
Abstract
Asbestos exposure is a well-established cause of malignant mesothelioma and other respiratory diseases, and quantifying inorganic fiber lung burden is crucial in forensic and medico-legal contexts for attributing disease causality. However, data on background asbestos exposure and chronological trends in the general population remain limited. This study analyzed autopsy lung tissue samples from 81 individuals (38 males, 43 females) from Northern Italy who died between 2001 and 2024, all with no documented history of occupational or environmental asbestos exposure. Inorganic fibers, including asbestos and nonasbestos types, were counted and characterized using scanning electron microscopy with energy dispersive spectroscopy, and concentrations were normalized per gram of dry lung tissue. Asbestos fibers were detected in 22.2% of cases, predominantly tremolite/actinolite, with higher concentrations observed in males. Ferruginous bodies were present in 17.3% of samples. Notably, asbestos lung content demonstrated a significant decline over time: only 9.5% of individuals born after 1946 had detectable asbestos fibers, compared to 35.9% of those born before 1946 (p < 0.05). Nonasbestos fibers, mainly talc, other phyllosilicates, and titanium dioxide, were also identified but did not show clear chronological trends. These findings indicate a marked decrease in asbestos lung burden in the general population, likely reflecting the effectiveness of asbestos bans. Current background levels are substantially lower than historical thresholds used for disease attribution, highlighting the need to revise reference values to ensure accurate causal attribution of asbestos-related diseases in forensic practice.
Introduction
Malignant mesothelioma (MM) is a fatal neoplasm with a well-established association to prior asbestos exposure, whether occupational or nonoccupational in nature.
1
In forensic and medico-legal practice, the determination of a causal relationship between MM and asbestos exposure often hinges on the quantification of fiber burden in lung tissue. Despite ongoing research into MM pathogenesis, the definition of a precise “threshold dose” of asbestos that significantly elevates disease risk remains unresolved.
2
Asbestos and other asbestiform minerals—some of which are not formally classified as asbestos but are nonetheless implicated in mesothelioma and other malignancies—are pervasive in both urban and natural environments. Consequently, virtually all individuals experience some degree of lifelong exposure, resulting in the potential accumulation of asbestos or other hazardous fibers in pulmonary tissue. However, forensic practitioners face a notable gap in the literature regarding the quantification of this so-called “background exposure.” Carbone et al. have proposed that a lung asbestos concentration below 500,000 ff/gdw may be considered within the background range.
2
The “Helsinki criteria,” published in 1997 and updated in 2014, provide reference thresholds for lung asbestos content, as determined by electron microscopy, to support causal attribution in disease investigations.3,4
over 0.1 million amphibole fibers (>5 μm) per gram of dry lung tissue or over 1 million amphibole fibers (>1 μm) per gram of dry tissue as measured by electron microscopy in a qualified laboratory.
Importantly, these guidelines recommend that each laboratory establish its own reference values, underscoring the absence of universally accepted cutoff concentrations for asbestos content. The Helsinki criteria have been subject to significant critique within forensic and scientific communities.
5
Key concerns include:
Heavy reliance on exposure history for causal attribution, which may be incomplete or unknown, especially in cases of environmental or anthropogenic exposure from widespread asbestos-containing materials. Lack of standardized methodologies across laboratories. The use of an outdated and limited control cohort (19 individuals from North Carolina, deceased between 1980 and 1995) to establish the background threshold of 100,000 ff/gdw.
6
Studies assessing inorganic fiber lung burden in the general population are scarce. Some have directly measured asbestos lung content in the general population,7–12 while others included individuals from the general population who served as controls for mesothelioma cases in case-control studies.6,13–23 With the exception of two recent Italian studies,12,23 most investigations focus on individuals who died in the 1960s–1980s, a period of widespread asbestos use. These older studies often report high asbestos concentrations (frequently above 100,000 ff/gdw), and their subjects may not be fully representative of the general population due to possible unrecognized exposures and the inclusion of cancer decedents. Furthermore, most did not assess nonasbestos inorganic fibers.
Only two studies, both carried out in Italy, investigated the asbestos burden in lung tissue of the general population after the asbestos ban. Casali et al. assessed lung content in people from Milan who died between 2009 and 2011, and found asbestos in 63.6% of the subjects. In this study not only asbestos, but also fibrous talc and titanium-rich fibers were detected. Asbestos was above 100,000 in only five out of 55 subjects. 12 Our group analyzed 50 individuals from the general population who were controls in a case–control study on mesothelioma, 23 and detected asbestos in 28% of them, in concentrations always below 100,000 ff/gdw. Data about nonasbestos inorganic fibers were not reported.
This literature review highlights a critical lack of recent data on inorganic lung fiber content in the general population—data that are essential for establishing forensic reference values for “background exposure” in disease attribution.
Another matter of forensic relevance is the chronological trend in asbestos exposure. Roggli et al. 24 documented a progressive decline in asbestos lung content among MM patients over the past four decades, a trend confirmed by our group. 23
Asbestos bodies (AB) may also be present in lung tissue. They are asbestos fibers covered with an amorphous substance, mainly composed of iron and proteins. 25 The coating process results from the failed attempt of the immune system to phagocyte the fiber (frustrated phagocytosis). 26 Asbestos fibers are, in fact, mostly too long to be engulfed by macrophages. Asbestos fibers are not the only fibers that can be coated, as some corpuscles appearing as AB were found to have a nonasbestos core. Therefore, if we are unable to assess the nature of the core fiber, it is more correct to refer to such corpuscles as ferruginous bodies (FB). FB can also be observed at light microscopy after proper preparation of the lung tissue and even in histologic sections. Even though the concentration of FB cannot be regarded as informative about the asbestos lung content, 27 Helsinki criteria provide a threshold value for AB as well: according to the authors, over 1000 AB/gdw are indicative of a past exposure to asbestos. 4 However, similar to asbestos fibers, there is a lack of data on FB content in the general population.
The primary objective of this study is to quantify asbestos in lung tissue from healthy individuals in the general population of Northern Italy and to assess whether asbestos exposure has changed over recent decades (noting that asbestos was banned in Italy in 1992). A secondary aim is to characterize the type and concentration of other inorganic fibers present in the lungs of healthy subjects.
Methods
This study was carried out on lung samples taken during autopsy from healthy individuals deceased between 2001 and 2024 from traumatic causes, according to the following criteria: age above 40 years; no medical history or pathologic evidence of neoplastic or respiratory disease; negative known history for occupational, household or environmental asbestos exposure. In each case, a complete forensic autopsy was performed, followed by routine histopathological examination (which includes the observation of Hematoxylin-Eosin slides of brain, heart, lungs, spleen, liver, and kidneys).
The following variables were extracted from the archive of our Forensic Medicine Department: age at death, sex, year of birth, and year of death.
The preparation procedure is the same we already described, 28 according to the protocol by Belluso and coworkers. 29 In brief, the formalin-fixed lung samples were put in 13% sodium hypochlorite for 72 h in a stove set at 60°C in order to eliminate any organic matter. Then the solution is filtered through a mixed-cellulose ester membrane (Millipore, Darmstadt, Germany) with a diameter of 25 mm and a pore size of 0.45 µm. The membrane was dehydrated and pasted on a pin-stub using a carbon tape and examined by SEM. While the preparation of samples was performed in the same laboratory, the observations were carried out in two different laboratories (Pavia and Torino) using, respectively, a COXEM EM-30 and a JEOL JSM IT300LV, both coupled with EDS Oxford INCA Energy 200 equipped with INCA X-act SDD thin window detector (Oxford Instruments NanoAnalysis, Bucks, UK). Samples were distributed equally between the two laboratories. In order to minimize possible bias due to different instruments and microscopists, the same observation protocol was strictly followed and a periodic inter-laboratory control was made, comparing images and spectra obtained. In addition, ten samples were analyzed by both observers (BB and SC), revealing homogeneous measurements. 23
The observation was performed on an area of 2 mm2 of filter at 4000 M using backscattered electrons. All inorganic fibers with parallel long sides, width <3 µm and a length-to-width ratio >3 were considered, according to regulation and guidelines. Specifically, WHO defines a fiber as “biologically more important, so-called “critical” fiber” based on the following dimensional characteristics: length ≥ 5 µm, diameter ≤ 3 µm, and length/diameter ratio ≥ 3. 30 The Italian law31,32 defines “respirable fibers” as fibers longer than 5 µm, thinner than 3 µm, having a length/diameter ratio greater than 3. Inorganic fibers thus defined with respect to their size will be overall referred to as “regulated fibers.” Fibers shorter than 5 µm were considered separately because they do not fulfill the above-mentioned criteria for fiber definition. FBs were also counted.
Each observed inorganic fiber was identified according to its morphologic appearance and EDS spectrum compared with a database internal to our laboratory.
Since the technique here used does not allow unequivocal identification of certain minerals having similar chemical composition and analogous morphology, it is not possible to distinguish chrysotile from asbestiform antigorite and tremolite asbestos from actinolite asbestos. Therefore, we used, respectively, the following mineral group names: chrysotile/asbestiform antigorite and tremolite/actinolite asbestos.
We identified the following categories: inosilicates belonging to amphiboles, subgrouped as asbestos (crocidolite, amosite, anthophyllite asbestos, and tremolite/actinolite asbestos), hornblende and other inosilicates; phyllosilicates (chrysotile/asbestiform antigorite, talc and other phyllosilicates), silicon dioxide (SiO2), and titanium dioxide (TiO2).
The number of detected inorganic fibers and FB were normalized to 1 g of dry tissue (ff/gdw and FB/gdw), reporting concentration in terms of the burden of inorganic fibers and FB per gram of dry lung tissue weight: ff/gdw.
The endpoints of the SEM-EDS analysis were the following: concentration and mean and length of all inorganic fibers of each category, extrapolating that of each asbestos type, and concentration of FBs.
The detection limit (DL) for this technique is 1000 ff/gdw.
The study protocol was approved by the Ethical Committee “Lombardia 6” on 22nd August 2023. The informed consent was waived because the participants are deceased subjects and relative are no longer reachable. Only biological material retrieved from our archive, collected at the time of autopsy for forensic and diagnostic purposes, was used for this study.
Results
Asbestos lung concentration was determined in lung samples obtained from 81 deceased people (38 females, 43 males) selected according to the above-mentioned criteria in Northern Italy, where asbestos was banned in 1992. The place of residence of each individual was mapped in Figure 1. Their mean age was 68.8 years (SD +12 years).

The residence map of the analyzed individuals.
Asbestos was detected in 22.2% of them, while FB in 17.3%. The concentration of asbestos ranged between 0 (i.e., under the DL) and 61,000 ff/gdw (M = 3354.8 ff/gdw). The concentration of FB ranged between 0 (i.e., under the DL) and 30,600 FB/gdw (M = 1658.6 FB/gdw). Chrysotile was detected in three cases (3.7%), tremolite/actinolite asbestos in 14 cases (17.3%); amosite and anthophyllite asbestos were detected in two cases each (2.5%). Crocidolite was never detected.
Average asbestos content was 4017.4 ff/gdw (SD = 9512.608) in males and 1184.5 ff/gdw in females (SD = 2780.73). FB were 2528.3 FB/gdw (SD = 6902.64) in males, and 2200.8 FB/gdw (SD = 9963.32) in females.
The chronological trends of both asbestos and FB lung content, in relation to the year of birth, were similar in males and females (Figure 2), but show a dramatic change in subjects born on or after 1946 independently from sex (Figure 3).
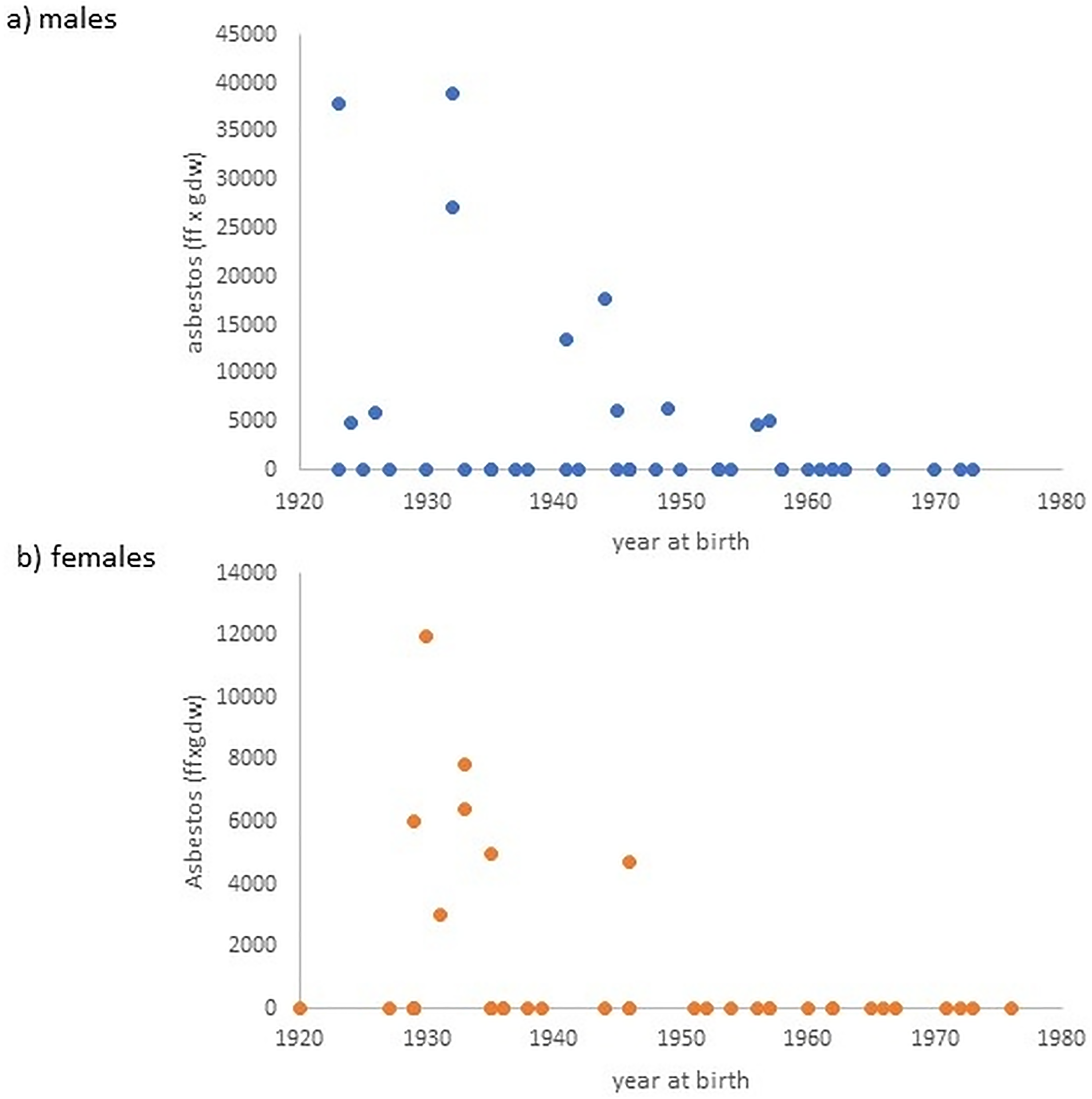
Time trends of asbestos concentrations plotted according to the year of birth. (a) Males and (b) females.
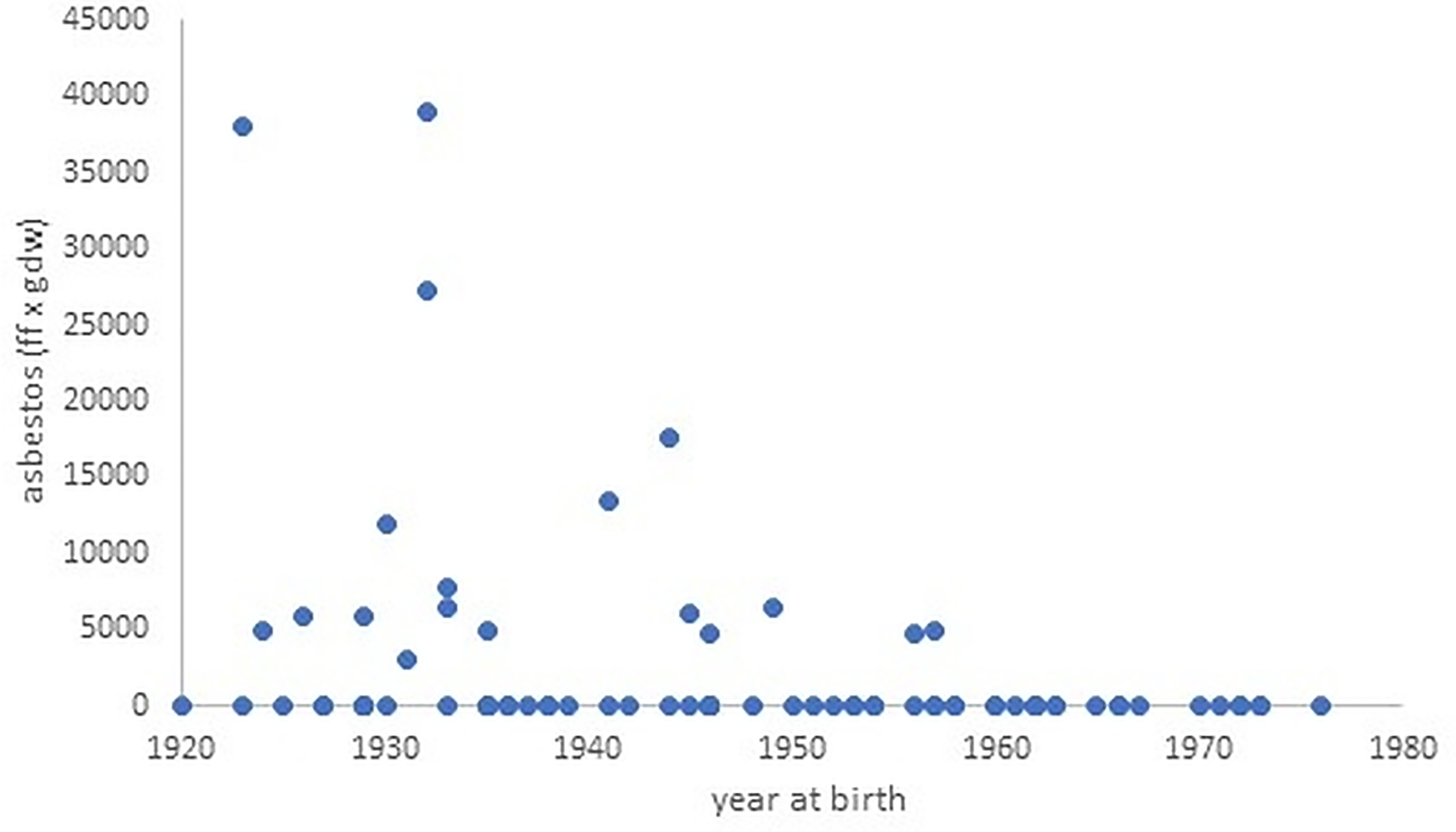
Time trends of asbestos concentrations plotted according to the year of birth (males and females).
Asbestos was present in lungs of 14/39 (35.9%) subjects born before 1946 versus 4/42 (9.5%) subjects born on or after 1946 (Fisher exact test = 0.0002, p < 0.05; Figure 2). FB were present in 13/39 (33.3%) and 1/42 (2.4%) subjects, respectively (Fisher exact test = 0.0012, p < 0.05). Similar results were also observed considering only tremolite/actinolite asbestos.
Moreover, in people born before 1946 both chrysotile and tremolite/actinolite asbestos (noncommercial asbestos) were detected, whereas in those born after 1946 we observed only tremolite/actinolite asbestos (noncommercial asbestos) in almost the totality of cases, whereas amosite and anthophyllite asbestos (both commercial asbestos) were observed in only one case. Finally, the concentration of asbestos showed an increasing trend according to age at death. Individuals with asbestos in lungs died between 68 and 90 years old (Figure 3). Asbestos was not found in individuals whose age at death was less than 68 years.
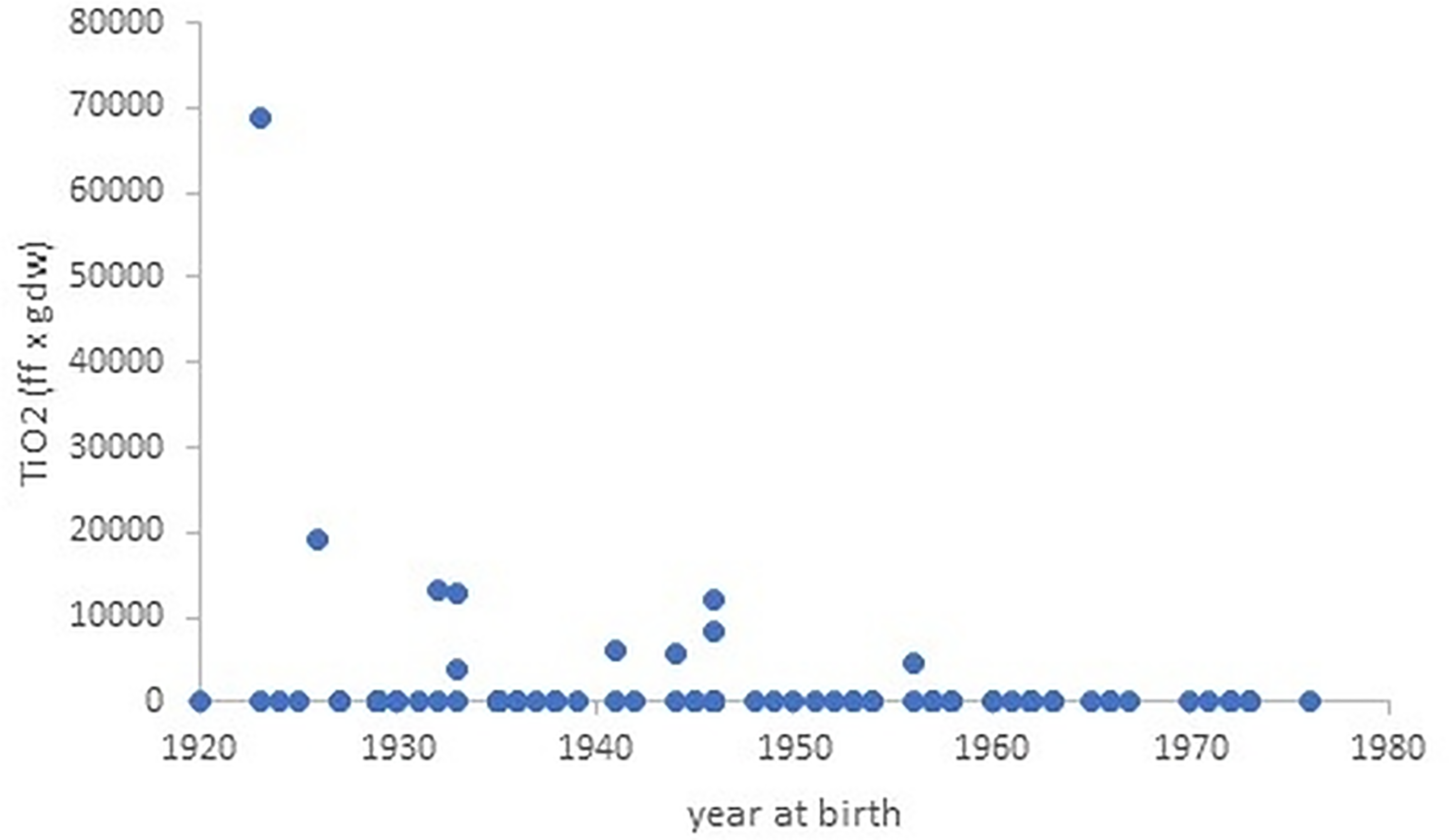
Time trends of TiO2 concentrations plotted according to the year of birth.
The length of asbestos fibers was not significantly different in people born on or after 1946 versus people born before 1946 (23.35 vs. 19.72 μm). Fibers shorter than 5 µm showing an EDS spectrum compatible with asbestos were classified separately and labeled as “short.” Short fibers with EDS spectrum compatible with chrysotile were detected only in 1 subject, whereas short tremolite/actinolite fibers were detected in five individuals, all born before 1946.
Nonasbestos inorganic fibers: in the present series we identified phyllosilicates (subgrouped as talc or others), inosilicates, SiO2, and TiO2 (in descending order). The most represented inorganic fibers were TiO2, talc, and other phyllosilicates. TiO2 fibers (regulated or short) were detected in 17 subjects, 11 of which were born before 1946 (Figure 4). The concentration of TiO2 fibers longer than 5 µm ranged between 0 (under the DL) and 69,000 ff/gdw (M = 2343 ff/gdw). The concentration of TiO2 showed a decreasing time trend according to the year of birth (Figure 4). Both talc and other phyllosilicates were observed in 15 out of 81 individuals (18.5%) (Figure 5) and did not show a decreasing trend according to the year of birth, but both were present in subjects born after 1946. The concentration of talc in lung tissue ranged between 0 (i.e., under DL) and 51,500 ff/gdw (M = 2760 ff/gdw), while the concentration of the other phyllosilicates ranged between 0 and 43,500 (M = 3330 ff/gdw). Inosilicates (subgrouped as hornblende and others) were detected in 5 subjects, in concentrations below 7650 ff/gdw. All the detected talc, other phyllosilicates, and hornblende fibers were longer than 5 µm.
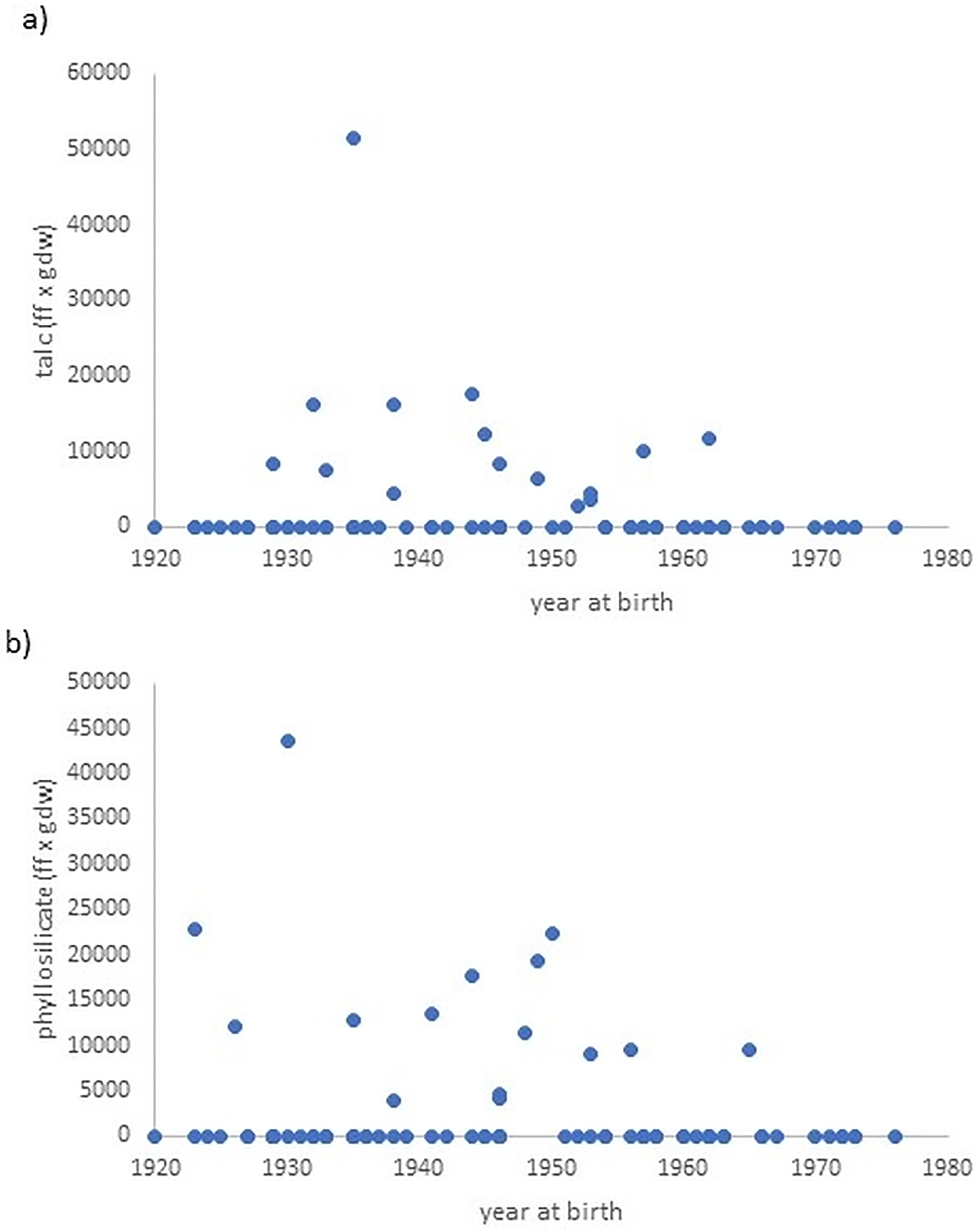
Time trends of fibrous talc (a) and other phyllosilicates (b) concentrations plotted according to the year of birth.
Discussion
In the present work, we analyzed the inorganic fiber lung burden in 81 deceased subjects from the general population of Northern Italy, and detected asbestos in 22% of them. The most represented type was tremolite/actinolite asbestos. Asbestos concentrations were significantly lower in females compared to males. The chronological trend of asbestos lung content shows a neat turning point represented by 1946: interestingly, we found asbestos in low concentrations in only 9.5% of the subjects born on or after that year. Besides asbestos, we found mainly TiO2, talcum and other phyllosilicates in lung tissue. These minerals did not show any clear chronological trend, being present in subjects born before and after 1946.
A possible limitation of this study is related to the potential geographic variability of the present measurements. Our study population derives from a restricted area of Northern Italy, and asbestos use, industrial activities, building materials and remediation policies have differed markedly across Italian regions and between countries, with later bans and prolonged use in some settings. In addition, it is difficult, in forensic settings, to systematically collect detailed residential information such as long-term residence in urban versus rural environments, which may influence cumulative background exposure through differences in traffic, industrial sources, and the density of asbestos-containing materials in place. These aspects limit the generalizability of the current results and suggest that dedicated studies in other geographic areas, explicitly comparing urban and rural settings with standardized analytical protocols, are warranted to determine how far the background lung asbestos burden observed in this Northern Italian series can be extrapolated to other populations.
Asbestos concentrations in lungs of this series of individuals from the general population are, overall, well below 100,000 ff/gdw, that is the threshold suggested by the Helsinki criteria for causal attribution of asbestos-related diseases. 4 Indeed, we found the maximum asbestos concentration of 39,000 ff/gdw, that is much lower than those found by the majority of studies on the general population. These results raise the question of whether the threshold of asbestos lung burden for causal attribution stated by the Helsinki criteria is still valid. Our findings suggest that the asbestos levels attributable to “background exposure” changed over time. In particular, in people born on or after 1946, asbestos concentrations in lung tissue were mostly below the detection limit. The present results suggest that the asbestos burden considered compatible with “background exposure” is currently likely to be lower than 100,000 ff/gdw. Moreover, if asbestos is found in lungs, even if below the threshold suggested by Helsinki criteria, the history of the subject should be carefully investigated in order to point out any previous exposure, even if the occupational history is negative. We believe, based on the present results and previous experience, that a negative assessment of asbestos lung content should not rule out previous exposure, but, if positive, it points out unknown or forgotten past exposures to be investigated through an accurate anamnesis. In fact, as shown by both our group33-35 lung clearance can hinder the correct evaluation of past exposure based on asbestos lung burden, especially for chrysotile.
On the other hand, in this series of individuals not exposed to asbestos, we found FB concentrations as high as 30,600 FB/gdw, with a mean FB concentration above the threshold suggested by Helsinki criteria (1000 AB/gdw). Other authors had previously suggested lower cutoffs: Roggli et al. considered a concentration below 20 AB per gram of wet lung (corresponding to 200 AB/gdw) as not indicative of previous asbestos exposure. 36 However, the same research group stated that AB can be found in the lungs of most people living in industrialized countries. 26 These data were obtained in the 70 s and 80 s, when asbestos was more diffused compared to today. More recently, Casali et al., investigating a series of 55 individuals from the general population of Milan deceased between 2009 and 2011, found AB in 16.4% of them, ranging from 10 to 110 AB/gdw. 12 Besides, it is not known if fibers other than asbestos, such as TiO2, currently widely used industrially, can form FB in human lungs.
In the interpretation of our results, we must underline that not all FB have an asbestos core, 37 and that quantifying FB using SEM-EDS rather than light microscopy tends to underestimate their concentrations, mainly because the amount of examined lung tissue is lower. However, compared to the above-cited previous studies, the FB concentrations observed in the present series are high, considering that we investigated the general population. Moreover, this data appears in contrast with the under-threshold concentrations of asbestos. The present results confirm the unreliability of FB concentration when determining past asbestos exposure, as previously pointed out by our group and others.27,38,39 Indeed, FB concentration is extremely variable and can be very different in subjects with identical asbestos exposure due to the different individual tendency to cover asbestos fibers.40,41 Moreover, the type and dimensions of fibers influence the efficiency of the covering process.42,43
In addition, our findings revealed a dramatic decrease of asbestos lung burden after 1946. This suggests a significant role of World War II (WWII), especially in males who, indeed, had mandatory draft. Asbestos-containing materials were largely used during WWII, for example for gas masks used by both the general population and soldiers.44,45 Besides, the use of asbestos as strategic material increased considerably during WWII (as tank cover, helmets, rockets etc.): the asbestos-containing materials used for such purposes were friable and easily air-dispersed. Therefore, during attacks to the cities and clashes a big amount of asbestos fires were air-dispersed and inhaled by the general populations. Moreover, bombing and other forms of military or terrorist actions provokes the destruction of buildings and the diffusion of asbestos-containing dust, as happened after the collapse of the World Trade Center towers on September 11, 2001. 46 This result points out the problem of asbestos exposure (both for professionals and the general population) related to wars and terrorist actions, which, unfortunately, we are still experiencing worldwide.
Most of the asbestos detected in the lung belonged to tremolite/actinolite asbestos (noncommercial amphiboles). Tremolite/actinolite asbestos is known to be naturally associated with other minerals, such as chrysotile (rarely) and talc (more often). It is difficult to determine if tremolite/actinolite asbestos was the result of the subject's exposure to chrysotile contaminated with tremolite/actinolite asbestos, due to chrysotile being rapidly cleared by the lungs and often not detected even if the person was exposed.33,47,48 However, tremolite/actinolite is generally more often associated with talc rather than chrysotile.
While chrysotile, being classified as asbestos, is banned in Europe (as in most developed countries), talc is widely used for manufacturing ceramics, paint, paper, plastics, rubber, roofing and cosmetics. 49 The terms “talc” and “talcum powder” are often used interchangeably, however talc is a naturally occurring substance mined for various commercial applications, talcum powder is a product made using talc as raw material. While tremolite/actinolite asbestos concentration in lungs follows a decreasing time trend according to the year of birth of the subject, talc did not show any clear chronological tendency, suggesting that talc exposure is still occurring. Talcum powder is currently used by the general population, therefore talc fibers are inhaled, as shown by the present data as well as by one of the few previous studies about inorganic lung content in the Italian general population. 12 Talc may not be dangerous by itself, but it can be contaminated by tremolite/actinolite asbestos. Talc from the Val Chisone (Piedmont region of Italy) was studied in 1972 by Pooley, who found amphibole asbestos contamination (tremolite and anthophyllite asbestos). However, more recent literature excluded the presence of asbestos in this area. 50
In previous literature, talcum powder exposure has been recognized as a source of asbestos exposure in women who died from mesothelioma without any known exposure.51,52 In a paper published in 2014, through multiple tests performed in three different laboratories, the authors found anthophyllite asbestos and tremolite asbestos in cosmetic talcum powder. 52 In the same work Gordon et al. analyzed with TEM-EDS lung tissue of a woman deceased from mesothelioma without any known exposure to asbestos but exposed to talcum powder and found tremolite asbestos and anthophyllite asbestos. 52 The hypothesis of an increased risk of developing mesothelioma as a consequence of talcum powder exposure is debated.53–55 However, the most recent epidemiological evidence from cosmetic talc miner/miller cohort studies did not confirm an increased risk of developing mesothelioma due to previous inhalation of cosmetic talc. 56 Ciocan et al. in 2022 published a study conducted on an Italian cohort of talcum miners and miller employed between 1946 and 1995 and reported no mesothelioma cases in the period of follow-up, nor an increased risk of lung cancer. 57
Other inorganic fibers detected in the studied population were phyllosilicates not ascribable to chrysotile nor to talc, found in lung tissue of 18.5% of the analyzed subjects. They belong to the mica group, a widely diffused mineral used in various products, such as for electrical insulation as well as in paints, pearlescent car paints, plastic materials, roofing, rubber and rubber products, textile and decorative coatings, well drilling mud, cement, in plasterboard, in balloons, in cosmetics. 58 It is, therefore, normal and expected to find mica in human lungs. The same can be stated for nonasbestos inosilicates and SiO2, found in, respectively, three and two subjects; there is no known pathological significance for these findings.
TiO2 was found in 12,3% of the investigated subjects and it did not show any clear time trend. TiO2 is generally considered as an inert material used for decades in paints, antiair pollutants, cosmetics (skincare and sunscreens), pharmaceuticals, surface protection, building energy-saving, etc. 59 Currently, TiO2 is widely used in the form of nanoparticles, rods, and nanorods: for instance, TiO2 nanoparticles (including ultrafine particles < 100 nm, and fine particles 0.1 to ca. 3 μm) are used as food additives. 60 A recent review suggested a possible risk associated with exposure to TiO2 nanoparticles, as they can induce oxidative stress and consequent inflammation, as well as apoptosis or chromosomal instability due to their genotoxic effect.60,61 These mechanisms have been observed in cell lines representative of alveolo-capillary barrier 62 and mesothelial cells. 63 Moreover, TiO2 is classified as Group 2B carcinogen (“possibly carcinogenic to humans”) by IARC. 64 However, there is a lack of recent data about the possible hazard of TiO2 for human health and more research is needed in this field.
From a forensic perspective, our findings demonstrate a substantial and progressive decline in asbestos lung content within the general population over recent decades. This trend strongly supports the effectiveness of regulatory measures, such as the ban on asbestos mining and use, in reducing population-level exposure, as already pointed out analyzing data from MM patients. 65 The predominance of noncommercial amphibole fibers, particularly those associated with talc products contaminated by tremolite asbestos, underscores the importance of considering environmental and nonoccupational sources in forensic investigations.
Crucially, our data provide, for the first time, evidence that World War II represents a significant historical breakpoint in asbestos exposure for the Italian general population, as reflected by lung fiber analysis. This insight is particularly relevant for forensic casework, where accurate reconstruction of exposure timelines is essential for disease attribution. Importantly, the current background asbestos burden in the lungs of individuals without known exposure is markedly lower than historical levels. This finding challenges the validity of existing reference thresholds for causal attribution, such as those outlined in the Helsinki criteria, which were established based on outdated and less representative control populations.
Forensic practitioners should therefore recognize that the lung asbestos content resulting from contemporary background exposure is significantly reduced compared to past decades. As a result, there is a compelling need to revise and update the criteria used for forensic attribution of asbestos-related diseases, ensuring they reflect current exposure realities and provide a more accurate basis for medico-legal judgments.
Footnotes
Ethical considerations
The study protocol was approved by the Ethical Committee “Lombardia 6” on 22nd August 2023 (Prot. No. 0043349/2b). As this is a retrospective study on histological preparations from autopsy specimens in subjects who were already deceased at the time of enrollment, it is not possible to obtain informed consent. Consequently, informed consent is not required under the “Provision containing prescriptions relating to the processing of particular categories of data, pursuant to Article 21, paragraph 1 of Legislative Decree no. 101 of 10 August 2018” (paragraph 5: Prescriptions relating to the processing of personal data carried out for scientific research purposes [General Authorization No. 9/2016]). Only biological material retrieved from our archive, collected at the time of autopsy for forensic and diagnostic purposes, was used for this study.
Authors’ contributions
Silvia D Visonà: conceptualization, methodology, investigation, data curation, formal analysis, writing—original draft, writing—review and editing, supervision, and project administration. Silvana Capella: methodology, investigation, resources, data curation, and writing—review and editing. Barbara Bertoglio: data curation, formal analysis, visualization, and writing—review and editing. Giovanni Cecchetto: investigation, resources, and writing—review and editing. Elena Belluso: methodology, resources, supervision, and writing—review and editing. Matthew Untalan: formal analysis and writing—review and editing. Emanuela Taioli: conceptualization, methodology, formal analysis, and writing—review and editing. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Guarantor of the study
Silvia D Visonà acts as the guarantor of this work and accepts full responsibility for the integrity of the study, had access to all the data, and controlled the decision to publish.