomy, it could prove useful in more complex TMJ surgeries.
Recent research has demonstrated the potential of the porcine TMJ model for high-level surgical innovation, with examples such as tissue-engineered vascularized TMJ reconstruction and biomaterial-based disc regeneration illustrating its broad applications from complex reconstructive surgery to regenerative therapies.18,19 However, despite the growing number of studies using the porcine TMJ for such advanced interventions, detailed and standardized descriptions of the surgical approach remain rare. In their study, Vapniarsky et al. illustrate surgical exposure of the joint but do not describe it in a reproducible step-by-step manner and appear to rely on a wide incision along the zygomatic arch with extensive soft tissue dissection. While effective for complex reconstructive procedures, such exposure might increase surgical morbidity and is not readily translatable to clinical human approaches, particularly for minimally invasive applications. By contrast, the retromandibular approach described in the present study was specifically developed to provide direct, reproducible and minimally invasive access to the porcine TMJ, exploiting the limited caudal bony coverage of the condylar head while avoiding unnecessary soft tissue or osseous disruption. To our knowledge, no study has reported implantation of a rigid alloplastic TMJ prosthesis in a porcine model, despite its anatomical similarity to humans and the recognized role of total joint replacement in clinical practice. Advances in patient-specific implants using 3D printing and computer-assisted design therefore represent a promising and unexplored field of research in this model.
Our findings are consistent with previous anatomical studies, while also highlighting the substantial variability of facial nerve branching in the porcine model. Millesi et al. 20 described up to five peripheral motor branches and proposed a classification based on ramification patterns, underlining the difficulty of establishing a unified nomenclature. Sasaki et al., 21 focusing on the lower face, identified only the buccal and cervical branches, whereas Aycart et al. 22 reported four main trunks based on proximal emergence without detailed distal dissection. Taken together, these discrepancies reflect the practical challenges encountered during surgical dissection and confirm that facial nerve identification in the pig is not straightforward. From a surgical and functional perspective, our dissections suggest that the dorsal and ventral buccal branches are the most consistent and clinically relevant branches, likely reflecting their predominant role in porcine mandibular and perioral function. In contrast, cranial branches appear more variable and less developed, which might be related to the comparatively limited role of facial mimicry in pigs compared with humans. Importantly, despite this anatomical variability, the proposed caudal surgical approach remains safe, as it is performed in a subperiosteal plane that avoids direct manipulation of the facial nerve branches. Regarding vascularization, Disuit 23 dissected vessels in the area to perform ear allotransplantation, reporting similar vascular structures in the TMJ region, although they described a rostral auricular artery arising as a tributary of the superficial temporal artery, which differs slightly from our findings and classical descriptions. 24
The main limitation of this study is its cadaveric design, which precludes assessment of intraoperative bleeding, postoperative healing and functional nerve outcomes. Future in vivo validation with neuromonitoring and postoperative evaluation will be required to confirm the safety and reproducibility of this approach.
Despite these limitations, this work provides the first standardized surgical description of porcine TMJ access, reducing variability between research teams and accelerating translational progress. By establishing a reproducible framework, it creates a robust platform for minimally invasive procedures, regenerative therapies and patient-specific prosthetic reconstructions, thereby strengthening the role of the pig model as a bridge between preclinical and clinical TMJ research.
Conclusion
Pigs are considered good models for TMJ research owing to anatomical similarities, though notable differences were observed, such as a less defined mandibular fossa, broad zygomatic arch and the presence of the parotidoauricularis muscle, which aids in safe dissection. The described surgical procedure ensures a safe approach to TMJ, preserving key facial nerve branches and avoiding vascular damage.
Supplemental Material
sj-docx-1-lan-10.1177_00236772261441431 – Supplemental material for Standardized surgical access to the porcine temporomandibular joint: Anatomical basis for translational research
Supplemental material, sj-docx-1-lan-10.1177_00236772261441431 for Standardized surgical access to the porcine temporomandibular joint: Anatomical basis for translational research by Jean-François Guignardat, Romain Nicot, Thomas Hubert and Florent Barry in Laboratory Animals
Footnotes
Acknowledgements
The authors gratefully acknowledge the technical team of the DHURE, whose support was essential for carrying out this work, and J. Masson and R. Van Huffel for their valuable assistance with the dissections.
Ethics approval and consent to participate
Not applicable. The study was performed on cadaveric specimens of S. scrofa domestica obtained postmortem from unrelated research projects, in compliance with Directive 2010/63/EU.
Consent for publication
Not applicable.
Author contributions
All authors contributed to all stages of the study. J.-F. Guignardat: conception, experimentation, manuscript drafting. F. Barry: conception, experimentation. R. Nicot: supervision, critical revision. T. Hubert: critical revision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
All data supporting the findings of this study are included in the article. Further details are available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.