
Abstract
Background
Traumatic grief is a risk factor for psychological and physiological impairment. In a school shooting incident in Finland, several people lost their lives, and a large number of bereaved family members were at risk for traumatic grief. Psychosocial support for these bereaved was therefore essential, and this article describes a program that was developed for that purpose.
Method
Professionally led peer support group process was provided for the relatives of the deceased in the school shooting in Kauhajoki, Finland, 2008. The 2-year-long process consisted of five weekend gatherings with psychoeducative and group-work elements. The content of the process was based on the existing knowledge of and recommendations for enhancing recovery after a traumatic loss.
Results
On the average, 50 relatives of the deceased in the school shooting participated in the process. The process was based on the principles of (a) timing of the group work and interventions according to stages of bereavement, (b) psychoeducation, awareness rising, and recognizing the signs of posttraumatic symptoms, (c) attachment theory-based elements in parents' and siblings' grief and group work, and (d) encouraging cohesion and strength of families' natural networks and support systems.
Conclusion
Professionally led peer support group process is a trauma-theory-based intervention, which reaches a large number of the bereaved with similar loss. Via group work, psychoeducation, and shared rituals, the bereaved have an opportunity to share and express emotions and experiences, as well as increase their skills in psychological recovery after a violent death of a family member.
A loss of a loved one due to a homicide is a shocking experience, and the grief following a violent death has been described as a grief like no other (Ellis, 2011). Mass violence, such as school shooting, constitutes a traumatic loss and causes pain to a large group of survivors, relatives of the deceased, and the whole community. That was also the case in Finland where two school shootings happened in 1 year.
Both of the Finnish school shootings resembled the Columbine and Virginia Tech massacres that happened in the United States. In Finland, the first shooting happened in November 2007 in Jokela, where an 18-year-old student shot to death six students, the school's headmaster, and the school nurse. He also threatened several other students and destroyed school premises before killing himself. Only 10 months later, in September 2008, a 22-year-old student of a University of Applied Sciences entered his school in Kauhajoki and shot to death nine of his fellow-students and his teacher. Afterwards, he threatened other students and staff with his gun, set several fires, and destroyed school premises. When the police entered the burning building, the perpetrator shot himself to death. Because of the fire, most of the victims were badly burnt making the victim identification difficult (Ministry of Justice, 2010). The loss of lives was very tragic and violent, and it happened without any warning. Many of the students' relatives had to wait for the confirmation of the feared news, and in some cases, it was not possible to recognize their deceased dear ones. All this contributed to the traumatic nature of homicide (Kristensen, Weisaeth, & Heir, 2012).
A violent nature of a death overwhelms the family members and friends, and it can form a risk for mental health problems (Armour, 2006; Clements, DeRanieri, Vigil, & Benasutti, 2004; Jerga, Shaver, & Wilkinson, 2011). Those who have suffered violent and traumatic losses have found to show higher levels of anxiety, mood changes, and prolonged grief disorder (PGD) than those whose loved ones have died natural deaths (Holland & Neimeyer, 2011; Johannesson, Lundin, Hultman, Fröjd, & Michel, 2011; Kristensen et al., 2012). The recovery after a traumatic loss is also slower than after a natural death (Kristensen et al., 2012). Based on earlier research findings, we could anticipate that there would be an increased risk for traumatic grief and mental health problems among the relatives of the Finnish school shooting massacres too, if they are not offered help.
Family and community networks are essential resources in trauma recovery. The role of the professional help is to mobilize the strength and potentials of natural social networks (Hobfoll et al., 2007; Witteveen et al., 2012). Survivors of a traumatic loss tend naturally to turn to each other for help and support and find it easier to share feelings with others with similar experiences (Murphy, Johnson, & Lohan, 2002; Walsh, 2007). In peer support groups, it is possible to ventilate despair, anxiety, anger, and bewilderment, which contributes to learning effective ways of coping with the loss. Some studies confirm that sharing traumatic experiences and ventilating feelings are associated with improved grief processes and mental health (Pennebaker, 2003).
Peer support groups for the bereaved of traumatic loss have been used, for example, after terrorist attacks (Walsh, 2007), homicide and other violent loss (Murphy, 2006), and natural catastrophes such as tsunami (Dyregrov, Straume, & Sari, 2009; Saari, 2006). They are regarded as ideal for exchanging information, sharing painful memories, providing mutual support, and encouraging hope and efforts for recovery (Dyregrov et al., 2009). The peer support group process applied to the relatives and friends of the school shooting victims in Finland was planned to supplement the support offered by their natural social networks and to strengthen their beneficial impacts. Timing, course, and healing elements of the peer support groups were based on the natural recovery process of grief, and the help was offered to those who were in the greatest need. As recommended in international guidelines, psychoeducation and enhancing feelings of safety and hope among the bereaved were pivotal elements in the process (Hobfoll et al., 2007; Witteveen et al., 2012). The aim was to create conditions for the bereaved to explore and to share their traumatic memories and grief with peers in a safe atmosphere together with crisis specialists.
In this article, we describe the theoretical principles and guidelines for helping the bereaved with traumatic loss and the planning and implementation of one of the interventions applied in the context of the Kauhajoki school shooting, 2008, titled Professionally Led Peer Support Group Process.
Violent Death and Traumatic Grief
Adaptation to a loss of a beloved person is a highly painful and demanding process. Just as each attachment relationship is unique, so is each grief reaction distinct (Shear, Gorscak, & Simon, 2006). Majority of the bereaved accommodate to the loss and continue their lives with support of their family and close friends while cherishing the memory of the deceased person. Traumatic loss, however, can be followed by complex course of bereavement that is also conceptualized as traumatic grief (Jerga et al. 2011; Raphael, Stevens, & Dunsmore, 2006).
Differences Between Normal Bereavement and Traumatic Grief (Modified From Raphael, Stevens, & Dunsmore, 2006).
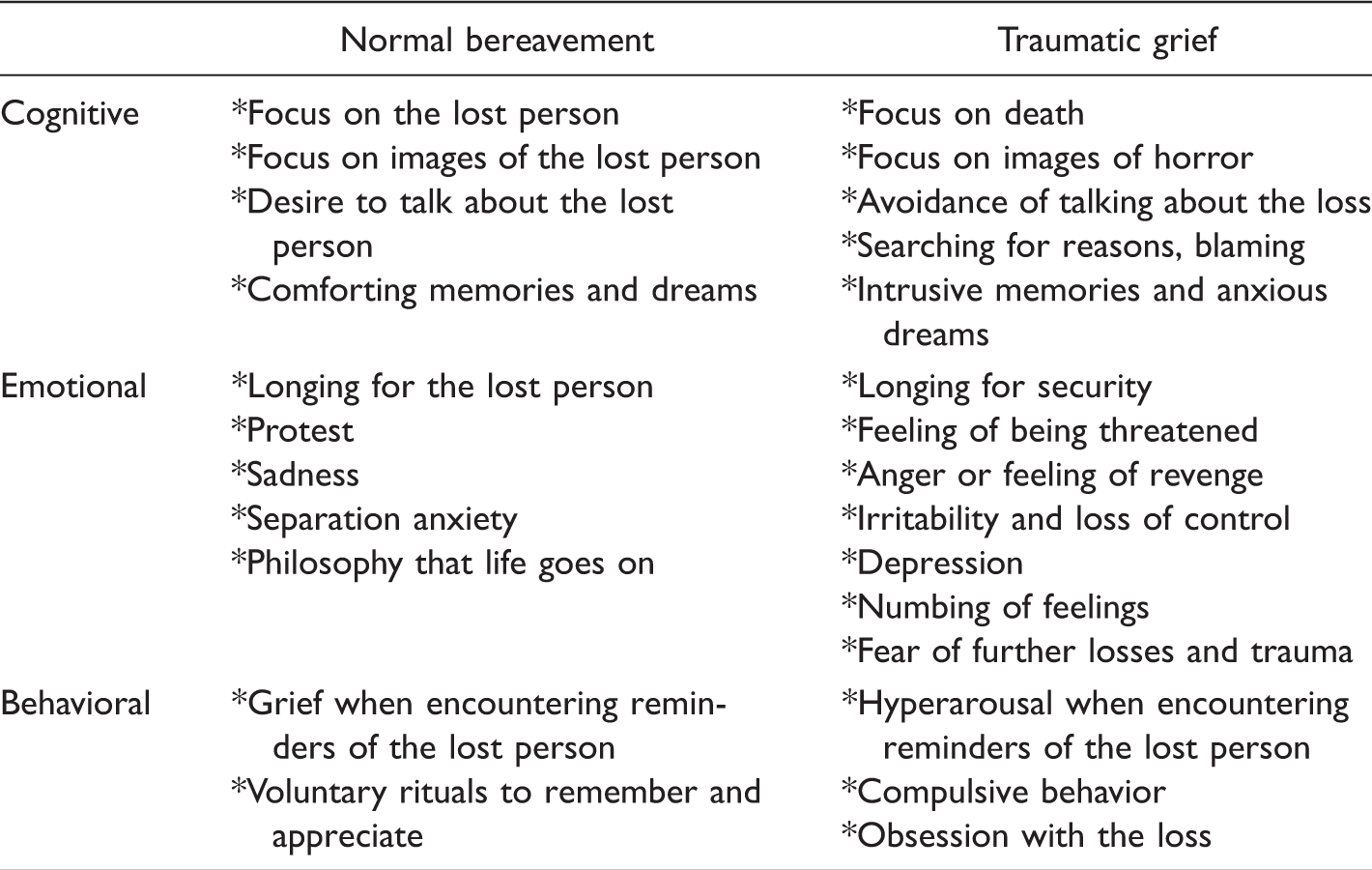
In normal bereavement, the bereaved misses the lost beloved, would like to talk about the deceased, and suffers from separation anxiety and sadness, but gradually accepts the reality of the death and loss (Bryant, 2012). Comforting memories and nocturnal dreams are common in normal bereavement, and there is little or no avoidance of reminders of the lost person (Shear et al., 2006). However, in traumatic grief, the memories and dreams may be filled with intrusive glimpses of the scene of the traumatic loss, and memories occur in fragmented form. When the death is caused by a homicide, the bereaved is haunted by horrible acts of the perpetrator inflicted to the beloved person and his/her suffering. These vivid and disturbing images are the very core of traumatic grief that further may complicate the recovery from the grief (Murphy et al., 1999; Raphael et al., 2006).
In the context of school shooting, media is intensively covering the events and family stories, police investigations, and trials. Death and loss of the family members are thus made public, which is constantly reevoking vivid memories of the violent loss, and keeps the bereavement going on without a natural closure (Murphy, Johnson, Chung, & Beaton, 2003; Poijula, 2010; Raphael et al., 2006). The risks and course of traumatic grief were acknowledged in tailoring the professionally led peer support group process, and the aim was to enhance normal grief among the bereaved relatives after the Kauhajoki shooting. Based on the prior knowledge, it was possible to tailor psychoeducational material, screening instruments, elements of group processes, and consultation topics.
Grief in a Family
In mass violence, such as school shootings, the number of the deceased is high, and the death thus touches many. It has been estimated that every victim has at least four to six family members and a variable number of next of kin (Poijula, 2010). Each family member has had a unique relationship with the deceased, and each one is searching for their own ways to cope, grief, and recover from the loss (Walsh, 2007). The challenge of the aftercare and crisis psychology is to recognize the different ways the trauma affects the roles and interactions between family members, in order to elicit their natural resources.
In bereavement, people tend to seek support from family members, and activating family support is the primary resource for resilience (Salloum & Rynearson, 2006). Traumatic loss of a family member often dramatically affects family roles and hierarchies and complicates the availability of support. Immediately after a traumatic loss, the family life is often chaotic, and all members feel lost and terrified. Parents may feel helpless and work at the limits of their own capacity, thus being unable to care and console their children in a way they would like to. Children may try to help parents by taking care of everyday family routines and by hiding their own, sometimes overwhelming, grief. This mutual supportive caretaking and sharing of responsibilities may be an adaptive response to the crisis in short-term. Yet, if extreme and prolonged, it involves a risk for parentification, as children have to take the parental role and carry responsibilities that are too heavy a burden for their age (Clements & Burges, 2002; DiCaccavo, 2006).
It is extremely hard for most parents to observe grief and pain in their children, and they may feel incompetent in providing adequate and sufficient emotional support to their children (Clements & Burges, 2002; Kaitz, Levy, Ebstain, Faraone, & Mankuta, 2009). Overidentification with the children's pain may result in loosening of normal family boundaries and rules. Parents can also become highly overprotective and set too strict boundaries for their children (Mannarino & Cohen, 2011; Salloum & Rynearson, 2006). Both parental overinvolvement and withdrawal can give children a message that the world is an unpredictable and unsafe place and that adults cannot protect them (Cohen, Mannarino, Greenberg, Padlo, & Shipley, 2002; Punamäki, 2006). In order to enhance children's sense of security, it is important to support parents in continuing normal everyday routines as much as possible because continuity and familiarity are pivotal for children when facing a violent loss (Mannarino & Cohen, 2011; Walsh, 2007).
Losing a family member during childhood means unique challenges, and it can make children more vulnerable in later adversities of life. Yet, research emphasizes the decisive role of adequate parental and family support in understanding the children's grief (Brown et al., 2006; Cohen & Mannarino, 2004). If support fails, children develop complicated grief that in turn predicts later mental health problems (Brown et al., 2006; Clements & Burges, 2002; Mannarino & Cohen, 2011). A study confirmed that the emotional reactions of parents at the time of death and the ways they expressed sadness and grief predicted whether bereaved children and adolescents (N = 132) developed complicated grief (Brown et al., 2006).
Traumatic grief is common among parents who have lost their child in a violent way, and it in turn forms a risk for long-term mental health problems (Dyregrov, Nordanger, & Dyregrov, 2003; Johannesson et al., 2011; Murphy et al., 2002; Poijula, 2010). Murphy et al. (2002) examined mental health consequences among 176 mothers and fathers who had lost their child (15 to 25 years) in an accident, suicide, or homicide. In the follow-up, they found that about 60% of both mothers and fathers suffered clinically significant psychiatric distress, and 28% of the mothers and 12% of the fathers still had posttraumatic stress disorder (PTSD) 5 years after the loss. According to the bereaved parents' own estimation, they would need 3 to 4 years to be able to get on with their own lives—yet, they felt that the loss had changed their lives for good and that there is no recovery (Murphy et al., 2002). Similarly, Dyregrov et al. (2003) found among bereaved parents (N = 235) that 5 years after the violent loss of a child, 60% still suffered from mental distress and 57% to 87% showed complicated grief. Finally, a study among bereaved relatives of the victims of tsunami showed that losing a child increased the risk for psychiatric distress and PTSD (Johannesson et al., 2011).
In accordance with these studies, the peer support group process was based on elements that gave support both to the grieving adults and the children in an attachment-informed, age-appropriate, and comprehensive manner, aiming at improving well-being, facilitating healthy grief, and increasing social empowerment.
Attachment in Enhancing Social Support
The attachment theory (Bowlby, 1969/1982) explains why people create strong and resistant bonds between each other and why breaking, or even threat of breaking, these bonds is highly likely to create anxiety and distress. The infant and the caregiver form unique communication patterns, in which the child learns whether it is possible to trust in the care when distressed. Whenever feeling threatened and distressed, the attachment system activates, and it makes the infant seek proximity, soothing, and safety. The emerging attachment style (secure, avoidant/dismissing, or ambivalent/preoccupied) captures the emotional availability of the caregiver and the infant's typical response pattern in early dyads (Ainsworth, Blehar, Waters, & Wall, 1978; Bowlby, 1969/1982).
These formative experiences within a significant early relationship are internalized as working models that will be generalized in new relationships. They will activate later in life when the individual is exposed to, for example, threat, traumatic stress, or violent loss (Mikulincer & Shaver, 2010). There is evidence that trauma survivors with different attachment styles show unique help-seeking behavior, coping strategies, emotion regulation, and mental health problems (Fraley, Fazzarri, Bonnano, & Dekel, 2006; Kanninen, Punamäki, & Qouta, 2003; Mikulincer, Ein-Dor, Solomon, & Shaver, 2011). Research in war context revealed that the survivors with secure attachment style used predominantly active and problem-focused coping strategies, while the insecure-avoidant relied on withdrawal and passive strategies (Mikulincer, Florian, & Weller, 1993). Furthermore, the secure survivors typically processed their trauma-related emotions in balanced ways, while the insecure-dismissing relied predominately on cognitive, and the insecure-preoccupied on behavioral and conflicting emotion regulation (Kanninen et al., 2003).
Research confirms that the attachment style affects the ways in which bereaved persons cope and response to the loss of a close person. A study of 368 bereaved adults (17 to 49 years) found that the bereaved with insecure attachment styles were more likely to suffer from prolonged grief symptoms than the securely attached (Jerga et al., 2011). There is evidence that the quality of the attachment with the deceased plays a role in grief responses. Jerga et al. (2011) showed that that the stronger the attachment bond with the deceased had been, the greater was the grief. Mancini, Robinaugh, Shear, and Bonnano (2009) found in their study of the bereaved spouses (N = 50) that in the context of high marital quality, persons with a dismissing avoidance attachment style managed and coped quite well in adjusting to life without thespouse. They state that persons with this kind of attachment benefit more from a therapeutic approach that is less focused on the loss itself (Mancini et al., 2009).
Health care professionals must be aware that a loss of an important attachment figure increases the likelihood of complicated or prolonged grieving process (Johannesson et al., 2011). The planning and tailoring of the peer support for the bereaved families after the school shooting relied on the knowledge on attachment style-related coping strategies, help-seeking behavior, symptom expression, and social affiliation. It enables considering the unique strengths and vulnerabilities of family members in the aftermath of traumatic loss. Attachment-based knowledge guided the choice of mutual rituals in peer meetings, forming the intensively working peer groups, and selecting themes and methods for the group work, for example, in group sessions both verbal and physical methods were used to process emotions because it is natural for those with secure attachment style to express emotions openly, and for those with avoidant style it can be uncomfortable.
Interventions for the Bereaved Parents and the Next of Kin After a Traumatic Loss
Valuable lessons for promoting family and community resilience can fortunately be learned from earlier tragedies. For example, after Oklahoma City Bombing in 1995, professionals, volunteers, and rescue workers joined forces for effective crisis intervention (Allen, Tucker, & Pfefferbaum, 2006). After the terrorist attack of 9/11 in 2001, similar multidisciplinary support was provided for traumatized and bereaved families (Walsh, 2007). Several interventions were implemented to facilitate the grief process, to give information about what has happened, to share the suffering, and to regain a sense of safety and structure in the victims' shattered lives. Multifamily and community-based approaches and the initial focus on children were common factors in these interventions. Psychoeducation, as in a form of normalizing reactions to trauma, was widely used in these interventions. The multifamily group intervention allows and encourages the family members with diverse skills, talents, and ages to contribute to the family resilience in unique and various ways (Walsh, 2007).
Some interventions have been developed specially to support and help the family members of homicide victims. The Parent Bereavement Program (PBP; Murphy, 2006) focuses on parents exposed to a violent loss of a child and aims at reducing bereaved parents' psychological distress. The program consists of 12 weekly two-hour sessions involving problem-focused and emotion-focused support. The problem-focused part offers skills-building exercises on various domains, for example, on managing the marital and other relationships, and on solving relational and practical problems. The emotion-focused part concentrates on feelings and loss-evoked emotions via group work and professionally led peer support. The efficacy of the PBP was analyzed in a noncontrolled study (N = 261) of bereaved parents in pre- and posttreatment setting. Results confirmed a significantly decreased level of psychological distress and PTSD symptoms among mothers, and these benefits were sustained in the 2-year follow-up. The program was highly endorsed by the parents and the participation rate was high; 94% of the parents attended all sessions.
A trauma and grief-focused group protocol was developed by Saltzman, Pynoos, Layne, Steinberg, & Aisenberg (2001), consisting of 20 weekly sessions with psychoeducation, cognitive and emotional processing of traumatic experiences, and practicing problem-solving skills. They studied its effectiveness among 26 adolescents exposed to severe community violence and suffering from psychological symptoms in pre- and posttreatment settings. Results show statistically significant improvement in symptoms of PTSD and traumatic grief.
Forming integrated, coherent, and meaningful narratives of the trauma seems to be a core element in peer group support interventions. The bereaved are encouraged to work on the course, meaning, and trauma-evoked emotions and to create a comprehensive narrative (Shaw, 2000). For instance, the effectiveness of Restorative Retelling Intervention (RRI) was tested in pre- and postintervention settings among 64 bereaved adults who had experienced a violent death of a loved one (Rynearson, Correa, Favell, Saindon, & Prigerson, 2006). Results showed a significant decrease in depressive, PTSD, and traumatic grief symptoms, as well as in behavioral problems, and alcohol and substance abuse.
The professionally led peer support tailored for the relatives and peers after school shooting trauma also follows Nordic tradition to help bereaved persons. The model allows them to share experiences and emotions with those who have had the same loss within the guidance of the crisis work specialists. The model of collective assistance for the bereaved has been widely applied after major disasters and violent deaths in the Nordic countries (Dyregrov et al., 2009; Harjajärvi, Kiikkala, & Pirkola, 2007; Palosaari, 2007; Saari, 2006). The approach is planned to support large amount of survivors and bereaved at the same time and to mobilize support to families, schools, and working places. It also involves elements that aim to create coherence and better understanding of the traumatic loss and normalize and validate people's experiences. Psychoeducation, individual and group coping mechanism, and teaching self-help methods form an integral part of the approach. Via collective assistance, it is also possible to identify those in need of individual assistance (Dyregrov et al., 2009).
Because of the uniqueness of the grieving process after a violent death, there is no single method or strategy for assisting that would work for everyone. That is why a combination of therapeutic approaches and elements may best assist the survivor in working through the trauma and grief of a violent loss (Allen et al., 2006; Asaro, 2001a, 2001b; Hatton, 2003).
Model of the Professionally Led Peer Support Group Process After School Shooting
Kauhajoki school shootings affected a great number of people in addition to those who directly witnessed the massacre. A multitask and multidisciplinary Kauhajoki-project organized and provided acute and long-term psychosocial support for the trauma-affected community and individuals (Ala-aho & Turunen, 2012). The recovery of the trauma-affected students was monitored and supported by the project, and the research results of a 2-year follow-up study confirm that most of the students recovered well in the follow-up time and appreciated the support they had received (Haravuori et al., 2012; Turunen, Haravuori, Pihlajamäki, Marttunen, & Punamäki, 2014; Turunen & Punamäki, 2014). Kauhajoki-project was administrated by the Hospital District of South Ostrobothnia, and it worked in close co-operation with other actors in crisis aftermath, including the police and the church. The project was funded by the Finnish government, and the expenses, for example, participation in the peer support group process, were covered by the project (Ala-aho & Turunen, 2012).
The professionally led peer support group process was organized for 2 years as a main psychosocial intervention for the relatives of the deceased. The process consisted of five weekend gatherings with common meetings to all participants and separate small peer group sessions. The process was based on following principles: (a) Right timing for group work and interventions according to the stages of bereavement, (b) Importance of psychoeducation and recognizing signs of possible posttraumatic and other symptoms, (c) Uniqueness of the grief process within families and attachment theory-informed elements in the group work, and (d) Encouraging cohesion and strength of families' natural social networks and support in facilitating emotional sharing and affiliation by group processes.
Right timing for the psychosocial help and therapeutic interventions is of great importance after a traumatic experience. The first peer support group gathering took place 4 months after the school shooting massacre. The timing was based on research and recommendations that (a) acute and immediate help should involve more practical and informative elements followed later by more psychosocial and therapeutic interventions if needed and (b) trauma-affected people need space and time to let natural cognitive-emotional process to work, and they should simultaneously be monitored for risks and dysfunctional psychosocial responses such as social withdrawal, denial, or acting out (Saari, 2006; Witteveen et al., 2012).
The second gathering was planned to take place on Mother's Day, 3 months after the first gathering. Special dates, such as Christmas or Mother's Day, evoke strong memories and longing in bereaved families, thus providing insightful material for group processes. Also anniversaries, birthdays of the deceased, and other nodal events may bring up painful memories of the beloved person (Murphy et al., 2002; Prigerson et al., 1997), and that was why the third gathering took place around the first anniversary of the massacre. Fourth gathering took place 1 year after the first meeting, 16 months after the tragedy. There is some evidence that symptoms of mental distress may decrease slowly after traumatic loss, but might increase again during the second year after the loss (Murphy et al., 2002; Prigerson et al., 1997). The fluctuations in loss-related distress may reflect dynamics of grief that the bereaved only gradually realize the finality and horrible nature of the loss. The bereaved are also often expected to feel better after the first year. If this is not the case, they may feel afraid and distressed (Kristensen et al., 2012). Meeting peers during the second year of bereavement is therefore important. As the recovery from a violent death of a close person is known to be a long process, the last gathering took place after the second anniversary of the tragedy (Bryant, 2012).
The second principle guiding the process was to give psychoeducation and to monitor and screen for possible risk factors and responses. Psychoeducation as a core element of the peer support process had multiple functions, such as increasing the understanding, normalizing the reactions, and practical guidance. Learning about normal and traumatic grief process after a violent death and about various ways of saying goodbye to the beloved person help the bereaved to recognize and appreciate others' grief. Psychoeducation also provided tools for arising awareness about the course, timing, and content of one's own and of other family members' grief. It also functioned as a normalizing element and helped the traumatized family members and peers to understand reasons for their new powerful and often uncontrollable reactions. Practical exercises taught various ways for how better to tolerate, manage, and regulate painful emotions and reactions.
Monitoring participants' well-being was essential through the 2-year peer support group process. The screening of possible signs of high levels of mental distress was performed by the group-leaders via personal interviews and self-filled questionnaires (Impact of Event Scale, Beck Depression Inventory, Audit), which included, for example, PTSD symptoms, sleeping difficulties, depression, increased substance use, and concerns on physiological well-being. Referrals to medical assessments and psychotherapy were made when necessary.
The third principle was to emphasize the uniqueness of the grieving process of each family member. The family with its hierarchical roles and attachment relations is unprepared for unexpected, overwhelming, and violent losses. The familial roles and responsibilities are shattered by the loss, and family members may feel deep helplessness that can be understood and shared with the peer with same kind of relationship to the lost person. The peer support group meetings therefore involved separate subgroups for mothers, fathers, siblings, and spouses of the deceased. There was also co-operation and communication between the subgroups and occasionally the participants worked with their family members.
The fourth principle relied on group sharing and encouraging of the group processes. The relatives of the homicide victims share experiences that are specific and distinctive for them. The weekend gatherings as a form of peer support and intervention for trauma survivors of natural and man-made disasters have been considered highly beneficial among the participants (Dyregrov et al., 2009; Harjajärvi et al., 2007; Poijula, 2010). Survivors attending the support groups have reported that they feel at home and safe among persons with similar loss, and that they dare to express multiple and sometimes conflicting feelings while being understood and accepted by the others (Armour, 2006).
Implementing the Peer Support Process
For a successful group process, three practical issues are vital: milieu where the group process is carried out, recruiting experienced professionals responsible for group work, and ensuring the homogeneity of groups. The criteria for an ideal milieu for multifamily support groups were the following: First, it had to ensure the anonymity and privacy of the participants as well as be easily reached from different parts of Finland. Second, it had to have suitable premises for working both in small and large groups, and with children (enough rooms, safety issues, easy access). It also had to have premises for joining together in the evening and spare time. Delicious food, possibilities for exercise and swimming, and a beautiful landscape were advantages.
Giving both acute and long-term psychosocial support after a major trauma is professionally demanding work, and it requires special personal and experiential qualifications. The leaders of the peer support groups must be capable of containing intensive pain, sorrow, and desperation without being vicariously traumatized (Saari, 2006). Twenty mental health professionals, mainly psychologists with experience in crisis management, grief, and psychotherapy, were recruited in the Kauhajoki-project. The leaders had frequent meetings during the weekend gatherings in order to prepare, update, and share information, as well as to ensure their own well-being. Every peer support group leader had a change to have an impact on the program by sharing their own special expertise and experiences from previous peer support processes as recommended by Dyregrov et al. (2009) and Saari (2006). After the 2-year peer support process was finished, the leaders had a final meeting with a possibility to evaluate the process by sharing their opinions of the pros and cons of the project in the guidance of experienced supervisors. Nurturing environment, sensorimotor exercises, and group discussions served as a possibility to ventilate and recover from the unique job they had done with a high degree of professionalism and commitment.
The preparation for the weekend gatherings was of great importance. The families of the deceased were informed of the upcoming peer support group process 6 weeks before the first gathering via invitation letter, in which the purpose and the schedule of the whole 2-year professionally led peer support process was described. It was further communicated to the families that the inviting professionals were aware of their painful loss and willing to support them. Every family member, regardless of age, was invited and the participation was naturally voluntary. About 50 relatives of the deceased students of the Kauhajoki school shooting participated in every gathering. The commitment to participate was high across the 2-year period: Ninety-six percent of the participants attended all five gatherings. Both separate subgroups and joint large group activities were implemented serving different purposes. The subgroup grouping was done according to the participants' relationship to the deceased as well as age and gender, as shown in Figure 1. Each group had three to 15 members, average number being nine. There were two experienced leaders in each subgroup, except in the children's group, which had three to five adults guiding the children (three psychologist and extra nannies whenever needed).
The large group and the sub groups of the professionally led peer support group process.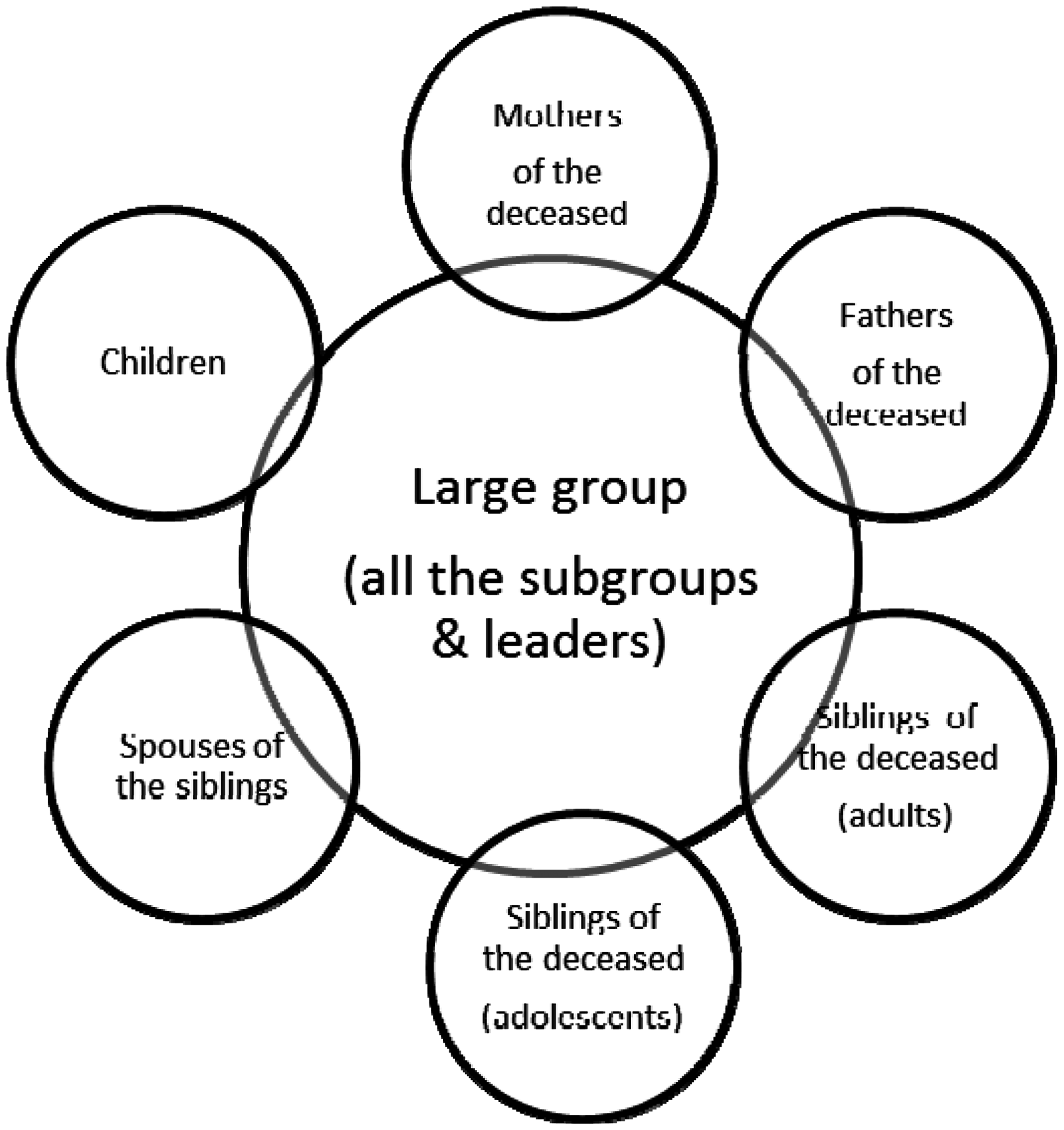
A mother is usually the primary caretaking figure in a child's life, and losing a child means a loss of a caregiving relationship (Jerga et al., 2011). The firm attachment between a mother and a child does not break entirely in death, but the bond gradually changes its form from concrete into more abstract. Because of this attachment bond, some mothers feel actual physical pain after their child's death (Harper, O'Connor, Dickson, & O'Carrol, 2011). The bereaved mothers have reported that the relationship with their child continues in a variety of ways, for example, through linking objects, such as jewelry or clothes special to the deceased, or by establishing a symbolic representation of the child in their daily lives (Harper et al., 2011).
Continuing bond exists also between a father and a child, father being often the other caretaking person to a child (Field & Filanosky, 2010). According to Johannesson et al. (2011), losing one's own child, compared with other types of loss (losing a partner, parent, or sibling), creates a risk of prolonged grief especially for fathers. Toller and Braithwaite (2009) documented differences between the bereaved parents in their expressions of grief so that the bereaved fathers expressed their grief more through activities, and the mothers cried and talked more about the loss. These different styles of expressing grief may sometimes create conflicts in families, and the peer support groups were tailored accordingly to offer a channel to discuss these unique and personal ways to grieve. Separate peer support subgroups were arranged for mothers and fathers in order to respect gender-specific responses. Earlier experiences with professionally led peer support groups had shown that bereaved fathers evaluate separate peer groups as highly positive (Aho, Tarkka, Astedt-Kurki, & Kaunonen, 2009). The subgroups of mothers and fathers had joint sessions as well.
The victims of the Kauhajoki massacre were young adults or adults, and most of them lived in a relationship. A loss of an intimate relationship is known to be very stressful and has comprehensive impacts on future life-course (Prigerson et al., 1997).The widowers and widows formed a peer support subgroup, and their leaders had previous experiences of working with spouse's conjugal grief.
The deceased had several siblings. Some of the bereaved siblings were adults with their own children and others were adolescents or young adults. The subgroups for the siblings were formed according to the age. Special concern was placed on the needs and demands of the youngest participants, and enhancing the sense of security was the core aim among the bereaved children. Their group was divided into smaller subgroups in order to provide age-specific attention and activities, for example, for the preschoolers and early adolescents. Co-operation with the parents was essential, and it included personal discussions with them about specific questions and concerns of their bereaving children. Parents were provided special and detailed psychoeducation about children's grief, as recommended by Cohen, Berliner, and Mannarino (2003). It was also important for parents to know that their children, including the infants, were cared for so that the parents could concentrate on their own process with their peers.
The spouses of the siblings of the deceased have a unique supportive role in the bereavement process, as they also have lost a close relative-in-law. There is a danger that they may feel that their own grief is less legible than that of the close relatives, and subsequently put their own needs and feelings aside from their spouse's needs. Again, earlier experiences of professionally led peer support group processes in Finland among relative-in-law subgroups were encouraging. They were found to clarify their twofold role in bereavement: to provide support for family members and to grieve their own loss (Saari, 2006). This is why a separate subgroup was formed for them as well.
The Phases and the Content of the Kauhajoki -Professionally Led Peer Support
The Process Model of Professionally Led Peer Support in Grief.

The common program started on Sunday morning with a joint large group meeting that again included short psychoeducative lectures. The subgroup sessions then continued, and the whole weekend was concluded with a large group meeting with a summary of the weekend. Consequently, the professionally led peer support group process consisted of psychoeducative, group work, symbolic, and commonly shared elements. Common rituals, such as building a memory box or a memorial service are found to be beneficial in the grieving process (Armour, 2006; Hawdon & Ryan, 2011; Toller & Braithwaite, 2009), and they were therefore included in the schedule of the peer support group process.
The theme of the first peer support group gathering was to get to know each other, and the aim was to create a confident and secure atmosphere for the process. The gathering began by a welcoming speech by one of the group leaders followed by an introduction of the other group leaders. The structure of the whole 2-year-long process and the program for the first weekend were presented. The rules of the gatherings were further discussed, that is confidentiality, commitment, and abstaining from substance use. The participants then presented themselves by telling their names and their relationship with the deceased. The deceased family members were symbolically present during the weekend: Ten white candles, representing the light, connection, and harmony of the deceased were burning at the table in the room where the families gathered for welcome. The candles were burning whenever there were sessions in the room. At the end of the weekend gathering, the burning candles were extinguished, and each family took the candle of their loved one with them.
The psychoeducative topics of the first gathering focused on increasing the understanding of the multiple consequences of a traumatic loss. The short lectures dealt with the common reactions to traumatic experiences in order to normalize the participants' experiences. They gave information about the similarities and differences, as well as the overlapping aspects, between trauma, grief, and traumatic grief. The implicit message was that the traumatic loss is an overwhelming experience, but also recovery is possible.
The aim of the subgroup sessions was to get to know each other and to make the participants feel safe and confident with each other by sharing their own stories about the tragedy. Group leaders emphasized that the participants should share their personal experiences in a way that they felt appropriate. Their work was based on the knowledge and understanding of the healing function of retelling the story of the violent death of the beloved one. There is evidence on narrating and sharing memories being restorative and beneficial for effective recovery of loss (Rynearson et al., 2006) and trauma (Witteveen et al., 2012).
The group leaders were aware that for some participants, retelling about violent death and tragedy may evoke overwhelming imaginaries and highly distressed memories. The group sessions thus involved a number of emotion stabilization techniques such as the safe-place imaginary, mindfulness, and deep breathing-exercise. They aimed at enhancing the dual-awareness of safety in the present situation and devastating insecurity in the past traumatic situation. The awareness helped the bereaving participants to modify fragmented memory glimpses into a more coherent form. The practical self-helping methods were applied throughout the 2-year peer support group process in order to familiarize the participants with them so that they could use them whenever upset and overwhelmed by the loss.
The Mother's Day was a central theme for the second peer support group gathering. The mutual program began again with a joint large group session. This time there were 10 dark red roses at the table as a symbol of the presence of the deceased, and at the end of the weekend gathering, the families got to take the roses with them. There was also a ceremony when every mother in the group received a rose for that Mother's Day before leaving for home. A red rose is the flower for the Mother's Day in Finland involving a strong symbolic value. Finally, the common ritual of the Power Circle (participants holding each other's hands) was conducted as a symbol of group cohesion and togetherness.
The psychoeducational topics of the second gathering focused on different ways to grieve and to express emotions, and on how the body keeps score of what has happened to us. Special issues concerning the children and loss were also considered. The group leaders taught techniques for relaxation, mindfulness, and relieving anxiety and reminded about the importance of taking care of oneself in a comprehensive manner. In addition, the participants shared with the others their own ways to remember the deceased and told about issues that have helped them cope.
The third peer support group gathering took place just before the first anniversary of the school shooting tragedy. The theme was the importance of anniversaries in the course of saying goodbye to the beloved persons, and how the day evokes a variety of memories, feelings, and emotions that anniversaries evoke. This time photographs of the deceased family members were placed on table with a burning candle for each of them, and in the closing session, the families got the pictures and the candles of their loved ones with them.
The psychoeducational lectures of the third gathering discussed the ways the deceased loved one travels with the families in their memories, and the layers of the grief. To introduce the topic about life after death, two peer group leaders (a crisis psychologist and a chaplain) shared their professional knowledge, experiences, and understanding. The participants joined the conversation reflecting their own experiences. The other lecture concentrated on the topic of How to go on. The second year without the deceased is about to begin, and the aim of the topic was to direct the attention more to the future.
As a commonly shared ritual of the first anniversary of the tragedy, the families prepared a memorial item for their lost beloved. They decorated white cardboard plates with the materials they collected from the autumnal nature. The materials reflected the unique memories of the deceased, for example, choosing particular colors or flowers that the deceased loved one had liked. The families shared the meanings of the memorial items with the peers in a joint large group session in the depth they preferred. When the darkness fell, it was time for the letting-go-ritual. Everyone gathered to the lakeside. Small candles were placed on the plates, and families released them off to the lake. The sight of floating candles in the darkness was breathtakingly beautiful and emotionally moving. The participants stood still until the last boat had got out of sight. The emotions, thoughts, as well as silences were shared with the peers in the warm and dark night.
The fourth peer support group gathering took place 4 months after the anniversary. This time the main theme was the continuum of time, the past–present–future. The aim for this gathering was to increase awareness about individual well-being, hopes, fears, and wishes for the future, as well as to help families in their struggle for cohesion and finding meaning after a traumatic loss. These themes were covered both in psychoeducative lectures and in commonly shared exercises. In the invitation letter, the families were asked to bring one or several items that reminded them of the deceased family member. They were also asked to share with the peers a story related to these items. The items were placed on a large table and were visible throughout the whole fourth gathering.
The group sessions included both lectures and exercises that aimed at encouraging emotional, symbolic, social, and cognitive ways to deal with the past trauma, present challenges, and the meaning of the future. The leaders asked the participants to write a letter, greeting, or a poem to each other. The address could be a specific person, one's own peer group, or all the families and relatives present at the fourth meeting. These greetings were touching and yet encouraging, some bringing tears to the eyes of the participants, some making the whole group laugh together. One of the participants expressed his feelings by writing a poem: We walk the path with misty minds. Without focus. I am alone, but not afraid. You are by my side, even though I cannot see you. You are present every moment. Yet, I feel sad. I don't know how to feel and how to think without you here. But the memory of you carries me. My wings are weak, but one day I will fly. Just wait and see.
The participants were also instructed to draw four circles in a white paper. The first circle represented time and feelings before the incident, the second one the actual school shooting tragedy, the third was the situation right now, and the fourth circle represented the future. Everyone, from a 2-year-old to over 80 years old concentrated in coloring the diagram of sorrow, sharing crayons, thoughts, and feelings with each other.
The time interval between the fourth and the fifth gatherings was relatively longer, 8 months, which served a meaningful preparation for the future. The purpose was to prevent the participants from becoming too dependent on the peer support process that was nearing its end. The last peer support group gathering was held a couple of weeks after the second anniversary of the school shooting tragedy. The timing was carefully planned, and the aim was to let the families form their own unique rituals for the special date. The psychoeducative lectures emphasized the importance of self-care and looking forward. The central theme was how to construct new meanings for the tragedy. Reflecting the time-bound meanings of the loss, accepting it as a part of the family history, and preparing for the future are considered important for the successful recovery after a death of a beloved person (Armour, 2006; Lannen, Prigerson, Onelov, & Kreicbergs, 2008). The flowers and candles representing the lost family members were placed on the table for the last time, and the families took them home with them at the end of the gathering.
The themes of the joint large group meetings related to encouragement of the cohesion and co-operation within the families. The participants joined a common ritual, titled a mural, as a symbol for hope and the future. Together they prepared a wall-size piece of art of a colorful mural. In the unique shapes and colors, they could express their inner thoughts and feelings about the future, as well as issues that have helped them in their bereavement, and those that make them feel good.
In the subgroups, the future prospects were exercised by a letter to me. The participants were instructed to write themselves a letter that was encouraging and caring for the future. They wrote about what they wished for themselves, the things they appreciated, and what they thought they could do better. The writing process was very intensive, and everyone concentrated on writing and even decorating the envelopes. The group leaders collected the letters and sent them back to the group members after 6 months.
Both the leaders and the participants gave speeches at the closing ceremony of the peer support group process. As an example, a participant told that he remembered how at the first gathering one of the leaders had said “Someday you will laugh again.” He could not believe it at the time, but now he realizes that it is true, and he feels as if the words had been an anchor, providing a safe place for a rocking boat. At the beginning, the task of the group leaders was to maintain hope, now the family members carry it on. Others agreed that they were able to laugh again, even through the tears.
The follow-up and the feedback of the peer support group process was made by phone calls 3 months later by the Kauhajoki-project, and the possible needs for more support were again screened. The feedback concerning the peer support group process was highly positive. One of the participants summed up that: “Overall, it has been great that this kind of process had been organized. The weekends have been quite hard, but at the same time you got energy from the peers with similar experiences,” and the other one commented: Every peer support meeting has been successful. It has been so nice to participate in them. The peers have become very close and important persons. The number of meetings was perfect and after every weekend I got a feeling of being understood and heard.
Conclusions
Losing a family member by a violent act causes grief and bereavement that cannot be compared with any other. Violent and unexpected death shatters the secure basis of living as it questions the beliefs about the goodness and benevolence of other people and of the world (Armour, 2006). It also increases the risk for the grieving process to complicate. In bereavement, people tend to seek support from family members and the presence of the family and other social support is a primary resource on resilience (Bonnano, 2006). Family members can activate their familiar stabilizing patterns and use both verbal and nonverbal ways to restore sense of safety and hope for the survival. This resilience is unique to each family before and after a death (Salloum & Rynearson, 2006), and active interventions aim to enhance it. The experiences of the professionally led peer support group process show that a long-term, multilevel, and theory-based professional psychosocial support is warranted as a complementary to the support offered by the natural social networks of the bereaved.
The professionally led peer support group process seems to be essential for the family members of those who lost their lives by a violent act. Spending time together as a family and as a peer to another bereaved in a safe and nurturing environment gives the bereaved relatives a possibility to concentrate in processing their painful experiences in multiple ways without the demands of everyday life (Palosaari, 2007). The overall, verbal and nonverbal, comprehension of what the other peers are going through is somewhat indescribable. The friendships that emerge might be short or life-long, but they are invaluable in the recovery process of grief. Seeing and observing other peers' coping can serve as an eye-opening experience from which everyone can learn from. The range of coping styles gets wider. The differences between personal and families' own habits, culture, and emotional expressions serve this purpose as well. There is no right or wrong way to grieve.
Professionally led peer support offers a channel to process different aspect of loss and grief under the guidance of experts. When the process is long enough, it gives the professional a change to observe the progress on both individual and group level. In cases when grieving stands still or complicates, or signs of depression or substance-abuse problems emerge, individual consultation and referral for further mental health service is simple. As the professionally led peer support reaches a large amount of bereaved relatives at the same time, it is also economically viable. Based on the experiences of the Kauhajoki school shootings peer support group process, this kind of multiprofessional collective assistance is an effective way to support the bereaved after a violent loss. The positive feedback from the participants and the professionals involved in the process allow us to recommend the intervention as an additional source of supporting the bereaved and their resilience in other countries as well. After all, the language of grief is universal, even if the expressions may vary culturally.
Footnotes
Acknowledgments
We warmly thank all the family members of those deceased in Kauhajoki school shooting for participating in the peer support group process and allowing us to walk beside them during the meandering paths of grief. We also thank Hospital District of South Ostrobothnia's management and Kauhajoki-projects board for making it possible to implement long-term psychosocial support. Tuija Turunen warmly thanks all her coworkers for co-operation and friendship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by Finnish Cultural Foundation's South Ostrobothnia Regional Fund (TT).