
Abstract
Adverse reactions to metal debris are inflammatory-necrotic changes that can occur in individuals with joint prostheses, particularly hips. They are triggered by the release of metal debris at both the periprosthetic tissue level and systemically. This was internationally recognised by 2012: several recommendations followed. Patients were advised to undergo careful clinical, laboratory and radiological follow-up with the potential need for prosthetic revision surgery. Concurrently, the primary manufacturers issued safety notifications and began recalling some prosthetic devices from the market. Notwithstanding, prosthetic implants with metal components continue to be widely used due to their favourable risk–benefit profile. We examined the cases of three patients whose hip arthroplasty had metal-type implants. Following the development of adverse reactions to metal debris, they underwent early prosthetic revision and even surgery to remove the prosthesis and clean up metal debris. Consequently, the patients requested a medico-legal evaluation to obtain compensation for the damage suffered. The investigations conducted in these three cases resulted in different allocations of liability: one to the manufacturing company, one to the healthcare professionals who treated the patients, one shared by both. This illustrates that, even after the risk has been identified, it remains a pertinent issue and provides insight into potential future scenarios regarding professional liability cases of a similar nature.
Keywords
Introduction
Hip prostheses contain multiple components that are either dynamically or statically related to one another. These may be classified as dynamically related (e.g. the femoral head and acetabulum) or statically related (e.g. modular elements). In the event that the components are made from contiguous metal elements, the prosthesis is designated as “metal-on-metal” (MoM). MoM prostheses (available since the late 1990s) offer some advantages over traditional implants so are still considered favourable in terms of risk–benefit for some patients. However, these advantages are offset by potential adverse effects associated with the release of metal ions.
The term ARMD (adverse reaction to metal debris) is used to describe the phlogistic-necrotic changes that can occur in individuals who have undergone MoM arthroplasty, particularly in their hips. The friction generated between the surfaces results in the release of metal debris, which accumulates in the tissue and is distributed systemically. 1 ARMDs may cause various pathological manifestations, which can also occur simultaneously. These include metallosis (excessive wear of the arthroplasty due to periprosthetic accumulation of metal debris, resulting in pain, failure of the prosthesis, and the need for early revision) and pseudotumour (solid- or liquid-component masses containing metal debris in soft tissues adjacent to the implant). Further, aseptic lymphocytic vasculitic-associated lesions (ALVAL) may occur, which are characterised by necrosis associated with macrophage, giant cell and diffuse perivascular lymphocytic reactions, leading to the destruction of periprosthetic soft tissue with potential involvement of multiple organs, particularly the capillary circulation at the retina, nerve tissue, kidney and bladder. 2
In 2012, safety concerns associated with metal prosthetic implants were brought to the attention of leading international orthopaedic scientific societies, 3 namely the Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR) and the European Commission. 4 In 2014, the committee had determined that all types of MoM hip replacements released metals which could cause adverse effects at both the local and systemic levels. 5 In 2015, Italy drew public attention to the issue through a dedicated page on the Ministry of Health website. 6 The following year, the Italian Society of Orthopaedics and Traumatology (SIOT) published a special paper on large-diameter MoM prostheses. 7
Concurrently, since 2012, manufacturers have issued safety advice and market recalls of some prosthetic implants, due to the potential risks associated with wear and tear and the production of metal debris. It was also recommended that surgeons using such implants subject patients to careful clinical, laboratory (haematochemical analysis including metal ion levels) and radiological (high-resolution techniques) follow-up. These examinations were to be repeated even when initial results are in the normal range. Should they reveal an ARMD, prosthetic revision should be considered.8,9
The cases described below concern three patients who underwent hip arthroplasty with metal-type implants. Several years after surgery, they began experiencing ARMD, which caused significant impairment. They sought a medico-legal evaluation to determine liability and obtain financial compensation.
Case descriptions, follow-up and outcomes
Case 1
A 65-year-old man underwent a correctly placed hip arthroplasty (modular MoM implant) in 2009 for high-grade right coxarthrosis. In 2010, prior to the identification of ARMDs, the patient presented with a history of right hip swelling. An ultrasound examination revealed an extensive pseudo formation with a liquid component infiltrating the greater and middle gluteus muscles. Six years after surgery, when ARMDs were well recognised, the radiograph revealed bone rarefaction at the trochanteric site, which was attributed to metallosis. At approximately ten years post-operatively, due to elevated blood levels of cobalt (Co: 3.40 mcg/l with VN < 1 mcg/l) and advancing osteolytic processes visible on radiologic images, the patient underwent a right hip revision (Figure 1), resulting in a 3 cm hypometria of the right lower limb. The patient currently presents with coxalgia, hyposthenia and a functional deficit in the right lower limb, with a significant impact on both static and dynamic incidences, as well as negative repercussions on the patient’s existential and relationship life.

(Colour.) Patient 1’s prosthetic implant exhibited advanced deterioration following its removal after ten years.
Case 2
A 54-year-old woman was diagnosed with bilateral high-grade coxarthrosis in 2010, more severe on the right side. She was recommended for surgical replacement with a prosthetic device. Subsequently, a modular metal-on-metal prosthesis was implanted in her right hip in 2011. In 2013, her left hip was also prosthesised with a non-modular implant (Figure 2). The postoperative course was uncomplicated in both cases. However, the patient was neither informed of the safety warnings and recall actions initiated in 2012 nor subjected to appropriate clinical, laboratory or radiological follow-up. In 2018, due to the onset of pain and functional limitation in the right hip, an MRI was performed (Figure 3), which detected a neoformation adjacent to the right prosthesis with involvement of the iliopsoas muscle. However, this was subsequently identified as a pseudotumour resulting from metal debris accumulation. In 2020, the patient was finally subjected to the appropriate blood tests, which revealed elevated levels of chromium (Cr: 0.97 mcg/l with VN < 0.1 mcg/l) and cobalt (5.90 mcg/l). Consequently, within a relatively short timeframe (less than 10 years following implantation), the patient had to undergo a series of surgical procedures, including the removal of the right arthroplasty with tissue clearance of metal debris and the application of a spacer, the removal of the pseudotumour through lumbotomy (a particularly invasive procedure), and, finally, the replacement of the right hip (Figure 4). Currently, the patient’s mobility is significantly impaired and she needs assistance with some basic activities of daily living.

Patient 2’s postoperative radiological control of right (modular) and left (non-modular implant) hip arthroplasty.
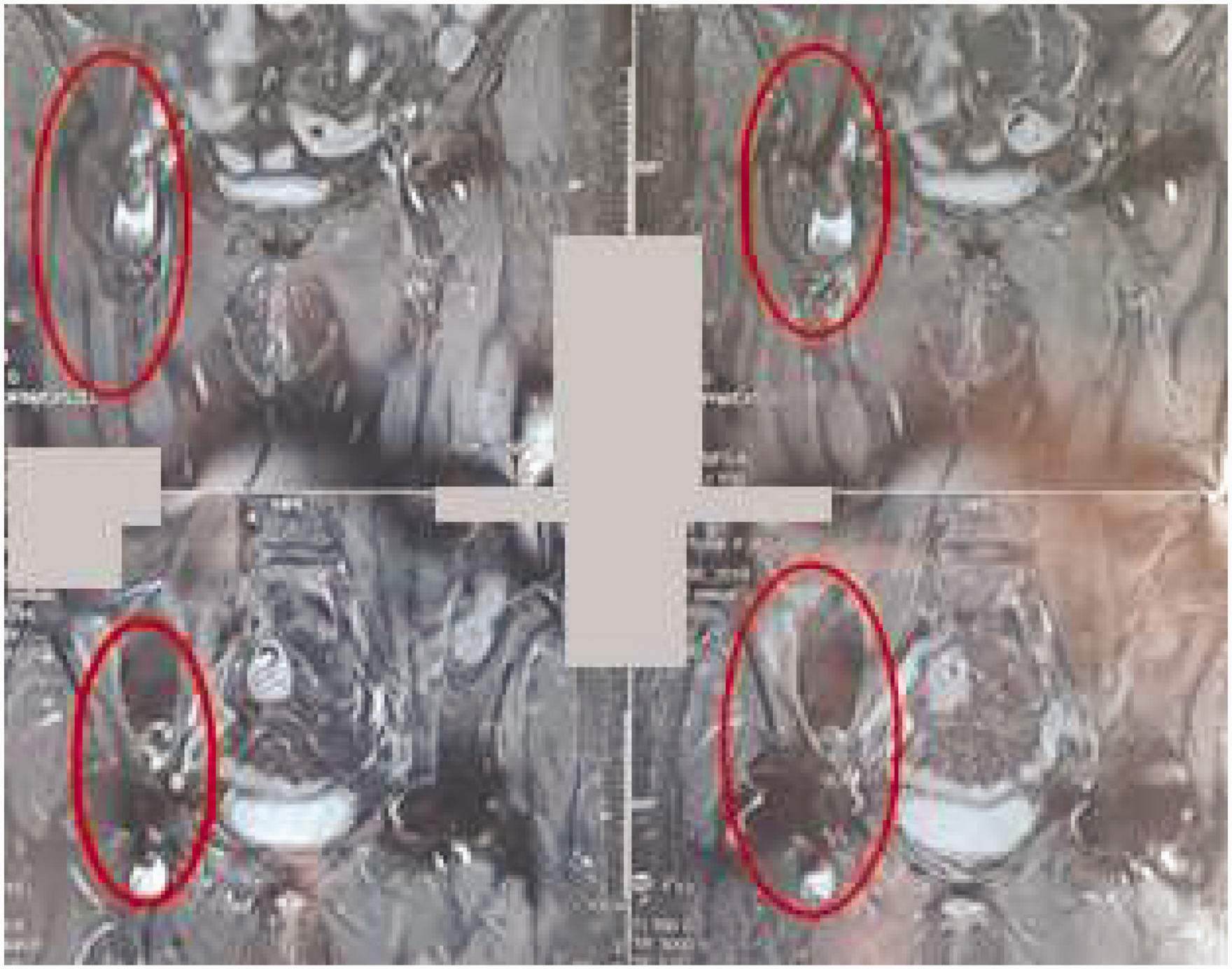
Patient 2’s MRI performed in 2018 for onset of pain and limitation detected the presence of a pseudotumour due to accumulation of metal debris, which was not recognised as such until 2020 when blood tests were performed with findings of elevated levels of chromium and cobalt.

Patient 2’s most recent radiographic review following right arthroplasty removal with tissue cleanup of metal debris during lumbotomy, hip reprocessing and spacer placement.
Case 3
In 2014, a 38-year-old woman was diagnosed with severe early left coxarthrosis. The following year, she underwent MoM Cr-Co type hip resurfacing arthroplasty (HRA) surgery on her left hip (Figure 5). This was carried out after appropriate information on the risks associated with the type of prosthesis to be implanted was provided and valid consent was obtained. The post-operative course was uncomplicated, and the patient underwent the requisite clinical and laboratory follow-up. However, follow-up radiological investigations were inadequate, as they employed only radiography instead of high-resolution techniques. In 2017, the patient presented with systemic symptoms (nausea, vomiting, headache) and underwent prosthesis loosening (Figure 6). It was only through the implementation of a comprehensive level II laboratory and instrumental investigation that metallosis with pseudotumour was identified. Consequently, a revision right hip arthroplasty was performed that year, resulting in the implantation of a total prosthesis (Figure 7) and the removal of the pseudotumour. Currently, the patient presents with symptoms of coxalgia and joint limitation of the left coxofemoral joint, accompanied by ipsilateral lameness.

Patient 3’s radiological control of left hip after HRA surgery with MoM Cr-Co type coating.
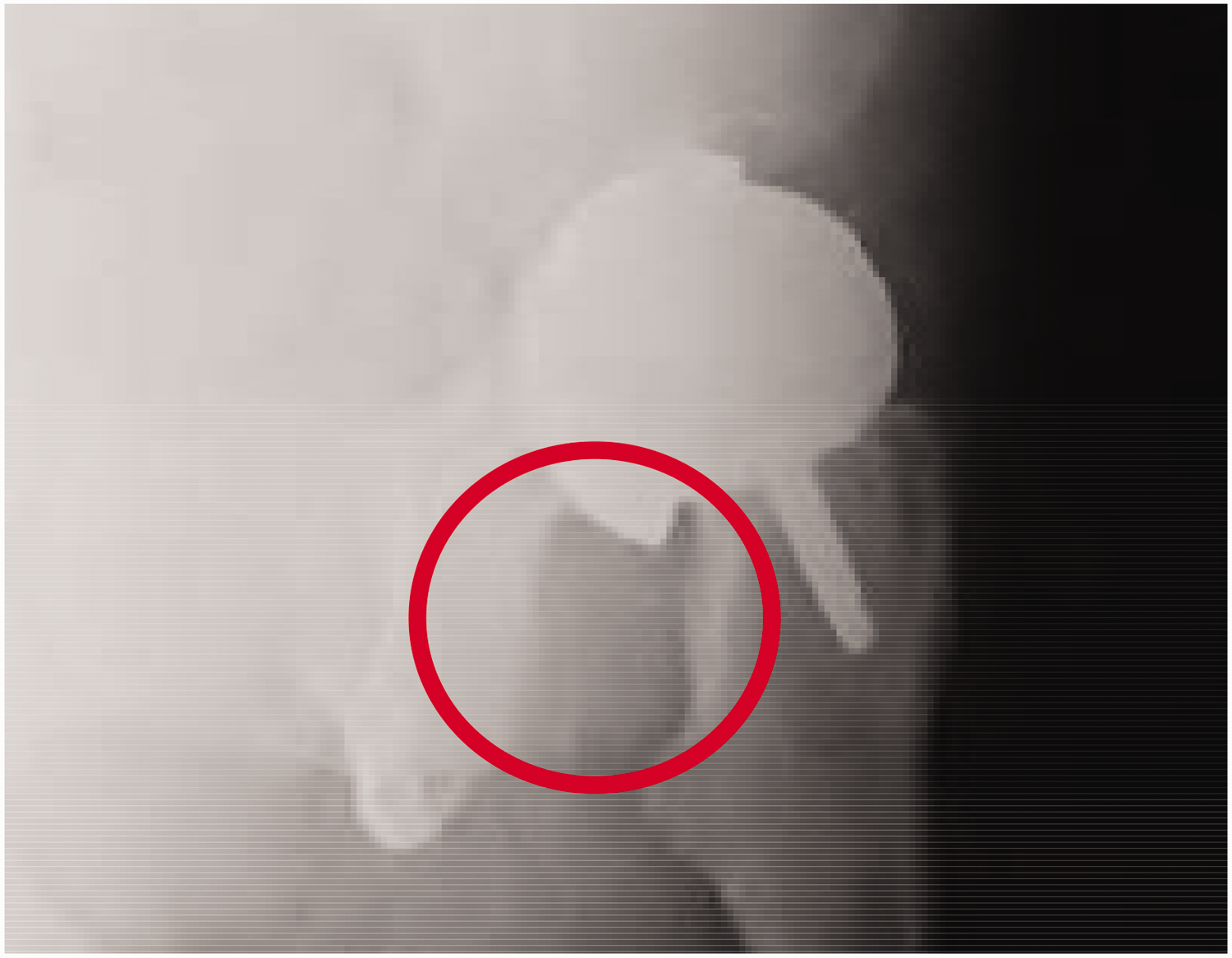
Patient 3’s radiological control that showed prosthesis loosening.
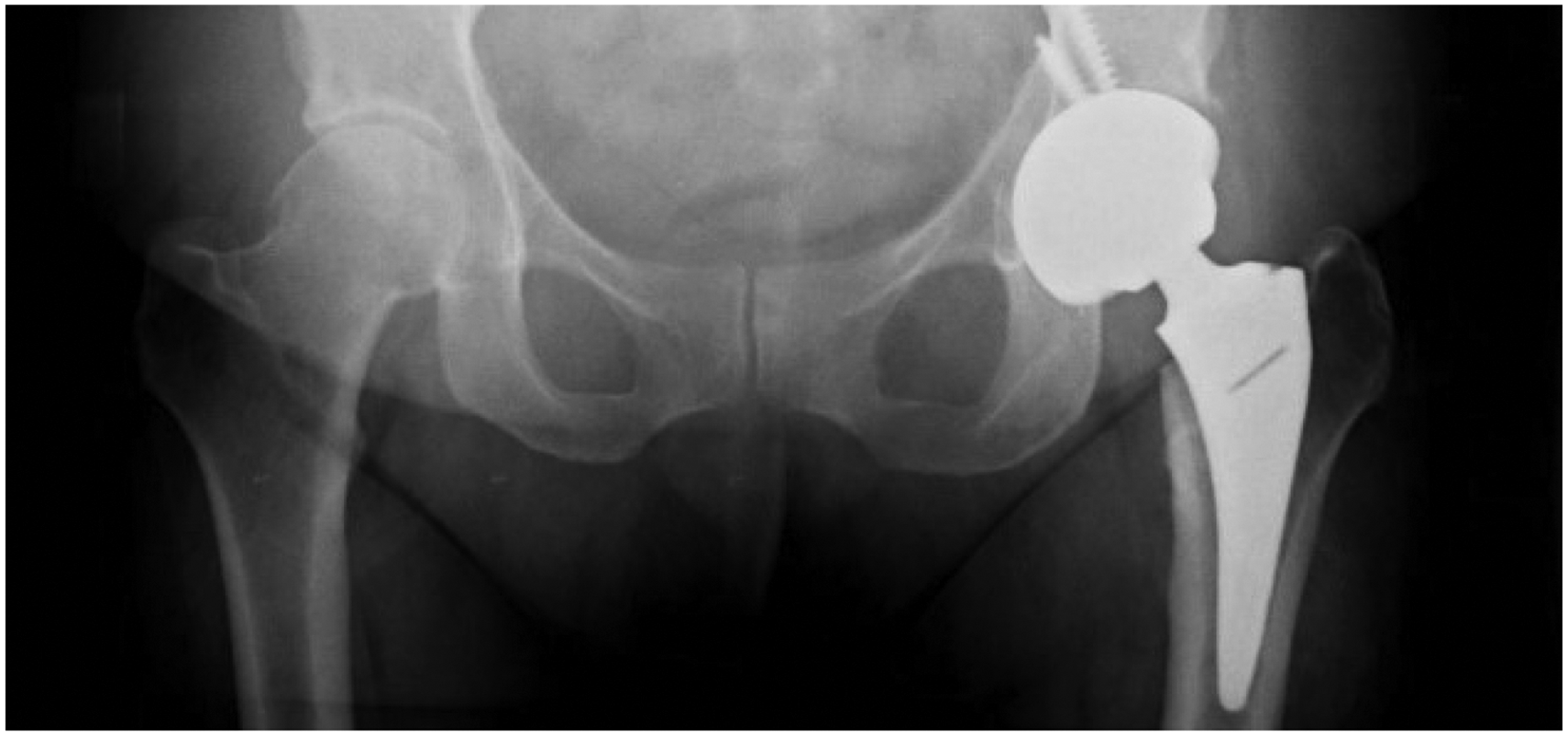
Patient 3’s radiological control conducted after revision of right hip arthroplasty with total prosthesis and pseudotumour’s removal.
Discussion
The choice of prosthetic material for joint replacements depends on the specific site. Hips require materials that integrate well with the bone and have high hardness and corrosion resistance. Cobalt-based alloys such as cobalt-chromium-molybdenum (Co-Cr, Co-Cr-Mo) and cobalt-chromium-tungsten-nickel (Co-Cr-W-Ni) are commonly used as they have these desirable characteristics. 10 MoM prostheses have advantages over conventional implants, including lower risk of issues like osteolysis, wear, and fracture. Studies in the early 2000s showed the efficacy of MoM prostheses, highlighting their better primary stability and reduced incidence of loosening and dislocation. 11 Large-diameter heads (>36 mm) and surface replacements allow for greater stability and range of motion, and lower risk of dislocation and fracture, compared to conventional heads. 12 Additionally, they result in less bone loss on the femoral side and offer anatomical and functional preservation of the hip joint. These advantages also contribute to shorter follow-up durations and decreased hospitalisation risk.13–16
Despite their well-recognised advantages, since 2012 it has been noted that friction between prosthetic surfaces can lead to the release of metal debris which may result in local tissue accumulation and the development of ARMD, with rare cases also exhibiting systemic effects. Importantly, this phenomenon is not limited to MoM prostheses but can also occur with metal-polyethylene or metal-ceramic combinations. However, in these heterologous couplings, the risk is lower due to the release of fewer and larger, less diffusible, metal particles. 1 Nonetheless, MoM prostheses remain in clinical use, particularly in younger patients, where their benefits are often considered to outweigh the risks.
Currently, international guidelines provide a framework for classifying patients by risk category and recommend standardised protocols for the use and monitoring of MoM implants. These include clinical assessments, laboratory tests and imaging studies to ensure the safety of individuals with existing implants or those being considered for them.17–19
Early detection of ARMD relies on a combination of clinical evaluation (noting nonspecific symptoms such as joint pain, functional limitations, nausea or headaches), haematochemical analysis (serum metal ion levels, which may not always correlate with disease severity), and advanced imaging techniques such as magnetic resonance imaging (MRI) and bone scintigraphy. These imaging methods are particularly effective for identifying structural complications, including pseudotumors, periprosthetic osteolysis, and muscle necrosis, at an early stage.
Prompt diagnosis and prosthetic replacement represent the most effective treatment options currently available for patients who have experienced adverse reactions to MoM prosthetic implants. Prompt intervention can mitigate the risk of joint damage and the incidence of reactive vasculitis in surrounding muscles and vital organs. Nevertheless, the prognosis for prosthetic implants that cause metallosis is less favourable in terms of durability and overall health, due to the depletion of bone marrow and damage to surrounding tissue caused by metal debris.20,21
In Italy, civil damages claims for ARMDs following the implantation of MoM prostheses are common, particularly where patients received these implants prior to 2012. A case-by-case examination is essential for a comprehensive medico-legal assessment, which aims to determine the appropriate allocation of responsibility. It is crucial to recognise that the aetiology of ARMDs is not solely attributable to faulty devices or improper medical conduct, as these factors may interact at various levels.
In the context of professional healthcare liability in Italy, the initial step in the medico-legal evaluation is to ascertain whether there was any misconduct on the part of the healthcare providers involved in the patient’s treatment. In the event that such conduct is identified, it is then necessary to prove a causal link between the misconduct and the reported damage. In the context of compensation, the incremental differential damage method is employed when there is a need for precise allocation among the responsible parties or when the impairment being assessed relates to a pre-existing condition. This allows only for the augmented biological damage resulting from substandard healthcare provision to professional liability, and the party responsible is liable for the incremental value of the impairment caused.
In the above cases, the primary diagnosis, surgical indication, and choice of prosthesis were appropriate. This is true even in cases 1 and 2, as the selection of the modular presidium was made prior to the issue of safety warnings in 2012 and the subsequent recall of these products. Further, the surgical procedure itself was correctly performed.
With regard to patient 1, he was promptly informed of the situation regarding the modular prostheses in 2012. Consequently, the patient underwent appropriate clinical, laboratory and radiological follow-up. The patient then underwent prosthetic revision when symptoms worsened, consistent with the guidelines then in force. It was concluded that the greater iatrogenic damage was not due to any misconduct by the healthcare providers but solely due to the marketing of an implant type by the manufacturing company that was later found to be unsafe for patients.
In contrast, patient 2 was never informed of the situation regarding the modular prostheses. This was despite the fact that the staff who treated her could not have misunderstood the circumstances. It should be noted that safety notices are sent to all hospital facilities that use them. These specify the defective lots with their respective code numbers. These numbers are to be compared with those on the labels applied in the medical records. This is to identify the patients to be informed and monitored. In addition to the failure to inform, patient 2 did not undergo the planned clinical, laboratory and radiological follow-up. As a result of this diagnostic delay, her condition worsened significantly, necessitating multiple surgeries, including demolition before prosthetic revision. Therefore, responsibility for the greater iatrogenic injury suffered was not only due to the manufacturing company (for the same reasons as in the previous case) but also, albeit to a lesser extent, to medical misconduct.
Ultimately, in the case of patient 3, who was adequately informed of the potential complications associated with MoM implants (which had been well-documented as early as 2015) and having explicitly consented to proceed with the HRA, the liability of the manufacturing company can be excluded. Indeed, given the existence of documented adverse effects and the absence of sufficient safety data for the device in question, the company’s responsibility for the aforementioned complication is negated, provided that the risk–benefit assessment favours the MoM prosthesis over an alternative implant. However, the patient underwent inadequate radiological follow-up, instead of the recommended higher-level imaging techniques, with the result that the diagnosis of metallosis with pseudotumour was delayed, leading to the worsening of the clinical picture and, consequently, delayed prosthetic revision with more pronounced local damage. Therefore, the responsibility for the greater iatrogenic damage was entirely due to medical misconduct.
Conclusions
The MoM prosthetic implant has been used in over a million patients worldwide, with many more opting for it due to its favourable risk–benefit ratio. Further, device failure due to ARMDs has prompted healthcare professionals to evolve their approach to deal with problems and early failures with aggressive hip revision surgery.
The prosthetic failure rate is low, particularly in patients who have had the implant for over a decade. Monitoring is preferred to revision to reduce invasive procedures. 22 However, MoM prostheses and their management remain controversial, with claims of damage from ARMD persisting in Italy, particularly among those who had arthroplasty before 2012 and an early revision. This case series offers insight into this situation. These cases illustrate the probable direction of future professional liability cases in similar instances. The current awareness of the potential adverse effects associated with MoM implants means that if they are nonetheless selected over alternative prostheses due to perceived advantages outweighing risks, then any complications cannot be attributed to the fault of the manufacturer. This is different from pre-2012 cases, where the issue was that a device was marketed prior to sufficient safety evaluation had been made. The optimal safeguard for both patients and healthcare personnel is to provide comprehensive risk–benefit information and proper patient follow-up which should detect adverse events and prompt intervention and reduce the risk of harm and healthcare liability.
Footnotes
Declaration of conflicting interests
All authors certify that they have no affiliations with or involvement in any organisation or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Funding
The authors declared no funding.