
Abstract
The objectives of this study are to examine trends in litigation related to emergency department care within the NHS. The study is based on retrospective database analysis. NHS Resolution databases of litigation activity pertaining to Type I emergency departments within the NHS are used. The main outcome measures were number of claims, number of successful claims, costs associated with litigation and costs per claim, all in comparison to patterns of ED attendance numbers and inflation. The results showed that the annual cost of litigation relating to emergency department care within the NHS has increased from £25.5 million in 2005/6 to £161.9 million in 2017/18. Mean cost per claim has increased from £58,252 in 2005/6 to £168,966 in 2017/18. The number of claims received has increased significantly; the proportion of these which were successful has remained constant. Therefore, it was concluded that the costs of litigation are increasing disproportionately to inflation and attendance numbers. Multiple potential causes are discussed, with significant implications for clinical practice.
Introduction
The burden of litigation within the National Health Service (NHS) should not be under estimated. 1 There is a significant psychological impact on the staff involved, 2 with 70–86% of medical staff undergoing litigation reporting symptoms of “tension, depression, frustration and anger”. 3 The concept of a “second victim” following medical error is also becoming well recognised in both the literature 4 and the popular press. 5 There are also financial considerations; between 2006/2007 and 2017/2018 clinical claim payments by the NHS rose sharply from £0.4 billion to £2.2 billion, with the number of reported claims doubling from 5400 to 10,600 in the same period. 6 NHS spending on clinical negligence claims is forecast to exceed £3.2 billion by 2020–2021. 7 Both individual and trust indemnity will become increasingly costly in response. 8
Publications examining litigation within the NHS are surprisingly limited; much of the existing literature originates in the United States where litigation has historically been more prevalent.9,10 However, British society is increasingly litigious 11 and an examination of trends within the NHS provides an opportunity to identify and address recurrent sources of patient dissatisfaction, poor clinical outcomes or clinician failings.
In 2017/18 the largest number of claims against the NHS related to Emergency Medicine. 12 Emergency departments (EDs) are pressured working environments with an unparalleled combination of volume and acuity. Presentations are undifferentiated and many time-critical decisions made, sometimes with incomplete information and without the benefit of prolonged observation and investigation. Increasing crowding due to “exit block” and rising hospital bed occupancy has led to increasing burden of risk within the ED. 13 This “perfect storm” of clinical risk has led to an above average rate of litigation in emergency medicine when compared to other specialties. 14
This study analyses data from clinical negligence claims related to ED care in the UK between 2006 and 2018 in order to identify both existing trends and any opportunities to improve practice and patient care.
This represents the first examination of litigation relating to ED care in the UK. Similar studies performed in other countries15,16 raise a number of transferable issues, but differences in models of healthcare provision mean direct comparisons are of limited use.
Method
Data requests were submitted to NHS Resolution (NHSR) using the Freedom of Information (FOI) Act 2000 as per their instruction. Full responses were received with justification provided for any data withheld under the terms of the Act.
Data collected concerned clinical negligence claims relating to ED care between April 2005 and March 2018; these were represented by financial year. The following information was obtained:
Number of submitted claims Number of settled claims Number of successful and unsuccessful claims Cost of claims (including defence costs, claimant costs and damages awarded) Commonest “cause codes” (the aspect of care deemed inadequate) Commonest “injury codes” (the harm resulting from the above)
Data regarding both the causes and the injuries leading to litigation had already been categorised by NHSR.
Data are presented using descriptive statistics where appropriate.
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Results
The total number of clinical negligence claims relating to the emergency department received by NHSR between April 2005 and March 2018 was 14,104. The number of claims received annually has increased steadily from a low of 628 in 2005/06 to a maximum of 1486 in 2013/14 and has remained relatively static in subsequent years. This increase in claim numbers far outstrips the increase that would be expected due to increased attendance numbers (Figure 1).
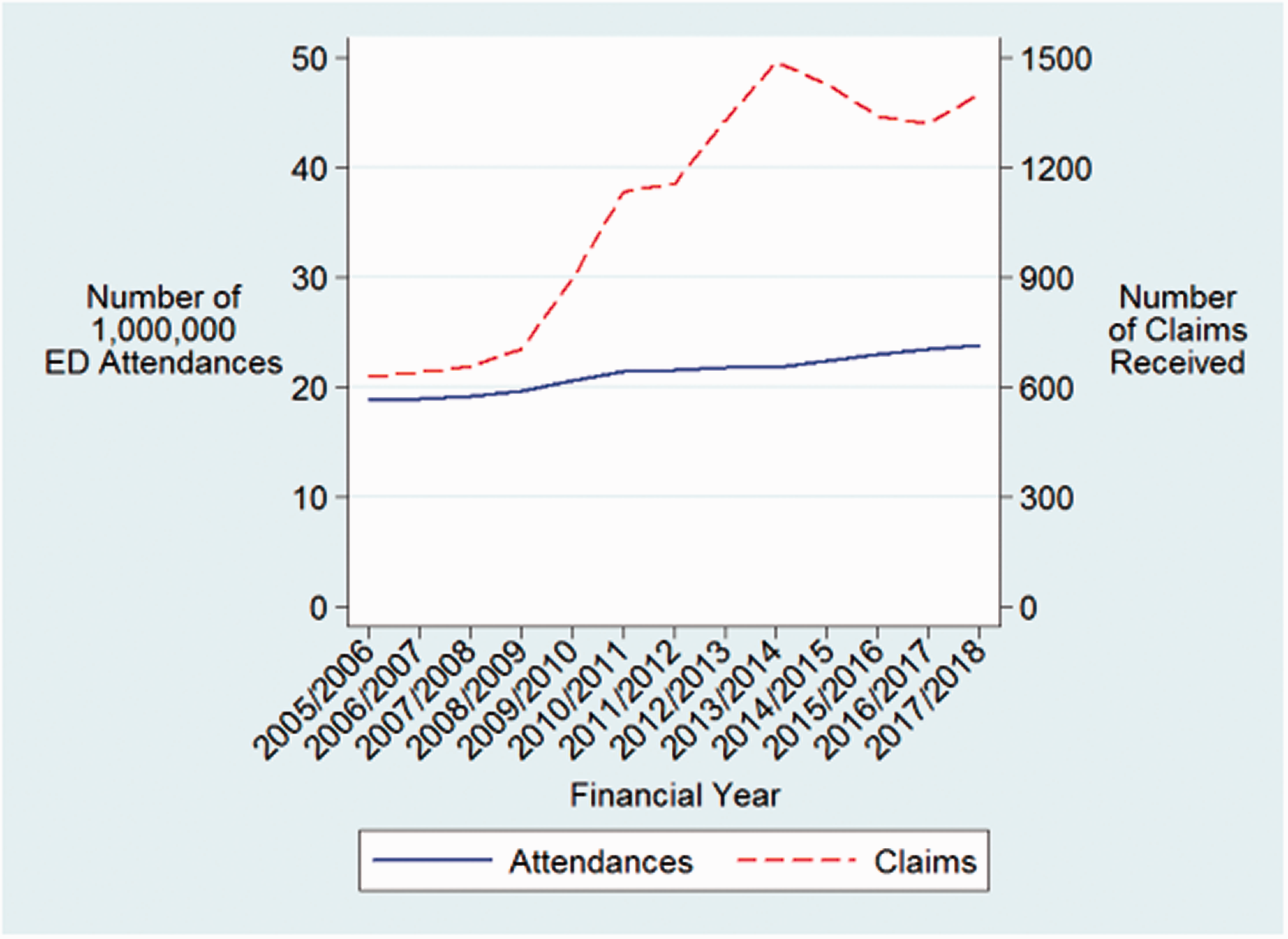
Claims received per year and ED attendances per year.
The number of successful claims (i.e. those where the claimant was successful in securing an award) settled per year ranged from 382 in 2005/06 to 943 in 2016/17, with an overall upward trend throughout the study period. Notably, successful claims (n = 8,356) outnumbered unsuccessful claims (n = 4202) at a ratio of approximately 2:1 over the study period (range 61–74%); this pattern was relatively consistent in individual years (Figure 2).
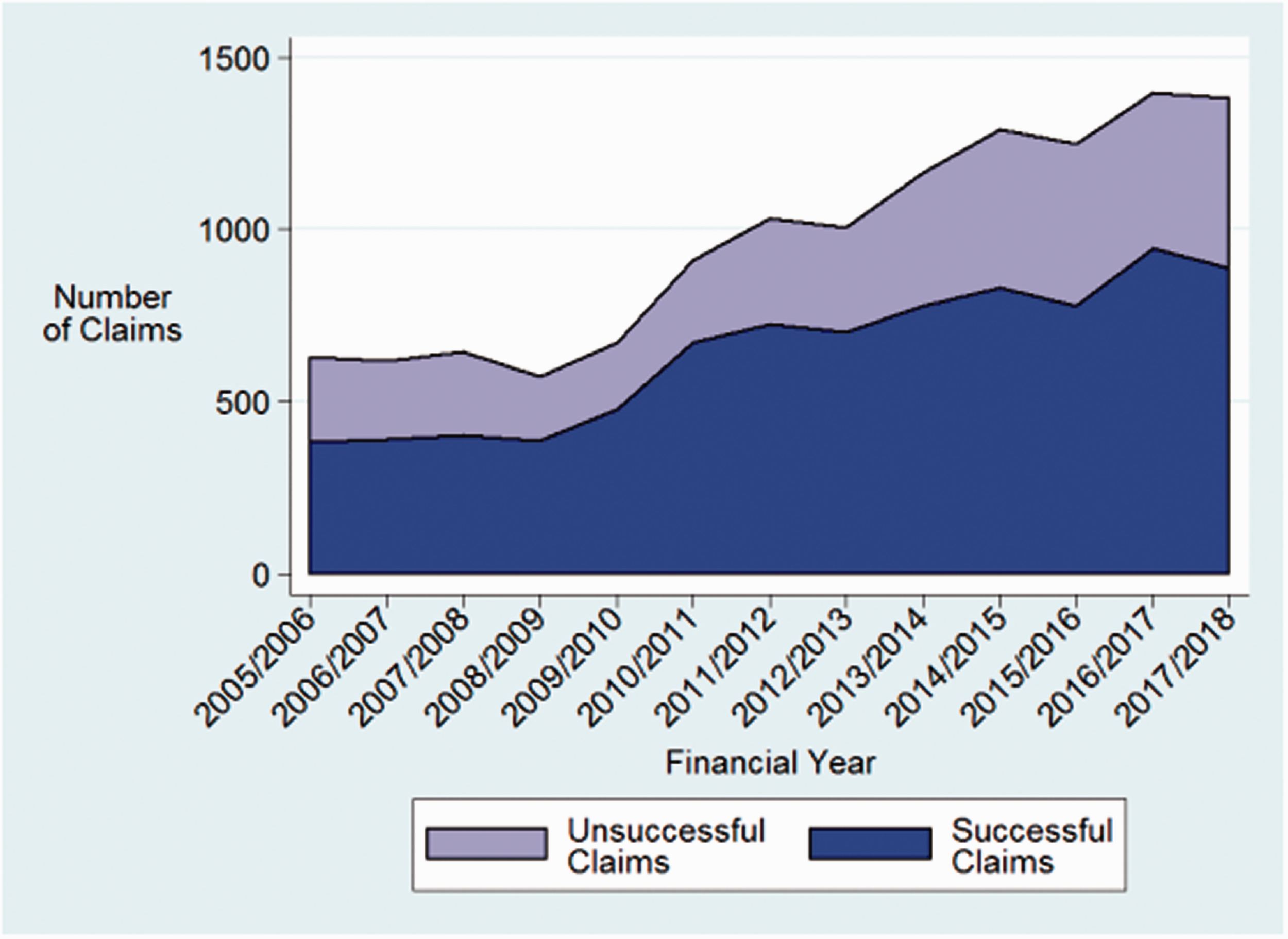
Successful and unsuccessful claims completed per year.
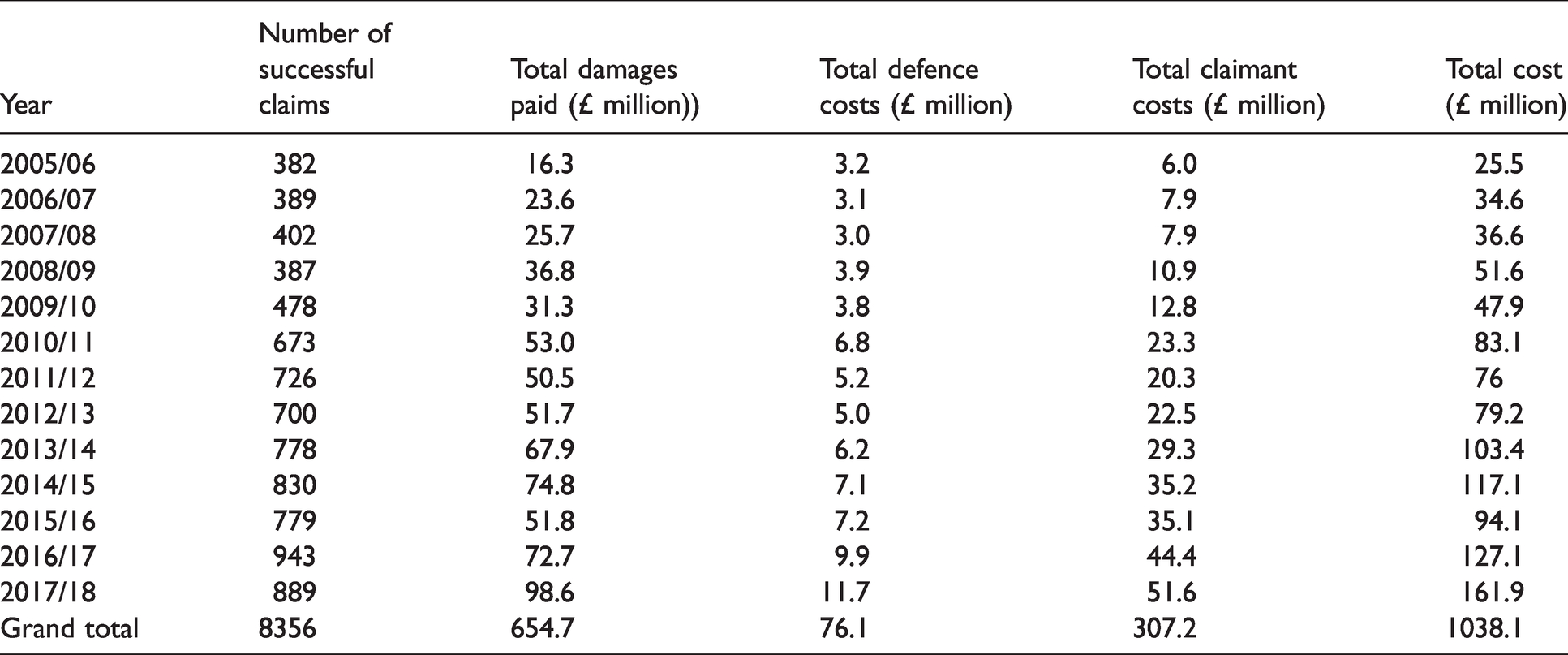
The total financial cost of all completed claims during the study period was £1.038 billion; damages, defence and claimant costs by year can be seen in Table 1.
Costs of completed claims.
The mean cost of a successful claim in each year within the study period increased from £58,252 in 2005/6 to a high of £168,966 in 2017/18 (Figure 3); this rise was significantly greater than that expected as a result of inflation alone. 17 Defence costs are excluded from these figures as the system for their attribution changed significantly in April 2013 with the introduction of Qualified One-Way Costs Shifting (QOCS); as such, trends in defence costs over the study period are difficult to interpret.
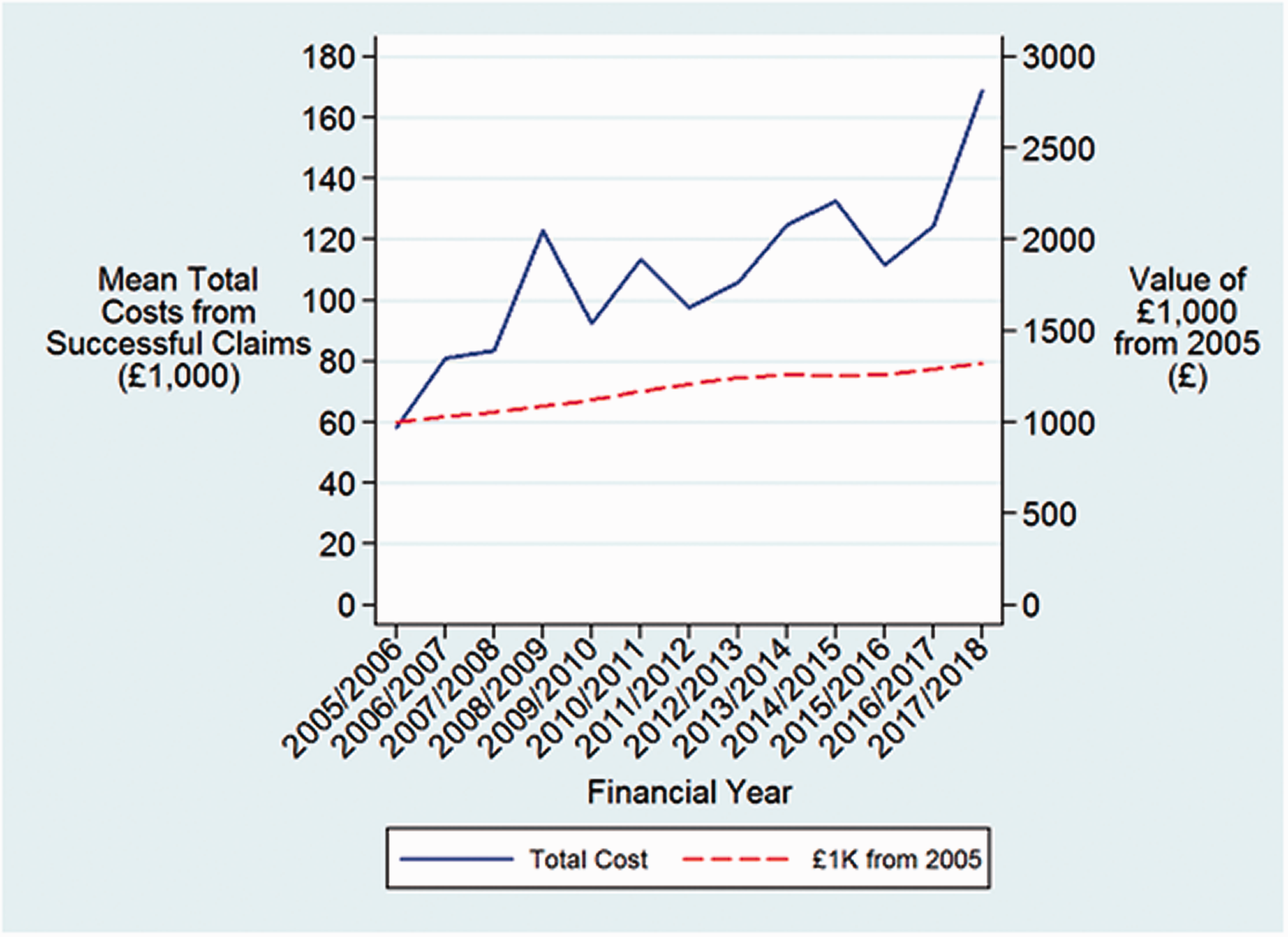
Mean total cost from successful claims vs. inflation represented as the change in value of £1000 over time.
Types of claim
By far the most frequent reasons for litigation were “delay/failure in diagnosis” (3683 [44%]) and “delay/failure of treatment” (1886 [23%]), with “failure to interpret X-ray” (541 [6%]) and “failure to X-ray” (479 [6%]) the third and fourth most common respectively (Figure 4).
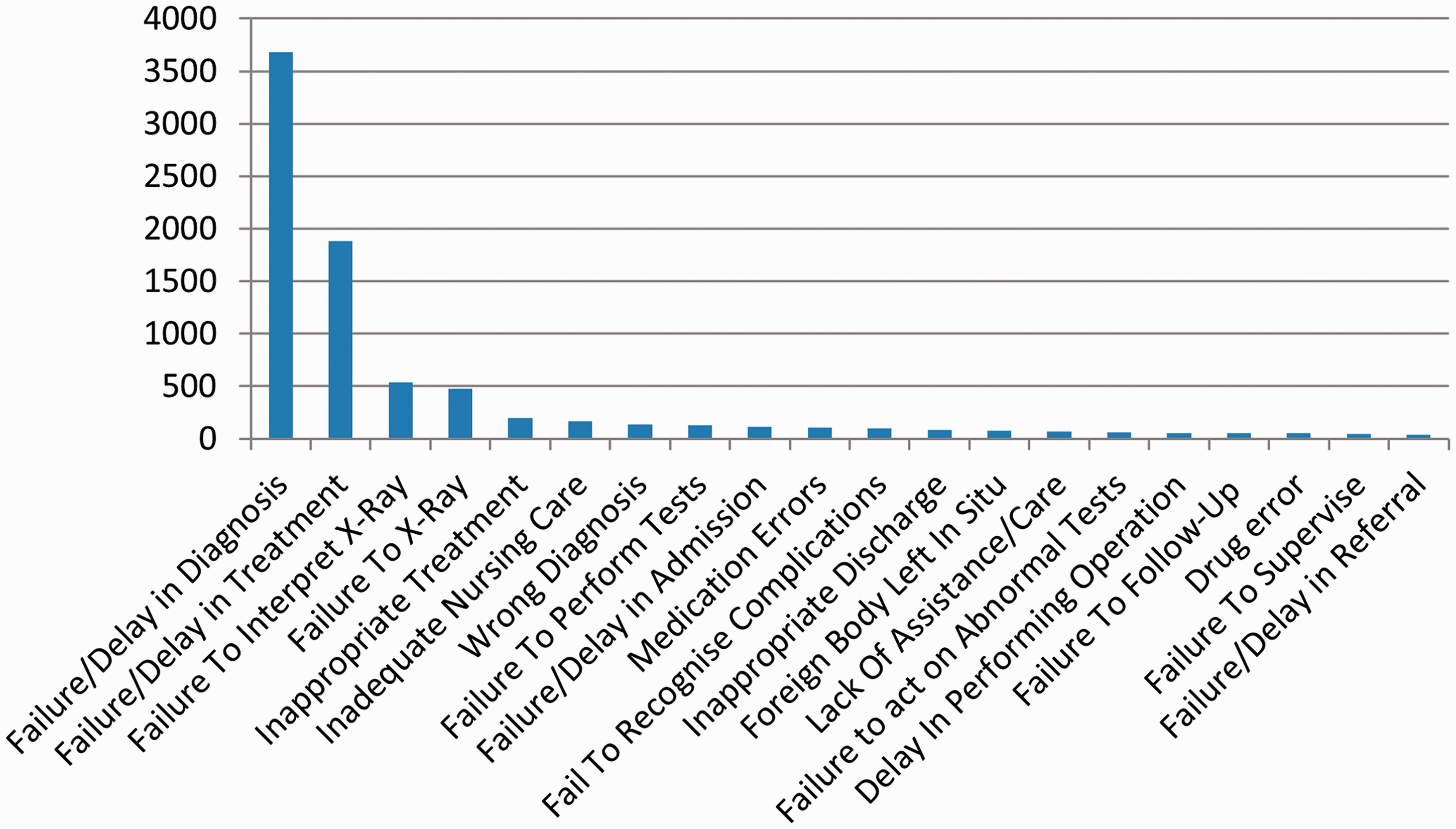
Total number of claims by cause code.
The most frequent injury codes associated with the claims were “unnecessary pain” (1865 [22%]), “fracture” (990 [12%]) and “fatality” (954 [11%]) (Figure 5).
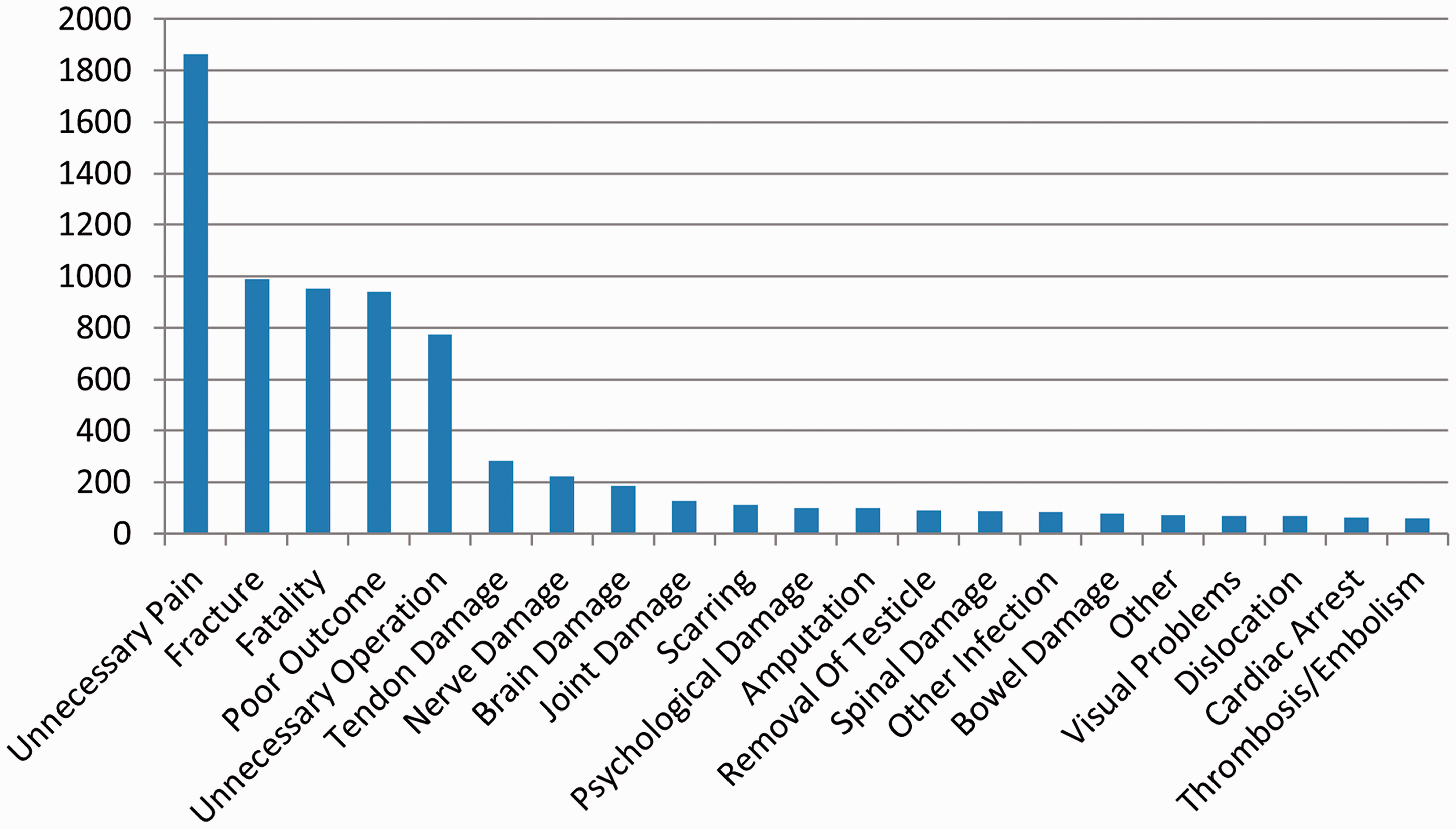
Total number of claims by injury code.
Discussion
The number of litigation claims received regarding ED treatment is increasing disproportionately (118%) to the number of patient contacts (28.6%) and the mean cost per successful claim is increasing disproportionately to inflation. This is leading to an ever-increasing financial cost associated with litigation in the ED. This change is not unique to Emergency Medicine, but can be seen across a variety of specialties. 8
Both trends will clearly have multifactorial explanations and causation cannot be determined by this observational study. Potentially contributory factors include: the increasingly litigious nature of society in general; 18 rising patient expectations; 19 an ever increasing real-terms funding gap for NHS services; 20 and the worsening crisis in staff retention, recruitment and morale (with the unfortunately associated increase in rates of “unprofessional conduct, lack of altruism 21 and increased rates of medical error”). 22 There is also a growing negative perception of the NHS and the medical profession, often propagated by media coverage, 23 that can only serve to worsen the “breakdown of trust in our society” that has been linked to increased rates of litigation. 24
Missed opportunities and poor handling of initial complaints may go some way to explain claimants’ motivations for seeking legal redress after a poor care experience. In one study over two thirds of claimants felt that they had received no explanation for problems experienced during their medical care, and one third felt that they received no apology. Only 6% felt that appropriate actions were taken to prevent similar recurrence of a similar incident in the future. 25
It is possible that increasing access to evidence-based guidelines and clinical standards over the last 20 years may have inadvertently increased rates of litigation. The provision of explicit standards to be met defines any care not achieving these standards as flawed, increasing the likelihood of successful litigation where previously an argument around standard of care would have been much harder to resolve with confidence. These standards are also much more widely accessible and available for both legal teams and patients, with a simple internet search accessing a wealth of national and international guidance. It must be acknowledged that evidence-based medical practice is the accepted gold standard and care that does not meet these standards may well be falling short of best practice. As such, it is possible that historically the rates of clinical negligence claims under-represented the instances of litigable practice and the recent rise in claim numbers merely reflects a rebalancing of the previously paternalistic nature of clinical medicine.
It is perhaps unsurprising that the commonest cause codes for litigation in the ED relate to either “failure/delay in diagnosis” or “failure/delay in treatment”. The time-pressured environment, high volume of patient contacts and multitude of potentially sinister and time-critical diagnoses renders this working environment ripe for this type of complaint. It may well be that these causes for litigation are common themes across many medical specialties; a cornerstone of the physician’s role is to diagnose and treat and it is to be expected that a failure in this area that results in harm will often lead to patient compensation.
The commonest injury code leading to successful claims in the ED is “unnecessary pain”; this is likely linked to the delays or failures in treatment discussed above. One key expectation of many ED patients is for the relief of pain and suffering; 26 indeed, it is also a Royal College of Emergency Medicine (RCEM) quality indicator 27 with very clear associated guidance. It is therefore unsurprising that delayed relief of pain (either through failures in acute management or through inaccurate diagnosis and treatment, e.g. a missed fracture with delayed identification and subsequent impaired healing) leads to dissatisfaction and subsequent legal action.
It is important to note that the ratio of successful to unsuccessful claims appears to be static; the rising number of claims therefore cannot be attributed to an increase in claims destined to be unsuccessful.
This study evaluates litigation rates rather than clinical negligence. Whilst clinical negligence is frequently involved in successfully litigated cases, litigation rates as discussed above are multi-factorial and the events that lead to litigation take place within a complex system. As such, the rate of successful litigation is not a suitable surrogate marker with which to assess quality of care.
Limitations
There would appear to be overlap between a number of cause and injury codes within the NHSR database, and the database is not maintained with research in mind; as such the categories applied to each case represent a broad and subjective generalisation for the underlying causative factors. In reality, the root cause of litigation is seldom so discretely defined with a single identifiable causative factor, but is instead often the result of system failings combined with sub-optimal clinical care and outcome.
NHSR were unable to provide data requested about individual cases (including grade of treating physician and underlying diagnosis) that may have provided useful insight into the circumstances leading to litigation; concern for patient confidentiality rightly took precedence.
The changes to the attribution of defence costs discussed makes analysis over the study period challenging. Given there will be variation in whether the defence costs of claims were chargeable to the NHS (and therefore present in NHSR database), it is also impossible to make reliable evaluations about the cost of defending claims. Data concerning the cost of unsuccessful claims would be particularly useful; these are often seen as a “win” on the part of the clinician and the Trust but still have significant implications. Whilst the financial impact is largely borne by the NHS, the psychological toll on clinicians can, as previously discussed, lead to “tension, depression, frustration and anger” 3 with a potential knock-on effect on both absence rates and the ability to provide optimal care.
Conclusion
The frequency and cost of litigation within the ED is increasing disproportionately to both ED attendance rates and economic inflation. The causes of, and injuries sustained by, cases that lead to successful litigation are largely unsurprising, and some are already a focus for quality improvement nationally. 27
Increasing rates of litigation may lead to increasingly defensive medicine, exacerbating problems of over-investigation and potentially causing both direct and indirect harm to patients.28–30 Given worsening ED crowding, 31 a national shortage of hospital beds 32 and staffing deficiencies, 33 defensive medicine is simply not a viable option in the modern ED environment. This analysis of litigation patterns provides an insight that enables further focus on the underlying causes, a potential improvement in patient care and hopefully a reversal of current litigation trends.
An improvement in complaint management may go some way to reducing the burden of litigation within the NHS; NHSR have identified that “more appropriate reactions, explanations and apologies [after a complaint] would have prevented the need for a claim going forward”. 25
License for publication
The corresponding author has the right to grant on behalf of all authors and does grant on behalf of all authors, a worldwide licence to the Publishers and its licensees in perpetuity, in all forms, formats and media (whether known now or created in the future), to (i) publish, reproduce, distribute, display and store the Contribution, (ii) translate the Contribution into other languages, create adaptations, reprints, include within collections and create summaries, extracts and/or, abstracts of the Contribution, (iii) create any other derivative work(s) based on the Contribution, (iv) to exploit all subsidiary rights in the Contribution, (v) the inclusion of electronic links from the Contribution to third party material where-ever it may be located; and, (vi) licence any third party to do any or all of the above.
Dissemination statement
Results of this study are not directly relevant to any identified patient group or organisation.
Transparency statement
The manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned (and, if relevant, registered) have been explained.
Data availability statement
Data is available upon reasonable request to the corresponding author.
Footnotes
Authors’ contributions
AT conceived the idea for the study. AT and GJ developed the study plan, undertook the literature search, requested relevant data, undertook data analysis, produced the first draft of the manuscript and completed manuscript editing. NT contributed to data analysis and manuscript preparation. MJ supported methodological design and data analysis, and produced figures and tables. AF contributed to data analysis and produced figures. NE provided a legal perspective, contributed to interpretation of data and editing of manuscript. All authors reviewed the final manuscript. AT and GJ act as guarantors for the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was supported by the hosting organisation. There was no formal funding.