
Abstract
We present the case of a 64-year-old woman who committed suicide by jumping from the open bedroom window of her second-floor apartment. However, during a head-first fall, the victim’s head was caught perpendicularly between two parallel metal strands of wire, used for drying laundry, on the first-floor window. This led to a 180° rotation of the body around the lower part of the neck, bringing the victim’s body into the legs-first position. This chain of events also caused short-term neck strangulation, for fractions of a second or a couple of seconds, which caused rupture of the peripheral venules and apparent neck, facial and conjunctival haemorrhages, above the level of strangulation ligature – the metal strands of wire. The presented case shows that even such incomplete, very short-term neck strangulation could raise venous/capillary pressure sufficiently to cause petechial haemorrhages on the neck and face above the level of ligature.
Introduction
Petechiae are pinpoint haemorrhages resulting from the rupture of small vessels. 1 Conjunctival and facial petechiae, although non-specific findings, are considered hallmarks of asphyxial deaths. 2 Although commonly present in cases of asphyxiation, petechial haemorrhages of the face, eyelids and conjunctivae are also present in deaths due to other unnatural (e.g. electrocution, cranio-cerebral trauma, intoxication) or natural (e.g. cardiac, central nervous system, infectious) causes. 3 They may also occur in situations of increased intra-thoracic or intra-abdominal pressure, resulting in inflow congestion and increased pressure to the veins and capillaries of the head and neck region (e.g. epileptic fit, asthma attack, sneezing, coughing, vomiting, giving birth, Valsalva manoeuvre).1–7 These haemorrhages are commonly observed in neck strangulation, 1 and they are commonly visible above the ligature marks.7–9
There is no consensus concerning the time necessary for the development of petechial haemorrhages in cases of neck strangulation (hanging or manual or ligature strangulation). According to some authors, the required time is at least 10–20 seconds up to several minutes of complete venous compression, 10 while others state that petechial haemorrhages may form within seconds or milliseconds.3,11 Herein, we present a case where the development of petechial skin and conjunctival haemorrhages happened in a very short time. This case emphasises that reconstruction of the event is very important for the correct interpretation of the injuries and their mechanism.
Case outline
A 64-year-old woman committed suicide by jumping from the open bedroom window of her second-floor apartment, from a height of about 6–7 m. She was found lying on her right side (Figure 1(a)) on a concrete surface. Since the victim was dead at the scene, no cardiopulmonary resuscitation was performed. The victim lived alone, and her apartment was secured with a chain lock from the inside. Everything inside the apartment was in order, and there was no disarray. The victim had no direct access to the roof from her apartment. The examination of the bedroom revealed partially elevated rolling shutters on the window from which she jumped. The couch was standing right beside this window. A kitchen knife with traces of blood was found in the room on a small table. No suicide note was found, and no prior suicide attempt was registered. The victim had been suffering from depression. There were no data about first-line relatives who committed suicide. The police investigation revealed a torn metal wire used for drying laundry on the window on the first floor, exactly below the spot from where the victim jumped (Figure 1(b)). The torn wire was stretched between two metal holders, which were slightly distorted. The police investigation of the scene excluded homicide, assault or any other physical violence inflicted by another person.
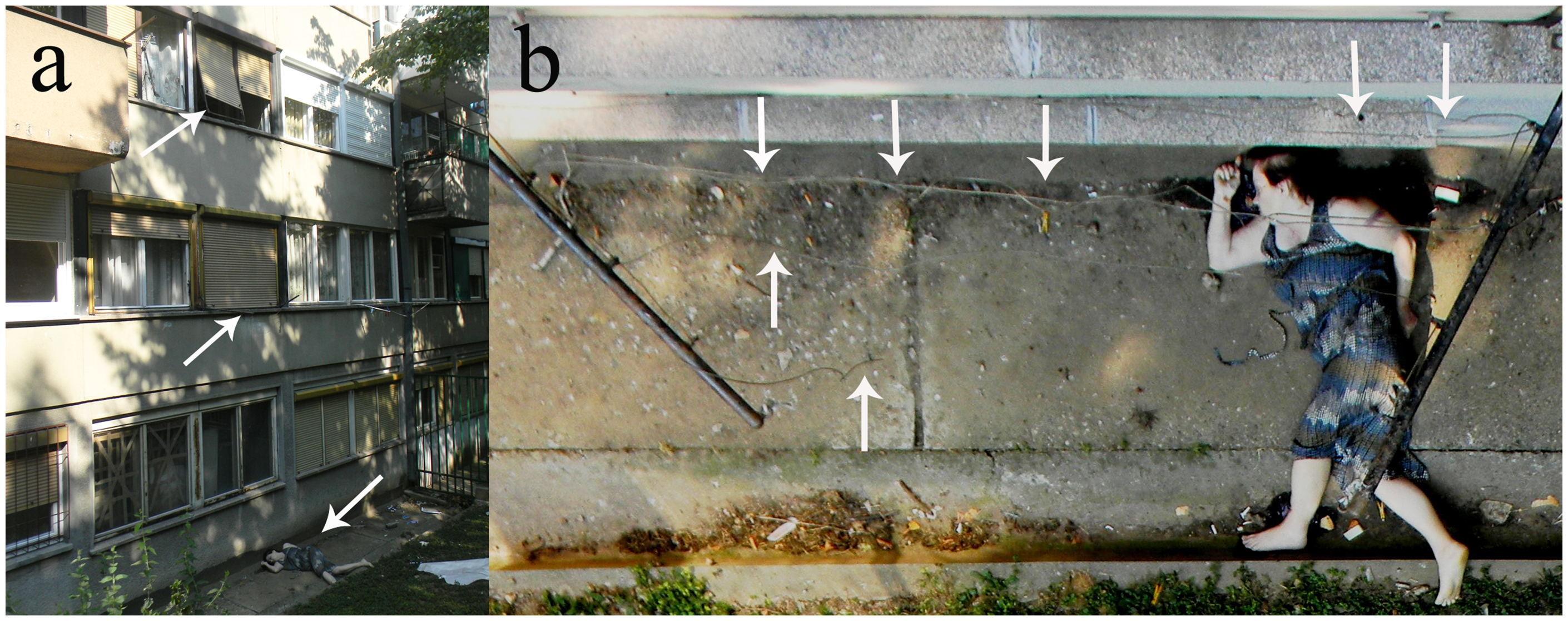
Police photos of the site. (a) Arrows point to the window from which the victim jumped, two metal holders with stretched wire between them (for drying laundry) and the body of the deceased. (b) A closer aspect of the distorted holders with wire stretched between them (arrows point to the intact and torn parts of the wire: the photo was taken through the window from which the victim jumped).
The deceased was 160 cm tall and weighed 62 kg. The victim had an irregular scalp laceration in the middle part of the parieto-occipital region, with surrounding bruising, as well as an adjacent longitudinal skull fracture (extending from the skull lambda, through the sagittal suture, along the middle part of the frontal bone and the left side of the anterior cranial fossa) and a 0.7-cm-long laceration of the dural superior sagittal sinus, located on the periosteal part of the dura. A subdural haematoma was absent, probably due to the location of this laceration as well as the rapidity of death. The victim suffered deep brain contusions on the left basal ganglia, and only a few contusions were present on the tip of the left frontal lobe. Other injuries, both external and internal, which were consistent with a fall from a height, included a fracture of the sternum and multiple ribs, with corresponding pulmonary contusions; burst fracture of the 10th thoracic vertebra; fractures of the spinous processes of the first 10 thoracic vertebrae with surrounding soft-tissue and muscle contusions and haemorrhages; and skin contusions and abrasions on the trunk, arms and legs. The autopsy revealed injuries which implied that the victim fell legs first, that is, the primary contact with the surface was with her feet, not with her head.
However, some of the injuries fell out of this ‘fall from a height’ pattern. First, multiple superficial parallel slash wounds, up to 4 cm in length, were found on both wrists, indicating that this was the primary planned method of suicide. Second, the external examination also revealed multiple petechial skin haemorrhages of the face and the anterior and lateral sides of the neck (Figure 2), as well as conjunctivae (Figure 3). On both lateral sides of the neck, two almost symmetrical rectangular-shaped skin abrasions were determined, implying ligature strangulation of the neck (Figure 2). The examination of all soft and solid neck structures prepared by the layers revealed bleeding and soft-tissue contusions surrounding the lower parts of both the sternocleidomastoid muscles and the left carotid artery. An additional rectangular-shaped abrasion was present on the lateral side of left upper arm.
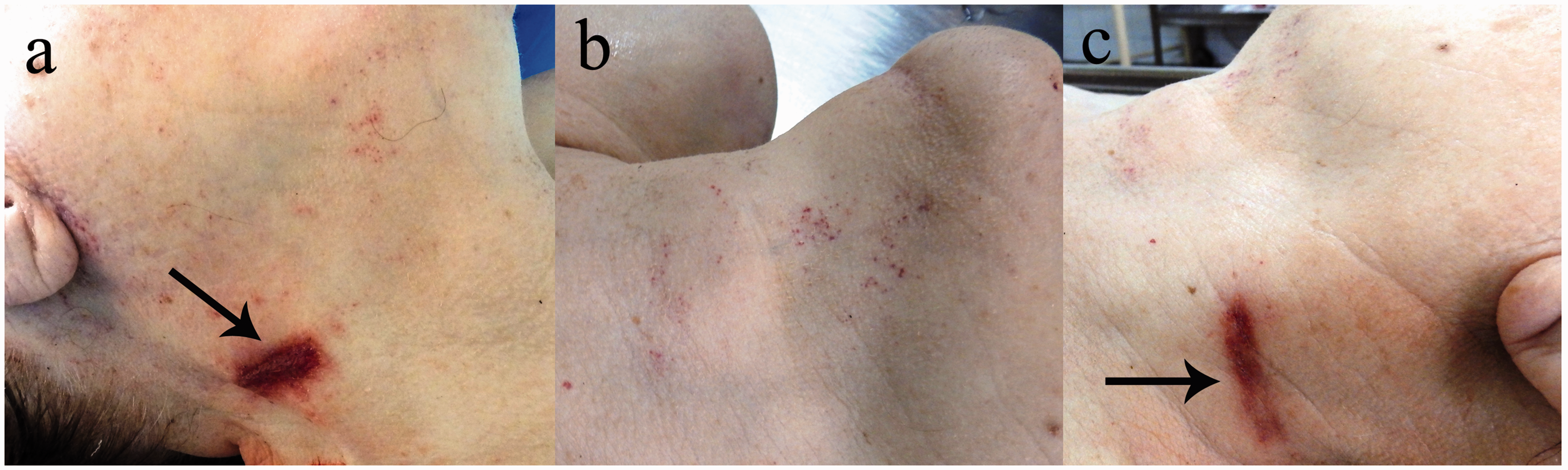
Right (a), anterior (b) and left (c) aspect of the neck. Petechial skin haemorrhages are visible on the neck and face. Arrows point to a ligature mark – skin abrasions.
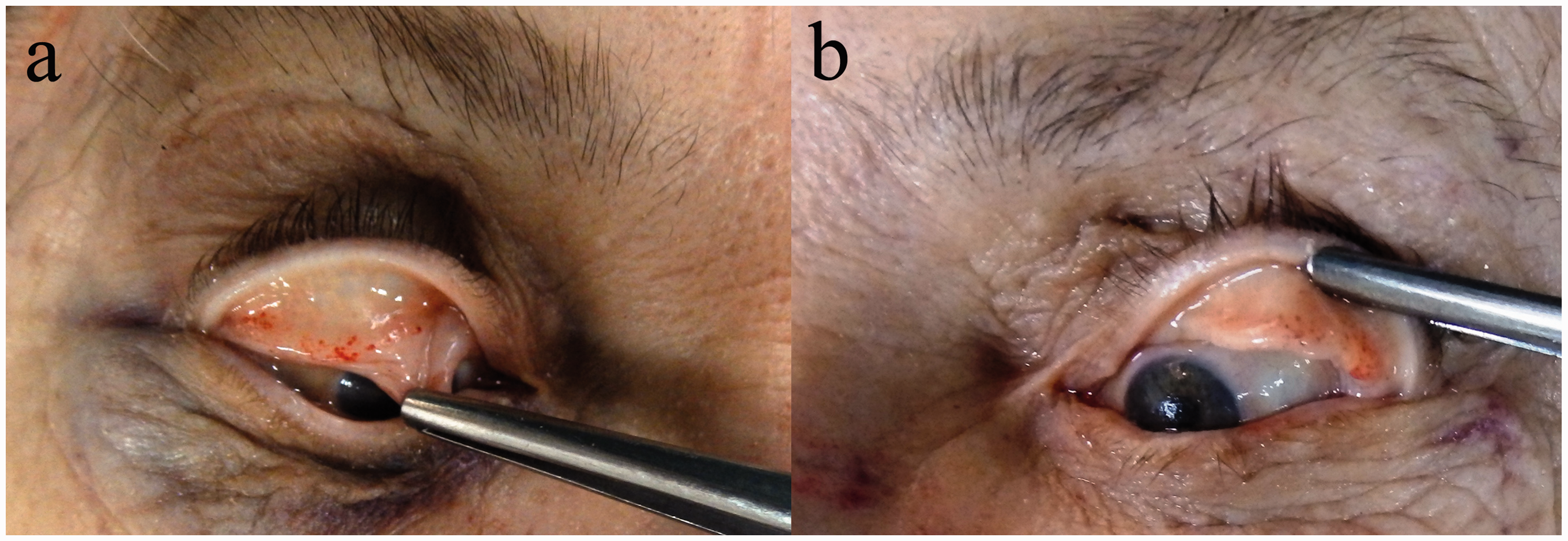
Petechial haemorrhages of the eyelids and conjunctivae of the right (a) and left (b) eye.
As a final note, there was no alcohol or drugs in the blood sample taken from the femoral vein. The cause of death was attributed to traumatic brain injury.
Discussion
Mechanical obstruction of venous return to the heart, in the setting of continued arterial blood flow, causes an increase in intravascular pressure that induces the over-distention of the thin-walled peripheral venules, and this can lead to rupture, as in mechanically caused rhexis haemorrhages. The venules located in areas that are low in connective tissue, such as the conjunctiva and sclera, the skin of the upper eyelid, the forehead, behind the ears and around the mouth, are more prone to rupture. 1 Other, multi-causal explanations include elevated intra-vessel pressure. Mechanical factors seem to be crucial in the occurrence of petechial haemorrhage, and although suggested by some authors, hypoxia is most probably not a relevant factor. 2 As a result of a prone position and/or the head lying lower than the rest of the body, petechiae may also develop post-mortem.2,3 Neither retrospective nor prospective investigations have shown any convincing evidence that facial or conjunctival petechiae result from cardiopulmonary resuscitation.4,5 In our presented case, no cardiopulmonary resuscitation was performed.
As stated before, there is no consensus concerning the time necessary for the development of petechial haemorrhages in cases of neck compression. One of the most commonly described situations where such haemorrhages may form within seconds or milliseconds is thoraco-abdominal compression or crush asphyxia (also known as Perthes’ syndrome). 12 In our presented case, none of these mechanisms were related to petechial haemorrhages: the police investigation did not reveal attempted suicide by hanging, or homicidal strangulation, while the autopsy did not reveal any defence injuries.
The most probable scenario of the victim's suicide, having taken into account her age and physical constitution, indicated that the only way she could have jumped through the window was that she had climbed onto the couch beside the window, squeezed through the semi-open shutters and fallen head first (Figure 4(a)). As some simulation studies have shown, in a head-first fall from a 6 m height, it would be expected that first the head and then the back of the shoulders hit the ground, absorbing most of the impact energy from the fall. 13 However, in the presented case, during a head-first fall, it seems that the victim’s head went perpendicularly between two parallel metal strands of wire (Figure 4(b)), with a gap of about 25–30 cm between the wires being wide enough for the head to go through, without being injured. The upper side of the shoulders prevented the victim’s body from falling further through the wires, and then gravity caused a 180° rotation of the body around the lower part of the neck, bringing the victim’s body into the legs-first position (Figure 4(c)). At that moment, the victim’s neck was tightened between two strained and probably crossed metal strands of wire, which left the symmetrical strangulation marks (abrasions) on the lateral sides of the neck and the rectangular-shaped abrasion on the lateral side of the left upper arm. In this way, the metal strands of wire used for drying laundry acted as a ligature, causing short-term strangulation. After the wire snapped under the weight of the victim’s body, the victim fell (Figure 4(d)) on her left leg, and then suffered injuries to the trunk, head and arms due to a secondary impact.

Graphic presentation of the most probable scenario of the event. (a) Victim squeezed through the semi-open shutters and fell head first. (b) During the head-first fall, the victim’s head went perpendicularly between two parallel metal strands of wire, with the junction of the neck and trunk being caught by these strands. (c) The neck and shoulders being caught in the wire led to a 180° rotation of the body around the lower part of the neck, bringing the victim’s body into the legs-first position and leaving the symmetrical strangulation marks (abrasions) on the lateral sides of the neck. (d) After the wire snapped, the victim fell on her left leg and then suffered injuries to the trunk, head and arms due to a secondary impact.
In the presented case, a short-term neck strangulation – fractions of a second or a couple of seconds – was sufficient to raise enough intravascular pressure to cause rupture of the peripheral venules and apparent neck, facial and conjunctival haemorrhages, above the level of strangulation ligature – the metal strands of wire. The examination of the scene, as well as the skin and deep soft-tissue injuries to the victim’s neck, revealed that this strangulation lasted for a very short period but was strong enough to cause the petechial head and neck haemorrhages.
Petechiae of the facial skin and conjunctivae are of significant value in forensic medical diagnostics. Knowledge of the possible differential diagnoses is essential for the correct forensic interpretation. In the presented case, both the police investigation of the scene and the autopsy enabled the correct reconstruction of the suicidal fall from a height. A reconstruction of the event revealed not only the underlying mechanism of neck strangulation in this case, but also pointed to the fact that even a very short-term (up to fractions of a second or a couple of seconds), incomplete neck strangulation could raise venous/capillary pressure sufficiently to cause petechial haemorrhages on the neck and face above the level of ligature.
Footnotes
Acknowledgements
This work was supported by the Ministry of Education and Science of the Republic of Serbia as a part of the project ‘Age related microarchitectural and mechanical bone properties: Implications for increased fragility’, grant number 45005.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.