
Abstract
This study focuses on college students’ experiences and beliefs, which affect attitudes toward assisted dying. Of 324 students, 35% wanted the option of assisted dying for a family member with a life-threatening illness. Results of multiple logistic regression indicate students who favored assisted dying were significantly influenced by having a family member die, experiencing hospitalization, thinking about end-of-life issues, and being comfortable with palliative care. Belief in an afterlife and being a caregiver were negatively associated with assisted dying. Students need to receive training in end-of-life care issues, as increasingly professionals will face such requests.
California is the fifth state to enact an aid-in-dying law, which went into effect June 9, 2016. With the passage and attempted repeal of the California End of Life Option Act, attitudes toward assisted dying are polarized. Many professions are impacted by the right to die law and interest in attitudes regarding assisted dying are important for public policy development and for those teaching in health care and related fields. The purpose of this study is to better understand the personal experiences and beliefs affecting college students’ attitudes toward assisted dying.
Much of the literature assessing student attitudes toward physician-assisted death, euthanasia, and the right to die has focused on students in health-care fields, such as nursing and medicine (Margalith, Musgrave, & Goldschmidt, 2003; Ozcelik, Tekir, Samancioglu, Fadiloglu, & Ozkara, 2014) . Often vignettes or questions are designed to manipulate patient characteristics in order to determine at what point attitudes toward physician-assisted death becomes acceptable (Bevacqua & Robinson Kurpius, 2013; Margalith et al., 2003; Stephens, Neal, & Overman, 2014; Weiss & Lupkin, 2009).
College students given scenarios on critically ill persons were more likely to shorten the life spans of older adults than they were for college age students (Stephens et al., 2014). Similarly, counseling students were more supportive of euthanasia for a 77-year-old with a life-limiting condition than a 25-year-old (Bevacqua & Robinson Kurpius, 2013). The authors hypothesized that the students were unable to relate to the older adults, and this influenced their likelihood of reducing life span.
Other studies on college students’ attitudes regarding euthanasia or the right to die have consistently indicated that several factors correlate with a higher acceptance or endorsement of assisted dying. These factors include, a more liberal viewpoint or affiliation with the Democratic Party, personal experiences with death, not identifying as religious, and identifying as White (Butt, Overholser, & Danielson, 2003; Horsfall, Alcocer, & Polk, 2001; Weiss, 1996; Weiss & Lupkin, 2009; Westman, Hunt, Cicillini, & Lewandowski, 1999).
Students in the health-care field or even practicing clinicians may not be comfortable with assisting in a death. Margalith et al. (2003) found among nursing students half were against legalizing physician-assisted death. Kranidiotis, Ropa, Mprianas, Kyprianou, and Nanas (2015) found nurses who expressed religious beliefs were less likely to be comfortable with assisted death. Similarly, counseling students who identified as religious were less accepting of euthanasia; however, those who had more clinical experience were more accepting of euthanasia (Bevacqua & Robinson Kurpius, 2013). Kopp (2009) found in a study of the general population, persons who were familiar with the legal options of physician-assisted death were less supportive of the practice.
Clinical students identified end-of-life issues as a major ethical dilemma affecting their profession. The authors suggest integrating student perspectives into the learning experience in order to address ethical issues that will arise in health-care professions (Buelow, Mahan, & Garrity, 2010). According to De Leo, Hawgood, and Ide (2012), 85% of undergraduate medical students they surveyed were interested in having assisted dying and right to die issues included in their curriculum. The need for undergraduate education on quality of life and right to die issues is globally urgent. Understanding individual factors, which influence the right to die, allows for developing curriculum sensitive to learners’ needs and understanding that not all will be comfortable with assisted dying.
This study differs from most studies of college students in that respondents were randomly selected from the general student population, vignettes were not used to determine right to die attitudes, and factors measuring family experiences with death and hospitalization were included as predictors. Understanding factors that influence college students’ beliefs about the right to die should inform college curriculum, as many student career trajectories will be in health and human services. This study adds to the slowly growing literature on death education and attitudes on college campuses.
Method
Participants
Participants were 324 college students. Seventy-one percent were female. Eighty-two percent were undergraduate, 12% graduate, and 6% other student categories. The average age of students was 25 years. Regarding ethnicity, 40% of the students identified as Hispanic, 37% as White, 20% as Asian, 6% Black, and 3% Native American, and the remaining 12% identified as other, or one or more ethnicities.
Procedure
Recruitment
The study was approved by the University Institutional Review Board. The survey was piloted in two classes and subsequently shortened for ease of online administration. During the pilot survey, some students were not familiar with the concept of palliative care. The final survey included definitions of palliative care derived from the World Health Organization in the consent form and in the actual survey. In the final survey, analysis not shown, 50% of the students said that they were very familiar with the concept of palliative care (due to course work), and the remaining said that they had some knowledge and with the information we provided felt comfortable answering the questions.
The survey was launched spring 2016 through the online platform, Qualtrics, and sent randomly to 2,500 of the 24,403 enrolled students. An introductory e-mail encouraged students to complete the voluntary survey, and two follow-up e-mails were sent over a 2-week period. Of the 2,500 students who received the invitation, 1,725 (69%) opened the e-mail, 460 read the consent form, 433 consented to take the survey, and 324 (19% of 1,725) fully completed the survey. Students did not receive any form of compensation.
Measures
Dependent variable
Assisted dying was assessed by one question, “If your family member were to have a terminal illness, would you want him or her to have the option of assisted dying?”
Independent variables
Death of a close family member. Death of a family member was determined based on the students’ answer to a question about whether a family member had died within the last 12 months.
Think about end of life care. Students who responded affirmatively to a question, “Do you ever think about end-of-life care?” were coded 1 if yes.
Caregiver status. Caregiver status was determined by the number of hours students provided care to an older family member. If student provided 5 or more hours of direct care, they classified as a caregiver. Examples of direct care include transportation, household chores, assistance with personal care, and general household management.
Belief in afterlife. Students who responded affirmatively to a question asking if they believed there was life after death were coded 1; 0 otherwise.
Hospitalization was coded 1 if the student or a close family member had been hospitalized in the last year.
Comfort with palliative care was assessed with one Likert-type question, “I would feel comfortable asking my health-care provider for more information about palliative care for myself or a loved one.” The question ranged from 1 to 4 with four indicating greater comfort (X = 2.98, standard deviation = .71).
Sociodemographic characteristics. Age in years indicates the students’ chronological age at the time of the survey. Dichotomous variables were gender (female) and race (White was the reference group).
Statistical Analysis
Correlation analyses were performed to examine the bivariate associations among study variables. Predictors of a student wanting a family member to have the option of assisted dying were examined using multiple logistic regression. The data were analyzed with StataIC 10.
Results
Student Demographics
Thirty-eight percent (24 students and 120 family members) had been hospitalized. Only eight students reported both self and family hospitalization. Slightly over a third (35%) of the students wanted their family members to have the option of assisted dying. Nineteen percent reported a death in the family. Forty percent of students reported caring for older family members. Forty-one percent reported thinking of care issues at end of life. Sixty percent reported believing in life after death. Table 1 shows the characteristics of the student respondents, and study variables, including the means and standard deviations for continuous variables, and percentages for dichotomous variables.
Student Demographics and Study Variables (N = 324).
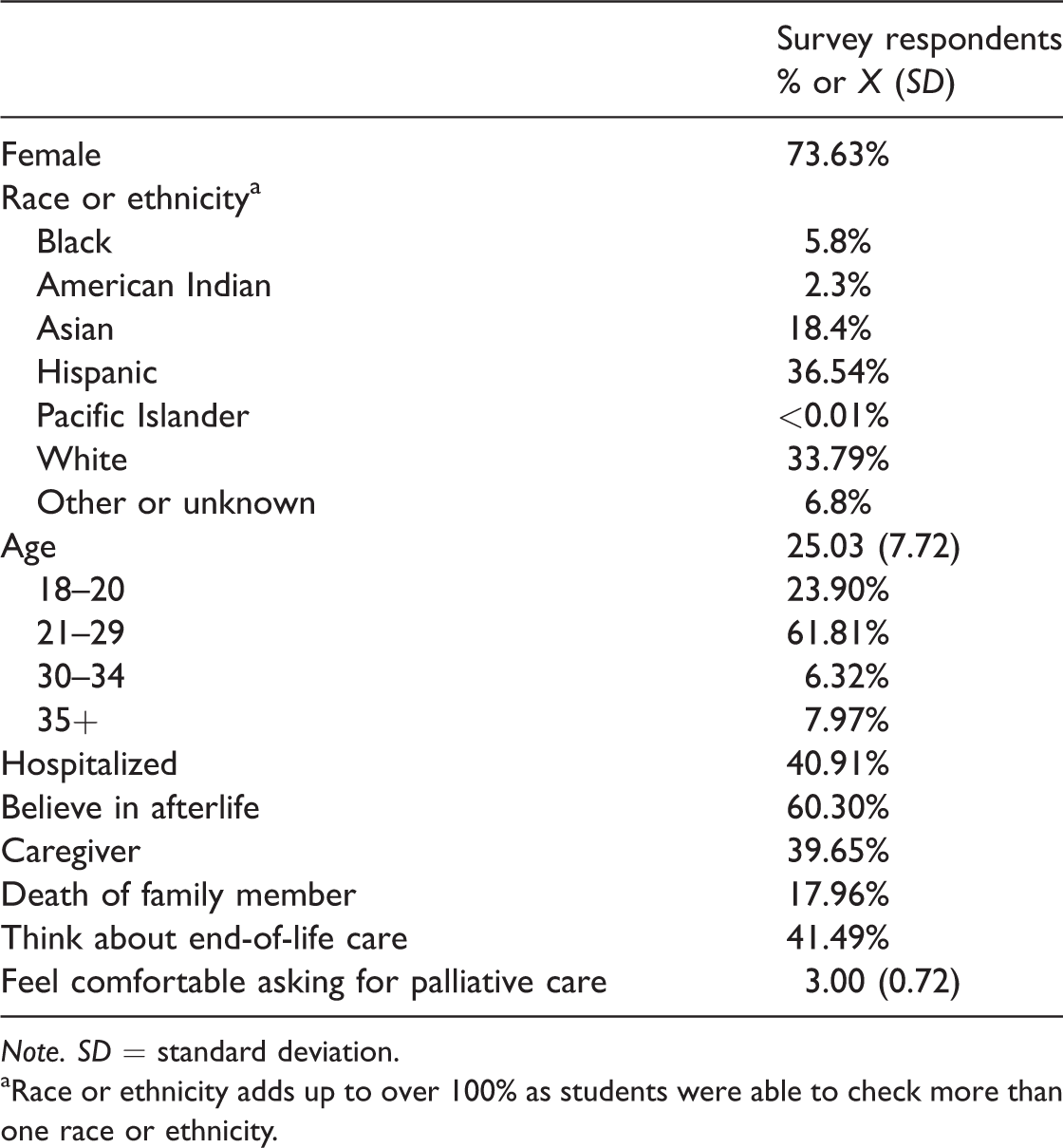
Note. SD = standard deviation.
aRace or ethnicity adds up to over 100% as students were able to check more than one race or ethnicity.
Bivariate Analyses
The results of the bivariate correlation analyses are shown in Table 2. The results indicate that female participants were more likely to be comfortable asking about palliative care and want their family member to have the option of assisted dying. Students who experienced a family hospitalization were more likely to be caregivers, have a family member die, and want the option of assisted dying. Students who felt comfortable asking about palliative care were more likely to think about end-of-life issues and want the option of assisted dying. Belief in life after death and being a caregiver were inversely correlated with wanting the option of assisted dying.
Correlations Among Study Variables (N = 324).
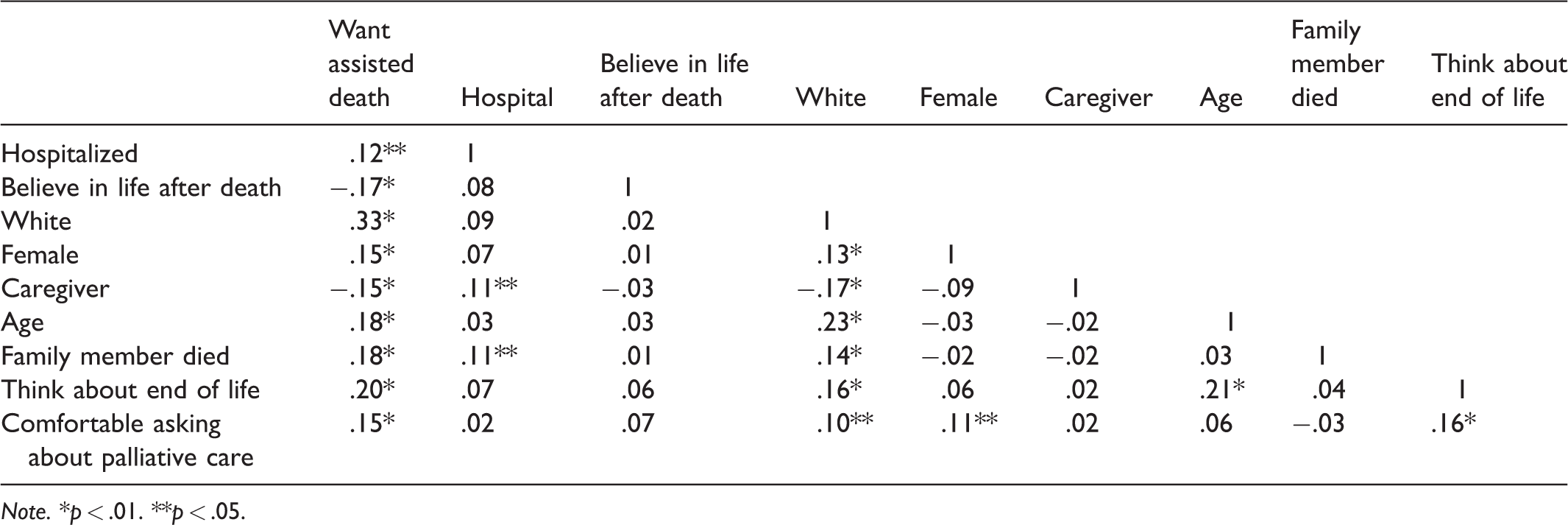
Note. *p < .01. **p < .05.
Multiple Logistic Regression
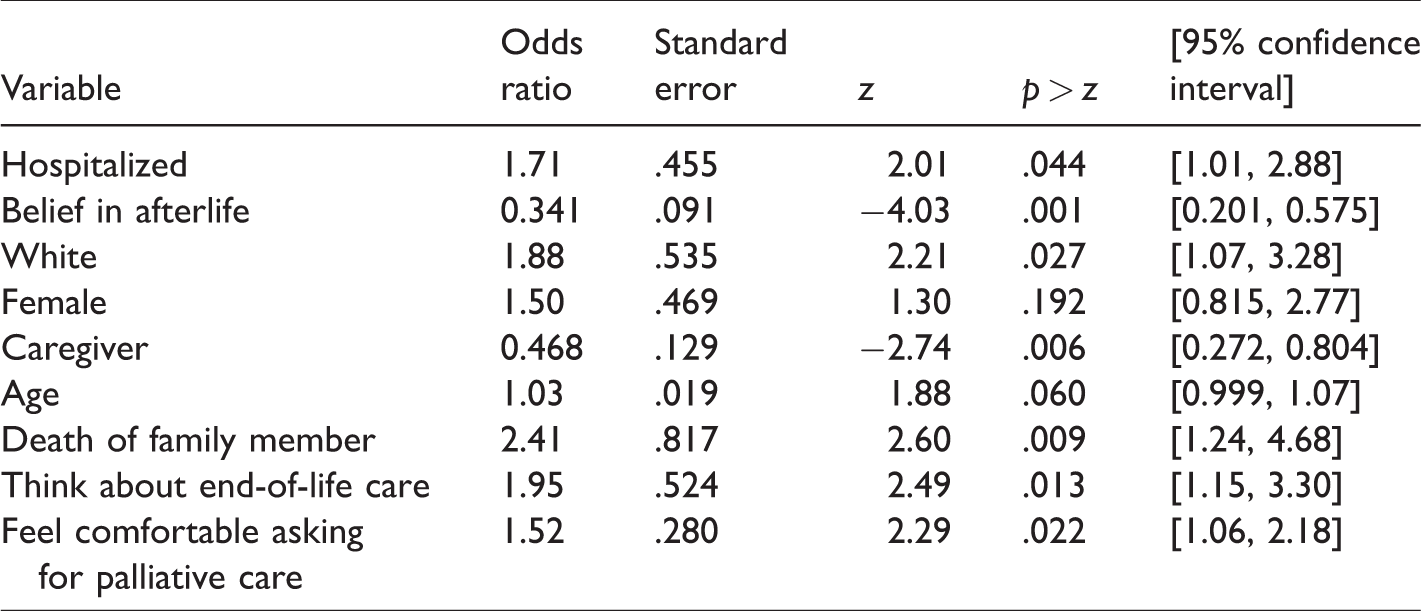
The odds of wanting the right to die are higher for students who are White, who had a family member die in the last year, who experienced hospitalization, who think about end-of-life care, and who feel comfortable asking for palliative care. The odds of wanting the right to die are lower for those who believe in life after death and caregivers. Psuedo R2 = .166, model χ2 = 71.88, df = 9, and p = .001. The results of the multiple logistic regression are in Table 3.
Multiple Logistic Regression Predicting Attitudes Toward Assisted Dying (N = 324).
Discussion
This study focused on understanding how college students feel about assisted dying. Only 35% were in favor of having assisted dying as an option for their family member. Perhaps this number was lower than other studies because the question asked about family and did not use an unknown person in a vignette. White college students were more likely to want their family members to have the right to die than were students from other racial or ethnic backgrounds. This may reflect cultural differences, in particular western European values, which aim at accommodating patients’ wishes over family wishes.
As this survey was administered before the End of Life Option Act was enacted, none of the students’ experiences with death involved assisted death. The finding that students who experienced a death in the family were more likely to want the option of the right to die, could indicate the students’ perception that end-of-life care lacked quality and comfort care. One interpretation could be that their experience with death was negative, and they would want their loved ones in the future to have the choice of assisted dying. Similarly, students who thought about end-of-life issues and who had the experience of hospitalization were also more likely to want the option of assisted dying. Future research should examine how the experience with a family member who has died influences attitudes toward assisted death.
Students who believed in an afterlife had lower odds of wanting the option of assisted death for family members. This may reflect religious beliefs, as many religions prohibit suicide and assisted dying. Student caregivers also had lower odds of wanting assisted death for family members. This may be because the caring relationship has increased emotional attachment they feel toward their older family members, where they could not imagine the loss. Caregiving could also indicate the students’ willingness to provide care, even as their loved one’s health condition worsens. Similarly, Newsome and Dickinson (2000) found over 77% of college students wanted to care for their hypothetical terminally ill parent at home.
This study examines attitudes toward assisted dying in a general college student population. Nevertheless, as in any cross-sectional study, interpretations of causality must be made with caution. A survey that included detailed questions on religious beliefs or experiences with the health-care system would allow for additional explanatory variables. For example, 9% of all students who had a family member hospitalized also had a family member die in the past year. However, the survey did not contain a question asking if the hospitalized family member died during hospitalization.
Attitudes toward assisted dying will continue to change as Californians become more familiar with, and perhaps have family members who use the End of Life Option Act. Understanding college students’ beliefs about assisted dying should inform and be incorporated into college curriculum as many students are embarking on career trajectories that will take them into the health and human service sectors. Increasingly shared decision-making or family centered models in decision-making are emerging as a form of practice. In part because the health-care system has grown so complex, family members are needed to understand and give input into the array of medical treatment and care options. Incorporated into palliative care curriculum should be ethical discussions, which will help students gain a foundation for working with complex issues surrounding the medical needs, emotional needs, and spiritual needs persons experience in end-of-life transitions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.