
Abstract

A meeting of the Society was held at the Medical Society of London, 11 Chandos Street, Cavendish Square, London, W1G 9EB, on Thursday, 10 December 2015. The President, Ms Linda Lee, was in the Chair.
I am Chair of the General Medical Council for four years and what I want to try and do is reposition it, as Linda said, as a 21st century patient safety organisation. It has already come a long way, but there remains more to be done. I want to illustrate why I believe this is so important and what we are doing.
I want to start with something the doctors in the room will know, which is that we like to think our NHS is safe. All of us who are doctors, nurses and other healthcare professionals, certainly don’t go to work to cause harm but we certainly, inadvertently, do cause harm and this has been well documented
So the NHS on the whole, I hope, (and I have worked in the NHS all my life) profoundly does more good than bad, but it can be a high-risk place. To paraphrase Sir Cyril Chantler, medicine used to be relatively simple, safe and largely ineffective, and now medicine is incredibly complex, sometimes unsafe and by and large very effective. We mustn’t forget, in all of these times of woe, in my professional lifetime longevity has increased; cot death is a quarter of what it was; survival from leukaemia is now 70% rather than 30% – these are huge advances, but it can be a risky business.
And I want to contrast that with a different safety critical industry. In about 2004, I spent a week with Shell in Aberdeen and I had a very Damascene experience there. I flew up from London. I was picked up by a taxi that, in a basically empty car park, reversed into a space. I asked the driver, “Why did you reverse in?” He said, “Oh, well Shell have looked at accidents in the car park and most accidents happen when people drive in in the morning and at the end of a long day reverse out in darkness and reverse into someone else, so everybody has to reverse in in the morning and drive out at night.” Then I was offered a cup of coffee, which I thought was very nice, but I was told I couldn’t walk around with that without a lid on it, and I said “Well, that’s interesting”, and they said, “Well, if you walk around on an oil rig with hot liquid and you spill it, you not only harm the person you spill the hot drink over, we now have to get a helicopter out from Aberdeen and you risk the lives of that crew.” And then I went up some stairs to an office and he said “Now, if you go up the stairs …” – I was feeling like a 4–year old by this time – “… you have to hold the bannister. If you don’t hold the bannisters in the building and then you go on an oil rig and you fall off, you have now risked your life, the lives of the crew that have to come out in the helicopter and the diver who has to be winched down and pull you out.” So Shell had a huge safety culture absolutely embedded in it and they had a mantra: “There are two ways of doing anything. There is the Shell way and the wrong way.”
Now contrast that with when I was a non-executive director of a large hospital, with 10,000 staff, 1300 beds, £600 million turnover. I went back to that hospital and we were struggling to get our doctors and nurses to wash their hands; an intervention that has been known to save lives since the time of Semmelweis in Vienna in the 19th century. The compliance rates of hand washing – Shell would just not accept it. At Shell first of all you get a verbal warning, then you get a written warning and then you are fired, and that is partly how they have reduced risky behaviours. They refuse to have people doing things that are not acceptable, and that is a huge contrast with our beloved NHS.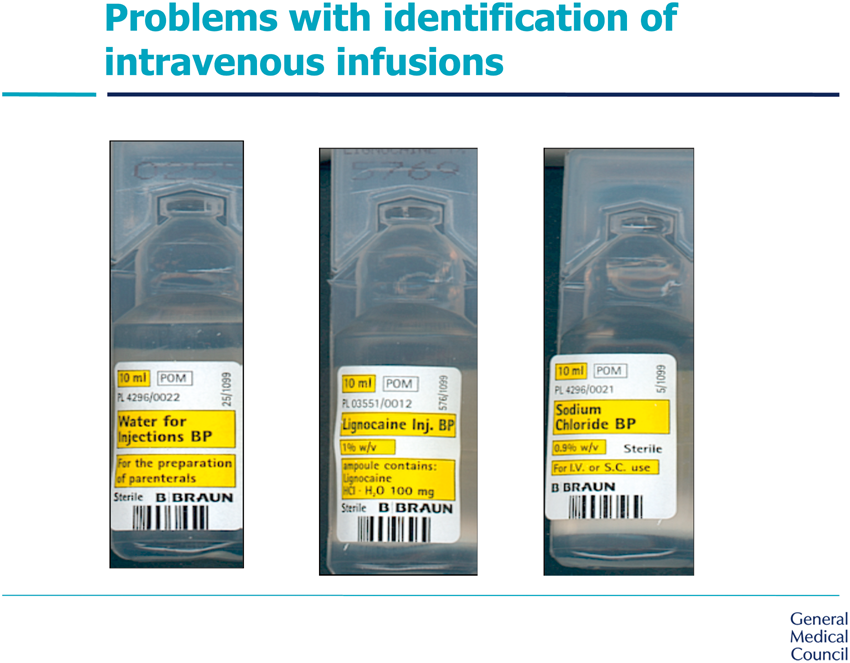
I then went to work for the National Patient Safety Agency; I was seconded for 3 years. The picture shows three drugs in a cardiac arrest situation, where seconds count and drugs are being drawn up quickly. They all look remarkably similar, don’t they? They are all clear liquids in identical plastic vials with yellow and black bar coding – very easy to give the wrong drug.
Another example is a case I managed involving two patients, a mother and her child. They were both my patients at the same time. I am a paediatrician. The mother is a 16-year old who I have looked after for over a decade with a long-term illness. She had a child who was born prematurely, weighing around a kilogram. I prescribed for both of those patients at the same time, but there is a 50-fold difference in weight and the capacity for getting drug doses wrong is huge. Yet it was just this month that electronic prescribing has become available: it has been available in general practice for 30 years and available in the United States for 20 years, it became available in my hospital for the very first time then to try and avoid these prescribing errors caused by incorrect calculations.
I could go on, but I think I have made the point. In a sense what I want to emphasise is that the NHS is a great thing, but any healthcare provider in the world, not just the NHS, carries risks. We need to reduce that, and I think the GMC has a part to play. Linda quite rightly said that when the GMC was established in 1858 it wasn’t envisaged as a patient safety organisation. The drive for it was not from the medical profession, nor indeed the legal profession, it was from parliamentarians. There were 11 attempts to get an Act through Parliament, and, if you want to try and understand why, you could do worse than read Middlemarch. Written about 1870, the primary plot is about the 1832 Reform Act of voting in Parliament but there is a sub-plot which is about the medical profession. Tertius Lydgate is one of the key characters and it is about the fact that in the 1830s the general public could not even distinguish between who was a doctor and who was a physician, who was surgeon and who was a barber surgeon, who was an apothecary, who was a bonesetter, who was a bonecrusher, who was a snake oil merchant. It was just incredibly difficult. Who had a degree like Tertius Lydgate from studying in Edinburgh, Paris or London? Who had spent 3 years sweeping their apothecary’s floor and who had been given an honorary degree by the Archbishop of Canterbury? The public was really struggling. So the idea of the Act of Parliament in 1858 was to create a medical register so the public could distinguish the proper doctor from the quack.
Once a register is established, four other duties flow. Number one is maintaining the register. Secondly, there has to be a mechanism to decide who gets on the register. So the GMC was given responsibility for overseeing the whole of medical education and training. The third responsibility is that the GMC should provide some guidance to help people stay on the register, guidance about ethics and consent and professional etiquette. Then fourthly and finally, there must be robust measures that allow people to be taken off the register if they don’t follow the straight and narrow path, and those processes have to stand up to scrutiny and they are quasi-judicial.
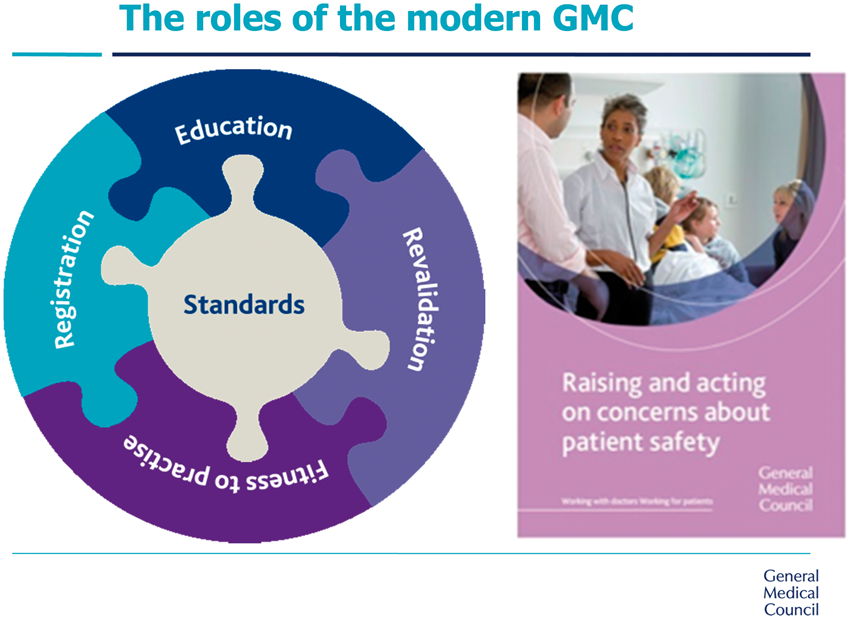
So all of those four functions: maintaining the register, the training to get on the register, the guidance to stay on it and the fitness to practise procedures to strike a doctor off, have existed for 150 years; they are the enduring mission of the GMC today. I want to take some examples from each of those four pillars of what we do and demonstrate how they actually affect patient safety.
I am sorry to say the register has barely changed in 150 years. I have the originals near my office in the GMC here in London. This is a photograph of the register from 1858, I think.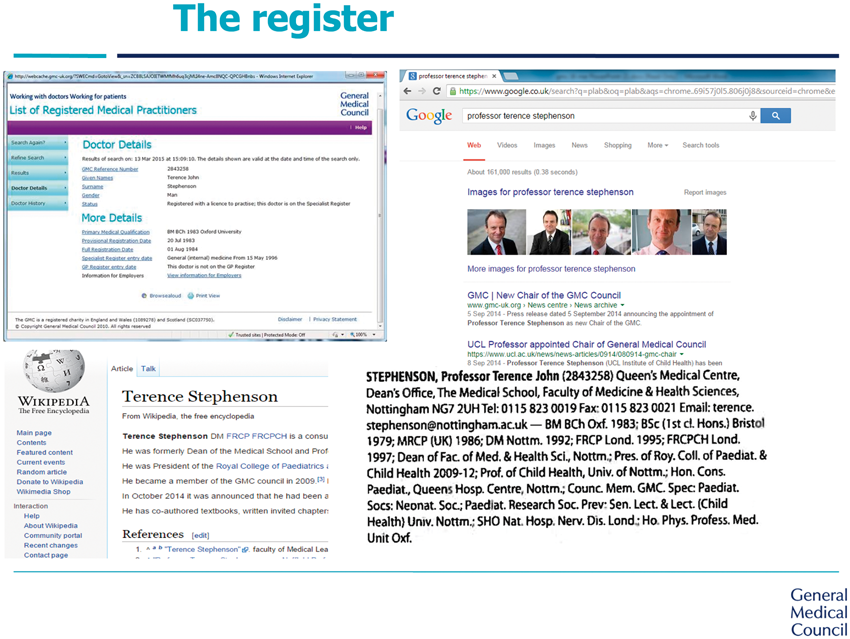
If you were to look up my entry in the register today, it has little more than my name, my date of birth and the university I qualified from, and that’s about it. If you really wanted to find out about me it would be much more illuminating to Google me, or look in Wikipedia, or the Medical Directory, which is a commercial publication, but you certainly wouldn’t refer to the GMC register.
Contrast that with the example of a surgeon from the North West of England. He is a doctor who thinks the public are entitled to know far more than is currently on the GMC register. Remember, the original purpose of the register was to establish whether you were a doctor or a quack. That is hardly sufficient for 2015/6. Surely the public and employers and other bodies want to know what kind of doctor you are and your level of training and experience. This surgeon is quite happy to have in the public domain the number of operations he has done in the last year, the particular types of procedures he has undertaken, and to publish his own mortality statistics and have them compared to mortality rates from surgery in other places in the United Kingdom. Most doctors are somewhere in between and there is a great range of views, but I do think it is something we need to explore as a regulator. We need to look at what information we can put in the public domain, and perhaps some of it we verify and quality assure, and some of it we say is self-declared, but make it clear that if you tell lies we will take action. This review of our register is something that we will be looking at in more detail over the next year.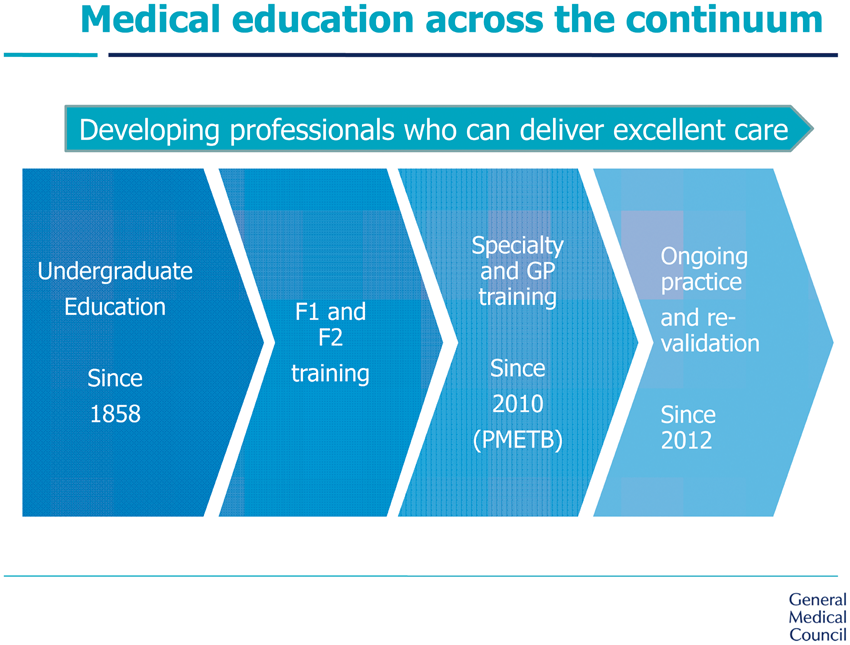
The second topic I want to address is getting on the register and the training that doctors undergo. Since 1858 we have been responsible for all the undergraduate medical schools in the United Kingdom and there are now over 30 different universities awarding medical degrees in the UK. In 2010, the GMC took over a body called the Postgraduate Medical Education and Training Board, which was responsible for postgraduate training, and since 2012, with revalidation, the GMC is now responsible for people’s lifelong learning and keeping up to date throughout their career.
I want to focus particularly on undergraduates but I will say something about the two other phases of medical education.
The GMC Council has decided that the United Kingdom should have a single Medical Licensing Assessment and we are exploring that actively. Let me give you some of the reasons for that.
Perhaps the most pressing is that when doctors come from other countries outside of the United Kingdom we are obliged by law not to discriminate against them and we have to set some assessment. The bar should be set to be comparable to our own doctors. Well, we don’t really know where the bar is. We have 32 different bars. We have data that shows that the standard of achievement in those different medical schools is not the same and that makes it very difficult. The exam that doctors from outside the EU take, called the PLAB exam, is accused of being both too difficult and discriminatory and being too easy and letting too many doctors into the UK who are not up to the standard of our own doctors. Well, the truth is, we just don’t know either way. We need a single assessment which all of our new doctors take and then everybody else can take too.
The second reason is that when I talk to the public most people assume that doctors qualifying in this country, like pilots, like newly qualified drivers, have met some common standard. They are quite surprised to learn that, just like a degree in English literature, the exam is set by the people who taught the students. Now, I don’t think in any postgraduate examination, be it professional law exams, accountancy exams, chartered engineer or any postgraduate medical exams that would be ideal today.
So in terms of assuring the public of what I think is the very high standard of our own doctors there are compelling arguments for having a single licensing examination, which has existed in the United States and Canada for over 100 years.
Just to give you one example of the data that suggests wide variability, we have the biggest national training survey in the world, 55,000 doctors, with over a 95% response rate, and they tell us what they think of their training, and here is a comparison. We ask them “How prepared do you think you were? How oven-ready were you on the day you started practising?” after your five or six years at medical school. There are big differences in the percentage who feel they were adequately prepared. So we know there is a difference between medical schools in what their own graduates think is being done to prepare them.
Let me move to postgraduate training. We have only been responsible for that for five years. It is extraordinarily important. About a third of the doctors practising in the NHS today will be trainees, so we are responsible for a very large number of people, and I think by and large the training in the United Kingdom is extraordinarily good and still highly thought of around the world.
I think that sometimes our training is very good on the technical aspects of being a doctor – prescribing, surgery, reading x-rays – but I will show you some evidence that we need to be concerned about doctors as professionals. I was asked by a very senior member of the medical profession, “What do you mean by it? What is a professional?” When I think of any professional – vet, dentist, lawyer or accountant – I think of a person you go to for independent advice, hopefully not influenced by the fact that you may be paying them, and some of that advice is highly technical. But at the same time all professionals are expected to listen to you, to treat you with dignity, not to be racist, not to be fraudulent. These are aspects of being as professional too – not just to give advice free of fear or favour – and these are the generic competencies we expect of all professionals.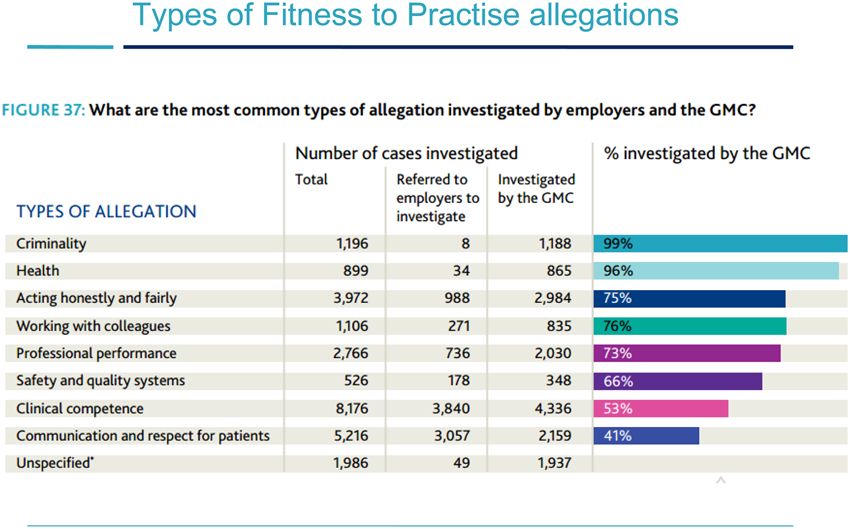
If we look at the reasons that people complain to the General Medical Council about doctors (and we get complaints against around 10,000 doctors per year), there may be more than one aspect of a doctor’s practice complained about. Thus, the total adds up to a great deal more than 10,000 different issues raised. You will see that a minority (only around 8000 of that total) are about clinical competence. So being technically competent isn’t sufficient; it is necessary but not sufficient. There are about 4000 complaints about acting dishonestly. There are over 1000 about criminal behaviour and over 1000 about how a doctor works with his or her colleagues. A doctor may be the best cancer doctor in the world but if he or she does not get on with their colleagues that team doesn’t function as well as it might. There are also allegations of sexual impropriety. A doctor might be the technically most gifted heart surgeon in the world but still exploiting a patient sexually. These are complaints about aspects of professionalism not clinical skill. In fact, most of the serious complaints that we deal with are not around technical competence at all.
We are working with the medical Royal Colleges on a framework for these generic professional capabilities. They are not peculiar to being an obstetrician or a radiologist or a GP, they are relevant to all of our trainees and to all trained doctors too.
I think our GMC guidance is very clear, comprehensive and detailed but where I think we have a problem is that it is not as accessible as it should be. In my own practice I had to look up recently about blood transfusion and Jehovah’s Witnesses. I always find the answer but it takes a long time and it is not very user friendly. When I am on the wards now generally I have a stethoscope and an iPhone, and that’s about it. I need to be able to access this guidance, and sometimes very quickly. I think the GMC can do better at getting its guidance into a format that is far more accessible for the modern world. The quality of the guidance is good but the accessibility could be much better.
So far, in terms of patient safety, I have talked about having a more informed public who can choose their doctor better if the register told the patient more, and we would get a safer health service if the patient can make a more informed choice. I have talked about education and training. I think we can assure the public that our doctors are safer if we know they are all reaching a common standard. We can assure them that they are not only technically competent but that they are acting in a professional way if we emphasise those generic professional capabilities. And I have talked about having a safer healthcare system if the guidance we spend so much time producing and updating is easily accessible for busy doctors in a frontline service.
I think revalidation of doctors also increases safety for patients. It has not been a popular innovation: when I go round the country the greatest pushbacks I get are about revalidation – I hear that it’s time consuming, box ticking and it wouldn’t detect another Shipman – and about our fitness to practise processes. What I say to the profession is that some of that may be true, of course. Revalidation is in its first wave, it has only been with us since I revalidated in 2013 and undoubtedly the second cycle will be refined and improved. But I think the profession needed to recognise that revalidation was imposed following the Shipman Inquiry.
When Dame Janet Smith undertook the Shipman Inquiry she was surprised to learn that a doctor, someone like myself, last took a professional exam in 1986, and she was perplexed that there seemed to be no system whereby doctors should demonstrate that they remained fit to practise, that they remained up to date, that they remained competent. She asked the GMC to go away and come up with a mechanism for reassuring the public that doctors remained fit to practise throughout their careers. There was a perception that “If you don’t get this right and come up with something more robust, then we will do it for you”. What we still have is professional self-regulation, at least to some extent. It is entirely funded by the profession, and revalidation, whilst it is an employer-led concept, involves doctors being revalidated by other doctors and by Medical Directors in their organisation.
The idea that we could have not had revalidation is false. We have to accept it was thrust upon the profession, like it or not. The profession had been talking about it for over a decade before that, following Ian Kennedy’s Bristol Inquiry in 1991, but it was given a huge push by Shipman. I too doubt if revalidation would have detected Shipman. If you read the testimonials from his patients in his practice, many were glowing. He was seen as the most fantastic doctor by some. He was trusted; he was thought to be kind, generous and available. However, he was a murderer and revalidation is not a technique to detect murderers.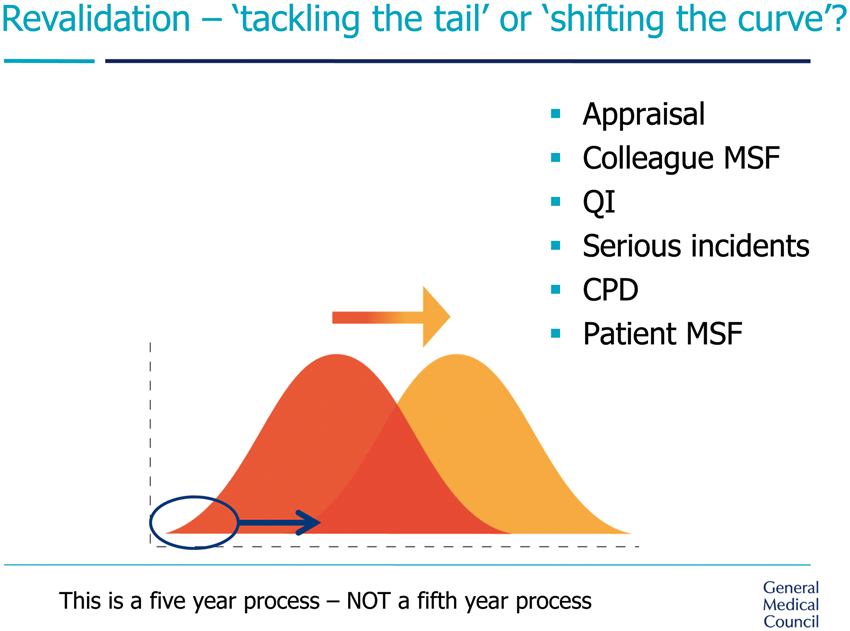
Revalidation has two dimensions. It is trying to tackle the tail of poor performance, perhaps one or two per cent of doctors in any healthcare system in the world who are performing below an acceptable standard who need remediation. But equally importantly it is about “shifting the curve”, improving the practice of the 267,000 doctors on the UK register. Even the best can do better and all of us can improve our practice. When doctors say to me they don’t like revalidation I say Which bit of this do you not want to do? You don’t want to sit down for an hour a year with your boss and talk about what you do? Are you not interested in feedback from your colleagues and your patients about your performance? You don’t want to discuss serious untoward incidents? You don’t want to demonstrate that you have kept up to date? Which bit of it do you think is an unnecessary imposition on you?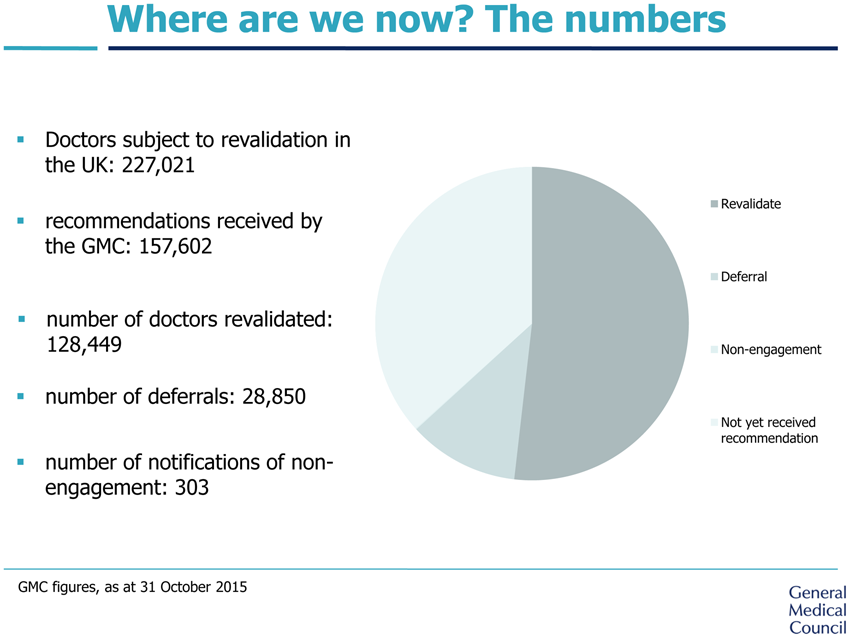
We have revalidated 130,000 doctors and deferred 28,000. Many of those are “administrative” deferrals depending on the date which trainees complete their training. But there are 300 doctors who are no longer able to practise in this country because they won’t engage with the process of revalidation, and frankly, if my doctor doesn’t want to demonstrate he or she is up to date, then I don’t want them to be my doctor. I don’t want a kind of system that says “Well, we know that doctor is awful, but as long as they don’t treat me …” and that has been a risk throughout my whole professional life. As a trainee doctor, I recall conversations – “Well, I wouldn’t go to that doctor. How come the public don’t know?” I think that is quite unacceptable.
Almost 25,000 doctors have chosen to give up their licence to practise, many of them elderly, some retired. Some might argue that they are just prescribing for themselves or for family relatives but that is not a trivial thing. If the doctor cannot demonstrate that he or she is up to date, then that doctor shouldn’t be prescribing for friends or relatives. A doctor is either up to date or not. A doctor needs to know the side-effects from the latest drug to give and the latest guidance. Revalidation has also had a huge effect on clinical governance in organisations. In three different hospitals in three different parts of the United Kingdom the threat of putting a hold on revalidation has led to changes. We never had to suspend revalidation but just the risk that this could happen had an effect. So although it has made an impact, I acknowledge revalidation is not perfect and I hope we can do it better in the next cycle.
The final topic I want to talk about is fitness to practise. You will all know that the number of complaints about doctors has been increasing. That is true for other professionals too – solicitors, accountants, dentists – and is a consequence of the fact we live in a more litigious society.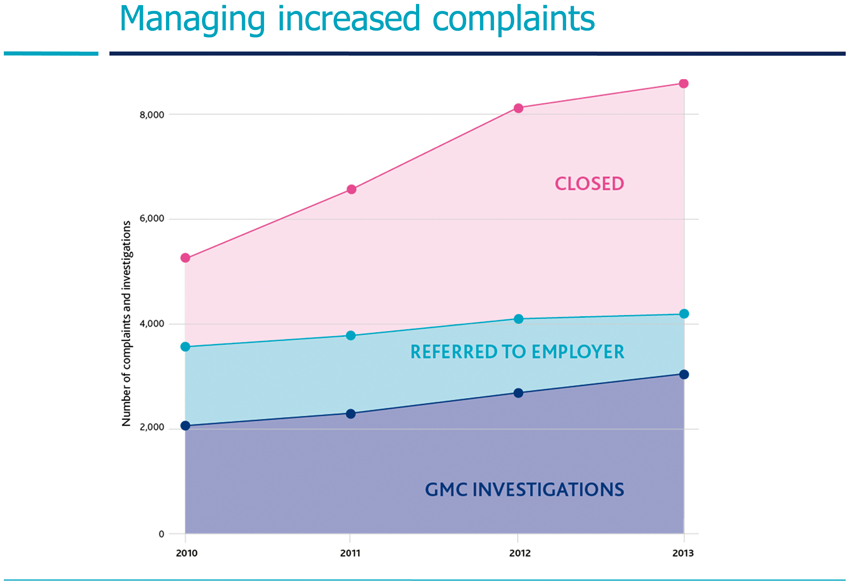
I am pleased to say that the number of complaints that we close quickly has expanded hugely. The actual numbers that are investigated hasn’t gone up quite as much as the total. The top line on the graph has gone up quite a lot more than the middle line. But, nevertheless, it partly explains why we have to work harder to stand still, and it partly explains why many regulators have to increase their fees. Complaints are also not only increasing in number but to some extent in complexity.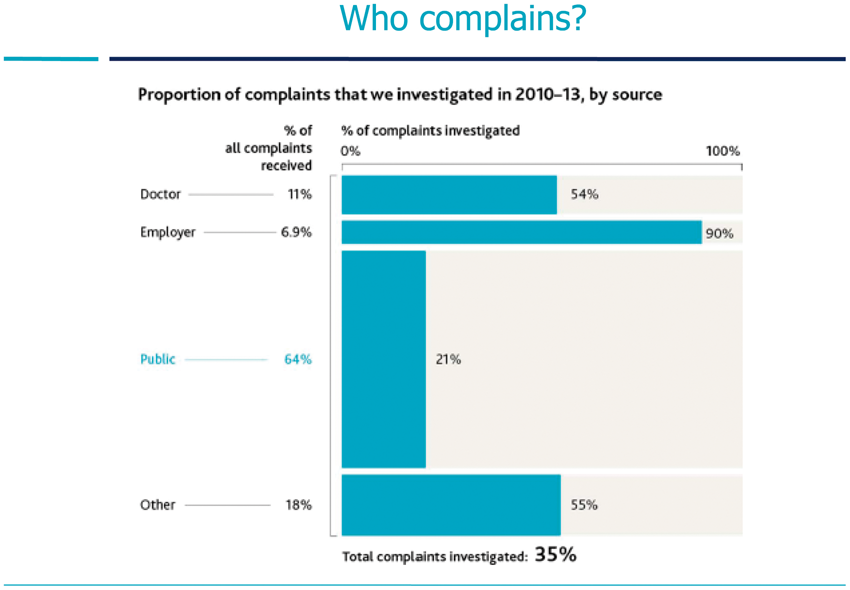
The source of complaints: approximately a third come from patients, a third from employers and a third from either colleagues, fellow doctors, or some other agency, like the police. I have been on the sharp end of this. I have been investigated twice by the GMC in my professional career. I have been complained about once by a patient and once by another doctor. I am pleased to say I was exonerated completely both times, but I know the Sword of Damocles that hangs over a doctor while you are being investigated by the GMC.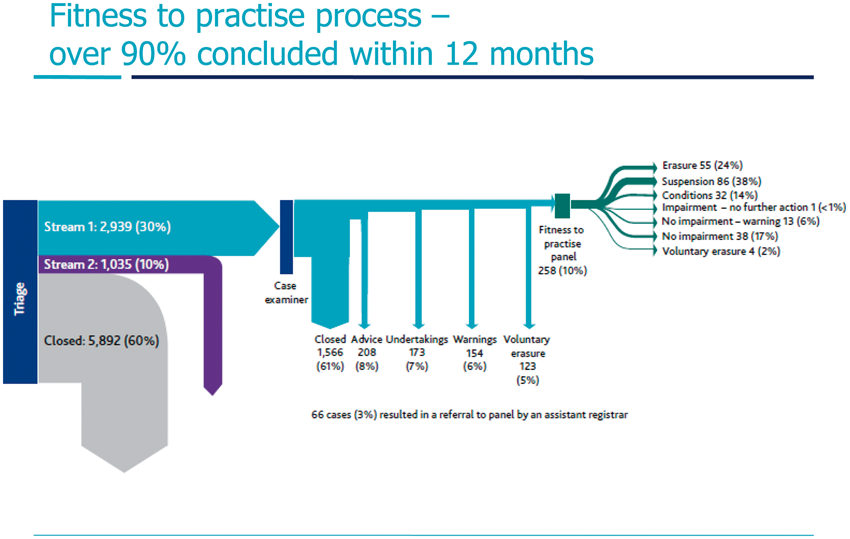
If we look at a representative year in which there were approximately 10,000 doctors complained about, some 6000 of those complaints were closed very quickly. We have more complaints which are closed quickly from the public and patients than from employers or colleagues. We have about another 1000 where there is an issue but we refer back to the employer, to the Responsible Officer. There is often a contractual problem but it is not a problem about the doctor’s fitness to practise. And that leaves us with 3000 that then go into our processes and ultimately in this year of data about 255 of those end up going to one of the medical practitioner tribunals in Manchester.
So, we have a hammer to crack a nut. We are creatures of statute: entirely governed by the 1983 Medical Act at the moment, and I will say more about that. But you will see from these figures that overall about 80% of those 10,000 complaints end up without any finding against the doctor. Of the 255 that get through to a tribunal about 80% have a sanction or warning made against them. So, at the very sharp end, I think broadly we are getting it right, but at the blunt end, at the beginning of the process, we are awash with complaints, some vexatious, some entirely inappropriate, and we would really like to see a lot of those complaints handled at a local level, particularly by the employer. The GMC is kind of a free recourse to action. If an organisation or a colleague has a problem, it costs nothing to pick up the phone or go online and complain to the GMC, and we are obliged by statute to look into the matter. We cannot just say we are not investigating.
Finally, I want to emphasise that we are a reforming organisation. We do want to reform these procedures that are too slow and we have done some things already.
We have Employer Liaison Advisors across all four nations who are trying to work with employers to say, “Do you really want to send that to the GMC? Is there not another way of dealing with this locally?”
We have created the Medical Practitioners Tribunal Service, based in Manchester, which handles those 255 most serious problems. (A full lecture on the workings of the MPTS was given to the Society by its Chairman HH Judge David Pearl and is published in Vol. 83 Part 3 (2015) pages 128–135.) I was on the Council of the GMC in 2008–12 when the MPTS was created. I am very proud of that, because I as a doctor felt it was wrong that the GMC was both the investigator, the policeman, the prosecutor and the judge and jury, and these are now entirely separate functions.
We have a Doctor Support Service, which we fund entirely. I don’t suppose any doctor would want the GMC who is investigating them to support them, so we let the BMA run it. When a doctor picks up the phone and contacts the Support Service for confidential help, it will be given by the BMA, but we fund it entirely.
We are pursuing what is broadly analogous to the concept of collaborative law, where the parties meet with their lawyers present and try and tease out the sometimes 80 or 90 per cent of things that are agreed and then say “Well, what is the 10% we want to go to court on”, and we have been having those meetings, at the moment separately with the doctor who is complained about and with the patient or employer who has complained, but we would like to move to a yet more collaborative format.
We have carried out a pilot project on what are called Provisional Enquiries. When those 10,000 complaints first arrive at the GMC, if we put quite a senior resource at the very front of the procedure, there may be just one document or one witness statement that we need in order to decide whether this can be closed or not. By doing that we found in our pilot that we reduced the time taken for investigating those cases from a median of 245 days to 63 days. So that is something we will be taking forward and rolling out. It has been very successful.
I mentioned there were about a thousand complaints where there is an issue, often contractual, that we refer back to the Responsible Officer in their hospital or their practice, rather than taking them through the GMC.
I said that we are a creature of statute, the 1983 Medical Act, and governed by the procedures set out in the Act. Therefore, to change any of these procedures, we need to get a section 60 amendment to the Medical Act. That requires lawyers in both the GMC and the Department of Health to spend (usually some) years drafting and redrafting these amendments and then we have to plead for parliamentary time from the Government to get the amendments through Parliament. It is a very time-consuming process. We have just got a section 60 through the Privy Council in May 2015 and that took several years from the first proposal. I will give some examples of how these new amendments will help streamline fitness to practise procedures.
Firstly, the section 60 amendment allows the GMC to have a Right of Appeal against the Medical Practitioners Tribunal if we think the sanction imposed is not sufficient to protect the public or inappropriate. At the moment we can’t appeal against the MPTS. The section 60 reforms which come in at the end of December 2015 would allow us to do that.
We have no sanctions at the moment when cases over-run, sometimes through the GMC’s fault but sometimes through the medical defence organisations, the employer or the doctors themselves. Every other tribunal service, I am told, has sanctions with teeth, so that its costs can be awarded against a party which is not complying with the case management.
We plan to have legally qualified chairs from 2016 and that would allow us to, hopefully, save time with panels that do not currently have a legally qualified Chair but are advised by a Legal Assessor. We are going to pilot that initially in the interim order tribunals. We will also be able to consider, where appropriate, “paper review”. Up until now we have had no capacity to just review the documents on, say, a technical point of law. Every party has to go in person to Manchester with their lawyer but the point may be resolved very swiftly and that could be done as a paper exercise by a legally qualified Chair.
Finally, what would we like to do? Well, we were very keen to see the Law Commissions’ Bill come forward. It was agreed by the Law Commissions of England and Wales, Scotland and Northern Ireland. It had support in both Houses and it was in the manifesto of two of the three largest parties going into the election. Unfortunately, it wasn’t in the manifesto of the party that won. It was not in the Queen’s Speech and I think it is unlikely to be in the next Queen’s Speech.
So that leaves us with a problem. We are going to need another section 60. In fact, all of the nine regulators want section 60s. The Law Commissions’ Bill would have given us a single overarching piece of legislation, an umbrella that the regulators could work under, could be fleeter of foot – and health is a rapidly changing set of disciplines – and we could have moved more quickly. So we are probably going to have to go back to ask for more section 60s.
Here are two examples of reforms we want to pursue further. Consensual disposal, where there is no dispute about what happened and the doctor and the GMC agree a kind of dishonourable discharge: “… we won’t go through a whole panel and tribunal, but you will be erased from the register”.
At the moment, if a doctor commits murder or is convicted of rape, we still have go through this whole exercise and waste public money, when the doctor is already in prison, just to take them off the register. We think there are some criminal convictions that should lead to automatic erasure.
So I think it is sad that the Law Commissions’ Bill is unlikely to happen. It looks like regulators for the moment are going to have to keep going with section 60 amendments.
In summary, I think the GMC today, unlike in 1858, can be understood first and foremost as a patient safety organisation. I think that through reforms to the register, which are overdue, a new medical licensing assessment for all doctors practising in this country, more accessible guidance and streamlined fitness to practise procedures we can do much to further protect the public.
Thank you very much. (Applause)