
Abstract
Olanzapine, a second-generation antipsychotic widely used in psychotic and autism spectrum disorders, is associated with significant metabolic side effects including hyperglycemia, dyslipidemia and weight gain. We present a rare case of olanzapine-induced de novo type 2 diabetes mellitus (DM) complicated by acute kidney injury (AKI) in a young female with autism. A 31-year-old female with a known history of autism spectrum disorder on long-term olanzapine (10 mg/day) presented with a recent fall, decreased urine output, poor appetite and generalised weakness. Laboratory evaluation revealed severe hyperglycaemia (GRBS 600 mg/dl), elevated HbA1c (9.8%) and serum creatinine (5.9 mg/dl), confirming acute kidney injury secondary to uncontrolled hyperglycaemia. Olanzapine was discontinued upon suspicion of drug-induced metabolic dysregulation. The patient was managed with insulin therapy, haemodialysis, intravenous antibiotics and fluid management. Risperidone (2 mg/day) was initiated for behavioural control. Gradual improvement was observed in glycemic profile, renal function and overall clinical status over 12 days. Early recognition and drug discontinuation are critical in preventing irreversible metabolic and renal damage. Substituting lower-risk agents such as risperidone can maintain psychiatric stability while minimising metabolic burden. This case underscores the importance of baseline and periodic metabolic screening in patients receiving atypical antipsychotics. Clinicians should remain vigilant for symptoms of hyperglycaemia or renal dysfunction. Prompt withdrawal of olanzapine and initiation of insulin therapy can reverse metabolic derangements effectively.
Keywords
Introduction
Olanzapine is a second-generation (atypical) antipsychotic agent that acts by antagonising multiple neurotransmitter receptors, including dopaminergic (D2), serotonergic (5-HT2A and 5-HT2C), histaminergic (H1) and adrenergic (α1) receptors. It is widely prescribed for the management of schizophrenia, bipolar affective disorder and behavioural disturbances associated with autism spectrum disorder (ASD). 1 Compared with first-generation antipsychotics, olanzapine is more effective in managing both positive and negative symptoms of psychosis, with a lower risk of extrapyramidal side effects. However, these benefits are often offset by significant metabolic complications such as weight gain, dyslipidemia, insulin resistance and new-onset type 2 diabetes mellitus (T2DM).2,3
The mechanisms by which olanzapine induces metabolic abnormalities are multifactorial but incompletely understood. Olanzapine antagonises serotonin (5-HT2C) and histamine (H1) receptors, result in increased appetite and weight gain. In addition, it affects hypothalamic adenosine monophosphate–activated protein kinase (AMPK) signalling, which promotes hepatic glucose production and disrupts insulin sensitivity. 4 Studies have also demonstrated direct pancreatic β-cell toxicity and impaired insulin secretion due to mitochondrial dysfunction induced by olanzapine exposure. 5 These effects collectively contribute to the development of insulin resistance, hyperglycaemia and ultimately, de novo diabetes mellitus. 6
Several case reports and retrospective studies have documented the onset of hyperglycaemia and diabetic emergencies in patients treated with olanzapine, typically within weeks to months of starting treatment.7,8 In most cases, its withdrawal and initiation of insulin therapy led to resolution of hyperglycaemia, confirming a causal relationship.9,10
This case report presents a young female with autism spectrum disorder who developed de novo type 2 diabetes mellitus and acute kidney injury secondary to olanzapine therapy and highlights the clinical importance of early detection, regular monitoring and interprofessional collaboration between psychiatrists, physicians and clinical pharmacists to prevent and manage antipsychotic-induced metabolic adverse effects.
Case presentation
A 31-year-old woman was admitted to the Department of General Medicine with complaints of decreased urine output, constipation, reduced appetite and poor sleep for the past 10 days. She also reported a history of a sudden fall 8 days before admission.
Her past medical history was significant for autism spectrum disorder (ASD), for which she had been on olanzapine 10 mg once daily and a combination of trifluperazine 5 mg/benzhexol 2 mg/chlorpromazine 50 mg twice daily for behavioural control. There was no known history of diabetes mellitus, hypertension or renal disease.
On examination
The patient was conscious, coherent and cooperative but appeared fatigued.
✔ Blood pressure: 160/90 mmHg
✔ Heart rate: 112 beats/minute
✔ Respiratory rate: 22 breaths/minute
✔ SpO2: 94% on room air
✔ Temperature: Afebrile
Systemic examination revealed bilateral pedal oedema but no hepatosplenomegaly or ascites. Cardiovascular and respiratory system findings were unremarkable.
Initial investigations
✔ Random blood glucose (GRBS): 600 mg/dl
✔ HbA1c: 9.8% (Normal <6%)
✔ Serum creatinine: 5.9 mg/dl (Normal 0.6–1.5 mg/dl)
✔ Blood urea: 63 mg/dl
✔ Fasting blood glucose: 229 mg/dl
✔ Urinalysis: Albumin (++), Ketones (+++), Pus cells (plenty), Epithelial cells (3–4/HPF)
✔ Microbiology: Positive for Candida albicans
✔ Complete blood picture: Leukocytosis
These findings suggested acute kidney injury (AKI) secondary to hyperglycemia and urinary tract infection (UTI).
Hospital course and management
Day 1 (Admission)
Olanzapine was discontinued due to its suspected contribution to hyperglycaemia. The patient was started on insulin therapy (Human Actrapid Injection TID) based on sliding scale and placed on a diabetic and renal-friendly diet.
Intravenous fluids were administered for rehydration.
Injection Furosemide 60 mg IV/day was given for diuresis.
Tablet Cilnidipine 20 mg/day was initiated for blood pressure control.
Day 2
The patient’s urine output remained low; however, blood glucose levels began to improve with insulin titration.
Antibiotic therapy with Injection Meropenem (1 g/day IV) and Injection Metronidazole (1500 mg/day IV) was initiated for suspected urinary tract infection.
Day 3
Urine output improved slightly. Blood glucose levels decreased to 178 mg/dl.
Serial monitoring showed a gradual decline in blood glucose levels with insulin therapy, along with stabilisation of blood pressure during hospitalisation.
One session of haemodialysis was performed due to persistent azotemia.
Day 7
Microbial culture reports revealed the presence of Candida albicans, confirming pyelonephritis with fungal infection.
Injection Fluconazole 200 mg/day IV was initiated.
Behavioural symptoms were managed by switching to Risperidone 2 mg/day and continuing a combination of trifluperazine 5 mg/benzhexol 2 mg/chlorpromazine 50 mg twice daily.
Outcome
By day 12, the patient’s blood glucose stabilised (average 160–170 mg/dl) with insulin therapy, and serum creatinine improved to 5.1 mg/dl. Renal parameters demonstrated gradual improvement during hospitalisation.
The patient’s behaviour remained under control with risperidone.
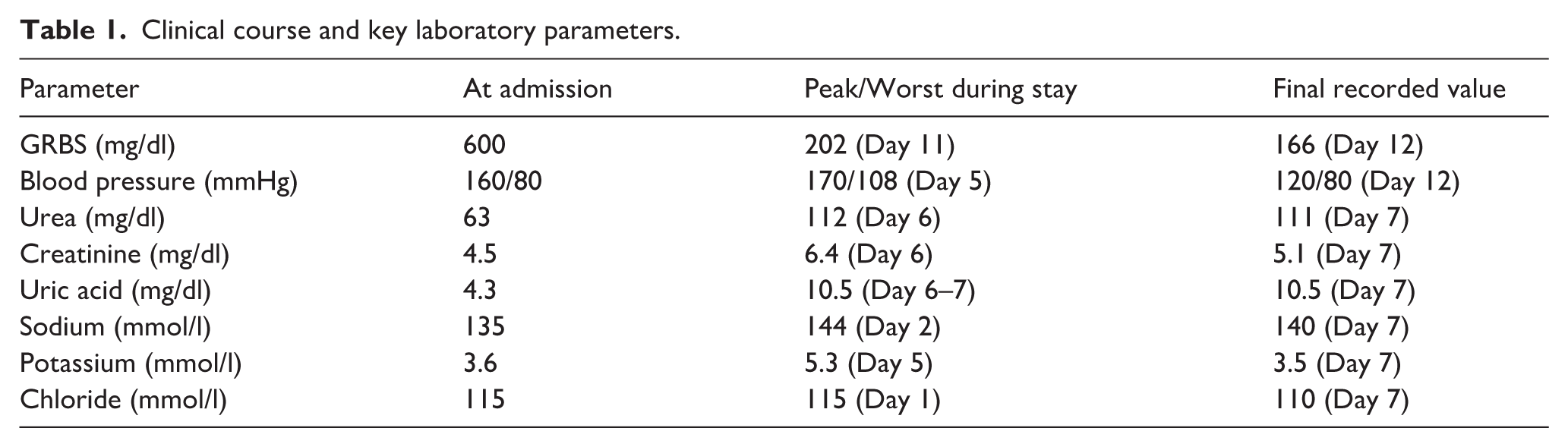
She was discharged in a stable condition with advice for regular blood glucose and renal monitoring, continuation of risperidone 2 mg/day, and follow-up with both psychiatry and endocrinology departments (Table 1).
Clinical course and key laboratory parameters.
Discussion
In this case, a young autistic woman developed de novo T2DM and AKI during olanzapine therapy but recovered after the drug was discontinued and given insulin initiation, which indicated a causal link.
Several studies have reported a 5–6 fold increased risk of T2DM with olanzapine compared to typical antipsychotics, with many cases resolving after drug withdrawal. 11 AKI may occur secondary to dehydration, osmotic diuresis, or rarely, direct nephrotoxicity and rhabdomyolysis induced by oxidative stress. 12
Pharmacovigilance and clinical management
This case underscores the importance of pharmacovigilance in psychopharmacology, especially in populations vulnerable to metabolic effects such as individuals with ASD, who often require long-term antipsychotic therapy. Routine monitoring of fasting blood glucose, HbA1c, lipid profile and renal function should be instituted prior to and during therapy.
If metabolic derangements are detected, clinicians should consider switching to an antipsychotic with a lower metabolic liability, such as risperidone or aripiprazole. In our patient, risperidone was introduced after discontinuing olanzapine, which maintained psychiatric stability without further metabolic complications.
Clinical implications and recommendations
Baseline and periodic screening for metabolic parameters should be mandatory for all patients receiving olanzapine.
In case of hyperglycaemic or renal impairment, immediate withdrawal or dose reduction of olanzapine should be considered.
Conclusion
This case highlights a rare but serious occurrence of olanzapine-induced de novo diabetes mellitus with acute kidney injury in an autistic woman. Clinicians should check for early signs of metabolic dysregulation and renal dysfunction during olanzapine therapy. Early recognition, prompt withdrawal of olanzapine, and initiation of appropriate therapy can prevent life-threatening complications and improve outcomes.
Footnotes
Author contributions
M. conceptualised the case report, and supervised the study. S.T. and I. collected clinical data and patient history. S.N. performed the literature review and assisted in data interpretation. M.N. prepared the figures and tables. M., S.T., I., S.N. and M.N. drafted the manuscript and critically revised it for important intellectual content. All authors reviewed and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was not required for this single-patient case report, as it does not contain any identifiable patient information.
Consent to publish
Written informed consent for publication of this case report was obtained from the patient’s legal guardian.
Data availability
All data generated or analysed during this study are included in this published article.