
Abstract
Keywords
Medication abortion is a common experience for women in the United States. Since its approval by the U.S. Food and Drug Administration in 2000, medication abortion has increased to over 50% of all abortions (Jones et al. 2022). During a medication abortion, a woman consumes mifepristone, an antiprogestin, and then takes the misoprostol, a prostaglandin, 24 to 48 h later. Approximately 95%–99% of women who take both mifepristone and misoprostol successfully terminate their pregnancies within the first trimester (Gatter, Cleland and Nucatola 2015). Women have reported choosing medication abortion over surgical abortion in order to have a more natural abortion and/or maintain the privacy and convenience of being at home (Biggs et al. 2019; Swica et al. 2013).
Yet, we do not know why some women who initially begin a medication abortion decide within 72 h after taking mifepristone to seek abortion pill reversal (APR). Currently, more than 2,500 women have contacted the Abortion Pill Rescue Network to inquire about abortion pill reversal. The Abortion Pill Rescue Network is an international association of more than 1,000 medical providers (e.g., OB-GYNs, nurse practitioners) and pregnancy organizations who prescribe a progesterone protocol developed by Dr. Delgado and colleagues (Abortion Pill Rescue Network n.d.; Davenport et al. 2017; Delgado et al. 2018). Annual public reports on the number of women who have contacted the Abortion Pill Rescue Network show that 615 women started the progesterone protocol in 2019, 1461 women started the progesterone protocol in 2020, and 1688 women began the progesterone protocol in 2021 (Abortion Pill Rescue Network, personal communication, December 2, 2022).
Beyond these public reports, there is no evidence-based research on the experiences of women who begin a medication abortion and then choose to attempt to halt their abortion in order to continue their pregnancy. Thus, we sought to undertake the first exploratory analysis of this population to understand their experiences seeking medication abortion and abortion pill reversal. Because health care providers have a unique and significant role in women's decision-making and access to medication abortion and abortion pill reversal, we focused on this interaction for the purposes of this analysis. For example, women's expectations of pain, bleeding, and side effects are typically formed during patient counseling and the perceptions of the interpersonal care that they receive from medical providers (Swica et al. 2011; Darney et al. 2018). Across the health and social science scholarship, the quality of the physician-patient interaction is increasingly recognized as an essential component of providing effective medical care (Bieber et al. 2010). The fiduciary relationship between women and their providers is critical to maintaining positive objective (e.g., blood pressure, bleeding), behavioral (e.g., adherence to treatment, coping, recovery), and subjective health outcomes (e.g., knowledge, reported pain, satisfaction) (Chipidza, Wallwork and Stern 2015; Gordon and Beresin 2015, 1).
Although medical and public health leaders have argued against legislative interference with the doctor–patient relationship (Weinberger et al. 2012), abortion remains a biopolitical public health issue. As of September 2021, 14 states have passed abortion “reversal” laws, with 10 of those laws in effect (Charlotte Lozier Institute 2021, 7). The recent Dobbs decision has provided states with more latitude for legislation that will directly impact the relationship between women and their abortion providers. Thus, we sought to understand what messages women received from providers during their medication abortion and abortion pill reversal interactions, and then compare women's perceived quality of their interactions with their two different medical providers.
Methods
Study Design and Recruitment
After receiving IRB approval from a large, comprehensive research university in the Midwest, a recruitment letter with a link to an online Qualtrics survey was initially emailed to 3,076 women. Two follow-up emails were sent to remind women about the survey. These women contacted Heartbeat International between 2018 and 2022 to seek information about medication abortion reversal after taking mifepristone. The women had agreed to the organization contacting them in the future for research purposes. Of those women, 108 started completing the survey, and 67 met the eligibility criterion by reporting that they had completed the 2-week APR protocol. Thirty-three of the 67 women who completed the 2-week APR protocol (49%) filled out the scale on the quality of the physician-patient interaction (QQPPI) and decision difficulty scales and demographic questions.
When completing the survey, women were encouraged to finish it in one sitting, although the survey settings permitted interruptions and allowed participants to skip questions. These settings permitted women to regulate their own fatigue, difficult emotions, and time management. The survey included a combination of open- and closed-ended questions about women's experiences with taking mifepristone and then seeking a progesterone protocol, in addition to demographic questions. Ten respondents reported that they had not completed the 2-week protocol, five were in process, and 26 did not answer the question; these responses were excluded from the analysis.
Instruments
We used the 14-item scale on the quality of the physician-patient interaction (QQPPI) to assess women's perception of their interaction with the medication abortion provider who prescribed mifepristone and misoprostol, as well as the perceived quality of their interaction with the abortion pill reversal provider who prescribed the progesterone protocol. Each item was measured on a 5-point Likert scale (1 = I do not agree to 5 = I fully agree). The QQPPI is a brief, valid, and reliable patient self-report instrument that assesses the quality of the physician-patient interaction in outpatient settings (Bieber et al. 2010). This scale is independent of patient characteristics (i.e., age, education, gender) and is not confounded by social desirability or health status. Individual items were averaged to produce an overall score, with higher scores indicating better perceived communication with the medical provider.
Respondents’ perceptions of their difficulty in choosing to take mifepristone and their difficulty in choosing to take progesterone for abortion pill reversal were measured on a 5-point Likert scale (1 = Very difficult to 5 = Very easy).
Analysis
Women's responses to the two questions: “Please explain why you chose to take mifepristone compared to a surgical abortion. Please describe if there were certain people or messages that influenced this decision” and “Please explain why you chose to take progesterone to reverse the effects of mifepristone. Please describe if there were certain people or messages that influenced this decision” were analyzed using thematic analysis (Braun and Clarke 2006). Given the focus of this exploratory analysis, we only analyzed women's responses that specifically included information about communication with a medical provider.
Patient characteristics were analyzed using descriptive statistics. Differences between the QQPPI scales and decision difficulty scales were compared using paired t-tests.
Results
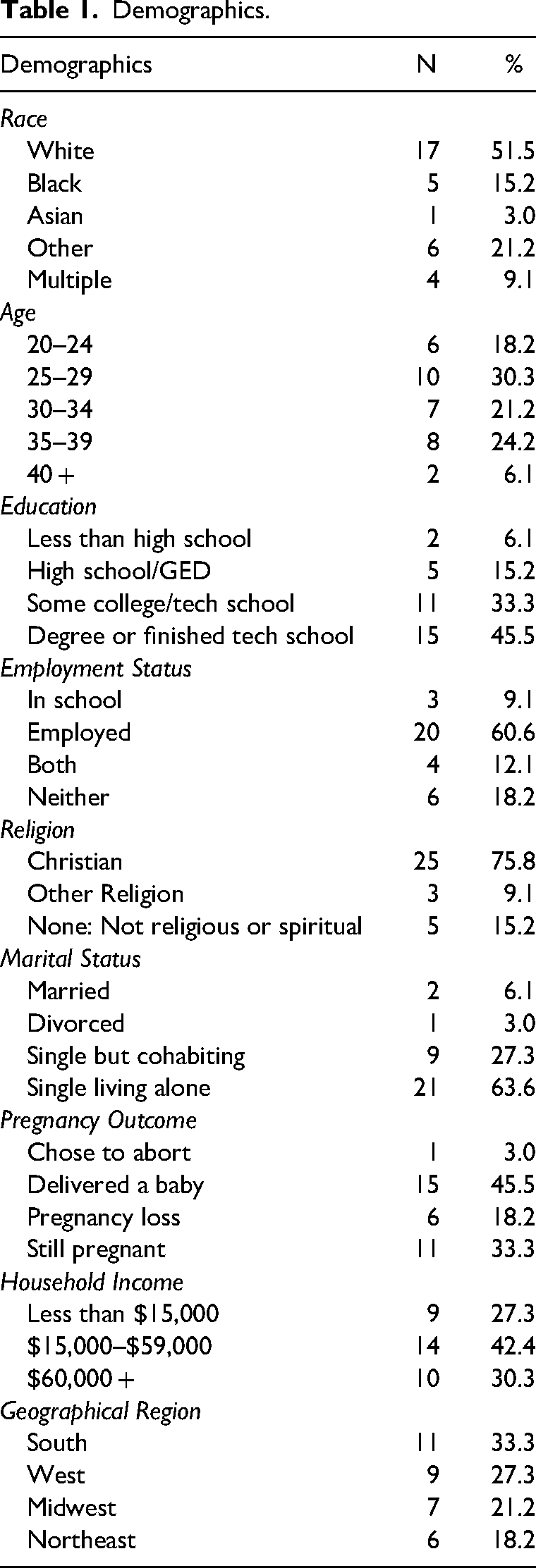
Most of the women were White (52%, n = 17), Christian (76%, n = 25), and unmarried (94%, n = 31) (Table 1). The mean age was 30 (SD = 6.27). Twenty-seven percent (n = 9) reported a household income of less than $15,000, 42% (n = 14) had a household income between $15,000 and $59,000, and 30% (n = 10) had a household income of $60,000 or more. Every geographical region of the United States was represented: 33% (n = 11) from the South, 27% (n = 9) from the West, 21% (n = 7) from the Midwest, and 18% (n = 6) from the Northeast. Sixty-one percent of the respondents were employed (n = 20), 9% were in school (n = 3), and 12% (n = 4) were both employed and in school. Forty-five percent (n = 15) had a college degree or technical certification. All women were in the first trimester when they started the progesterone protocol for abortion pill reversal. At the time of taking the survey, one-third (n = 11) were still pregnant, 45% (n = 15) had delivered a baby, 18% (n = 6) had experienced a pregnancy loss, and 3% (n = 1) decided to have an abortion after beginning the APR process.
Demographics.
Women reported that choosing whether to take mifepristone was significantly more difficult (p < 0.0001) than choosing abortion pill reversal. Twenty-eight women (85%) reported that choosing to take mifepristone was very difficult or somewhat difficult, compared to just eight women (24%) who said choosing abortion pill reversal was very or somewhat difficult (Table 2). Ease of choosing abortion pill reversal was negatively correlated with age (r = −0.32) although this was not significant. White women reported more difficulty than non-White women in choosing abortion pill reversal (p = 0.012), and women with college degrees had more difficulty choosing APR than did women without a college degree (p = 0.012). Women who were in a relationship with the father of the baby reported less difficulty in choosing APR than women who were not in a relationship with the baby's father or uncertain of the status of the relationship (p = 0.031). Women who had chosen abortion pill reversal a year or more ago (27%) reported that the decision was easier on average (M = 4.2, SD = 1.09) than women who had chosen abortion pill reversal less than a year ago (73%) (3.5, SD = 1.47), although the difference was not significant. There were no significant differences in difficulty in choosing APR or medication abortion based on family income level, employment status, marital status, religion, or subsequent pregnancy outcome.
Decision-Making Difficulty and Questionnaire on the Quality of Physician Patient Interaction (QQPPI) Scores.
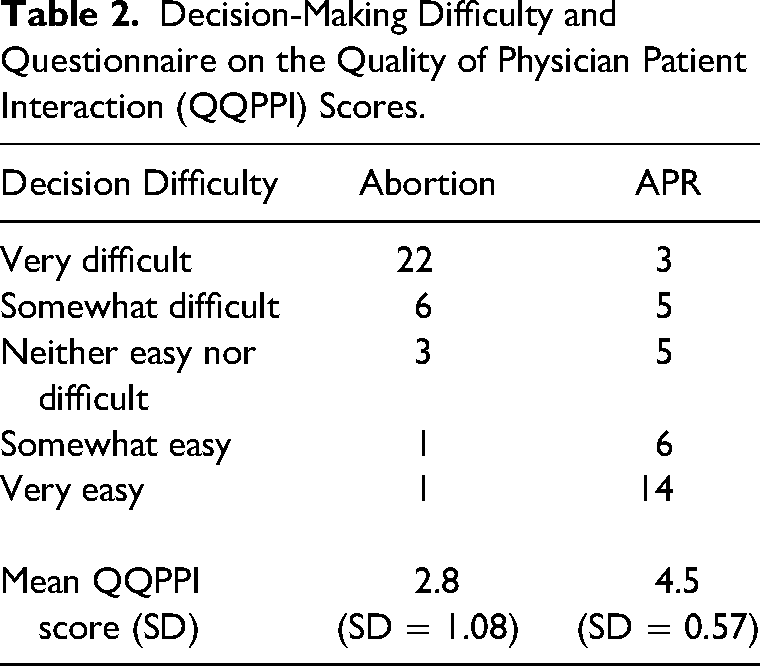
Most women reported receiving their medication abortion pills from planned parenthood and/or from a nurse, physician, or office person at a clinic. Three women said that they had obtained the abortion pills from a website or looked them up online. All women were informed about the APR from a provider affiliated with Heartbeat International. Women scored their interactions with their APR providers as demonstrating significantly better communication than their interactions with their abortion providers (p < 0.0001). Interactions with abortion providers received an average score of 2.8 (SD = 1.08) on the five-point Likert scale, while APR providers received an average score of 4.5 (SD = 0.57) (Table 2).
Only one woman described her communication with the medical provider who prescribed mifepristone, stating: “I was scared because the medical provider told me once I take it, I can’t go back because the baby will have problems” (woman 13). One woman described her communication with her therapist during the decision-making process after she started her medication abortion: “I talked to my therapist who has worked with both crisis pregnancies and post-abortion experiences, and she said that the long-term effect of post-abortion is much more difficult than with having a child.” Eight women included information in their personal narratives about their communication with the medical provider during the APR process. Four women specifically mentioned contacting the abortion reversal hotline, noting that “we talked about the decision, and they consoled me” (woman 12), “the nurse who helped me made me feel understood and supported” (woman 11), “[The doctor] made me more at ease… He reassured me it would be okay, making me more confident about my decision to take the progesterone” (woman 13), and “I called them from the side of the road. They asked me a ton of questions and told me that the sooner I did something the better the chances are that we would see success. She asked me when I took the pill and I looked at my phone and I said, ‘I don’t know – 15–20 min ago?’ She immediately walked me through the steps, the chances, the process.” (woman 15) Collectively, these messages offered some initial insights into the interactions that women have with APR medical providers, and the messages about taking the progesterone protocol.
Discussion
In light of the recent Dobbs vs. Jackson Women's Health Organization Supreme Court ruling, demand for medication abortion and consequently for abortion pill reversal is projected to increase (Jones et al. 2022). Our study is the first to provide peer-reviewed, evidence-based research on women's communication with their different providers as they begin a medication abortion and then attempt a medication abortion reversal. The women who responded to our survey were mostly diverse, representing a wide variety of ages, races, religions, socioeconomic backgrounds, and residing in different geographical regions of the United States.
We found that the majority of women in our study reported that taking mifepristone was difficult. Similarly, other scholars have found that medication abortion decision-making is often not a flippant decision, but instead ripe with tension (Rafferty and Longbons 2021; Alvarez, Wolfe and Scharp 2022). The decision to begin APR was regarded as less difficult for women, but was still considered more difficult for White women and those women who started APR within the past year, as well as for women with college degrees and those who were not in a relationship with the baby's father. We believe that the greater difficulty for White women could be associated with the higher preference for medication abortion in this population compared to Black women; similarly, college-educated women are more likely to have early abortions compared to women who have not graduated from college (Wingo et al. 2021, 271; Jones and Jerman 2022, 7). Relationship problems or a desire to avoid single parenthood are common reasons for U.S. women to choose abortion (Finer et al. 2005). Consequently, women who were no longer in a relationship with the father of the baby may have had more difficulty in deciding whether reversing the abortion was the right choice given their current family living situation. However, the survey respondents nearly uniformly indicated that choosing medication abortion was difficult, with little variation due to demographics or socioeconomic background. These findings suggest that difficulty deciding to get an abortion increases the likelihood of choosing APR for all women.
Finally, when comparing the quality of interaction with the abortion provider to the quality of interaction with the APR provider, we found that women reported having more satisfaction and higher quality interactions with their APR provider than with their abortion provider. Studying women's interactions with abortion and APR providers is important because abortion decision-making is often independent from a woman's regular gynecologic provider (Chor et al. 2016). Medication abortion typically occurs in a context of limited contact within the traditional healthcare system, and some online services allow women to obtain pills with no face-to-face interaction with a medical provider (Longbons 2022). Some women positively regard tele-health abortion encounters because of the ease of accessibility and maintenance of privacy (Raymond et al. 2020). However, limited communication with women's healthcare providers can be problematic because it undermines the exchange of important health information and the provision of optimal ongoing reproductive health care, while also increasing the probability of preventable adverse events (Lippke et al. 2019). Furthermore, the quality of communication between pregnant women and their healthcare providers has ramifications for women's physical and mental health (Nicoloro-SantaBarbara et al. 2017). Specifically related to medication abortion, if complications from a medication abortion are miscoded by emergency room personnel as a natural miscarriage, the woman is twice as likely to be admitted for surgery for retained products of conception and at a significantly greater risk for recurring hospital admissions for treatment complications (Studnicki et al. 2022).
There are several limitations with this exploratory analysis. All women were all over the age of 20 and the majority of women were White and Christian. It is also important to note that our sample size was small, and thus, it should not be presumed as representative of the national population. However, the demographics for our sample are similar to demographic trends reported elsewhere indicating that White women, older women, and those women concerned about religious judgment are more likely to choose early or medication abortion compared to non-White, younger women who are less concerned with religious judgment (Wingo et al. 2021, 271; Jones and Jerman 2022, 7). Additionally, religious women may have greater ambivalence about the acceptability of abortion, which may put this particular demographic of women at greater risk of regret after having an abortion, and thus inquiring about abortion pill reversal after taking mifepristone (Frohwirth, Coleman and Moore 2018). Having a low sample size was not surprising, as low response rates are typical of survey research studying abortion (Tierney 2019), and Heartbeat International employees reported that many women fall out of contact due to an eagerness to move past their experience with abortion and APR. Finally, some critics of APR state that there is no high-quality evidence from a randomized control trial to assess its effectiveness, and thus any research on this topic is invalid. However, the absence of clinical trials does not deem a treatment as ineffective (Pruski, Whitehouse and Bow 2022). In several clinical specialties, such as pediatrics, oncology, or the treatment of rare diseases, off-label drugs or treatments with limited high-quality evidence are often utilized and prescribed for these patients. Furthermore, APR's biological effect has been demonstrated (Abortion Pill Rescue Network n.d.; Davenport et al. 2017; Delgado et al. 2018), and for a clinician to fail to offer APR to a pregnant woman who wants to preserve her pregnancy after taking mifepristone would be unethical (Pruski, Whitehouse and Bow 2022). Thus, the dearth of scholarship on this topic and population of women allows our study to provide an initial understanding and baseline for future research from the voices of muted and marginalized women.
In sum, health care providers play a crucial role in ensuring that pregnant women's rights to informed consent are maintained (Kavanaugh, Jerman and Frohwirth 2019). Clinicians should respect a woman's choice throughout every stage of the medication abortion process and include APR as a robust part of their informed consent process. This protocol is particularly important for clinicians who conduct telemedicine abortions, since other scholars have found poorer communication and relational outcomes during patient-provider telehealth interactions compared to face-to-face encounters (Gordon et al. 2020). Previous scholarship on comprehensive abortion counseling has emphasized the need to recognize that some women are ambivalent or torn about their abortion decision and need space and time to explore all options (Joffe 2013). Our study underscores the importance of including information on abortion pill reversal when counseling women who are considering medication abortion.
This study received IRB approval from the Iowa State University.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Charlotte Lozier Institute.