
Abstract
In child physical abuse cases, a clinical forensic medical examination (CFME) is performed to document medical evidence, such as lesions and scars. In Denmark, however, not all cases are referred by the police to a CFME, and we aimed to study the key characteristics of police reported cases of child physical abuse (N = 136, ages 4–17 years) – case context, the child's disclosure and sociodemographic factors – that could influence the police's selection process. Associations between case characteristics and CFME referrals were studied using univariate and multivariate logistic regression models, which were supported by age- and sex-matched conditional logistic regression models. CFME referrals were found to be less common for cases with children from a low socioeconomic status family or with previously reported concerns (such as a report to the social services), and more common when the violence endured by children involved punching/striking of limbs or left visible marks. Moreover, the number of victims in a sibship seemed to be associated with CFME referrals. Referrals were not influenced by parents’ origin or the suspect–child relationship. A biased referral process may lead to unequal case handling and undermine the rule of law. By identifying the characteristics relevant to this process, we aimed to contribute to a systematic and consistent approach to case management. Future qualitative interview studies with police officers and prosecutors and studies focused on larger populations can offer further valuable insights into the selection process.
Keywords
Introduction
Although it became explicitly prohibited by law in Denmark in 1997, 1 corporal punishment of children persists, with 16% of 14–15-year-old children experiencing it from a parent in the last year. 2 Worldwide, the estimated prevalence of violence faced by children from their parents is 17.3%; in Europe 12.7%. 3 Being exposed to such violence can cause cognitive, educational, mental and physical issues and even death. 4
Because many children are still exposed to physical violence, it is important that suspected cases are identified and examined carefully. In Denmark, the investigation procedures of a police reported child physical abuse case may include a video-recorded police interview with the child (VRI), which is a forensic interview designed to preserve the child's statement for the court hearing, 5 and a clinical forensic medical examination (CFME), which, performed by forensic medical doctors, document lesions and scars, and other signs of violence.6,7 The injury documentation works as evidence to facilitate the investigation and is also used in court, but a CFME is not conducted in every police-reported child physical abuse case.7–9 However, lack of corroborating evidence is one of the main arguments for closing child physical abuse cases before a court hearing. 10 In 2019, at Danish Child Advocacy Centres (CACs), CFME was conducted in only 2.3% of 1816 cases of physical and/or sexual abuse with children under 17 years as victims. 11 This low rate of referrals raises concerns about the consistency and transparency of the cases selected for CFME. Prematurely closing a case, before securing medical evidence, potentially increases the risk of further harm and long-term health consequences. Moreover, no published, structural guidelines exist in Denmark that clarify the CFME case selection process. 9
In Sweden, a CFME referral rate in police-reported child physical abuse cases has been reported to be 7%. Cases with younger children (less than three years of age) and cases with two suspected perpetrators were referred more often. 12 A multicentre study of four United States CACs found that cases of child sexual abuse are typically referred if the victims are girls, if penetration is suspected, if the victims are physically injured, if there is a non-offending, supporting caregiver, and also the child's ethnicity seemed to play a role. 13 However, literature on the selection process in child physical abuse cases is limited.
We aimed at studying cases of suspected child physical abuse to identify key characteristics, such as case context, the child's disclosure and sociodemographic factors, that may influence police decision-making regarding referrals to a CFME. Inconsistencies or biases in the CFME referral process may lead to unequal case handling and undermine the rule of law. By identifying characteristics relevant to the referral process, this study seeks to support a systematic and consistent approach to case management involving CFME referrals.
Materials and methods
The study sample comprised children between 4 and 17 years of age who were suspected of being victims of physical abuse by a perpetrator in the same household and reported to the Copenhagen police between 2016 and 2019. We included two groups of children: those the police referred to a CFME and those the police did not. The first group (CFME cases) was identified using the case files retrieved from the routine database at the Department of Forensic Medicine in Copenhagen; the second group (non-CFME cases) was identified using the case files at the Copenhagen Police and the Copenhagen District Court. We included a subgroup of non-CFME cases. The sample was randomly selected by using the CFME cases as the baseline population; for each identified case, as far as possible, two age-and-sex-matched controls unreferred to a CFME – one from the archives of the Copenhagen Police and one from the archives of the Copenhagen District Court – were selected. Generally, in contrast to the cases from the Copenhagen Police, which were closed earlier in the legal process, the cases at the Copenhagen District Court proceeded to a court hearing. Age matching was performed in the following age groups (years): 4–6, 7–8, 9–10, 11–12, 13–14 and 15–17. We excluded cases involving sexual abuse, as these follow different forensic examination procedures in our setting. Emotional abuse and neglect were not identified or classified. Although the study was restricted to cases defined as physical abuse, co-occurring emotional abuse or neglect cannot be ruled out. Non-CFME cases with siblings among the CFME-cases were also excluded.
Data were extracted from CFME documents, police reports, which included VRI transcripts, and court documents. The Statistics Denmark registry data were provided in an anonymous and secure format, with cases linked to registry information via a unique identification number assigned to all Danish citizens and immigrants. The extracted data were linked with the Statistics Denmark registry data using children's identification number, the legal parents’ identification number and their family's identification number.
Variables
We divided cases based on whether they were a (i) CFME case or a (ii) non-CFME case. The former was the outcome in logistic regression analyses, while the latter was the reference.
Having another origin than Danish was defined as citizenship and a birth country other than Denmark. It was categorised into (i) one or both parents were Danish, or (ii) none of the parents were Danish, with (i) being the reference category.
The suspect–child relationship was categorised into (i) father as the only suspect, (ii) mother as the only suspect, (iii) both father and mother as suspects, and (iv) non-parent (potentially combined with a parent as perpetrator), with (i) being the reference category.
Statistical analysis
Initially, we used univariate logistic regression models (primary analysis) to analyse the association between, on the one hand, characteristics such as family composition, contact with social services, the completion of VRI, disclosure of inflicted violence, the type of violence, the body parts affected by violence, socioeconomic position, parents’ origin and suspect–child relationship, and, on the other hand, the outcome of CFME referral. Further, we analysed the covariate socioeconomic position using multivariate logistic regression models in which parents’ origin and the suspect–child relationship were stepwise adjusted for.
To account for age- and sex-based matching, univariate conditional logistic regression models (matched analysis) were used with the strata previously defined using sex and age. We studied the association between each characteristic and the outcome of CFME referral.
The database was created using Microsoft Access, and data analysis was conducted using SPSS version 29.0.2.0 (20). The point estimates are odds ratios (OR) with 95% confidence intervals (CI).
Sensitivity analysis
In the group of children who underwent a CFME, siblings were included. To account for clustering within sibling groups, a sensitivity analysis that randomly included one sibling per sibship together with singleton children was performed, resulting in 121 children. Using this analysis, performed using univariate conditional logistic regression models, we examined the associations between each characteristic and the outcome of CFME referral. Using multivariate logistic regression models, we also conducted a sensitivity analysis in which parents’ origin and suspect–child relationship were stepwise adjusted for.
Results
Study population
In total, there were 47 CFME cases and 89 non-CFME cases. The 4–7 age group comprised 47 children (34.6%); 8–14, 75 children (55.1%) and 15–17, 14 children (10.3%). There was an almost equal distribution of boys and girls (51.5% boys and 48.5% girls).
The family composition, contact with social services and undergoing a VRI
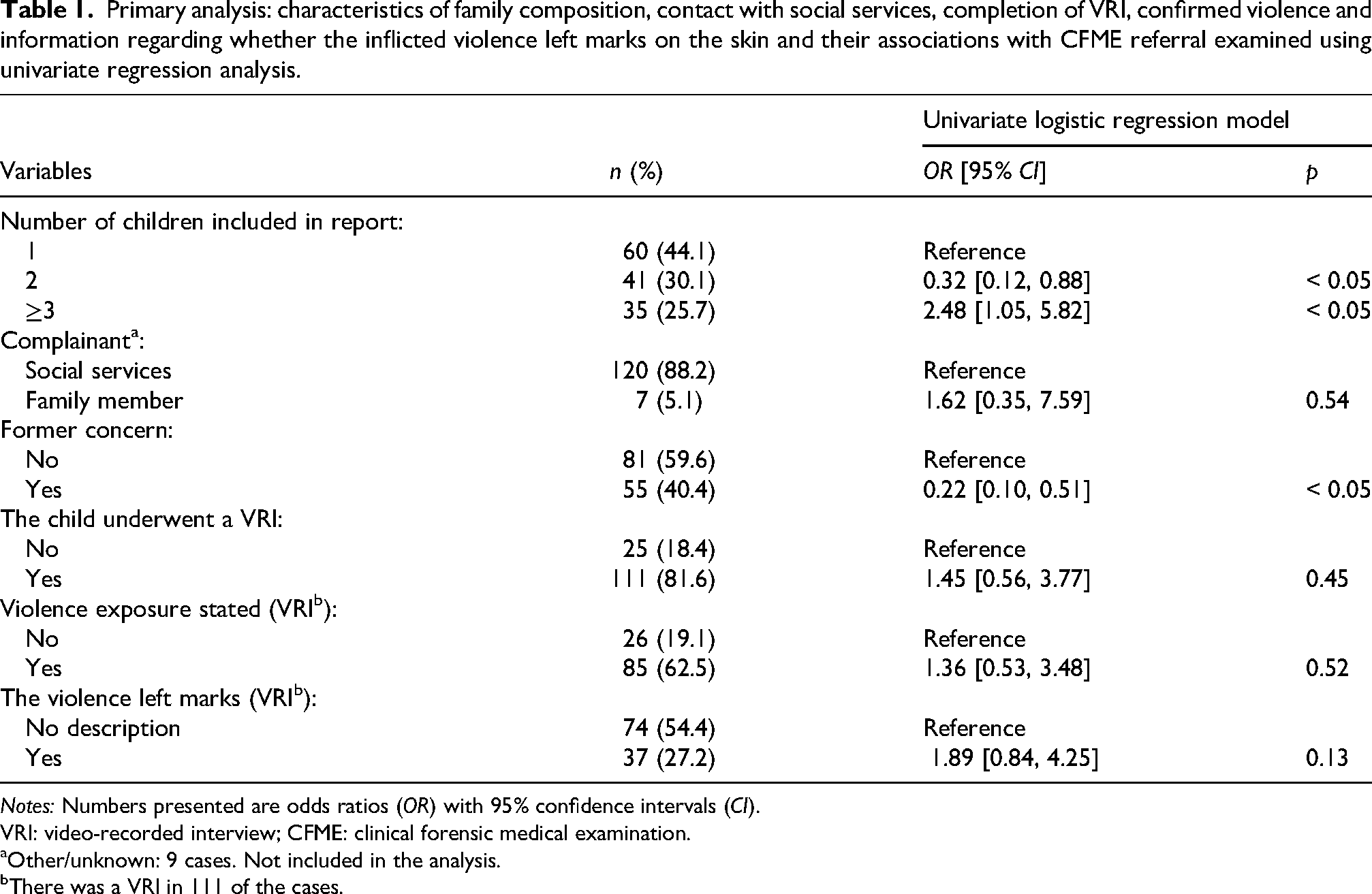
In the primary analysis, we observed a conclusive negative association with referral to CFME when the child was part of a sibship and two victims were included in the police report compared to one (OR = 0.32, CI [0.12, 0.88]) (Table 1, Tables S1 and S4). In the matched analysis, this association was borderline conclusive (OR = 0.41, CI [0.16, 1.02]); in the sensitivity analysis that did not include siblings, it was conclusive (OR = 0.35, CI [0.13, 0.94]). The primary analysis also revealed a conclusive positive association when the child was part of a sibship with three or more victims (OR = 2.48, CI [1.05, 5.82]), but this association was not conclusive either in the matched analysis or in the sensitivity analysis that did not include siblings.
Primary analysis: characteristics of family composition, contact with social services, completion of VRI, confirmed violence and information regarding whether the inflicted violence left marks on the skin and their associations with CFME referral examined using univariate regression analysis.
Notes: Numbers presented are odds ratios (OR) with 95% confidence intervals (CI).
VRI: video-recorded interview; CFME: clinical forensic medical examination.
Other/unknown: 9 cases. Not included in the analysis.
There was a VRI in 111 of the cases.
We observed a negative association between CFME referral and former concerns, an association that was conclusive in all three analyses (primary analysis: OR = 0.22, CI [0.10, 0.51], matched analysis: OR = 0.30, CI [0.14, 0.64], and in the sensitivity analysis not including siblings: OR = 0.26, CI [0.11, 0.63]).
No conclusive associations were found between CFME referral and the source of the police report (the person or authority who filed the police report), whether the child did undergo a VRI, or if they confirmed violence during a VRI. In the sensitivity analysis that did not include siblings, mentions of marks on skin were conclusively associated with CFME referral (OR = 3.03, 95% CI [1.30, 7.05]).
Information disclosed during VRI
In the primary analysis, and in the sensitivity analysis that did not include siblings, being struck with a fist was conclusively associated with CFME referral (primary analysis: OR = 3.83, CI [1.19, 12.39] (Table 2, Tables S2 and S5). In the sensitivity analysis that did not include siblings, hair forcibly pulled (OR = 2.86, CI [1.04, 7.90]), and being struck on the arms (OR = 2.40, CI [1.06, 5.43]) and legs (OR = 2.39, CI [1.09, 5.27]) were conclusively associated with CFME referral. However, in the primary analysis and the matched analysis, the association was positive but inconclusive. Regarding the types of violence and body parts affected, none of them were conclusively associated with CFME referral in the conditional logistic regression models.
Primary analysis: characteristics of the type of violence and the affected body parts described in the VRI and their association with CFME referral examined using univariate regression analysis.
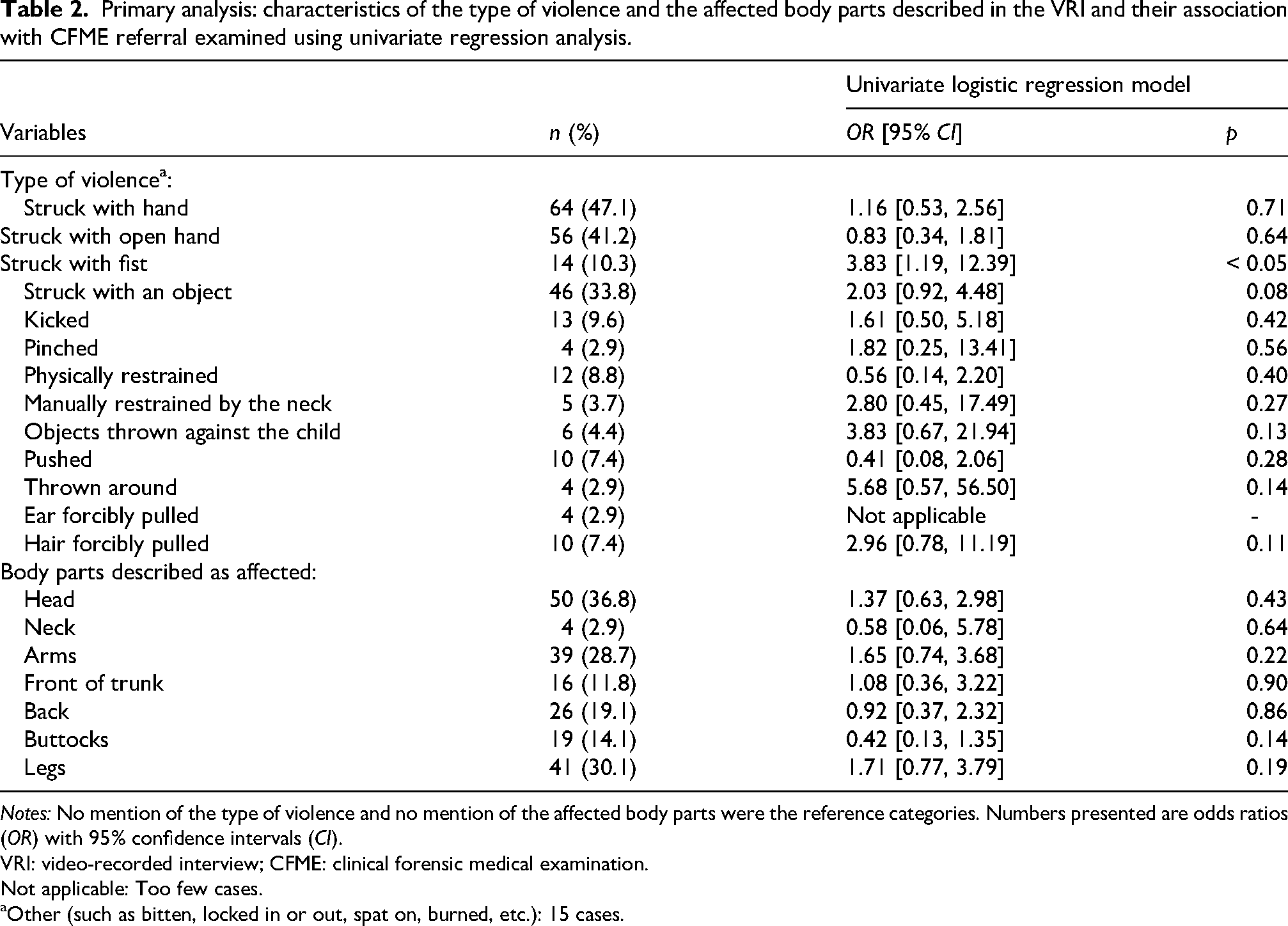
Notes: No mention of the type of violence and no mention of the affected body parts were the reference categories. Numbers presented are odds ratios (OR) with 95% confidence intervals (CI).
VRI: video-recorded interview; CFME: clinical forensic medical examination.
Not applicable: Too few cases.
Other (such as bitten, locked in or out, spat on, burned, etc.): 15 cases.
Socioeconomic position, immigration status and suspect–child relationship
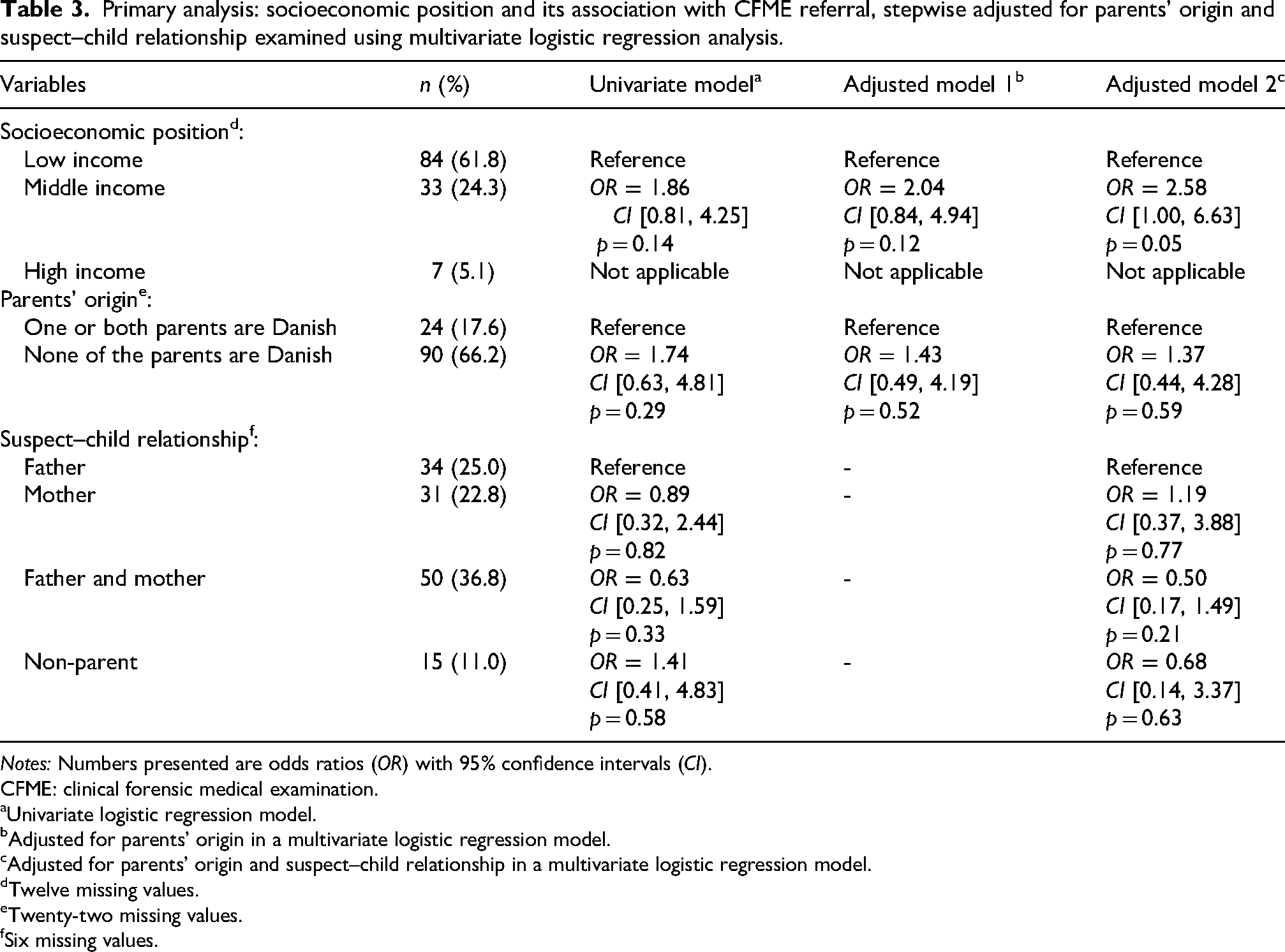
The low-income group comprised 61.8% of children, while only 5.1% were in the high-income group (Table 3, Tables S3, S6 and S7). The number of children who underwent CFME in the low-income group was 26 (31.0% of the strata) and in the middle-income group 15 (45.5% of the strata). No high-income group children underwent CFME, so it was impossible to conduct a regression analysis of this socioeconomic position. Compared to cases with low income in the matched analysis, an indication of an association between middle income and CFME referral was found (OR = 1.75, CI [0.89, 3.44]).
Primary analysis: socioeconomic position and its association with CFME referral, stepwise adjusted for parents’ origin and suspect–child relationship examined using multivariate logistic regression analysis.
Notes: Numbers presented are odds ratios (OR) with 95% confidence intervals (CI).
CFME: clinical forensic medical examination.
Univariate logistic regression model.
Adjusted for parents’ origin in a multivariate logistic regression model.
Adjusted for parents’ origin and suspect–child relationship in a multivariate logistic regression model.
Twelve missing values.
Twenty-two missing values.
Six missing values.
In the multivariate logistic regression model that included socioeconomic position, parents’ origin, and suspect–child relationship, a positive association between middle-income and CFME referral was borderline conclusive (middle-income: OR = 2.58, CI [1.00, 6.63]). Moreover, in the models (adjusted models 1 and 2), the associations between parents’ origin and suspect–child relationship, and CFME referral remained inconclusive. Further, there were no conclusive associations between socioeconomic position, parents’ origin and suspect–child relationship in the sensitivity analysis that did not include siblings.
Discussion
Children with previously reported concerns – reports to social services, police reports on family members, past stays at a women's shelter or any parental conflicts at The Danish Agency of Family Law – or children who were part of a sibship (and two victims in total) were referred to a CFME to a lesser extent. An indication that socioeconomic position might influence CFME referrals was also observed.
The types of past concerns were not further subcategorised, and we did not know whether a child had undergone CFME in connection with an earlier police report or whether other measures for abuse prevention were instigated after past concerns were reported. It was also not known whether there was additional corroborating evidence in the cases at hand that strengthened the cases concerning the sibling pairs, evidence that might have supported each individual sibling's statement, which may have led the police and prosecution service to conclude whether a case could proceed or close without a CFME.
The former concern variable indicates, among other things, that a child or their family is already familiar to social services. Police decisions, such as regarding whether to close a case, could thus be influenced by the police's awareness that social services are already familiar with the family. To explore the potential relationship between police-reported child physical abuse cases and the processes for the child provided by social services, further research is needed, and this could include qualitative interview studies with police officers, prosecutors and social workers. We have not studied why not all cases of suspected child physical abuse are referred for a CFME. However, we speculate that it might involve several factors such as lack of understanding of the role of the CFME, that the process is labour intensive, is associated with a further financial cost, and could introduce a further time lag in the system. However, this could be researched further in future studies.
The primary and sensitivity analyses found that the children who were punched were often referred to a CFME, but this was not the case in the matched analysis, which is why this result should be cautiously interpreted. A punch could possibly be considered a more severe form of abuse than a slap; the police could also interpret it as associated with, for example, the presence of marks on skin – which, in turn, was also indicated to be associated with CFME referral in the sensitivity analysis. Moreover, in the sensitivity analysis, being struck on the arms or legs was associated with CFME referral, but this was not observed in the primary or in the matched regression analysis. Arms and legs were two of the three most frequently affected regions, and this should be considered when interpreting the results of the models, in light of the low statistical power. Moreover, we argue that the sole statement of having had their hair pulled is not enough for a CFME referral (found in the sensitivity analysis that excluded siblings). This act seldom leaves any marks, so this statement probably co-exists with other factors important for a CFME referral. Alternatively, it could be a random finding due to multiple comparisons.
Mother and father in combination were the most frequent suspects. The variable was extracted from who was registered as the suspect at the time of filing the police report – and not who the prosecution filed preliminary charges against – to reflect the known factors at the time of CFME referral. The associations were neither conclusive nor borderline conclusive, which is why there does not seem to be an association between the suspect–child relationship and CFME referral.
Notably, no high-income group children were found to be referred to a CFME, and the middle-income group of children were, to a larger extent, referred compared to the low-income group children – this finding reflects the influence of socioeconomic characteristics on the referral process. Again, it cannot be concluded whether other substantial supporting evidence exists in these cases or whether social services are involved to a larger extent in some socioeconomic strata. To elucidate the potential association between socioeconomic position and CFME referrals, further research is needed.
In contrast to the findings from the multicentre study in the United States, no association was observed between ethnicity and CFME referrals. 13 However, our analysis suffered from low statistical power.
The 47 included CFME cases are child physical abuse cases in close relationships over a four-year period in Copenhagen, and the number corresponds to approximately one per month. This is in contrast to the fact that the population of children aged between 4 and 17 years in the Copenhagen area in 2016–2019 was around 97,000. 15
We acknowledge that the steps that must be taken in an investigation must be prioritised and that a concrete, case-specific assessment of the necessity of each investigative step is essential. However, there is the risk of missing the opportunity to secure medical evidence if a CFME is not performed. If lesions and scars are undocumented, the opportunity to document fresh lesions is gone once the lesions heal. A CFME can serve justice not just for children but also for suspects, as the absence of lesions and scars also offers information.
Furthermore, the CFME can serve purposes beyond the strictly forensic. A CFME may uncover other health and wellbeing concerns that demand appropriate follow-up from social services, medical professionals or dental care providers. 16 ,17
Limitations
Based on information in the police report, we excluded siblings in the non-CFME cases. However, in the data set obtained from Statistics Denmark, which also included data on which family the child lived with, we observed that the exclusion was not complete as there were still a few siblings included. These were, however, also excluded in the sensitivity analysis. Our research sample comprised children aged between 4 and 17 years, but 4 to 14 years is the typical age range for conducting a VRI 5 and some of the children who did not undergo a VRI because of their age thus underwent traditional interviews, which the police documented in their reports, but we did not include them. This could have influenced our results, as a larger group of children may have confirmed to the police that they were exposed to violence. Moreover, our statistical method – conditional logistic regression – accommodated age matching and, therefore, minimised the impact of the fact that older children often did not undergo a VRI. The frequency matching of age group and sex prevented us from analysing the association between these variables and the outcome of CFME referral. We intended to match CFME cases with non-CFME cases with a ratio of 1:2, but this was not possible for every CFME case. Consequently, some were matched with the nearest age-group category, or no suitable non-CFME case could be retrieved, resulting in a CFME-case to non-CFME case ratio of 1:1.9. This limitation, we argue, did not substantially have an impact on our results. Moreover, the time from being exposed to violence to the filing of a police report may vary, and this could also be considered in the CFME selection process – this information, however, was not available at the time of the study.
Disclosures of violence against arms and legs were in the sensitivity analyses excluding siblings conclusively associated with referrals to a CFME. It is a possibility that the police officers by themselves, at the VRI, can observe lesions on exposed body parts such as the face, forearms, and lower legs, which in turn may affect the decision to request a CFME.
We used the total household income as a proxy for socioeconomic position. The variable is not related to the number of children in the household. The total household income is one aspect of socioeconomic position but does not directly correspond to the resources available for each child. Lastly, our small study sample resulted in low statistical power.
Conclusion
We explored characteristics of suspected child physical abuse cases that may influence police decision-making regarding CFME referrals. We found that the variables of former concern, belonging to a sibship (and thus there being two victims in total), and being from a low socioeconomic position were associated with fewer CFME referrals. Moreover, whether the child was punched, struck at arms and legs, or marks were left on the skin seemed to be associated with CFME referrals. However, no association between CFME referrals and parents’ origin or the suspect–child relationship was found.
We argue that, in accordance with the principle of treating each case on its own merits, a CFME is important for documenting the lesions and scars of each child individually. Future qualitative interview studies with police officers and prosecutors as well as studies on larger populations can offer valuable insights into the underlying mechanisms of the CFME referral.
Supplemental Material
sj-doc-1-msl-10.1177_00258024261466036 - Supplemental material for Characteristics of child physical abuse cases that are referred by the police for a clinical forensic medical examination
Supplemental material, sj-doc-1-msl-10.1177_00258024261466036 for Characteristics of child physical abuse cases that are referred by the police for a clinical forensic medical examination by Liselott Slot, Daniella Justesen, Lykke Thorlacius-Ussing, Anne Birgitte Dyhre Bugge, Niels Lynnerup, Jytte Banner and Carl Johan Wingren in Medicine, Science and the Law
Supplemental Material
sj-docx-2-msl-10.1177_00258024261466036 - Supplemental material for Characteristics of child physical abuse cases that are referred by the police for a clinical forensic medical examination
Supplemental material, sj-docx-2-msl-10.1177_00258024261466036 for Characteristics of child physical abuse cases that are referred by the police for a clinical forensic medical examination by Liselott Slot, Daniella Justesen, Lykke Thorlacius-Ussing, Anne Birgitte Dyhre Bugge, Niels Lynnerup, Jytte Banner and Carl Johan Wingren in Medicine, Science and the Law
Footnotes
Acknowledgements
We acknowledge legal advisor Søren Nielsen and his colleagues at the Legal Section at Copenhagen Police. We thank forensic nurses Maria Balsløv and Andrea Lykke Thanning and research coordinator Stéphanie Palombi at the Department of Forensic Medicine, Copenhagen, for their help with the research.
Ethical considerations,consent to participate and consent for publication
Copenhagen Police approved the perusal and data collection from the police reports and court documents. Approval of processing personal data in research projects was granted by Copenhagen University (514-0703/22-3000, 514-1023/24-3000). Since this is a registry-based study based on forensic routine data (004-0022/18-7000) and data from Statistics Denmark, no other approvals were needed.
ORCID iDs
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported from the Danish Victims Fund [21-610-00133]. The execution, content and results of the materials are the sole responsibility of the authors. The analysis and viewpoints that have been made evident from the materials belong to the authors and do not necessarily reflect the views of The Council of The Danish Victims Fund.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets generated for the current study are confidential.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.