
Abstract
There is limited research that comments on whether there are recurring patterns for incidents or significant events during inpatient admissions to psychiatric units. This is even more so the case for an adolescent population. This study looked at 30 consecutive female patient admissions to Bluebird House, a medium secure adolescent unit in the South of England, to identify whether both the ‘honeymoon effect’ (low incident rate in the first 28 days following admission) and ‘gate fever’ (high incident rate in the last 28 days prior to discharge) were identifiable phenomena. Analysis of the incident rate found that in our secure adolescent population, the number of incidents both in the first week and at the first 28 days was higher in comparison to the whole admission. We also did not find a consistent increase in incidents in the final 28 days of the admission.
Background
The way that children or young people can access Child and Adolescent Mental Health Services (CAMHS) depends on the type of support that is needed. There are four tiers of service provision, each providing different types of intervention. 1 Tier 4 provides specialist CAMHS support, including secure forensic mental health services. 1 There is a national network that provides provision for medium secure adolescent care, which includes Bluebird House in Hampshire.
If adolescent patients become involved with the criminal justice system, or if the risk they pose to other people is significantly high, then referral for secure inpatient admission may be considered. Adolescent patients in secure hospitals may have multiple diagnoses, including psychotic, affective and neurodevelopmental disorders. There may also be behavioural disturbances, including conduct disorder and features of emerging personality disorder. 2 A previous study of 30 consecutive female patients admitted to Bluebird House found a high number of patients (70%) fulfilling the criteria for mixed disorder of conduct and emotions, with their presentation consistent with the adult diagnosis of emotionally unstable personality disorder. 3 Also identified were high incident levels involving both self-injurious behaviour and aggression towards staff, and that incident rates in female adolescent patients detained in secure hospitals can be much higher than for male patients. 4
The management of incidents is an important factor for treatment in adolescent secure hospitals. Restraint and/or use of seclusion facilities may be required in order to manage the acute risk that develops. Other factors that may increase the need for restraint and/or seclusion include younger age, longer length of inpatient admission and prior inpatient admissions. 5
In addition, the challenges that adolescence itself brings, with emotional difficulties, mood disturbance and physical and biochemical change, play an important part that can modify behaviour and influence psychiatric co-morbidity. Emotional dysregulation itself is a risk factor for the adolescent development of symptoms of anxiety, depression, eating pathology, substance abuse6,7 and aggressive behaviour. 8 The ‘adolescent hormonal milieu’ may also play a part in the pathogenesis of psychosis. 9
Admission to adolescent psychiatric inpatient units is challenging for both the patients and their families. In secure adolescent hospitals, all the patients are detained under the Mental Health Act 1983. At Bluebird House, there is a wide therapeutic team including practitioners delivering education, psychology, occupational therapy, art therapy, nursing and medical care. The change from open to secure settings brings with it anxiety about what the admission signifies and whether there are long-term consequences. Living alongside other patients with mental health problems can be challenging but also educational and informative for each individual patient.
Both admission to and discharge from inpatient units can be a particularly challenging time for patients. Changes in the environment, more restrictive practice and greater distance from family and loved ones can all have a significant impact on the first few weeks in a new inpatient unit. Anxiety that arises towards the end of the admission, as the patient prepares to move on to a new environment and continue recovery, can lead to acting out and an increase in the number incidents prior to discharge.
Honeymoon effect
The ‘honeymoon effect’ is well established as a social psychological phenomenon that may be seen during a transitional period. For an initial time, the adjustment to transition or change may bring with it a perceived sense of stability, which may be short-lived. This may also be seen in a hospital setting. For an adolescent inpatient population, there may also be a change in behaviour when comparing the initial days or weeks of inpatient admission to the later stages of admission, which may lead to an emergence of symptoms. 10 There may be a strong apparent wish to please for children entering into a residential facility. 10
The expectation that staff have of newly admitted patients may also change as the admission progresses. 11 In order to reduce the anxiety that new patients can experience, staff may be more accommodating and less restrictive in the early stages of admission. When early therapeutic relationships are formed, the staff then may adopt a more boundaried approach.
Shorter inpatient admissions may even mask the difficulties that a child faces, as the healthcare team may only observe ‘suppressed behavioural difficulty’. 12 Early acknowledgement of patients who present with the most challenging behaviours during their admission is important when thinking about the therapeutic milieu and for allocation of therapeutic resources. 5 Masked behaviour, as a result of a honeymoon effect, can make this difficult.
There have been attempts to study this phenomenon, but the data are limited and not recent. One study has shown that for a group of 28 children admitted to an inpatient unit, there was a clear increase in symptomatology (uncontrolled aggression, misbehaviour and excessive dependency) at 60 days into the admission in comparison to at 14 days. 13 In a study of 98 child psychiatric inpatients, 34% presented with ‘well-controlled behaviour’, 15% showed some improvement and 30% presented with no clinical change in the initial stages of admission, but this led onto a significant deterioration after a an average of 6.8 days. 11 For patients with hyperkinetic disorders, Blader et al. 11 hypothesised that the honeymoon effect may occur due to the novelty or heightened stimulation that can produce an improvement in behavioural regulation.
In a study looking at incidents that involved the use of seclusion and restraint, there was a peak in incidents in both the second and third months of admission in comparison to the first month. 5 In another study that analysed the effects on incident rate after physical changes were made to the unit environment, the number of incidents in the first six months following the environmental change reduced to 54% of the amount that took place during the preceding year. 14
Gate fever
The concept of ‘gate fever’ is less described in the literature. In clinical practice, it is a term used more frequently in prison populations, although the phenomenon has not been widely examined, even less so than the honeymoon effect. For the prison population it has been described as ‘a state of pervading restlessness prior to liberation’, most likely a transient phase in which the prisoner contemplates the transition between incarceration and release. 15 Multiple factors may contribute to the development of gate fever, including duration of custodial time, transition plans on release from prison, emotional state and presence of mental illness. 15
There is some suggestion that an increased number of prison sentences builds more anxiety prior to release. 15 This may reflect the difficulties that more institutionalised prisoners may have with re-adjusting to non-custodial environments.
Prison can provide a containing environment and the regime and structure can appeal to offenders who have not previously experienced this. For some offenders, in particular those who are younger, the prison officers may well take on a more parental role, by both conscious and unconscious mechanisms.
In a UK high secure hospital, a leavers’ group has been established in order to offer support during the transition when moving on from high secure care. 16 For patients who had undergone a lengthy admission and for transferred prisoners continuing with hospital treatment beyond their prison tariff, the group has proved to be of valuable therapeutic benefit. This highlights how intervention at this crucial stage can assist and motivate patients for change and onward recovery.
In an adolescent population, who are naturally more dependent on adult caregivers, it is likely that a significant amount of anxiety will be triggered for an inpatient transferring into the community, not unlike that described in the prison population. Frequently, the influence of stressors in the family home are incorporated into the psychological formulation of adolescent secure patients, and so potential return to this environment could understandably lead to anxiety and distress. Likewise, it can be challenging for patients transferring onto other inpatient units or community residential settings to form new relationships with staff and peers, in particular those with significant interpersonal and attachment difficulties.
As discharge plans come to fruition, the patient may experience anxiety about moving on, which may present with acting-out behaviour and even aggression. 17 There are many variables that may play a part in modifying this phenomenon, including the strengths/skills that help the patient, the parents and the staff prepare for change. 10 Even with achievement of inpatient treatment goals, discharge may bring with it feelings that the residential team have abandoned the patient, which may in turn lead to regressive behaviour. 17 Feelings of abandonment may also arise in the parents, who may show feelings of rejection that both they and their children are being ‘let go’, and this may be an indicator of their own dependence on the hospital and its staff. 17
Anxiety and frustration experienced by the patients may be taken out on themselves or other people and this may reflect an attempt to prolong the current admission in order to maintain the environmental and psychological structure within which they have been working.
This study aimed to test the hypothesis that incident rates are lower in the first week and month of an admission (honeymoon effect) and increase in the last month of the admission (gate fever).
Method
Incidents were reviewed on a retrospective basis for 30 female consecutive patients admitted to Bluebird House between 2008 and 2012. This patient group has been the subject of a previous paper looking in detail at their clinical characteristics. 3 As part of that study, the number of incidents per occupied bed day (incident rate) was calculated for the whole admission for each patient. Data were gathered from incident form logging, via the trust electronic incident form database whose completion is required following incidents that occur within the unit. Incidents were classified as occurrences of aggression, violence or self-harm. The patients have all now been discharged, with the final patient being discharged in 2015.
The incident rates were calculated per day for the first week, the first 28 days and the last 28 days of the admission. These rates were subsequently compared with the overall incident rate for their admission to establish if incident rates at the beginning and end of the admission were different to the overall incident rate. The honeymoon effect is defined as when the incident rate for a patient is lower in the first week or 28 days of the admission than the average for the whole admission. Gate fever is defined as when the incident rate is higher in the last 28 days of the admission compared to the average for the whole admission.
Results
The sample
The first 30 female patients were admitted to Bluebird House between February 2008 and June 2012, and they were discharged by May 2015. This sample consisted of 30 discharged patients. The sample ranged in age from 14.38 to 17.93 years at admission, with a mean age of 16.41 years. Twenty-three (77%) were of white British background, with four (13%) mixed race and three (10%) black British. The sample was admitted from a variety of sources, but the majority came from other hospital settings (n = 20; 66%). The remaining 10 (33%) were admitted from non-hospital secure settings; youth offender institutes (n = 5), secure training centres (n = 1) and secure children’s homes (n = 4).
Patients’ length of stay ranged from 35 to 1364 days, with a mean length of stay of 412 days. The total combined number of occupied bed days of all patients within the sample was 12,362 days.
All patients were detained under the Mental Health Act. Twenty one (70%) were initially detained under Section 3 (six-month treatment section), one was detained under Section 2 (28-day assessment section), three (10%) were detained under Section 37 (Hospital Order as a court disposal; none of these had Section 41 Restriction Orders) and five (17%) detained under Section 47 or Section 48 (transfer of sentenced or remand prisoners from custody to hospital, all with Section 49 Restriction Orders). 3
Course of admission
The total number of incidents recorded for all 30 female patients between February 2008 and May 2015 was 15,051, giving an incident rate per occupied bed day of 1.22. This means, on average, each female young person had approximately one incident a day during their admission.
For the number of incidents within the first seven days of admission, the total was 424, giving an incident rate of 2.01 (SD = 1.41) per occupied bed day. This means, on average, each female patient had approximately two incidents a day during their first week at Bluebird House. Only five out of 30 patients had lower incident rates during the first seven days of admission when compared to their overall incident data.
During the first 28 days of admission, the total number of incidents was 1502, which is an incident rate per occupied bed day of 1.79 (SD = 1.18). When compared with overall incident data, this is also higher. All except two patients had higher levels of incidents within their first 28 days when compared to their overall incident data.
The total number of incidents within the last 28 days of their admission was 509, which is an average of 0.60 (SD = 0.89) incident rate per occupied bed day. This is lower than the overall incident rate. There were six cases that had higher levels of incidents during their final 28 days at Bluebird House when compared to their overall incident data.
As the data were skewed, a Wilcoxon signed rank test was run. It revealed a statistically increased level of incident rates during the first 28 days of admission when compared to the overall incident data for the entire length of stay (z = –4.08, p < 0.001), with a large effect size (r = 0.53). This indicates that there was a higher level of incidents when the patients were first at Bluebird House compared to the overall incident data for the rest of their stay. This was also completed to compare the last 28 days to the overall incident data. This revealed a statistically decreased level of incident rates (z = –4.04, p < 0.001), with a large effect size (r = 0.52), which suggests that the level of incidents leading up to the patients’ discharge was lower when compared to their overall incident rate at Bluebird House.
Discharge destination
Discharge destinations included open non-hospital settings, open hospital settings, low secure inpatient settings and medium/high secure inpatient settings.
Thirteen (43%) patients went to an open non-hospital setting, such as a community placement or residential care. For this group, the age range at admission was 14.38–17.92 years and at discharge it was 14.98–18.75 years. The average length of admission was 211 days, with a range of 35–740 days.
Four (13%) patients went to an open hospital setting. Their ages ranged from 15.41 to 17.08 years on admission and from 16.86 to 18.78 years on discharge. The average length of stay for a young person who went on to an open hospital setting was 404 days, with a range of 46–749 days.
Five (17%) patients went to a low secure inpatient setting, whose age ranged from 15.35 to 17.78 years at admission and from 16.78 to 18.71 years at discharge. The average length of stay for a young person who went on to a low secure facility was 521 days, ranging from 153 to 980 days.
Eight (27%) patients moved on to a medium/high secure unit. Three out of four cases with higher levels of incidents during their last 28 days at Bluebird House fell within this group. The age ranged from 14.47 to 17.92 years on admission and from 18.03 years to 18.90 years on discharge. The mean length of stay for these patients was 676 days, with a range of 63–1364 days.
Despite the large variance between lengths of stay, these data indicate that a longer length of stay relates to being discharged to a secure unit instead of an open unit.
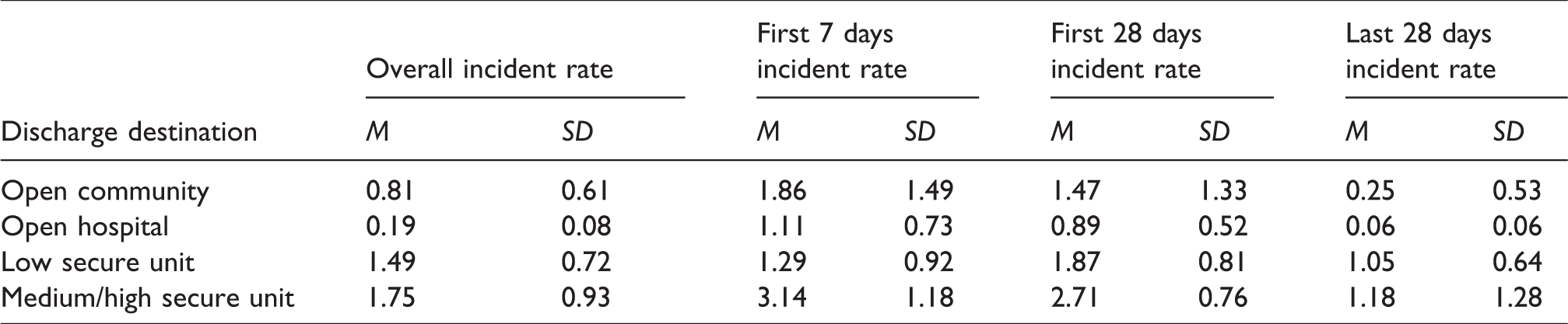
These data also indicate that patients who have progressed on to secure units, as opposed to a non-secure placement, have a higher incident rate. Specifically, the level of incidents across the different time points (first seven days, first 28 days, last 28 days and overall) appear to be highest within the group discharged to medium/high secure unit (mean levels of incidents within the last 28 days were 1.18, SD = 1.28, whereas for an open non-hospital setting they were 0.25, SD = 0.53). Interestingly, discharge to open hospital was associated with lower levels of incident rates at each time point when compared to discharge to an open non-hospital setting.
Mean (M) and standard deviations (SD) of the incident rate for each discharge destination.
Discussion
These results demonstrate some interesting contradictions to existing theories about the honeymoon effect and gate fever. The results showed a peak in the incident rate both in the first week and also the first 28 days of the admission in comparison to the incident rate for the whole admission. This is clearly not a honeymoon effect. In our group of patients, only five (16.7%) patients had an incident rate lower in the first week and only had a lower rate in the first 28 days than the incident rate for the whole admission. Only six (20%) patients had a higher incident rate in the last 28 days compared to the average for the whole admission, which suggests that gate fever is uncommon. Neither the honeymoon effect nor gate fever was commonly observed in our sample, despite these terms being used in conversations between staff in inpatient units.
The data indicate how difficult the first few weeks of inpatient admission are for young people admitted to a secure hospital. Whilst the destabilising effects of the patient’s environment prior to admission can act as a perpetuating factor for distress, it is clear that the move to what may end up being a more containing environment is initially an incredibly difficult adjustment. It places emphasis on the importance of trying to meet and form a therapeutic relationship with the patients before they are admitted, wherever possible. Developing this relationship during their admission can help improve their sense of security and attachment to the team, allowing them to explore difficult aspects of their lives and can ultimately enable them to develop skills to manage their behaviours. This is turn could have a positive effect on patient outcome. 18 No patients were admitted from home, and it is important to reflect on how disruptive the time preceding their admission may have been, possibly with numerous inter-hospital transfers or time spent in custody.
The rarity of the honeymoon effect in our adolescent cohort highlights just how underdeveloped the patients’ ability is to deal with change and to form new relationships.18,19 Many of our patients have very disrupted care histories with fewer opportunities to form secure attachments in childhood. Furthermore, there is evidence of young people within these types of secure settings regularly showing insecure attachment styles. 20 It is perhaps unsurprising that until the newly admitted adolescent patient has built relationships with the staff team, there will be a high level of incidents. Whilst the overall incident rate is lower than in the early stages, the average of 1.22 incidents per day per patient is high and provides an idea of how disruptive and destabilising admission into secure adolescent care can be.
The complex nature of the patients admitted into secure care places great emphasis on the need for close collaboration between members of the multidisciplinary team. Multi-agency working, as well as the use of graded transition programmes using extended Section 17 leave, can help smooth the process of leaving hospital. Long-term Section 17 leave can also allow for reduced time spent in inpatient settings immediately prior to discharge, which may provide some explanation as to why gate fever is a rare phenomenon in our inpatient group.
There is a relationship between the higher incident rate throughout the admission and discharge to another medium or high secure unit. This is seen especially in the first 7 and 28 days of admission. This suggests that incident rates in the first month of admission in our female sample may be somewhat predictive of the level of security they will require on discharge.
Unanswered questions and future research
Overall, the incident rate appears to fall throughout the admission, and it may be that some of the difficulties that the patients experience may improve not only with treatment but also with consistent support and caregiving figures, as well as with advancing age and maturity. Our study included a small number of very complex patients, but these data join a very limited amount of information already available in the literature about this subject. We suggest further research in this area in larger samples and different clinical populations to establish whether the honeymoon effect and gate fever are common phenomena in other institutions and in order to allow for comparison of groups that do and do not show either phenomenon. We have also not undertaken a sub-analysis to look at different types of incidents (e.g. aggression vs. violence vs. self-harm) and these results may further add relevant findings.
Understanding how incident rates change during the course of admissions to psychiatric hospitals is an important aspect of clinical management and policymaking, and is worthy of more detailed studies.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.