
Abstract
The Dual Process Model of Coping with Bereavement (DPM) was put forward as a framework to help understand reactions to the death of a loved person. Since its inception, there have been various developments and further specifications regarding the model’s parameters. A number of researchers have assessed the model’s contribution and put some of its parameters to empirical test. It has also been applied in clinical practice. Despite generally positive assessment among both scientific and applied communities, we recently discovered what we consider to be a major shortcoming. The concept of overload has been neglected. Incorporation of this feature helps explain the preponderance of mental and physical health problems beyond the previous DPM focus on complications of grief. In this article, we incorporate the phenomenon of overload within the original framework, illustrating its application, and we discuss broader implications for coping and adaptation to bereavement.
Bereavement is understood as the situation of losing a loved one through that person’s death, one that is associated with mental and physical health difficulties, including increased risk of the bereaved person dying (Stroebe, Schut, & Stroebe, 2007). Not surprisingly, then, bereavement has become the subject of increasing scientific investigation, including our own development of the Dual Process Model of Coping with Bereavement (DPM; Stroebe & Schut, 1999). The DPM was designed to overcome limitations in the previous phase (e.g., Bowlby, 1980) and task (Worden, 1991) models, while also building on and integrating their strengths (cf. Stroebe & Schut, 2015). In the years since our original publication of the DPM, there has been encouraging interest in the model from both researchers and clinicians. To illustrate, on one hand, scientists have gone to considerable lengths to put parameters of the model to empirical test, as reflected in a Special Issue of Omega: Journal of Death and Dying (edited by Richardson, 2010). Such efforts have continued since that publication (e.g., Ryckebosch-Dayez, Zech, Mac Cord, & Taverne, 2016). On the other hand, mental health practitioners have, for example, used and even reproduced the DPM figure in guidelines for counseling professionals and other caregiving practitioners (e.g., Wilson, 2014). Its relevance to therapeutic intervention for those with complications has been examined by researchers and clinicians alike (e.g., Caserta & Lund, 2007; Caserta, Lund, Utz, & Tabler, 2016; Caserta, Utz, Lund, Swenson, & de Vries, 2014; Shear, Frank, Houck, & Reynolds, 2005; Zech, 2016). Furthermore, interest in the model has spread to diverse countries. To illustrate, its components have been integrated in a complicated grief intervention model designed for the South African context (Drenth, Herbst, & Strydom, 2010) and—further afield and in a different setting again—the model was reported in a review of new perspectives in bereavement for Chinese readership, including the DPM figure in translation (Liu & Li, 2007).
Does the DPM adequately capture the nature of coping with loss in all its complexity? We would be the first to admit that—like the earlier models—it has limitations, and some shortcomings have been identified by others too (e.g., Carr, 2010). We have tried to refine the model and explore its broader application over the years since initial publication (cf. Stroebe & Schut, 2010, 2015). For instance, we have recently integrated a family-level coping perspective more systematically and extensively than in previous accounts (Stroebe & Schut, 2015). Nevertheless, we have come to a remarkable realization: Despite long acquaintance with and many deliberations about our model, we have actually been missing what we now consider to be an important link in our scientific description of what bereaved people have to deal with (stressors), how they go about dealing with such manifestations (coping), and consequently, with the adequacy of the coverage of complications associated with this stressful life event (including those requiring professional care). In short, we have neglected the possibility of stress overload (having more to cope with than one feels one can manage, defined more precisely later). Furthermore, this concept has not received specific attention in other models of coping with bereavement. Not surprisingly, then, the possibility that overload may lead to something like burnout among bereaved persons has also been neglected (while burnout is a well-acknowledged negative outcome among caregivers grieving the deaths of their patients or clients, e.g., Lyckholm, 2001). Therefore, in this article, after summarizing the main parameters of the original DPM, we describe the extension to the original rationale and description, to include the phenomenon of overload and its implications for coping with bereavement and the range of health-related consequences.
Summary of the Original DPM Framework
We have described the DPM elsewhere (e.g., Stroebe & Schut, 1999, 2010), so only a brief overview will be given here. The model is not complex; Figure 1 portrays its basic parameters. The DPM is a taxonomy of coping with bereavement. It is compatible with the earlier, generic cognitive stress theory (CST) of Lazarus and Folkman (1984; Folkman, 2001). The purpose in developing a specific bereavement model was to describe ways that people come to terms with the loss of a loved person. Unique aspects of the DPM include the integration of two sources of stress, labeled loss- and restoration-oriented stressors. Such stressors can be understood as perceived concerns/preoccupations, or burdens, which have to be confronted and addressed or dealt with in some way. Which brings us to coping. Coping refers to processes, strategies, or styles of managing (reducing, mastering, and tolerating) the (perceived) situation in which bereavement places the individual (cf. Folkman, 2001). A basic component of the DPM is an emotion regulation coping process, labeled oscillation, represented by the jagged line in the middle of Figure 1. We elaborate on these components next.
Dual process model of coping with bereavement (Stroebe & Schut, 1999).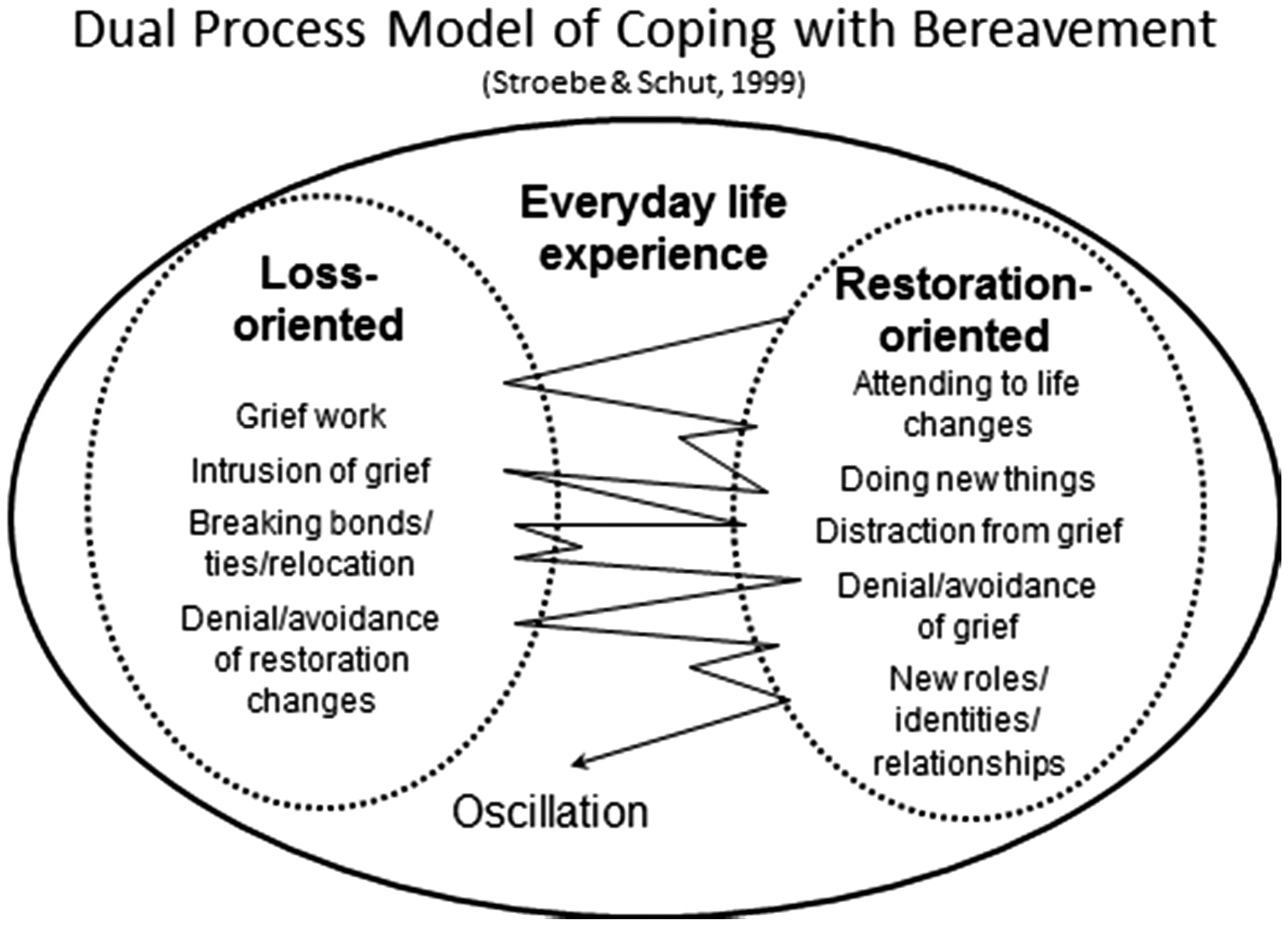
Loss orientation (LO) refers to the bereaved person’s focus on aspects of the loss experience itself, including the process of confronting, trying to accept the fact of loss, reminiscing about the deceased person, and visiting the burial place to remain close to him or her. As such, they encompass the “grief work” concept of earlier theories (e.g., Bowlby, 1980; Freud, 1917/1957), the notion that one must confront the reality of loss in order to adapt to it and move on (cf. Stroebe, 1992). Many decades ago, Parkes (1972) caught the essence of grief work, pinpointing the preoccupation with thoughts of the lost person, the painful repetitious recollection of the loss experience, and the repeated attempts to make sense of the loss. Grief work can probably be well understood as the essence of grieving; it is incorporated in loss-oriented coping, where the bond with the deceased person also features prominently. LO not only occurs on an individual but also on an interpersonal level (for details, see Stroebe & Schut, 2015). Bereaved persons do not typically grieve alone; for example, the death of a loved person leaves the family as a whole to grieve. On one hand, family members may support each other through their grief, but on the other hand, they may also at times experience difficulties associated grieving alongside each other.
Restoration orientation (RO) refers to the secondary stressors that are associated with the occurrence of a bereavement. These hassles do not relate directly to the loss of the person per se but come about as an indirect result of it. They include reorientation in a world that has changed in many ways due to the death. Many aspects of one’s daily life may need to be rethought and planned afresh. To illustrate, it may be essential to relocate to less expensive living quarters, or go out to work, to earn an income lost due to the death of the breadwinner; or to seek help with upbringing and home care of children, had the deceased partner been the primary caregiver. And just as there are interpersonal aspects in LO coping, so does RO encompass such aspects too (e.g., family-level decision-making regarding relocation). RO as well as LO are sources of stress, associated with emotional consequences such as distress and anxiety, as well as other mental and physical health ramifications.
According to the DPM, both LO and RO are part of the grieving process; one needs to attend to each orientation in order to adjust to a world in which the loved person is no longer physically present. This brings us to a feature of the DPM which is one of its most distinctive, namely, the notion of oscillation. Oscillation is a dynamic, regulatory coping process, based on the principle, indicated earlier, that the bereaved person will at times (have to—in order to come to terms with the bereavement) confront aspects of loss (deal with LO stressors), while at other times he or she will (have to) avoid them. The same applies to restoration (RO) tasks: At times, these need to be attended to (at which times LO coping cannot take place) and this goes hand-in-hand with avoidance of RO at other times too. But one cannot cope the whole time, it is exhausting to do so a lot of the time; time off is needed, where nonbereavement-related activities are followed or when the person simply relaxes and recuperates. Life goes on, and this, in and of itself, can at times be quite beneficial and healing. The components described earlier combine to make coping with bereavement—according to the DPM—a complex regulatory process of confrontation and avoidance.
A feature of the DPM that is central to identifying the overload missing link is its integration of forms of complicated grief. The original DPM-enabled placement of previously established types labeled as chronic, as well as absent, delayed or inhibited grief, following the early categorization of complications described, for example, by Lindemann (1944) and Parkes and Weiss (1983). Chronic grief refers to the long-lasting presence of symptoms of intense grief, associated with an absence of progress in coming to terms with loss, and can be understood as a loss-oriented syndrome, the focus being quite exclusively on the lost relationship and continued attachment to the deceased person. Chronic grief is similar to Prigerson’s prolonged grief construct (cf. Prigerson & Jacobs, 2001). By contrast, absent, inhibited, or delayed grief is more controversial and is typified as being overly restoration-oriented, characterized as it is by persistent avoidance of confrontation with the reality of death, tenacious efforts to carry on as normal, perhaps by plunging back into work, and by dealing with the secondary (indirect) changes that have occurred due to the death. In both of these types of complicated grief—loss-oriented and restoration-oriented—reactions are understood to be extreme, with extensive focus on one and avoidance of the other orientation—and possibly, little time off taken for respite and recuperation (e.g., chronic grief may be dominant and pervasive most of the time).
We also described a different type of complication, associated with the oscillation process. Traumatic bereavements may cause difficulties in alternating smoothly (less balanced or controlled or coherent) between the LOs and ROs (and in taking time off). While we are describing a coping process, not patterns of symptoms, this disturbed process can perhaps be understood in the context of the diagnostic criteria for posttraumatic stress disorder, namely, intrusion-avoidance symptomatology (cf. American Psychiatric Association, 2013; see also Horowitz, 1986).
The Missing Link: Overload
Defining the Concept
As indicated earlier, we consider an important missing link in the original DPM to be something well captured in the term overload. Overload can be defined as the bereaved person’s perception of having more than s/he feels able to deal with—too much or too many activities, events, experiences and other stimuli. 1 As such, it incorporates but is broader than the concept of bereavement overload (the occurrence of multiple losses of loved ones in close succession, Kastenbaum, 1969 2 ). In the original DPM, we only identified loss-oriented and restoration-oriented sources of stress. Although we described the need for balancing between these two types of stressor (because both of these components of the bereavement situation need to be tackled), we did not explicitly state the possibility that bereaved persons may actually encounter more loss- or more restoration-oriented stressors than they feel able to deal with or that they may actually experience a sense of conflict between dealing with stressors (i.e., the feeling that one should be dealing with something else when one is trying to manage a particular stressor). We did not take account of the possibility that there can be perception that one cannot cope, that the burdens are too overwhelming, there is too much to deal with. At such times, overload may lead one to feel pressure, making one worried, worn out, distressed, and anxious. This phenomenon tallies too with the reports of many bereaved persons themselves that they feel extreme fatigue and inability to deal with the demands surrounding them (cf. Dyregrov & Dyregrov, 2008).
Stressor Overload
In principle, within the DPM framework, it would not be difficult to inventorize multiple LO and RO stressors and assess the subjective feelings of overload associated with them. The weighing scales depicted in Figure 2 illustrate this.
One potential case of overload: loss-oriented.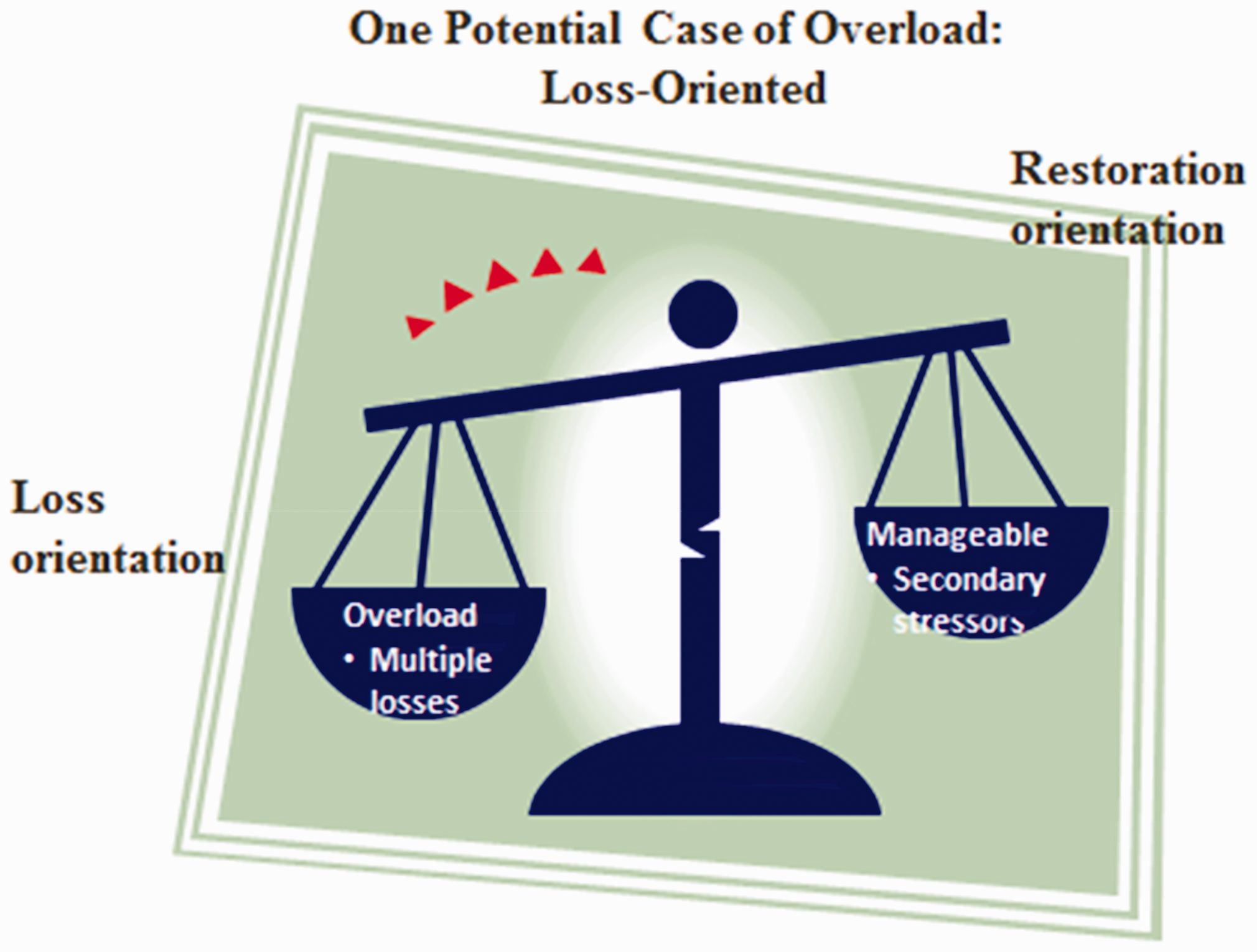
Overload as depicted here involves too much to deal with on the loss-oriented side.
3
If more than one bereavement occurs simultaneously or in quick succession, it may be difficult to grieve for the different losses at the same time. However, overload can also derive from experiencing too many restoration stressors. Interpersonal difficulties (e.g., quarrels and disagreements) may contribute to a feeling of overload. Furthermore, too many stressors may occur in both loss and restoration categories (e.g., multiple bereavements combined with financial and rehousing consequences). Finally, making it even more multifaceted—loss- or restoration-oriented overload may be augmented by an overload of things that have nothing to do with the bereavement, either directly or indirectly (e.g., extraneous to bereavement demands on one’s time; too much to do at one’s workplace). An example in the last category is the occurrence of a relative becoming seriously ill and needing time-consuming care, leaving little time for grief and grieving. An even more complex possibility comes to mind: The occurrence of positive experiences at the same time during the loss of a loved one (e.g., the case of twin birth, where one twin lives, while the other dies); it would seem very hard to make and break a bond at one and the same time. These alternative possibilities for experiencing overload are placed in the traditional DPM framework (Figure 3).
DPM: Effects of multiple stressors.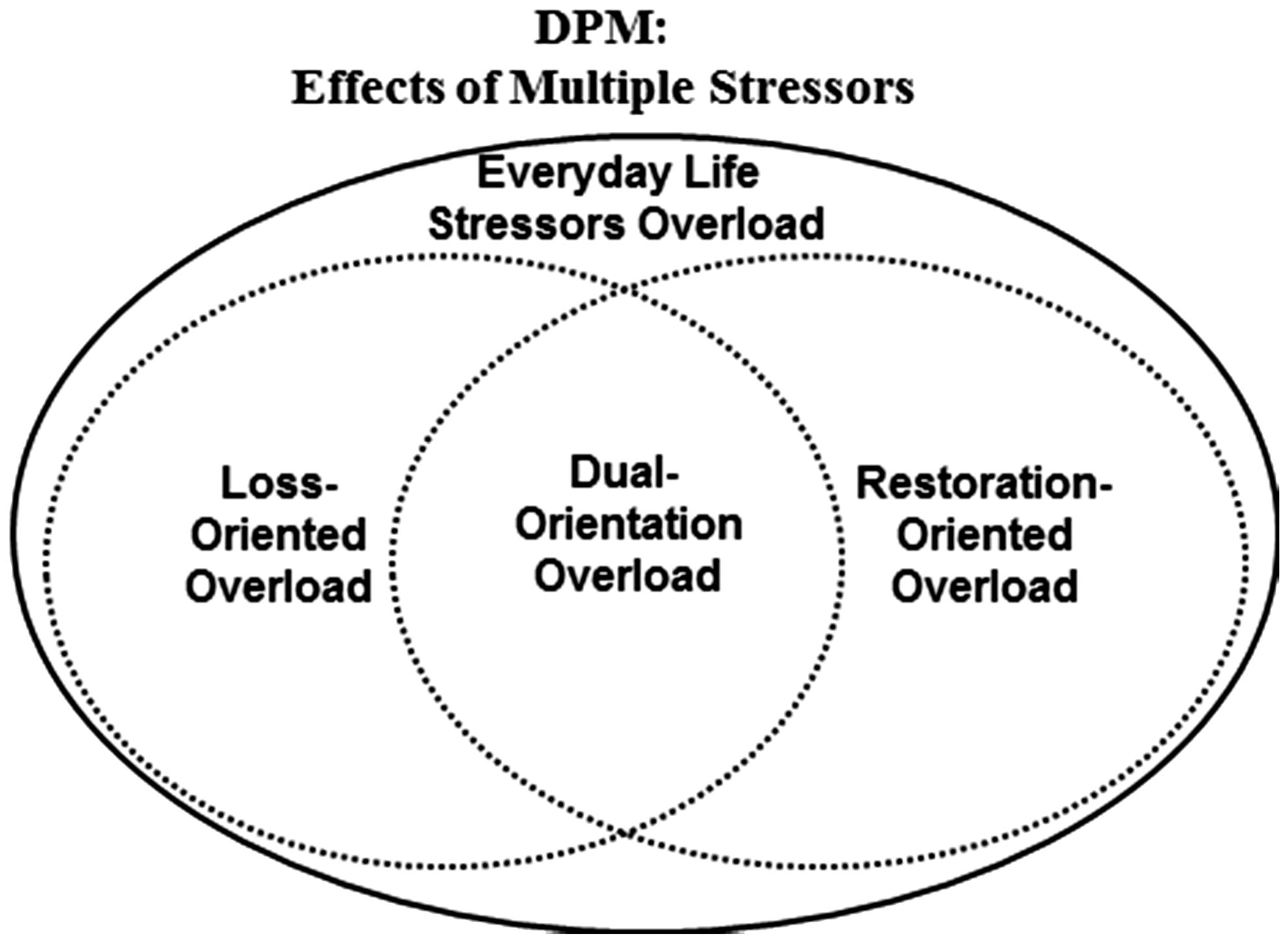
Coping With Overload
The original DPM focused on the process of confrontation avoidance of stressors and the need for balance—emotion regulation—between the LOs and ROs, described as the need for oscillation. However, although relevant, this oscillation process may not be an adequate description of how bereaved people deal with overload. It may not make a lot of difference to adaptation if one simply switches from one source of stress to another. If a person experiences stressor overload, taking action to gain control over the overload would seem necessary. How does one go about this? Different lines of research give clues. One line of thinking involves the concept of the bereaved person becoming directive in order to gain control regarding the stressors. The work of Dyregrov and Dyregrov (e.g., 2008) is relevant. They describe what they call openness, an assertion of personal needs This word implied sincerity, honesty and direct speech, so that to a large extent it was a matter of giving clear signals to their surroundings … such signals were an important means of informing others of what had happened, how they were feeling, the type of support needs they had and how others best could support them. (Dyregrov & Dyregrov, p. 118)
Overload and Health
The original DPM described the forms of complicated grief outlined earlier (chronic, absent, and traumatic grief). Inclusion of the concept of overload necessitates broadening the scope of the DPM to cover the wider range of mental and physical health consequences, ones which have actually been well established as consequent to bereavement (Stroebe et al., 2007). Overload not only brings about feelings of disturbed well-being, upset, and anxiety, but like other stressful situations, it is also linked to various other mental and physical ailments and disorders (see Figure 4). For example, burnout (characterized by emotional and physical exhaustion, cf. Schaufeli, Leiter, & Maslach, 2009) would seem to be a possible outcome relating to overload. Future research could usefully examine the extent to which overload during bereavement is associated with the complex, varied reactions descriptive of burnout (e.g., negative attitudes to work/life, chronic fatigue/depletion of energy, disparagement of self/others, cynicism, sense that nothing really matters, helplessness/hopelessness).
Grief complications and the missing link in the DPM: Additional effects of overload.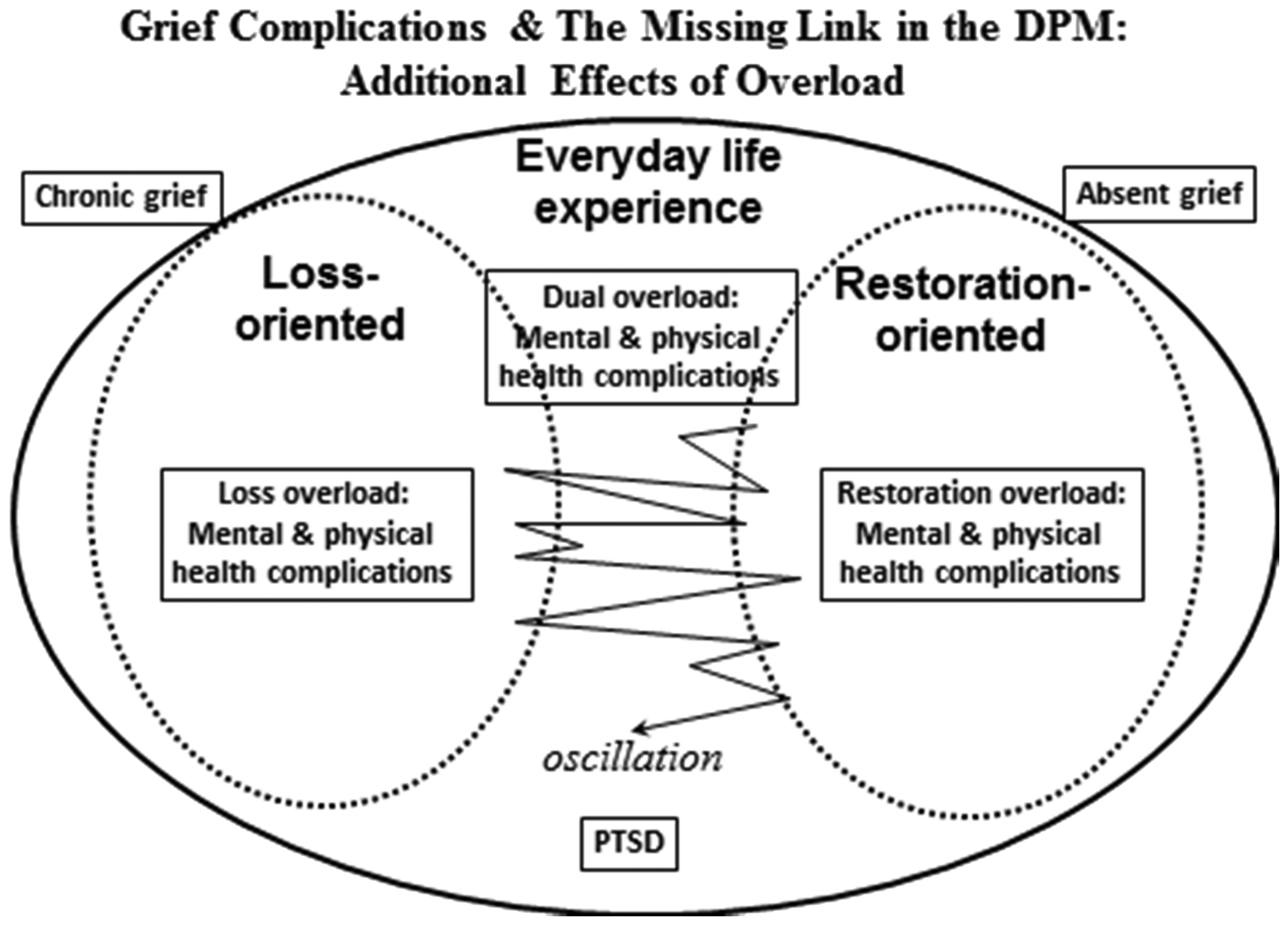
So integration of overload in the DPM actually enables representation of consequences beyond grief complications, some of which we already know to be associated with loss of a loved person, and at least one other that has not, to our knowledge, yet been highlighted.
Conclusions
To summarize, overload is a concept familiar in organizational psychology (role, job, and work overload), but it has been largely neglected in the field of bereavement research, neither being incorporated within the original DPM nor—to our knowledge—within any other model of coping with this stressful life event. The identification of this missing link does not negate the importance of the original premises of the DPM but rather adds to the model’s scope. While we had originally argued the case for inclusion of two types of stressor, loss- and restoration-oriented, we now not only describe the need to attend to each of these but also draw attention to the possibility that such stressors may accumulate in a way that is too much to manage. We had originally also given little attention to everyday life stressors; after all, nonbereaved persons experience these as well, they are not special to bereavement. However, once one considers the possibility of overload, these become particularly salient too. The fact that one has a demanding job may be manageable under normal circumstances but may be overwhelming when bereavement occurs.
Likewise, we had originally argued the case for oscillation between the two types of stressor. Extension to include the possibility of overload suggests that it may not be enough to regulate emotions, dealing at times with loss, at times with restoration, and also at times taking time off. While such oscillation remains fundamental, what is essential in the case of overload is control over the stressors—efforts need to be made to reduce their impact. A number of ways have been suggested (building on earlier approaches) as to how bereaved people can profitably go about dealing with them. In our view, Dyregrov and Dyregrov’s (2008) concept of openness is a viable suggestion for addressing overload, as indicated earlier. The bereaved person can be encouraged to be direct, frank, and honest about his or her needs; supporters need to learn to listen, understand, and respond appropriately. While in practice it may not always be so simple, it is not hard to see how a strategy of openness could help a bereaved person to say no, controlling his or her level of burdens and more effectively managing to cope with the different types of stressors.
The nature of stressors causing overload in bereavement needs to be more finely worked out. Perhaps one can begin to understand the nature of stressors and overload by inventorizing a bereaved person’s perception of what he or she has currently to deal with, and whether he or she feels able to cope with these. (Leading questions could be: “Was there anything that happened to you recently that felt like it “broke the camel’s back?”. The list (either generated by the person or from a stressor list derived from personal and professional reports, compiled by the investigator) could include the various types of stressors illustrated earlier and assessment of their impact. Adding questions such as the Dyregrovs’ “what has helped you the most to cope with your difficult situation?” should lead to better understanding of effective coping strategies (putting our DPM propositions to the test).
Finally, we need to evaluate the impact of bereavement over time in terms not only to do with complications in grieving itself but also relating to the broader range of mental and physical health (and other) consequences that may be specific to overload. Revision of the DPM to include the concept of overload makes it a more comprehensive taxonomy of what bereaved persons have to deal with, describing a broader range of effective ways that they can go about dealing with them, and deeper understanding of the difficulties experienced in adapting to loss.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.