
Abstract
Prior research has found high levels of distress in parents who experience the death of a child; however, Romanian parents, whose experiences are influenced by the nation’s shared historical trauma, have not been studied. This mixed-methods study found very high levels of distress in a sample of 237 bereaved parents in Romania, primarily women. Specifically, 89% of respondents scored above the clinical cutoff for trauma responses, 66% did so for anxious responses, and 82% did so for depressive responses. Qualitative analyses of respondents’ narratives suggest that, through complex interactions between political, social, and medical systems, the lack of care after the death of a child seems to incite additional distress in parents. These findings warrant further exploration of traumatic grief in Romania, especially in the context of historical and political trauma, and of ways in which support can be provided to grieving parents in this unique cultural milieu.
The death of a child has been shown to result in long-lasting parental grief, often at a greater intensity than is observed in other bereaved populations (Kersting, Brahler, Glaesmer, & Wagner, 2011; Neria et al., 2007). A number of adverse psychosocial outcomes have been noted in bereaved parents, including anxious, depressive, and trauma responses. For instance, in a Norwegian sample, 34% to 52% showed significant trauma responses over a year after the death of a child (Dyregrov, Nordanger, & Dyregrov, 2003). In a Swedish sample, depression and anxiety were more common in parents whose children had died of cancer 4 to 6 years prior than in matched controls (Kreicbergs, Valdimarsdottir, Onelov, Henter, & Steineck, 2004). In a study based in the United States (U.S.), 37% of parents showed significant anxious symptoms, 58% showed significant depressive symptoms, and 42% showed significant trauma responses over 4 years after a child’s death (Cacciatore, Lacasse, Lietz, & McPherson, 2013–2014). In another U.S.-based study of bereaved individuals (primarily parents) seeking grief counseling, intake mean scores were at or above the clinical cutoff indicating significant distress for all measures of anxious, depressive, and trauma responses (Thieleman, Cacciatore, & Hill, 2014). In a Finnish sample of parents attending a peer-support weekend intervention, mean scores were above the clinical cutoff for three trauma response clusters (Aho, Malmisuo, & Kaunonen, 2017).
However, much of the research on grief in bereaved parents comes from Scandinavian and primarily English-speaking countries. Little is known about the experiences of bereaved parents in other countries, and even less is known about the ways in which the experience is nested within a particular sociopolitical context. For example, China’s one-child policy has led to particular difficulties for parents who are unable to have another child (Cao et al., 2013). Parental grief has not been studied in Romania despite the unique experience of historical trauma, including reproductive health policies that have shaped the context in which child death is experienced today. This study sought to measure the extent of trauma, anxious, and depressive responses and explore the lived experiences among bereaved parents in Romania.
Recent Romanian History and Reproductive Health
The communist government of President Nicolae Ceausescu from 1965 to 1989 enacted a number of policies intended to reverse the declining birthrate in Romania and supply a labor force to build the socialist state. These included prohibiting the importation of contraceptives and banning abortion except under a very narrow range of circumstances. Policies were backed up with government surveillance of gynecology units and maternity clinics to investigate suspicions of unauthorized abortion, and those who sought or provided abortions were subject to fines and imprisonment (David & Baban, 1996; Hord, David, Donnay, & Wolf, 1991; Kligman, 1992).
Although many doctors did their best to help women in their care, an atmosphere of fear pervaded and the relationship between health-care providers and women was profoundly impacted by these laws. Pregnant women and those suspected of having past abortions were surveilled or hospitalized to prevent pregnancy loss, women whose infants died after birth were encouraged to record them as being stillborn in order to artificially decrease the infant mortality rate, and physicians in hospitals were subject to repercussions if they treated women after an illegal abortion without notifying authorities (Hord et al., 1991; Kligman, 1992).
These policies were ineffective at increasing the birthrate over the long term; as material conditions in the country worsened, the birthrate dropped further as families tried to avoid having more children (Hord et al., 1991; Kligman, 1992). By 1989, the maternal mortality rate was the highest ever recorded in Europe at 159 deaths per 100,000 live births (Hord et al., 1991). It is estimated that 87% of maternal deaths in 1989 were due to unsafe and illegal abortions sought by women who could neither obtain contraception nor provide for another child; many more women were injured (Hord et al., 1991). The death count of women who died due to complications from illegal abortions was 9,452 between the years of 1965 and 1989 (Kligman, 1992).
Improvements after the overthrow of the Ceausescu government led to the maternal mortality rate dropping by almost half in the following year (Hord et al., 1991). Although there were many steps taken to address the country’s dire social and economic conditions, challenges persisted, including a distrust of the government and its health system. In addition, people had difficulty with cooperation in personal relationships due to the climate of suspicion that had prevailed (Hord et al., 1991; Kligman, 1992).
Despite improvements over the past few decades, Romania continues to have an elevated infant mortality rate compared with other European Union countries at 9.2 deaths per 1,000 in 2013 (Martian, 2015), down from 10.11 in 2012 (Burlea, 2012). Statistics on infant mortality do not include deaths prior to and during birth (stillbirth), of which there were 3.9 per 1,000 births in Romania in 2010 (defined as death at or beyond 22 weeks of gestation or 500 g if gestational age is unknown; Zeitlin et al., 2016). However, despite the importance placed on parenthood, child death is rarely discussed and the loss of a baby “is generally surrounded by silence and assumed guilt in Romanian daily life” (van der Sijpt, 2017a, p. 2).
Child Birth and Death in Romania Today
Even among mothers of healthy infants in Romania, psychological distress may be common. In a cross-sectional study of Romanian women being followed in an obstetrics clinic, over half of the sample (53.8%) met criteria for postpartum depression 6 to 8 weeks after birth compared with the estimates of 10 to 15% of women worldwide (Enatescu et al., 2014). Elevated levels of anxiety were also noted, with 46.3% showing moderate to severe anxiety. Expectations for Romanian women to fill multiple sociofamilial roles and the negative effects of socioeconomic conditions were posited as possible causes for the elevated rates of postpartum depression.
In this cultural context, the death of a child is especially difficult. A recent study based on 15 months of fieldwork and interviews with bereaved Romanian mothers highlighted a number of difficulties for this group, many of which are linked to the legacy of the communist era (van der Sijpt, 2017a). Specifically, prior communist control of health care “instilled a feeling that the uncertain process of reproduction should be put in the hands of medical experts” (p. 4); this belief coexists with growing disillusionment with the national health-care system, often a source of pain for women who lose babies.
Grieving mothers in van der Sijpt’s (2017a) study identified “the destructive role” that both the national health-care system and individual physicians played in either causing the death of their child or in handling the loss, including failing to provide information, delivering bad news without compassion or consideration, and failing to provide follow-up care (p. 4). In Romanian hospitals, children who are born dead are quickly removed from their parents, incinerated, and seldom spoken about again. Parents attempting to hold or take their stillborn children home are required to navigate a number of bureaucratic steps before being allowed to do so, and many are never told that this is an option. The deaths of babies before 26 weeks of gestation are referred to as “abortions” and often no further paperwork is provided. Babies who die after 26 gestational weeks are provided a death certificate without a first name, and children who die shortly after birth often are not issued birth certificates. Regrets related to not having proof of a child’s existence, of not having the opportunity to view a deceased child, and of being unable to bury a child were noted to be common themes (van der Sijpt, 2017a).
Another source of dissatisfaction among bereaved mothers in van der Sijpt’s (2017a) study was the Orthodox Church, which established itself as “a de facto state church” after the fall of the communist regime (p. 6). Within this framework, “unbaptized babies are not entitled to a full funeral service or a proper burial place. . . . At best, they can be buried . . . at the margins of the cemetery and without a usual tombstone” (p. 6). Unbaptized babies and all those who die during or prior to birth are considered to exist in “a ‘dark world’ rather than in heaven” (p. 6). Because stillborn babies are routinely incinerated by the State, most parents do not have the option to bury their child. This causes additional difficulties in a culture that places a high value on commemoration, such as through lighting candles and bringing flowers to the grave. Children who die before age 7 are not given a full burial which may cause additional suffering for their families (van der Sijpt, 2017a).
Despite the end of draconian reproductive policies, van der Sijpt (2017a) found that any public discussion about a baby who died “is generally met with unease, suspicion, and a desire to avoid the topic altogether” (p. 7). Women in this study described being told not to mourn and lacking a public space in which they could discuss their losses. The current study is intended to measure the extent of anxious, depressive, and trauma responses among grieving Romanian parents and to explore their lived experiences, keeping in mind the shared historical trauma and its aftereffects. Anticipating the possible effects of the manner in which child death is routinely handled in Romania today, it was hypothesized that bereaved parents would show high levels of trauma, anxious, and depressive responses.
Methods
This cross-sectional survey was conducted online between June and November of 2013 using Qualtrics software. The survey link was shared through a Romanian organization for bereaved parents. Respondents were recruited through this predominantly female group of more than 500 members and through snowball sampling; the survey was also open to nonmembers of the group. The survey was developed in English and was translated into Romanian by a native Romanian speaker and then back-translated into English by a second native Romanian speaker. Text entry responses were translated from Romanian into English by the first translator. The study was approved by an institutional review board at Arizona State University and approval was also granted by the organization in Romania that advertised the survey. All respondents viewed and indicated agreement with an informed consent letter provided in Romanian.
Sample
The sample consisted of 237 Romanian speakers, primarily women, who completed at least one of the survey’s standardized measures. Although most of the respondents lived in Romania, some lived in other countries when they took the survey. To be included, respondents had to be at least 18 years of age and have experienced the death of a child from any cause. Those who had experienced pregnancy loss (miscarriage) were also included.
Quantitative Methods
Measures
The survey asked questions related to demographics, the loss experience, psychotropic medication use before and after the loss, and help-seeking behaviors postloss. It included two standardized instruments measuring trauma responses, anxious, and depressive symptoms. It included open-ended questions about psychosocial care by providers, interpersonal relationships, and personal stories of loss.
Impact of Event Scale-Revised
The Impact of Event Scale-Revised (IES-R) is a self-report measure with 22 items inquiring about the degree to which trauma symptoms related to an event (in this case, the death of a child) have distressed the respondent over the past 7 days (Weiss & Marmar, 1997). It is scored on a 5-point Likert-type scale in which 0 corresponds to not at all and 4 corresponds to extremely. It has three subscales that mirror Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition diagnostic criteria for posttraumatic stress disorder: intrusion, avoidance, and hyperarousal. An overall mean and subscale mean scores are calculated. A score of 1.5 or above is widely considered to indicate clinically significant trauma symptoms (Creamer, Bell, & Failla, 2003). The IES-R has shown high reliability in samples of bereaved parents; for instance, Cacciatore et al. (2013–2014) reported an α of .95 for the full scale and Thieleman et al. (2014) reported αs of .80 to .92 for the full scale and subscales.
Hopkins Symptom Checklist-25
The Hopkins Symptom Checklist-25 (HSCL-25) is a self-report measure with 25 items inquiring about the degree to which respondents have experienced anxious and depressive symptoms over the past 7 days. It is a shortened version of the original 58-item scale developed by Parloff, Kelman, and Frank (1954) scored on a 4-point Likert-type scale in which 1 corresponds to not at all and 4 corresponds to extremely. An overall mean and anxiety and depression subscale scores are computed. A score of 1.75 or higher has been used to indicate clinically significant symptoms in bereaved parents (Cacciatore et al., 2013–2014; Thieleman et al., 2014). The HSCL-25 has shown high reliability in samples of bereaved parents, with αs for the full scale and subscales ranging from .87 to .96 (Cacciatore et al., 2013–2014; Thieleman et al., 2014).
Statistical Analysis
Qualtrics recorded a total of 426 attempts to take the survey. However, Internet connectivity problems in Romania caused the survey to close before many respondents had completed it; a number of respondents reported this to the Romanian survey contact. Due to the anonymous nature of the survey, it was impossible to determine how many individuals attempted to complete the survey. Out of the total number of attempts, 69.2% completed it. The primary analysis was limited to the 237 individuals who met inclusion criteria and completed at least one of the two standardized measures.
The primary purpose of the statistical analysis was to describe this sample in detail using descriptive statistics, with the expectation that high levels of psychological distress would be observed. Quantitative data were analyzed using the Statistical Package for the Social Sciences, version 25. Scale and subscale scores on the two standardized instruments, the IES-R and HSCL-25, were calculated and used in analyses if at least 50% of the items were answered. Most of the missing data consisted of respondents missing one to three items on these instruments. There was a small percentage of missing data for most of the standardized instrument items (<2% for most IES-R items with a maximum of 3% missing and <4% for most HSCL-25 items with a maximum of 6.3% missing).
Quantitative Results
Demographics
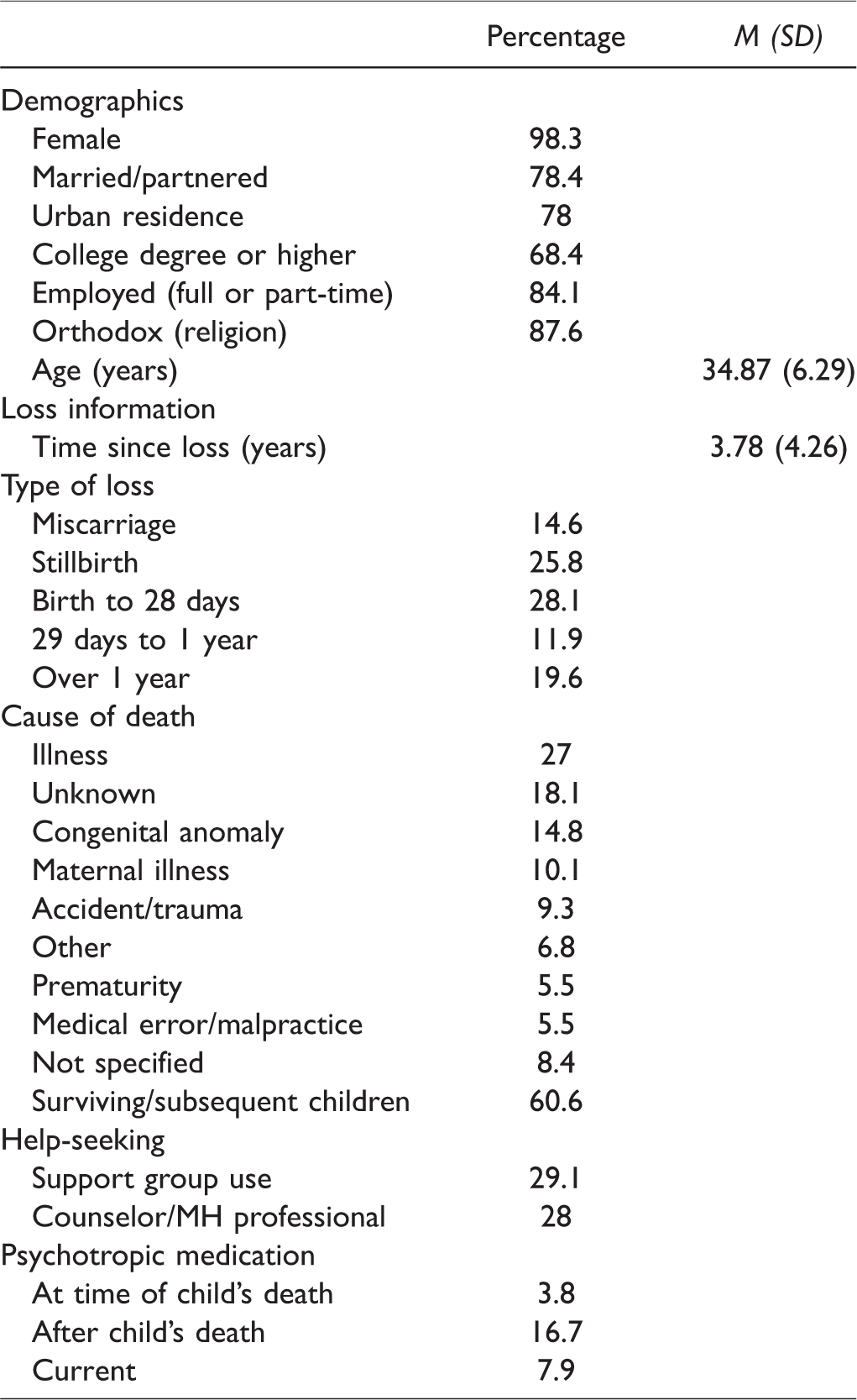
The sample (n = 237) was 98.3% female, with a mean age of 34.87 years (SD = 6.29). In addition, 78.4% indicated they were married or partnered; 68.4% had the equivalent of a bachelor’s degree or higher; 84.1% were currently employed full- or part-time. Religiously, 87.6% identified as Romanian Orthodox.
Loss Experience
All respondents had experienced the death of a child and 3.9% reported the death of more than one child. The most recent loss was used for all analyses. The mean time since the loss was 3.78 years (SD = 4.26), calculated by subtracting the year of the child’s death from the year the survey was taken. The most common age ranges at death were stillbirth (25.8%), neonatal death between 1 to 28 days after birth (28.1%), and infant death between 29 days and 1 year after birth (11.9%).
Respondents were asked to describe their child’s cause of death in their own words which were then grouped into categories. The most common causes of death were illness (27%), unknown (often resulting in stillbirth; 18.1%), congenital anomaly (14.8%), maternal illness (often resulting in stillbirth; 10.1%), and accident/trauma (including birth-related traumas; 9.3%). Only 22.2% of respondents who had experienced stillbirth reported seeing or holding their child, while 73.2% of those who lost an infant or child in a manner other than stillbirth reported doing so (miscarriage excluded); among those who did not see or hold their child, most (83.1%) regretted this decision (miscarriage excluded). Among parents whose children were stillborn, 20.6% reported burying their baby.
Help-Seeking and Medications
Less than one third of the sample reported having ever attended a support group (29.1%) or seeking help from a counseling or mental health professional (28%).Very few respondents (3.8%) reported they were taking psychotropic medications at the time of their child’s death. However, 16.7% reported being prescribed such medications after the death. Among these, 38.5% reported benzodiazepines, 20.5% reported antidepressants, 15.4% reported sleep aids or sedatives, and 15.4% reported nonprescription supplements, while 33.3% could not remember the medication type and 23.1% reported multiple prescriptions either concurrently or sequentially. Prescribing occurred within 1 day of the loss for 29.7%, between 1 day and 1 week postloss for 18.9%, between 1 and 4 weeks postloss for 24.3%, between 1 and 6 months postloss for 16.2%, and after 6 months postloss for 10.8%. Among those prescribed medications, 20.5% reported that they never took the medications, while 30.8% used them for less than a month, 20.5% used them between 1 and 6 months, 12.8% used them for more than 6 months, and 15.4% did not specify the length of use.
At the time of the survey, 7.9% of the entire sample reported currently taking psychotropic medications prescribed to help them deal with their child’s death; in all cases, this was a combination of antidepressants and benzodiazepines. Demographic, loss, and help-seeking data are provided in Table 1.
Demographic, Loss, and Help-Seeking Descriptive Statistics.
Mental Health Functioning
High reliability was found for the full IES-R (α = .91) and two subscales (α = .89 for intrusion, α = .85 for hyperarousal), with lower but fair reliability for the avoidance subscale (α = .68). The mean score was 2.29 (SD = .79) for the full scale, 2.87 (SD = .92) for the intrusion subscale, 1.80 (SD = .76) for the avoidance subscale, and 2.17 (SD = 1.1) for the hyperarousal subscale. In this sample, 83.5% of respondents scored at or above the clinical cutoff of 1.5 on the full scale, 89.4% did so on the intrusion subscale, 67.2% on the avoidance subscale, and 71.1% on the hyperarousal subscale.
The HSCL-25 showed high reliability on the full scale (α = .96) and anxiety and depression subscales (α = .94). The mean score was 2.57 (SD = .81) on the full scale, 2.33 (SD = .87) on the anxiety subscale, and 2.72 (SD = .84) on the depression subscale. In this sample, 78.7% scored at or above the clinical cutoff of 1.75 on the full scale, 67.2% did so on the anxiety subscale, and 82.3% did so on the depression subscale.
A number of independent samples t tests were used to analyze differences within groups based on prior research findings. All distributions used in these analyses approached normal. Group means and standard deviations are provided in Table 2.
Means and Standard Deviations by Analysis.
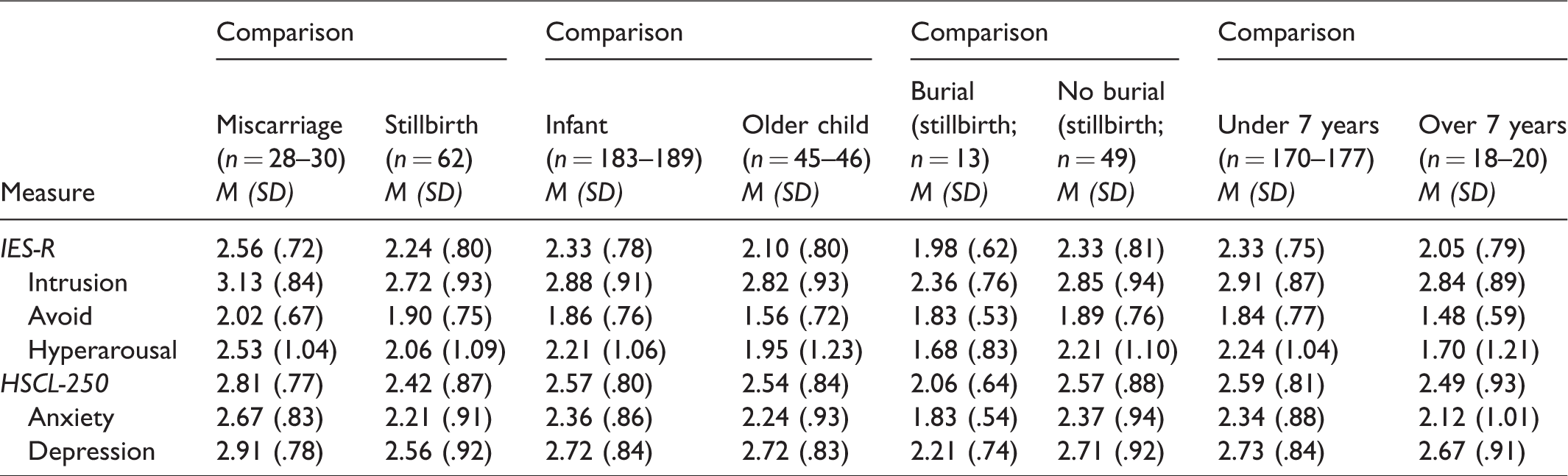
First, scores on the IES-R and HSCL-25 were compared for those who experienced miscarriage versus stillbirth using the definition of stillbirth as occurring at or beyond 22 weeks of gestation. Although various gestational ages have been used to distinguish miscarriage from stillbirth, 22 weeks is the criterion used in calculating the stillbirth rate in Romania (Zeitlin et al., 2016). Prior research in Western countries suggests that miscarriage may have different outcomes and traumatic grief intensity when compared with the death of a child from stillbirth or older children (Brier, 2008; Shreffler, Hill, & Cacciatore, 2012). In this sample, the miscarriage group showed higher scores on all measures; the difference was significant for the IES-R intrusion subscale, t(90) = 2.06, p = .043, 95% CI [0.01, 0.81], with a medium effect size (Cohen’s d = .46), the HSCL-25, t(88) = 2.07, p = .041, 95% CI [0.02, 0.78], with a medium effect size (Cohen’s d = .47), and the HSCL-25 anxiety subscale, t(88) = 2.29, p = .024, 95% CI [0.06, 0.86], with a medium effect size (Cohen’s d = .53).
Second, because the manner in which perinatal death is routinely handled in Romania is painful for many women (van der Sijpt, 2017a), differences between parents who lost a child before or during birth and up to 1 year of age (infant loss) were compared with those who lost a child older than 1 year (older child loss). The infant loss group had higher scores on all measures, indicating greater psychological distress, except the HSCL-25 depression subscale (on which scores were identical); however, the difference was only statistically significant on the IES-R avoidance subscale, t(232) = 2.41, p = .017, 95% CI [0.06, 0.55], with a medium effect size (Cohen’s d = .41).
Third, given the importance of burial in Romanian society, parents whose babies were stillborn were compared based on whether or not they buried their child. Those who buried their child had lower scores on all measures, indicating lower psychological distress than those who did not bury their child; however, the difference was statistically significant only for the HSCL-25, t(74) = −2.0, p < .05, 95% CI [−1.03, −0.003], with a medium effect size (Cohen’s d = .66), and its anxiety subscale, t(29.04) = −2.81, p < .01, 95% CI [−0.93, −0.15], with a medium effect size (Cohen’s d = .70).
Finally, because the Romanian Orthodox Church does not permit full mourning rites for children who die before 7 years of age, Orthodox parents who lost children before age 7 were compared with Orthodox parents who lost children after age 7 (miscarriage excluded). On all measures, parents who experienced the death of a child under 7 years of age had higher scores, indicating greater distress. However, the difference was only statistically significant for the IES-R hyperarousal subscale, t(193) = 2.04, p = .043, 95% CI [0.02, 1.05], with a medium effect size (Cohen’s d = .48).
Qualitative Methods
Using an inductive approach (Braun & Clarke, 2006), qualitative data pertaining to five open-ended questions were thematically analyzed: (a) how respondents were treated by hospital staff around the time of the child’s death, (b) what their experience of holding and seeing a child after death was like, (c) why, in cases of stillbirth, respondents did not bury the baby, (d) how others around them responded to the child’s death and their grief, and (e) how they dealt with the loss (personal story). All responses to these questions were analyzed (n = 103–238), regardless of whether the standardized measures were complete. Every response was read in its entirety twice in order to become familiar with the data. Initial codes were based on narratives found in these data. The primary discrete categories that emerged included: (a) nature and subjective experience around the child’s death, (b) medical and psychological care by providers, and (c) social support. Drilling further into the themes, respondent primary response patterns were thematically analyzed and related ideas were reduced (Braun & Clarke, 2006; Fereday & Muir-Cochrane, 2006).
Qualitative Results
The Nature and Subjective Experience of a Child’s Death
Forty-five of the respondents described their experience as traumatic with subthemes related to: (a) the sociopolitical system, (b) the medical system, and (c) specific details of trauma during the acute loss period. For example, one mother cited national indifference as a contributing factor to the avoidance and cruelty of the medical system which included neglect in care for patients’ physical and emotional well-being: The labor was very painful and I virtually gave birth alone, on a bed. The medical staff was looking at me as if I were already mentally deranged . . . my baby was treated like garbage after her birth. They put (her) in a garbage bag and threw (her) on the scale . . . then I was moved to a room with other four women who had live babies and would go to breastfeed and tell each other about their little miracles. She said, “I’m sorry. We did everything we could for her, but unfortunately, she passed away.” I wanted to die at that moment, I wanted to wake up and realize it was just a bad dream, but the nightmare had turned into reality. I screamed, I saw my husband wallowing and screaming. We gave him a Christian burial, but when I saw him in the coffin, I didn’t have the courage to take him in my arms and take a picture, nobody told me how much I would regret this . . . I didn’t have the strength to think. Ten hours of horrible and excruciating labor and as I gave birth, the female doctor told me not to look at the baby, which makes me feel sorry now, but at the time, I was unaware that I could hold my baby girl, stroke her and cry with her in my arms.
Medical and Psychological Care
Respondents reported negative experiences with medical providers during the acute crisis of their child’s death that seemed to exacerbate their subjective experience of traumatic grief. Almost 40% shared perceived transgressions and negative interactions with medical staff: They threw the baby in a dirty bucket and called him ‘runt.’ I asked to see him and they said ‘there is not to see, it’s ugly.’ (It was) as if he never existed, I wasn’t even given the chance to see or bury my baby. You are young, you will have other babies! No psychological counseling in the hospital! Indifferent; the doctor didn’t have the decency to talk to us directly. On a scale from 1 to 5, I would say 3. A little bit different than they should have or I needed. Still, it was acceptable. They were very close, understanding, compassionate, maybe because it didn’t happen in a maternity, but in a children (sic) hospital. The baby’s treating doctor was always by our side. The personnel was (sic) beyond reproach, they were all extremely humane. The doctor treated me fine, as a patient, my doctor supported me greatly, but the neonatologist showed no compassion, professionalism. In a nutshell, it was horrible because they didn’t treat my baby right, because he had good chances to survive. The doctor ok, the pediatrics nurse ok, the nurse from the new mothers’ ward said “don’t think that I will care for you now that you have no baby!” showing no support whatsoever. From a medical perspective—impeccably, but no empathy whatsoever; they blamed me for losing my baby. I was treated well, but within the boundaries of mediocre thinking in Romania and I say this because they refused to show me my baby girl and pushed me into signing the consent for incineration the very next day, when I was still sedated and they insisted it was best for my mental health. I understood way too late that this was the mistake of my life and I will regret it for as long as I live because I didn’t take my princess home to bury her, although the Orthodox Church doesn’t provide service to unchristian babies.
Social Support
When asked what helped them to cope with their babies’ death, respondents overwhelmingly cited family support as significant sources of support: The experience was difficult on me and my husband, but it brought us even closer together and proved that we were stronger than we thought. It was painful, even atrocious, but day by day, my husband was by my side, giving me moral support. They had very diverse reactions, from saying “it is better that he died, otherwise you would have suffered watching him struggle,” “you will have another,” as if I lost a shoe, “it was God’s will,” which made me doubt everything and my faith is somewhere, in standby, I haven’t really felt them by my side, they all behave as if this tragedy never happened. Why am I crying all the time, because there is nothing I can do? It hurts that I can’t even mention his name. They cannot understand that I lost a part of me, of my soul and heart, that my life has lost its meaning, that it is hard to move on, regain my self-confidence. Indifference, hiding any trace of empathy. They think that if they minimize the loss, it doesn’t exist anymore. They are not comfortable talking about the baby, it is best if I behave normally, as if nothing happened.
Discussion
This study had two aims: to measure the extent of trauma, anxious, and depressive responses among bereaved parents in Romania and to explore this group’s lived experiences through their responses to open-ended questions focused on psychosocial care by providers, interpersonal relationships, and personal stories of loss. Both quantitative and qualitative findings suggest high levels of psychological distress, specifically trauma, anxious, and depressive responses, an average of almost 4 years after a child’s death.
On the IES-R, measuring trauma responses, mean scores were above the clinical cutoff for the full scale and the intrusion, avoidance, and hyperarousal subscales. In addition, the full scale mean score was substantially higher than the mean score in a similar U.S. study with a slightly longer mean time since the loss (Cacciatore et al., 2013–2014). Romanian mean trauma scores were also slightly higher than those of a treatment-seeking sample in the U.S. comprised primarily of bereaved parents (Thieleman et al., 2014), excepting the hyperarousal subscale, where the Romanian mean score was marginally lower. The higher levels of distress in the Romanian sample are notable, given that they had a mean time since the loss more than twice as great as that of the treatment-seeking sample. Compared with a Finnish sample (Aho et al., 2017), where the majority had experienced bereavement in the past year, the Romanian sample had a higher mean intrusion score, a similar hyperarousal score, and a lower avoidance score. Over four fifths of the Romanian sample scored at or above the clinical cutoff on the full scale, a figure almost twice that noted in the U.S. study (Cacciatore et al., 2013–2014), and over two-thirds of the sample scored above the cutoff on each of the three subscales.
On the HSCL-25, measuring anxious and depressive responses, the mean scores were above the clinical cutoff for the full scale and the anxiety and depression subscales. Mean scores on all three scales were above the means reported in a similar U.S. study (Cacciatore et al., 2013–2014). Romanian mean scores were also higher than those in a U.S. treatment-seeking sample for the full scale and depression subscale and identical on the anxiety subscale (Thieleman et al., 2014), showing prolonged distress. Overall, almost four fifths of the Romanian sample scored at or above the clinical cutoff on the full scale, compared with one-half in a U.S. study (Cacciatore et al., 2013–2014); a greater percentage of the Romanian sample also scored above the cutoff for the anxiety and depressive subscales relative to the U.S. sample.
Romanian parents who experienced miscarriage showed significantly higher scores on the IES-R intrusion subscale, the HSCL-25, and the HSCL-25 anxiety subscale. These higher levels of distress may be due to the way in which miscarriage is conflated with selective abortion in Romanian culture (van der Sijpt, 2017a). One bereaved mother who participated in this study noted that miscarriages and abortion are treated with the same cultural shaming and language in Romania, and that women who miscarry are treated as sinners, as are women who elect to have an abortion.
Parents who experienced perinatal death (stillbirth and up to 1 month of age) showed significantly higher avoidance scores than parents who lost older children and slightly higher scores on all but one other measure of psychological distress. Higher trauma scores in parents who lose younger children may represent the internalization of cultural norms that endorse avoidance through social shame, delegitimization (van der Sijpt, 2017a), and rescinding of full mourning rites. Those who reported an opportunity to bury their stillborn child showed significantly lower scores on the HSCL-25 and its anxiety subscale, and nonsignificantly lower scores on all other measures. These findings suggest that the ability to engage in final disposition rituals may help alleviate distress in parents who experience stillbirth.
Orthodox parents whose children died before 7 years of age, the age at which the Church permits full mourning rites, showed significantly higher hyperarousal scores when compared with parents who lost older children and nonsignificantly higher levels of distress on all other measures. It is possible that social attitudes toward the child who died, that is having a child’s life and death fully recognized in a religious context, may also help reduce stressors associated with child death.
Help-seeking was lower in this sample than in a similar U.S.-based sample (Cacciatore et al., 2013–2014), with less than one-third seeking support from either a mental health professional or a support group. While in the hospital, under 13% reported seeing a counselor. By comparison, 42.3% in the U.S. sample attended support groups, while 53.5% had sought help from a counselor or mental health professional. These findings are likely related to the Romanian sociopolitical culture; as van der Sijpt (2017a) noted, while physicians recognize the need for psychological care after the death of a child, they do not feel they have the time or resources to provide it. In addition, many women view support groups with suspicion, fearing hidden agendas, an attitude noted to be “typically Romanian,” and growing out of experience under the former communist regime (van der Sijpt, 2017a, p. 8).
A very small number of Romanian parents reported being prescribed psychotropic medications before their child’s death. However, a trend of increased prescribing in the days and weeks after the death of a child, noted elsewhere (Lacasse & Cacciatore, 2014), was observed. Among those prescribed medications after a child’s death, almost half reported that this was within 1 week of the loss. However, almost half of those who received prescriptions postloss reported never taking the medications and some respondents included herbal supplements, making the rates of psychotropic medication use even lower. At the time of the survey, 7.9% were currently taking medications, lower than the rate reported in a U.S. sample (Cacciatore et al., 2013–2014).
The qualitative analysis of parents’ narratives suggests that the quantitative findings of significant distress can be related to social attitudes toward grief, the medical and psychological care provided during the acute crisis of their child’s death, and their personal and subjective experiences of loss. van der Sijpt (2017b) found that grieving Romanian mothers “share critical attitudes toward the biomedical, religious, and political establishments in their country,” while they “lament the neoliberal health-care reforms, the increasing ideological influence of the Orthodox Church, and a pervasive societal silence around reproduction that—in their view—make the experience . . . even worse” (p. 1). Of particular interest in this sample is that many grieving parents expressed being further traumatized by uncaring medical providers. One respondent linked this to a macro system of indifference and a prior study linked “a legacy of communist oppression” to the silence around perinatal death (van der Sijpt, 2017a, p. 10).
Evident in the narratives of these bereaved parents is the experience of disenfranchised grief, which occurs when individuals “incur a loss that is not or cannot be openly acknowledged, publically mourned, or socially supported” (Doka, 1989, p. 103). This is especially true for parents whose babies died before, during, or shortly after birth in a culture in which perinatal death is treated as anathematic and “children that (sic) show no sign of life upon birth are immediately taken away, and are rarely mentioned or shown to the parents afterwards” (van der Sijpt, 2017a, p. 4). In addition, those who experienced late miscarriages face additional stigma by having their losses conflated with elective abortion, considered sinful by the Romanian Orthodox Church.
These findings converge with those of van der Sijpt (2017a) depicting intense dissatisfaction and resultant emotional pain regarding how child death is handled in Romania. These findings call for further investigation into ways in which the care provided to parents during and after a child’s death can be improved, taking into consideration the country’s unique sociopolitical history and current cultural values. For instance, using respectful and sensitive language following a baby’s death and allowing parents to hold, see, and bury an infant could help reduce additional psychological distress, as could the provision of psychological care in the hospital. Likewise, providing outlets for parents to share their experiences and openly express their grief could help counter the tendency to avoid and minimize grief noted by many participants.
Limitations
This study was conducted with a convenience sample; participants cannot be considered to be representative of bereaved parents in Romania. There may be significant differences between individuals who choose to participate in a study on child death and those who do not, particularly in a cultural context in which perinatal death is such a sensitive topic. In addition, as is the case with the majority of bereavement research, the sample was mostly female; the perspective of Romanian fathers may be different and is, as yet, unstudied. Finally, in some cases, the sample sizes used in analyses were small, and these findings should be interpreted with caution.
Further limitations arise from the fact that the survey was translated into Romanian and back-translated into English. Although both standardized measures generally had high internal consistency, it is possible that some items were not interpreted as intended by respondents, leading to inaccurate results. However, respondents’ own words regarding their experience suggest high levels of psychological distress.
Conclusion
These findings suggest a high degree of psychological distress in parents, particularly mothers, after the death of a child in Romania. Qualitative findings confirm much of what was noted in van der Sijpt’s (2017a) study, as respondents noted the role of the sociopolitical and medical system in causing additional emotional pain and trauma around the death of their child. Respondents also described inhumane treatment of their deceased children, being unable to hold and see them, feeling pressured to consent to incineration, having their experience of loss minimized by others in both medical and social milieus, and the perception of cruelty or indifference in health-care providers. Many parents also noted indifference and avoidance from their families and communities, reflecting cultural norms around perinatal death (van der Sijpt, 2017a). These findings warrant further exploration of traumatic grief in Romania, especially in the context of historical and political trauma, and of ways in which support can be provided to grieving parents in this unique cultural milieu.
Footnotes
Acknowledgments
The authors wish to thank Dana Timotin for her translation services, the families of E.M.M.A. and their beloved children, and all the grieving parents who participated and shared their experiences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.