
Abstract
Advance directives provide health-care instruction for incapacitated individuals and authorize who may make health-care decisions for that individual. Identified factors do not explain all variance related to advance directive completion. This study was an analysis of an association between advance directive completion and death attitudes. Surveys that included the Death Attitude Profile—Revised were completed anonymously. Comparisons of means, chi-square, and logistic regression tests were conducted. Among individuals who did not consider themselves religious, the mean death avoidance attitude scores differed significantly among those with advance directives (mean = 1.93) and those without (mean = 4.05) as did the mean approach acceptance attitude scores of those with advance directives (mean = 5.73) and those without (mean = 3.71). Among individuals who do consider themselves religious, the mean escape acceptance attitude scores differed significantly among those with advance directives (mean = 5.11) and those without (mean = 4.15). The complicated relationships among religiosity, advance directives, and death attitudes warrant further study.
Introduction
The purpose of this study was to determine if there is an association between attitude toward death and whether one has executed an advance directive. An advance directive provides instruction regarding preferred health-care treatment when one cannot make decisions for oneself. The living will portion of the advance directive specifies the desired treatment, and the durable power of attorney for health-care portion gives permission to a specific individual to make health-care decisions on behalf of another individual (National Hospice & Palliative Care Organization [NHPCO], 2005). Laws about whether these documents are legally binding vary from state to state in the United States (NHPCO, 2005).
An advance directive guides care and aids in medical decision making that supports the individual’s wishes when the individual becomes unable to express those wishes (NHPCO, 2005). An advance directive may also reduce stress and conflict among family members and between family members and health-care providers (Centers for Disease Control and Prevention [CDC], 2012). Not having advance directives can result in expensive treatments and procedures being performed at the end of life that an individual may not have desired (CDC, 2012; Keenan, Varon, Walsh, Kish, & Fromm, 1996). Despite the benefits of advance directives and despite the Patient Self-Determination Act of 1990, which mandated that health-care facilities inquire about a completed advance directive and inform individuals of their right to complete an advance directive (Patient Self-Determination Act, 1990), estimates of the prevalence of advance directive completion in the United States range from 18% to 36% of the adult population (Pollack, Morhaim, & Williams, 2010; U.S. Department of Health and Human Services, Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy, 2008).
Some individuals do not know what advance directives are or why it may be important to have advance directives (Alano et al., 2010; Douglas & Brown, 2002; Golden, Corvea, Dang, Llorente, & Silverman, 2009; Salmond & David, 2005). Some fear that having an advance directive will result in a reduced level of care overall, highlighting a lack of trust in the health-care system (Bullock, 2006; Johnson, Kuchibhatla, & Tulsky, 2008). A belief that the physician or family will see that the patient receives the desired care may be present (Cohen, McCannon, Edgman-Levitan, & Kormos, 2010; Dupree, 2000; Kierner, Hladschik-Kermer, Gartner, & Watzke, 2010; Sahm, Will, & Hommel, 2005) or that God controls when death occurs, making advance directives irrelevant (Bullock, 2006; Cohen et al., 2010; Dupree, 2000). Some simply procrastinate, believing an advance directive may be necessary later, but not now (Douglas & Brown, 2002). Those who do have advance directives tend to have the following characteristics: older age, being female, being Caucasian, having a higher education, being religious, and being of higher socioeconomic status (Alano et al., 2010; Dobbins, 2007; Golden et al., 2009; Sam & Singer, 1993; Su, 2008; Wu, Lorenz, & Chodosh, 2008). Although in one study it was found that adults possessing higher health literacy were less likely to have executed advance directives (Campbell, Edwards, Ward, & Weatherby, 2007), other studies indicate an association between higher health literacy and completion of advance directives (Volandes et al., 2008; Waite et al., 2013).
Attitudes and their association with death-related variables have been measured in several studies. Education on end of life has been shown to positively influence health-care professionals’ and students’ attitudes toward death and older people as well as toward care of patients who were dying (Barrere, Durkin, & LaCoursiere, 2008; Eskildsen & Flacker, 2009; Frommelt, 2003; Smith-Cumberland & Feldman, 2006). In a 2006 study on the effect of end-of-life education, study participants who dropped out of the study were less likely than those who completed the study to state that talking about and planning for death was important (Braun, Karel, & Zir, 2006).
Families with a loved one who is ill or who may be at the end of life often want their physicians to be more straightforward about their loved one’s illness, prognosis, and planning for end of life (Braun, Beyth, Ford, & McCullough, 2007). Among health-care professionals, a positive attitude toward death and advance directives makes them more likely to not only have their own advance directives but also to discuss advance directive completion with their patients (Black, 2007; Campbell et al., 2007; Douglas & Brown, 2002). Patients who are asked by a health-care professional to complete an advance directive are more likely to do so (Alano et al., 2010).
Individuals who have devoted thought to making decisions about advance directives may desire to control their own health care or avoid aggressive care at the end of life (Eisemann & Richter, 1999). Attitudes toward advance directive completion may also be influenced by race and ethnicity (Bullock, 2006; Dupree, 2000; Eleazer et al., 1996; Johnson, Elbert-Avila, & Tulsky, 2005). For example, African Americans may not trust the health-care system or providers to provide adequate care if advance directives are in place or to follow completed advance directives (Bullock, 2006; Dupree, 2000). African Americans may also be more likely to rely on family members to make end-of-life decisions for them or on God to control one’s time of death (Dupree, 2000; Johnson, Elbert-Avila, & Tulsky, 2005). Steenpass and Smith (2008) found that Hispanics and African Americans were less likely to have advance directives than Caucasians. Eleazer et al. (1996) found that Asians are not likely to put end-of-life wishes in writing.
Individuals with anxiety about death or their own mortality may be more likely to not complete advance directives and to prefer life-prolonging treatment at the end of life (Ejaz, 2000; Golden et al., 2009). Those with less fear of death have been shown to be more likely to have completed advance directives (Dobbs, Emmett, Hammarth, & Daaleman, 2012).
Although multiple studies have shown that death-related thoughts and feelings may be associated with advance directive completion, none have examined the potential relationship between four death attitudes and the completion of advance directives. The current study analyzes fear of death, death avoidance, approach acceptance of death, and escape acceptance of death attitudes to explore the possibility of a relationship between these attitudes and the completion of advance directives.
Methods
Subject Recruitment
Study participants waiting for an appointment in the offices of a primary care physician, chiropractor, or ophthalmologist were asked by the staff at the appointment registration desk if they would like to participate in the study. Participants gathered for an activity at a senior living or activity center were approached for study participation by either the program activity director or the primary researcher.
A cross-sectional survey research design was used in this study conducted with individuals in waiting areas of physician offices in the southwest Michigan area as well as with individuals involved with activities at two senior centers in southwest Michigan. The population was adults 18 years of age or older gathered in the offices of a primary care physician, chiropractor, ophthalmologist, or clinic or at a senior living center in southwest Michigan.
Measures
A survey tool collected information about seven factors previously identified as being associated with advance directives in the literature: age, sex, race, education, religiosity, income, and health literacy. Because of the small sample size, information about age was initially collected categorically and was later dichotomized into groups of individuals 18–59 years of age and 60+ years of age. Race was dichotomized into Caucasian and non-Caucasian. Education was categorized into two groups: high school degree or less and bachelor’s degree or higher. Religiosity was defined as whether the individual taking the survey considered himself or herself religious (Alano et al., 2010). Income was divided into two groups: at or below $76,385 (the estimated household median income in Michigan for a family of four in 2010–2011 [U.S. Department of Health and Human Services, Administration for Children and Families, 2010/2011]) or above $76,385. Health literacy, measured with the Newest Vital Sign (Weiss et al., 2005), was categorized as adequate or less than adequate.
Yes–no questions were asked about the presence of a living will and a durable power of attorney for health care, and definitions were provided for each. A living will was defined as “a written document that specifies the health care treatment you want if you become unable to make health care decisions for yourself.” A durable power of attorney for health care was defined as “a written document that identifies who you want to make health care decisions for you if you become unable to make health care decisions for yourself.” A yes answer to the presence of either a living will or a durable power of attorney for health care or both was counted as yes to having advance directives.
The survey tool also included the Death Attitude Profile—Revised (DAP-R), which collected data about death attitudes. The reliability of the DAP-R, measured by internal consistency, had alpha coefficients of 0.84 to 0.97. Regarding validity, all items in the DAP-R achieved 70% to 90% agreement with other validated scales (Wong, Reker, & Gesser, 1994). The DAP-R measures level of agreement with five different death attitudes. Fear of death or dying (shortened to fear of death by Wong et al., 1994) and death avoidance are both negative attitudes toward death. The approach acceptance subscale measures one’s agreement with the idea that what happens after death is positive, serene, and beautiful. The escape acceptance subscale measures one’s agreement with the notion that death is a welcome alternative to the difficulties of this life. The neutral acceptance subscale was found by two studies to be measuring two constructs—natural acceptance of death and neutral acceptance of death—rather than one construct (Clements & Rooda, 1999–2000; Ho, Chan, Chow, Pon, & Ng, 2010). Since the other death attitude subscales could be used individually (Clements & Rooda, 1999–2000), the neutral acceptance subscale was not used in the current study.
Two medical doctors, one an expert on care at the end of life and former chair of a university institutional review board and the other a hospice medical director, hospital chief of staff and an internist with his own practice, reviewed the survey instrument tool and the methodology. As health-care professionals adept at discussing death and dying with their patients, their review was helpful in determining the order of the questions on the survey as well as streamlining the data collection process. The researcher then conducted a pilot study in the office of a primary care physician in southwest Michigan to test the proposed data collection process. No revisions were required in the tool or the methodology. The final tool comprised 46 items with an overall fifth-grade reading level (Online-utility.org, n.d.) and could be completed in approximately 10 minutes. Approval was obtained from Western Michigan University’s Human Subjects Institutional Review Board to conduct this research.
Research Procedure
Each participant received an informed consent letter and a survey to be completed anonymously. Consent to participate was demonstrated by returning completed surveys to a box in a central location at each site.
The estimated size of the target population was 2,000 adults, that is, the total number of adults in the physicians’ offices and senior centers. For a confidence level of 0.05, an effect size of 0.5 and statistical power of 0.8, the minimum sample size required for the study was 64 individuals (DanielSoper.com, n.d.). Participation rate was estimated at 33% of individuals approached about participation. Seventy-one surveys were collected for the sample, but due to missing data on advance directives only 67 surveys or 94% of the total collected surveys were used.
Data were entered into a Statistical Package for the Social Sciences database. Frequencies and mean death attitude scores were obtained, and chi-square and multivariable binary logistic regression tests were conducted to determine whether there was an association between attitude toward death and the presence of an advance directive after controlling for potential confounders.
Results
Selected Characteristics of Participants Completing Advance Directives.
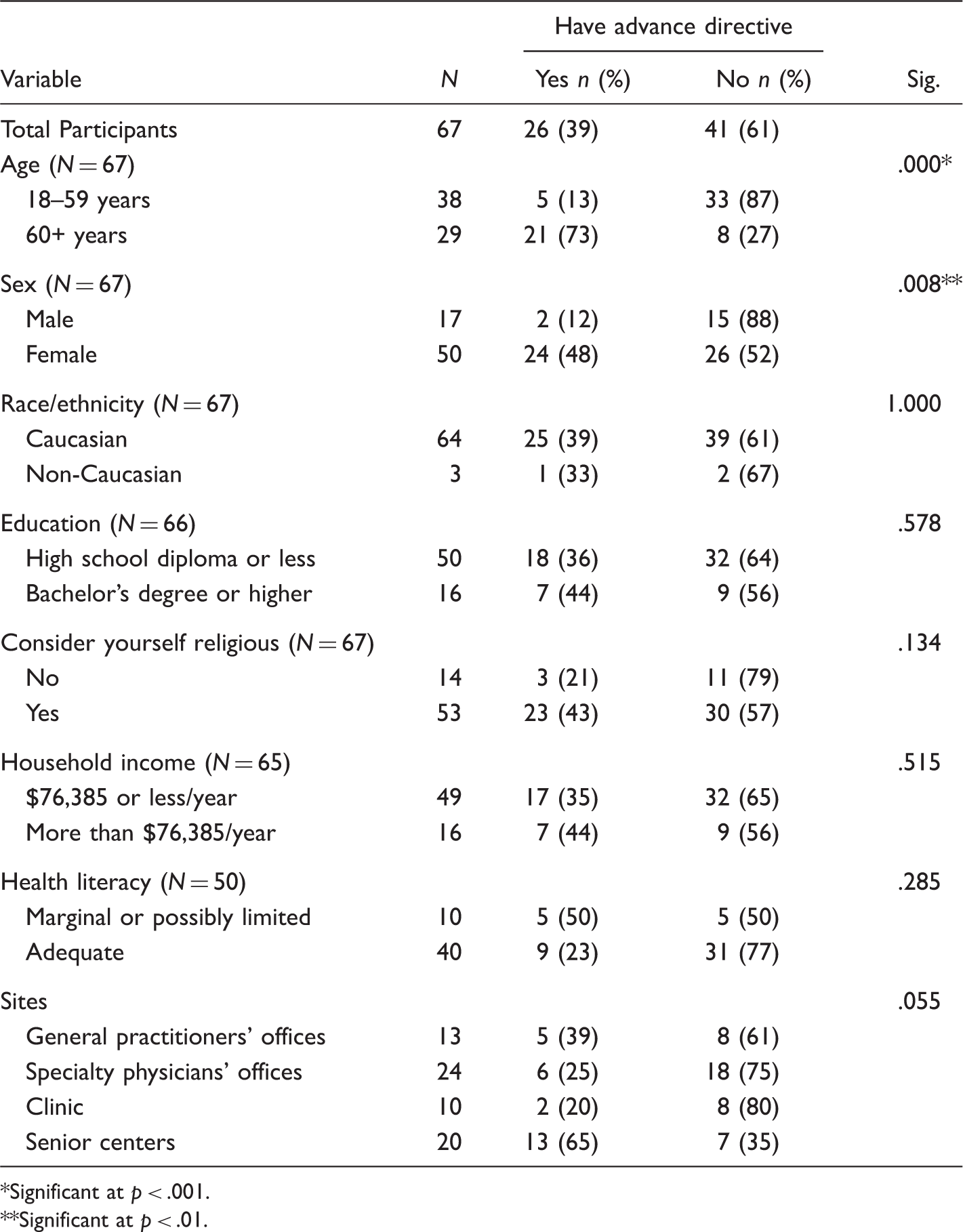
Significant at p < .001. **Significant at p < .01.
Association Between Demographics and Advance Directive.
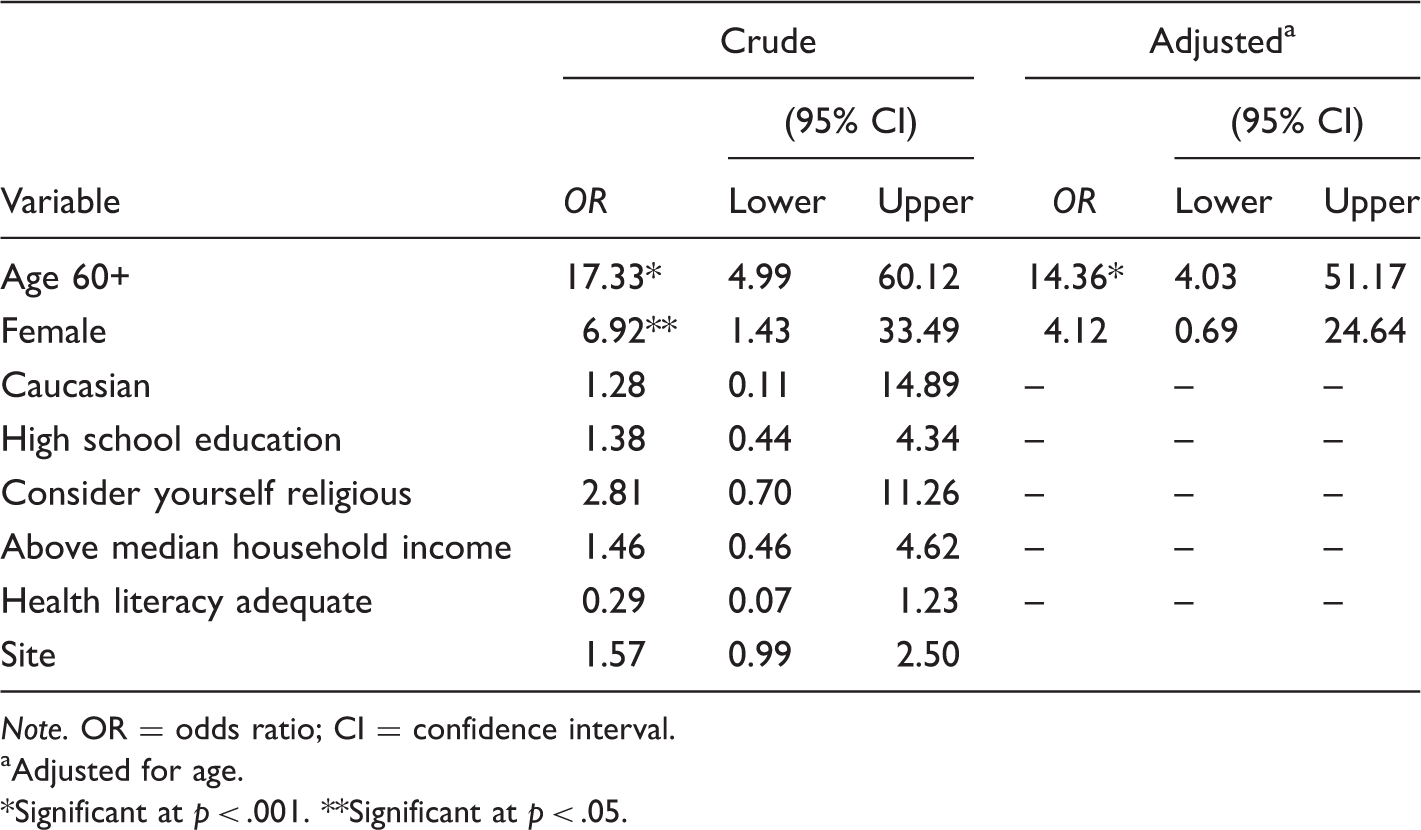
Note. OR = odds ratio; CI = confidence interval.
Adjusted for age.
Significant at p < .001. **Significant at p < .05.
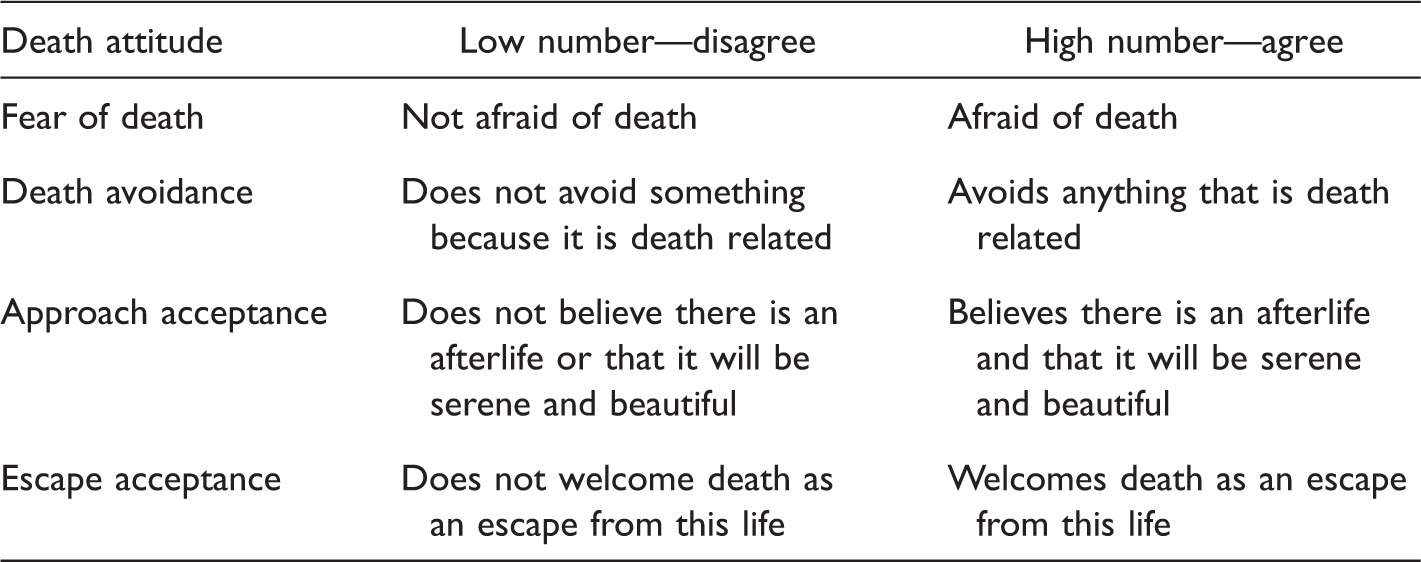
Death Attitudes and Meaning of High/Low Scores.
The mean score for the attitude fear of death was 2.96; 79% of study participants had some level of disagreement with this attitude. The attitude death avoidance had a mean score of 3.07; 73% of participants disagreed with this attitude. The approach acceptance attitude had a mean score of 5.51 and agreement by 76% of participants. The attitude escape acceptance had a mean score of 4.54. Eighteen percent of participants were undecided regarding this attitude, and 51% agreed with it. Frequencies of agreement and disagreement with each of the death attitudes as well as the mean score of each attitude are listed in Figure 1.
Types, frequencies, and mean scores of death attitudes. Levels of agreement–disagreement: strongly disagree (1), disagree (2), moderately disagree (3), undecided (4), moderately agree (5), agree (6), and strongly agree (7).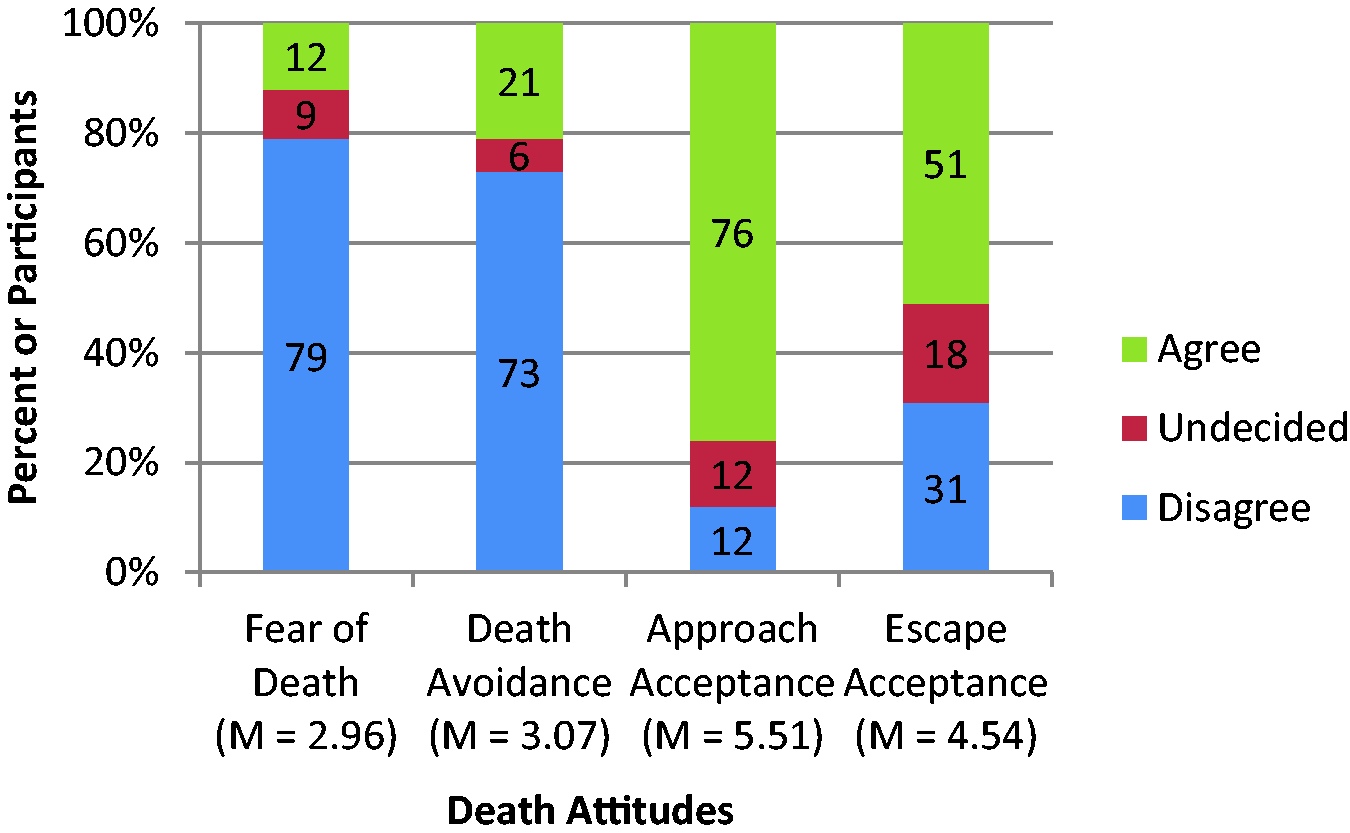
Association Between Death Attitude and Advance Directive: Crude and Adjusted Analyses.
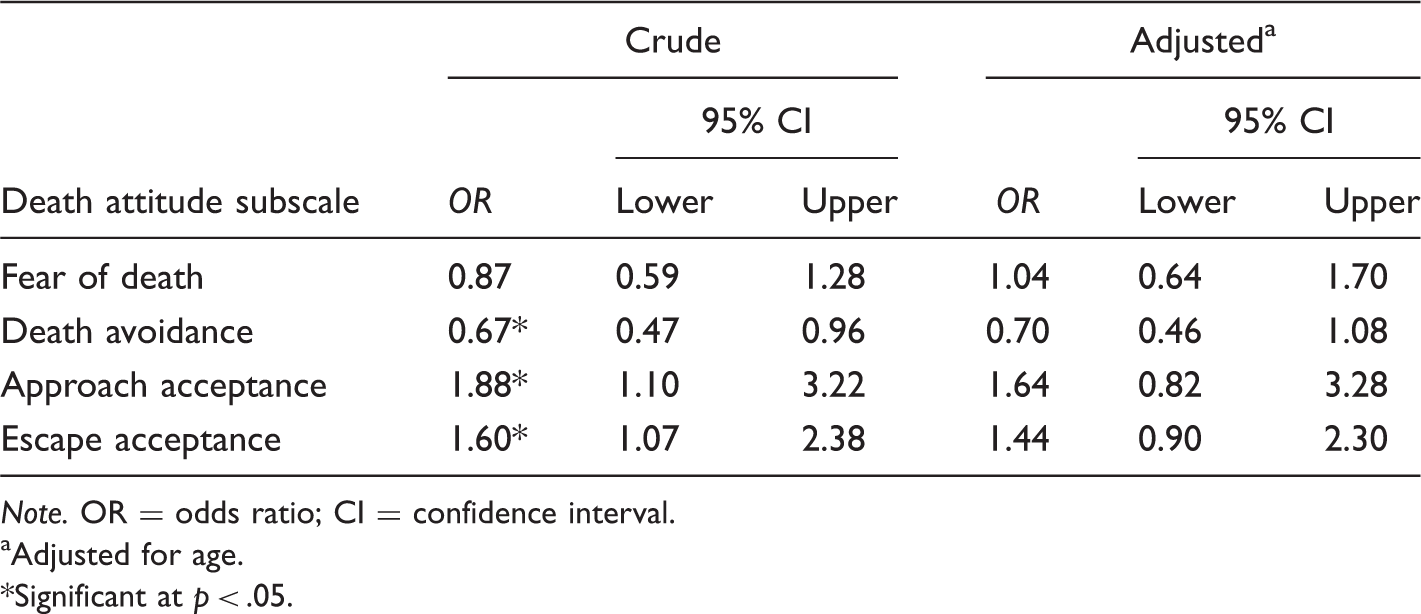
Note. OR = odds ratio; CI = confidence interval.
Adjusted for age.
Significant at p < .05.
Comparison of Death Attitude Mean Scores by Presence/Absence of Advance Directives and Religiosity.
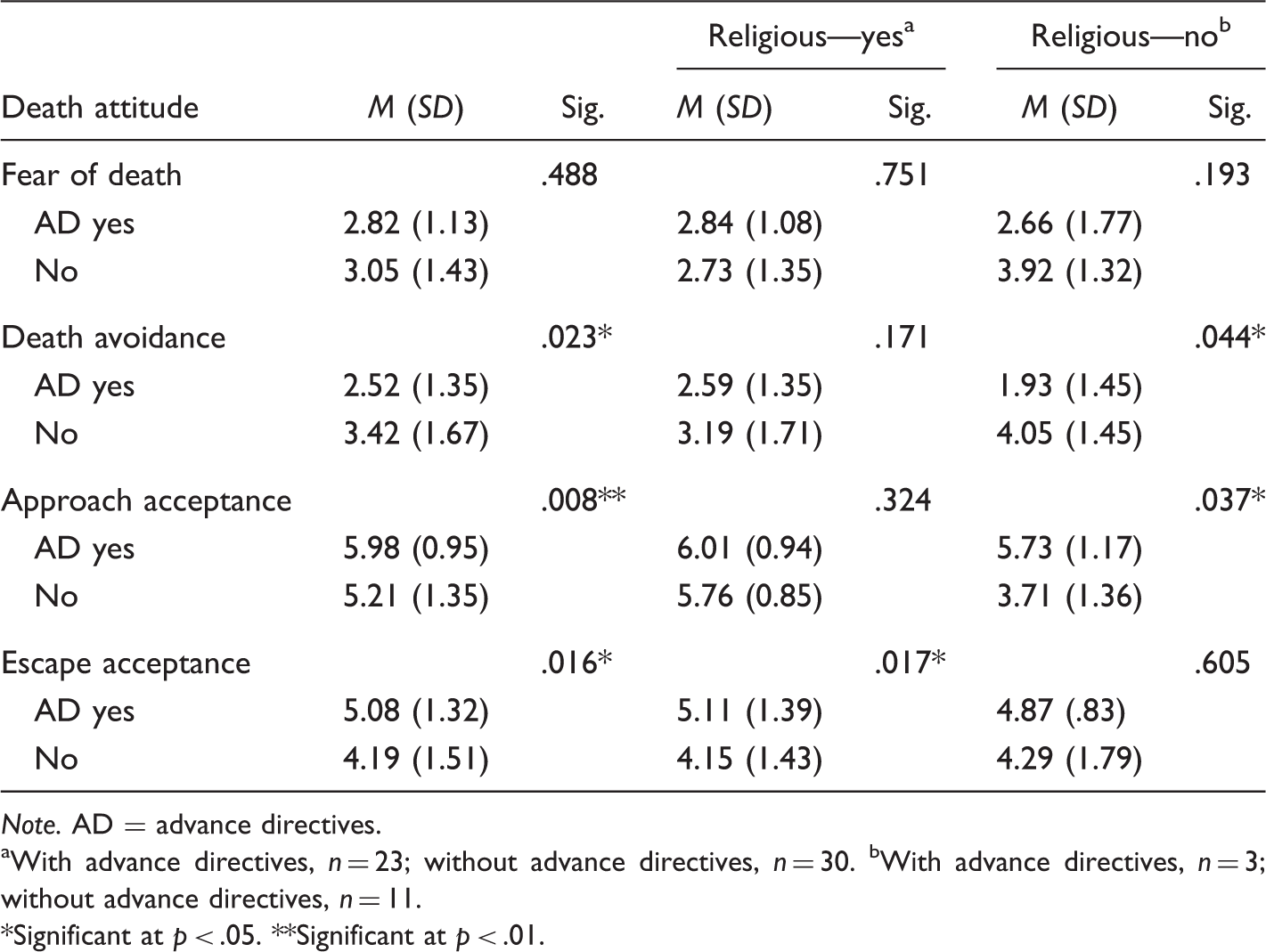
Note. AD = advance directives.
With advance directives, n = 23; without advance directives, n = 30. bWith advance directives, n = 3; without advance directives, n = 11.
Significant at p < .05. **Significant at p < .01.
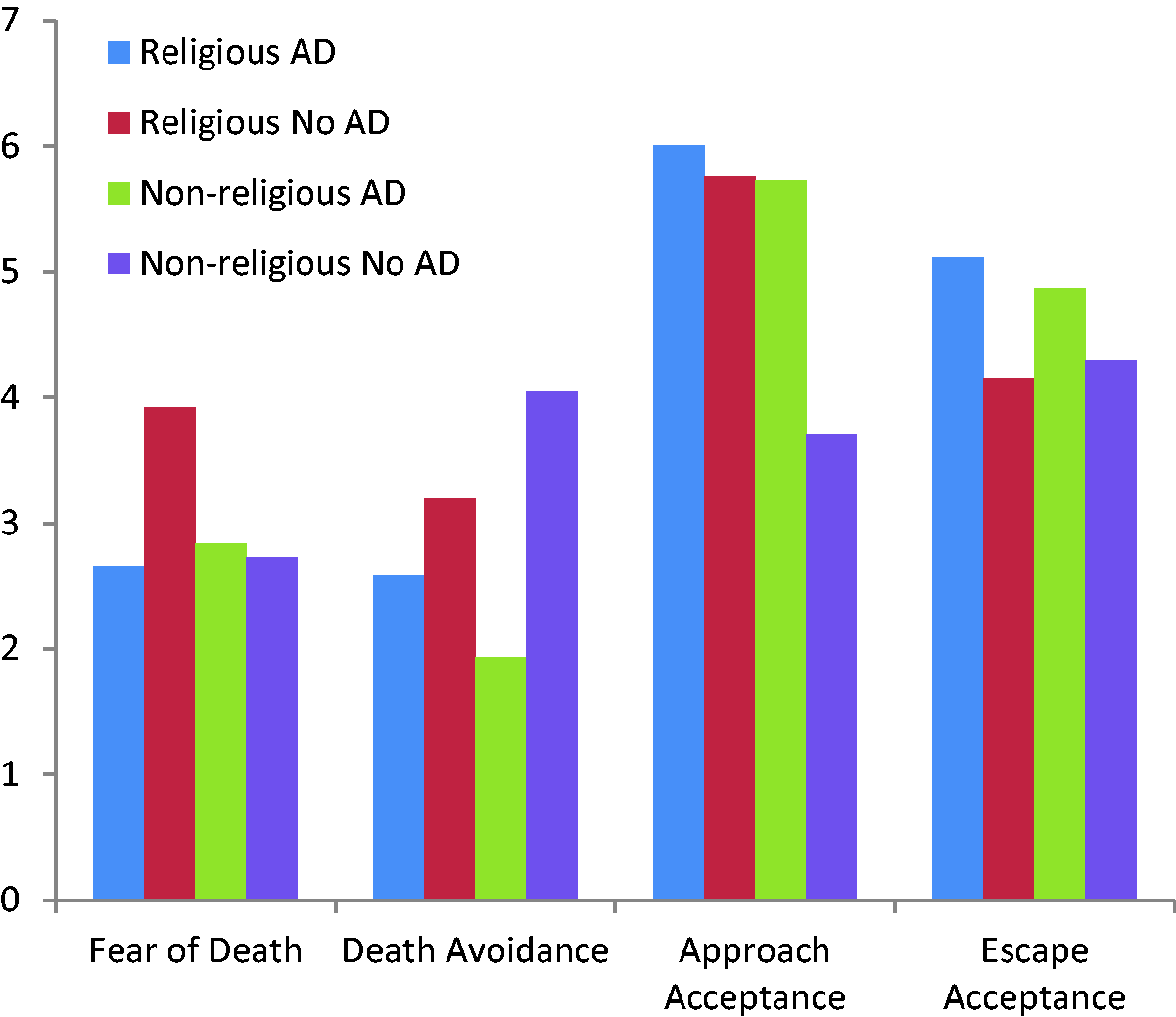
Mean death attitudes scores by advance directives and religiosity. For each death attitude, mean scores are displayed for those with and without advance directives and for those who did and did not consider themselves religious.
Discussion
Regarding the research question, for all death attitudes except fear of death, there was a significant difference in mean death attitude scores among those with advance directives compared with those without advance directives. However, when the variable of religiosity was added, the results were only significant in the same three death attitudes according to whether one did or did not consider oneself to be religious. Among study participants who considered themselves to be religious, those with advance directives agreed more strongly with the death attitude escape acceptance than those who did not have advance directives. Among study participants who did not consider themselves religious, those with advance directives disagreed more strongly with the death attitude death avoidance than those who did not have advance directives. Finally, among study participants who did not consider themselves religious, those with advance directives agreed more strongly with the death attitude approach acceptance than those who did not have advance directives.
No significant differences between mean death attitude scores for fear of death and the presence or absence of advance directives were found regardless of whether one considered oneself religious. This does not support Dobbs’ et al. (2012) finding that there is an inverse relationship between fear of death and the presence of advance directives.
Religious individuals with advance directives agreed more with the escape acceptance attitude toward death than religious individuals without advance directives. Having this type of acceptance of death represents a desire to leave the difficulties of this world (Wong et al., 1994). It is logical that individuals with this death attitude would be more likely to have advance directives, as advance directives could be considered a tool to avoid having futile health-care treatment at the end of life that may create a barrier to escaping this world. An advance directive may also be perceived as preventing a delay in entering a positive afterlife. In this study, it was nonreligious individuals with advance directives who agreed more strongly with the approach acceptance attitude than nonreligious individuals without advance directives. Wong et al. (1994) define death acceptance as the “cognitive awareness of one’s own finitude and a positive (or at least neutral) emotional reaction to this cognizance” (p. 124).
There were only three non-religious study participants who had advance directives. Two of these individuals had the same death avoidance score (1—strongly disagree) and similar approach acceptance scores (6—agree and 7—strongly agree). The third individual, however, was undecided about the death avoidance attitude and only moderately agreed with the approach acceptance attitude. Were this study to be repeated, it would be desirable to have a larger sample overall, but it would be particularly important to have a larger subset of nonreligious individuals with advance directives.
Among nonreligious individuals, those without advance directives were more undecided about the death attitude death avoidance than were those participants with advance directives. The latter group disagreed strongly with this death attitude. It is again important to note that the latter group was composed of just three individuals with relatively widely varying scores.
The role of religion in this study is not immediately obvious. The difference between religion and spirituality may be a noteworthy distinction. Some individuals may consider themselves religious or spiritual (Cicirelli, 2011), and this may have affected the outcome of this study. Religious may be defined as relating to shared ritual and unique traditions of a faith community, and spiritual may be defined as relating to meaning and purpose of life and connectedness with a power greater than oneself (Gilbert, 2007; Neal, 2007).
Black (2007) found that health-care professionals, including physicians, with an approach acceptance attitude toward death were more likely to initiate a conversation about advance directives with their patients than health-care professionals who did not possess this attitude toward death. Gordon (1999) found that patients who were asked by a physician or nurse about their preferences for care at the end of life were three times as likely to complete advance directives. Health-care professionals may also want to consider exploring an individual’s religious or spiritual beliefs in a conversation about advance directives.
In the study, a higher percentage of participants who considered themselves religious had advance directives compared with those who did not consider themselves religious. This is consistent with the literature, which states that being religious is associated with having advance directives (Alano et al., 2010). Most of the surveys were collected in rural communities, and this may have influenced the results. In a qualitative study of family members of nursing home residents with dementia, Gessert, Elliot, and Peden-McAlpine (2006) found individuals from rural communities to be more accepting of the possibility of death for their loved ones than those family members who lived in urban areas. Future research could employ data-collection methods that permit a comparison of rural and urban death attitudes and advance directive completion.
The results of the study also showed that there was a positive association between age and the presence of an advance directive. Among the participants in the study sample, the older the participant was, the greater the odds were that one had an advance directive. There may be multiple explanations for this result. Compared with younger adults, older adults may be significantly less afraid to discuss death (Sessanna, 2008). Some studies have shown that anxiety about death is lower among older adults than it is among younger adults (Fortner & Niemeyer, 1999; Hallberg, 2004; Schrader, Nelson, & Eidsness, 2009–2010), and some have shown no difference between the two age groups (Conte, Weiner, & Plutchik, 1982; De Raedt, Koster, & Ryckewaert, 2013; Moody, Beckie, Long, Edmonds, & Andrews, 2000). Future research could include a longitudinal study to discover whether attitudes toward death change over time.
Another finding was that more than half of the study participants who lived at senior living centers had advance directives, which may make advance directive completion in these settings more of a social norm. People may prefer to discuss their own advance care planning with someone who has been specifically trained to discuss it (Michael et al., 2013). Perhaps individuals moved into assisted living when their spouse died and as a result they felt their own mortality more acutely, and perhaps facility admission staff are specially trained in the methods of having discussions about advance directives. Widowed individuals are more likely than married individuals to choose to spend their end of life in a facility other than their home (Wilson, Cohen, Deliens, Hewitt, & Houttekier, 2013), and individuals without partners are more likely to have advance directives (Bischoff, Sudore, Miao, Boscardin, & Smith, 2013). Perhaps widowed study participants had been exposed to hospice care with their dying spouse and wanted to ensure that comfort care for themselves (Bischoff et al., 2013). Individuals whose spouses died after having completed advance directives are more likely to do their own advance care planning (Carr, 2012).
Perhaps the very act of moving into a senior living center was part of a larger advance care plan for these study participants. Finding themselves alone after the death of a spouse, an individual’s adult children may have encouraged them to enter assisted living as a way of initiating some form of advance care planning. The more encouraging an adult child is for his or her elderly parent to do advance care planning, the more likely that child is to be selected by the parent to be the durable power of attorney when the parent does execute advance directives (Boener, Carr, & Moorman, 2013).
The advance directive completion rate among 60+ year olds living in the community was similar to the advance directive completion rate of the same age group living in senior centers. Among all study participants who had executed advance directives, half lived in the community and half lived in senior centers. These do not support Hopp’s (2000) finding that most adults who live in the community (as opposed to living in a facility) do not have advance directives. However, Black and Reynolds’ (2008) finding that older adults living alone are less likely to have advance directives may have contributed to this if the households of older study participants in the community included other people. The advance directive completion rate of this study is also not consistent with results found by Hirschman, Abbott, Hanlon, Bettger, and Naylor (2012), that residents of assisted living facilities had higher advance directive completion rates than residents who lived in the community or at home.
Demographically, the results of the study are largely consistent with the literature on advance directives. A higher percentage of advance directives were found with older people, women, and individuals with a higher socioeconomic status. More highly educated individuals had advance directives, and among all those with advance directives, a higher percentage had higher health literacy. The outcome on race or ethnicity could not be determined because too few individuals who identified as non-Caucasian participated in the study.
The sample was representative of the two-county population in race and education only. A larger sample from each county may have been more demographically representative of each county overall. More important would be the collection of a sample that is representative of attitudes toward death in the two counties. Most of the surveys were collected at the sites of health-care practitioners. This excludes those who may not see a health-care practitioner, and who may, subconsciously or otherwise, fear death. Or some individuals may have a death avoidance attitude that is manifested by avoiding visits to health-care practitioners.
One of the major strengths of this study is that, to the researchers’ knowledge, it is the first to analyze the association between four attitudes toward death and the presence of advance directives. The other major strengths are the strong reliability and validity of the DAP-R.
Limitations include measuring religiosity with one question with dichotomous answers. A more sophisticated tool showing degree of religiosity and distinguishing religiosity and spirituality may show more nuanced results. The NIA–Fetzer Short Form for the Measurement of Religiousness and Spirituality (Idler et al., 2003) contains measures of religiosity and spirituality that may pertain to health and would likely provide a more thorough analysis of religiosity or spirituality.
Another limitation is the use of a small convenience sample in two southwest Michigan counties; therefore, the results are not generalizable. Additionally, it might have improved the study to use a different household income figure than the figure for a family of four because that family size may not represent the family size of many older adults. More pertinent information might have been collected if a household income for a family of one or two had been used.
Conclusion
In this study, death attitudes, religiosity, and the presence or absence of advance directives combine in varying ways that make rendering any definitive conclusions difficult. More research is needed to fully analyze the relationships among the three variables and particularly to understand the nuanced influence of religion and spirituality. Age was found to be significantly associated with having advance directives, supporting previous research. Learning whether attitudes toward death change as one ages, particularly as attitudes relate to changing religious or spiritual beliefs could also be a focus of future research.
Most study participants who lived at senior living centers had advance directives. The possible influence on advance directive completion of residing in assisted living may be a topic for future research. A potentially confounding variable in the current study is the rural versus urban demographic, and it may be important to include this variable in any future studies.
Future research on death attitudes, advance directive completion, and the role of religiosity should be done with larger groups of individuals representing the population demographically. A wide range of death attitudes and relatively equal numbers of those with and without advance directives should be represented. Finally, the influence of diagnosis and quality of life and their relationship to attitude toward death and advance directive completion would add valuable information to the field of advance care planning.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.