
Abstract
This study sought to determine how often a medico-legal (coronial) autopsy contributes by identifying the source of infection when there has been a clinical diagnosis of sepsis prior to death. Autopsy reports were retrieved in which it was documented there had been a clinical diagnosis of sepsis preceding death. The autopsy report was reviewed to determine if a source for sepsis had been identified. It was found the autopsy was contributory in this respect in less than one fifth of all cases (35 of 198, 18%). It was also determined if there was a post-autopsy diagnosis of sepsis or if sepsis was excluded by a definite alternative diagnosis. During the study, of the 198 cases, sepsis was excluded by an alternative diagnosis in 78 (39%). Thus, the autopsy may be of more application to confirming or excluding a diagnosis of sepsis than identifying a source for sepsis.
Introduction
Sepsis has been defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. 1 The annual incidence of severe sepsis has been estimated as 0.77 per 1000 population in Australia and New Zealand, 2 with a mortality of around 21% in adult intensive care patients. 3 Deaths attributed to sepsis may be reported to a coroner for investigation. However, it is not established how often an autopsy will provide information regarding the aetiology of the sepsis. 4 This study aimed to determine how frequently a coronial autopsy provided contributory information when the clinical opinion was that death had resulted from sepsis. Due to difficulties surrounding post-mortem microbiology, 5 it was hypothesised that in the majority of cases an autopsy would not provide contributory information regarding the source of sepsis that was not known before death.
Methods
Autopsy reports from 1998 to 2017 at Forensic Science SA were searched for the words ‘sepsis’ or ‘septic’. All documents containing one or both of these keywords were collected. Cases that involved police investigation or investigation of concerns raised by next of kin were excluded. Deaths of infants were also excluded. Based on the pre-autopsy history (clinical information) in the autopsy reports, cases were classified as ‘sepsis’ when it appeared that the clinicians were confident of the diagnosis and as ‘possible sepsis’ when sepsis was included in the differential diagnosis, indicated as a considered possibility or had been diagnosed during the hospital admission and not subsequently excluded prior to death. From the conclusion and comments of the autopsy report, it was determined if there was a post-autopsy diagnosis of sepsis or if sepsis was excluded by a definite alternative diagnosis. In cases of pre-autopsy and post-autopsy diagnoses of sepsis, the autopsy report was reviewed to determine if the autopsy was considered ‘contributory’, that is, it had provided information about the source or agent of sepsis that had not been known prior to the autopsy. Ethical approval was provided by the University of Adelaide HREC (ref. H-2018-145).
Results
A total of 198 cases with a pre-autopsy history that suggested a clinical diagnosis of sepsis were included in the study. From these, it was determined that 74 (37.4%) had a post-autopsy diagnosis of sepsis, and 78 (39.4%) had a post-autopsy diagnosis that excluded sepsis. A post-autopsy diagnosis of sepsis could not be confirmed or excluded in the remaining 46 (23.2%) cases.
Of the 74 pre-autopsy and post-autopsy sepsis cases, there were 38 (51%) males and 36 females, with a median age of 61 years (interquartile range (IQR) 50.5–73 years). In 35 of these 74 cases (47%), comprising 18% of the total cases, it was considered that the autopsy had been contributory by identifying a source of sepsis. A review of the clinical information on the autopsy report indicated a pre-autopsy diagnosis of sepsis had been made in 53 (72%) cases, whereas sepsis was considered a possible diagnosis in 21 cases. The proportion of contributory cases when the pre-diagnosis was sepsis (23/51; 45%) was not significantly different from cases with a possible diagnosis of sepsis (12/23; 52%). The time interval between clinical diagnosis of sepsis and death could be determined in 43 cases. A cumulative frequency curve using the number of contributory cases from this group (18/43) against days from diagnosis to death showed that most contributory cases occurred when death was a day or less from diagnosis of sepsis, with fewer contributory cases occurring with a longer pre-death diagnosis of sepsis, as would be expected (Figure 1).
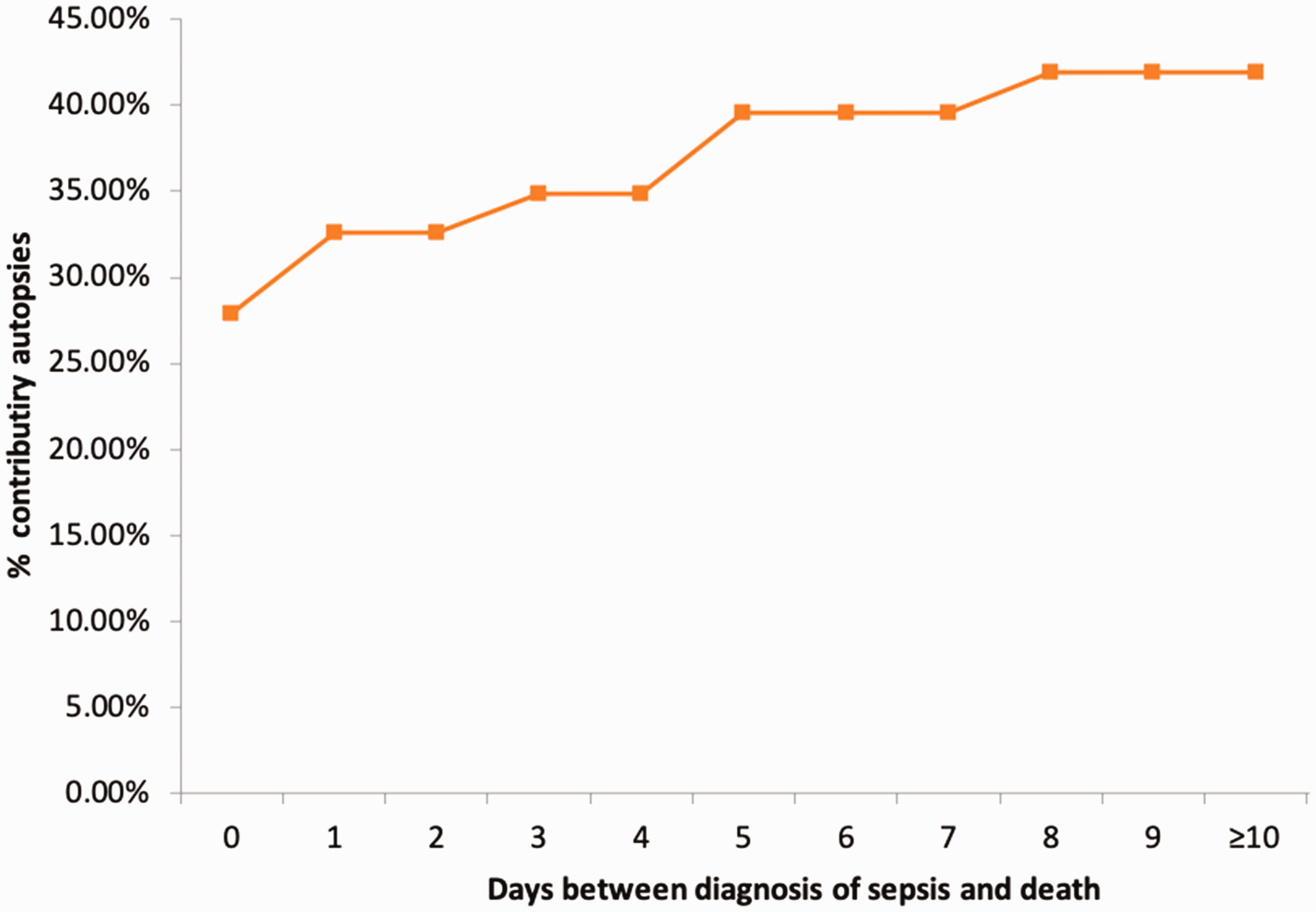
Cumulative frequency plot of cases considered contributory when sepsis was considered as a pre-autopsy diagnosis and sepsis was diagnosed by autopsy, in relation to the length of time between the clinical diagnosis of sepsis and death. Data derived from 43 cases with identified interval from diagnosis of sepsis to death.
In 78 cases, there was a pre-autopsy diagnosis of sepsis, but the post-autopsy diagnosis excluded sepsis. There were 42 (54%) males and 36 females. The median age was 76 years (IQR 62–84 years), which was significantly greater than the groups with pre- and post-autopsy diagnoses of sepsis (Mann–Whitney U-test p < 0.001). A pre-autopsy diagnosis of sepsis had been made in 31 (40%) cases, but had been suggested only as a possible diagnosis in 47 cases. The proportion of cases of possible sepsis was significantly greater in this group (47/78; 60%) than in the previous group that had a post-autopsy diagnosis of sepsis (21/74; 28%; chi-square test p < 0.001). There was a range of post-autopsy diagnoses, including cardiovascular disease, pancreatitis, pulmonary thromboembolus, haemorrhage, cancer/lymphoma and pulmonary disease. Of these, a cardiac cause of death was recorded in 33 cases. The number of days from the diagnosis of sepsis to death during the hospital admission could be ascertained in 57 cases. A frequency distribution plot (Figure 2) showed most cases had been considered to have a septic illness for three days or less prior to death. However, there were a number of cases in this group with a terminal illness of more than 15 days.
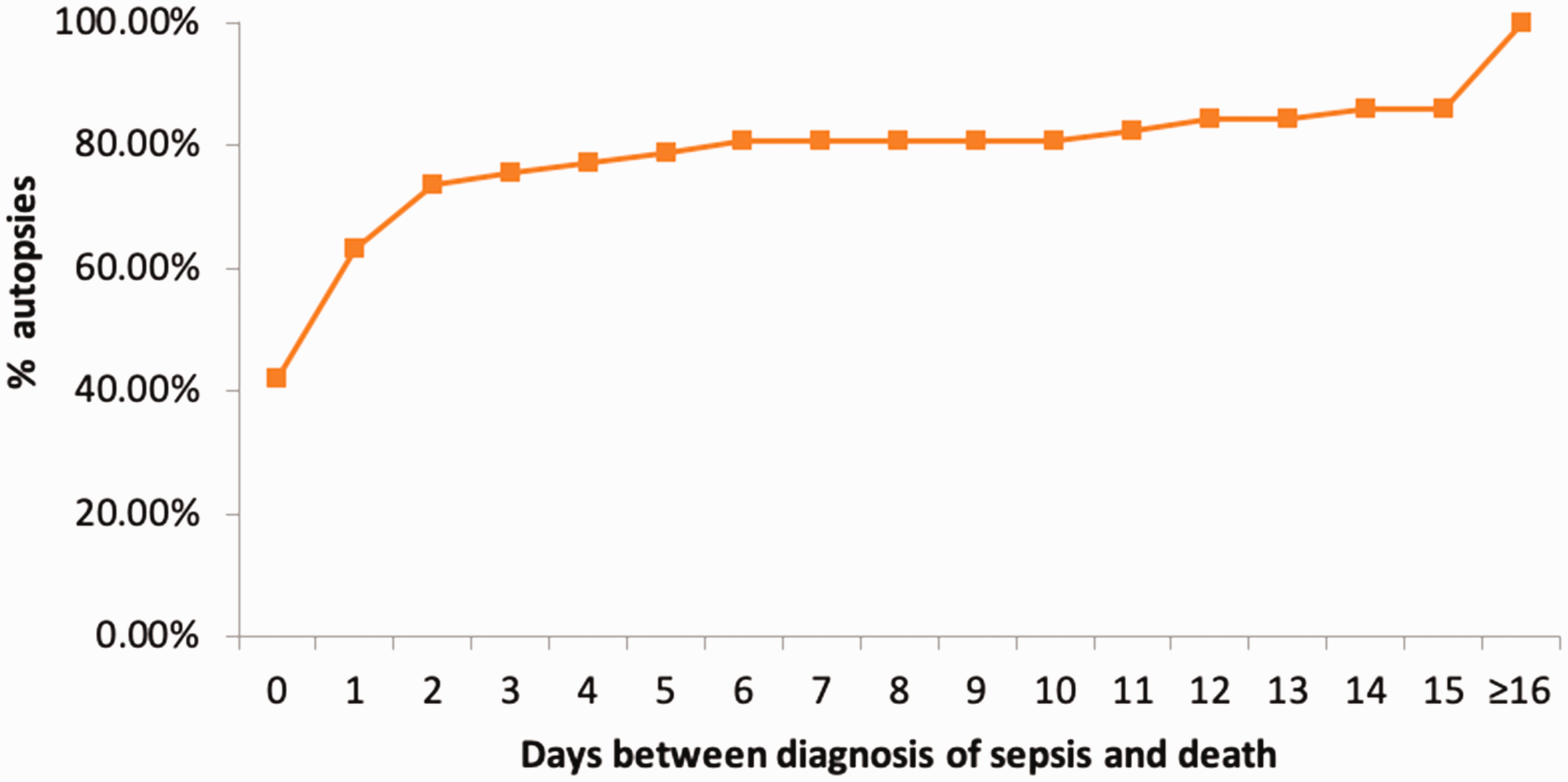
Cumulative frequency plot of cases where sepsis was considered as a pre-autopsy clinical diagnosis, but an alternative diagnosis was made by autopsy, in relation to the length of time between the clinical diagnosis of sepsis and death. Data derived from 57 cases with identified interval from diagnosis of sepsis to death.
Discussion
This study sought to determine how frequently an autopsy within the coronial medico-legal system is contributory by identifying the source of infection when there had been a clinical diagnosis of sepsis prior to death. A search of the literature was performed to find any comparable studies. There are publications comparing the accuracy of clinical diagnoses in the light of post-mortem diagnoses, but papers specifically addressing the question of how often an autopsy is contributory when a diagnosis of sepsis was made during life were not identified. This confirms the observation there is little information in the literature on the rates of autopsy to identify the cause of fatal sepsis. 4
Of the 198 total cases, a diagnosis of sepsis was excluded by an alternative specific autopsy diagnosis in 78 (39%) cases. It is recognised that sepsis can be over-diagnosed clinically and discrepancies between pre- and post-autopsy diagnosis of sepsis occur. 6 This may be partly explained by the observation that non-infective disorders may present similarly to sepsis, as the same signalling pathways may be activated.7,8 Recognised mimics of sepsis include cardiac disease, pulmonary thromboembolus, haemorrhage and pancreatitis. 9
There were 46 (23%) cases for which a diagnosis of sepsis was not confirmed or excluded by the autopsy. These cases may reflect the difficulty of establishing a post-mortem diagnosis of sepsis, as autopsy findings in suspected sepsis cases often lack specificity and sensitivity.10,11 Furthermore, the current clinical diagnosis of sepsis is defined by a life-threatening organ dysfunction due to a dysregulated response to infection, 1 which is difficult to prove at autopsy.
The aim of the study was to determine if the autopsy was considered ‘contributory’. The criterion applied was for the autopsy to have provided information about the source or agent of sepsis that had not been known prior to the autopsy. This occurred in only 35 (18%) of the 198 cases that had a clinical diagnosis of sepsis. This may partly reflect difficulties in interpreting post-mortem microbiological results.12,13 However, the low figure may reflect the number of cases in which autopsy excluded a diagnosis of sepsis. If only cases in which there was clinical and autopsy diagnosis of sepsis are considered, then a source of infection was identified in 47% (35/74) of the cases.
Consequently, of the 198 cases with a pre-mortem clinical diagnosis of sepsis or possible sepsis in this study, an autopsy was regarded as contributory by identifying the source of sepsis in 35 cases, but the autopsy could also be regarded as beneficial by excluding sepsis in 78 cases. This retrospective study has shown the autopsy mostly did not identify a source of sepsis. However, contrary to initial expectations, overall the autopsy could be considered useful in 113/198 cases, which is just over half (57%) of deaths following a clinical diagnosis that considered sepsis in the cause of death. Autopsies following death within three days of diagnosis had the highest yield. The intention of this study was not to determine the relevance of the autopsy to medico-legal aspects around the clinical diagnosis or management, and cases that involved police investigation or investigation of concerns raised by next of kin were excluded.
The main limitations of this study are considered to lie in the acceptance of the clinical and autopsy diagnoses without verifying the criteria and confirming the validity of the conclusions. It was not determined if pathologists performed optimal microbiological investigations5,14 in all cases. Nonetheless, as a first study of the contribution of medico-legal autopsy to the investigation of death following a clinical diagnosis of sepsis, useful information has been obtained.
This study was performed because a number of cases with a clinical pre-mortem diagnosis of sepsis had been referred to our coroner with a request for autopsy to determine the underlying cause. Although the cases had been referred to the coroner for investigation, in cases with no medico-legal issues, the policy statement by the Royal College of Pathologists of Australasia 15 indicates that these cases would have been more appropriately investigated outside of the coronial system. The autopsy can provide useful microbiological information in cases of sepsis. 5 However, the medico-legal autopsy generally does not focus on issues of medical audit, education and research. Consequently, following a diagnosis of sepsis, it appears it would be beneficial for clinicians to request an autopsy through the hospital system, unless there are mandatory reporting issues surrounding a death that necessitate referral into the coronial or other medico-legal system.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by a University of Adelaide Summer Research Scholarship.