
Abstract
Tracheo-innominate fistula is a rare but recognised life-threatening complication most commonly associated with prolonged endotracheal intubation. We report the case of a 16-year-old boy who developed a tracheo-innominate fistula secondary to the prolonged intubation after a pool accident. After 16 days of hospitalisation, the patient died as a consequence of a massive haemorrhage into the tracheobronchial tree and asphyxia. This is a rare complication, and to our knowledge, no case of tracheo-innominate fistula or any other case series concerning this rare complication has been reported in Serbia recently. This case report addresses the epidemiology of a trachea-innominate fistulisation as a complication of prolonged tracheal intubation, with a special overview of its forensic importance as an iatrogenic injury.
Introduction
By definition, tracheoarterial fistula represents an abnormal communication between the tracheobronchial tree and anatomically close blood vessels – the innominate or carotid artery. 1 Its incidence is <1%, and it most commonly occurs as a result of prolonged mechanical ventilation. 2 Although endotracheal intubation is a commonly used procedure required to set up an airway in critically ill patients that request artificial mechanical ventilation for a long period, it can sometimes be accompanied by complications, of which tracheoarterial fistulisation is a rare but recognised one. 1 Regarding pathogenetic mechanisms, currently, the most frequently seen is chronic trauma due to prolonged tracheal intubation. The final outcomes can sometimes be very serious, with a possible fatal evolution. 2
On the other hand, when the previously described complication is attributed to an iatrogenic injury, from the perspective of forensic pathology, deaths related to medical therapy present several challenges, especially if we consider the fact that one of the aims of the medical profession is to be able to detect complications in patients during diagnostic tests and treatments.3–6 With the aforementioned facts in mind which refer to the iatrogenesis on one hand and the most common mechanism of tracheoarterial fistulisation on the other, we herein represent a case of tracheoinnominate artery fistula (TIF) formed as an iatrogenic injury, which was diagnosed at autopsy.
Case report
Clinical summary
After a pool accident, a 16-year-old boy was brought unconscious to the hospital. He was intubated but was unable to be weaned off the ventilator. Excessive oropharyngeal haemorrhage occurred 16 days later during a routine bedding procedure. Colloids, intravenous fluids and unmatched blood were given in an effort to resuscitate the patient, but he died within 45 minutes. The otorhinolaryngologist could not identify the source of bleeding.
Pathological findings
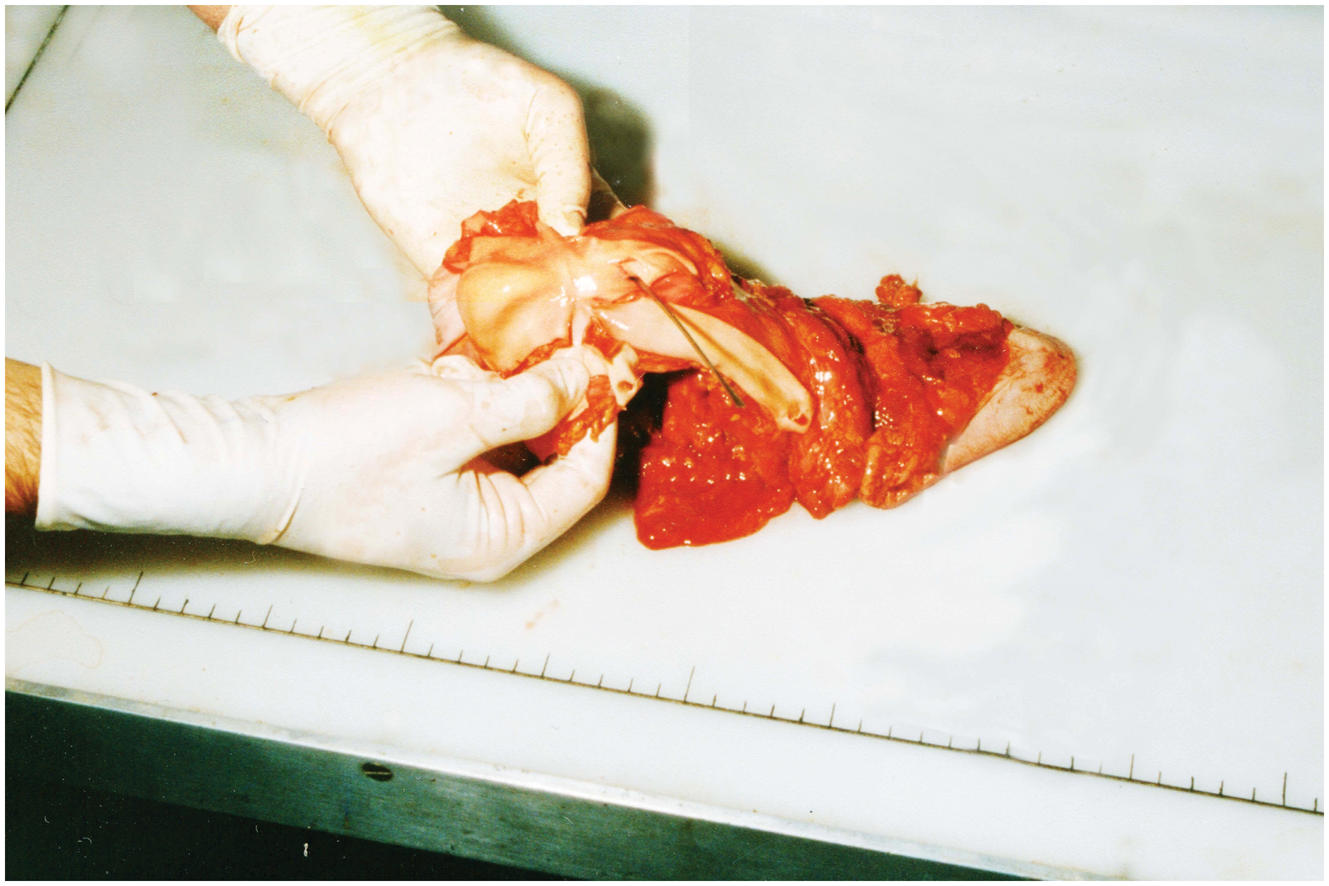
The autopsy revealed a lesion on the anterior wall of the trachea, 15 mm × 10 mm in diameter, whose central part communicated with the lumen of the innominate artery (Figures 1 and 2). Approximately 300 mL of blood in the stomach was observed, along with autopsy evidence of blood in the lungs and in the airways. Therefore, the post-mortem diagnosis of the patient was excessive loss of blood and blood aspiration caused by TIF.
Tracheo-innominate fistula: a lesion on the anterior wall of the trachea whose central part communicate with the lumen of the innominate artery. Tracheo-innominate fistula: a communication between the lesion on the anterior wall of the trachea and lumen of the innominate artery.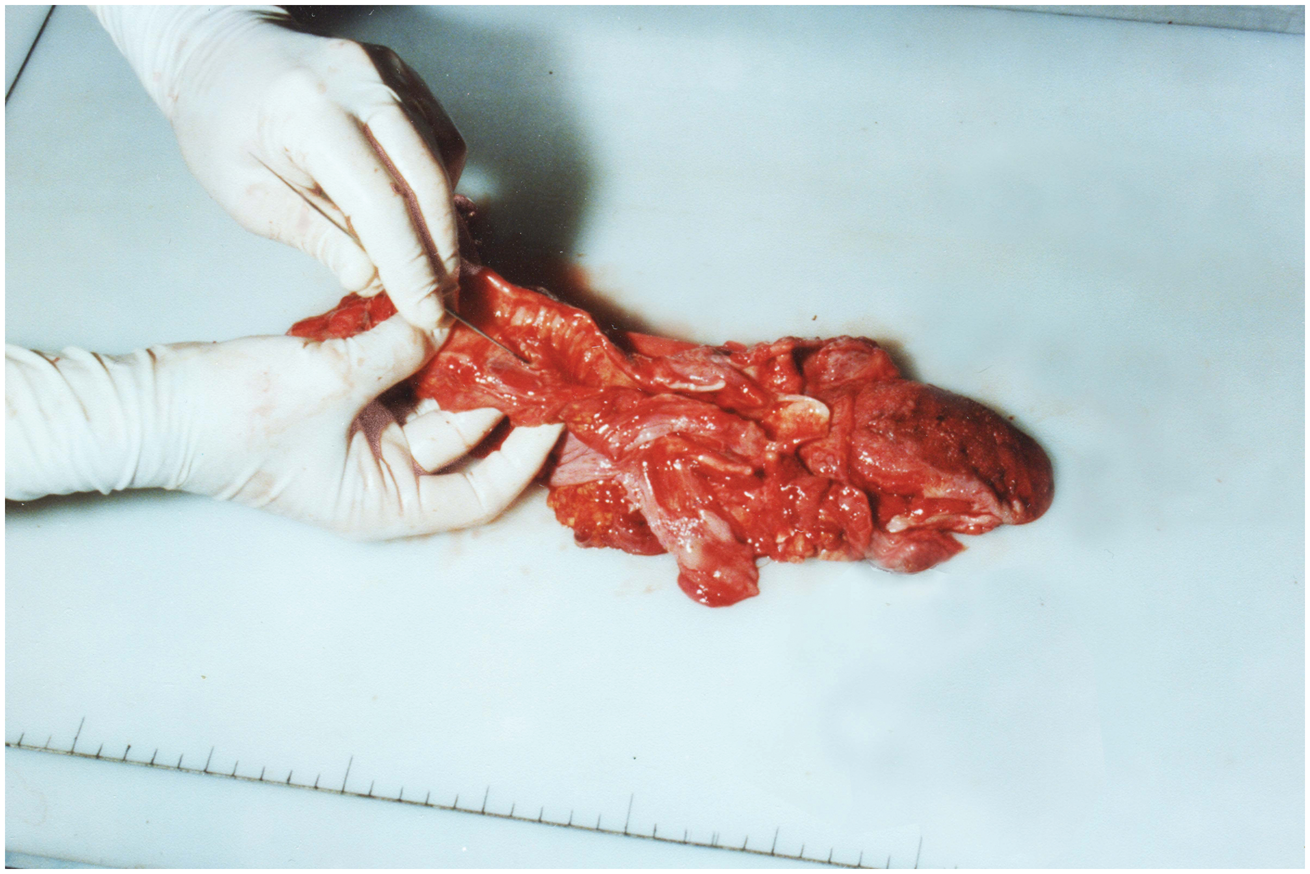
Discussion
Brachiocephalic artery haemorrhage is a life-threatening complication that most probably occurs because of prolonged mechanical ventilation. 7 The possible mechanisms described are high cuff pressure, inappropriate cuff size, and some neurological disorders followed by atypical head and neck positions of the patient, but the most common are pressure ulcerations from local inflammation. 8
The previously mentioned facts are even more important considering that warning symptoms, such as aspiration of blood or bleeding beside the tracheal cuff, can be absent. Usually, in cases where contact between the tissue and the cuff is tight, the first signs of bleeding can be misleading, and they most probably occur as a nasooropharyngeal haemorrhage. 7
According to the literature data, there are two types of TIF that occur from prolonged tracheal intubation. The first one, usually localised immediately beneath the curve of the ventilation tube, occurs as a consequence of artery erosion, and the second one is caused by the erosion either of the cuff or the tip of the ventilation tube. 2 Our study describes the second type of TIF – the anterior tracheal wall lesion, whose central part communicates with the lumen of the innominate artery and forms the fistula.
The retrospective study of Scalise et al., which included 544 patients in a long-term care facility, showed that TIF was diagnosed in 0.7% of the cases, and that there is no difference in the incidence when it comes to long- and short-term tracheostomy tubes. 1 Profuse bleeding following the rupture of the fistula frequently occurs in the first several weeks after the intervention. It is well-known that when it comes to TIF presenting as a massive haemorrhage, the only life-saving procedure is immediate arterial compression by over-inflation of the cuff, followed by the control of the airway and subsequent surgical treatment of the injured blood vessel. Despite fast initial treatment involving immediate control of profuse haemorrhage, this event is fatal in about 75–80% of patients. 9
On the other hand, from the perspective of forensic pathology, fatal iatrogenic injuries such as the one presented here represent a special forensic and medicolegal problem, especially in cases when they involve people whose injury was caused as part of a criminal act, or in cases when iatrogenesis is closely related to a violent manner of death. In those cases, when forensic expertise is in progress, the most important aim is to determine whether the fatal outcome is directly related to seminal injuries. Additionally, when it comes to this important decision, it is not so rare that an iatrogenic injury results in causal link termination.5,10
In conclusion, TIF is an uncommon but life-threatening condition which should be taken into consideration when sudden and unexplained massive upper gastrointestinal haemorrhage occurs. In such cases, only rapid diagnosis and immediate intervention can reduce high mortality. However, in our case, the exact location of bleeding was not identified when the haemorrhage occurred. Had the patient had a computed tomography examination performed during the stabilisation period after endoscopy, this may have provided a clear diagnosis of TIF, which could have saved him.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interests with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.