
Abstract
Medical errors and adverse effects of treatment are inherent to medical practice. Like any other medical specialty, rheumatology is not exempt. Although the problem is imprecisely quantified, according to some authors it affects up to 10% of hospitalised patients. Describing and qualifying misdiagnoses in rheumatology will help us to understand and reduce these. Further, misdiagnosis generates unjustified costs and medico-legal consequences with errors in initial diagnosis the basis for medico-legal disputes involving assessment of work incapacity.
Introduction
Medical errors and undesirable effects of treatments are inherent in medical practice and quantifying the problem is challenging. The definition of medical error, medical malpractice and iatrogenic side effects has yet to be fully determined.1,2 Several studies document numerous medical errors affecting 10% of hospitalised patients, and an equally alarming number of deaths. 3 A quantitative approach has already been carried out in various medical specialities,4–6 but these do not include rheumatology. Musculoskeletal diseases rank as the second most frequent cause of long-term disability (lasting over a year) in Belgium, comprising around a quarter of all cases. Diagnostic errors in rheumatology may have significant medico-legal and medico-social implications. This study confirms the presence of diagnostic errors in rheumatology and aids the understanding of their causes and outcomes with the aim of improving outcomes.
Material and method
Between end of 2014 and December 2023, cases of unconfirmed rheumatology diagnoses after reassessment were collected from two distinct groups. The first is defined by the collection of unconfirmed diagnoses of rheumatic pathologies observed during medical assessment. The second from the collection of misdiagnoses of rheumatic diseases observed during consultations in a single hospital’s rheumatology department. All the patients were examined by the same practitioner, a rheumatologist since 1991, who specialised in medical review since 1994. The misdiagnosis evaluation was verified through collegial advice given during department meetings. In accordance with Belgian law, the hospital’s Ethics Committee gave approval for the collection of medical data. Since 2014, doctors, with patients’ consent, have access to review all the data and previous medical reports or protocols. The possibility of error is increased when the clinic fails to comply with established criteria for a rheumatological diagnosis. Misdiagnosis is established when patients do not fulfil rheumatoid arthritis classification criteria that guide the diagnosis, 7 the ankylosing spondylitis criteria.8,9 In Belgium, reimbursement of prescribed anti-TNF, anti-interleukin 6 or anti-interleukin 17 treatments is subject to rigorous Social Security regulations. Prescription of these medications is limited to rheumatologists who must have patients’ files that contain a detailed clinical description, a biological examination, an assessment of disease activity 10 using DAS28 scale (disease activity scale of rheumatoid arthritis) and a health assessment quality of life scale (HAQ scale) 11 (health assessment questionaire – rheumatoid arthritis). For ankylosing spondylarthritis the file must include an assessment of functional disability related to the disease 12 using the BASFI Index (Bath Ankylosing Spondylitis Functional Index) and an evaluation of the disease’s activity 13 using the BASDAI index (Bath Ankyloing Spondylitis Disease Activity Index), accompanied by a rise in CRP. Given the absence of established standards identifying false rheumatological diagnosis in the literature, the incorrect diagnosis will rely on a minimum of three out of the six criteria outlined below. These include the objective parameters included in the diagnostic and classification criteria for rheumatoid arthritis and ankylosing spondylarthritis. The lack of a completed self-assessment-questionnaire in the files suggests non-compliance with the regulations for receiving reimbursement for anti-TNF and anti-interleukin drugs in Belgium.
Criteria of false rheumatological diagnosis
Lack of inflammatory syndrome more than three times. Unobserved radiological lesions (absence of erosions, absence of vertebral or sacroiliac lesions for spondylitis). Failure to comply with the rules for prescribing anti-TNF, anti-IL17, or anti-IL6. The absence of fully filled-out self-questionnaire assessing disease activity. Improper use of diagnostic techniques (such as the use of bone scan isotopes to validate arthritis). Analysis of medical data in computerised patient records for the therapeutic sector cohort revealed any absence of lesions and/or inflammatory syndrome.
Results
Medical expertise
See Table 1. The study analyses 9 women (56.25%, average age 54.7 y) and 7 men (43.75%, average age 48 y). The review was motivated by a refusals disability recognition by the SPF Handicap administration (4 judgments), to extend the duration of disability (5 judgments), to assess one post-traumatic rheumatism following a work injury (1 judgment) and assess 6 incapacity for work in the context of guaranteed income insurance. Erroneous diagnoses (14/16, 87.5%) were made in the rheumatology department of a university hospital and 2 (12.5%) in a regional hospital. Initial diagnoses include 8 (50%) ankylosing spondylarthritis, 1 associated with Sjögren syndrome, 5 (31.25%) rheumatoid arthritis, 1 associated with psoriatic arthritis and another one with Sjögren syndrome, 3 Sjögren syndrome, 3 psoriatic arthritis, 1 of which was associated with rheumatoid arthritis. Those associated diagnoses have also not been demonstrated. The self-assessment questionnaires usually carried out twice a year were only collected in 2 cases. Based on these stated diagnoses, 7/16 (43.75%) claimants were treated with anti-TNF or anti-IL6 prescribed, 6/7 in university and 1/7 in regional hospitals. In 6 cases (37.5%), the medical review was requested by the medical advisor of a private insurance company. In 10 out of 16 (62.5%) cases involving legal assessment, the assignment concerned notification of the end of incapacity for work (5/16, 31.25%), a refusal to recognise disability (4/16, 25%), and an assessment of damages in the context of an accident at work (1/16, 6.25%). It should be noted that the final diagnosis was proposed 14 times out of 16 (87.5%) during the medical assessment, based on the medical data transmitted and/or collected. These diagnoses correspond to psychiatric diseases such as post-traumatic stress disorder (2) or depression (7) (9/16, 56.25%). The other pathologies correspond to mechanical low back pain, rheumatism of undetermined origin, skin psoriasis associated with depression, 1 digital osteoarthritis and 1 gout.
Medical review cohort: clinical characteristics.
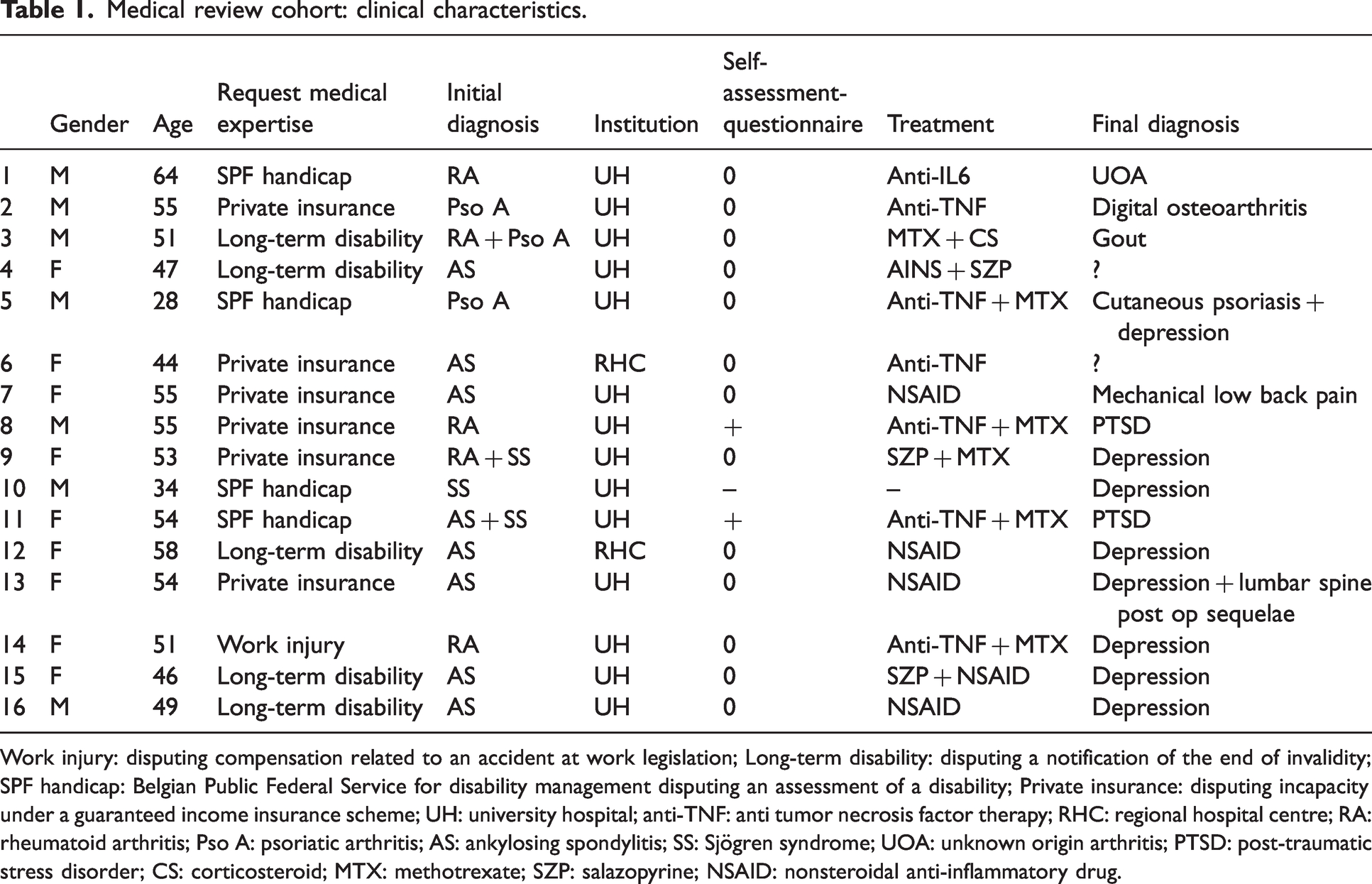
Work injury: disputing compensation related to an accident at work legislation; Long-term disability: disputing a notification of the end of invalidity; SPF handicap: Belgian Public Federal Service for disability management disputing an assessment of a disability; Private insurance: disputing incapacity under a guaranteed income insurance scheme; UH: university hospital; anti-TNF: anti tumor necrosis factor therapy; RHC: regional hospital centre; RA: rheumatoid arthritis; Pso A: psoriatic arthritis; AS: ankylosing spondylitis; SS: Sjögren syndrome; UOA: unknown origin arthritis; PTSD: post-traumatic stress disorder; CS: corticosteroid; MTX: methotrexate; SZP: salazopyrine; NSAID: nonsteroidal anti-inflammatory drug.
Patients seen in consultation
See Table 2. The population consisted of 19 (73%) women with an average age of 51.3 years and 7 (27%) men with an average age of 32.4 years. Misdiagnoses were mentioned more frequently in women than in men. There was also a preponderance of false diagnoses mentioned in university hospitals (14/26, 53.8%) compared with private consultations (8/26, 30.8%) and regional hospitals (4/26, 15.4%). These false diagnoses also justified the prescription of biological treatments in 4 cases (15.4%), 3 of which were prescribed at the university hospital. The initial diagnosis was mainly rheumatoid arthritis (19/26, 73%) (including 1 associated with Sjögren syndrome), ankylosing spondylitis (6/26, 23.1%) and psoriatic arthritis. It should be noted that a therapeutic change was prescribed for 22 of the 26 patients (84.6%) and that a therapeutic abstention was recommended for 4 patients. In the absence of evidence of the rheumatological pathologies initially suggested, the investigations led to the final diagnoses of 8 secondary drug effects, 3 depressions, 1 post-traumatic stress syndrome, 5 cases of major vitamin D deficiency, 3 cases of erosive osteoarthritis, 1 mechanical lumbago, 1 pseudo-rheumatoid arthritis. No diagnosis could be made for 4 patients. It should be noted that 17/26 (65.4%) of this population were not working due to illness, invalidity, pension or career break. Only 5 people were working, including 3 surface technicians. The occupations of 2 patients could not be specified. When the results of the 2 tables are added together, there is a clear preponderance of false diagnoses in rheumatology from consultations at university hospitals (28/42, 66.7%), and prescriptions for anti-TNF and anti-IL treatments are mainly from university hospitals (9/11). Analysis of the expert reports revealed that only 2 out of 16 files included the necessary self-assessment-questionnaires (HAQ, DAS28 for rheumatoid arthritis, and BASDAI-BASFI for ankylosing spondylitis) for the preparation of a file requesting reimbursement for anti-TNF or anti-IL treatment, which in Belgium is required to obtain approval for reimbursement of treatment by Social Security. We should also point out the difference in motivation between claimants in the expert assessment procedure and patients seen in consultation. In the consultation group, 17 out of 26 people were invalids or pensioners, but the reason for the consultation was essentially medical, motivated by the proposed therapeutic ineffectiveness, whereas in the review group, it focused on an assessment of their contested incapacity for work. Let us focus on the fact of the low incidence of other revised inflammatory diseases (only 2 cases of 42) in the two groups.
Consultation cohort: clinical characteristics.
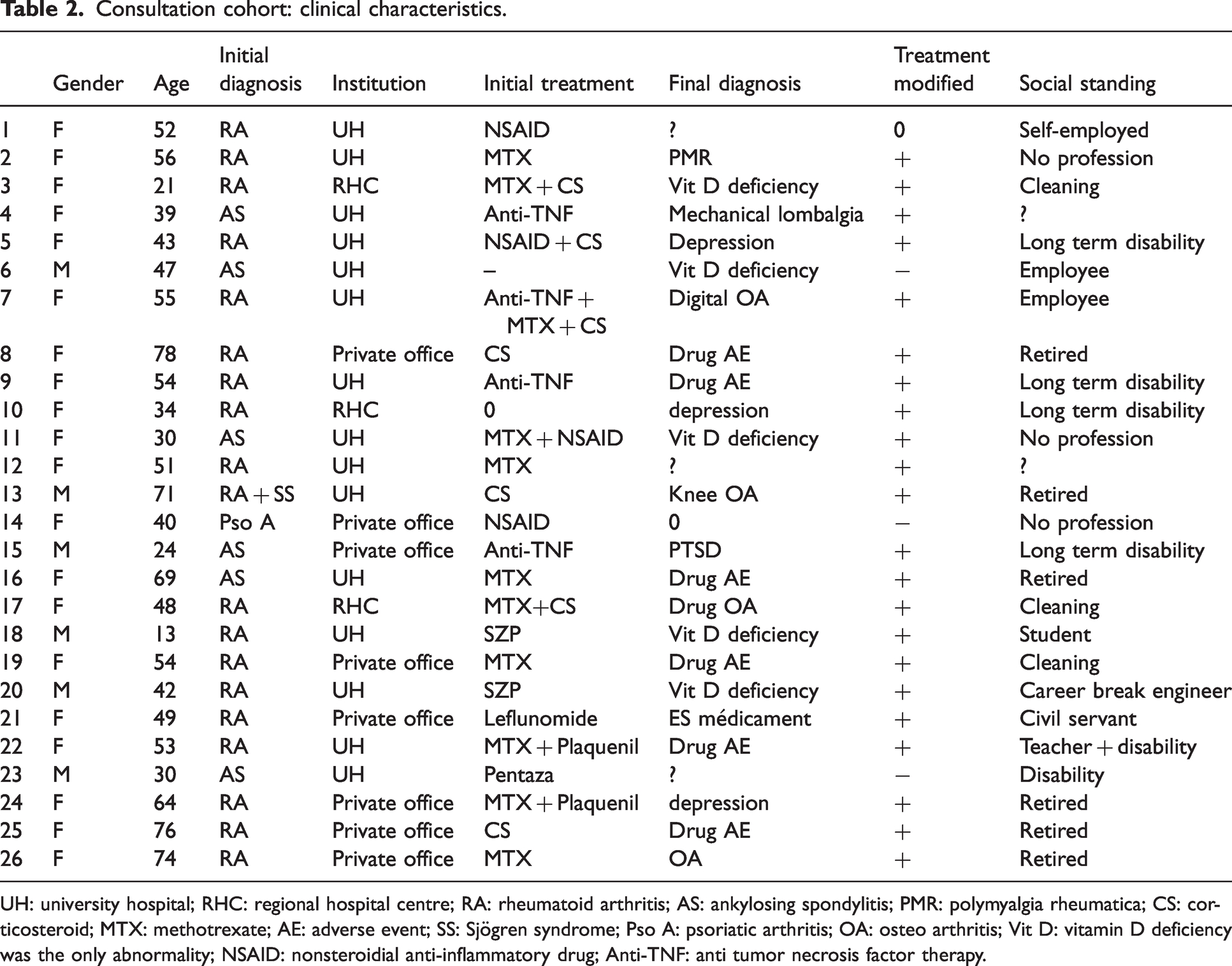
UH: university hospital; RHC: regional hospital centre; RA: rheumatoid arthritis; AS: ankylosing spondylitis; PMR: polymyalgia rheumatica; CS: corticosteroid; MTX: methotrexate; AE: adverse event; SS: Sjögren syndrome; Pso A: psoriatic arthritis; OA: osteo arthritis; Vit D: vitamin D deficiency was the only abnormality; NSAID: nonsteroidial anti-inflammatory drug; Anti-TNF: anti tumor necrosis factor therapy.
Table 3 describes the percentages of diagnostic errors, anti-TNF or anti-IL treatments prescribed, psychiatric and inflammatory pathologies.
Percentages of diagnostic errors, anti-TNF or anti-IL treatments prescribed, psychiatric and inflammatory pathologies (final diagnosis).
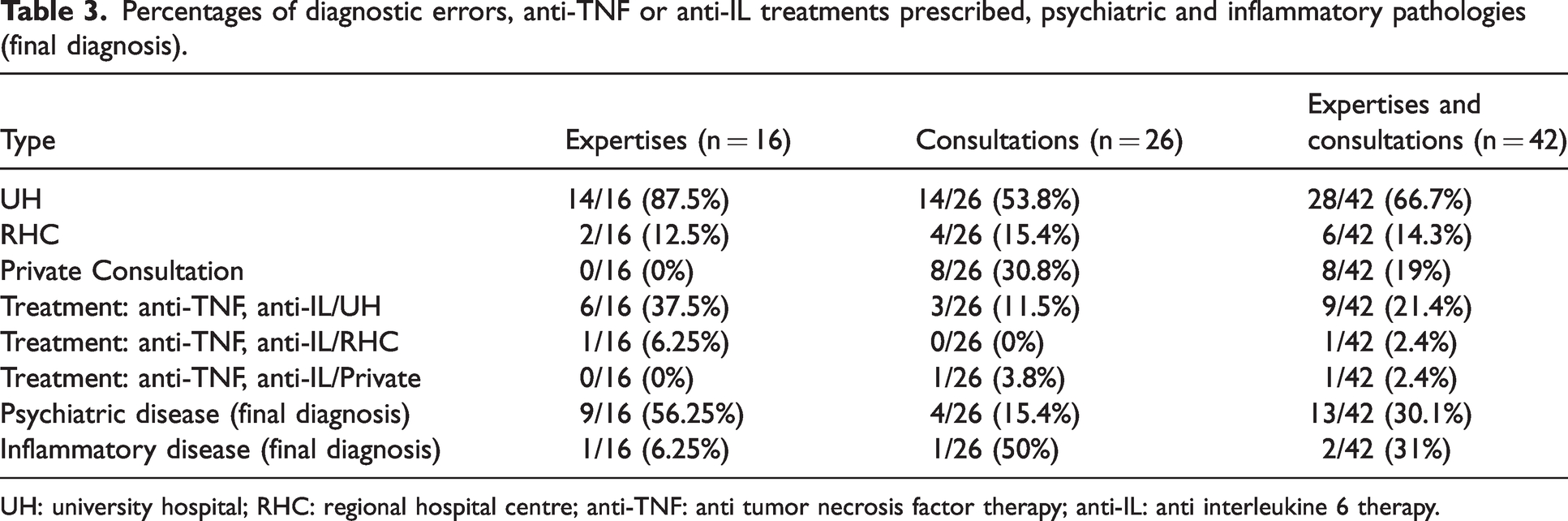
UH: university hospital; RHC: regional hospital centre; anti-TNF: anti tumor necrosis factor therapy; anti-IL: anti interleukine 6 therapy.
Discussion
The study’s weakness stems from its inherent nature, as well as the fact it was conducted by a single investigator experienced in rheumatology and medical review. Research on misdiagnosis is rare, irrespective of the medical specialty, while it seems to be on the increase. The US Food and Drug Administration is encouraging consumers of medical products to report errors, malpractice, iatrogenic pathologies, and treatment-induced side effects. 1 The subject remains a delicate one to tackle and is probably underestimated, especially as medical errors may be associated with symptoms of depression found among practitioners.14–15 This study merely reveals the existence of diagnostic errors in rheumatology but lacks an epidemiological design and does not specify the percentage of erroneous diagnoses made by rheumatologists. Complex disorders such as rheumatoid arthritis or spondyloarthropathies can be misdiagnosed. The rationales behind the phenomenon necessitate thorough examination to minimise the risk of errors (which can be applied to other specialties). The elevated proportion of misdiagnosis stemming from university departments can be explained both by the size of the department and the higher number of practitioners managing more consultations. Nevertheless, this explanation does not appear to be the sole factor, as shown by the absence of self-assessment-questionnaires in 13/15 forensic cases and the failure to demonstrate a diagnosis in the case of Sjögren’s syndrome despite repeated normal biological tests and in the absence of any abnormality on biopsy of the accessory salivary glands. Within the forensic group, anti-TNF and anti-IL treatments were prescribed by university hospital practitioners (6/7), although the available diagnostic and monitoring tools were not used, even though these are required to obtain financial coverage by Social Security. These findings reveal an erroneous interpretation of good rheumatology practice.
Incorrect diagnoses were the primary cause for the medical review, and therefore generated indirect, non-medical expenses on the part of public (10/16 reassessment cohort, 6/26 consultation cohort) and private (6/16 expertise cohort, 0/26 consultation cohort) insurers. Most clinical trials related to inflammatory rheumatism are conducted in university hospitals, where the investigators receive compensation through the hospital. However, the actual impact of pharmaceutical companies on this subject cannot accurately be quantified. Consequently, investigators would be inclined to overestimate rheumatic diseases, knowing that diagnosis criteria do not have absolute sensitivity and specificity. Practitioners would apply them without taking account other pathologies. Further, the subjective dimension of assessment grids in rheumatology is important. For instance, rheumatologists use the DAS28 and HAQ questionnaires, which are directly influenced by the subjective experience of individuals to assess the therapeutic follow-up of rheumatoid arthritis. The quantification of BASDAI and BASFI questionnaires for ankylosing spondylitis is equally dependent on the participation of the applicants. 16 Within the framework of a judicial review, when these forms are filled in, the patients themselves, interested in the importance of their complaints, tend to overestimate their functional handicap. Unaware of this initial subjectivity, a university practitioner wishing to involve patients in a clinical study is inclined to diagnose a rheumatic pathology in patients expressing the most subjective complaints which will then be documented in a report from the therapeutic sector used in medical assessment. The written reports generated by the university validate the discordance between complaints and objective examinations, such as an absence of inflammatory blood tests and/or a lack of joint erosion. The impact of cognitive biases, including confirmation bias,17–18 is also underestimated. Cognitive biases influence a group’s general thinking and the practitioner’s ability for independent thinking and diagnostic process. In cases of diagnostic error, the factual elements, such as the normality of the biological or radiological tests, are disregarded. The academic setting inherently encourages the diagnosis of inflammatory diseases. This would explain the preponderance of prescribing biological therapy by academic rheumatologists in this context, which is present in the medical review group, in contrast with the consultation group; this escalation of treatment will be used as evidence by the claimant to support his case. The expert assessor is faced with medical reports attesting to a pathology that he is unable to validate and his report will contradict the many reports provided by the claimant. This may cause the court to question the thoroughness of the assessor’s conclusions.
This study reveals the frequency of active psychiatric pathology, post-traumatic stress disorder, and depression, especially in the medical review group (9/16, 56.25%) which probably explains the inflated score of the evaluation scales provided. Within this context, psychiatric pathology and diagnostic errors appear to be the two primary causes of the disagreement justifying the medical review. 19
In conclusion
This study of medical error is the first of its kind in rheumatology. Although not an epidemiological study to quantify the percentage of diagnostic errors in rheumatology, it does demonstrate the existence of false diagnoses in rheumatological practice. These might be inherent in the use of diagnostic criteria and guidelines without critical analysis. It is notable that there was a failure to complete and provide rheumatological self-assessment-questionnaires. The higher frequency of misdiagnosis from university departments has probably a multifactorial origin, involving cognitive biases mechanisms, academic performance pressure, the influence of pharmaceutical companies promoting expensive biological treatments, the need for cases to be included in paid clinical research, and probably a lack of a culture of personal feedback concerning the diagnosis of the disease itself. Indeed, teaching good rheumatology practice is conducted by university practitioners, who are not challenged. Put simply, it is the responsibility of any rheumatologist, to challenge their own diagnosis in the absence of objective elements such as the absence of blood inflammatory syndrome or radiological signs. These shortcomings in practice have medico-legal implications; diagnostic errors contribute to avoidable healthcare costs, including the prescription of expensive treatments and prolonged claimed job disability. These inaccurate diagnoses are also the primary prompt for judicial medical review. The medical review expert’s final report does not accord with multiple medical reports from the therapeutic sector, predominately from universities. For these reasons, the expert’s report must include all comprehensible information based on a review of the objective medical data contained in the individual’s file and collected during the assessment. By adopting this approach, the final report can be educational and understood by all the parties and the tribunal.