
Abstract
Background
Reports in the medical literature indicate that there are patients who have initiated medical abortions by taking mifepristone but not misoprostol and have attempted to continue their pregnancies by taking exogenous progesterone.
Objective
We sought to evaluate the effectiveness and adverse events of exogenous progesterone taken after mifepristone.
Methods
This is a retrospective cohort of consecutive patients who contacted a nonprofit hotline from October 13, 2021 to January 5, 2024. The primary outcome was the rate of continuing pregnancy two weeks after progesterone initiation; secondary outcomes included demographics, progesterone dose and route of administration, and adverse events. A small subset was evaluated for a secondary outcome of gestational age at delivery. Data from a small subset were evaluated for preterm birth and birth defects. Adverse events at two weeks were analyzed. Patients were included if they wanted to attempt to continue their pregnancies after taking mifepristone for medical abortion. Exclusion criteria included never starting progesterone therapy, initiating progesterone more than 72 h after ingesting mifepristone, gestational age at the time of mifepristone ingestion greater than 11 weeks 6 days or undocumented, and surgical or additional medical termination of pregnancy.
Results
From 1,466 patients screened, 765 met the inclusion criterion and did not meet exclusion criteria; 418 (55%) had confirmed continuing pregnancies two weeks postinitiation of progesterone therapy. Earlier gestational age at mifepristone use was associated with a decreased likelihood of continuing pregnancy at two weeks (39% vs. 58%, p < .001). Significant bleeding was reported by 0.3% of the patients; 3% visited the emergency department; and hospitalizations occurred in 0.5% of the cases. There were no blood transfusions nor maternal mortalities.
Conclusions
Continuing pregnancy was noted in 55%, superior to the 25% rate documented in the literature for mifepristone alone without intervention. There were a few adverse events associated with progesterone use. These retrospective data suggest the potential benefit of exogenous progesterone administration for patients seeking to continue their pregnancies after taking mifepristone but not misoprostol. Further research, including randomized controlled trials, is needed
Keywords
Background
Medical abortion utilizing mifepristone has been available in the United States since 2000. In 2023, the Guttmacher Institute estimated that 63% of U.S. abortions were medical abortions, most of them utilizing mifepristone and misoprostol (Guttmacher Institute n.d.). Some women who start the medical abortion process change their minds and take exogenous progesterone in an effort to continue their pregnancies (Delgado et al. 2018).
Mifepristone is typically administered up to 70 days after the last menstrual period in a single 200 mg dose to detach the decidua from the trophoblast, effecting embryonic or fetal demise (Creinin and Gemzell Danielsson 2009; Johannisson et al. 1989; Schindler et al. 1985), followed 24–48 h later by a single dose of misoprostol 800 μg to stimulate myometrial contractions to expel the embryo and trophoblast (US FDA n.d.-b). Misoprostol is included in the protocol due to a 20% to 40% incomplete abortion rate with mifepristone alone, as determined by the endpoint of complete expulsion (Creinin and Gemzell Danielsson 2009).
Studies using rabbit and rat models found that mifepristone is antagonized by progesterone, allowing for normal pregnancy and delivery in a high percentage of cases (Camilleri and Sammut 2023; US FDA 2000; Yamabe, Katayama, and Mochizuki 1989). A randomized, placebo-controlled trial of progesterone after mifepristone was terminated early due to hemorrhage requiring transfusion or curettage in two patients who received mifepristone without progesterone (Creinin et al. 2020). In that study, four out of five women who received progesterone after mifepristone had continuing pregnancies, compared to two out of five who received mifepristone without progesterone. Though not statistically significant due to the sample size, this is consistent with observational studies that suggest progesterone after mifepristone is associated with a 48% to 68% likelihood of continuing pregnancy compared to mifepristone alone, which is estimated to be 25% (Garratt and Turner 2017; Delgado et al. 2018; Turner et al. 2023). In the randomized dataset, patients who received progesterone did not experience adverse effects more often than the placebo group (Creinin et al. 2020).
Progesterone after mifepristone for patients who desire continuing pregnancy despite initial mifepristone use has not been incorporated into general guidelines around medical abortion. We sought to add to the available data in order to better support and counsel women who request progesterone to continue pregnancy after taking mifepristone.
Methods
This was a retrospective cohort study of a de-identified dataset—which had never been previously analyzed—of consecutive cases of women who took mifepristone and subsequently took progesterone in an attempt to continue pregnancy, between October 13, 2021 and January 5, 2024. The study was deemed exempt from needing approval by the Franciscan University of Steubenville Institutional Review Board (IRB protocol number 2023-01, approval date January 24, 2023).
Data were originally collected prospectively by an informational and referral hotline operated by Abortion Pill Reversal Network, Columbus, OH, which obtained written consent within the clinical setting for treatment and ongoing data collection for future research, before connecting women with local prescribers for progesterone. Signed informed consent was obtained from subjects prior to the commencement of the study. Data were collected mostly from the patients via electronic or voice communication and from clinicians and their reports. All clinical evaluations were conducted by treating physicians and other treating clinicians. Progesterone doses, frequencies, route of administration, and duration were at the discretion of the treating prescribers.
Patients were included if they wanted to attempt to continue their pregnancies after taking mifepristone for medical abortion (the standard U.S. mifepristone dose is 200 mg; (Macnaughton, Nothnagle, and Early 2021; US FDA n.d.-a). Exclusion criteria included taking misoprostol, never starting progesterone therapy because they decided not to attempt to continue their pregnancies, initiating progesterone more than 72 h after ingesting mifepristone, gestational age at the time of mifepristone ingestion greater than 11 weeks 6 days or undocumented, and surgical or additional medical termination of pregnancy after hotline contact.
The primary outcome was continuing pregnancy two weeks after initiation of progesterone therapy, as determined by sonographic or Doppler detection of embryonic or fetal cardiac activity. This endpoint matches the primary outcome in the randomized trial on this intervention (Creinin et al. 2020) and the last follow-up in studies of medical abortion (Peyron et al. 1993; Spitz et al. 1998) and is reasonable since pregnancy loss after two weeks of progesterone is not likely attributable to mifepristone (Bernard et al. 2013). Additionally, the half-life of mifepristone (18–32 h; DrugBank 2005; Sarkar 2002) supports the choice of a two-week endpoint.
Variables examined included demographics, progesterone route and dose, interval between mifepristone ingestion and first progesterone dose, gestational age at the time of mifepristone ingestion, and the incidence of adverse events, which were included in the dataset, which were vaginal bleeding, emergency department (ED) visits, hospitalizations, transfusions, antibiotic use, and maternal mortality. A small subset of the subjects in the database had information regarding birth defects and preterm birth (delivery prior to 37 weeks of gestation) reported.
Statistical Analysis
Continuing pregnancy rates were analyzed using one-sample proportion and two-sample proportion tests between treatment and historic control groups, with subgroup comparisons based on gestational age. Categorical variables were analyzed using the Pearson's chi-squared test and Fisher's exact test, while continuous variables were compared using the Wilcoxon rank-sum test. Logistic regression was employed to examine associations between the primary outcome and significantly associated demographics and clinical factors. Unadjusted odds ratios (OR) with 95% confidence intervals (CIs) were calculated. All statistical analyses were performed using R, version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria), and a p value <.05 was considered statistically significant. This report was prepared in accordance with the STROBE statement for cohort studies (Cuschieri 2019).
Results
The initial database consisted of 1,466 women who stated to the hotline that they had taken mifepristone or other abortifacient drugs and sought to continue their pregnancies. Of these, 1,436 met the inclusion criterion (thirty had not actually taken mifepristone); 533 were excluded for not starting progesterone therapy because they chose not to attempt continue their pregnancies; three were excluded for starting progesterone more than 72 h after taking mifepristone; 112 were excluded for gestational age unknown or greater than 12 weeks at the time of mifepristone ingestion; 20 were excluded for subsequently taking misoprostol to reinitiate the abortion process, and three were excluded for completion of abortion via a surgical approach, leaving 765 cases remaining. Of the 765, 670 took mifepristone 200 mg; one took 600 mg, and 94 had an unknown dose strength, likely 200 mg. After confirmation of the primary outcome at two weeks, 105 women had data on delivery outcomes available. There were no birth defects, and there were 8 deliveries prior to 37 weeks of gestation (7.6%) (see Figure 1).
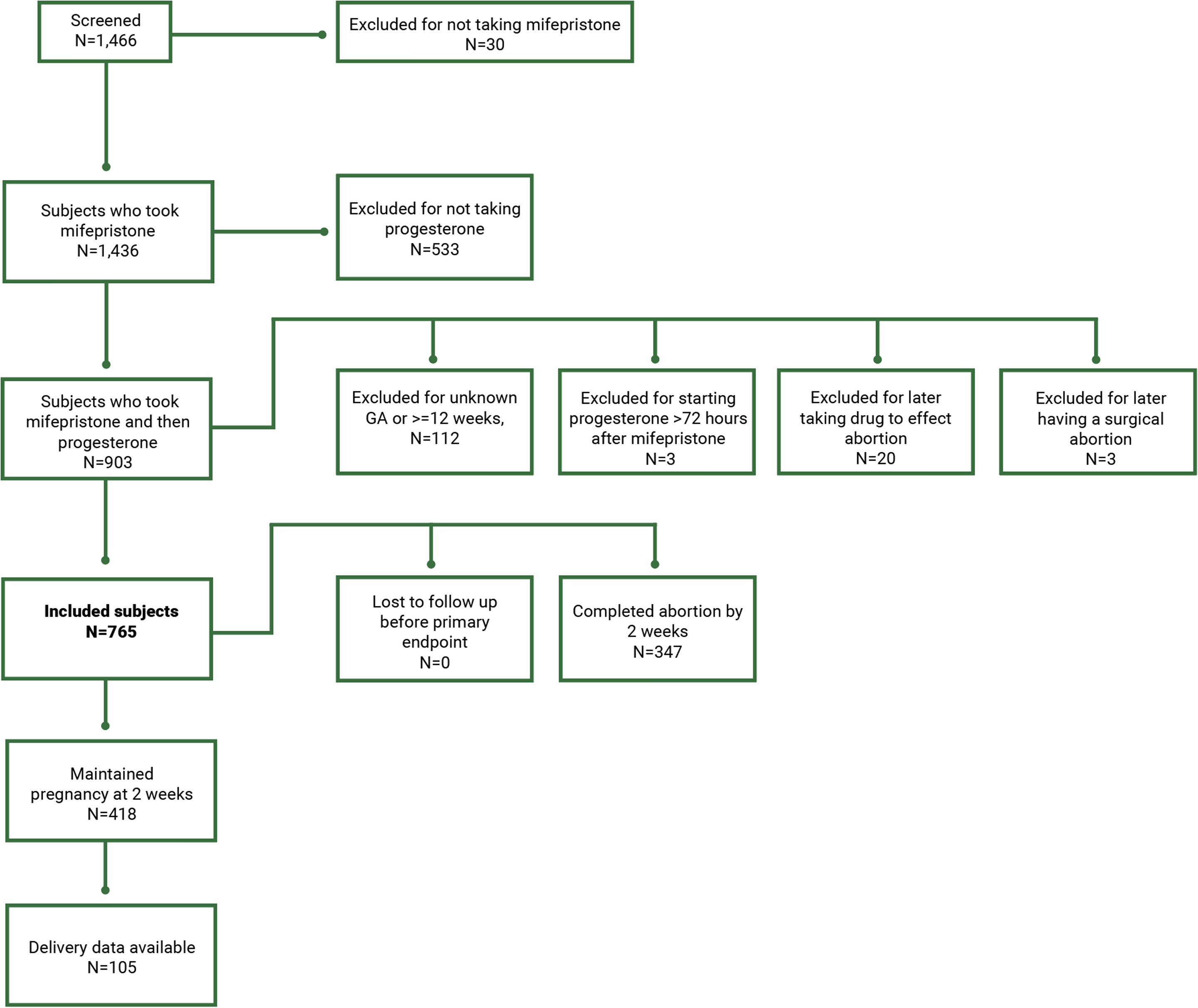
Flow Chart of Potential Participants Screened.
Demographic information is provided in Table 1. Racial and ethnic groups were diverse, with 30% of the participants being white, 29% Black, 31% Hispanic, and 11% other. Most participants were covered by health insurance (84.5%), with 82.4% in the completed abortion group versus 86.2% in the continuing pregnancy group (p = .2). The majority of the study participants (92.3%) were from the United States, with the remaining 7.7% from other countries.
Demographics of 765 Women.
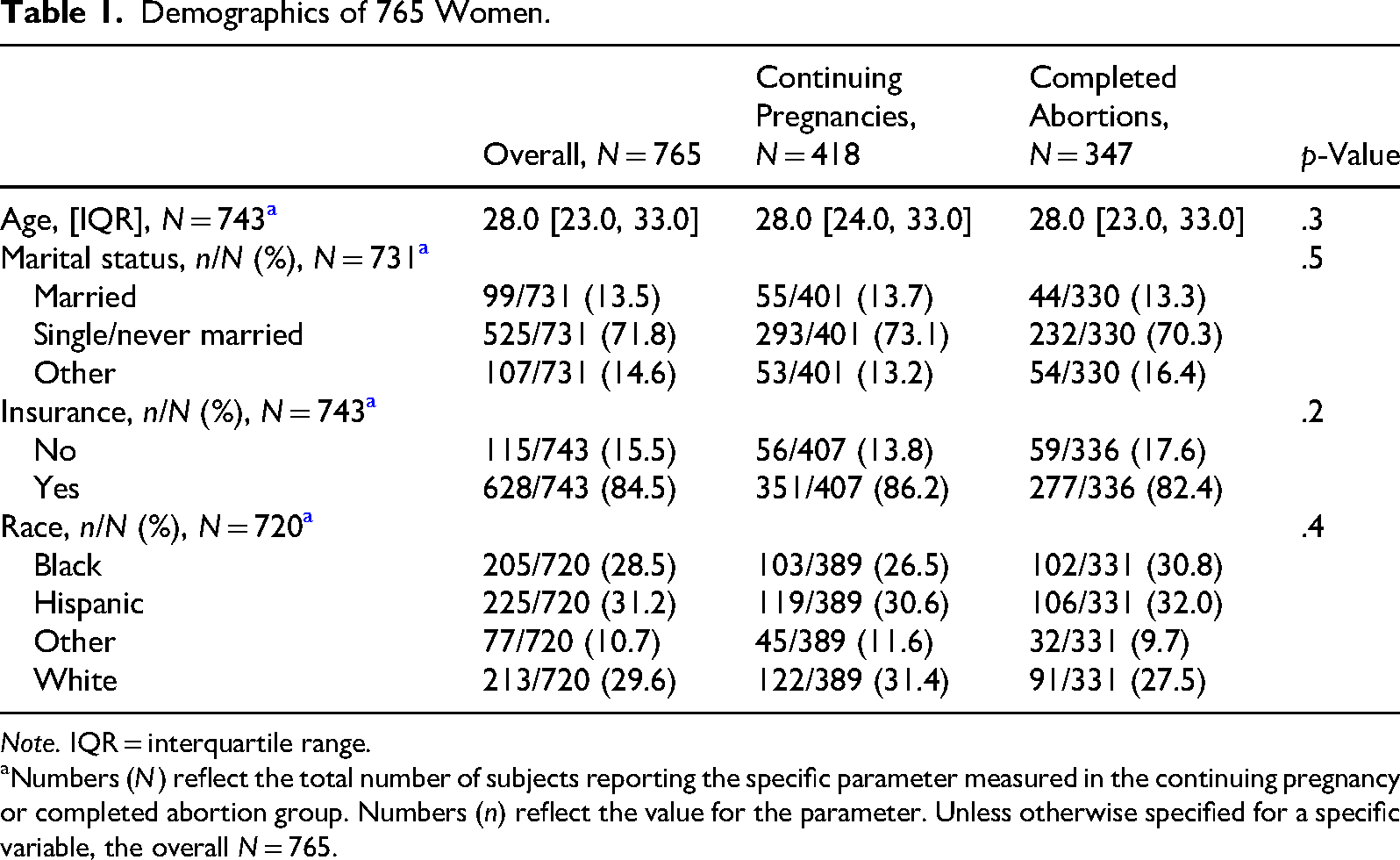
Note. IQR = interquartile range.
Numbers (N) reflect the total number of subjects reporting the specific parameter measured in the continuing pregnancy or completed abortion group. Numbers (n) reflect the value for the parameter. Unless otherwise specified for a specific variable, the overall N = 765.
Continuing pregnancy two weeks or longer after initiation of progesterone therapy was found in 418/765 (54.6%) (see Table 2). The continuing pregnancy rate for gestational ages over 6 weeks (366/632, 57.9%) was significantly higher (p < .001) than for gestational ages of 6 weeks or lower (52/133, 39.1%) (see Table 3). The primary outcome was not significantly associated with treatment dose, interval between mifepristone ingestion and first progesterone dose, maternal age, or route of administration; however, a higher gestational age was significantly associated with the outcome (OR 1.21, 95% CI 1.11–1.30) (see Table 2).
Variables Associated With Progesterone Use After Mifepristone in 765 Women.
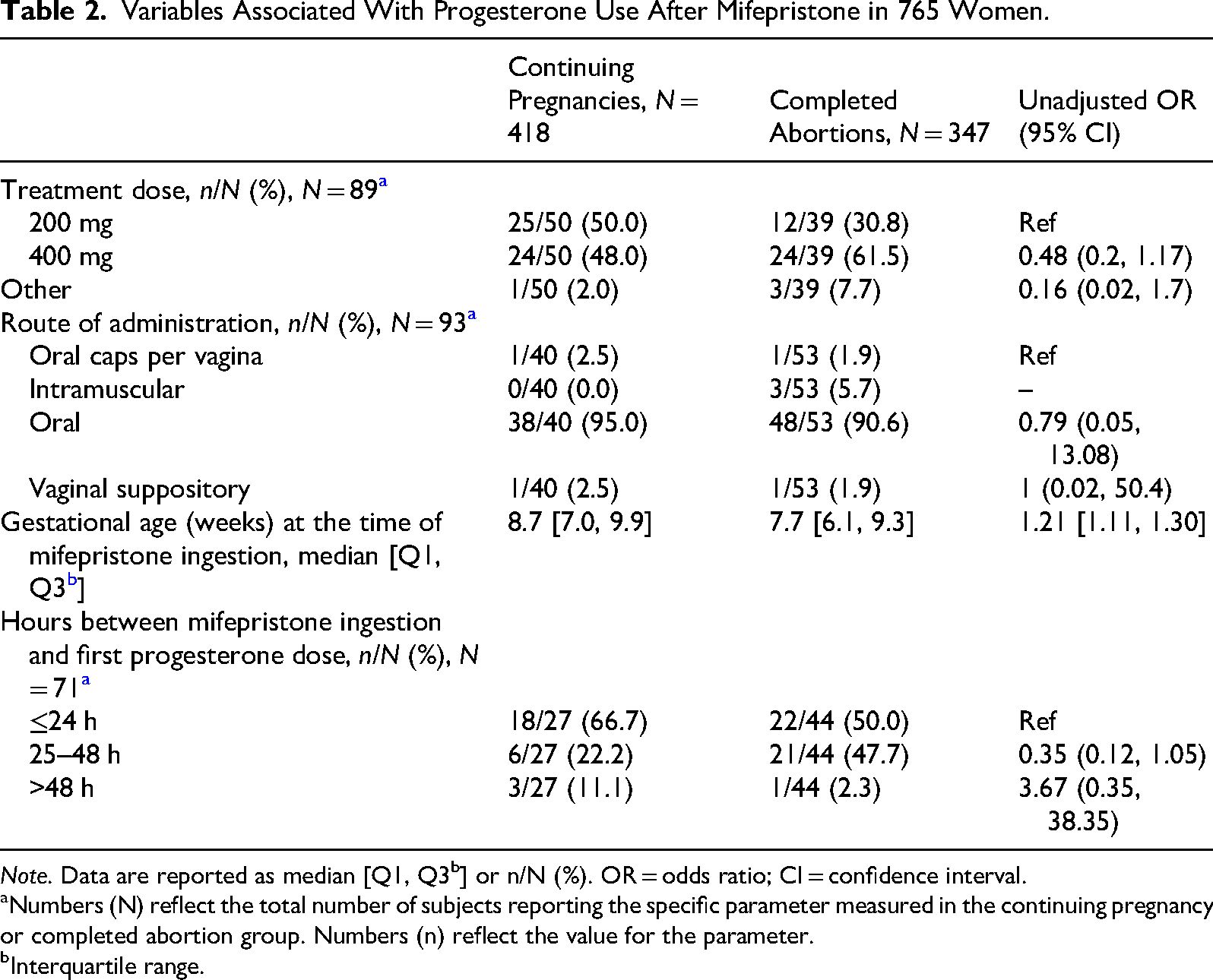
Note. Data are reported as median [Q1, Q3b] or n/N (%). OR = odds ratio; CI = confidence interval.
Numbers (N) reflect the total number of subjects reporting the specific parameter measured in the continuing pregnancy or completed abortion group. Numbers (n) reflect the value for the parameter.
Interquartile range.
Continuing Pregnancies by Weeks of Gestation in 765 Women.
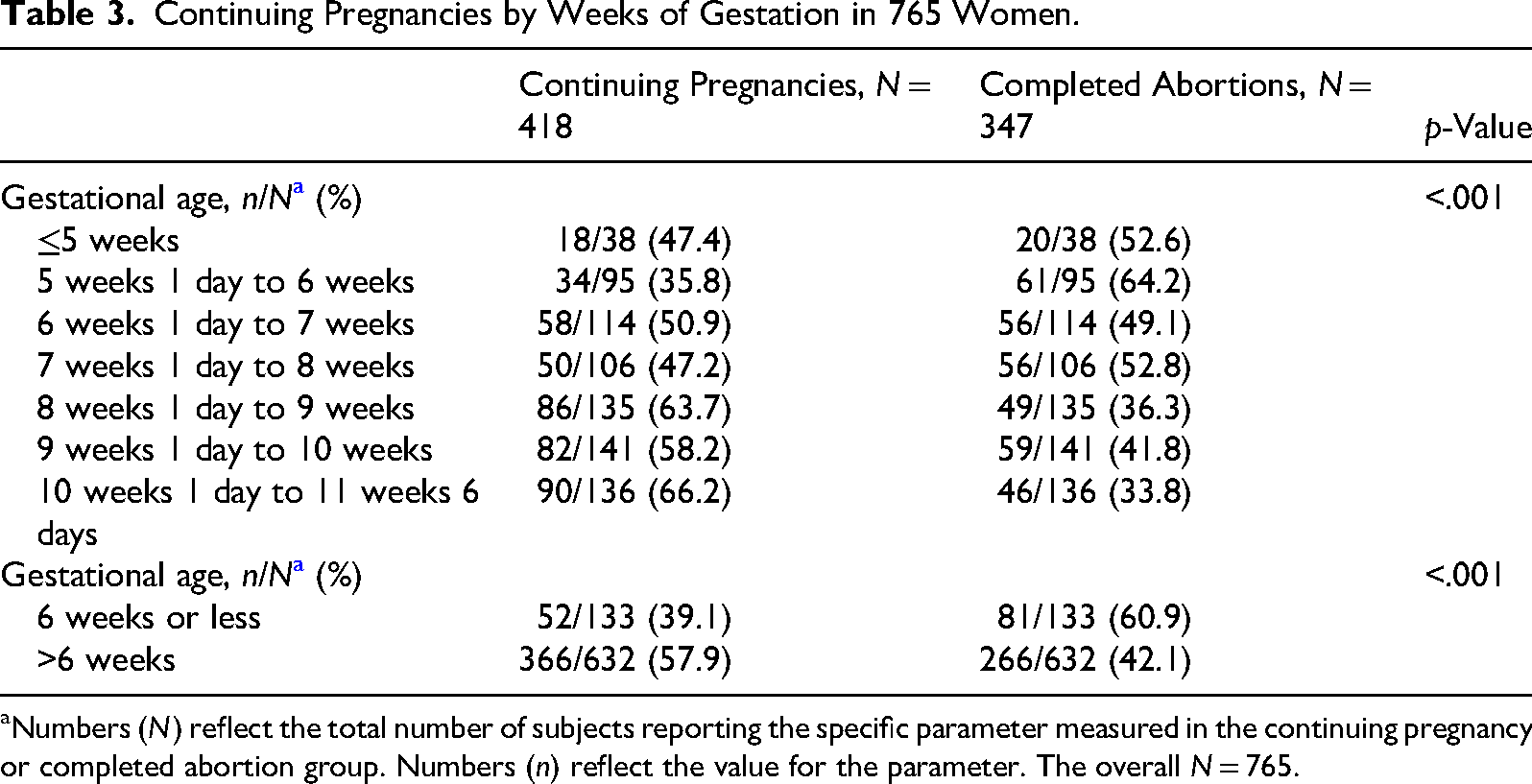
Numbers (N) reflect the total number of subjects reporting the specific parameter measured in the continuing pregnancy or completed abortion group. Numbers (n) reflect the value for the parameter. The overall N = 765.
Table 4 presents adverse events at two weeks post-initiation of progesterone therapy. Overall, 36/756 (4.8%) patients experienced at least one complication, with a significantly higher prevalence in the completed abortion group (25/342, 7.3%) compared to the continuing pregnancy group (11/414, 2.7%, p = .003). Bleeding more than a normal period was not different between the two groups, 2/756 (0.3%) overall. ED visits occurred in 21/765 (2.7%) cases, with a higher incidence in the completed abortions (15/347, 4.3%) compared to continuing pregnancies (6/418, 1.4%, p = .015). Hospitalizations were rare, occurring in only 0.5% of cases, 4/347 (1.2%) in completed abortions, compared to 0/418 in continuing pregnancies (p = .042). There were no cases requiring antibiotic treatment nor transfusion of blood products, and there was no maternal mortality.
Complications at Two Weeks Associated With Initiation of Progesterone After Mifepristone Use in 765 Women.
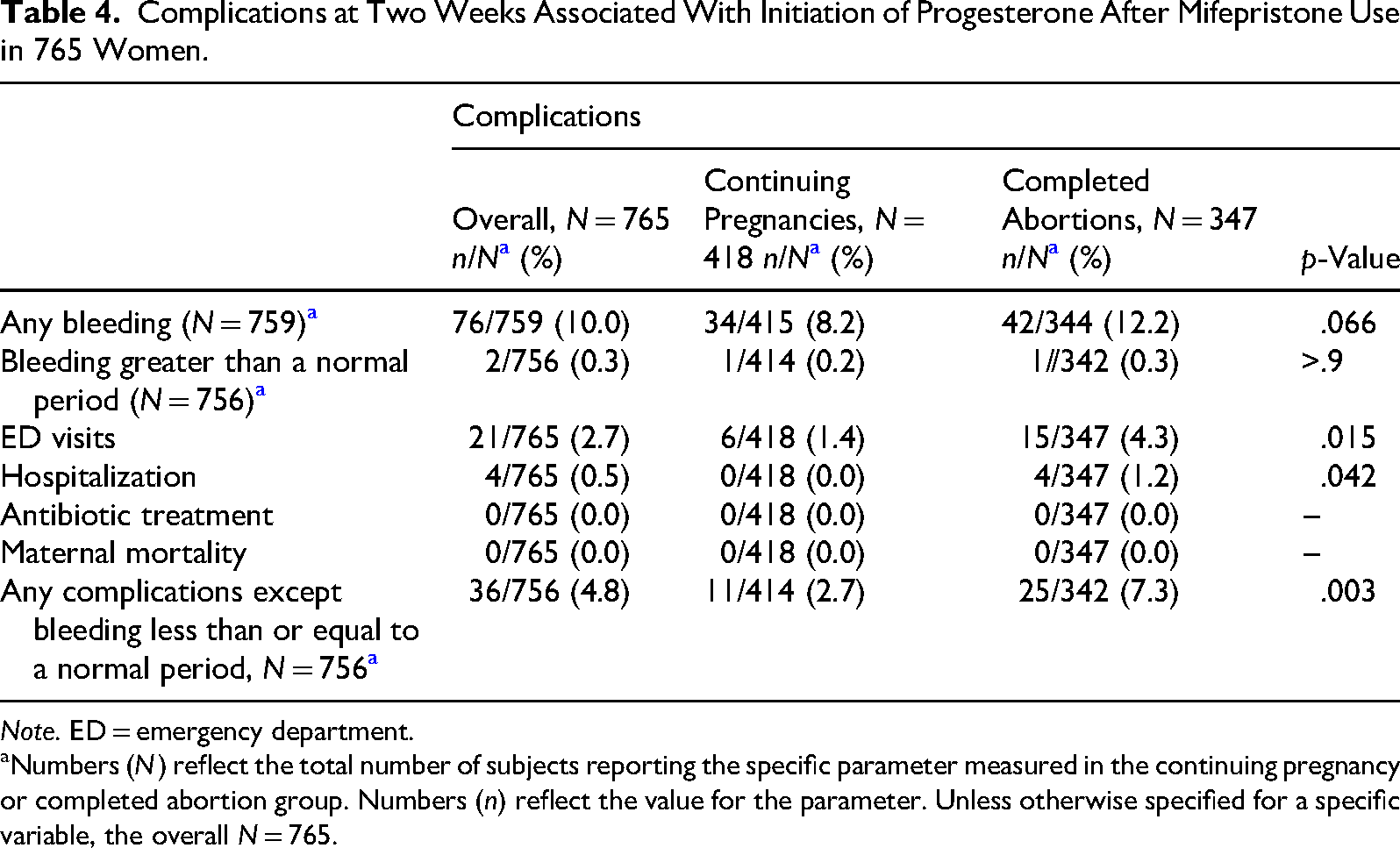
Note. ED = emergency department.
Numbers (N) reflect the total number of subjects reporting the specific parameter measured in the continuing pregnancy or completed abortion group. Numbers (n) reflect the value for the parameter. Unless otherwise specified for a specific variable, the overall N = 765.
Data regarding birth defects and preterm delivery were available for 105/418 participants who met the primary endpoint (25.1%). There were no birth defects, and there were only eight deliveries prior to 37 weeks of gestation (7.6%).
Discussion
Principal Findings
Women who took progesterone after mifepristone in an attempt to maintain pregnancy achieved their desired outcome in 55% of the cases, with greater success (58%) over 6 weeks of gestational age. Cases that achieved continuing pregnancy and cases that did not were similar in demographics in a racially diverse cohort. There were no cases requiring antibiotics or transfusions, and there were no maternal deaths. Higher gestational age was related to higher continuing pregnancy rates.
Results in the Context of What is Known
Overall, the continuing pregnancy rate was 55%, which is significantly higher (p < .001) than the historic rate of continuing pregnancy after mifepristone without progesterone of <25% (Delgado and Davenport 2012; Davenport et al. 2017). The odds of continuing pregnancy increased with increasing gestational age in these data, which fits with the diminishing effectiveness of mifepristone with advancing gestational age (Spitz et al. 1998). There were no birth defects in progesterone recipients followed to birth, compared to the rate in the U.S. general population of about 3% (CDC 2009). This is consistent with the literature documenting that mifepristone has no teratogenic potential (Committee on Practice Bulletins—Gynecology and the Society of Family Planning 2020; Creinin and Gemzell Danielsson 2009; Dante, Vaccaro, and Facchinetti 2013; Delgado et al. 2018) and that progesterone has no long-term risks when used in pregnancy (Practice Committee of the American Society for Reproductive Medicine 2008). Additionally, the preterm delivery rate was 7.6%, lower than the U.S. general population rate of 10% (CDC 2024). Further, there was no increased risk of adverse events in patients receiving progesterone, consistent with a previously published randomized controlled trial of patients receiving progesterone or placebo after mifepristone (Creinin et al. 2020).
Clinical Implications
A change of mind after starting the medical abortion process is not rare (Rafferty and Longbons 2023). In 2021, a study evaluating 19 years of mifepristone adverse event reports’ data by Aultman et al. revealed that 102 of 452 patients (22.6%) with ongoing pregnancy after taking mifepristone regimens changed their minds and continued their pregnancies (Aultman et al. 2021). Moreover, a study in the United Kingdom found that 10% of women whose pregnancies had continued, despite taking both mifepristone and misoprostol, chose to maintain their pregnancies (Hsia et al. 2019). The data presented in this study suggest that progesterone, given after informed consent about the risks and alternatives, may be effective in supporting the choice of women who desire to attempt to continue their pregnancies after taking mifepristone.
The rate of adverse events was higher in the completed abortion group (7%) than in the continuing pregnancy group (3%). This was primarily due to more ED visits (4% vs. 1%) in the completed abortion group.
Research Implications
Mifepristone is a competitive antagonist of progesterone at the progesterone receptor (PR). It binds to the PR about twice as avidly as progesterone (Heikinheimo, Kekkonen, and Lähteenmäki 2003). The half-life of mifepristone is approximately 18–32 h (DrugBank 2005; Sarkar 2002), while that of progesterone is 25–50 h (DrugBank 2025). Mifepristone and its metabolites can be measured up to 72 h after an ingested dose (DrugBank 2005). The U.S. Food and Drug Administration has given progesterone a category B rating in pregnancy, in contrast to synthetic progestins (US FDA n.d.-c). Further research is required to determine the most acceptable route and dose of progesterone, given the pharmacology of mifepristone and progesterone, and to collect adequate ongoing safety outcomes for this treatment. Researchers may also want to explore if higher progesterone doses might be indicated at lower gestational ages.
Strengths and Limitations
To our knowledge, this is the largest cohort in the literature examining the effects of progesterone supplementation after exposure to mifepristone but not misoprostol. Strengths of this study include continuous case collection by an organization that has been the first point of contact for most cases of progesterone therapy after mifepristone for the past seven years, complete reporting for the primary endpoint, continuing pregnancy at two weeks postinitiation of progesterone therapy, and very high report rates for adverse events at two weeks. Limitations include this study's retrospective design, heterogeneity in the practice of individual clinicians prescribing progesterone, and the lack of documentation of ultrasound confirming viable pregnancy prior to progesterone use (95% of cases), which could lead to an underestimation of progesterone efficacy. Despite complete data for the primary outcome at two weeks, 313/418 (75%) patients were lost to follow-up for delivery outcomes.
This study is not a placebo-controlled randomized trial, as it would be difficult to recruit patients seeking to continue their pregnancies to a placebo or expectant management group when data are publicly available about the possible advantage of progesterone.
Although not a limitation of the present study itself, the comparison of our data to the historic control is limited by the fact that only 44 patients in the systematic review that established the control had gestational ages up to 70 days (Davenport et al. 2017). The current sample had 136 patients with a gestational age greater than 70 days.
Conclusion
In this large cohort, 55% of women who took progesterone after mifepristone because they desired to continue pregnancy had an ongoing pregnancy after two weeks, which is more than double the historic control (Davenport et al. 2017). Adverse effects were of low frequency and severity in this study. Clinicians may encounter patients who would like to continue pregnancy after ingesting mifepristone, and these data may be useful in counseling them. Future trials would be useful to ensure safety and optimal dosing.
Footnotes
Abbreviations
Ethical Considerations and Consent to Participate
The study was approved by the Franciscan University of Steubenville Institutional Review Board (IRB protocol number 2023-01, approval date January 24, 2023). Signed consent was obtained to collect data for research.
Author Contributions
BC was the principal investigator. BC, SS, and GD designed the study. BC and GD wrote and edited the manuscript. SS and CJW analyzed the data and wrote the Methods and Results sections. SS provided edits of the manuscript. AJ researched citations. AJ, KG, SS, and CJW reviewed the design and manuscript drafts. All authors read and approved the final draft of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GD is an unpaid medical advisor to the Abortion Pill Reversal (APR) Network and originally founded the network. GD and KG may have treated some of the participants in the study. KG was previously a hotline nurse. The remaining authors have nothing to disclose.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.