
Abstract
Background
The Ethical and Religious Directives (ERDs) guide the delivery of health care in Catholic hospitals across the United States.
Purpose
This study seeks to understand the perceptions and experiences of medical trainees in a Catholic health care system on key ethical issues pertaining to the ERDs.
Methods
Medical students from a Jesuit Catholic university were recruited via email to complete a self-administered online survey on seven contemporary ethical issues: Catholic Healthcare Systems as Safety Nets; Contraception and Sexually Transmitted Infection (STI) Prevention; Gender-Affirming Care; Fertility; Maternal Endangerment and Pregnancy Termination; Elderly Care; and Brain Death and Organ Donation. Each student ranked the seven issues in order of priority and responded to further questions for the top three issues ranked. Free responses were analyzed with reflexive thematic analysis with an interpretivist approach.
Results
Forty respondents (40/972; 4.12%) completed the entire survey. Maternal endangerment was the most commonly selected issue (N = 37). A statistically significant association was identified between religion (observance and self-identification) and the selection of Contraception and STI Prevention (p = 1.0 × 10−4; p = 0.011, respectively). In qualitative analysis, concern for patient welfare, navigation of value conflicts, and expression of uncertainty emerged across themes.
Conclusion
The findings of this study suggest that medical students’ ethical reasoning and experiences may be in tension with the ERDs. Recommendations include promotion of familiarity and alignment with the ERDs through the exploration of specific scenarios and exposure to ERD-coherent practices throughout medical training.
Non-Technical Summary
Medical students from a Jesuit Catholic university were surveyed for their opinions on seven contemporary issues related to the Ethical and Religious Directives, which guide Catholic healthcare provision in the United States. The issue of Maternal Endangerment and Pregnancy Termination was the most commonly chosen topic. An association between religion and selection of the topic of Contraception was detected. Free responses across topics demonstrated concern for patient welfare, navigation of value conflicts, and expressions of uncertainty.
Short Summary
Medical students from a Jesuit Catholic university were surveyed for their opinions on the Ethical and Religious Directives.
Keywords
Introduction
Medical students in Catholic health care systems must engage with the ethical frameworks guiding what and how care is provided in these systems. The Ethical and Religious Directives (ERDs), composed by the United States Conference of Catholic Bishops (USCCB), constitute the pillars of this framework. Student familiarity with, perceptions of, and alignment with the ERDs has not been explored. We conducted a cross-sectional, self-administered online survey of medical students enrolled at a Jesuit Catholic medical school to examine this question.
When considering institutional ethics, both organizational and individual-level components are pertinent. On the one hand, institutional longevity is established when core values remain relevant over time; the institution adheres to them in the face of economic, social, or other pressures; and these values transcend a particular industry (Sturmberg and Taher 2025). The long moral tradition of the Catholic Church, upon which the ERDs are based, satisfies the first and third criteria. The second criterion, in healthcare, depends upon each institution, its governing bodies, and its mechanisms of regulation. This adherence to core values has also been articulated through the lens of moral reliability, that is, the coherence between policies and practices. Consistency between practiced norms and established policies is fundamental to establishing moral reliability (Charlton and DiStefano 2024). To gauge the moral reliability of Catholic health care institutions as perceived by medical students, observations in Catholic health systems were featured prominently in the present study. Just the same, individual inculcation of core values is also crucial, particularly in the medical field where interpersonal actions and interactions are the fundamental unit of service (Sturmberg and Taher 2025). Among medical students, alignment with the ERDs may serve as an early indicator of the continuity of institutional values in Catholic health systems from the organizational height to the inter- and intra-personal depth.
The vast majority of American healthcare institutions have some sort of ethics program, regardless of religious affiliation (Danis et al. 2021). Ethical frameworks in secular institutions tend to emphasize professional standards, moral norms, and pluralism. The orientation of Catholic health care ethics is Christological, transcendent, and inherently situated within a particular moral tradition (O’Callaghan et al. 2017). Although the former may generate less controversy than the latter by nature of its pluralistic and materialistic stance, ethical tensions nonetheless arise. Most prominently, the issue of moral distress and moral injury has been explored extensively in secular health institutions (Kherbache, Mertens and Denier 2021). These concepts are relevant to the present study because the inability to do what one believes to be morally correct because of internal or external barriers ethically undermines professionals, resulting in burnout, diminished job satisfaction, and poor patient care (Kherbache, Mertens and Denier 2021).
Naturally, neither patients nor practitioners in Catholic health institutions necessarily share the values which underpin the ERDs. Several studies have investigated the experience of ethical conflict among medical practitioners who have practiced in Catholic health systems. Liu et al. (2019) and Hasselbacher et al. (2020) both reported that practitioners perceived restrictions on contraceptive and abortion services to be burdensome and the cause of delays to patient care. Stulberg et al. (2010) explored the general perspectives of primary care physicians in religious institutions, reporting that physicians with no religious affiliation were three times as likely to believe that physicians should provide an intervention even if prohibited by hospital policy. These studies demonstrate the tension encountered by healthcare professionals in Catholic institutions, especially those with no religious allegiance. These tensions could be the source of moral distress and moral injury for professionals in Catholic health systems, a concern for the well-being of those professionals and the patients for whom they care.
However, to the authors’ awareness, this tension has not been explored among medical trainees, nor explicitly focused on the ERDs as such. As medical students represent the next generation of providers who will be responsible for applying the ERDs to medical practice, this work aims to understand how students engage with these directives. The medical school used in this study is uniquely positioned for this investigation because it is a Jesuit Catholic institution with a student population of various (religious) backgrounds. The university also has two campuses in two different states (Nebraska and Arizona) with distinct regulatory and sociocultural environments. Most importantly, clinical rotations occur primarily within Catholic hospital systems.
Given the depth and breadth of the ERDs, seven topics were chosen by the authors of the study as the most relevant to current medical students and the broader context of medicine in the United States. These topics include the status of Catholic Hospitals as Safety Nets, Contraception and Prevention of Sexually Transmitted Infections (STIs), Gender-Affirming Care, Fertility, Maternal Endangerment and Pregnancy Termination, Elderly Care, and Brain Death and Organ Donation.
The primary aim of this survey-based study was to qualitatively explore the perceptions, observations, and alignment of medical students at a Jesuit Catholic university with the ERDs across seven clinically salient domains. We hypothesized that the religious affiliation of medical students would influence their alignment with the ERDs.
Methods
Participant Recruitment
We conducted a cross-sectional, self-administered online survey (Qualtrics 2025) to medical students enrolled at a Jesuit Catholic university. All medical students at both the Omaha and Phoenix campuses, aged 19 years or older, who were subscribed to the email listservs for the classes of 2025, 2026, 2027, and 2028 were eligible for participation. Students currently completing alternate tracks (e.g., MPH, PhD, MA) were also included if they were subscribed to any of the four listservs listed. In this population, there were 972 eligible students. Power analysis was not performed given the finite population. An initial recruitment email was sent from the PI of this study (AMa) on June 9, 2025. A reminder email was sent on June 23 and July 7, and the survey was closed July 21. As compensation, participants had the option to be entered in a drawing for one of four $25 Visa eGift cards upon completion of the survey. Entrance into the drawing was completed in a separate form not linked to the survey to preserve anonymity. Using a random number generator (Haahr 2025), winners were selected and contacted by email (KF). The email list was destroyed after the cards were sent.
To ensure data validity, response IP addresses were screened for multiple responses. In three cases, the same IP address displayed multiple incomplete responses which were consolidated into a single response per IP address for analysis.
Survey Instrument
The research information sheet and bill of rights were presented before the survey in Qualtrics (Qualtrics 2025). If the respondent was not 19 years of age or older, the survey was programmed to end immediately. Consent was presumed from the act of advancing the survey.
The instrument comprised 33 items across seven topic domains and a demographics section (Supplement A.1). The first question asked participants to rank the seven ERD-related topics from the highest level of perceived importance to the lowest. Then, the participants proceeded to answer further questions for the sections marked as the top three priorities. By limiting survey respondents to three sections, we intended to reduce survey length and response drop-off due to fatigue. A response was required for all questions within each topic, including open-ended responses.
The sections of the survey were as follows: Catholic Healthcare Systems as Safety Nets; Contraception and STI Prevention; Gender-Affirming Care; Fertility Technology; Maternal Endangerment and Pregnancy Termination; Care for the Elderly; Brain Death and Organ Donation; and Demographics. As relevant background, each section included the pertinent directives from the ERDs or, for sections with no existing directive, a succinct explanation of the issue's context and the relevant teachings or consensus of the Catholic Church as evidenced in official Vatican documents. Because the goal of this survey was to gain thoughtful reflections on the current ERDs, links to more in-depth explanations, context, and relevant articles were provided for interested respondents but were not required for response. A link to the full manuscript of the 2016 ERDs was provided in each section. Each section contained two to four questions that were multiple-choice (e.g., Likert scale; only one response allowed) and/or multiple-selection (more than one response allowed) and one required open-ended question.
Demographic information was collected at the end of the survey. Demographic variables collected included campus, year in medical school, specialty interest (3 selections allowed), sex, gender identity, marital status, self-identified religion (multiple selections allowed), degree of religious observance (rated on a scale of 0–100), religion of immediate family members (multiple selections allowed), previous attendance in Catholic educational institutions, and hometown ZIP code.
The survey was reviewed by a content expert (bioethicist, n = 1) and piloted for technological performance and cognitive validity (n = 7 students).
Because this survey of medical student opinions and understandings regarding the ERDs involves soliciting participant responses on sensitive and controversial ethical topics, there was risk of social desirability response bias. However, social desirability scales have been scrutinized as to whether they truly measure deceptive response bias, as opposed to personality traits or socially oriented self-control (Perinelli and Gremigni 2016; Tan et al. 2021). Given these doubts and to preserve survey brevity, no measure of socially desirable response bias was included. Other methods that have been shown to decrease the risk of socially desirable responding were employed in the survey medium (i.e., self-administered online survey and neutral questioning).
Data Analysis
The primary endpoint of this study was to characterize the perceptions, observations, and alignment of medical students with the ERDs as expressed in free-text responses. Reflexive thematic analysis with an interpretivist approach was employed to generate subthemes.
Thematic analysis of free-text responses was conducted as follows: Themes were defined according to the seven domains broached by the survey. All text passages related to a main category (e.g., Contraception and STI Prevention) were compiled. Subthemes were developed and refined iteratively. Two investigators (AMa, AMi) open-coded responses in each category by paraphrasing responses into short sequences of words summarizing the main points of each text. Both investigators paraphrased the same subset of responses for comparability and consistency. These open codes were grouped into summative subcategories (“subthemes”). After subthemes were defined, all text passages were recoded and reviewed by two investigators (AMa, AMi). Representative quotes for each subtheme were selected by AMa and reviewed for representativeness by AMi. This process was followed for each of the seven domains. The software Dedoose 10.0.35 was used for thematic analysis (Dedoose 2025).
The demographic composition of the survey respondents was summarized, after collapsing variables such that no variable category contained less than five responses. Self-identified religion and religion of immediate family members were simplified into three groups: Roman Catholic, Other Christian (Orthodox, Lutheran, Baptist, non-denominational), and Other (Muslim, Jewish, Buddhist, Hindu, no religion but believe in God, Atheist, prefer not to say, and other [with option for text response]). Degree of religiosity was divided into three groups—minimal, moderate, and devout—corresponding to self-ratings of 0–30, 31–60, and 61–100, respectively. Specialty was dichotomized to “interest” or “no interest” in a primary care specialty. If a primary care specialty (i.e., internal medicine, family medicine, emergency medicine, obstetrics and gynecology, and pediatrics) appeared in a respondent's selection, the respondent was categorized as having an interest in a primary care specialty. Marital status was dichotomized into single and not single. The latter category included married, domestic partnership, separated/widowed/divorced, prefer not to say, and other (with option for text response). Prior education in Catholic institutions was dichotomized to yes, the respondent previously attended a Catholic educational institution, and no, the respondent did not previously attend a Catholic institution. Attendance considered elementary, intermediate, high school, undergraduate university, and postgraduate university (not including current enrollment). ZIP codes were classified into the corresponding rural-urban continuum (RUCC) classification using the Economic Research Service 2023 specifications (USDA 2024). Classifications were then further simplified into “Metro,” “Nonmetro,” and “Did not provide.” Even so, there were fewer than five “Nonmetro” respondents.
The primary quantitative outcome was domain prioritization, operationalized as “yes,” the topic was ranked in the top three priorities, and “no,” the topic was not ranked in the top three priorities. Statistical analyses were performed in Python 3.12 in the Google Colab environment (Python Software Foundation 2025; Google 2025), using the pandas (Robert et al. 2024) and NumPy (“NumPy 2.0.2 Release Notes” n.d.) libraries for data manipulation. Chi-square tests and standardized residual analyses were conducted using SciPy and visualized with seaborn (Schult et al. n.d.; Seaborn Developers 2025). When expected cell frequencies were below 5 and degrees of freedom < 3, a Monte Carlo simulated Fisher's exact test was performed via rpy2, interfacing with the R statistical environment (Ushey et al. 2025; The R Core Team 2025). Binary logistic regressions were estimated with statsmodels (Seabold and Perktold 2010), reporting coefficients, p-values, odds ratios, and confidence intervals. Chi-square analysis for RUCC groups (derived from ZIP codes) was not valid because the minimum expected value was less than 5 and the matrix size too large for Fisher-exact tests (for this analysis, the groups were not compressed as in Table 1, but were maintained in the RUCC groups to which the original responses belonged). Only binomial logistic regression was considered for RUCC group analysis. Tabular and graphical results were exported to Microsoft Excel using XlsxWriter (XlsxWriter Developers 2025). The scripts employed for demographic summarization and statistical testing are included in Supplements B.1 and B.3. The purpose of this study was exploratory, so a false detection rate was not accounted for.
Survey Respondent Demographics.
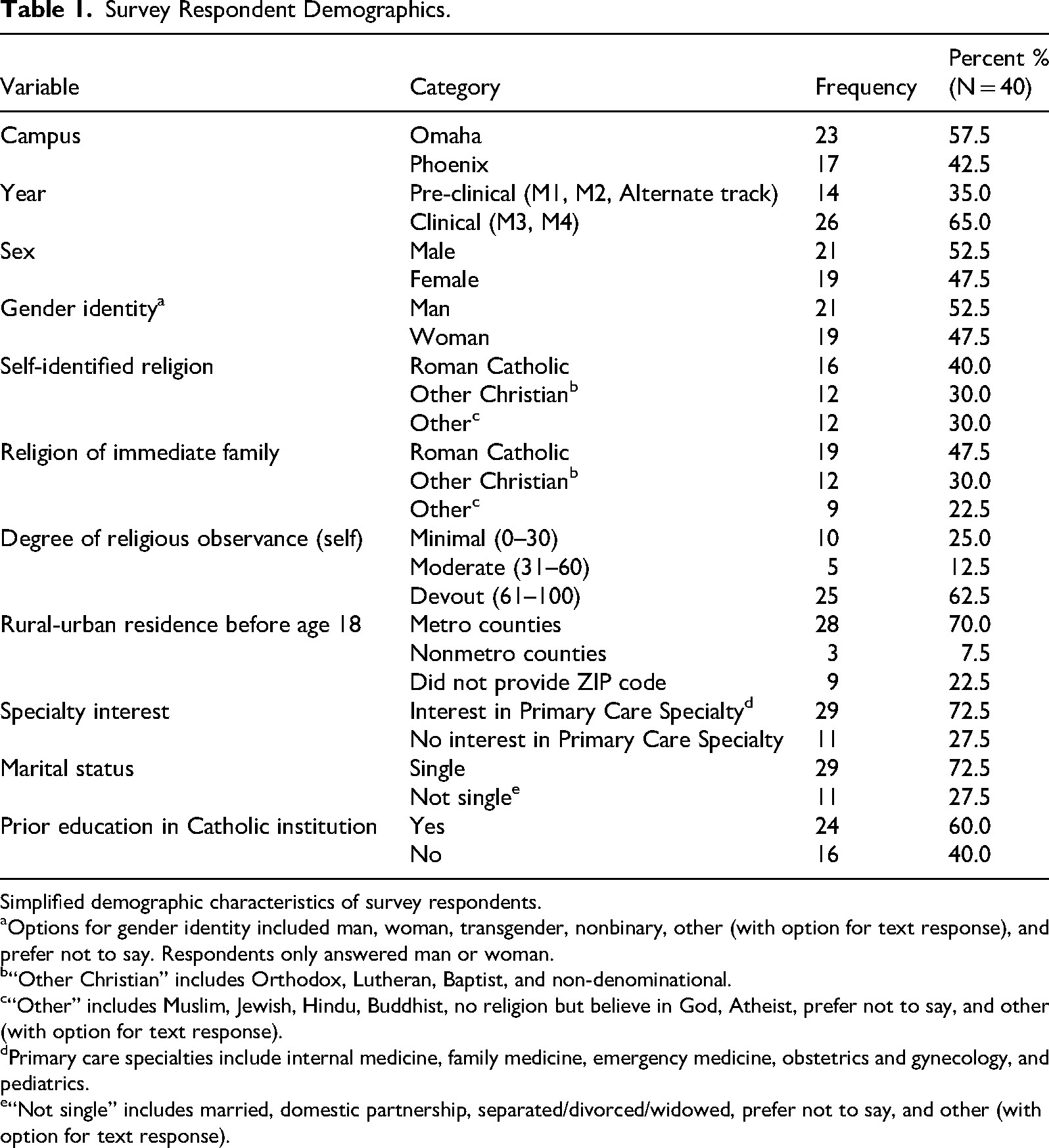
Simplified demographic characteristics of survey respondents.
Options for gender identity included man, woman, transgender, nonbinary, other (with option for text response), and prefer not to say. Respondents only answered man or woman.
“Other Christian” includes Orthodox, Lutheran, Baptist, and non-denominational.
“Other” includes Muslim, Jewish, Hindu, Buddhist, no religion but believe in God, Atheist, prefer not to say, and other (with option for text response).
Primary care specialties include internal medicine, family medicine, emergency medicine, obstetrics and gynecology, and pediatrics.
“Not single” includes married, domestic partnership, separated/divorced/widowed, prefer not to say, and other (with option for text response).
The frequency of multiple-choice responses was tabulated using Python 3.12 in Google Colab (Python Software Foundation 2025; Google 2025). Frequencies were displayed as a histogram created using Excel 16.102.2 (Microsoft Corporation 2025). Supplement B.2 displays example code for frequency tabulation.
Frequency of qualitative subthemes by topic was visualized using a custom “bubble–pie” diagram. For each subtheme, a total across topics was computed; circle area encodes this total (so radius ∝ √total), while each circle's interior is partitioned into colored wedges proportional to the share contributed by each topic. Each subtheme's position was the weighted average of topic centroids based on the proportion of responses in each subtheme for a given topic. Totals were labeled inside circles and subtheme names above; a color legend mapped topics to wedge colors. Analyses were run under Python 3.12 in Google Colab, NumPy 2.0.2, pandas 2.2.2, and Matplotlib 3.10.0 (Python Software Foundation 2025; Google 2025; “NumPy 2.0.2 Release Notes” n.d.; Robert et al. 2024; Matplotlib Development Team 2024) (see Supplement B.4).
Results
A total of 89 participants began the survey. Of the 89 participants who began the survey, 60 ranked the seven issues covered by the survey in order of perceived priority. Forty students completed the entire survey, including demographic information. With 972 medical students across the Phoenix and Omaha campuses, this is a 6.17% partial response rate (ranking 7 issues) and a 4.12% total response rate (completing the survey). Figure 1 displays survey participation.
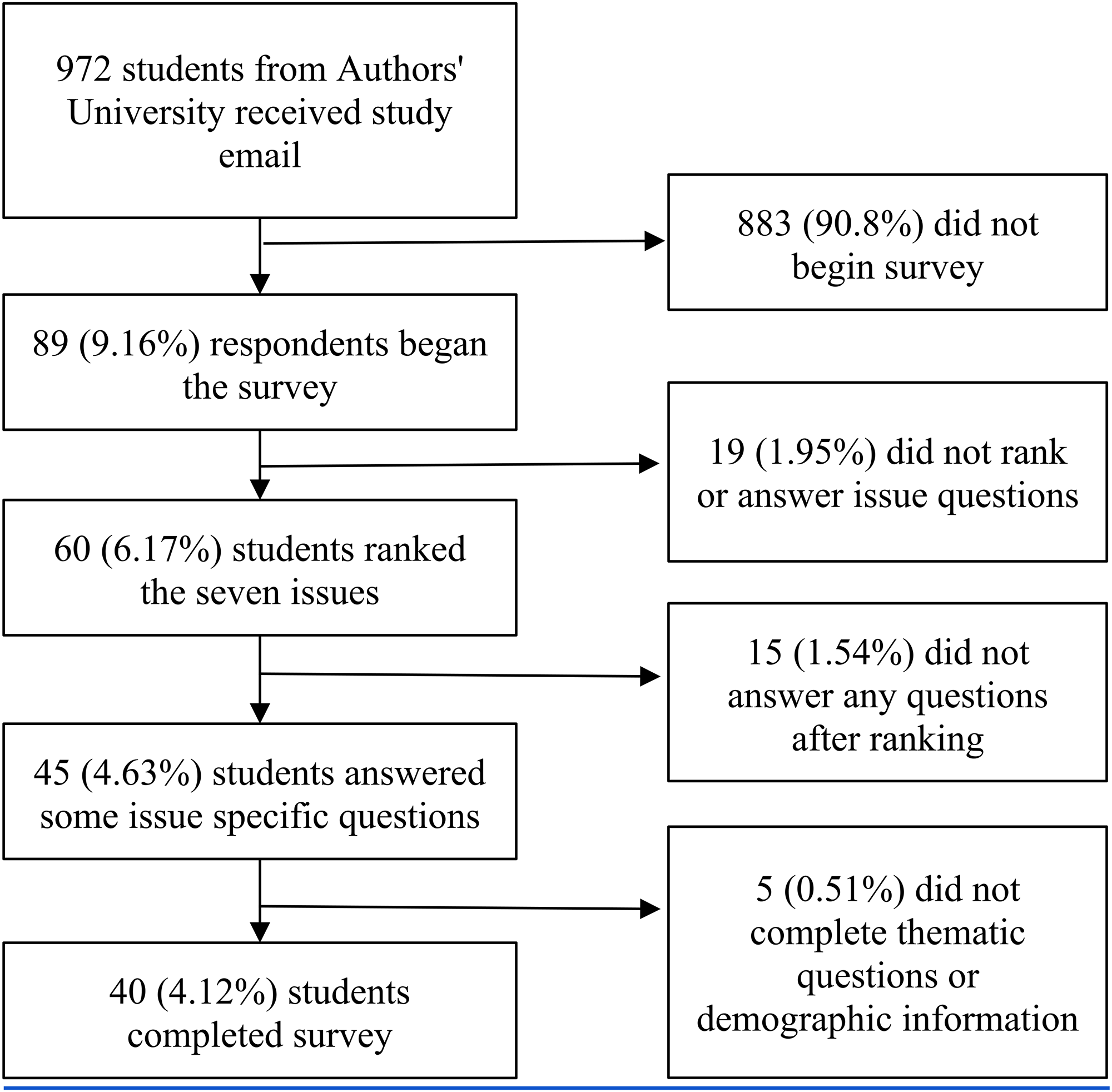
Survey response of the 972 medical students on both the Omaha and Phoenix campuses. Eighty-nine respondents began the survey. 60 students ranked the seven issues covered by the survey according to the student's perceived priority. 45 students proceeded to answer some issue-specific questions based on the student's top three ranked themes. 40 students answered all theme-specific questions and completed demographic information.
As shown in Table 2, Maternal Endangerment was most often ranked in the top three positions, followed by Gender-Affirming Care and Contraception. Although respondents were instructed to complete questions for their top three issues, two students responded to only two issues, and three answered only one. One participant did not complete demographic information but completed all selected topic questions. Supplemental Figure C.1 displays graphically how students ranked each issue from priority 1 to priority 7.
Issue Question Response.
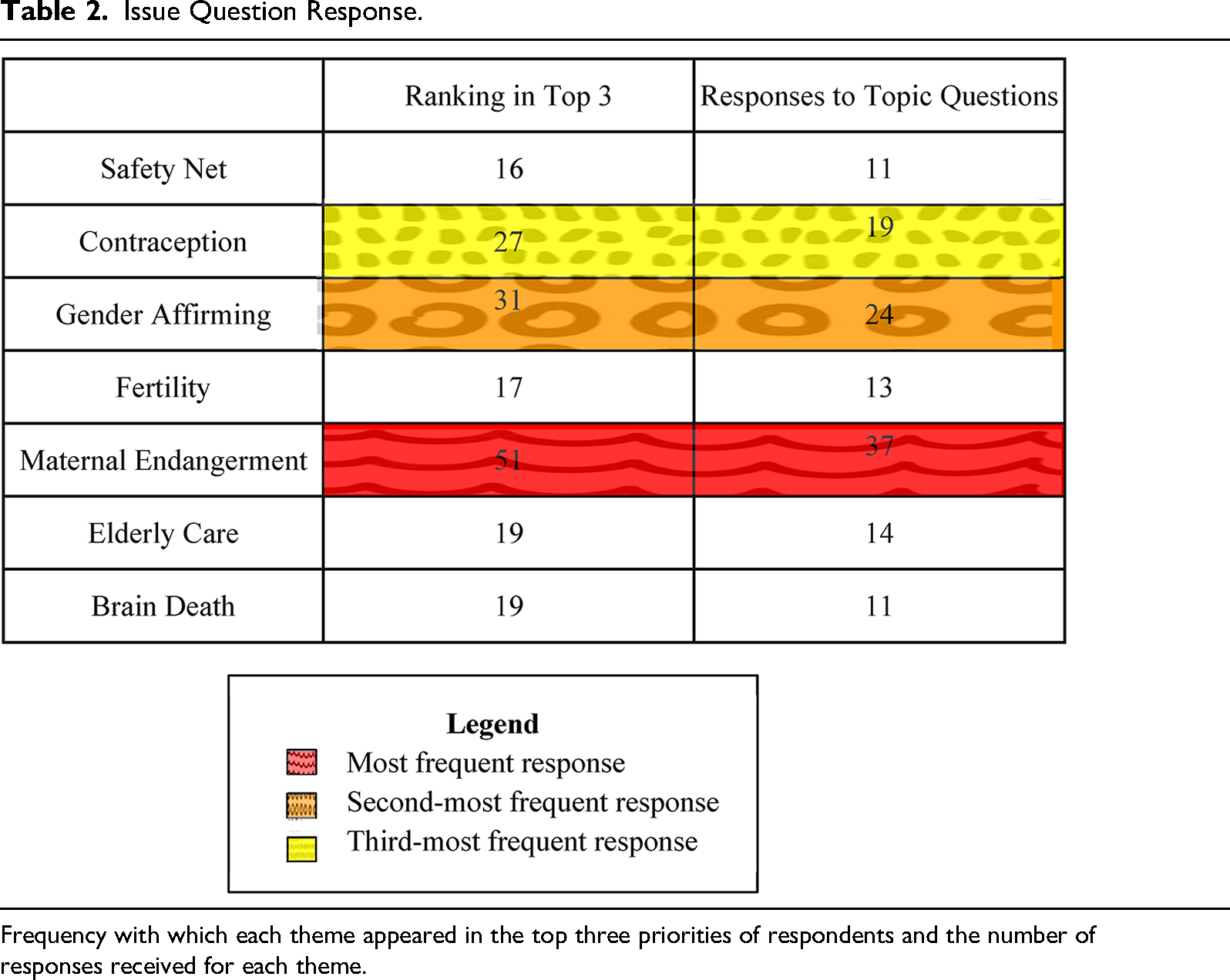
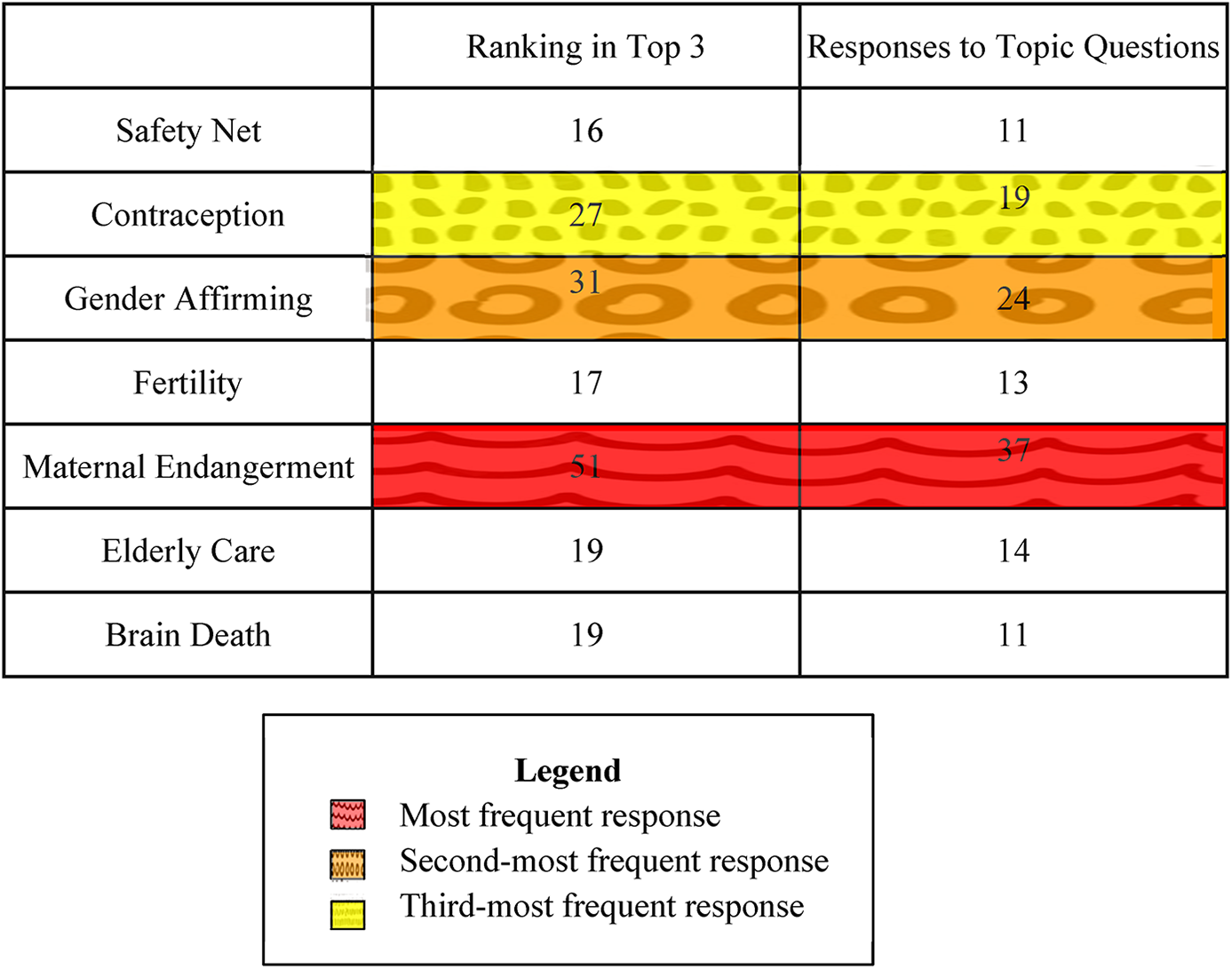
Frequency with which each theme appeared in the top three priorities of respondents and the number of responses received for each theme.
Demographic Composition
Forty respondents provided demographic information (Table 1). Most were from the Omaha campus (57.5%) and in clinical rotations (65%). Sex and gender identity were evenly distributed. A plurality identified as Roman Catholic (40%) or other Christian (30%) and reported devout religious observance (63%). Most grew up in metropolitan areas (70%), had prior education in Catholic institutions (60%), and expressed interest in primary care specialties (73%). This demographic distribution closely resembled the general medical student population by campus (Omaha: 54.5%) and sex (male: 48.7%).
Statistical Analysis
Self-identified religion significantly influenced selection of Contraception and STI Prevention (pChi=0.011). Adjusted residuals indicated that respondents identifying as “Other Christian” were less likely to select this issue, whereas respondents identifying as “Other” were more likely (Supplemental Figure D.1). Binomial logistic regression confirmed a reduced likelihood for “Other Christian” respondents (pregression=0.0384; odds ratio=0.0909, 95% CI [0.00940, 0.850], using Roman Catholic as the reference category.
Religious observance also affected prioritization of Contraception and STI Prevention (pFisher=1.0*10−4), with devout respondents less likely and minimally observant respondents more likely to select the issue. Supplemental Figure D.2 demonstrates the residual values in a heatmap. Logistic regression was significant for devout observance and Contraception (pregression=0.00116; odds ratio=0.0212, CI95[0.00207, 0.217]), using minimal observance as the reference.
Religious observance significantly influenced Elderly Care selection (pFisher=0.0152), with devout respondents prioritizing it more. Logistic regression did not detect significance, likely due to small sample sizes. Supplemental Figure D.3 illustrates a heatmap of adjusted residuals.
Family religious identification also impacted issue selection. Immediate family identifying as “Other Christian” significantly affected Brain Death and Organ Donation selection (pregression=0.0500; odds ratio=5.33, CI95 [1.00, 28.4]), and family identifying as “Other” influenced Gender-Affirming Care selection (pregression=0.0314; odds ratio=0.132, CI95[0.0208, 0.835]). No other Chi-squared, Fisher-exact, or binomial regressions were significant. Full results are shown in Supplemental Tables D.1 and D.2.
Free Response Analysis and Closed-Response Weaving
Free-text responses were categorized into subthemes, with one response potentially contributing to multiple subthemes (Supplemental Table E.1). Responses such as “none,” “n/a,” or similar were excluded (one participant wrote “all of the above.” This response was also excluded). Limited numbers of meaningful responses precluded subgroup analysis. Verbatim responses are provided in Supplemental Table E.2. Supplemental Figure E.1 depicts subtheme distribution, with circle size representing response frequency and color indicating contributions from multiple themes.
Catholic Hospitals as Safety Nets
Six of the 11 respondents who ranked Catholic Hospitals as Safety Nets provided substantive free-text responses. For the most part, participants expressed lack of awareness of or doubts about the effect on finances. Participants offered conflicting perceptions of the hospitals associated with the Phoenix campus. One respondent shared their perception that “In Phoenix, the catholic hospital is not the safety net hospital for the area. While I know that the [sic] do provide some financial assistance, it is not my impression that they do this for a representative amount of the Phoenix population that would require this” (Participant 44). In contrast, another student stated that “St. Joe's and especially Valleywise (not religiously affiliated to my knowledge but still associated with [the university]) are located around less affluent areas of Phoenix and are therefore more likely to accept these patients” (Participant 5).
Eleven participants completed the Likert and multiple-selection questions in this section. Likert responses indicated that most students perceived Catholic hospitals as “probably yes” meeting safety net criteria (n = 7), with community health programs and social services most frequently observed (n = 8 each; Supplemental Table E.3).
Contraception and Sexually Transmitted Infection Prevention
Twelve students shared their concerns about contraception and STI prevention, emphasizing patient welfare and autonomy. Several respondents expressed opposition to the ERDs’ stance on contraception and argued that religious or moral standards should not be prioritized above a patient's right to make an informed decision. Those without an explicit stance of opposition tended to ask questions about how to strike a balance between the values of a Catholic hospital as expressed in the ERDs while ensuring patients are cared for and that public health is protected.
Among 19 multiple-selection responses, screening for interpersonal violence (n = 19) and sexual risk education (n = 17) were the most commonly identified services (Supplemental Table E.4). One student provided additional comments in response to the question and suggested that health systems should “Talk about human sexuality in a more positive/less shameful light, while emphasizing its sacredness and the need for monogamous [sic] and marriage.” (Participant 22).
Gender-Affirming Care
A total of 21 free-text responses were provided on this topic. The discussion of gender-affirming care centered around the tension between institutional and patient and healthcare professional values. Respect featured prominently. This included the obligation of the physician to act according to the patients’ best interest, particularly as recommended by evidence of benefit for gender-affirming care. At the same time, other students expressed uncertainty about how to maintain a vision of sexuality consistent with Catholic theology while ensuring patients are cared for and respected.
Among the 24 multiple-selection responses, psychiatric care (n = 22), support groups (n = 21), and family counseling (n = 20) were indicated as key services (Supplemental Table E.5).
Fertility
Six participants provided free-text responses related to this topic. The theme of navigating the tension between the ethical principles of the ERDs and honoring the values and desires of patients while offering high-quality care emerged. Other students emphasized promotion of Natural Procreative Technology (NaPro) for its efficacy, cost-effectiveness, and ethical soundness.
Eleven multiple-selection responses highlighted commonly known technologies such as IVF, IUI, and pharmacological ovulation stimulation (n = 13 each; Supplemental Table E.6).
Maternal Endangerment and Pregnancy Termination
A total of 24 free-text responses were provided on this topic. Some students expressed doubt as to what measures, and at what point, intervention to save the mother, but endanger the child, would be licit. Students perceived a necessity to act to protect the mother from potentially fatal consequences, especially when the likelihood of fetal survival is low.
Significant concern was expressed over the perceived connection between restrictions on abortion and patient safety. It is important to note that for most students, “patient” generally refers to the mother only. This was closely linked to the theme of professional latitude, in which healthcare professionals are given the leeway to act according to their understanding of the patient's best health interest, without fear of repercussions. A few students noted that doctors may hesitate in crucial moments out of fear of transgressing a directive and the consequences that may bring to bear. “I think more needs to be done to ensure patient safety, especially in conditions where the pregnancy is not viable or fetal demise has already occurred. I also do not think that providers at Catholic hospitals are comfortable in practice saving the life of the mother if it risks fetal demise due to the history of repercussions for this type of scenario,” commented one student (Participant 13).
As with the two previous themes, accommodation of patient values featured prominently and is closely linked with how students balance the life of mother and child. There was suspicion surrounding the history and motivation underlying the ERD position on abortion, as evidenced by this comment: “Abortion should not be prevented, especially when the mother's life is at risk. The fetus should not be prioritized over the mother's life. This directive is rooted in historic misogyny and has led to the deaths of patients and has lead [sic] to patient harm, thus going against the main requirement of physicians” (Participant 14).
The previous comment also demonstrated the link several students drew between poor maternal health outcomes and restrictions on abortion. One student linked an article to the same extent in their comment (Participant 18; Supplemental Table E.7).
Thirty-seven participants responded to multiple-selection questions, with most agreeing with the ethics committee's decisions while opposing revocation of St. Joseph Hospital's Catholic affiliation (Supplemental Table E.7). One student stated in an additional comment that “more information is needed to understand the severity of the case and how unstable the patient was” and another added that “fear of punishment from hospital/authority” was also at play (Participant 39; Participant 5).
Elderly Care
Three free-text responses addressed end-of-life care clarification. Fourteen participants responded to Likert and multiple-selection items, emphasizing the value of elderly care and observations of transportation, housing, pastoral support, and family assistance (Supplemental Table E.8).
Brain Death and Organ Donation
Three free-text responses highlighted uncertainty regarding brain death criteria and organ donation, supported by 11 multiple-selection responses focusing on concern about guidance gaps and observations of pastoral support (Supplemental Table E.9).
Discussion
This study explored medical students’ perceptions and alignment with the ERDs at a Jesuit Catholic medical school. Across themes, concern for patient autonomy and high-quality care was prominent. Statistical analyses suggested associations between personal and family religious identity or observance and prioritization of certain issues (i.e., Contraception, Gender-Affirming Care, Elderly Care, Brain Death), though small sample sizes and multiple tests limit definitive conclusions.
Although several studies have explored practitioner experiences of ethical conflict related to topics such as abortion, contraception, and medical aid in dying in Catholic hospitals (Liu et al 2019; Hasselbacher et al. 2020; Stulberg et al. 2010), none have explicitly explored the perspectives of medical trainees related to the ERDs.
Synthesis of qualitative and quantitative information for each topic elucidates a variety of student opinions. The students’ perceptions and observations of Catholic health systems generally endorsed the idea that such systems are viewed as “safety nets,” which are “hospitals with a stated mission to care for and treat vulnerable patients, regardless of ability to pay, health insurance status, or immigration status” (from survey; n = 9). Comments on this theme further highlight the obligation of Catholic healthcare systems to play this role: “Catholic social teaching requires this” stated one student (Participant 42).
On the topic of Contraception and STI Prevention, the additional observation of advocacy for increased contraceptive and elective abortion access by one student augmented the theme of value conflict, not only between the values of the health system and those of patients, but also between the health system and medical practitioners. As is evident in both the qualitative comments and the selection of services Catholic health centers should provide, many students prioritized reducing communicable infection and avoiding the imposition of Catholic values on patients or practitioners even though Directive 52 does not permit “promot[ing] or condon[ing] contraceptive practices” (USCCB 2016).
Gender-Affirming Care, not currently addressed in the ERDs, emerged as the second-most prioritized domain, reflecting its importance to trainees. The three most selected services medical students believed should be available (psychiatric care, support groups, and family counseling) are consistent with Catholic teaching on gender and sexuality (Supplemental Table E.5), exhibiting the possibility of robust gender care services in Catholic health systems that are simultaneously coherent with the values of the institution(s). Both clinical and pre-clinical students reported not having observed gender-affirming care services, suggesting that the lack of observation may not be entirely due to a lack of clinical experience. The small sample size limits generalizable conclusions about the clinical experience of medical students as a whole.
Although Directive 52 instructs Catholic health systems to promote methods of natural family planning, Natural Procreative Technology (NaPro) was the least familiar fertility technology to survey respondents. The lack of exposure to NaPro technology was noted in student comments as well. Together, these findings point to a paucity of training on, and therefore clinical utilization of, the types of fertility technology that are most coherent with the ERDs. Just as for Gender-Affirming Care, those who had no observations of any type of fertility care in Catholic healthcare systems were both clinical and pre-clinical students, suggesting lack of observation was not necessarily the result of lack of clinical experience.
The strong consensus of agreement with the ethics committee and disagreement with the revocation of the St. Joseph Hospital's Catholic affiliation was robustly corroborated by text-responses stressing professional latitude and outcome impact. Opinions regarding prioritizing a patient's desires over the system's and prioritization of the mother's life also coincide with this consensus. The additional comment added by a student regarding fear of consequences echoed other responses discussing the hesitancy medical practitioners may feel within Catholic health systems when faced with difficult situations such as the one described.
Notably, the issue of abortion care emerged outside of Maternal Endangerment, being featured in voluntary comments offered in the Contraception and STI Prevention issue as well as Gender-Affirming Care.
Comments provided for Elderly Care were few. One comment highlighted how palliative care should be promoted in this population as a means of increasing quality of life and not reserved for critically ill persons only.
Comments and selected responses converged on uncertainty amidst the ambiguity and controversy surrounding Brain Death and Organ Donation.
Several themes emerged that spanned multiple issues (Supplemental Figure E.1). First, survey respondents repeatedly conveyed the conviction of their role as physicians not to do harm and to care genuinely and respectfully for all patients. One student wrote simply, “Patients need to be cared for” (Participant 53). Although responding to the issue of Gender-Affirming Care, this captures a concern evident across all the themes addressed in this study. Students frequently noted the obligation to make decisions based on what is best for the patient.
Given the common desire to care for patients respectfully, the question of how to demonstrate this naturally follows. In other words, how does one manage tension between the values of a Catholic institution while offering excellent, evidence-based care for patients who do not share these values? This second overarching theme of value conflict (N = 37) also includes medical practitioners who may not share the values of the Catholic health system in which they work. Some students simply asked the question of how to manage these conflicts, while others decisively advocated for accommodation of the patient's (or practitioner's) standards, with the understanding that this is what would be in the patient's best interest.
Student responses demonstrated the salience of addressing how to navigate disagreement between the values of patients, practitioners, and Catholic health institutions. One student asked, “How do we create a culture, including in Catholic hospitals, where people who believe in Catholic social teaching have a space to speak freely without fear of judgment for our beliefs?” (Participant 4). Other participants expressed that practitioners may delay acting promptly according to their best clinical judgment, fearing reprimand (Participant 5, Participant 13). Thus, it is vital that subsequent revisions of the ERDs and/or their implementation be robustly supported with guidance on how to approach ethically contentious situations. Although ethics committees serve this role on a greater scale, this study identified a gap in the individual capacity of medical trainees to negotiate this conflict in the context of the application of the ERDs in Catholic hospitals.
Survey answers to both free response and multiple-choice questions evidenced a tendency in ethical reasoning to prioritize the desires or lifestyle of the patient and guidelines from major medical societies over adherence to the stated directives. Therefore, as mentioned above, the question of patient autonomy and value conflict is one that must be addressed directly, especially in cases where the Catholic health system is the only one in the area and the desired service contradicts the ERDs. Equally important, a framework to understand how to interpret and apply evidence-based guidelines in light of moral boundaries is particularly critical for medical trainees. O’Callaghan et al. (2017) similarly found that nurses and junior clinicians in an Australian Catholic hospital were often not aware of the ethical framework particular to the Catholic institution nor used it as a guide in daily ethical decision-making. Furthermore, these healthcare professionals expressed the need for education on how the ethical framework could be applied in specific situations. Enriching medical education in Catholic institutions with concrete scenarios that interface with the ERDs and exposing medical students to services consistent with the ERDs may contribute to a greater alignment and decreased sense of tension.
Addressing this tension in trainees is also an opportunity to promote their well-being as future professionals. The moral distress that can arise from the inability to do what a student believes is “the best for the patient's health” because of the ERDs has ramifications for both trainees and the patients in their care (Participant 14). Stimulation of dialogue and creation of a culture of open ethical reflection and discussion are positive coping mechanisms that can be cultivated in trainees through pre-clinical and clinical medical education (Kherbache et al. 2021).
Rigorous research is essential for Catholic health systems to ensure high-quality care and demonstrate that the ethical principles of the ERDs do not compromise patient outcomes. NaPro technology is one such example of a well-researched, clinically beneficial approach consistent with the ERDs (Hilgers 2004; Tham et al. 2012; Kiani et al. 2020). Thus, it is critical that Catholic health systems prioritize the development, investigation, and implementation of evidence-based, ERD-approved guidelines in order to maintain moral reliability while advancing patient care.
Limitations
This study is limited in a few ways. First, because the survey was voluntary, the study is susceptible to response bias. Because of the small number of participants who completed the entire survey, sub-analysis was limited.
The survey itself was not validated, although it was pilot tested for flow, clarity, and conciseness by non-university affiliated non–university-affiliated and medical school matriculants, as well as the research team. The topics of this study were chosen by the research team, potentially biasing the issues covered towards those deemed important by those on the research team rather than those of the student population or the USCCB. However, as medical students, the research team has a sense of relevant issues for medical students at Jesuit Catholic school of medicine. Unfortunately, the research team does not have any representation from the Phoenix campus, potentially biasing relevancy towards issues more prominent in the Omaha community compared to the Phoenix campus.
All members of the research team are practicing Catholics or Christians, which may have biased the phrasing of questions and closed answer responses. The survey was reviewed by a content expert to reduce this bias.
The survey was administered during the summer, using Listservs for the classes of 2025 through 2028. At this point, the class of 2025 had already graduated, and the class of 2027 had already begun clinical rotations. Only the class of 2028 was pre-clinical, potentially biasing responses towards students with clinical experience. However, given that the class of 2027 had no more than 2 months of clinical rotation experience, in addition to the emphasis of this study on observations, this over-representation of clinical students is appropriate for the aims of the study.
Collapsing demographic categories may have obscured potential associations. This loss of granularity was unavoidable given the small number of participants and the necessity to maintain anonymity.
No adjustment for false detection rate was performed for statistical analyses. Given the large number of tests performed, the probability of false positives was high. However, the emphasis of this study was exploratory, so the possibility of type I error was accepted to identify all potential relationships.
In the qualitative analysis, choosing a truly representative quote from a small sample with relatively diverse approaches proved difficult and could cause a reader to think that the opinions offered were more monolithic than they were in actuality. To represent more completely the responses of students, additional quotes were included in the results and discussion, and all responses are provided in Supplement E.2.
Conclusion
This study examined perceptions, observations, and alignment of medical students at a Jesuit Catholic university with seven ERD-related domains. Maternal Endangerment and Pregnancy Termination was most prioritized, followed by Gender-Affirming Care. Free-text analysis highlighted concern for patient well-being and respect for patient values, especially in maternal, gender-affirming, contraceptive, and fertility care. Exploratory associations between religious identity or observance and topic prioritization were identified, though inferential conclusions are limited.
Recommendations include developing, expanding, and promulgating frameworks to navigate ethical tensions, enhancing research and quality improvement in Catholic health systems, and intentionally exposing students to ERD-consistent practices to support both moral integrity and patient-centered care.
Supplemental Material
sj-docx-1-lqr-10.1177_00243639261429396 - Supplemental material for Survey of Medical Trainee Perspectives on the Ethical and Religious Directives: Single University Experience
Supplemental material, sj-docx-1-lqr-10.1177_00243639261429396 for Survey of Medical Trainee Perspectives on the Ethical and Religious Directives: Single University Experience by Alexandra Mauritsen, Hannah Fleming, John Sweeney, Alexa Mistichelli and Kevin FitzGerald in The Linacre Quarterly
Footnotes
Acknowledgements
Ethical Considerations
This study was approved and deemed exempt from continuing review by the Biomedical Institutional Review Board of Creighton University (Protocol Number 2005572-01). It also received approval from the Education Program Committee which approves all research to be administered to medical students. All investigators completed CITI training prior to conducting the study. Location data and contact information were not collected. Data was stored in Creighton's secure DFS network, limited to team members approved by the IRB. No attempt was made to re-identify subjects. All identifiers collected, including emails collected in the separate gift card drawing form, were destroyed when all the data was collected and after analysis.
Consent to Participate
Participant consent was obtained before beginning the online survey, on the first page.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for respondent prizes was received from the Creighton University Department of Medical Humanities,
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Supplemental Material
Supplemental material for this article is available online.
Biographical Notes
To mitigate these biases, domain selection and survey formulation was considered by the whole team and reviewed by an expert; the survey was piloted for cognitive feedback prior to recruitment of participants; the survey was self-administered online and anonymized; and free-text coding was performed independently by two investigators. The research team is composed of members of varying religious backgrounds and ethical approaches, mitigating individual biases. All confirmatory and non-confirmatory findings are reported for transparency.