
Abstract
Keywords
Introduction
Opioid use disorder remains a serious problem in jails and prisons worldwide, and substance use is a risk factor for incarceration.1,2 Nevertheless, based on data collected in 2016–2017, 19% of 39 Member States of the WHO European Region do not offer OST in prison. 1 To date, OST in U.S. prisons and jails is uncommon, and access is often limited to pregnant women, individuals who received OST prior to incarceration, or those with an early release.3,4 The effectiveness of OST in community settings is well-documented, but there is limited research among incarcerated individuals.
There are many factors to consider in incarceration-based OST that are less relevant in community settings. There is no free choice of doctor 5 ; the institution's goal is to ensure safety of the general population and rehabilitation of the incarcerated individuals rather than health care; individuals with substance use problems are overrepresented1,2,6; there is an increased risk of illegal trade with prescribed drugs in prisons; and medical staff are less inclined to prescribe OST. 7 It is becoming clear that research data collected from community populations cannot be easily transferred to incarcerated populations.
Moore et al. 8 provided an initial overview of the topic and integrated existing research published through 2017. This meta-analysis and systematic review investigate the effectiveness of medication-assisted treatment offered in prisons, which includes not only OST (opioid agonist treatment with methadone or buprenorphine) but also opioid antagonist treatment with naltrexone. In a meta-analysis, the authors found that methadone substitution therapy delivered during incarceration increased community treatment engagement and decreased illegal opioid use as well as injection drug use, but did not have an effect on legal recidivism. 8 However, only randomised controlled trials (RCTs) offering incarceration-based methadone were integrated into the meta-analysis; observational studies were included only in a narrative review. Excluding studies with lower methodological rigour (e.g. quasi-experimental) is not ideal, as ethical concerns could prevent researchers from conducting RCTs. Furthermore, the number of buprenorphine and naltrexone studies identified by the authors was insufficient for meta-analysis. 8 This led to a small number of studies included in the meta-analysis (n = 4), which makes interpretation difficult. 8
Although a wide range of literature reviews and meta-analyses exist on the overarching topic of OST,9–12 little research has focused on studies carried out on incarcerated populations, as other researchers have already pointed out.8,13–16 To integrate the existing data, to evaluate the current state of research in this area and to find out whether the criticised research gap has closed in recent years, we have carried out a meta-analysis of OST studies in correctional settings.
Aim and research question
Our main aim was to describe the effects of incarceration-based OST on substance use, treatment engagement post-release and re-incarceration. As there is an overrepresentation of research conducted in the U.S., our initial intention was to focus on empirical data collected in Europe. However, research conducted in Europe turned out to inadequately cover the effects of incarceration-based OST. Consequently, we refrained from defining geographic restrictions. Considering the fact that empirical data collected all over the world presents difficulties due to the strongly diverging correctional and treatment settings, we decided on a wide definition of the term ‘incarceration’, including prisons and jails while excluding probation and parole populations, to take different legal systems into account without getting too much variation in the database. Empirical data collected after release from prison or jail (follow-up data) were of particular interest, as we wanted to examine the long-term effects of OST.
Our main research question is: Does OST during incarceration reduce illegal opioid and other drug use, enhance treatment engagement post-release and diminish re-incarceration, compared with no or alternative treatment?
Method
Search strategy and inclusion criteria
PubMed, APA PsychInfo and Psychology and Behavioural Science Collection databases were searched using the following query: (heroin OR opioid OR heroin dependence OR opioid dependence OR heroin use disorder OR opioid use disorder OR heroin addiction OR opioid addiction OR opioid-related disorder OR substance use OR drug abuse OR Heroinabhaengig* OR Opioidabhaengig* OR Substanzabhaengig*) AND (methadon* OR buprenorphin* OR naltrexon* OR naloxon OR substitution OR substitution treatment OR methadon* maintenance treatment OR buprenorphin* maintenance treatment OR naltrexon* maintenance treatment OR medical assisted treatment OR drug abuse treatment) AND (prison OR prisoner* OR correctional population OR correctional setting OR jail OR inmate OR incarceration OR gaol OR criminal* OR criminal recidivism OR Haft OR Inhaftierung OR Gefaengnis) AND (evaluation OR evaluation study OR randomized control trial OR quasi-experiment OR effectiveness OR treatment outcome OR follow-up studie* OR randomisierte Kontrollstudie OR Evaluationsstudie OR Wirksamkeit OR Effektivitaet).
We searched for articles and reports published in English or German language from January 1, 1990, through July 7, 2020. Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines were used to display study search and selection process. 17 Randomised controlled trials, quasi-experimental studies and observational studies were included.
We included studies on individuals who used opioids and were incarcerated in a prison or jail. Another inclusion criterion was an OST intervention in the treatment group. Eligible studies had a comparison group of incarcerated individuals, and reported data collected after study participants were released from prison or jail.
Exclusion criteria: At first, we considered any medication-assisted intervention (with methadone, levo-alpha-acetylmethadol, buprenorphine and/or naltrexone) provided during incarceration. However, differences emerged when comparing studies that use full opioid agonist treatment (methadone, levo-alpha-acetylmethadol), partial opioid agonist treatment (buprenorphine), and opioid antagonist treatment (naltrexone). Ultimately, we excluded studies that examined only the use of naltrexone because of different pharmacodynamics (competitive antagonist vs. μ-opioid receptor binding) and reasonable concerns that study participants who are willing to be treated with naltrexone – despite its low acceptance – could exhibit different characteristics (external validity concerns; also see Di Paola et al. 18 ). Also, we strived to keep heterogeneity as low as possible, thus the inclusion of a different treatment and a potential different population seemed ill-advised. Studies on any medication-assisted treatment for the sole purpose of detoxification were excluded.
Outcomes included the use of illegal drugs, treatment engagement post-release as well as re-incarceration. Records were initially screened based on title and abstract, in the further course of the selection process full-text articles were assessed for eligibility criteria (see Figure 1). The meta-analysis was preregistered at AsPredicted.org. Finally, N = 15 studies met the eligibility criteria and were therefore included in the present meta-analysis (see Online Supplement A). The integrated studies19–33 are marked in the bibliography (*).
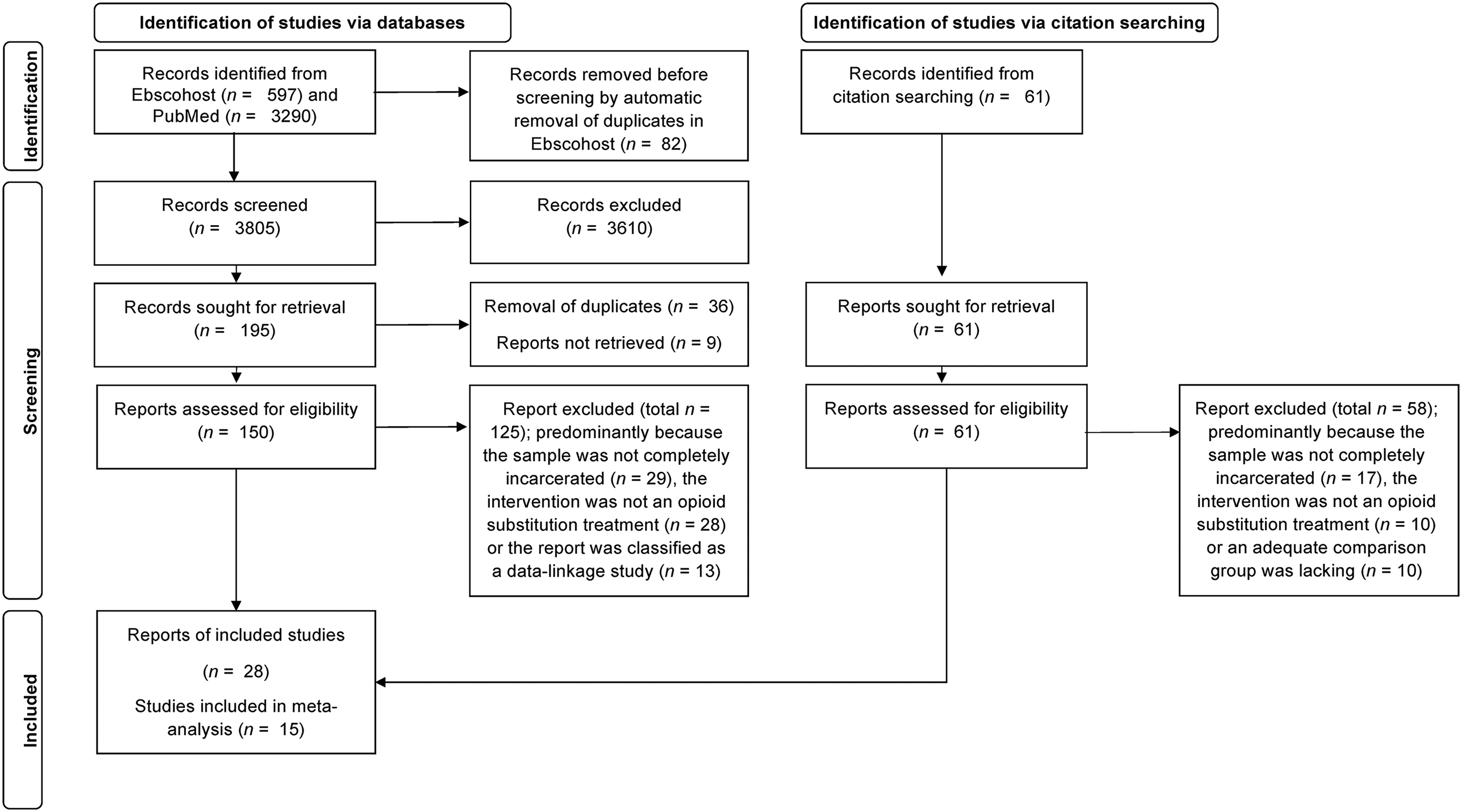
PRISMA flow diagram. The diagram represents the selection process that resulted in N = 15 studies included in the meta-analysis.
Data extraction and management
We constructed a coding sheet to record study information. Each study was coded by two researchers independently, compared, and any differences were discussed until consensus was reached. Extracted data included general information (e.g. publication year), study characteristics (e.g. study design), population characteristics (e.g. sample size), type of intervention (e.g. type of medication used in experimental and comparison group), type of analysis (intent-to-treat vs. as-treated), and evaluation of results (e.g. examination of group differences). Furthermore, outcome variables (illegal opioid and other drug use, engagement in treatment post-release, re-incarceration) were extracted. Data were entered and processed in IBM SPSS Statistics 26 (www.ibm.com) and JASP 0.16.2 (www.jasp-stats.org).
Measures of treatment effect
As most studies used dichotomous outcomes (e.g. opioid use yes/no), odds ratios were computed. For metric outcomes, effect sizes were converted into odds ratios. Where data were missing (i.e. odds ratios were reported without standard error) the missing value was imputed by mean substitution of comparable outcome variables. Odds ratios > 1.00 represent a benefit for the treated group, whereas odds ratios < 1.00 demonstrate a benefit for the comparison group. After conversion into log-odds, outcome variables were aggregated into four main categories: opioid use, other drug use (e.g. alcohol, cannabis, cocaine), treatment engagement post-release (retention/engagement in OST, inpatient/outpatient treatment, self-help program), and re-incarceration. Health-related outcome variables (e.g. HIV viral suppression, overdose, syringe sharing) were considered, but ultimately, we decided against the inclusion as the variables were diverse.
Studies reported follow-up data at different time points; we categorised follow-up periods as short (≤3 months after release), middle (3–6 months after release) and long (≥6 months after release). When more than one measurement fell into a follow-up period (e.g. 1-month and 3-month follow-up), the latest available time point was used. For the following analyses, the longest interval after release was used to assess the viability of each treatment in the long term.
Data analysis
Random effects models of the four main dependent variables were computed following the maximum likelihood procedure. Funnel plots and rank correlation tests for funnel plot asymmetry were assessed for empirical signs of bias. Additionally, a file-drawer analysis was used to assess the robustness of the effect. As there was concern regarding publication bias, an additional meta-analysis was performed with robust selection models. Different modes of analysis are recommended to ascertain the stability of effect. 34 When using robust selection models, log-odds were transformed into d effects sizes. Significance level for testing publication bias was set to α = .10 as is recommended for these types of tests. 34 For all other tests the levels were set to α = .05. In order to assess the influence of methodological differences on effect size, we conducted moderator analyses of length of follow-up and randomisation on all outcome variables. Due to small sample size, we refrained from conducting more extensive moderator analyses, for example, on treatment or sample variables.
Results
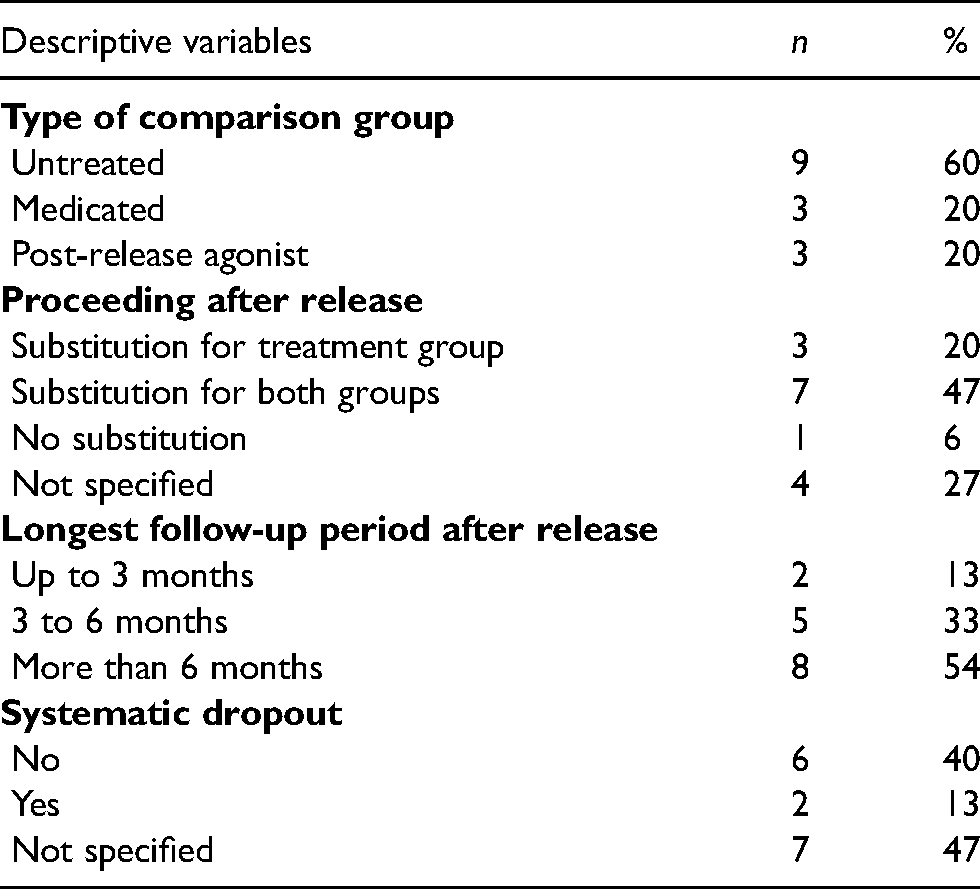
The N = 15 studies included in this meta-analysis were published between 1993 and 2020 (only one published before 2000) in journals (all except one peer-reviewed). The majority (n = 12) of the studies were carried out in the U.S., the remainder were in Norway (n = 1), Canada (n = 1) and Australia (n = 1). Sample sizes ranged from 44 to 589 subjects (M = 244.07; SD = 184.36). The mean age of subjects was M = 35.97 years (SD = 3.93). The mean percentage of women was M = 16.52% (SD = 15.68). Five studies included only male subjects, n = 10 studies included mixed samples, and no studies included only female subjects. More than half of the studies (60%) were randomised controlled trials. Most of the studies were carried out in prisons (n = 9), while n = 5 studies examined samples in jails and n = 1 study in both types of detention facility. The majority (n = 10) received methadone as substitution treatment, the rest received buprenorphine (n = 4) and levo-alpha-acetylmethadol (n = 1). Regarding baseline differences between treatment and comparison group, most studies (n = 8) reported no differences between groups, two studies reported minor differences and in five studies the group were non-equivalent. Tables 1 and 2 display additional characteristics. Figures 2(a)–(d) show forest plots for the outcome variables (opioid use, other drug use, treatment engagement post-release and re-incarceration) at the latest follow-up measurement.
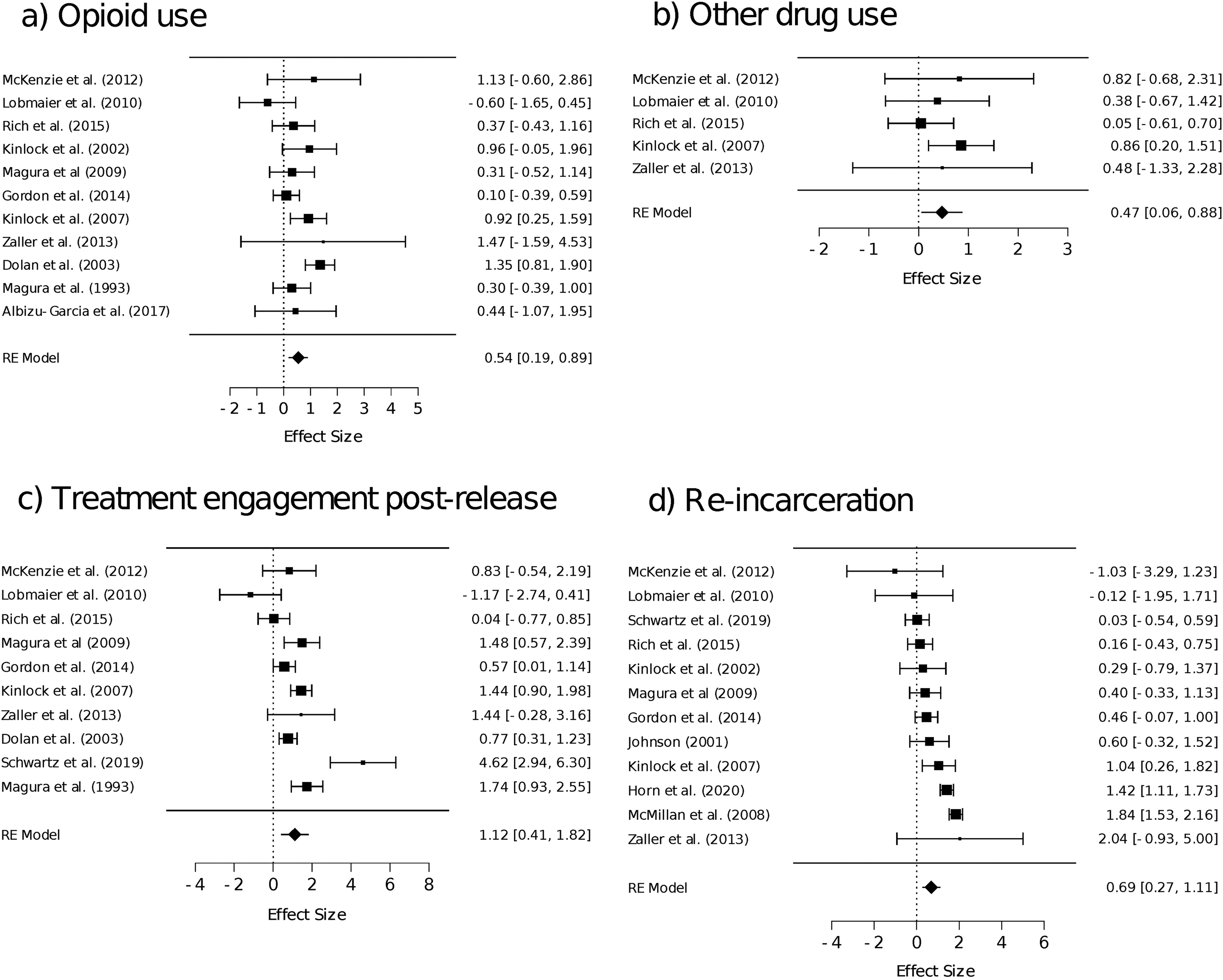
Forest plots of the different outcome variables, effect sizes in log-odds. (a) Opioid use, (b) Other drug use, (c) Treatment engagement post-release, and (d) Re-incarceration.
Descriptive characteristics of interventions (categorial variables, N = 15).
Descriptive characteristics of metric variables (N = 15).
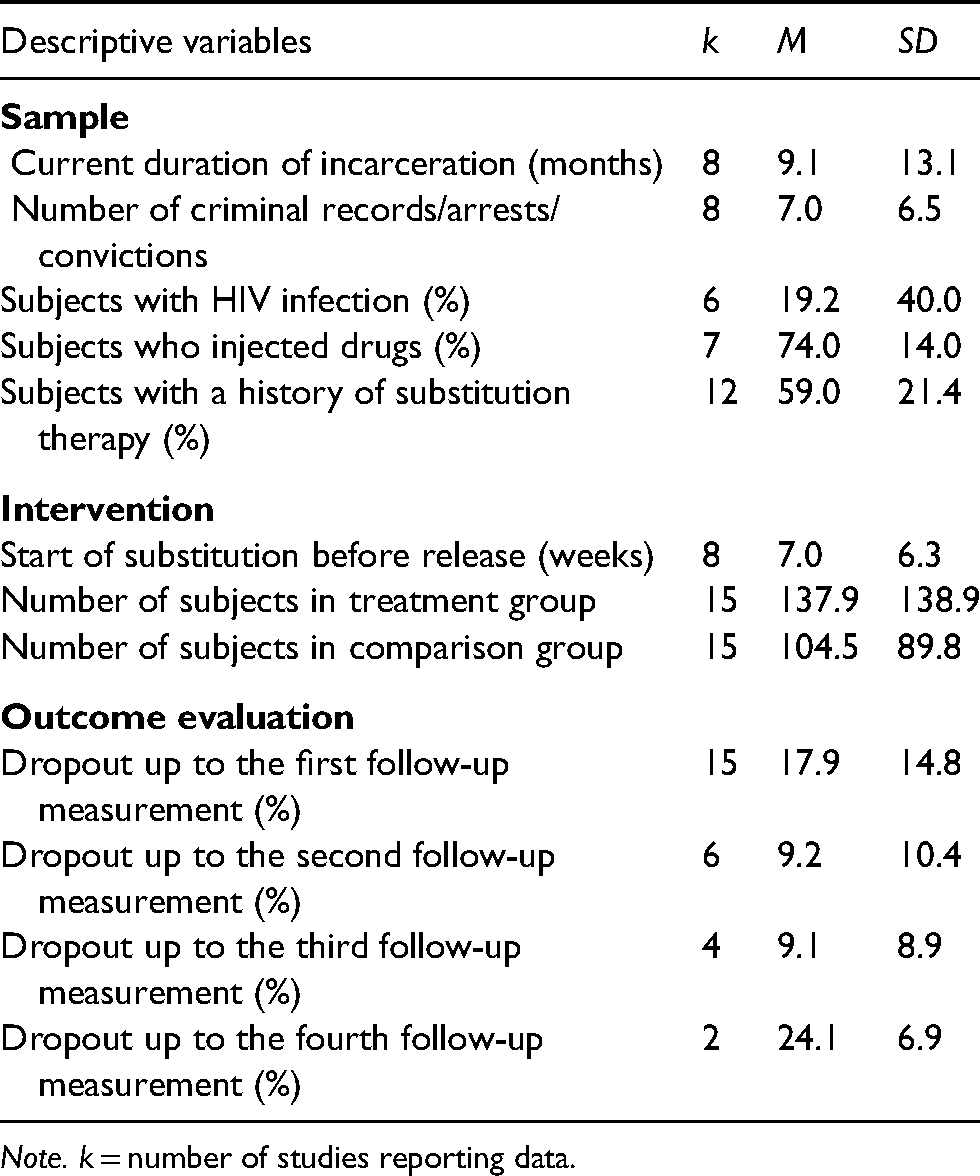
Note. k = number of studies reporting data.
Opioid use
Eleven studies (see Figure 2(a)) examined opioid use (total N = 2036). Participants treated with OST were more likely to stay clean from illegal opioids after release than participants in the comparison group (OR = 1.72, 95% CI = 1.19–2.49, p = .004, Q = 19.95, p = .03, I2 = 49.93). In the classical meta-analysis, there was no evidence of bias (τ = 0.018, p = 1.00). Selection models showed significant heterogeneity (Q = 19.96, p = .04) with indication of publication bias (χ2 = 3.40, p = .06) resulting in adjusted random effects estimate of OR = 2.43 (95% CI = 1.51–3.93, p < .001). A robustness test showed that a Fail-Safe N of 62 additional studies with a zero effect would be necessary to raise the significance over the .05 threshold.
Other drug use
Five studies (see Figure 2(b)) reported other drug use (total N = 674). Treated subjects refrained significantly more often from using other drugs than individuals in the comparison group (OR = 1.60, 95% CI = 1.01–2.54, p = .044, Q = 3.162, p = .531, I2 = 16.78). There was no evidence of bias (τ = 0.00, p = 1.00), and a robustness test showed that a Fail-Safe N of five additional studies without a significant effect would be needed to cross the significance threshold. There were not enough studies for a robust analysis.
Treatment engagement post-release
Ten studies (see Figure 2(c)) examined treatment engagement after release (total N = 2293). Treatment engagement post-release was positively affected by treatment status during incarceration. Treated participants were more likely to be engaged in treatment after release than participants in the comparison group (OR = 3.00, 95% CI = 1.55–5.78, p < .001, Q = 40.749, p < .001, I2 = 86.65). There was no evidence of bias (τ = 0.018, p = 1.00). Selection models showed significant heterogeneity (Q = 40.71. p < .001) but no indication of publication bias (χ2 = 0.414, p = .52), leading to a robust estimate of OR = 3.05 (95%-CI = 1.51–6.17, p = .002). The robustness test showed that a Fail-Safe N of 282 studies would be needed to invalidate this significance.
Re-incarceration
Twelve studies (see Figure 2(d)) assessed re-incarceration after release (total N = 2788). The treatment group was significantly less likely to have been re-incarcerated than the comparison group (OR = 1.98, 95% CI = 1.28–3.05, p = .002, Q = 66.89, p < .001, I2 = 79.12). In the classical meta-analysis, there was no evidence for bias (τ = 0.061, p = .84), with a Fail-Safe N of 291. Selection models showed a high heterogeneity (Q = 66.87, p < .001) with indication of publication bias (χ2 = 3.93, p = .047) leading to adjusted random effects estimate of OR = 3.13 (95% CI = 1.91–5.10, p < .001).
Moderator analysis
As meta-analytic integration showed high heterogeneity in study results, moderator analyses seemed appropriate. As our study base was too small to consider extensive moderator analyses, we restricted our moderator analyses to the two most relevant methodological aspects: Length of follow-up and randomisation. The length of follow-up appeared to be a significant moderator (see Table 3) when analysing the effect on opioid use and treatment engagement post-release, to the extent that effects diminished with length of follow-up. Descriptively, the effect also exists with re-incarceration; unfortunately, there was no study on re-incarceration that provided data for a long follow-up period. Regarding the study design (randomised controlled trial vs. observational/quasi-experimental design) as a moderator, it appeared that there was no effect on opioid use and treatment engagement post-release (see Table 3). However, there was a strong significant moderation effect of study design on re-incarceration, randomised studies reported a smaller benefit for the treatment group.
Moderators ‘length of follow-up’ and ‘randomisation’ for outcome variables opioid use, treatment engagement post-release and re-incarceration.
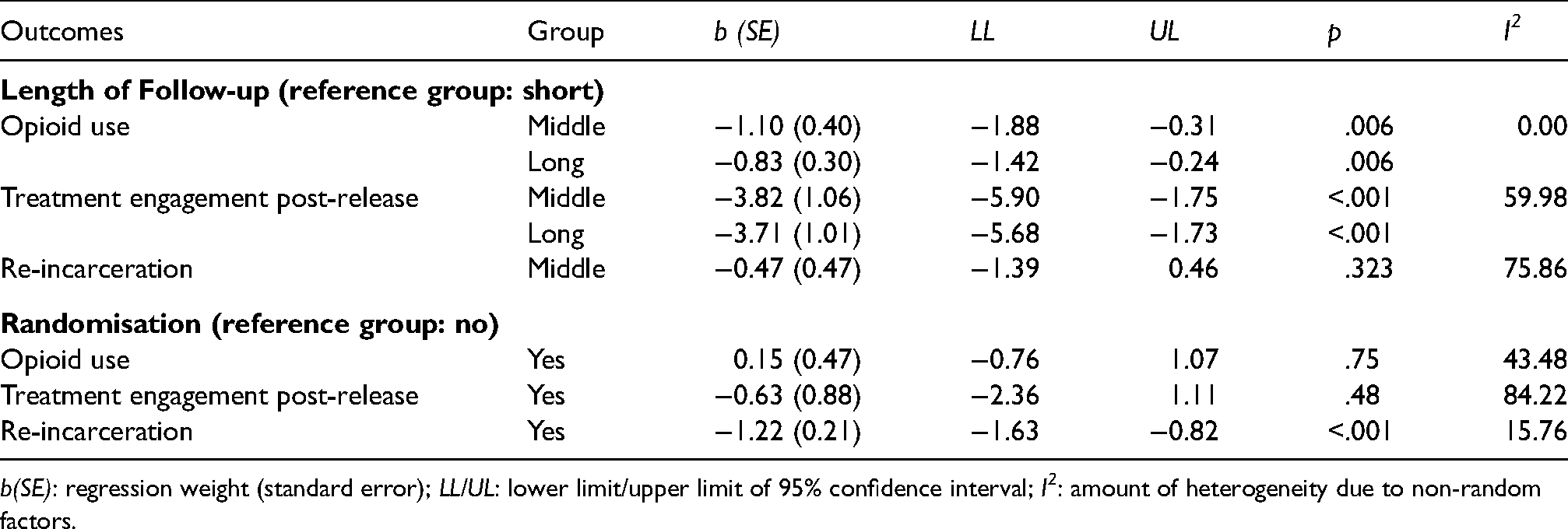
b(SE): regression weight (standard error); LL/UL: lower limit/upper limit of 95% confidence interval; I2: amount of heterogeneity due to non-random factors.
Discussion
The results of our meta-analysis show – in line with previous results – that OST during incarceration leads to significantly higher treatment engagement post-release and significantly reduces opioid use and other drug use after release. Furthermore, a significant effect of OST on re-incarceration was observed in the present meta-analysis, whereas Moore et al. 8 found no effect on legal recidivism. Moderator analyses showed some influence of length of follow-up period on opioid use and treatment engagement post-release: As could be expected, longer follow-up periods led to smaller treatment effects. The effect of OST thus decreases over time. The influence of study design (randomisation vs. no randomisation) was not significant concerning most outcomes, justifying our decision to include quasi-experimental and observational studies in addition to RCTs. Regarding re-incarceration, however, it appeared that in RCTs the treated group benefited less from OST. We had planned analyses on other secondary outcomes (e.g. health-related outcomes, employment, housing status), but data were insufficient.
Originally, we aimed to shed more light on the situation in European countries, since differences in the judicial and social systems limit comparability with U.S. studies. However, despite a broad search and comparatively ‘open’ search criteria (e.g. in contrast to Moore et al. 8 no restriction to randomised controlled trials), only one European study was found. Nevertheless, this paper includes studies from other countries than the U.S., thus broadening the perspective of incarceration-based OST compared to Moore et al. 8 We were able to include studies which were excluded in the meta-analysis by Moore et al. 8 because they were quasi-experimental. Integrating RCTs, quasi-experimental and observational studies in meta-analysis is controversial; however, our data show that study design had little influence on the effects. Especially in the field of incarceration-based OST, randomised group assignment is difficult to achieve due to ethical restrictions. Only including RCTs in a meta-analysis on this topic would therefore increase internal validity, but severely reduce external validity. Furthermore, n = 11 additional studies were incorporated in the meta-analysis due to the different inclusion criteria (including studies on buprenorphine treatment) and longer time span of inclusion (December 2017 vs. July 2020), thus strengthening and expanding the findings of the previous meta-analysis by Moore et al. 8
Limitations
There are several limitations to the present meta-analysis. As noted earlier, most studies we included were conducted in the U.S, where the judicial and health system differs from other countries in many ways (e.g. punitivity), which makes generalisation difficult. There was heterogeneity in our data, which presented a familiar problem in meta-analyses, known as the danger of ‘comparing apples with oranges’. However, our aim was to present a picture that is as comprehensive as possible. Although the number of scientific publications related to incarceration-based OST is increasing, we only found N = 15 relevant studies. Given the limited number of studies, results must be interpreted with caution. Furthermore, as we were particularly interested in the long-term effects of OST, we used data only from the last follow-up, which represents a conservative estimate and may have led to an underestimation of effects (e.g. continued OST is necessary to retain beneficial effects on mortality 35 ). In addition, due to insufficient data, we were unable to consider the dose of the administered medication, although this may have been relevant.36,37 However, individualised medical treatment was at the physician's discretion and, therefore, dose was not standardised and dose-response analyses could not be completed.
There were no signs for bias for the variables opioid and other drug use. For treatment engagement post-release and re-incarceration, there was evidence for publication bias. Even with adjustment for bias, the effect sizes stayed significant. Nevertheless, any causal relationships should be interpreted with caution.
Research prospects
We excluded studies (n = 4) using antagonist treatment (naltrexone) during incarceration, as their inclusion would have increased heterogeneity even further. Although we had good reasons to exclude these studies, it is an important topic for future research. Differing from the narrative review from Moore et al., 8 we excluded data linkage studies on incarceration-based OST (n = 13), due to significant differences in the methodology. These studies also contribute in-depth information about the effectiveness of incarceration-based OST and will be evaluated and reported in a separate paper.
Conclusion
We integrated data from N = 15 studies on the effects of incarceration-based OST. Participants treated with OST during incarceration had significantly higher rates of treatment engagement post-release and significantly lower rates of illegal drug use after release than individuals in the comparison group. Further, study participants treated with OST were significantly less likely to be re-incarcerated than participants in the comparison group.
Despite positive results, the effects were moderate, suggesting that other treatment or participation characteristics may play a role in drug use, treatment engagement and criminal relapse after release from incarceration. A comprehensive set of approaches in the treatment of incarcerated individuals who use opioids as well as in the evaluation of incarceration-based OST is needed. 11
There are major differences around the world regarding the number of people incarcerated, prevalence of incarcerated individuals who use opioids, and access to OST. Unfortunately, the topic has not yet received much research attention in Europe. However, partially because of lawsuits from individuals who demand equivalent medical treatment in correctional facilities,4,38 availability of OST for incarcerated people in Europe has the potential to improve in the near future. These changes, especially in Europe, offer chances for naturalistic experiments and should be accompanied by extensive research.
Supplemental Material
sj-docx-1-msl-10.1177_00258024221118971 - Supplemental material for A meta-analysis on the effects of incarceration-based opioid substitution treatment
Supplemental material, sj-docx-1-msl-10.1177_00258024221118971 for A meta-analysis on the effects of incarceration-based opioid substitution treatment by K. Boksán, M. Dechant, M. Weiss, A. Hellwig and M. Stemmler in Medicine, Science and the Law
Footnotes
Acknowledgements
This work was supported by the Bavarian State Ministry of Justice and is part of an ongoing research project regarding incarceration-based opioid substitution.
Authors’ note
K.B. and M.D. share first authorship equally. Geological information: Erlangen, Germany. The data is available on request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bavarian State Ministry of Justice.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.