
Abstract
Complete Freund’s adjuvant (CFA) is used in laboratory animals to stimulate strong immune responses. However, it can cause persistent local inflammation and tissue damage, raising welfare concerns. This scoping review aimed to (i) assess how frequently welfare-relevant outcomes are reported in CFA immunisation and antibody-production studies in mice, rats and rabbits; (ii) describe reported welfare-relevant outcomes and the methods used to assess them; (iii) chart CFA regimen details across studies; and (iv) summarise reported alternatives to CFA, including welfare comparisons where available. We followed a protocol registered in Systematic Reviews for Animals and Food and reported in accordance with PRISMA-ScR. We searched PubMed and Embase from 2015 onwards. Screening was conducted in two phases (title/abstract; full text) by one reviewer, with uncertainties resolved by a second reviewer. Data were charted on animal characteristics, CFA regimen details, welfare monitoring, reported local/systemic outcomes, analgesia/humane endpoints and comparator adjuvants. Of 1608 records screened, 689 were assessed at full-text level and 43 met inclusion criteria by reporting a welfare-relevant outcome (including ‘no adverse effects’): local outcomes were reported in 24/43 and systemic in 8/43; structured pain or behaviour monitoring occurred in 4/43 and formal scoring in 1/43 studies. Alternatives were evaluated in 32/43; in studies involving head-to-head comparisons with CFA (28/32), alternatives were more often better tolerated (22/28) than similar (6/28), with efficacy usually comparable or higher (31/32). Despite well-recognised welfare concerns with CFA, welfare-relevant outcomes are rarely reported. Standardised reporting of CFA regimens, welfare assessment methods and results is needed to support evidence-based refinement and comparison with alternatives.
Introduction
Adjuvants are used in immunology to enhance immune responses. Complete Freund’s adjuvant (CFA) is among the most potent adjuvants and is typically formulated as a water-in-oil emulsion containing heat-killed mycobacteria. 1 CFA is often described as providing strong immune stimulation and a ‘depot’ effect that prolongs antigen exposure. 2
CFA remains widely used in research, vaccine development and vaccine production despite well-recognised welfare concerns, including marked injection-site reactogenicity and occasional systemic adverse effects. These concerns are particularly relevant given the continued use of large numbers of animals for antibody production, estimated at approximately one million animals per year in the European Union alone. 3 CFA activates innate immune responses, which might lead to persistent inflammation and tissue damage, with associated pain and distress. Reported adverse effects include swelling, ulceration or necrosis, sterile abscesses, and granulomatous lesions in draining lymph nodes. In some cases, similar lesions have been observed in distant organs, consistent with dissemination of emulsion material.4–9 Minimising such adverse effects through adjuvant selection and regimen design is therefore a key refinement consideration aligned with the 3Rs.1,10
Regulatory and institutional guidance generally emphasises that CFA use should be justified, limited and replaced where feasible. For example, the NIH Office of Animal Care and Use as well as multiple US university Institutional Animal Care and Use Committee policies advise using alternatives whenever possible and typically limiting CFA to primary immunisation, with incomplete Freund’s adjuvant (IFA) preferred for subsequent boosting unless repeating CFA is specifically justified and approved. 11 Similarly, the Swiss Federal Food Safety and Veterinary Office technical information recommends selecting the lowest-burden adjuvant compatible with the scientific objective and notes that adverse effects depend on factors such as species, antigen, injection site and volume. 12 It also discourages repeated CFA and recommends boosters without adjuvant or with lower-burden alternatives.
Although pathology summaries and narrative reviews describe CFA reactogenicity, 1 the contemporary literature has not been systematically mapped with respect to how often welfare-relevant outcomes are reported in CFA immunisation and antibody-production studies, how these outcomes are assessed and which alternatives have been evaluated alongside CFA. To address this knowledge gap and support evidence-based refinement, we conducted a scoping review to: (i) assess how often welfare-relevant outcomes are reported in CFA immunisation and antibody-production studies in mice, rats and rabbits; (ii) describe and categorise reported welfare-relevant outcomes and the methods used to assess them; (iii) chart CFA regimen details across studies; and (iv) summarise reported alternatives to CFA, including head-to-head welfare comparisons where available.
Materials and methods
Protocol and reporting
This scoping review was conducted according to a predefined protocol registered in the Systematic Reviews for Animals and Food (SYREAF) submitted prior to data extraction (accessible at SYREAF: URL). Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) guidelines 13 were followed, although some adaptations were made considering that PRISMA-P was developed for systematic reviews. The protocol is provided as Supplemental material 1 online (and is also available via BORIS: BORIS link). Reporting followed the PRISMA extension for Scoping Review (PRISMA-ScR) guidelines; 14 the PRISMA-ScR checklist is provided as Supplemental material 2.
Review question and eligibility criteria
The review question was framed using the PICo framework: what are the reported welfare-relevant outcomes of CFA use in laboratory animals?
Population (P): mice, rats, rabbits; the population was restricted a priori to mice, rats and rabbits to maintain a focused and methodologically comparable evidence base within the main mammalian laboratory species relevant to CFA immunisation and antibody-production settings. Other species, including guinea pigs and larger laboratory animals, might also be relevant in specific contexts, but were outside the predefined scope of this review.
Interest (I): animal welfare; for this review, animal welfare was defined as the state of an animal in relation to its attempts to cope with experimental conditions and their consequences. 15 Accordingly, eligible outcomes were limited to reported clinical signs, behavioural changes and macroscopic findings potentially indicating pain, distress, suffering, impaired health or reduced well-being after CFA administration.
Context (Co): CFA use in immunisation and antibody-production models.
The following eligibility criteria were used: (i) publication year ⩾ 2015 to capture contemporary welfare evidence together with current standards in husbandry, veterinary care and adjuvant formulation; (ii) English language; (iii) peer-reviewed original experimental research; (iv) species: mice, rats, rabbits; (v) context: immunisation and antibody-production models (disease and pain-induction models excluded); (vi) exposure: administration of CFA, including primary and/or booster injections. Studies in which Freund’s adjuvant was incompletely specified were also included when CFA use could be inferred from the immunisation protocol.
All studies meeting the population, context and exposure criteria proceeded to full-text screening. For data extraction, we included only studies that reported at least one welfare-relevant outcome, including explicit statements of ‘no adverse effects’. Studies that reported no welfare-relevant outcomes were retained to quantify non-reporting, defined as the absence of any explicit welfare-relevant outcome attributable to CFA in the available report.
Information sources and search strategy
Concluding electronic searches were performed in PubMed and Embase on 2 October 2025. The search strategy combined terms for laboratory animals (mice, rats, rabbits/leporidae), immunisation or antibody production, and CFA. The Boolean operator ‘AND’ was used to combine these three conceptual groups in order to retrieve records at their intersection. Searches were conducted using both free-text terms (title/abstract) and controlled vocabulary (MeSH in PubMed; Emtree in Embase). The full search strategies as run in each database are provided in Supplemental material 1. No additional sources were searched.
AI-assisted workflow and verification
ChatGPT (OpenAI; GPT-5.2 Thinking) was used with standardised prompts (Supplemental material 1) to support text identification, retrieval and organisation during screening and data extraction. Specifically, ChatGPT was used to (i) locate and compile potentially relevant passages within full texts, (ii) provide non-binding include or exclude suggestions, and (iii) generate paper-specific preliminary extraction tables containing verbatim quotes and citation details to facilitate rapid navigation to the original context. ChatGPT outputs were used only as aids to navigation and organisation; eligibility decisions were made by human reviewers according to the screening procedure described below. Data included in the final dataset were manually verified against the original full texts. Subsequently, one of the reviewers manually compiled the final consolidated extraction table across all included papers, using the ChatGPT-generated paper-specific tables only to locate the relevant source text.
Study selection
References were imported into Rayyan (Link) for deduplication and title and abstract screening. Screening was conducted in two phases (title/abstract and full text). During title and abstract screening, a high-sensitivity approach was adopted such that uncertain records were retained for full-text assessment.
Calibration exercises were conducted for both title and abstract screening (20 randomly selected articles) and for full-text screening (five randomly selected articles). The calibration exercises consisted of a screening by two reviewers followed by a discussion. They ensured that the screening process was standardised and helped to identify features in the screening process that required adaptations.
A single-reviewer approach was used for screening for both title/abstract and full-text screening. All uncertainties were flagged for review by a second reviewer and resolved through discussion. In addition, a second reviewer checked a 10% subset of full-text screening decisions.
Data extraction (data items)
Data extraction was conducted manually in Microsoft Excel using a predefined extraction form (Supplemental material 3). A reviewer manually compiled the final consolidated extraction table across all included papers, using the ChatGPT-generated paper-specific tables only to locate the relevant source text.
Key data domains included animal characteristics, CFA regimen details, welfare monitoring and outcomes, analgesia and humane endpoints, and comparator adjuvants. All extracted items were verified against the original source articles to ensure accuracy.
Welfare-relevant outcomes were extracted verbatim. Reported clinical signs, behavioural changes and visible pathological findings were considered welfare-relevant regardless of whether the original authors explicitly described them as welfare concerns or reported observable disturbance in the animals.
Synthesis
Extracted variables were summarised using descriptive statistics (counts and frequencies) and qualitative welfare-relevant outcomes were synthesised using thematic grouping.
Results
Study selection
The literature search identified 1848 records (PubMed, n = 567; Embase, n = 1281). After removal of 240 duplicates, 1608 unique records were screened at title and abstract level and 753 were sought for full-text retrieval. Sixty-four records could not be retrieved, leaving 689 studies assessed for eligibility. Of the 689 full texts assessed for eligibility, 43 met all inclusion criteria—namely, CFA immunisation or antibody-production studies reporting at least one welfare-relevant outcome, including explicit statements of ‘no adverse effects’—and were included for detailed data extraction (Figure 1).
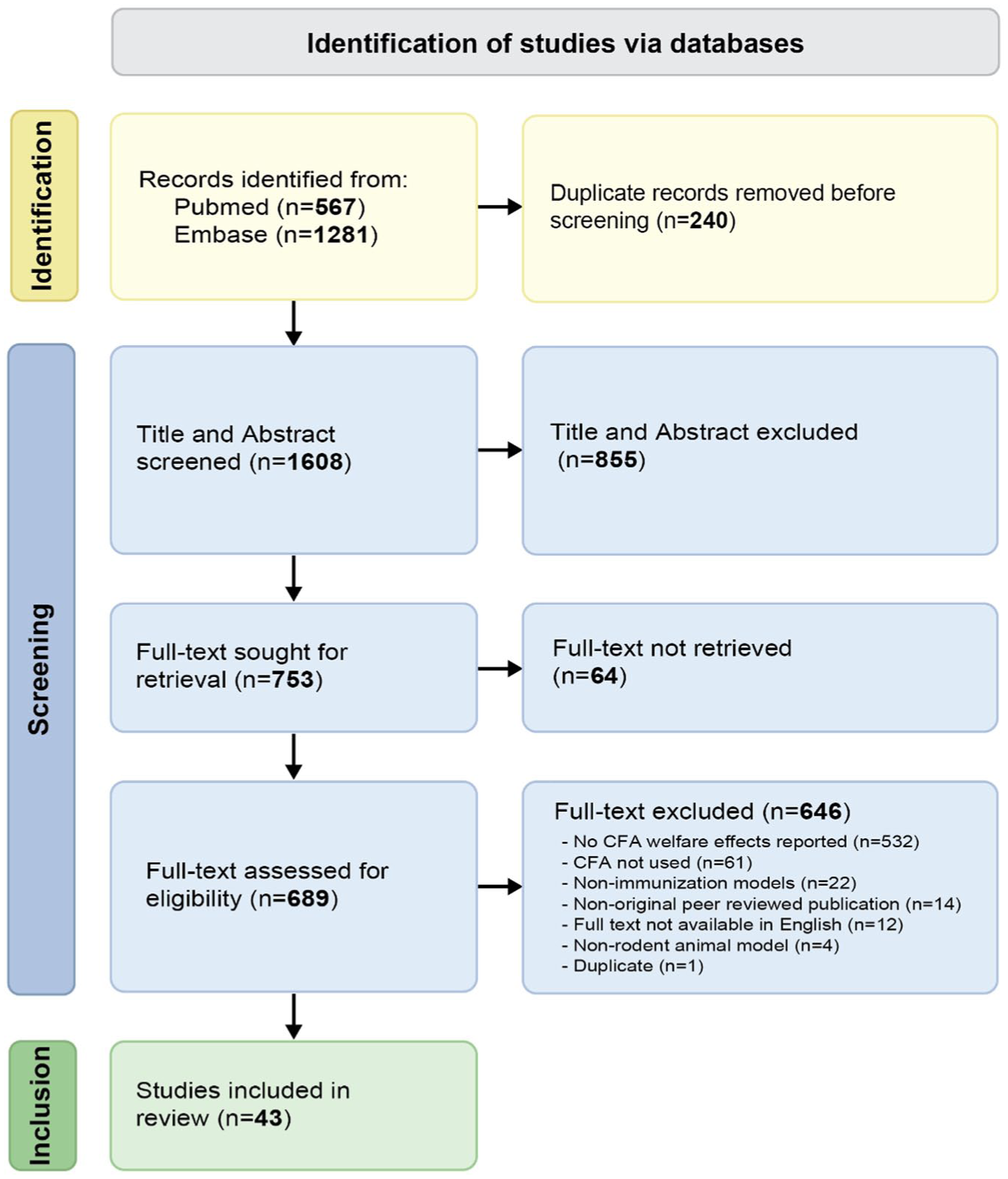
PRISMA-ScR flow diagram of study selection.
The remaining 646 full texts were excluded for the following reasons: non-reporting of welfare-relevant outcomes (n = 532; classified as non-reporting), absence of CFA use (n = 61), non-immunisation models (n = 22), non-original peer-reviewed publication (n = 14), full text not available in English (n = 12), wrong animal species (n = 4) and duplicate publication (n = 1).
Characteristics of included studies
Of the 43 studies included (Table 116–58), 38 used CFA in mice and five in rabbits; none involved rats. In the 38 mice studies, BALB/c (25/38) and C57BL/6 (10/38; including one genetically modified C57BL/6 model) were the predominant strains, while ICR, Kunming and Swiss albino stocks were each used in 1/38 studies. Among rabbit studies, New Zealand White was most common (4/5), with strain unreported in 1/5 studies. Most studies used female animals (35/43), with fewer using males (4/43) or mixed sexes (1/43); sex was not reported in 3/43 studies. Animal age was reported in 36/43 studies, most commonly 6–8 weeks (20/43), followed by ⩽6 weeks (9/43) and >8 weeks (7/43); age was not reported in 7/43 studies.
Overview of included immunisation and antibody-production studies using complete Freund’s adjuvant (CFA) and reporting welfare-relevant outcomes.
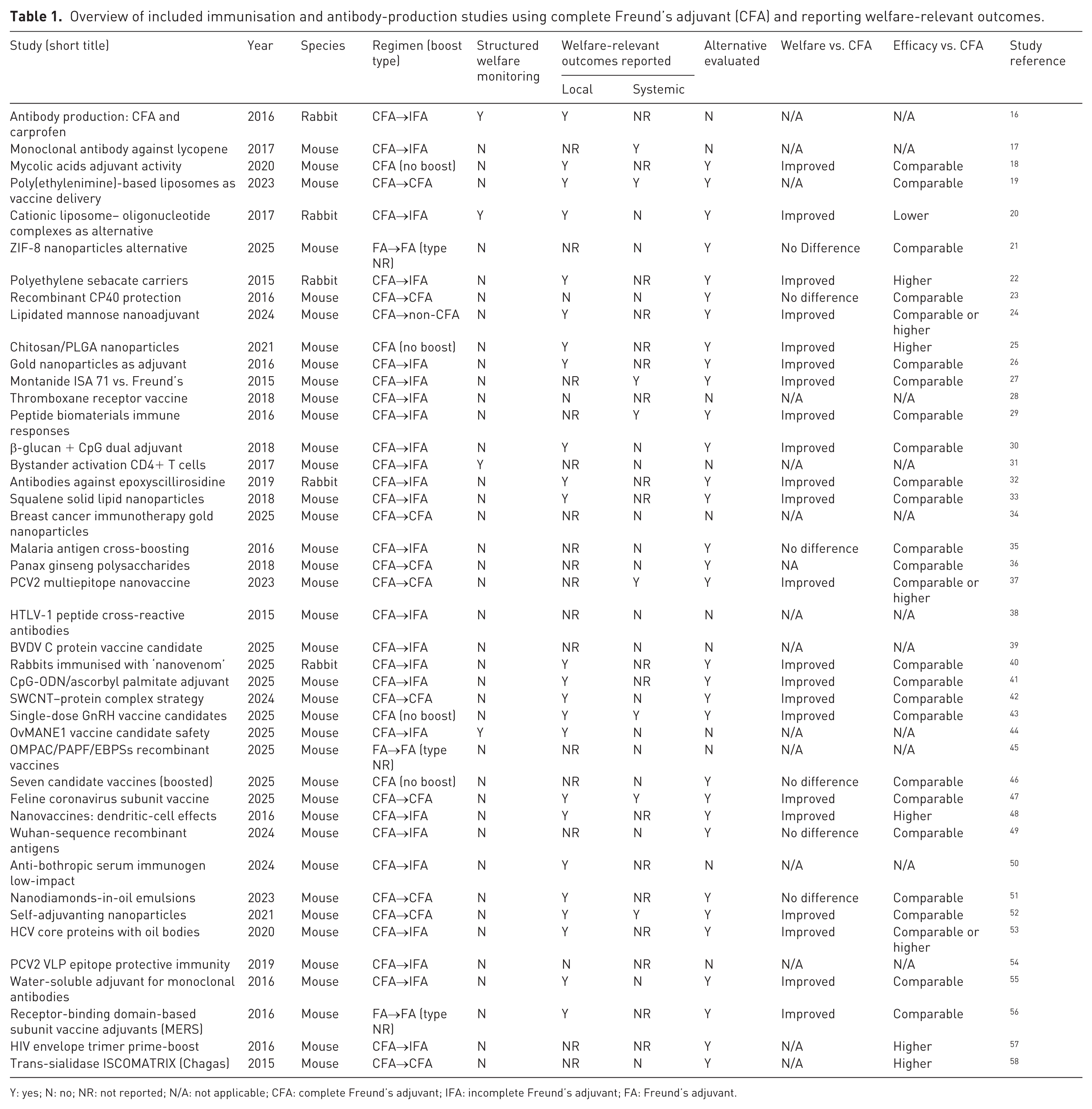
Y: yes; N: no; NR: not reported; N/A: not applicable; CFA: complete Freund’s adjuvant; IFA: incomplete Freund’s adjuvant; FA: Freund’s adjuvant.
CFA administration characteristics
Prime–boost adjuvant regimens
The most common regimen was CFA for priming followed by IFA for booster immunisations (25/43 studies). Repeated use of CFA for both priming and boosting was reported in 10/43 studies. Four studies used CFA for priming without subsequent boosters, and one study used CFA for priming with subsequent injections using a different (non-CFA) adjuvant. In three studies, ‘Freund’s adjuvant’ was reported for both priming and boosting without specification of complete versus incomplete formulations (Table 1).
Administration routes
CFA-based immunisations were most commonly administered via the subcutaneous route (27/43 studies). Intraperitoneal administration was reported in 6/43 studies, while intradermal and intramuscular routes were reported in 2/43 studies each. One study reported intradermal administration combined with footpad injection. In four studies, administration route varied across immunisation stages (e.g. priming versus boosting) and/or across study arms. Route of administration was not reported in 1/43 studies.
Injection sites
Injection site was not reported in 24/43 studies. Among studies reporting a site, administration commonly involved dorsal regions (e.g. dorsum or dorsal skin, sometimes distributed across multiple injection sites) and the tail base. Tail base administration was explicitly reported in 6/43 studies (including studies specifying two tail-base sites and/or tail-base booster injections). Other reported sites included hind footpads, ear, neck and thigh/quadriceps. In three studies, multiple injection sites were reported without specifying the anatomical location.
Number of injections
The number of immunisations per study most commonly comprised three injections (24/43 studies). Fewer studies used one (4/43), two (6/43), four (3/43) or five injections (2/43). In four studies, the number of injections was reported as a range, differed by trial or varied by study arm, including one heterologous schedule in which the initial immunisation used CFA and subsequent injections used a different adjuvant.
Timing of injections
Booster spacing most commonly followed biweekly (18/43 studies) or three-weekly intervals (9/43 studies), with other or mixed intervals in 12/43 studies with ⩾2 injections; 4/43 studies reported a single immunisation only.
Injection volume
Injection volume was reported in 31/43 studies (not reported: 12/43) and ranged from 30 µl to 1000 μl. In mice, reported volumes were typically 100–200 μl (18/38 studies), with other volumes less common. In rabbits, 1000 μl was frequently reported (3/5), including studies in which comparator (non-CFA) arms used different volumes (e.g. 300 μl or 3000 μl).
Emulsion preparation
The antigen–adjuvant emulsion ratio was reported as 1:1 in 25/43 studies, while the emulsion ratio was not reported in 18/43 studies.
Reported welfare outcomes and assessment approaches
Monitoring and assessment approaches
Structured monitoring of pain or behavioural indicators was reported in 4/43 studies. Only one study used a formal scoring approach (an in-house rabbit health ABCD scale); the remaining studies either reported non-specific clinical monitoring (e.g. general condition, clinical signs, body weight or after challenge) or did not describe monitoring at all (25/43). Welfare-relevant outcomes were primarily documented through narrative observations, and none applied validated or quantitative tools (e.g. grimace scales, validated pain scores, behavioural assays or predefined clinical scoring systems).
Local adverse effects
Local injection-site welfare-relevant outcomes were reported in 24/43 studies. Three studies explicitly reported no local adverse effects.
Types of local adverse effects
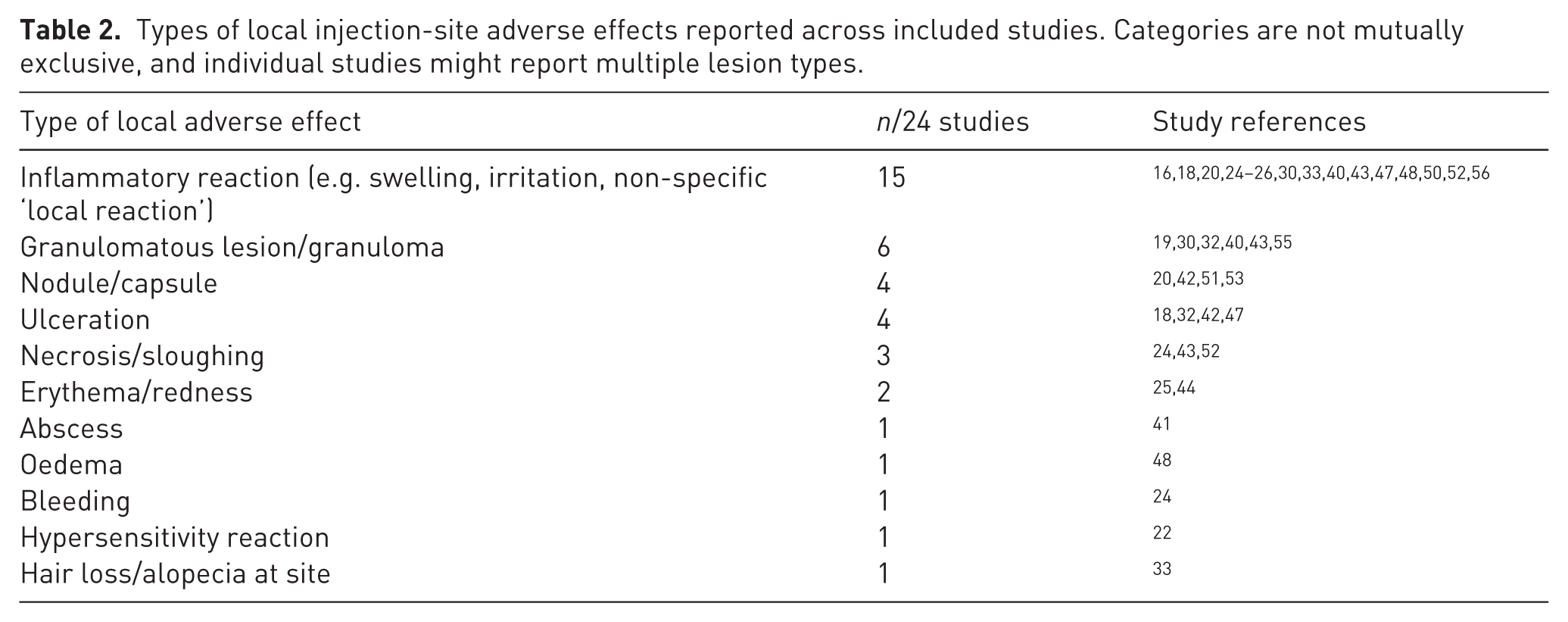
Among the 24 studies reporting local injection-site effects (Table 2), inflammatory reactions (including swelling, irritation or non-specific ‘local reactions’) were most frequently described (15/24). Granulomatous lesions were reported in 6/24 studies, while nodules/capsules, ulceration, and necrosis/sloughing were each reported in 3/24 studies. Less commonly reported local outcomes included erythema/redness (2/24) and abscesses, oedema, bleeding, hypersensitivity reactions and hair loss (each 1/24). Lesion-type categories were not mutually exclusive. Qualitative descriptors of severity (e.g. ‘mild’, ‘low-grade’, ‘severe’) were used inconsistently and without standardised definitions or timepoints, precluding reliable synthesis of severity across studies.
Types of local injection-site adverse effects reported across included studies. Categories are not mutually exclusive, and individual studies might report multiple lesion types.
Systemic effects
Systemic welfare-relevant outcomes were reported in 8/43 studies, while 17/43 studies explicitly reported no systemic adverse effects.
Types of systemic effects
Among the eight studies reporting systemic welfare-relevant outcomes, reports were narrative and heterogeneous. Severe outcomes were described in five studies, including mortality (3/43) and euthanasia or poor clinical condition requiring euthanasia (2/43). Other reported systemic or general effects were non-specific and included ruffled fur with reduced mobility or slower recovery (1/43), delayed wound healing (1/43), visible discomfort (1/43) and reduced physical activity (1/43). Categories were not mutually exclusive and reporting detail was limited.
Alternatives to CFA and comparative findings
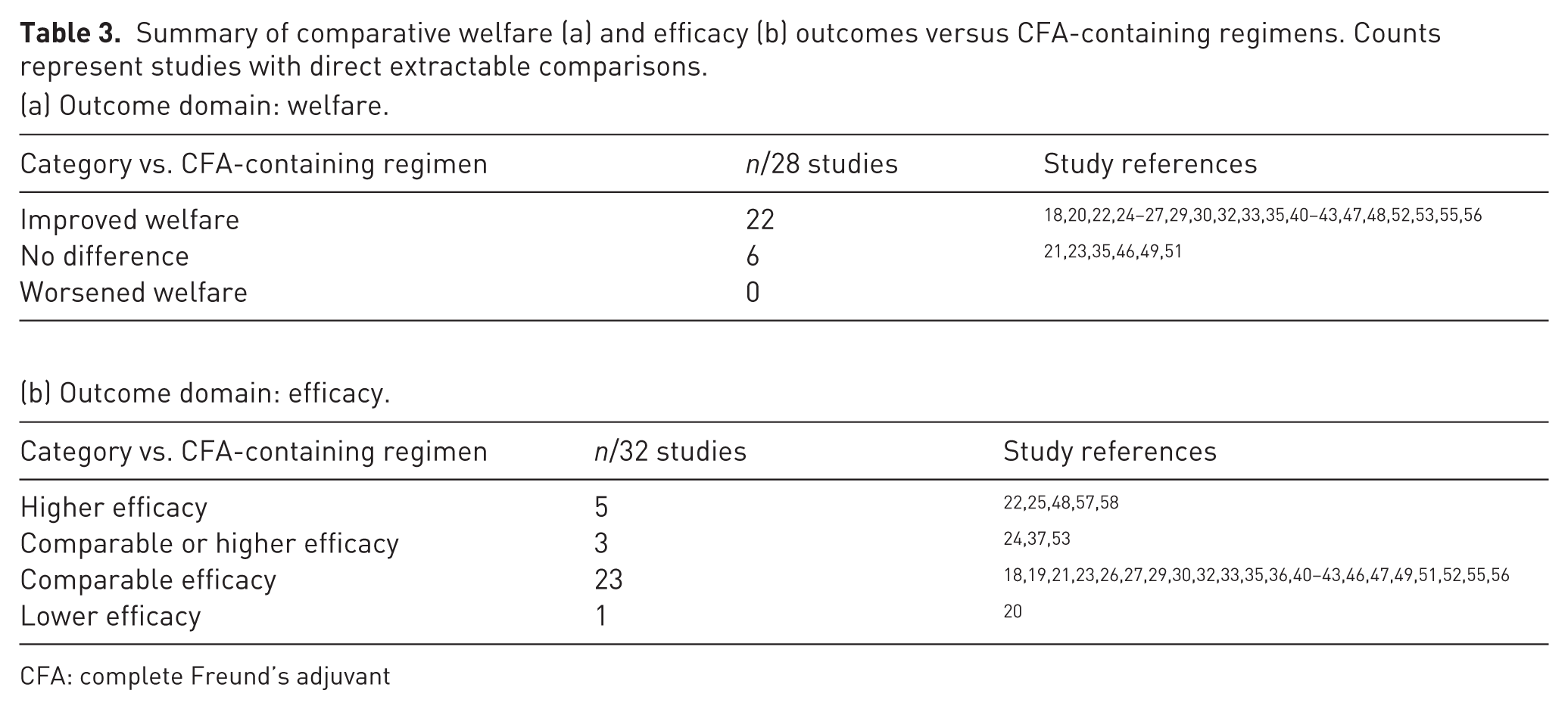
An alternative adjuvant component or delivery approach was evaluated in 32/43 included studies. Among these, 28/32 studies reported welfare-relevant outcomes in a manner that enabled head-to-head comparison with a CFA-containing regimen, whereas 4/32 did not provide direct welfare comparisons between CFA and the alternative. Where a head-to-head welfare comparison between an alternative formulation and a CFA-containing regimen was available (28/32), alternatives were more frequently reported as having improved welfare outcomes (22/28 studies) than similar welfare outcomes (6/28 studies) (Table 3).
Summary of comparative welfare (a) and efficacy (b) outcomes versus CFA-containing regimens. Counts represent studies with direct extractable comparisons.
(a) Outcome domain: welfare.
CFA: complete Freund’s adjuvant
Secondary outcome: reported immunogenicity or efficacy
Although this review focused on welfare-relevant outcomes, studies that evaluated alternative formulations often also reported immunogenicity or efficacy endpoints for contextual comparison. Efficacy was most frequently reported as comparable to CFA-containing regimens (23/32 studies), with a further 3/32 studies reporting efficacy as comparable or higher. Higher efficacy relative to CFA was reported in 5/32 studies, while lower efficacy was reported in 1/32 studies. Efficacy comparisons were not applicable in 11/43 studies because no alternative or comparator arm was included (Table 3).
Identified alternatives to CFA
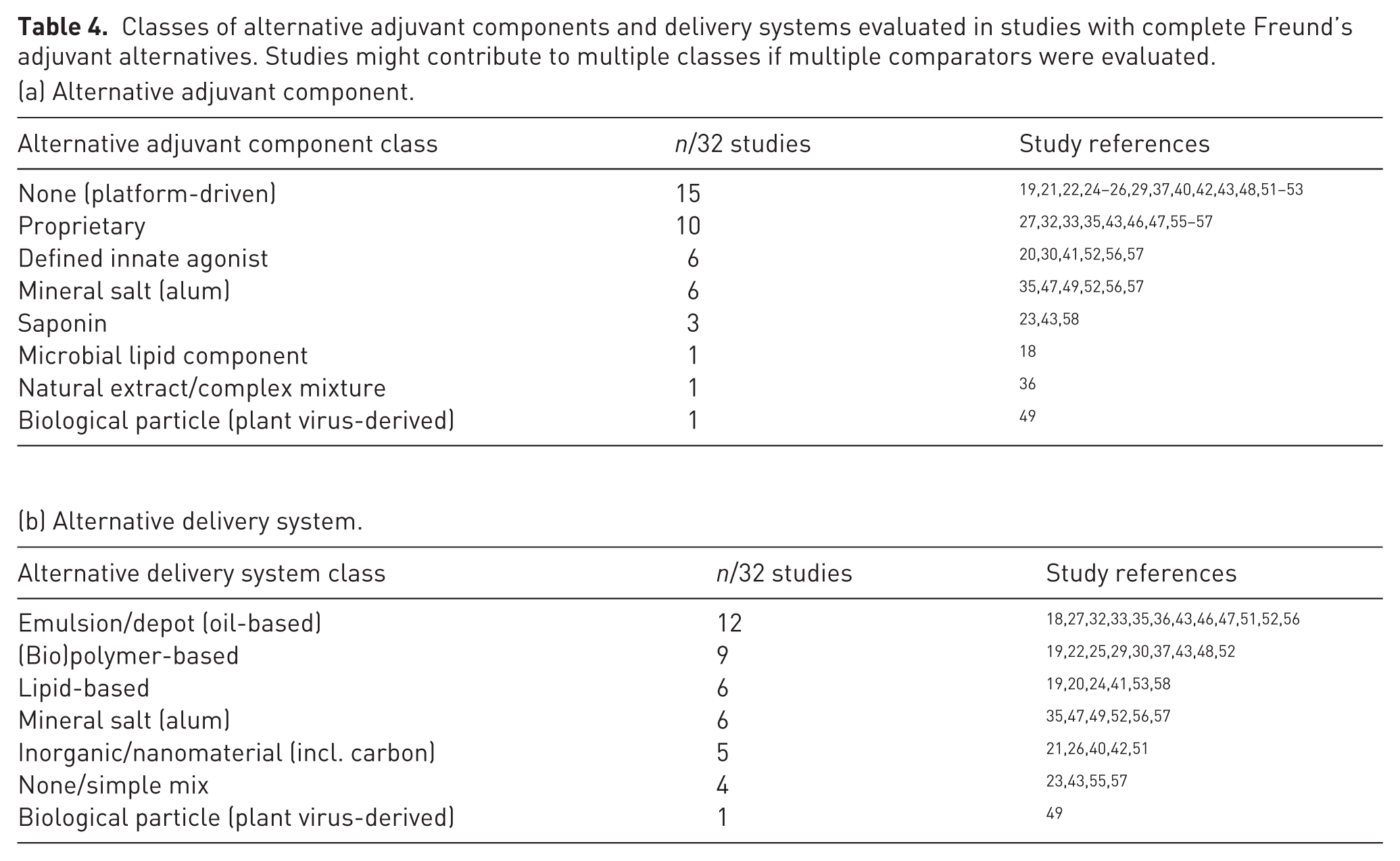
The evaluated alternatives comprised (i) alternative adjuvant components (immunostimulatory ingredients) and (ii) alternative delivery systems (formulation platforms that package and present antigen). Across the 32 studies with an alternative, the most common adjuvant strategy was platform-driven immunostimulation (15/32 studies), meaning no separate immunostimulatory component was added and any adjuvant effect was attributed to the formulation platform itself. Where specific alternative adjuvant components were used, these included proprietary formulations (10/32), defined innate agonists (6/32), mineral salts (alum) (6/32) and saponin-based adjuvants (3/32). Microbial lipid components (1/32) and natural extract or complex mixtures (1/32) were each evaluated in a single study. Regarding delivery systems, oil-based emulsions or depot formulations were most frequent (12/32 studies), followed by (bio)polymer-based platforms (9/32), lipid-based platforms (6/32), mineral salt (alum) depots or particles (6/32) and inorganic or nanomaterial platforms (5/32). None/simple mix (4/32) and biological particle delivery (1/32) were uncommon (Table 4).
Classes of alternative adjuvant components and delivery systems evaluated in studies with complete Freund’s adjuvant alternatives. Studies might contribute to multiple classes if multiple comparators were evaluated.
(a) Alternative adjuvant component.
Refinement measures and morbidity/mortality
Reporting of welfare mitigation measures was rare. One included study reported administration of a non-steroidal anti-inflammatory drug (carprofen) alongside an CFA-based immunisation protocol in rabbits; carprofen did not appear to reduce inflammation in the examined tissues, as reported by the authors. Morbidity/mortality was reported in a small number of studies: two studies reported euthanasia of a mouse (limited details reported). Mortality was reported in three studies and was described in CFA-containing groups; one study reported 2/5 mice died in the CFA group, one study reported that mice became sick and subsequently died in two experimental groups without specifying the number of deaths and one study reported one dead mouse. Descriptions suggested an association with CFA-based immunisation in these reports; however, details on timing and cause were inconsistently reported, limiting attribution.
Discussion
Summary of evidence
This scoping review examined reporting of welfare-relevant outcomes in peer-reviewed CFA immunisation and antibody-production studies in mice, rats and rabbits (2015–2025). Because many otherwise eligible studies did not report welfare-relevant outcomes, the findings primarily reflect reporting practices rather than the overall frequency or severity of CFA-associated effects.
Across 43 included studies, welfare reporting was mostly narrative and inconsistently detailed. Local injection-site effects were reported more often than systemic outcomes. Structured pain or behaviour monitoring was rare and no validated assessment tools were used. In head-to-head comparisons, alternatives to CFA were often reported as better tolerated, with similar or higher efficacy.
Overall, limited and unstandardised welfare assessment and reporting restricts cross-study comparison and weakens the evidence base for refinement decisions. Clearer, more consistent reporting would improve transparency and align with existing guidance on welfare monitoring and adverse event reporting. 59 Generalisability is also limited, as most studies used female BALB/c or C57BL/6 mice and New Zealand White rabbits.
CFA regimens and reporting gaps
CFA administration varied substantially across studies, including prime–boost design, route, injection site, number and timing of injections and injection volume. This heterogeneity likely contributes to variation in reactogenicity, consistent with evidence that tolerability is influenced by protocol features as well as adjuvant choice. 5
Interpretation and reproducibility were further constrained by missing key regimen details. Injection site was unreported in 24/43 studies, injection volume in 12/43 and emulsion ratio in 18/43; three studies did not specify whether ‘Freund’s adjuvant’ was complete or incomplete at each stage. These omissions affect reproducibility and scientific validity and intersect with broader ‘3Vs’ considerations alongside the 3Rs. 60 They also conflict with ARRIVE 2.0 expectations for transparent reporting of procedures and adverse events. 59
Most studies used CFA for priming followed by IFA for boosters (25/43), broadly aligning with recommendations to limit CFA exposure. 1 However, repeated CFA use for priming and boosting was reported in 10/43 studies, and in three studies the booster formulation was unclear. At minimum, future studies should state whether CFA or IFA was used at each immunisation step.
Welfare monitoring and assessment
Only 4/43 studies reported structured pain or behaviour monitoring, and only one used a formal score. As a result, it is often unclear whether observations reflected systematic monitoring or incidental observation. This limits interpretation of severity and duration, and statements such as ‘no adverse effects’ cannot be distinguished from limited monitoring.
Welfare-relevant outcomes reported
Local effects were diverse (inflammatory reactions, nodules or granulomas, ulceration, necrosis or sloughing, abscesses, oedema and other lesions), consistent with known CFA reactogenicity. 1 However, severity terms (e.g. ‘mild’ or ‘severe’) were used inconsistently and rarely linked to explicit criteria or timepoints, making it difficult to distinguish transient inflammation from persistent tissue damage.
Systemic outcomes were reported less often, but ranged from non-specific clinical signs to severe outcomes including euthanasia and mortality. Reports of severe outcomes often lacked detail on timing, progression, monitoring intensity and plausible alternative explanations, limiting causal interpretation.
Alternatives to CFA and implications for refinement
Alternatives were evaluated in 32/43 studies. Where head-to-head welfare comparison with CFA-containing regimens was possible (28/32), alternatives were more often described as better tolerated (22/28) than similar (6/28). Efficacy was usually comparable or higher (31/32).
These findings should be interpreted cautiously, given the limitations noted above, including incomplete reporting of administration parameters across comparator arms and non-standardised welfare assessment and reporting. Even so, the overall direction of comparative reporting supports a refinement message: head-to-head evaluation of alternatives is feasible and often suggests improved tolerability without apparent loss of efficacy.
Non-reporting in the wider eligible CFA literature
A notable finding was the extent of non-reporting: Among 575 studies (43 included + 532 with no CFA welfare effects reported; Figure 1) otherwise eligible by species, context and CFA use, only 43 (7%) reported any welfare-relevant outcome, whereas 532 (93%) did not.
Absence of reporting should not be interpreted as absence of harm. Rather, it likely reflects under-assessment and/or under-reporting, consistent with broader evidence on incomplete reporting of welfare information and analgesia in animal studies.61,62 This prevents a clear assessment of the extent of welfare impacts associated with CFA use and weakens the basis for evidence-based refinement, reinforcing the importance of ARRIVE 2.0 and related initiatives. 59
Reporting recommendations
To support reproducibility, cross-study comparisons, and refinement decisions, studies using CFA or comparing alternatives should report: (i) complete regimen details (species/strain, sex, age; antigen and dose; adjuvant formulation and amount per injection; route; injection site(s) and number of sites; volume per site; emulsion ratio and preparation; number and timing of injections; and any deviations from protocol) 59 ; (ii) predefined welfare monitoring and adverse-event reporting (timepoints, denominators, explicit event definitions and clinical course for high severity outcomes), ideally including quantitative pain or behaviour assessment where feasible, such as validated grimace scales for rodents and/or lagomorphs;63,64 combined with basic clinical metrics (e.g. body weight, coat condition, posture, mobility) in a predefined scoring sheet; 65 (iii) analgesia and humane endpoints (drug, dose, timing, rescue criteria and endpoint triggers); 66 and (iv) prospective planning frameworks (e.g. PREPARE) to embed monitoring and endpoints from the outset. 67
Where alternatives are compared, administration parameters should be standardised across arms and welfare endpoints prespecified to reduce confounding.
Limitations
A predominantly single-reviewer approach might increase the risk of missed eligible studies and extraction errors; this was mitigated through calibration exercises, discussion of uncertainties with a second reviewer and independent checking of 10% of full texts. The review was restricted to English-language peer-reviewed studies, and welfare information reported in non-standard formats might not have been captured during screening.
Conclusion
Welfare-relevant outcomes in CFA immunisation and antibody-production studies (mice, rats, rabbits; 2015–2025) were often not reported and when mentioned were usually described narratively. Across the 43 included studies, local injection-site effects were reported more often than systemic outcomes. Structured pain or behaviour monitoring was rare, and no studies used validated welfare assessment tools, leaving severity and duration poorly characterised and limiting cross-study comparability.
Accordingly, this review primarily maps welfare reporting practices rather than enabling robust inference about the underlying frequency or severity of CFA-associated impacts, which constrains the evidence base for refinement decisions.
Where alternatives were directly compared with CFA-containing regimens, they were more often reported as better tolerated, while efficacy was usually comparable or higher. However, incomplete reporting of administration parameters and non-standardised welfare assessment across comparator arms introduce uncertainty in these comparisons.
Overall, more systematic and transparent welfare monitoring and reporting—using clear definitions, denominators and timepoints (and validated tools where feasible)—is needed to strengthen the evidence base for refinement and improve evaluation of alternatives to CFA.
Supplemental Material
sj-pdf-1-lan-10.1177_00236772261459546 – Supplemental material for Complete Freund’s adjuvant in laboratory animals: Reported welfare-relevant outcomes and alternatives—a scoping review
Supplemental material, sj-pdf-1-lan-10.1177_00236772261459546 for Complete Freund’s adjuvant in laboratory animals: Reported welfare-relevant outcomes and alternatives—a scoping review by Valerie Hungerbühler, Agathe Verhulst, Cristian Berce, Otto Maissen, Beat Thomann and Luís Pedro Carmo in Laboratory Animals
Supplemental Material
sj-pdf-2-lan-10.1177_00236772261459546 – Supplemental material for Complete Freund’s adjuvant in laboratory animals: Reported welfare-relevant outcomes and alternatives—a scoping review
Supplemental material, sj-pdf-2-lan-10.1177_00236772261459546 for Complete Freund’s adjuvant in laboratory animals: Reported welfare-relevant outcomes and alternatives—a scoping review by Valerie Hungerbühler, Agathe Verhulst, Cristian Berce, Otto Maissen, Beat Thomann and Luís Pedro Carmo in Laboratory Animals
Supplemental Material
sj-xlsx-3-lan-10.1177_00236772261459546 – Supplemental material for Complete Freund’s adjuvant in laboratory animals: Reported welfare-relevant outcomes and alternatives—a scoping review
Supplemental material, sj-xlsx-3-lan-10.1177_00236772261459546 for Complete Freund’s adjuvant in laboratory animals: Reported welfare-relevant outcomes and alternatives—a scoping review by Valerie Hungerbühler, Agathe Verhulst, Cristian Berce, Otto Maissen, Beat Thomann and Luís Pedro Carmo in Laboratory Animals
Footnotes
Acknowledgements
We used ChatGPT (OpenAI; GPT-5.2 Thinking) to support text retrieval and organisation during screening and data extraction, including generation of preliminary, quote-supported extraction tables. All study selection decisions and all extracted data were determined by the reviewers and verified against the full-text publications.
Ethical considerations
Not applicable (scoping review of published literature).
Informed consent
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The review received funding from the Swiss Federal Food Safety and Veterinary Office. The funding agency did not influence the research results or the decision to publish.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.