
Abstract
This article canvases several sexually transmitted infections (STIs). It explains in detail their prevalence, how they are contracted, and their sequelae. The article closes by arguing that engaging in promiscuous sexual activity is a violation of justice. The advance the article makes is that typical arguments against promiscuous sexual activity focus on some aspect of the Church's sexual teachings. It is an underexplored terrain to develop an argument against such behavioral patterns from the standpoint of justice, insofar as appeals to justice are more ecumenical.
Overwhelming medical evidence demonstrates the serious harm of STIs on patient health and well-being. This article presents the case for chastity as promoting both sexual health and the justice that human beings owe to each other and to their community. The Congregation for the Doctrine of the Faith's (CDF) instruction Persona humana, says the following: “Experience teaches us that love must find its safeguard in the stability of marriage, if sexual intercourse is truly to respond to the requirements of its own finality and to those of human dignity” (CDF 1975, no. 7). In what follows, we see what “experience teaches us…” We examine a select group of sexually transmitted infections (STIs), focusing on the human burden of these diseases: bacterial vaginosis (BV), chlamydia, and gonorrhea (which can cause pelvic inflammatory disease, or PID), herpes simplex virus (HSV), hepatitis B virus (HBV), human papillomavirus (HPV), human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (HIV/AIDS), syphilis, and trichomoniasis. Each disease section contains four subsections. In the “Human Burden of the STI” subsection, STI incidence rates from circa 2010–2020 are presented, estimated by monitoring groups such as the Centers for Disease Control (CDC) (Weinstock et al. 2021; Kreisel et al. 2021) and the World Health Organization (WHO) (Rowley et al. 2019). We also examine data measuring the economic burden resulting from STIs. After briefly examining how each infectious agent attacks the human body in “How the STI Attacks,” we discuss “Acute and Chronic Damage by the STI.” Finally, the section will end with “Prevention of the STI.” Specifics of diagnosis and treatment will not be discussed in this focused review—we instead encourage physicians to consult CDC guidelines (Workowski et al. 2021) often, as available diagnostic methodologies and best-evidence treatment regimens can change frequently.
The overall burden of STIs among the general population remains dramatic. In 2018, there were 26.2 million incidents (i.e., newly diagnosed) STIs in the United States, with the 15- to 24-year-old age group accounting for nearly 46% of all incident STIs (Kreisel et al. 2021) (likely a combination of newly acquired cases as well as targeted screening (CDC 2018). HPV comprised 50% of all incident infections and 63% of all prevalent STIs in the United States, regardless of age group; taken together, HPV, chlamydia, herpes, and trichomoniasis caused 93% of all incident U.S. STIs and 98% of all prevalent (i.e., total present) STIs (Kreisel et al. 2021). Worldwide in 2016, there were 376.4 million incident STIs, indicating that more than 1 million STIs are acquired across the world each day (Rowley et al. 2019). Trichomoniasis comprised approximately 41% of all incident STIs worldwide; chlamydia, 34%; gonorrhea, 23%; and syphilis, 1.6% (Rowley et al. 2019). Hearteningly, worldwide rates of congenital syphilis (which is most often derived from a mother's sexually acquired infection) decreased from 2012 to 2016, with a case rate of 473 per 100,000 live births in 2016 (down from 539 congenital syphilis cases per 100,000 live births in 2012) (Korenromp et al. 2019), but the current case rate remains far above the WHO goal of ≤50 per 100,000 live births in 80% of countries (WHO 2016).
There are also groups of individuals at higher risk for acquisition and transmission of STIs. Both in the general population and among men who have sex with men (MSM), there is a disproportionate effect of STIs among younger individuals, racial/ethnic minority groups, and people of lower socioeconomic status (CDC 2018). MSM, individuals who identify as “transgender” or other alternative gender identities, and people with previously diagnosed STIs (including HIV) face an increased risk for STI acquisition (WHO 2016). Women who identify as lesbians—and are oftentimes assumed to be in a sexually “low-risk” group—are also at risk for STIs, including trichomoniasis, HPV, HIV, syphilis, and BV (Gorgos and Marrazzo 2011). The sexual risks these women face should not be discounted. As national reporting programs do not draw data on sexual or gender identity, statistics on these “at-risk” groups are often based on findings from sentinel and enhanced surveillance systems, limiting the ability to fully assess the burden (CDC 2018). According to 2017 data compiled by the CDC, ∼68% of primary and secondary syphilis cases in the general population were diagnosed among MSM, and the gonorrheal strains isolated from MSM showed greater antimicrobial resistance than those isolated from the population in general (CDC 2018).
Economically, the U.S. 2018 STI burden totaled approximately $15.9 billion in direct medical costs, with the 15- to 24-year-old age group accounting for 26% of the cost (∼$4.2 billion) (Chesson et al. 2021). By disease breakdown, most of the economic cost was borne by sexually transmitted HIV and HPV, to the tune of $13.7 billion and ∼$0.8 billion, respectively (Chesson et al. 2021). Worldwide STI costs can be difficult to estimate; often, the concept of the disability-adjusted life-year (DALY) is used instead. DALY is a complex metric that attempts to condense morbidity and mortality into a single number, capturing either the health costs associated with contracting a disease (or the costs spared by treating a disease). One DALY is meant to equal one year of full health, unaffected by any disease. Using this metric, an untreated case of gonorrhea costs a member of the general public 4.5 DALYs, while a high-risk individual (such as someone who sells or trades sex) with untreated gonorrhea loses 37.3 DALYs (Aral et al. 2006). Overall, it is thought that preventing or curing STIs in high-risk groups provides approximately ten times the DALY benefit of the same intervention in the general population (Aral et al. 2006).
Speaking generally, we note that most STIs do not cause symptoms or signs that are easily recognized at the patient level. On the whole, women are more likely to have asymptomatic STIs, while men are more likely to be diagnosed with symptomatic STIs (WHO 2016). Even symptomatic STIs may be easily misconstrued for other disease processes. STIs nonetheless have an incredible negative impact on sexual, reproductive, and psychological health (WHO 2016), as we discuss in greater detail for each disease in the sections below. The negative effects on reproductive health are most striking for women (WHO 2016). Overall, acquisition of any STI may lead to cellular changes that increase the risk for consequent cancer development or for acquisition of HIV (WHO 2016). These are ethically relevant details for how STIs are acquired and function. As such, we give the reader the cellular and pathophysiological details of each disease.
As the name suggests, STIs are largely spread through sexual contact—therefore, commitment to chastity can avoid most of the occurrences and outcomes of STIs. Abstinence from sex (the Catholic concept of continence) virtually eliminates the chance of acquiring STIs, while mutual monogamy narrows the sexual network to two partners only, decreasing the risk of STI incidence and transmission by decreasing the likelihood of exposure and spread. Interestingly, while sexual risk behaviors have declined across low-income countries (e.g., the age of coitarche increased and the number of casual sex partners decreased in Uganda across the early 2000s), risk behaviors in the United States and Europe have increased (Aral et al. 2006). There is speculation that the ability to treat and prevent HIV, for example, may lead to sexual disinhibition (Aral et al. 2006; Workowski et al. 2021). The concept of prevention fatigue (i.e., the inability to maintain STI prevention techniques across the long term) may contribute to increased sexual risk behavior (Aral et al. 2006). For men who have sex with women, medical male circumcision decreases the risk of acquiring HIV by ∼60%, of oncogenic HPV by ∼33%, and of HSV by ∼30%; additionally, the female partners of medically circumcised males have reduced risks of oncogenic HPV (∼28%), BV (∼40%), and trichomoniasis (∼48%) (Tobian and Gray 2011). Test-and-treat strategies to identify present infections not only limit the damage suffered by the diagnosed patient but also prevent further spread of STIs, and are therefore integral in prevention strategies (WHO 2016). Where possible, adopting a “couple's approach” combines counseling and screening efforts while expediting partner therapy (WHO 2016). Finally, pre-exposure prophylaxis may be useful for patients at high risk for bacterial STIs (doxycycline against syphilis) or for HIV (various antiretroviral regimens referred to as “PrEP” against HIV) (Workowski et al. 2021).
Bacterial Vaginosis
Human Burden of the STI
BV is not, strictly speaking, a true STI. As opposed to the sexual transmission of a single organism causing disease, BV is a synergistic infection by multiple microorganisms that displace the physiologic, Lactobacillus-dominant cervicovaginal microbiota. While Haemophilis vaginalis (later renamed Gardnerella vaginalis) was initially thought to be the causative organism of BV, attempts to induce BV solely by inoculating Gardnerella vaginalis were not as successful as inoculation of fresh vaginal discharge from patients diagnosed with BV—suggesting that the effect of the single organism is not as causative as the changes to the microbiota overall (Bennett et al. 2009). Pathophysiology is discussed in greater detail below. Epidemiologically, BV is primarily found in sexually active women who are likely to be diagnosed with other STIs (Bennett et al. 2010). Though BV is common among heterosexual women who engage in sexual activity, women who have sex with women have an increased risk of BV compared to women who have sex with men (45.2% versus 28.8%) (Gorgos and Marrazzo 2011), perhaps due to the greater likelihood of exchanging vaginal microbiota. BV is also associated with new/multiple sexual partners and negatively correlated with condom usage (Bennett et al. 2010). For these reasons, BV is considered here among the other, more typical STIs.
Prevalence of BV varies widely within and between regions across the globe. Approximately 20–30% of U.S. samples show evidence of BV, while frequency can range from 17% to 52% across varying African regions (McKinnon et al. 2019; Joseph et al. 2021). Women above the age of 25 appear to have a slightly greater likelihood of BV diagnosis; women who sell or trade sex are at higher risk than the general population (Joseph et al. 2021). Given the heterogeneity of studies, it is unclear if socioeconomic factors impact BV frequency. Regardless, the global economic burden of BV in 2021 has been estimated at ∼US$4.8 billion (Joseph et al. 2021).
How the STI Attacks
The establishment of the cervicovaginal microbiome begins after birth. While the bacterial community can be diverse and dynamic throughout a woman's life, the physiologic cervicovaginal microbiome is predominated by Lactobacillus. In addition to producing hydrogen peroxide and thus making the environment acidic and hostile to other microorganisms, many Lactobacillus species secrete other anti-microbial compounds (Joseph et al. 2021). In BV, by contrast, the pH of cervicovaginal secretions increases from the typical 4.0 to above 4.6 in ∼90% of cases (Bennett et al. 2010) associated with disruption of the optimal cervicovaginal microbiota. In place of Lactobacillus as the dominating species, other anaerobic organisms are identified from women with BV, including Gardnerella, Prevotella, Megasphaera, Coriobactericeae, Lachnospira, Sneathia, Gemella, and Eggerthella (Bennett et al. 2010; McKinnon et al. 2019). High bacterial diversity is often seen in BV with greater “evenness” of the microbiota (no one predominating species) (McKinnon et al. 2019). Of note, metagenomic studies also indicate the presence of bacterial colonization throughout the upper female genital tract, including the uterus, fallopian tubes, ovaries, and placenta—and again, the optimal microbiota appears Lactobacillus-dominated (Peric et al. 2019). BV-related changes in the female genital microbiota are associated with a pro-inflammatory state, the exact spectrum of which may depend on the specific bacterial content of the non-optimal microbiota (Mitchell and Marrazzo 2014). Overall, BV is associated with genital mucosal inflammation, disruption of the mucosal integrity, alteration of the protective innate immune response, and even increased production of HIV-1 target cells (Mitchell and Marrazzo 2014). This process may be true in the upper genital tract as well: small studies in women with endometriosis or recurrent fertility issues have similarly shown non-Lactobacillus-dominated endometrial microbiota (Peric et al. 2019). Pathophysiology of BV (as well as identification of the optimal endometrial microbiota) is an area of highly active research.
Acute and Chronic Damage by the STI
The presence of greater numbers of anaerobic organisms in the non-optimal cervicovaginal microbiome leads to increased vaginal discharge and malodor—which can be distressing to and even stigmatizing for patients. Some women also note itching, though this symptom is less common as vulvovaginal irritation is not prominent in BV (Bennett et al. 2010). Cervicitis may be appreciated (Mitchell and Marrazzo 2014). Given new research utilizing metagenomics to identify the content of cervicovaginal bacteria, we now know that women can have a non-optimal microbiota without being acutely asymptomatic; that is to say, women can have BV without having any obvious symptoms (McKinnon et al. 2019). The presence of non-optimal cervicovaginal microbiota, regardless of presentation, increases risk for infection after gynecologic surgeries, including abortion procedures (Bennett et al. 2010). BV is associated with an increased risk for endometritis and salpingitis; during pregnancy, BV is associated with preterm membrane rupture, preterm labor, and postpartum endometritis (Bennett et al. 2010). The overall pro-inflammatory state increases the likelihood of STI transmission, including HIV—women with BV have an increased risk for contracting and transmitting HIV during sex (McKinnon et al. 2019). BV is considered treatable but has a high rate of persistence and recurrence (Bennett et al. 2010). The reestablishment of the optimal cervicovaginal microbiome, which cannot occur merely by anti-infective treatment, is likely integral in curing disease and preventing recurrence.
Prevention of the STI
We again note that BV is not a “typical” STI, and it is possible for women without a history of sexual activity to have a non-optimal cervicovaginal microbiome. Nonetheless, abstinence from sex, small numbers of sexual partners, and use of condoms during penile–vaginal intercourse decreases the likelihood of BV. For patients with recurrent/persistent BV, it is reasonable to consider that treatment of sexual partners may improve BV outcomes. However, small studies evaluating BV treatment for the male sexual partners of women with BV have not demonstrated improved female outcomes (Bennett et al. 2010). Depending on shared decision making, such approaches—which have no current supporting scientific evidence—may yet be reasonable for individual couples.
Chlamydia, Gonorrhea, and Pelvic Inflammatory Disease
Human Burden of the STI
In this section, we discuss sexually transmitted chlamydia and gonorrhea jointly, as coinfection is common and both pathogens cause similar types of acute and chronic damage to the human person. Chlamydia is caused by Chlamydia trachomatis (CT) and gonorrhea is caused by Neisseria gonorrhoeae (GC). After ascending from the cervix, pathogenic bacteria such as CT and GC drive inflammation in the upper genital tract, potentially causing PID. In fact, CT and GC are the most common known causes of PID. Sexual contact is the primary risk driver for both infections, with chlamydia infection heavily driven by frequency of sexual contact and gonorrhea primarily by new sexual partnering (Bennett et al. 2010). Factors associated with chlamydia diagnosis include age 15–24 years, female sex, and Black or Hispanic race/ethnicity; for GC, men are the primary diagnostic group, likely driven by the frequency of GC among the sexual networks of MSM (Bennett et al. 2010). People with repeated positive GC tests are more likely to have any of the following characteristics: male, aged ≥25 years old, co-infected with HIV or CT, or being tested at an STI clinic (which may indicate decreased repeat testing at primary care centers) (Wijers et al. 2020). When narrowing to individuals tested solely at STI clinics, people repeatedly diagnosed with GC are more likely to have urogenital symptoms or proctitis, have been notified of the need for STI testing, or to be MSM (Wijers et al. 2020). PID risk factors—in addition to the aforementioned younger age, new sexual partnering, number of sexual partners, and frequency of sexual contact—include BV, cigarette smoking, douching, substance use, intrauterine devices, and possibly oral contraceptives (Bennett et al. 2010).
Per the global 2016 WHO data, reported chlamydia case rates surpassed gonorrhea case rates in all regions (WHO 2016). CDC modeling for 2018 disclosed 4 million incident chlamydia infections among U.S. individuals aged 15–39 years, with women accounting for 60% of chlamydia diagnoses; for gonorrhea, there were 1.6 million incident diagnoses in the U.S. population, with women accounting for 55% of gonorrhea diagnoses (Kreisel et al. 2021). By age stratification, the 15- to 24-year-old group accounted for approximately two-thirds of all incident chlamydia diagnoses and just over half (51%) of all incident gonorrhea diagnoses (Kreisel et al. 2021). Worryingly, 804,000 (52%) of incident U.S. 2018 gonorrhea infections demonstrated rising resistance to frequently used antibiotics (Kreisel et al. 2021). WHO global incidence estimates showed 127.2 million new chlamydia cases and 87.6 million new gonorrhea cases in 2016 (Rowley et al. 2019). Global prevalence of chlamydia was highest in upper-middle-income countries (noting that prevalence of chlamydia in females was highest in the WHO region of the Americas, while the WHO African region accounted for most male diagnoses of chlamydia). Gonorrhea prevalence was highest in low-income regions by economy and in the WHO African region territorially (Rowley et al. 2019).
Estimated lifetime medical costs to treat chlamydia and gonorrhea in males average $46 and $78, respectively (Kumar et al. 2021). Similar costs to women average $262 for chlamydia and $254 for gonorrhea, sensitive to the probability and cost of consequent PID (Kumar et al. 2021). Using these dollar averages against the aforementioned incidence cases, chlamydial economic cost sits somewhere between $184 million and $1.048 billion in the United States, while ranging between $5.8 and $33.3 billion worldwide. Gonorrheal economic cost sits somewhere between $125 and $406 million in the United States, while the global incident gonorrheal cost range is $6.8 billion to $22.3 billion. Note that the low end of these ranges reflects the cost if all cases were diagnosed in males (who have lower attendant lifetime medical costs), while the upper end overestimates by applying the female average cost to all incident cases. As (1) overall prevalence is higher than incidence, (2) the estimations do not reflect non-sexual cases such as neonatal chlamydial conjunctivitis, and (3) national/worldwide sexually derived cases almost certainly go undiagnosed and unaccounted for (especially given low rates of pharyngeal and anal screening) (Bennett et al. 2010; Kreisel et al. 2021), the true economic cost that chlamydia and gonorrhea cause to the human species is likely even higher.
How the STI Attacks
We will limit discussion on C. trachomatis strains (or serovars) to those which cause genital tract disease (serovars D through K) and lymphogranuloma venereum (LGV; serovars L1, L2, and L3). While genes are highly conserved across CT strains, antigenic cross-reactivity differentiates the serovars and is associated with differences in virulence, accounting for distinctions in clinical presentation by serovar (Bennett et al. 2010). The transmissible elementary body of CT attaches to and enters human epithelial cells, where (presuming it can acquire needed nutrients from the host) it forms a cytoplasmic inclusion, transitions into the reticulate body, and replicates by binary fission (Murray and McKay 2021). On the second day, the reticulate bodies begin converting into elementary bodies. Within 72 h from initial infection, anywhere from 100 to 1,000 new elementary bodies exit the host cell (sometimes—but not always—causing host cell death in the process) (Bennett et al. 2010). LGV usually completes the lifecycle more rapidly; additionally, LGV serovars are carried to the lymphatic system, where they infect phagocytic cells. In doing so, LGV can infect systemically, giving rise to bacteremia and CNS disease. Host cells infected by CT produce cytokines, driving immune and inflammatory responses. Some individuals can clear CT without treatment. However, it appears CT can evade immune clearance for a sustained period—likely by remaining arrested intracellularly—during which replicative cycles cause ongoing inflammatory signaling (Murray and McKay 2021). Natural infection seems to confer little longstanding immunity, and persistence or reinfection is common.
While CT is obligately intracellular, GC is facultatively intracellular. N. gonorrhoeae can attach to and enter epithelial cells, crossing into the subepithelial space. This process is facilitated by outer membrane proteins (Opa proteins), some of which can even bind B and T cell receptors, downregulating the host immune response and likely contributing to the difficulty in clearing the infection (Bennett et al. 2010). The organism's lipo-oligosaccharide has endotoxic activity and its peptidoglycan appears to contribute to a pro-inflammatory state (Bennett et al. 2010). As the pro-inflammatory state drives clinical symptoms, GC varies its surface proteins to evade the host response (Murray and McKay, 2021). Through a variety of mechanisms, GC recruits neutrophils, protects itself from neutrophil-induced damage, and then manipulates the adaptive immune cell response toward a Th-17 response, driving additional inflammation and preventing protective immunity from arising (Murray and McKay, 2021). Additionally, GC has developed a number of resistance pathways against antibiotics: penicillin-binding protein alteration and β-lactamase production; plasmid-mediated tetracycline resistance, chromosomal mutation resistance against penicillins, fluoroquinolones, and cephalosporins; and antibiotic efflux mechanisms (Bennett et al. 2010). Indeed, the rising antibiotic resistance of N. gonorrhoeae is so concerning that untreatable strains may well spread (Rowley et al. 2019).
Acute and Chronic Damage by the STI
Acutely, CT may cause salpingitis, epididymitis, or proctitis. Neonates can acquire the infection during vaginal birth, developing conjunctivitis and pneumonia (Bennett et al. 2010). LGV primarily presents with inguinal lymphadenopathy or severe proctocolitis (Bennett et al. 2010). Serovars D through K can cause an acute conjunctivitis; individuals with inclusion conjunctivitis may well have a simultaneous genital tract infection despite the absence of symptoms. (Inclusion conjunctivitis is not to be confused with trachoma, the chronic keratoconjunctivitis caused by serovars A through C in highly endemic areas—trachoma is not spread by sexual contact.) Gonorrheal infection may present acutely with purulent urethritis or epididymitis in males, with penile lymphangitis, periurethral abscess, and acute prostatitis less common (Bennett et al. 2010). Men can often clear the infection (Kreisel et al. 2021). GC infection in women is often subclinical but may present acutely with dysuria or perhaps increased vaginal discharge or bleeding (Bennett et al. 2010). Rectal gonococcal infection is also usually asymptomatic but may cause proctitis, tenesmus, or rectal discharge. Yet again largely asymptomatic, pharyngeal GC may cause submandibular/cervical lymphangitis or overt pharyngitis. Neonates can also acquire a congenital gonococcal infection. Finally, GC may disseminate, causing arthritis-dermatitis syndrome or septic arthritis (less common presentations include endocarditis, meningitis, osteomyelitis, septic shock, and acute respiratory distress syndrome) (Bennett et al. 2010).
Presence of gonorrhea or chlamydia increases the risk of HIV transmission and acquisition (Rowley et al. 2019). Chronically, the inflammatory response to CT and GC can lead to extensive tissue scarring, causing end-organ damage (Bennett et al. 2010). Perhaps as much as 10% of untreated chlamydial infections in women give rise to diagnosed PID; risk from untreated gonococcal infection is likely higher (CDC 2018). While PID is declining nationally, it is still a major cause of morbidity in women. PID can present with endometritis, salpingitis, tubo-ovarian abscess, pelvic or lower abdominal pain, and even perihepatitis. Ectopic pregnancy and infertility may result in the setting of primary CT/GC infection or of PID (Bennett et al. 2010). Chronic pelvic pain, dyspareunia, and pelvic adhesions may also result. LGV may also give rise to chronic ulceration and fibrosis of the affected urogenital and gastrointestinal tracts.
Prevention of the STI
The main risk for acquisition of GC and non-trachoma CT is sexual contact; limiting intimate interaction (noting that for GC, this also includes orogenital sex and deep kissing) drastically reduces STI risk, as does utilization of condoms. A mainstay of public health control of STIs, screening of sexually active individuals for chlamydia and gonorrhea is indicated with special attention to women <25 years, pregnant women of all ages, individuals with high-risk sexual practices (multiple partners, MSM, people who sell or trade sex), or people evaluated at detention centers or STI clinics (Bennett et al. 2010). Note that screening should not be limited to urine alone, but vaginal and extragenital sites (pharynx and anus) should also be considered. Sex partners should be referred for treatment as well. Given the high risk of STI recurrence (especially of GC due to rising resistance), people with diagnoses of CT or GC undergo repeat testing, usually at least within 3 months.
Interest in C. trachomatis vaccination is driven in large part by the organism's role in causing blindness (C. trachomatis serovars A, B, Ba, and C cause trachoma, a leading infectious cause of blindness) (Bennett et al. 2010). Advances in anti-chlamydia vaccination have been made; however, it may prove difficult for a single vaccine to provide wide protection against all serovars (Murray and McKay 2021). Vaccination efforts against gonorrhea remain of great interest but are limited by the incredible antigenic variability of the organism (Bennett et al. 2010).
Human Papillomavirus
Human Burden of the STI
HPV types are widespread in nature but remain species-specific; of the HPV strains infecting humans, some are high risk for cancer induction (HPV types 16, 18, 21, 22, 45, 52, and 58), while others cause genital warts (HPV 6 and 11) (Senkomago et al. 2019). Almost all people who have sexual encounters are thought to be diagnosed with HPV in their lifetime; risk is elevated further by young age of coitarche, number of sexual partners, frequency of intimate contact, and presence of HPV in sexual partners (Bennett et al. 2010). Note that women with HPV can transmit HPV to female sexual partners; women who have sex only with women should not be excluded from HPV screening or prevention efforts (Gorgos and Marrazzo 2011). In 2018, at least 26 million people in the United States aged 15–59 years old were diagnosed with a disease associated with HPV (e.g., genital warts, precancerous HPV-changes, or HPV-induced cancers), with the greatest number of diagnoses in the 15- to 24-year-old age group (Kreisel et al. 2021). Women were most likely to be newly diagnosed with HPV-associated disease. HPV not only accounted for 50% of all U.S. STIs diagnosed in 2018 but was also the most prevalent STI overall (63%) (Kreisel et al. 2021). In the United States, HPV accounts for ∼35,000 cancer diagnoses (Senkomago et al. 2019). The WHO estimates that 291 million women have HPV worldwide (Rowley et al. 2019). Per WHO data in 2016, HPV was responsible for ∼530,000 cases of cervical cancer globally—and at least 264,000 deaths from the same (Rowley et al. 2019).
How the STI Attacks
In breaching the epithelium, HPV viral particles bind to the basement membrane and basal cell layer (Bennett et al. 2010). The viral DNA replicates as the basal layers advance toward the surface, eventually releasing virions into the epidermis. Excessive viral-induced cell proliferation at this stage will produce acanthosis, parakeratosis, and hyperkeratosis, observed clinically as warts or condyloma. If, instead, the excessive proliferation occurs at the basal layer of the dermis, a high number of abnormal mitoses may occur and give rise to malignancy. Oncogenic HPV-induced basal cell proliferation is associated with angiogenesis, cytokine production, and chemokine release. For the host's part, the immune system appears able to clear some HPV infections (though without reliable development of humoral or cellular immunity); mechanisms of host clearance and immunity are unclear. Most HPV infections are transient, lasting no longer than 14 months (Bennett et al. 2010). However, HPV appears more persistent, frequent, and severe in individuals with immunocompromising conditions such as HIV and common variable immunodeficiency—these individuals may not be able to clear HPV once acquired, and ongoing inflammation and dyskaryosis may result.
Acute and Chronic Damage by the STI
Genital warts may be observed by the patient or their sexual partner(s); often grey or flesh colored, these hyperkeratotic and exophilic papules may be pedunculated or merge together into plaques (Bennett et al. 2010). In men with HPV, the penile shaft is the most common site for genital warts with varying involvement of the urethral meatus, which may cause obstructive symptoms. For MSM, the perianal area is also commonly involved; the likelihood of perianal involvement is increased for MSM who have HIV. Lesions in females will often be noted at the posterior of the vaginal introitus, but may involve the labia or clitoris. Neonates can acquire HPV during passage through the infected vaginal canal, later presenting with recurrent respiratory papillomatosis (often around age 3).
Presence of HPV increases the risk of HIV acquisition in women by increasing the permeability of genital tissue; this observation may be true for men as well (Houlihan et al. 2012). Malignant transformation of HPV-induced genital warts to condyloma may occur. High-risk oncogenic HPV can also cause intraepithelial neoplasia, whether of the cervix (CIN), vulva (VIN), vagina (VAIN), penis (PIN), or anus (AIN). Intraepithelial neoplasia may advance to cancer; oropharyngeal cancer can also arise from HPV contracted during orogenital sex—and rates of HPV-associated oropharyngeal cancer outpace HPV-associated cervical cancer (Senkomago et al. 2019). For areas other than the cervix, squamous cell cancer is most likely to occur; cervical cancers may be adenocarcinomas or squamous cell carcinomas (Senkomago et al. 2019).
Prevention of the STI
Avoidance of sexual contact, limiting of sexual partnering, and use of condoms decrease the likelihood and rate of HPV acquisition (Bennett et al. 2010). Medical male circumcision is protective against HPV, reducing male risk of HPV acquisition by 32–35% and reducing the risk to female partners by 28% (Tobian and Gray 2011). Cervical screening for HPV and associated changes should be performed in accordance with CDC guidelines. There is rising interest in anal HPV screening for people with a history of receptive anal sex, but no clear guidelines are codified as of this writing.
The quadrivalent HPV vaccine (active against types 6, 11, 16, and 18) has a 98.2% efficacy in preventing cervical intraepithelial neoplasia (CIN) in women without preceding evidence of HPV infection (Bennett et al. 2010). Vaccine efficacy against CIN fell to ∼44% when women with prior exposure to HPV or known atypical squamous cells of unknown significance were included in the analysis. However, efficacy against external genital lesions was as high as 76% (Bennett et al. 2010). For boys and girls aged 9 to 15 years, post-vaccine neutralizing antibody levels appear to correlate with protection. Use of this vaccine in the adult population of people with HIV is also based on neutralizing antibody levels, but importantly, no minimum protective antibody level has been established. At this time, vaccination against HPV in the HIV community is considered to have greater potential benefit than possible harm. Overall, in locations where vaccination has been deployed, HPV incidence has dropped in women and in men who have sex with women by as high as 90% (Bennett et al. 2010).
Hepatitis B Virus
Human Burden of the STI
HBV is widespread and endemic in many areas of the world. HBV can be transmitted sexually, perinatally, and by contaminated blood products or in hemodialysis (Bennett et al. 2010). Close household contacts of HBV and people who work in centers for the developmentally disabled may acquire the virus, with some form of blood transmission likely underlying the method of acquisition. We have included HBV as the disease can be transmitted in the same way as HIV. Sexually transmitted HBV is more commonly seen in MSM, people who have sex with multiple partners, people whose sexual partners have HBV, and people with prior or current STI diagnosis (Kreisel et al. 2021). The rate of HIV-HBV coinfection is as high as 25% in HBV-endemic areas. HBV and hepatitis C coinfection is more likely in endemic areas as well, especially in the setting of substance injection.
Please note that statistics may fail to capture the true burden of sexually transmitted HBV in light of the multiple routes of possible transmission of this widespread virus. The CDC estimated 8,300 sexually transmitted cases of acute HBV in 2018 (Kreisel et al. 2021). Chronic HBV in the United States is most frequent in the foreign-born population and therefore more likely to be endemically derived than sexually acquired; accounting for this in the modeling, the CDC estimated 103,000 cases of sexually acquired chronic HBV in the United States in 2018 (Kreisel et al. 2021). Worldwide estimates are not usually distinguished by method of acquisition, so data presented here refer to the entire global population of people who have HBV. Worldwide, the WHO estimated there were 269 million people known to have chronic HBV in 2019, and 820,000 people died from the virus that year (WHO 2021). Another 1.5 million people were newly infected with HBV in 2020 (WHO 2021).
How the STI Attacks
HBV primarily attaches to and enters hepatocytes but does not immediately cause them damage. HBV's partially double-stranded DNA closes into a circle after entering the nucleus; in the covalently closed circular DNA form, HBV is more resistant to host immune action as well as antiviral therapy. Recovery from acute infection—perhaps through natural killer, virus-specific, and cytotoxic T lymphocyte responses—often confers immunity against HBV (Liang 2009; Bennett et al. 2010).
However, individuals with impaired cellular response may have difficulty in clearing the infection, setting up chronic HBV (Bennett et al. 2010). HBV also uses viral RNA for transcription and can integrate into the host genome; this integration may enable the virus to better persist in infected cells (Liang 2009). The mechanisms by which HBV evades the immune response and foils the ability of the host clearance remain poorly understood (Bennett et al. 2010). Persistent infection leads to chronic HBV with longstanding necroinflammatory activity, causing fibrotic damage. Chronic HBV infection can also spur oncogenesis, though the exact trigger(s) again remain unidentified: Genomic instability due to repeated viral-host integrations; effects on DNA repair, apoptosis, and oxidative damage; and overall inflammatory state have been implicated.
Acute and Chronic Damage by the STI
HBV's disease spectrum is wide. Some two-thirds of patients will remain asymptomatic carriers of the virus throughout their lives (Liang 2009). The host inflammatory response, should it occur, can result in a self-limited hepatitis (causing fatigue, nausea, and possibly mild jaundice) or may cause fulminant liver failure (causing fever, vomiting, jaundice, disorientation/confusion, coma, and even death) (Bennett et al. 2010). A serum-sickness-like syndrome may be seen, as can polyarteritis nodosa or membranous glomerulonephritis (Liang 2009). Acute presentations of hepatitis B are usually seen within 4 months of acquisition (Bennett et al. 2010).
One-third of patients who acquire HBV will develop chronic disease (Liang 2009). HBV acquisition in MSM or people with HIV is more likely to progress to chronic hepatitis, which risks the complications of cirrhosis, hepatocellular carcinoma, end-stage liver disease, and death (Bennett et al. 2010).
Prevention of the STI
Factors decreasing the risk of acquiring sexually transmitted HBV include limiting sexual partnering (including abstinence) and use of condoms. Sexual and close contacts of people with HBV should be screened and either vaccinated or treated if indicated. Ensure that individuals with HBV cover open wounds and do not share toothbrushes or injection equipment (Bennett et al. 2010). Pregnant women with HBV can be administered hepatitis B vaccine with immunoglobulin to decrease the risk of perinatal transmission; this regimen can also be administered as postexposure prophylaxis to the nonimmune sexual contacts of people with HBV (Bennett et al. 2010).
All people with HIV or at risk for HIV should be screened for hepatitis. It is exceedingly important that the antiviral regimen of patients with HIV/HBV coinfection has activity against both HIV and HBV. Patients with untreated chronic HBV will continue to produce HBV antigen, and (usually) HBV DNA; those on HBV-active treatment should have undetectable HBV DNA titers. Vaccination against hepatitis is also of preventative and public health interest in the general population and of integral importance in the HIV cohort. Testing showing anti-HB core with anti-HB surface indicates prior infection, while anti-HB surface alone indicates immunity by vaccination (Liang 2009). Stimulation of HBV protection can be difficult in people with HIV, perhaps due to attenuated HBV-specific memory B cell response (Bennett et al. 2010). The typical vaccination schedule against HBV requires immunization at time 0, 1–2 months, and 6–12 months; double-dosing the series should be considered in people with HIV who are not protected against HBV.
Herpes Simplex Virus
Human Burden of the STI
HSV types 1 and 2 (HSV-1 and HSV-2) are widespread but limited to humans; most humans will acquire HSV-1 by their 50s (Bennett et al. 2010). Traditionally, HSV-1 is considered the cause of orolabial lesions while HSV-2 is associated with genital herpes; as such, many consider HSV-2 the sexually acquired herpes virus. However, receptive orogenital sex has now been associated with HSV-1 genital herpes acquisition (Gorgos and Marrazzo 2011), making it more difficult to utilize seroprevalence of HSV types to monitor genital herpes. Risk factors for sexually transmitted HSV include female sex (perhaps due to increased amount of tissue exposed to the virus), frequency of sex with the same partner, and the presence of BV (Gorgos and Marrazzo 2011). Women who have sex with both men and women appear to have a higher likelihood of acquiring genital herpes than women who only have intimate contact with one sex. Neonatal HSV infections are usually perinatally transmitted; these infections are uncommon but may be underestimated as neonatal HSV is not a nationally notifiable/reportable condition (CDC 2018).
Estimates of herpes-related genital lesions often use HSV-2 seroprevalence statistics only, so the burden of sexually transmitted HSV may be underestimated. The CDC estimated at least 572,000 new HSV-2 infections in 2018 among U.S. individuals between 15 and 49 years of age, with 52% of diagnoses among males by sex and 42% of diagnoses among 15 to 24 years old by age (Kreisel et al. 2021). Overall, there were 18.6 million prevalent HSV-2 infections in the United States in 2018 (Kreisel et al. 2021). The WHO estimates that 417 million people have HSV-2 worldwide (Rowley et al. 2019).
How the STI Attacks
After gaining entry at mucosal sites or disrupted skin, HSV replicates in the epidermis and dermis, later traveling along the nerves (Bennett et al. 2010). HSV attaches to different cell types—including sensory neurons—and thus replicates in multiple tissues of the body. If completing the production cycle, HSV exerts a cytopathic effect on cells within one day. If instead neuronal cells are infected, the viral genome may persist in a repressed, latent state; viral copy number is highly variable between neurons, and daughter virions may be nearly continuously shed without apparent damage to the neuron. Infection of epithelial cells by daughter virions released from neuronal cells is called reactivation. Here, the virus may shed subclinically or cause blistering and ulceration. When untreated, genital tract reactivation of HSV may occur multiple times per month (Bennett et al. 2010). Both innate and acquired host immunity work to defeat the virus, with mucosal interactions impacting the development of clinical disease. Pregnant women who acquire HSV-2 late in their pregnancy may not have any symptoms, yet can shed the virus subclinically and pass it to their child during delivery without also having a large antibody level from which the child can benefit. HSV-2-specific CD8+ T cells help to hold the virus at bay, containing HSV at infected tissues and preventing dissemination (Bennett et al. 2010).
Acute and Chronic Damage by the STI
Primary infection by HSV-2 results in 10–12 days of painful lesions, which can appear as vesicles, pustules, and/or erythematous ulcers, possibly producing clear mucoid discharge or may crust (Bennett et al. 2010). One-quarter of people with genital HSV-2 develop extragenital lesions, commonly orolabial. Associated symptoms of primary HSV-2 include fever, headache, malaise, myalgias, dysuria, vaginal or urethral discharge, and tender inguinal lymphadenopathy. Notably, the painful aspect of the dysuria is usually more pronounced than the observed urethral discharge. Painful cervicitis may also be seen, and while the clinical presentation may be difficult to distinguish from CT and GC, cervical ulceration and necrosis are often pathognomonic for HSV-2. Infection via anal sex is associated with proctitis, rectal ulceration, and perianal involvement, causing anorectal pain and discharge, tenesmus, and constipation—these presentations are often more symptomatic and severe in people with HIV. Infrequently, acute infection may present with endometritis, salpingitis, or prostatitis. Neonatal herpes can be truly severe, causing even seizures or failure of the respiratory system and liver.
Acute HSV-2 infection can cause extragenital presentations, such as overt viral meningitis (Bennett et al. 2010). Very rarely, acute meningitis may be the only presentation of primary HSV-2 infection. Genital HSV infection is also associated with autonomic nervous dysfunction, characterized by hyperesthesia/anesthesia, urinary retention, and constipation. Transverse myelitis and bloodborne dissemination rarely occur.
Genital herpes reactivation occurs frequently in the untreated state but can do so asymptomatically (Bennett et al. 2010). Recurrence of genital lesions during viral reactivation is usually localized, mild or moderate in presentation, and shorter in duration than the primary infection. A prodrome varying from mild tingling to shooting pain may precede the appearance of lesions by 1 to 5 days. Reactivation in patients with meningitis can cause recurrent meningitis, which resolves without neurologic sequelae. Reactivation in immunosuppressed individuals can parallel primary presentation in neonates (meningitis, interstitial pneumonia, hepatitis) and can be life-threatening.
HSV-2 infection is associated with an increased risk for acquiring HIV (Bennett et al. 2010). Bacterial superinfection of genital lesions can also be seen; fungal vaginitis and concurrent yeast infection are seen more frequently in women with HSV. It is unclear if HSV activity increases the likelihood of developing BV or if the association between BV and HSV is driven by BV-induced disruption of the cervicovaginal microbiome. Finally, genital herpes can cause psychological distress and impact intimate emotional relationships.
Prevention of the STI
Avoiding or minimizing sexual partnering decreases risk for acquisition of HSV-2; use of barrier protection during sexual activity (including during orogenital sex) also limits risk. In addition to lowering risks associated with other STIs, medical male circumcision decreases the risk of acquiring HSV by 28–34% and lowers the risk of genital ulceration by 47% (Tobian and Gray 2011). People with HSV-2 can transmit the virus to their sexual partners even without active symptoms; persistent subclinical shedding is more common in HIV/HSV coinfection (Bennett et al. 2010). Because of this, patients with HSV-2 should be counseled to be sexually abstinent during prodrome or when genital lesions are present. Valacyclovir suppresses viral shedding and therefore decreases the likelihood of transmission of HSV—but, importantly, use of valacyclovir does not nullify the risk of transmitting HSV during recurrence, and abstinence should still be pursued during prodrome or active symptoms even if on valacyclovir. Efforts to create a functioning vaccine continue.
HIV/AIDS
Human Burden of the STI
HIV was first identified as the causative agent of AIDS (autoimmune deficiency syndrome) in 1983 (Bennett et al. 2010). HIV is primarily spread via sexual transmission, with heterosexual sex accounting for most infections in sub-Saharan Africa, Asia, and the Caribbean. In all actuality, the risk associated with acquiring HIV through one episode of condomless penile–vaginal sex is low (see Table 1); but risk is raised if penile–vaginal sex occurs during menses, if the male is not medically circumcised, if individuals have genital ulcer disease, if the partner with HIV is in acute primary infection or advanced infection, and in presence of other STIs (e.g., BV, chlamydia, gonorrhea, HPV, HSV, and trichomoniasis—all of which may be asymptomatic at the time of sex) (Bennett et al. 2010; Houlihan et al. 2012; Leitsch 2016; Rowley et al. 2019). Therefore, what an exposed individual perceives as their risk of HIV acquisition may be much lower than their actual risk. As can be seen in Table 1, anal intercourse carries a high risk, especially for the receptive partner (Patel et al. 2014). In the United States, Black MSM are currently at the greatest risk for HIV diagnosis (Bennett et al. 2010). In addition to MSM, men who identify as “transgender” are also at increased risk of HIV acquisition. There is an increased rate of anal receptive sex in the MSM and “transgender” identifying populations, as well as greater rates of sexual partnering, condomless sex, use of substances during sex, and high prevalence of HIV and syphilis within sexual networks (Bowers et al. 2012; Fujimoto et al. 2018). Women who have sex with women may be able to acquire HIV from their female partners, though this manner of acquisition appears quite rare—certainly, women who inject substances or women who have sex with men are at greater risk for HIV acquisition (Gorgos and Marrazzo 2011). Injection use disorder (wherein individuals utilize needles to inject compounds into the venous system in order to produce euphoria) accounts for perhaps one-third of HIV infections outside of Africa (Bennett et al. 2010). Injection use may be coupled with sexual activity, increasing the risk of HIV transmission in injection use disorder. Finally, people in prison or without secure housing, individuals in conflict zones, and people who sell or trade sex are at increased risk for HIV acquisition (Rowley et al. 2019). These high-risk groups (MSM, people who identify as “transgender,” people who sell or trade sex, individuals in prison or conflict zones, and those who inject drugs) account for 62% of new HIV infections worldwide (WHO 2021).
Risk of HIV Acquisition by Exposure.
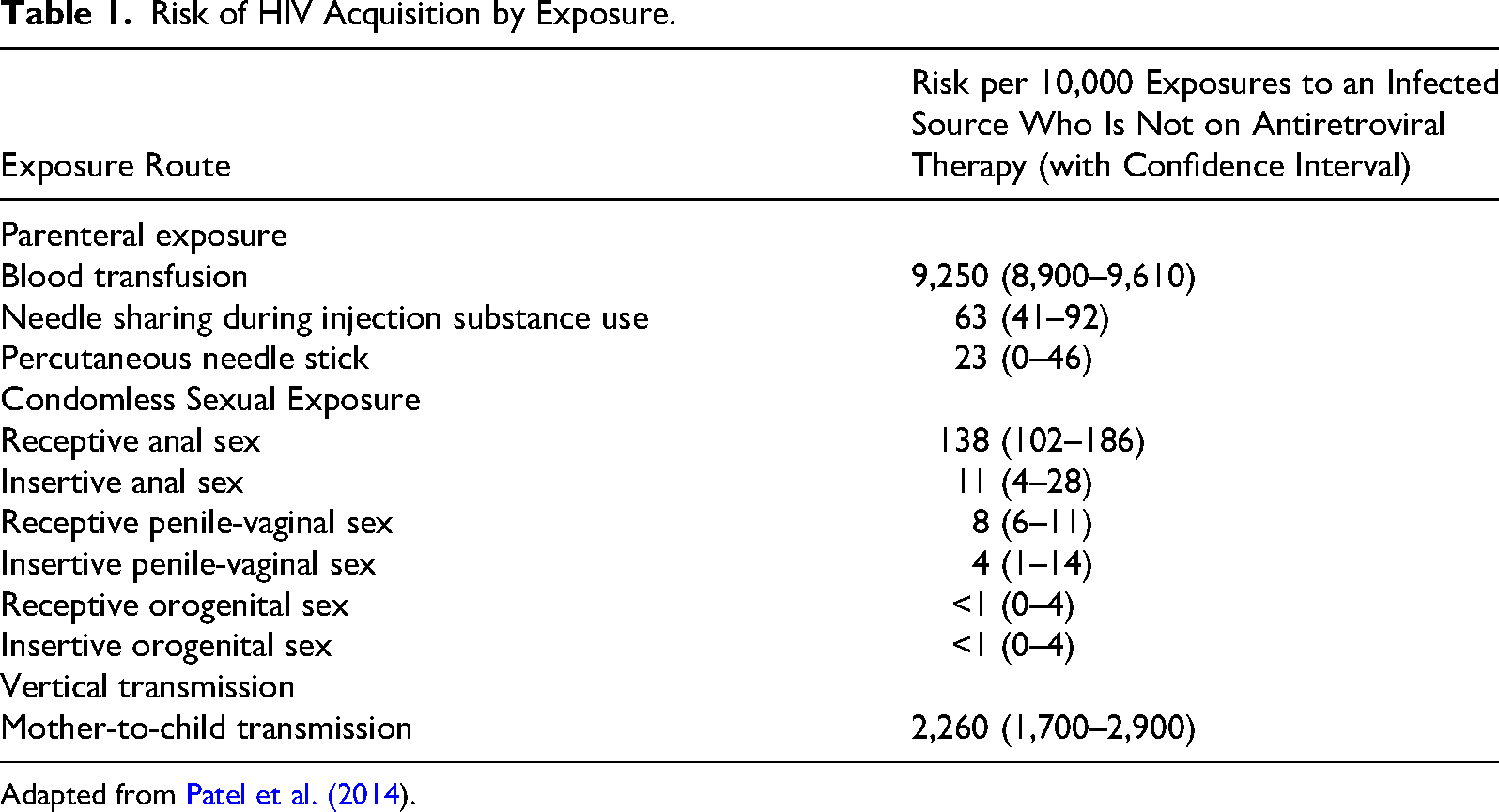
Adapted from Patel et al. (2014).
2018 U.S. data revealed 32,000 new sexually acquired HIV diagnoses among people aged 13 years or older; almost 83% of these new HIV infections were among males (Kreisel et al. 2021). A concerning 22% of new HIV infections were diagnosed among people 13 to 24 years old (Kreisel et al. 2021). In total, there are an estimated 984,000 people with HIV living in the United States (Kreisel et al. 2021). Per WHO estimates, there are at least 37.7 million people in the world living with HIV, with an additional 1.5 million people acquiring HIV in 2020. The disease killed at least 680,000 people in 2020 (WHO 2021), and a disproportionate share of these deaths occurred in Africa (Bennett et al. 2010).
How the STI Attacks
After entry into the body, HIV quickly migrates to regional lymph nodes and disseminates through the bloodstream to other lymphoid tissues, binding to CD4+ cells, macrophages, and Langerhans cells at both CD4 and the CCR5 chemokine receptors (Bennett et al. 2010). There are some antiretroviral therapies (ART) that attempt to target viral docking, fusion, and entry, but these ART do not form a reliable backbone of therapy. After fusion, viral proteins and RNA enter the host cell cytoplasm, where reverse transcription occurs; this is a major target area for some ART. Following active transportation into the nucleus, viral DNA is integrated into the host DNA (another ART target); following transcription, viral RNA is exported to the host cytoplasm for translation, processing, and assembly (additional ART targets). If viral replication has progressed unimpeded by ART, virions will then bud from the host cell membrane, released back into the tissue and bloodstream to infect other targets.
Host antibodies do bind HIV proteins early after infection, but unfortunately, this binding is non-neutralizing and does not protect against ongoing infection (Bennett et al. 2010). Antibodies with some neutralizing capability appear several weeks after infection, but cannot eliminate all the circulating virus—the host immune response does not “catch up” to the infection. Host CD8+ T cells restrict viral replication but do so inadequately; also of great importance, virus-specific CD4+ cells—one of the cell types destroyed by HIV—are critical to create and maintain an effective CD8+ response. HIV boasts an impressive variety of immune evasion techniques, which include (but are not limited to) envelope protein glycosylation, co-receptor binding, and genetic variation (the population of circulating HIV is highly diverse, and “escape” mutants are especially adept at evading the host response).
Amazingly, some people off ART can somehow control HIV for many years. These “long-term nonprogressors” or “elite controllers” (LTNP/ECs) have low viral loads and normal CD4 counts, despite the lack of ART (Bennett et al. 2010). Many studied LTNP/ECs have been found to produce strong HIV-specific CD4+ responses, but other patients whose HIV disease progresses have been found to produce this response as well. The total set of mechanisms at play in LTNP/ECs are unclear, but the existence of LTNP/ECs hints that there is some conglomeration of human immune responses that together can control HIV, at least for a period of time. It should be noted that almost all these LTNP/EC individuals will eventually progress to AIDS if left untreated; all people with HIV are recommended to be on ART even if they appear to control the virus.
Acute and Chronic Damage by the STI
Though one-third of patients with acute HIV infection may be asymptomatic, individuals experiencing symptoms may note an acute “mononucleosis-like” syndrome (Bennett et al. 2010). The acute retroviral syndrome is marked by fever, adenopathy, pharyngitis, rash, and myalgia/arthralgia; less commonly seen are leukopenia, thrombocytopenia, headache, oral aphthous ulcers, thrush, nausea/vomiting, diarrhea, elevated aminotransferase levels, hepatosplenomegaly, neuropathy, and encephalopathy. Persistent generalized lymphadenopathy can be seen in 50–70% of people (Bennett et al. 2010). While this usually responds to ART (perhaps enlarging before involuting), infections and cancers should remain on the differential for physicians treating this presentation. Months to years after primary infection, patients may note anxiety/depression, mild wasting and constitutional symptoms, hypogonadism, and pyomyositis. Cutaneous manifestations are especially diverse along the HIV-infection timeline.
Approximately 75% of individuals with chronic, untreated HIV inexorably progress to adult immunodeficiency syndrome (AIDS) within ∼10 years (Bennett et al. 2010). The diagnosis of AIDS—again, if left untreated—confers a mean survival time of 12–18 months (Bennett et al. 2010). Without prophylaxis, many opportunistic infections can occur during AIDS status, including cytomegalovirus, HSV, varicella zoster virus, Cryptosporidia, microsporidia, mycobacteria (especially Mycobacterium avium complex and M. tuberculosis), Candida species, Pneumocystis jiroveci, Histoplasma, Cryptococcus, and Toxoplasmosis gondii. Bartonella henselae and HHV-8-induced Kaposi's sarcoma (cutaneous presentations of these can appear similar) are also commonly seen in AIDS. Molluscum contagiosum and scabies infections may occur. People with AIDS status are prone to pneumonias caused by Streptococcus pneumoniae and Haemophilis influenzae; this patient group is also at higher risk for pneumonia from Staphylococcus aureus, Pseudomonas aeruginosa, Nocardia species, and Rhodococcus equi. Hepatitis B or C may be seen (Lin et al. 2020).
AIDS additionally causes a wide variety of non-infectious clinical syndromes (Bennett et al. 2010). Primary CNS lymphoma is the most common HIV-associated brain malignancy; HIV-related dementia and distal sensory polyneuropathy cause significant morbidity. Oral hairy leukoplakia, gingivitis, and periodontitis may be observed. Noninfectious dysphagia or odynophagia may be due to reflux esophagitis, pill esophagitis, esophageal carcinoma, and lymphoma. Cardiac manifestations include accelerated atherosclerosis and myocardial infarction, as well as myocarditis and pericarditis. Non-infectious pulmonary concerns again include lymphoma; lymphocytic interstitial pneumonitis may rarely be seen. Drug-induced liver injury has been observed in some ART regimens, but is less common with modern ART; acalculous cholecystitis and cholangitis are similarly rare when ART is plentiful. HIV-associated enteropathy can cause culture-negative diarrhea, though Clostridium difficile is the most common cause of diarrhea in HIV-infected patients (Bennett, Dolin and Blaser 2010). HIV-related nephropathy may also occur. Finally, patients with AIDS who start ART can develop immune reconstitution syndrome (IRIS), which is usually considered either “paradoxical” or “unmasking.” Paradoxical IRIS indicates that an illness previously diagnosed or discovered gets worse during treatment of the disease in the presence of ART. Unmasking IRIS indicates that a disease previously extant but undiagnosed presents itself in the presence of ART. In either case, the resurging immune system appears to drive worsening clinical presentation, but ART should be continued, as should the pathogen-directed therapy; depending on the disease, nonsteroidal anti-inflammatory medications and corticosteroids may be indicated.
People with HIV—well-controlled or not—also have a high burden of CT and GC coinfection, and coinfection rate is increased in patients with HBV or HCV, patients who practice orogenital sex, and patients who use mobile dating applications (Lin et al. 2020).
Prevention of the STI
Avoidance of sexual partnering is the primary method to eliminate the risk of HIV acquisition; condom use and avoidance of high-risk sexual activity greatly decrease risk. Spermicides do not prevent HIV or STI acquisition; in fact, spermicide's irritative effect on the vaginal tissue may actually increase HIV transmission (Bennett et al. 2010). Screening all pregnant women for HIV is integral to limiting mother-to-child transmission of HIV. Screening for STIs including HIV should also occur after new sexual partnering or with regularity (e.g., every 3 months) in high-risk groups such as MSM who have condomless sex, people who identify as “transgender,” people who sell or trade sex, and individuals using pre-exposure prophylaxis (PrEP, discussed below).
Additionally, the ability of a person with HIV to transmit the virus sexually falls essentially to zero if the patient's HIV viral load is undetectable (Bennett et al. 2010). This concept, “undetectable equals untransmittable” (U = U), speaks to the incredible success of current ART in not only keeping the treated HIV community healthy for their natural lifespans but in potentially arresting the spread of HIV.
Pre-exposure prophylaxis (PrEP) is the use of antiretrovirals prophylactically for those at an elevated risk of possible HIV acquisition; for example, HIV discordant married couples, young MSM, people who identify as “transgender,” people who sell or trade sex, and individuals whose sexual partners have unsuppressed HIV. Ethically speaking, however, there needs to be some distinctions. First, prevention of serious disease is a clear value agreed to by everyone. The best way to prevent the transmission of sexually transmitted diseases, however, is chastity. Second, PrEP requires a doctor to prescribe an anti-retroviral regimen. In doing so, Catholic clinicians need to be careful and thoughtful so that they are not perceived as endorsing immoral sexual activity, which is harmful not only physically, but also emotionally and spiritually. 1 Combination prevention (which includes behavioral interventions, community support, PrEP, U = U, and “treatment as prevention” [TAsP]; Bennett et al. 2010) raises the hope that if almost all the HIV community is diagnosed, engaged in care, and virally suppressed, then the virus will eventually pass from the human experience.
Lastly, there are multiple HIV vaccine candidates in development, some of which have made it to Phase III prior to failure (Bennett et al. 2010).
Syphilis
Human Burden of the STI
Venereal syphilis, caused by the spiral-shaped bacterium Treponema pallidum subspecies pallidum, has captured the attention of many medical professional since approximately the 15th century (Tobian and Gray 2011). Venereal syphilis remains a disease of great—and increasing—burden. Having reached a nadir in the United States between 2000 and 2001 at 2.1 cases per 100,000 individuals, syphilis rates have since increased among all age groups (including neonates) regardless of race/ethnicity or region (Kojima and Klausner 2018). As of 2016, primary and secondary syphilis case rates among men rose to 15.6 cases per 100,000 males, compared to 1.9 cases per 100,000 females. By 2018 CDC modeling, there were 32,000 incident syphilis infections in the 14–24 age group in the United States (Kreisel et al. 2021). Groups at especially high risk for primary and secondary syphilis include MSM (whether with HIV coinfection or not) and Black Americans (Kojima and Klausner 2018). Syphilis affecting pregnancy is estimated by the WHO to cause more than 300,000 in utero and neonatal deaths each year, further placing another 215,000 infants at increased risk of early death (WHO 2016).
Medical professionals should recall that some American syphilis studies were performed with unacceptable and indefensible ethical protocols—extending beyond Alabama (the “Tuskegee Study of Untreated Syphilis in the Negro Male” from 1932 to 1972; Bennett et al. 2010) to other states (the “American Plan” from 1910 to 1950; Stern 2018) and even outside the United States (the “Guatemalan syphilis experiments” from 1946 to 194; Bennett et al. 2010). While the history of syphilis is oftentimes dark, the disease also spurred the Belmont Report, the creation of the National Human Investigation Board, and the modern requirement for institutional review boards (Bennett et al. 2010).
How the STI Attacks
Direct skin-to-skin contact of T. pallidum subspecies pallidum during sexual contact carries a transmission risk of 16–30%. Having gained access through the human epithelium, the treponemes disseminate substantially in early syphilis, capable of invading each organ system by binding the vascular endothelium and passing through the tight junctions (Bennett et al. 2010). The organism's lack of surface-exposed lipoproteins appears to enable T. pallidum to avoid the initial immune response (Cruz et al. 2012), disseminating even to the central nervous system or the placenta of pregnant women in early infection, often without obvious clinical signs or symptoms. It is the subsequent intense cellular immune response that presumably leads to clinical presentations, which are discussed in further detail below. While macrophages can eventually phagocytose the bacteria to control the infection, some of the treponemal population can survive for years and later recrudesce, especially in the absence of antibiotic treatment (Cruz et al. 2012). Syphilologists currently favor an infection model wherein the treponeme population manipulates the phagocytic host response to avoid eradication (Cruz et al. 2012). If immunity occurs after infection, it is short-lived and cannot be relied upon to prevent reinfection (Bennett et al. 2010).
Acute and Chronic Damage by the STI
During the primary stage of infection, painless chancres and regional lymphadenopathy may occur 2 to 6 weeks after initial acquisition at the site of bacterial inoculation (Ghanem, Sanjay Ram and Rice 2020). Thus, while genital chancres are classically known to clinicians, it is important to note that oral or perirectal mucocutaneous lesions are also common. The detection of abnormalities in these areas during routine physical examination should prompt a sexual history interview. Occasionally, meningitis can be seen in primary syphilis. The patient's infection is highly transmissible at the primary stage, whether to sexual partners or perinatally (causing the greatest damage to an unborn child in the second and third trimesters; Bennett et al. 2010), as discussed in further detail at the end of this subsection.
Signs and symptoms beyond the primary stage are driven by the immune system’s response to the treponemal infection, and thus may be easier to detect. Fever, pharyngitis, lymphadenopathy, palmar/solar nonpruritic rash, oral mucous patches, condyloma latum, alopecia, arthralgias, periostitis, nephritis, and even hepatitis can be seen during secondary syphilis (Bennett et al. 2010; Ghanem, Sanjay Ram and Rice 2020). The protean manifestations of secondary syphilis are primarily responsible for syphilis’ moniker as “the great imitator” (Bennett et al. 2010). Syphilis remains highly transmissible during the second stage, which often occurs within 30–60 days after initial acquisition (Ghanem, Sanjay Ram and Rice 2020). Because of its ability to imitate other diseases, infected individuals may not know they have a sexually transmissible disease and carelessly infect others if they are promiscuous.
By contrast, tertiary syphilis is not transmissible, yet presentation remains complex: granulomatous findings (gummas), myocardial or aortic involvement (e.g., aortitis, ascending aortic aneurysm), meningovascular disease (e.g., aphasia, hemiplegia, seizures), destruction of the dorsal spinal roots (tabes dorsalis causing ataxic gait, bladder or fecal incontinence), and chronic dementia-like manifestations may occur (known by the mnemonic PARESIS which stands for
Often detected only by serologic testing, latent syphilis is subdivided by likelihood of relapse, which differs by length of time since exposure. Early latent syphilis, defined as positive serologic testing within 12 months of sexual exposure, carries a greater risk of relapse compared to late latent syphilis, which is defined as positive serologic testing more than 12 months from sexual exposure. During latency, patients are largely asymptomatic, though transmissible skin findings (now more annular in appearance) may occur (Bennett et al. 2010). The absence of symptoms during latency should not be interpreted as complete resolution of infection, but instead as quiescence with risk for recurrent or active spirochetemia (Bennett et al. 2010). For example, pregnant women with even late latent syphilis may yet pass the infection to their unborn children, increasing the risk of miscarriage (spontaneous abortion), stillbirth, and congenital syphilis infection in the neonate (Bennett et al. 2010). If an apparently asymptomatic patient with positive testing does not have a history of treatment, antibiotic therapy should be pursued in accordance with CDC guidelines (Workowski et al. 2021).
Central nervous system involvement can occur at any stage of syphilis infection (Bennett et al. 2010). Regardless of the suspected time course of syphilis infection, a neurologic review should be done. In all suspected or proven syphilis cases, even minimal ocular and otic complaints should be evaluated.
Congenital syphilis is most often caused by in utero infection of the developing child, who can be infected in any trimester of pregnancy relative to the spirochetemia of the mother (therefore, the risk is highest whenever the mother has untreated primary or secondary syphilis). The spirochete infects the placenta and umbilical cord, infiltrating chorionic villi and small blood vessels and presumably leading to inadequate nutrition. In the infected developing child, hepatic dysfunction, severe hematologic anomalies, and even multiorgan compromise can result, with up to 7% of children with congenital syphilis being stillborn (Bennett et al. 2010). Surviving children with clinical disease may have rhinitis (“snuffles”), diffuse rash with sloughing, pemphigus syphiliticus (notably, these skin lesions are teeming with spirochetes), alopecia, hyperbilirubinemia, anemia, glomerulonephritis with nephrotic syndrome, osteochondritis or perichondritis, and even acute syphilitic leptomeningitis (Bennett et al. 2010).
Though these are painful details, in many senses, we give them to destabilize the mantra that one's sexual choices are his or her own. They are not. They clearly affect, and in many cases, infect others.
Prevention of the STI
Abstinence from all forms of sexual activity essentially precludes syphilis transmission, while use of condoms during sexual encounters (thereby placing a barrier between the skin/mucocutaneous tissues of sexual partners) dramatically decreases syphilis spread. In the interests of both improving female sexual health care and limiting congenital syphilis infection, initial prenatal visits should include syphilis screening; the screen should be repeated at 28 weeks’ gestation in high-risk patients (Ghanem, Sanjay Ram and Rice 2020). We encourage diagnosis and complete treatment of active cases among exposed individuals to prevent further syphilis infection within a sexual network. This treatment includes recommending chastity and motivating its importance. Because many patients may not be Catholic or otherwise at all sympathetic to the Church's teachings on love for the human person, chastity may be communicated not strictly in moral terms, but as sound medical prevention.
In this regard, it is important to understand that incomplete treatment of a partner network may result in repeated reinfection. Physicians should be aware that syphilis networks are commonly interwoven with HIV networks, especially in the sexual networks of MSM (Billock et al. 2020). If a patient qualifies for syphilis testing, he/she likely qualify for HIV testing as well (the reverse is also true; suspicion or diagnosis of incident HIV infection should lead to syphilis testing) (Fujimoto et al. 2018). We stress that every diagnosis of syphilis is an opportune time to discuss with patients the risks involved in having multiple sexual partners, the risks of syphilis spread in the community, and the need for potentially exposed partners to be tested and possibly treated.
For nonpregnant patients at high risk for acquisition (including MSM as well as individuals who sell or trade sex), doxycycline prophylaxis strategies have shown decreased rates of syphilis infection (Kojima and Klausner 2018; Workowski et al. 2021). Efforts to develop an effective syphilis vaccine continue (Kojima and Klausner 2018) but are likely limited by the paucity of potential targets on the spirochetal surface (Bennett et al. 2010).
Trichomoniasis
Human Burden of the STI
Trichomoniasis is caused by Trichomonas vaginalis, first described in 1836 and now considered the most common curable STI worldwide (Menezes, Frasson and Tasca 2016; Rowley et al. 2019; Billock et al. 2020). The parasite infects only humans and is considered one of the world's neglected parasites (Menezes, Frasson and Tasca 2016). In 2018, there were 6.9 million incident Trichomonas infections in the United States, with just over half (3.5 million) diagnosed in women (Kreisel et al. 2021). Women who inject substances, who douche, or who have more than two sexual partners are at increased risk for trichomoniasis (Bennett et al. 2010). Note that woman can also transmit the disease to their female sexual partners (Gorgos and Marrazzo 2011). Men are affected in relatively equal numbers to women but are often less likely to be screened for the disease (Leitsch 2016). Rates are disproportionate by race/ethnicity, with Black Americans experiencing more than ten times the case rates of their White counterparts (Bennett et al. 2010). In 2016, the WHO estimated the global trichomoniasis incidence rate at 40 cases per 1,000 women and 42 cases per 1,000 men, with the highest overall incidence rates in the WHO African Region (Rowley et al. 2019). The WHO (2016) case rate estimation indicated at least 156 million new Trichomonas vaginalis infections globally (Rowley et al. 2019). Global trichomoniasis prevalence was estimated at 5.3%—higher than the combined prevalence of gonorrhea, chlamydia, and syphilis. As lifetime medical costs are approximately $5–36 per case of trichomoniasis (costs to female patients are higher than to males) (Kumar et al. 2021), the overall incident cases amount to a minimum range of $34.5 million to $248 million in America and $780 million to US$5 billion globally. Note that all of the aforementioned estimates are limited in scope, likely underestimations, as trichomoniasis is not a notifiable/reportable condition and remains difficult to diagnose (Petrin et al. 1998; Menezes, Frasson and Tasca 2016).
How the STI Attacks
After introduction into the reproductive tract, T. vaginalis phagocytoses epithelial cells, erythrocytes, leukocytes, viruses, and bacteria (which may well be why great reductions in Lactobacillus species are noted in the affected vagina); its surface proteins adhere to the surface epithelium, lysing cells and creating microulcerations (Leitsch 2016). This process is upregulated in the presence of iron (Petrin et al. 1998). The parasite transitions to an amoeboid form (Leitsch 2016) and may be able to avoid some of the host’s immune response by surviving beneath the epithelial cell layer. Researchers are confident that T. vaginalis activates the alternative complement pathway; this, in addition to phenotype switching, appears to be a major method by which the parasite evades the host immune response (Petrin et al. 1998). Overall, a proinflammatory state ensues and can be worsened by the presence of pathogenic bacteria such as Mycoplasma hominis (Leitsch 2016). Persistence and reinfection are common, especially among women with HIV (Bennett et al. 2010), mirroring the clinical experience with BV—and reinforcing the notion that optimal cervicovaginal microbiota has been thoroughly disrupted.
Acute and Chronic Damage by the STI
While most patients note no symptoms, trichomoniasis may present acutely with malodorous discharge, vaginitis, cervicitis (presenting clinically as colpitis macularis, the “strawberry cervix”), endometritis, salpingitis, adnexitis, balanoposthitis, nongonococcal urethritis, epididymitis, or prostatitis (Bennett et al. 2010; Menezes, Frasson and Tasca 2016). This STI increases the risk of acquiring other STIs, including HPV and HIV—in fact, the presence of T. vaginalis in women increases risk of HIV acquisition some 2- to 3-fold (Leitsch 2016). In men, the presence of the parasite is often self-limited and resolves within 10 days; in women, trichomoniasis may persist for years (Petrin et al. 1998; Leitsch 2016). Clinical worsening during menses is likely related to the increased presence of iron (Petrin et al. 1998). In pregnant women, trichomoniasis is associated with low birthweight, premature rupture of membranes, and preterm delivery (Bennett et al. 2010; Leitsch 2016). Though uncommon, neonates can develop respiratory infection by acquiring trichomoniasis during vaginal delivery (Bennett et al. 2010). Chronic damage associated with genital T. vaginalis infection includes infertility in both males and females, cervical cytologic changes, and cervical and prostate cancer (Petrin et al. 1998; Leitsch 2016; Menezes, Frasson and Tasca 2016). Overall, this is a potentially dangerous disease too often overlooked or minimized (Petrin et al. 1998).
Prevention of the STI
Avoiding sexual contact with multiple partners decreases the likelihood of acquiring Trichomonas vaginalis, as does condom use. It is important to note that vaginal douching does not decrease but increases the risk of the disease (Bennett et al. 2010). Medical male circumcision decreases female partner rates of trichomoniasis by ∼48% (Tobian and Gray 2011). Interest in vaccination against trichomoniasis remains, but the process has not been successful thus far (Bennett et al. 2010).
A Note on Justice and Charity
The issues canvassed in this paper raise a serious question about justice. In contemporary bioethical discourse, the concepts of autonomy and social justice seem to take center stage. Both ideas have their place, but the notion of justice relevant here is slightly different.
To get us thinking about the relevant notion of justice, consider how interdependent we are on another's work. You didn’t make your own house. You didn’t grow your own food, or raise such animals and care for them. You did not make your own car. You do not give yourself an education. You did not build the roads that you drive on, or the buildings that you work in. You had very little to say about the economic structure and market into which you entered for gainful employment. You do not take your own garbage or recycling away—and do so in a way that is most environmentally friendly. When you get sick, you don’t typically treat yourself—even if you are a doctor. So far, I have given examples of people whom we don’t even know who have contributed to the functioning of our lives. I haven’t even mentioned the role that one's parents and broader family play. We are individually almost completely dependent upon other people's work and practices for our own well-being.
All our work contributes collectively to the being of society. Just as you and I have being in the sense that we are living human beings with a human nature, society also has being. And just as the human being can be healthy or ill, society's being can be healthy or ill. Justice is the moral virtue in each of us that contributes to the healthy functioning of society.
St. Thomas Aquinas provides a definition of justice that is as succinct as it is informative. He states that “justice is a habit whereby a man renders to each one his due by a constant and perpetual will.” Since Aquinas here is defining a virtue, it must be a stable source of one's actions. That is why justice is defined as a habit. It “renders each one his due” in the sense that justice perfects our relations with others. In this regard, it is important to point out that justice is one of the four cardinal virtues. The term “cardinal” is derived from the Latin term that meant doorpost (Rhonheimer 2011). The four cardinal virtues are those on which other virtues hinge. And it is important to point out that the four cardinal virtues are logically exhaustive. Courage is the habit of acting in accordance with reason when the passions of a person recoil from acting, but reason says that one ought to act. Temperance is the habit of acting in accordance with reason when the passions of a person desire to act, but reason says that one should recoil from acting. Prudence is the habit of picking out appropriate means to the ends of the other virtues. (So, if courage says that one ought to speak up when one's employment position is vulnerable, prudence dictates the means by which one can voice one's moral concerns while minimizing possible fallout). Courage, temperance, and prudence perfect the person. Justice is the habit of acting in accordance with reason in one's intercourse with others. (Of course, Aquinas admits that we can speak, albeit metaphorically, of one and the same man being just, “in so far as the reason commands the irascible and the concupiscible [passions], and these obey reason…” (Summa Theologica II-II. Q 58, a. 2.)).
The virtues are understood to perfect certain powers of the human person. Prudence, for example, perfects the intellect. Justice perfects the will. But it perfects the will in making it will in accordance with reason. Reason is understood to be an objective feature of moral reality. Reason, for Aquinas, can sometimes refer to a specific faculty of the human person. But typically, he reserves the term intelligere (intellect) to refer to the faculty of the mind. The term ratio (reason), especially when he is discussing the virtues, means order, proportion, or fittingness. Aquinas even suggests that the rectitude of the will in accordance with reason can also go by the name of truth (ST II-II, Q 58, a. 5). Elsewhere, Aquinas defines truth as “an adequation” (adequatio) between mind and world. Adequatio means due proportion and fittingness. This excursion into etymology has a point: justice should be visualized as acting in a way that fits the circumstances; it is adequate to producing society's flourishing.
Justice, then, involves habitually acting towards others in a way that is fitting or commensurate with the common good. The common good has a long-standing meaning within Catholic moral theology, but it might be helpful to translate it into the language of society having a being. Just as human beings can flourish when they actualize their distinctive human potencies (Napier and Travaline 2024), so too society flourishes insofar as it has being. To put the point more concretely, justice involves acting towards others in a way that conduces to our collective flourishing.
We can now see the problem that has been canvassed in this paper: acting in a way that involves a serious compromise to one's own health and to others, an immediate sequela of which is the enormous health care expense, is an unjust action. These are not cases in which someone is just exercising one's autonomy, the immediate consequences of which are borne only by those who engage in promiscuous sexual activity. Rather, these are actions with a wider net of effects, and these effects compromise the health of society.
We should note that engaging in promiscuous sexual activity is commensurate with autonomy understood in one sense, but understood in another, it is an enslavement. Any notion of autonomy worth the moral value we place in it should be understood as acting in accordance with reason. Actions that clearly compromise one's own health and those of others are discordant with reason. To justify such actions as the satisfaction of one's sexual desires simply recapitulates the claim that one's will is enslaved by one's sexual desires. It is hard to say that sexual desires are bad. They are quite good when they are ordered towards binding oneself to another in a way that perfects one's love for that person and ensures a stable and loving community within which to welcome new human life. Since justice implies a relation, the relevant relation here is between one's actions and the goods of the relevant community—in this case, the family. Acting on one's sexual desires in a way that's respectful of those values is acting in accordance with reason. If one does not desire a family, one should not engage in actions that create one. Doing so is contrary to reason.
The general point is that having a will that is rectified, that is, ordered to reason, implies a relationship between the agent's action and some other end. That end in the case of justice is the flourishing of the society, or the relevant community. Actions that involve grave financial consequences to health care infrastructure and create a culture in which human beings’ sexuality is objectified—human persons are seen as a means to satisfy one's sexual desires—frustrate the being of society. Such actions are unjust; they fail to give “each one his due.” Vis-à-vis the frustration of society's being, ubiquitous, promiscuous sexual activity is unjust for the same reasons that, for example, garbage collectors collectively not showing up to work simply because they don’t want to, is unjust; or that medical professionals not showing up to work just because they don’t want to is unjust. One can see with these examples that autonomy is not much of a value when the practices are seen to immediately affect the good of society. But how one treats others, particularly in the sexual dimension, is important vis-à-vis the good of society.
This last point invites a brief reflection on the virtue of charity. The virtue of charity is a settled habit of acting for another's good or fulfillment. When a person loves another, the lover wills the good and fruition of the beloved. So, we may ask whether promiscuous sexual behavior in fact wills the good of one's “partner”? Two reflections are sufficient to answer “clearly not.”
Psychiatrist Paul McHugh remarks on an exchange he had with a young woman who came to him for counseling with a chief complaint of depression and a lack of perceived self-worth. She complains, among other things, that she feels unattractive or unloved in her romantic relationships. Her experience recapitulates a similar pattern: she begins dating an attractive man who initially manifests interest in her. The relationship quickly becomes sexually intimate, and after several months, she begins to hope that they will marry. Invariably, the men recoil at making such a “serious commitment,” and she concludes that the men are not sufficiently interested in her. Repeat this pattern several times over and any woman will feel worthless and unlovable. But the problem, McCugh urges, is not in her. He comments that, “in expecting intimacy to lead to commitment, she is the one who is acting in a natural way; and her boyfriends are not” (McHugh 2004, 24).
Sexual intimacy should bind the partners to one another, but when sexual intercourse is used as a means to bind, and not an expression of the couple's bond, intercourse becomes a tool, a means, and possibly even a weapon. He continues, “[c]ontemporary sexual mores, supported by easy contraception [and abortion], tend to emphasize what one receives from an intimate relationship rather than what one brings to it - i.e. taking something from another rather than making something together…” (McHugh 2004, 24). McHugh observes that the young woman, and many others, unintentionally cooperate with a system that permits men to remain in “perpetual adolescence.” Such a system involves using others, not benefiting others.
A second reflection considers from the first-person perspective, the prospect of engaging in an enjoyable activity that is highly causally associated with disease and disability not just in oneself, but in one's child and others. Suppose, for a moment, you and your children were invited to a friend's house to have dinner. Suppose it was a magnificent dinner with a buffet of gustatory delights of your choosing. But you also know that by doing so you will give yourself neurologic disorders, chancres, sores, immune suppression, cancer, as well as expose your children to such disorders, and possibly even death. The alternative is to simply stay at home and politely decline. Would you decline? Viewed through the lens of charity, namely, love for yourself and your children, you should choose the alternative. The copious empirical evidence canvassed above suggests that our sexual choices face the same situation. The doyen of the sexual revolution, that is, promiscuity, is a recipe for harm, not love.
Conclusion
HIV, viral hepatitis, and STIs cause or contribute to the deaths of approximately 2.3 million people each year (WHO 2021). While HIV and syphilis are rightly recognized for their great human burden, many of these STIs are neglected despite the great economic, physical, and emotional burdens they perpetuate. We especially draw attention to the mounting evidence that disruption of the optimal cervicovaginal microbiota (or, one could argue, the natural state of the vaginal microbiome) is implicated in multiple STIs and may well be a shared pathophysiology driving some of the poor maternal and reproductive outcomes seen in these diseases. Disruption of a woman's optimal cervicovaginal microbiota occurs with a rising number of sexual partners, whether those partners are male or female. Women who have sex only with women are not a “no- or low-risk” group and should be screened for STIs the same way as women who have sex with men (Gorgos and Marrazzo 2011). Men who have sex with women are at risk for acute and chronic STI-induced damage, even if the men themselves note no symptoms; this damage can impact male fertility and cancer risk. Men who have anal sex with men constitute a high-risk group even when in monogamous relationships; here again, rising numbers of sexual partners compound the risk of acute and chronic STI-induced damage—and carry a great risk of HIV and syphilis co-infection among sexual networks. The tempering, moderating, or excluding of sexual practices (e.g., minimization of sexual partnering, avoidance of high-risk sexual behaviors, or abstinence/continence) drastically reduces the risk of acquiring and/or transmitting STIs, limiting the potential harms sustained by all individuals involved.
We hope that each diagnosis of a STI presents an opportunity to share—charitably—the reality of increasing STI rates nationally and worldwide, as well as to discuss prevention techniques. Patient-physician encounters with individuals who are participating in sexual activities of any kind are also opportunities for physicians to learn about sexual networks and experiences in the local community. Physicians should ensure that patients understand the risks involved with expanded sexual networks, including the risk that incomplete treatment of a partner network may result in repeated reinfection or new STI(s). Encourage patients to self-screen for gonorrhea and chlamydia, to undergo sexual health screening regularly (prior to pursuing new sex partners and after establishing new sexual contact), and to recognize the potential mental and emotional health effects of sexual entanglements.
Clinicians should discuss sources of emotional support with patients who use electronic/digital applications to establish or expand sexual networks, as—especially among MSM—increased online dating network use is associated with worsened depression, lower sleep quality, greater substance use, and lower measures of well-being and life satisfaction (Obarska et al. 2020). We encourage physicians to inform patients of these modern realities of online sexual partnership and the consequent STI risks, especially for incident HIV and syphilis infections. Often, patients at risk for STIs do not have the opportunity to discuss the role of chastity with their social networks or with their physicians in a truly informative, non-judgmental manner. We exhort physicians to acknowledge with their patients—especially patients of non-heterosexual sexuality—how difficult it can be to find positive emotional support and to develop healthy relationships without sexualization or objectification. In patients practicing continence and/or cultivating chastity, STIs themselves, as well as their attendant health risks, are considerably attenuated.
Footnotes
Acknowledgments
We would like to thank two anonymous reviewers for very helpful comments on previous drafts of this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.